caring for glucose-6-phosphate dehydrogenase …. in this article, we will explore the biochemical...
TRANSCRIPT

572 P&T® • September2015 • Vol.40No.9
INTRODUCTIONGlucose-6-phosphate dehydrogenase (G6PD) deficiency is
the most common enzymopathy worldwide, affecting an esti-mated 400 million people.1,2 The major morbidity associated with G6PD deficiency is hemolytic anemia, which in some individuals may be life-threatening. Hemolysis can be triggered by infection, hyperglycemia, certain foods, and certain medica-tions. Though G6PD deficiency exists in concentrated pockets in Africa, the Middle East, and Southeast Asia, about one in 10 African-American males are affected in the United States.3 The disease may have greater relevance in the future as foreign travel to the U.S. increases and immigrants access the U.S. health care system, leading to higher-than-predicted prevalence.
Greater awareness of G6PD deficiency in select U.S. popula-tions and advances in laboratory diagnostics, including genetic testing and enzyme activity assays, have led to more common screening of at-risk populations for G6PD deficiency. Many hospitals are increasingly utilizing patient-specific data in the electronic medical record (EMR) coupled with clinical deci-sion support (CDS) tools to facilitate safer and more effective patient care. For example, many hospitals use computerized prescriber order-entry (CPOE) systems with built-in CDS applications, such as drug–disease screening, that can inform the clinician of interactions critical to patient safety.4 In the case of a less common disease such as G6PD deficiency, electronic disease-screening tools can generate essential safety alerts for clinicians who may not be familiar with the patient or with this condition. In this article, we will explore the biochemical and physiological basis of G6PD deficiency and further define the critical role that health care informatics can play in optimizing the treatment of the G6PD-deficient patient.
G6PDDISEASEOVERVIEWG6PD deficiency is an X-linked genetic disorder with 187
known allelic mutations.5 G6PD, a critical enzyme in the pentose phosphate pathway, exhibits diminished activity in these patients, leading to inadequate production of protective intracellular thiols during oxidative stress.6 While the deficiency is ubiquitous across cell types, erythrocytes are particularly vulnerable to oxidative stress in the G6PD-deficient state, and the disease has been associated with neonatal hyperbilirubine-mia, acute hemolysis, and chronic nonspherocytic hemolytic anemia. The World Health Organization (WHO) has classified G6PD deficiency according to the magnitude of the enzyme deficiency and hemolysis severity.7 Class I through Class III describe deficiency states ranging from the most severe chronic nonspherocytic hemolytic anemia to mild deficiency
that manifests hemolysis only with exposure to certain meta-bolic conditions, infections, drugs, and foods. Classes IV and V define nondeficient and high-enzyme-activity states.
Hemolytic anemia is the most common life-threatening manifestation of G6PD deficiency. In a typical course, patients present with findings of jaundice, fatigue, back pain, tachyp-nea, and tachycardia. Relevant laboratory findings include decreased hemoglobin and red blood cell counts, reticulocy-tosis, increased lactate dehydrogenase, and increased uncon-jugated bilirubin.
To understand the biochemistry of G6PD deficiency, one must first understand the enzyme’s normal function. The mitochondria of human cells are responsible for manufacturing energy (adenosine triphosphate) via aerobic respiration, the byproducts of which include free radicals and reactive oxida-tive species (ROS) from the “leaky” electron transport chain.8 Free radicals such as superoxide, hydrogen peroxide, and hydroxyl radical can harm DNA, lipoproteins, and cell mem-branes, leading to cellular damage and cell lysis. This state is often referred to as oxidative stress.9 Human cells use multiple mechanisms to neutralize the harmful free-radical species by synthesizing antioxidants to combat oxidative stress. One such in vitro antioxidant is the thiol glutathione. In its reduced (cell-protective) form, glutathione scavenges free-radical species to prevent cell damage. However, once a glutathione molecule reduces a free radical, it must be regenerated in a pathway utilizing the reducing coenzyme NADPH. The pentose phos-phate pathway generates a supply of NADPH through a reac-tion dependent on G6PD. In the pentose phosphate pathway, G6PD catalyzes the conversion of glucose-6-phosphate to 6-phosphogluconolactone and in the process generates reduced NADPH used to regenerate glutathione. Other mechanisms for producing cellular antioxidants involve ascorbate, alpha-tocopherol, and carotenoids.10
The main problem with G6PD deficiency is that patients cannot regenerate adequate amounts of protective glutathione. In most cells, this deficiency is inconsequential, since other mitochondrial processes sustain a supply of natural antioxidants to eliminate damaging ROS. However, erythrocytes naturally lose organelles, including mitochondria, during cell maturation and depend solely on the cytosolic pentose phosphate pathway and generation of reduced glutathione for oxidative protection.11 G6PD deficiency, however, diminishes these cells’ ability to regenerate glutathione, leaving red blood cells vulnerable to oxidative damage and eventual death.
