caregiver negative affect is a primary determinant of caregiver report of pediatric asthma quality...
TRANSCRIPT
Caregiver negative affect is a primarydeterminant of caregiver report of pediatricasthma quality of lifeMarcella R. Price, MSPH*; Donna L. Bratton, MD*† and Mary D. Klinnert, PhD*†
Background: Quality of life has increased in popularity as an outcome measure in health research. However, the measurementof quality of life has been questioned on methodologic grounds, as it often shows little association with objective measures ofdisease status.Objective: For this report we studied the determinants of pediatric asthma caregiver report of quality of life and its relationship
to disease burden.Method: Ninety-eight children who were admitted to a Pediatric Day Program for an asthma evaluation were enrolled in an
outcome study. A complete set of medical records for the 2-year period before and after the admission was collected andsystematically coded for health care utilization. Using the Pediatric Asthma Caregiver’s Quality of Life Questionnaire, data werecollected at baseline, discharge, and year after the admission. Caregiver negative affect (anxiety and depression), measured withthe Brief Symptom Inventory, was also collected at baseline and discharge.Results: Caregiver report of quality of life was unrelated to health care utilization at baseline but instead was significantly
related to baseline caregiver negative affect. A significant relationship between health care utilization and quality of life waspresent at followup. The Emotional Function scale from the quality of life measure can account for most of the relationshipbetween quality of life and negative affect.Conclusions: Caregiver affect may have a considerable influence on report of quality of life. Understanding the individual
characteristics of the respondent is important when using a quality of life instrument as an outcome measure.Ann Allergy Asthma Immunol 2002;89:572–577.
INTRODUCTIONMeasurement of quality of life has gained considerable pop-ularity during the past decade as an important measure ofhealth outcome. Many questionnaires exist which capturechild self-report, adult self-report, and parent report of asth-ma-related quality of life. The popularity of quality of life iseasily understood because, in addition to objective or clinicalmeasures, investigators can demonstrate improvement in diseaseburden as perceived by the patient or caregiver.1–3 As such,quality of life measures are regularly reported to be influencedby clinical, pharmacologic, or psychosocial intervention.4–6Despite the importance of quality of life in the intervention
literature, quality of life is a broad concept that lacks anabsolute definition or a gold standard, and there are method-ologic issues involved in its measurement. First of all, qualityof life scales often correlate poorly or not at all with clinicalor physiologic measures of disease severity.7,8 Second, thereports of validation for these instruments are subject tomethod variance. The same respondent often provides re-
sponses to both the quality of life questionnaire and thevalidating instrument (eg, parent report of quality of life andparent report of disease symptom status).8 In addition, therespondent has expectations and biases that similarly influ-ence their responses to the different measures. The measureswill therefore reflect these biases and are more likely to berelated because of the biases as compared with measurestaken by an alternate method (eg, interviewer observation).9Finally, there are psychosocial factors that may complicatethe measurement of quality of life.1,2 For example, there maybe a tendency for anxiety or recent stressful life events toinfluence how someone would respond to a question. There-fore, quality of life is a subjective health measure that can beinfluenced by a subject’s perceptions, expectations, and in-terpretations about health.To illustrate the influence of psychosocial factors on ques-
tionnaire responses further, it has been shown that negativeaffect (NA) is associated with self-report of poorer medicalcondition.10 Specifically, among adults self-report of qualityof life was inversely correlated with NA (the primary symp-toms being anxiety and depression) in a sample of asthmaticpatients.11 Similarly children’s self-reported anxiety was theprimary predictor for low quality of life in a study of childasthmatic patients.12 This influence on perception of healthstatus is potentially similar with parent-report measures. Withthis in mind, the context in which the quality of life instrumentis being administered is important to recognize because quality
* National Jewish Medical and Research Center Department of Pediatrics,Denver, Colorado.† University of Colorado Health Sciences Center, Denver, Colorado.Funding for this project was provided by NIH General Clinical ResearchCenter grant # M01-RR0051 and the Dr. Scholl Foundation.Received for publication April 13, 2001.Accepted for publication in revised form March 28, 2002.
572 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY

of life is often subject to underlying and unmeasured factors,such as respondent affect, that may confound analysis.For this report we studied the determinants of caregiver
report of quality of life for children with asthma and therelationship between quality of life and objectively measureddisease burden. To this end, we analyzed the data from anoutcome study involving children who were admitted into apediatric day program for evaluation and treatment of severeasthma. We questioned 1) the relationship between quality oflife and the health care utilization in this population and 2)whether caregiver quality of life (CqoL) was influenced byparent affect state. Additionally, we hypothesized that 3) afteraccounting for NA, the relationship between quality of lifeand health care utilization would be more apparent. Corre-lates of quality of life were studied before and after anintensive intervention and at 1 year of followup.
METHODSThe data for this analysis were gathered as part of the Pedi-atric Outcomes Study (POS) which examined the progress ofchildren who were admitted to an intensive pediatric dayprogram for treatment of asthma. The methods and resultsfrom this study are published elsewhere5; however, a briefdescription follows. The institutional review board approvedthis protocol, and informed consent was obtained from allstudy participants.SubjectsFamilies of 114 pediatric patients, who were consecutivelyadmitted to the National Jewish Medical and Research Cen-ter, pediatric day program for asthma refractory to outpatientcare, were eligible for POS enrollment. Entry criteria in-cluded a primary diagnosis of asthma, no admissions toNational Jewish during the previous 5 years, age �19 years,and the presence of a parent or legal guardian at admission.Of the 111 families meeting entry criteria, 13 declined to par-ticipate, resulting in a final study population of 98 patients.Although not an inpatient stay, families were admitted to
the day program and participated in treatment from morninguntil evening, leaving nights and weekends, until discharged(approximately 15 weekdays).ProcedureUpon arrival at National Jewish, caregivers brought a com-pleted initial evaluation questionnaire regarding family de-mographics and their child’s asthma history. Within the first2 days in the day program, the patient and a primary caregivermet a research assistant from the POS. Informed consent wasobtained and the caregivers filled out baseline questionnairesabout themselves and their child. At discharge from the dayprogram, caregivers again filled out questionnaires, and med-ical record release forms were obtained for all medical facil-ities where their child had been seen within the past year.Patient families were contacted by mail or phone for followup1 year after leaving the day program. Again, medical recordrelease forms were obtained for all medical facilities the childvisited during the year since discharge. All medical records
were collected from 1 year before admission through the1-year anniversary of discharge from the day program, thuscollecting 2 full years of patient medical records.MeasuresMedical records outcomes coding. A standardized method ofcoding medical records was used for objective measurementof health care utilization. As the more severe cases of asthmaaccount for the most health care utilization,13 the medicalrecord data were used as a proxy to disease severity andburden. Coding procedures and psychometrics for thismethod are available elsewhere.14 Specifically, each subject’smedical