G6PD deficiency can be detected via several methods, the most common being a quantitative laboratory assay for G6PD enzyme activity. A G6PD enzyme activity level below 5 units per gram of hemoglobin constitutes deficiency.12 In addition, genetic testing can be performed to confirm the diagnosis.
CaringforGlucose-6-PhosphateDehydrogenase(G6PD)–DeficientPatients:ImplicationsforPharmacy
Jeff Bubp, PharmD; Marilyn Jen; and Karl Matuszewski, MS, PharmD
Jeff Bubp is Manager, Disease Decision Support Group, Clinical Editorial, at First Databank in South San Francisco, California. Marilyn Jen is a Doctor of Pharmacy candidate at the University of Michigan College of Pharmacy in Ann Arbor, Michigan. Karl Matuszewski is Vice President, Clinical Editorial, at First Databank.
Disclosure: The authors report no commercial or financial interests in regard to this article.
Vol.40No.9 • September2015 • P&T® 573
Current practices typically do not include routine testing for the disease. However, testing should be considered in:13
•Patients of African, Middle Eastern, or Asian descent presenting with hemolytic anemia.
•Males with a family history of jaundice, splenomegaly, or cholelithiasis.
•Newborns with severe jaundice.
G6PDTRIGGERSFORHEMOLYTICANEMIAThe three main triggers for hemolytic anemia in G6PD-
deficient patients are infections, certain foods, and certain drugs. Food ingestion triggering hemolysis can be a telltale sign for a positive diagnosis. Historically, G6PD deficiency has been referred to as “favism,” named after the observed hemolytic effect that fava beans can have on patients with G6PD deficiency. The fava bean (Vicia faba) is a type of legume consumed worldwide that contains high amounts of divicine, convicine, and isouramil—chemicals that are suspected to be highly oxidative.14 Patients with G6PD deficiency should avoid fava beans.
Infections are the most typically cited cause of hemolytic anemia in the G6PD-deficient patient.15 During infections, the immune system incites an inflammatory response that also generates oxidative species. Erythrocytes of G6PD-deficient patients cannot overcome the oxidative stress, subsequently leading to cell lysis.
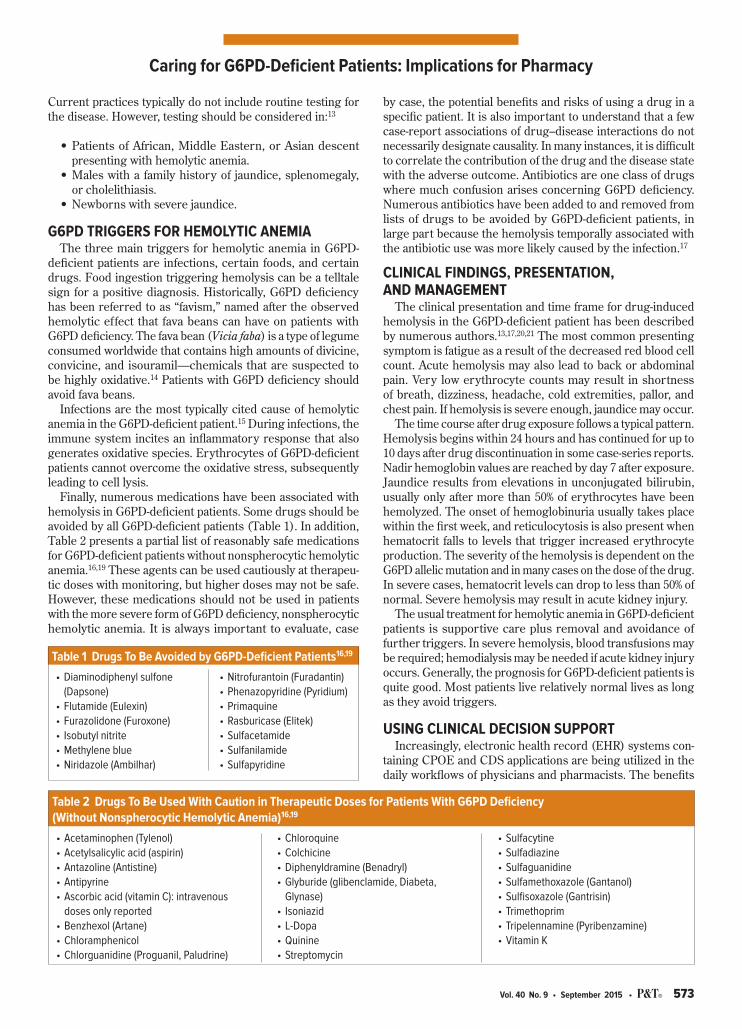
Finally, numerous medications have been associated with hemolysis in G6PD-deficient patients. Some drugs should be avoided by all G6PD-deficient patients (Table 1). In addition, Table 2 presents a partial list of reasonably safe medications for G6PD-deficient patients without nonspherocytic hemolytic anemia.16,19 These agents can be used cautiously at therapeu-tic doses with monitoring, but higher doses may not be safe. However, these medications should not be used in patients with the more severe form of G6PD deficiency, nonspherocytic hemolytic anemia. It is always important to evaluate, case