records were coded for every health care encounterover a 1-year period. Encounter categories included: cortico-steroid bursts, asthma-related sick visits to a physician, andasthma-related hospitalizations and emergency departmentvisits. Finally, an asthma episode was counted each time oneof the above visits was coded greater than 10 days apart.Categories were summed across time for a count in eachcategory spanning an entire year. Two individual raters dualcoded 25% of the compiled records to evaluate reliability;interrater correlation coefficients ranged from 0.82 to 0.97(0.66 to 1.0), suggesting very good reliability.Using principle component analysis, two factor scores
were derived from the five utilization categories above, ex-plaining 80% of the variance. The two factor scores, Hospi-tal-based Utilization and Asthma Exacerbations, were used inthe analysis. The Hospital-based Utilization factor includedthe number of hospitalizations and emergency departmentvisits for each patient, whereas the Asthma Exacerbationsfactor had the number of episodes, corticosteroid bursts, andsick visits.CQoLQuality of life was measured by the Pediatric Asthma Care-giver’s Quality of Life Questionnaire.8 This self-report mea-sure has been validated using other health-related quality oflife and child asthma status questionnaires. The CQoL ques-tionnaire includes an Emotional Function (nine questions)and an Activity Limitation scale (four questions). Caregiverswere given this questionnaire to fill out during their initialenrollment into the POS and again at discharge from the dayprogram. The families were then mailed this questionnaire atthe 1-year anniversary of discharge. If a subject did notrespond by mail, the family was called and a telephoneinterview was completed. Higher scores on this measureindicate better quality of life.NACaregiver mental health status was independently measuredusing The Brief Symptom Inventory.15 This is a generalscreening questionnaire that measures cross-sectional mentalhealth status. This questionnaire was administered to thecaregivers both at baseline and at discharge from the dayprogram. The Brief Symptom Inventory has several scales,including Anxiety and Depression. To determine the numberof caregivers in the clinical range of anxiety and depression,
VOLUME 89, DECEMBER, 2002 573
a cut was made at 1.5 standard deviations above the publishedmeans for a nonclinical sample. An NA variable was derivedby averaging the anxiety and depression scales. At baselineand discharge, the NA scores obtained a coefficient � of 0.89and 0.86, respectively. Higher scores on this scale indicateworse NA.Statistical AnalysisBecause of the nonnormal distributions for many of thevariables, data were summarized using the median and range,and the previously derived health care utilization factorscores were used. Spearman correlations were used to test theunivariate relationships between the quality of life, healthcare utilization, and affect variables. Finally, multiple regres-sion analysis was used to test the relationship between CQoLand the utilization variables independent of caregiver NA.CQoL, the dependent variable, was transformed (rank aver-aged) at the followup timepoint to obtain a more normaldistribution for use in the multiple regression. All tests wereconsidered significantly different at P � 0.05.
RESULTSNinety-eight children along with a primary caregiver com-pleted the baseline portion of the POS. Eighty-six of thesecaregivers were the biologic mothers of the child, 10 were thebiologic fathers, and 2 were either a grandparent or a fosterparent. The average age of the participants in the project was11 years with a range of 9 months to 18 years. They were43% female. This cohort was 84% European-American, and25% were insured by Medicaid. The children participated inthe program an average of 15.6 weekdays.Of the 98 families enrolled in the study, complete medical
records were available for 94 of the patients at baseline. Thedischarge session was complete for 86 the families. Finally,83 of the families completed both the followup session andcomplete medical records for the year after discharge.Most of the children in this cohort had severe asthma, with
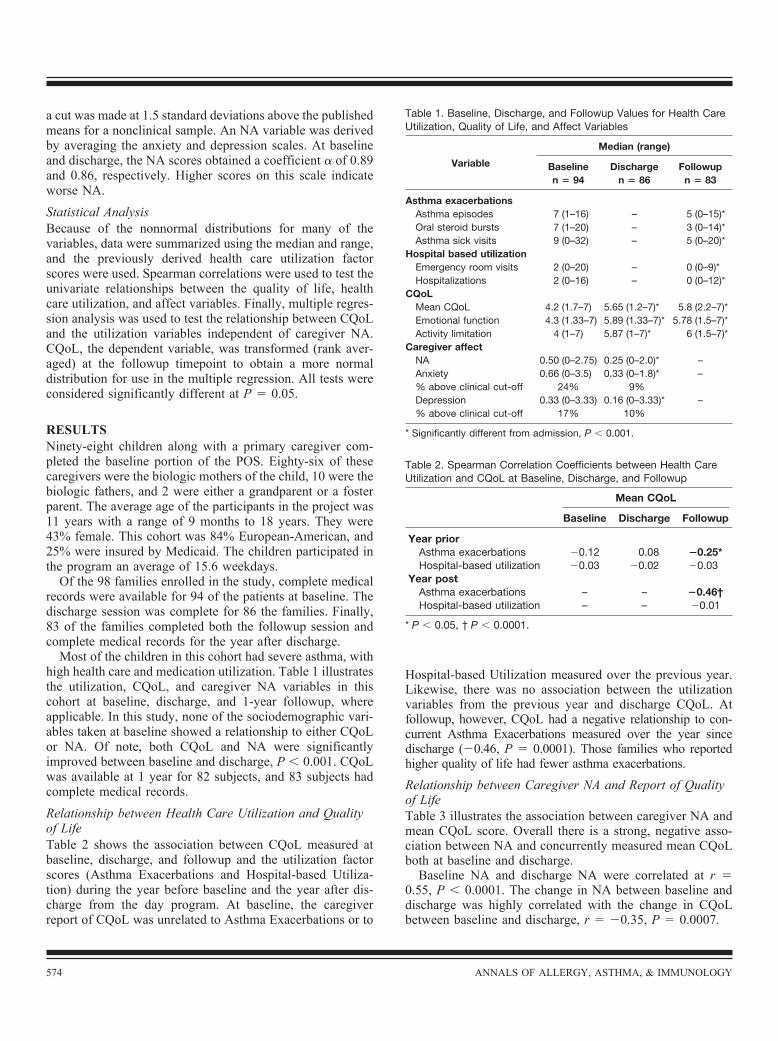
high health care and medication utilization. Table 1 illustratesthe utilization, CQoL, and caregiver NA variables in thiscohort at baseline, discharge, and 1-year followup, whereapplicable. In this study, none of the sociodemographic vari-ables taken at baseline showed a relationship to either CQoLor NA. Of note, both CQoL and NA were significantlyimproved between baseline and discharge, P � 0.001. CQoLwas available at 1 year for 82 subjects, and 83 subjects hadcomplete medical records.Relationship between Health Care Utilization and Qualityof LifeTable 2 shows the association between CQoL measured atbaseline, discharge, and followup and the utilization factorscores (Asthma Exacerbations and Hospital-based Utiliza-tion) during the year before baseline and the year after dis-charge from the day program. At baseline, the caregiverreport of CQoL was unrelated to Asthma Exacerbations or to
Hospital-based Utilization measured over the previous year.Likewise, there was no association between the utilizationvariables from the previous year and discharge CQoL. Atfollowup, however, CQoL had a negative relationship to con-current Asthma Exacerbations measured over the year sincedischarge (�0.46, P � 0.0001). Those families who reportedhigher quality of life had fewer asthma exacerbations.Relationship between Caregiver NA and Report of Qualityof LifeTable 3 illustrates the association between caregiver NA andmean CQoL score. Overall there is a strong, negative asso-ciation between NA and concurrently measured mean CQoLboth at baseline and discharge.Baseline NA and discharge NA were correlated at r �
0.55, P � 0.0001. The change in NA between baseline anddischarge was highly correlated with the change in CQoLbetween baseline and discharge, r � �0.35, P � 0.0007.
Table 1. Baseline, Discharge, and Followup Values for Health CareUtilization, Quality of Life, and Affect Variables
Variable
Median (range)
Baselinen � 94
Dischargen � 86
Followupn � 83
Asthma exacerbationsAsthma episodes 7 (1–16) – 5 (0–15)*Oral steroid bursts 7 (1–20) – 3 (0–14)*Asthma sick visits 9 (0–32) – 5 (0–20)*
Hospital based utilizationEmergency room visits 2 (0–20) – 0 (0–9)*Hospitalizations 2 (0–16) – 0 (0–12)*
CQoLMean CQoL 4.2 (1.7–7) 5.65 (1.2–7)* 5.8 (2.2–7)*Emotional function 4.3 (1.33–7) 5.89 (1.33–7)* 5.78 (1.5–7)*Activity limitation 4 (1–7) 5.87 (1–7)* 6 (1.5–7)*
Caregiver affectNA 0.50 (0–2.75) 0.25 (0–2.0)* –Anxiety 0.66 (0–3.5) 0.33 (0–1.8)* –% above clinical cut-off 24% 9%Depression 0.33 (0–3.33) 0.16 (0–3.33)* –% above clinical cut-off 17% 10%
* Significantly different from admission, P � 0.001.
Table 2. Spearman Correlation Coefficients between Health CareUtilization and CQoL at Baseline, Discharge, and Followup
Mean CQoL
Baseline Discharge Followup
Year priorAsthma exacerbations �0.12 0.08 �0.25*Hospital-based utilization �0.03 �0.02 �0.03
Year postAsthma exacerbations – – �0.46†Hospital-based utilization – – �0.01
* P � 0.05, † P � 0.0001.