CaringforG6PD-DeficientPatients:ImplicationsforPharmacy
by case, the potential benefits and risks of using a drug in a specific patient. It is also important to understand that a few case-report associations of drug–disease interactions do not necessarily designate causality. In many instances, it is difficult to correlate the contribution of the drug and the disease state with the adverse outcome. Antibiotics are one class of drugs where much confusion arises concerning G6PD deficiency. Numerous antibiotics have been added to and removed from lists of drugs to be avoided by G6PD-deficient patients, in large part because the hemolysis temporally associated with the antibiotic use was more likely caused by the infection.17
CLINICALFINDINGS,PRESENTATION, ANDMANAGEMENT
The clinical presentation and time frame for drug-induced hemolysis in the G6PD-deficient patient has been described by numerous authors.13,17,20,21 The most common presenting symptom is fatigue as a result of the decreased red blood cell count. Acute hemolysis may also lead to back or abdominal pain. Very low erythrocyte counts may result in shortness of breath, dizziness, headache, cold extremities, pallor, and chest pain. If hemolysis is severe enough, jaundice may occur.
The time course after drug exposure follows a typical pattern. Hemolysis begins within 24 hours and has continued for up to 10 days after drug discontinuation in some case-series reports. Nadir hemoglobin values are reached by day 7 after exposure. Jaundice results from elevations in unconjugated bilirubin, usually only after more than 50% of erythrocytes have been hemolyzed. The onset of hemoglobinuria usually takes place within the first week, and reticulocytosis is also present when hematocrit falls to levels that trigger increased erythrocyte production. The severity of the hemolysis is dependent on the G6PD allelic mutation and in many cases on the dose of the drug. In severe cases, hematocrit levels can drop to less than 50% of normal. Severe hemolysis may result in acute kidney injury.
The usual treatment for hemolytic anemia in G6PD-deficient patients is supportive care plus removal and avoidance of further triggers. In severe hemolysis, blood transfusions may be required; hemodialysis may be needed if acute kidney injury occurs. Generally, the prognosis for G6PD-deficient patients is quite good. Most patients live relatively normal lives as long as they avoid triggers.