574 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
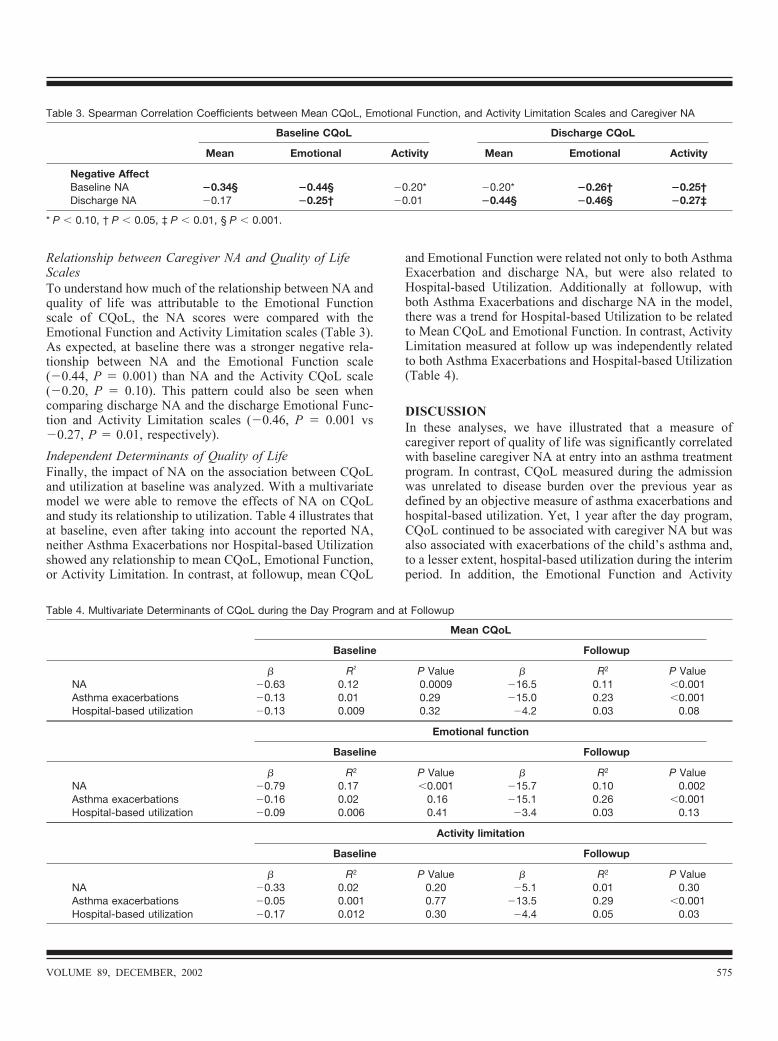
Relationship between Caregiver NA and Quality of LifeScalesTo understand how much of the relationship between NA andquality of life was attributable to the Emotional Functionscale of CQoL, the NA scores were compared with theEmotional Function and Activity Limitation scales (Table 3).As expected, at baseline there was a stronger negative rela-tionship between NA and the Emotional Function scale(�0.44, P � 0.001) than NA and the Activity CQoL scale(�0.20, P � 0.10). This pattern could also be seen whencomparing discharge NA and the discharge Emotional Func-tion and Activity Limitation scales (�0.46, P � 0.001 vs�0.27, P � 0.01, respectively).Independent Determinants of Quality of LifeFinally, the impact of NA on the association between CQoLand utilization at baseline was analyzed. With a multivariatemodel we were able to remove the effects of NA on CQoLand study its relationship to utilization. Table 4 illustrates thatat baseline, even after taking into account the reported NA,neither Asthma Exacerbations nor Hospital-based Utilizationshowed any relationship to mean CQoL, Emotional Function,or Activity Limitation. In contrast, at followup, mean CQoL
and Emotional Function were related not only to both AsthmaExacerbation and discharge NA, but were also related toHospital-based Utilization. Additionally at followup, withboth Asthma Exacerbations and discharge NA in the model,there was a trend for Hospital-based Utilization to be relatedto Mean CQoL and Emotional Function. In contrast, ActivityLimitation measured at follow up was independently relatedto both Asthma Exacerbations and Hospital-based Utilization(Table 4).