USINGCLINICALDECISIONSUPPORTIncreasingly, electronic health record (EHR) systems con-
taining CPOE and CDS applications are being utilized in the daily workflows of physicians and pharmacists. The benefits
•Diaminodiphenylsulfone(Dapsone)
•Flutamide(Eulexin)•Furazolidone(Furoxone)• Isobutylnitrite•Methyleneblue•Niridazole(Ambilhar)
•Nitrofurantoin(Furadantin)•Phenazopyridine(Pyridium)•Primaquine•Rasburicase(Elitek)•Sulfacetamide•Sulfanilamide•Sulfapyridine
Table1DrugsToBeAvoidedbyG6PD-DeficientPatients16,19
Table2DrugsToBeUsedWithCautioninTherapeuticDosesforPatientsWithG6PDDeficiency (WithoutNonspherocyticHemolyticAnemia)16,19
•Acetaminophen(Tylenol)•Acetylsalicylicacid(aspirin)•Antazoline(Antistine)•Antipyrine•Ascorbicacid(vitaminC):intravenousdosesonlyreported
•Benzhexol(Artane)•Chloramphenicol•Chlorguanidine(Proguanil,Paludrine)
•Chloroquine•Colchicine•Diphenyldramine(Benadryl)•Glyburide(glibenclamide,Diabeta,Glynase)
• Isoniazid•L-Dopa•Quinine•Streptomycin
•Sulfacytine•Sulfadiazine•Sulfaguanidine•Sulfamethoxazole(Gantanol)•Sulfisoxazole(Gantrisin)•Trimethoprim•Tripelennamine(Pyribenzamine)•VitaminK

574 P&T® • September2015 • Vol.40No.9
of an EHR system can include increased access to medical information, improved patient safety and outcomes, improved care coordination, and increased practice efficiency.18 The EMR contains all of the patient data that once existed in paper charts, but it is now arranged in a standardized format, with much of the data coded for computability.
The electronic patient problem list is one part of an EMR where the patient data is coded in the back-end database of the record. Standard terminologies used for the patient problem list include ICD-9, ICD-10, and SNOMED CT. ICD-9 and ICD-10 are disease classification schema maintained in the U.S. by the Centers for Medicare and Medicaid Services. Either may be used to populate the electronic patient problem list. SNOMED CT is a true medical terminology specifically intended for use in EMRs and maintained by the International Health Terminology Standards Development Organisation, which is owned and governed by 27 countries.
Rare, genetically based conditions are often not well rep-resented in ICD-9 and ICD-10 terminologies because of the classification schema they use. In some instances, these rare conditions are grouped with other related conditions under a single code. This practice of aggregating diseases for clas-sification purposes does not work well for CDS that depends on problem-list details; ambiguous CDS alerts can result. Fortunately, G6PD deficiency is represented with sufficient major subtype codes in both ICD-9 and ICD-10. SNOMED CT is also sufficiently detailed and in addition includes codes based on the WHO classification schema.
The utility of the coded patient problem list is that it can be leveraged by computerized drug–disease interaction-checking applications. In the case of G6PD, the patient problem list could be populated with a disease terminology code for G6PD deficiency that serves as a trigger for drug–disease interaction checking. While G6PD may not be routinely entered into the patient’s problem list, its notation in other parts of the medical record, such as in the history or allergy sections, is likely to lead to it being missed or unavailable for computable disease interac-tion CDS. Although health information systems help clinicians improve care with CPOE and pharmacist order verification, rare inherited disease states often become missed opportunities for drug-safety interventions. CDS support can, however, improve the clinician’s awareness of problematic drug therapies for these rare conditions, thereby improving patient safety.
For example, consider a scenario in which a patient with G6PD deficiency is admitted to an inpatient medical floor and the physician orders several medications, including nitrofuran-toin for a bacterial urinary tract infection. During prescription verification by the pharmacy, a drug–disease interaction applica-tion could query the patient’s electronic problem list and new medication order and alert the pharmacist to a G6PD interaction with nitrofurantoin. This demonstrates how an application of technology can improve patient care and outcomes.
CONCLUSIONAdvancing technology is driving better diagnostic tools and
patient safety checks via computerized workflows, enhancing individualized health care. G6PD deficiency, a rare but manage-able disease, requires strict avoidance of food and drug triggers. Physician use of computerized workflows that include disease
interaction CDS can mitigate the risk of a G6PD-deficient patient receiving a “trigger” drug. All health-system-based pharmacists, including clinical pharmacists as members of the health care team, can utilize CDS tools in their workflows, adding a level of safety to the care of the G6PD-deficient patient.
REFERENCES1. Cappellini MD, Fiorelli G. Glucose-6-phosphate dehydrogenase
deficiency. Lancet 2008;371(9606):64–74.2. Nkhoma ET, Poole C, Vannappagari V, et al. The global prevalence
of glucose-6-phosphate dehydrogenase deficiency: a systematic review and meta-analysis. Blood Cells Mol Dis 2009;42(3):267–278.
3. Genetics Home Reference, U.S. National Library of Medicine. Glucose-6-phosphate dehydrogenase deficiency. May 2006. Avail-able at: http://ghr.nlm.nih.gov/condition/glucose-6-phosphate-dehydrogenase-deficiency. Accessed February 3, 2014.
4. Van der Sijs H, Aarts J, Vulto A, et al. Overriding of drug safety alerts in computerized physician order entry. J Am Med Inform Assoc 2006;13(2):138–147.
5. Minucci A, Moradkhani K, Hwang MJ, et al. Glucose-6-phosphate dehydrogenase (G6PD) mutations database: review of the ‘old’ and update of the new mutations. Blood Cells Mol Dis 2012;48(3):154–165.
6. Luzzatto L. Chapter 106: Hemolytic anemias and anemia due to acute blood loss. In: Longo DL, Fauci AS, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine, 18th ed. New York, New York: McGraw-Hill; 2012. Available at: http://accessmedicine.mhmedical.com/content.aspx?bookid=331§ionid=40726844. Accessed February 11, 2014.
7. WHO Working Group. Glucose-6-phosphate dehydrogenase defi-ciency. Bull World Health Organ 1989;67(6):601–611.
8. Cadenas E, Davies KJ. Mitochondrial free radical generation, oxida-tive stress, and aging. Free Radic Biol Med 2000;29(3–4):222–230.
9. Frei B. Reactive oxygen species and antioxidant vitamins: mecha-nisms of action. Am J Med 1994;97(3)(suppl 1):S5–S13.
10. Chaudière J, Ferrari-Iliou R. Intracellular antioxidants: from chemi-cal to biochemical mechanisms. Food Chem Toxicol 1999;37(9–10):949–962.
11. Glucose 6-phosphate dehydrogenase plays a key role in protec-tion against reactive oxygen species. In: Berg JM, Tymoczko JL, Stryer L. Biochemistry. 5th ed. 2002. W. H. Freeman and Company. Available at: http://www.ncbi.nlm.nih.gov/books/NBK22389. Accessed February 3, 2014.
12. GlobalRPh.com. Common laboratory (lab) values. Glucose-6-phosphate dehydrogenase. June 2012. Available at: http://www.globalrph.com/labs_g.htm#Glucose-6-phosphate. Accessed February 3, 2014.
13. Frank J. Diagnosis and management of G6PD deficiency. Am Fam Physician 2005;72(7):1277–1282.
14. McMillan DC, Schey KL, Meier GP, Jollow DJ. Chemical analysis and hemolytic activity of the fava bean aglycon divicine. Chem Res Toxicol 1993;6(4):439–444.
15. Beutler E. G6PD deficiency. Blood 1994;84(11):3613–3636.16. Beutler E. Glucose-6-phosphate dehydrogenase deficiency: a
historical perspective. Blood 2008;111(1):16–24.17. Luzzatto L, Seneca E. G6PD deficiency: a classic example of
pharmacogenetics with on-going clinical implications. British J Haematol 2014;164(4):469–480.
18. HealthIT.gov. Benefits of electronic health records (EHRs). Avail-able at: http://healthit.gov/providers-professionals/benefits-electronic-health-records-ehrs. Accessed July 25, 2015.
19. Youngster I, Arcavi L, Schechmaster R, et al. Medications and glucose-6-phosphate dehydrogenase deficiency: an evidence-based review. Drug Saf 2010;33(9):713–726.
20. Edwards CQ. Anemia and the liver. Hepatobiliary manifestations of anemia. Clin Liver Dis 2002;6(4):891–907, viii.
21. Pamba A, Richardson ND, Carter N, et al. Clinical spectrum and severity of hemolytic anemia in glucose 6-phosphate dehydrogenase-deficient children receiving dapsone. Blood 2012;120(20):4123–4133. n
CaringforG6PD-DeficientPatients:ImplicationsforPharmacy