DISCUSSIONIn these analyses, we have illustrated that a measure ofcaregiver report of quality of life was significantly correlatedwith baseline caregiver NA at entry into an asthma treatmentprogram. In contrast, CQoL measured during the admissionwas unrelated to disease burden over the previous year asdefined by an objective measure of asthma exacerbations andhospital-based utilization. Yet, 1 year after the day program,CQoL continued to be associated with caregiver NA but wasalso associated with exacerbations of the child’s asthma and,to a lesser extent, hospital-based utilization during the interimperiod. In addition, the Emotional Function and Activity
Table 3. Spearman Correlation Coefficients between Mean CQoL, Emotional Function, and Activity Limitation Scales and Caregiver NA
Baseline CQoL Discharge CQoL
Mean Emotional Activity Mean Emotional Activity
Negative AffectBaseline NA �0.34§ �0.44§ �0.20* �0.20* �0.26† �0.25†Discharge NA �0.17 �0.25† �0.01 �0.44§ �0.46§ �0.27‡
* P � 0.10, † P � 0.05, ‡ P � 0.01, § P � 0.001.
Table 4. Multivariate Determinants of CQoL during the Day Program and at Followup
Mean CQoL
Baseline Followup
� R2 P Value � R2 P ValueNA �0.63 0.12 0.0009 �16.5 0.11 �0.001Asthma exacerbations �0.13 0.01 0.29 �15.0 0.23 �0.001Hospital-based utilization �0.13 0.009 0.32 �4.2 0.03 0.08
Emotional function
Baseline Followup
� R2 P Value � R2 P ValueNA �0.79 0.17 �0.001 �15.7 0.10 0.002Asthma exacerbations �0.16 0.02 0.16 �15.1 0.26 �0.001Hospital-based utilization �0.09 0.006 0.41 �3.4 0.03 0.13
Activity limitation
Baseline Followup
� R2 P Value � R2 P ValueNA �0.33 0.02 0.20 �5.1 0.01 0.30Asthma exacerbations �0.05 0.001 0.77 �13.5 0.29 �0.001Hospital-based utilization �0.17 0.012 0.30 �4.4 0.05 0.03
VOLUME 89, DECEMBER, 2002 575

Limitation scales of the quality of life instrument were eachrelated in distinctive ways with caregiver NA.Because quality of life measures are intended to capture the
respondent’s perception of disease burden, they are heavilyinfluenced by respondent affective state. The very significantrole of NA on perception of health problems has been dem-onstrated by others, who found that self-reports of decreasedhealth status were related to self-report of NA, but not toobjective measures of morbidity.10 Juniper16 suggests that thequality of life measured in two patients with the same phys-iologic states can be quite different depending on the lifestyleand personality of those individuals. One person will reportmore impairment than another if the one is more anxious innature or has a more active lifestyle. Additionally, this asso-ciation has been found when the respondent is a parent. In areport of an earlier but similar cohort from National Jewish,17levels of emotional distress and social support for the parentpredicted their reports of quality of life.In this study the parents’ report at baseline of quality of life
over the recent past was completely unrelated to objectivemeasures of disease morbidity for the past year. Rather, theonly significant determinant of CQoL was the parents’ NA.This result is similar to that found in the Childhood AsthmaManagement Program (CAMP) study12 where child’s self-report of anxiety was the strongest predictor to self-report ofquality of life. The Emotional Function scale of the CQoLaccounted for much of the correlation between the parents’reports of NA and quality of life. This strong relationship wasto be expected, since the Emotional Function scale of theCQoL inquires about the caregiver’s worry, frustration, andextent of being bothered by their child’s disease, a series ofquestions essentially asking about NA, albeit specific to thechild’s illness. It should be noted that the Emotion Functionscale encompasses 9 of the 13 questions from the CQoL, withthe remaining four questions tapping Activity Limitations.The high correlation between CQoL and the respondent’saffect occurs because the two scales are basically measuringthe same underlying construct.However, the lack of any relationship with objective mea-
sures of disease morbidity before the admission was some-what surprising. It seems likely that parents’ extreme distressrelated to the uncontrolled asthma, possibly combined withhigh anxiety related to travel to National Jewish and admis-sion to the day program, created a high level of NA associ-ated with recent stressful activities. In contrast, a year afterdischarge from the day program the parents’ report of qualityof life was associated with objectively measured diseaseburden over the interim year. At the same time, the parents’affect during the day program admission continued to play arole in the relationship between disease and quality of life 1year later. This suggests some continuity in persistent parentNA. However, the data also indicate a link between thechild’s asthma morbidity and the parents’ reports of quality oflife that occurred within the year after the day programadmission. For those families with meaningful decreases in
their child’s asthma morbidity, quality of life was reported assignificantly higher at followup.We have previously shown an increase in CQoL and a
decrease in asthma exacerbations and related health careutilization over the year after admission to the pediatric dayprogram.5 In this current report, we have shown that thisquality of life increase and NA decrease occurred during thecourse of the child’s 15-day stay. The levels for both qualityof life and NA 1 year later essentially show maintenance ofthe levels reached by the time of discharge. There are anumber of factors that probably account for the significantchanges during the child’s admission. In this circumstance ofthe pediatric day program the families traveled to another citybecause their child had severe disease previously controlledineffectively by outpatient care. Upon arrival, families typi-cally report high levels of anxiety and apprehension associ-ated with the logistics of the admission (eg, travel arrange-ments, insurance issues) and the expectations of the dayprogram’s ability to help, as well as the accumulated effectsof the chronicity of their child’s disease. It is important tonote that this program was not an admission for acute treat-ment, as the children were usually stable upon admission, acondition required for travel.5 Therefore, although many fac-tors affect families’ attitudes and affect at admission, thebaseline CQoL was not temporarily depressed because ofacute illness.During the day program admission, thorough medical eval-
uations are conducted and treatment provided for the patient.However, the day program also intervenes with the entirefamily on all aspects of asthma management and quality oflife. Addressing disease concerns and teaching coping andmanagement not only improves management skills but alsoincreases perceptions of control. Psychosocial evaluationsaddress families’ adaptation to the illness, including difficul-ties that predated the loss of control of the asthma, as well asemotional and behavioral reactions to the disease burden thefamilies have experienced. Ideally, families identify maladap-tive patterns of functioning and begin to take control over theillness and its effect on them. We believe that it is themultiple facets of this multidisciplinary program that influ-ence parents to experience less depression and anxiety andmore optimism, together with a higher quality of life, at thetime of discharge. The correlation between higher quality oflife and lower asthma morbidity a year later suggests that theday program leads to changes in behavior as well as to bettersubjective feelings.Quality of life instruments are widely used, but as many
authors note,1,2 there is no gold standard and its definition isoften called into question. In fact, quality of life may not haveits own unique meaning, as an individual’s personality, per-sonal value, experience of illness, and approach to life willinfluence the meaning for each respondent.18 As such, thesequestionnaires are difficult to validate. Nevertheless, it hasbeen argued that the ambiguity surrounding this concept doesnot diminish the value of evaluating quality of life.19
576 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY

In this report we have attempted to clarify exactly what isbeing evaluated with the CQoL measure. Despite being com-prised predominantly of an Emotional Function scale, thereseems to be a lack of recognition of the extent to which thescale simply evaluates respondent affect. Because it is largelya measure of affect, it is highly sensitive to situational factors.At the same time, it can be expected to correlate with respon-dents’ trait-like affective predispositions. The correlationwith parents’ responses to a psychiatric symptom checklistcan thus be considered one form of validity. However, wehave demonstrated validity of another sort in that, after treat-ment, changes in morbidity were associated with changes inquality of life. Further, after participation in a treatmentprogram, Asthma Exacerbations, in concert with affect,proved to be a significant determinant of the complete scaleand both subscales, and health care utilization was a signif-icant determinant of the Activity Limitations subscale.Unfortunately, a measure of NA was not taken at followup.
This would have allowed for a concurrent look at NA andquality of life at the 1-year followup point. Additionally, anindependent, interviewer-rated measure of caregiver mentalhealth would have diminished the method variance in thisanalysis. Nevertheless, this report on a group of severelyasthmatic children with high health care utilization allowedthe careful analysis of convergent measures of morbidity.
CONCLUSIONQuality of life instruments are popular measures of the psy-chosocial correlates of disease severity and appear to berobust tools reporting outcomes of studies. Quality of life isimportant in developing a whole picture of disease and cangive rise to opportunity for intervention. However, it is im-portant that investigators who use quality of life measures toevaluate outcomes understand what is measured by theseinstruments and the manner in which resulting data are in-fluenced by situational factors and respondent characteristics.
REFERENCES1. Bender B. Measurement of quality of life in pediatric asthmaclinical trials. Ann Allergy Asthma Immunol 1996;77:438–447.
2. Gill T, Feinstein A. A critical appraisal of the quality of quality-of-life measurements. J Am Med Assoc 1994;272:619–626.
3. Osman L, Silverman M. Measuring quality of life for youngchildren with asthma and their families. Eur Respir J 1996;9(Suppl)21:35S—41S.
4. Mahajan P, Pearlman D, Okamoto L. The effect of fluticasonepropionate on functional status and sleep in children with
asthma and on the quality of life of their parents. J Allergy ClinImmunol 1998;102:19–23.
5. Bratton D, Price M, Gavin L, et al. Impact of a multidisciplinaryday program on disease and healthcare costs in children andadolescents with severe asthma: a two year followup study.Pediatr Pulmonol 2001;31:177–189.
6. Legorreta A, Leung K, Berkbigler D, et al. Outcomes of apopulation-based asthma management program: quality of life,absenteeism, and utilization. Ann Allergy Asthma Immunol2000;85:25–34.
7. Asmussen L, Olson L, Grant E, et al. Reliability and validity ofthe Children’s Health Survey for Asthma. Pediatrics 1999;104:e71.
8. Juniper E, Guyatt G, Feeny D, et al. Measuring quality of life inthe parents of children with asthma. Qual Life Res 1996;5:27–34.
9. Schmier J, Chan K, Leidy N. The impact of asthma on health-related quality of life. J Asthma 1998;35:585–597.
10. Watson D, Pennebaker J. Health complaints, stress, and distress:exploring the central role of negative affectivity. Psychol Rev1989;96:234–254.
11. Put C, Bemedts M, Van Den Berg O, et al. Asthma symptoms:influence of personality versus clinical status. Eur Respir J1999;13:751–756.
12. Annett R, Bender B, Lapidus J, et al. Predicting children’squality of life in an asthma clinical trial: what do children’sreports tell us? J Pediatr 2001;139:854–861.
13. Todd W. New mindsets in asthma: interventions and closermanagement. J Care Manag 1995;1:37–44.
14. Wamboldt F, Price M, Hume L, et al. Reliability and validity ofa system for coding asthma outcomes from medical records. JAsthma 2002;39:299–305.
15. Derogatis L, Melisaratos N. The Brief Symptom Inventory: anintroductory report. Psychol Med 1983;13:595–605.
16. Juniper E. Effect of asthma on quality of life. Can Respir J1998;5(Suppl):77A–84A.
17. Frankel K, Wamboldt M. Chronic childhood illness and mater-nal mental health: why should we care? J Asthma 1998;35:621–630.
18. Testa M, Simonson D. Assessment of quality-of life outcomes.N Engl J Med 1996;334:835–840.
19. Rutishauser C, Sawyer S, Bowes G. Quality-of-life assessmentin children and adolescents with asthma. Eur Respir J 1998;12:486–494.
Requests for reprints should be addressed to:Mary KlinnertNational Jewish Medical and Research Center1400 Jackson Street, G220Denver, CO 80206E-mail: [email protected].
VOLUME 89, DECEMBER, 2002 577