cartilage splitting without stitches
TRANSCRIPT

Cartilage Splitting Without StitchesTechnique and OutcomesDéborah Obadia, MD; Julien Quilichini, MD; Vincent Hunsinger, MD; Patrick Leyder, MD
O toplasty is an old and common surgical procedure forprominent ears,1 and numerous techniques have beendeveloped over the years. The most frequent causes
of prominent ears include conchal valgus, conchal excess, anda lack of antihelical fold.2 Otoplasty methods can be classi-fied into the following 2 categories: (1) those that score the car-tilage and (2) those that use a posterior absorbable or nonab-sorbable suture to bend the cartilage.3-5 Techniques can becombined,6 and a concha-mastoid suture can be added to cor-rect the protrusion of the concha, as described by Furnas.7 Inhis Atlas of Plastic and Aesthetic Surgery,8 G. Jost describes atechnique using cartilage splitting and cartilage scoring witha number 15 scalpel blade. This technique, unevaluated to datein the literature, has been performed at Hopital R. Ballanger,Aulnay-sous-Bois, France, for more than 10 years. The objec-
tives of this study were to highlight the technical details of theotoplasty procedure involving cartilage splitting withoutstitches and to evaluate its complications and outcomes.
MethodsSurgical TechniqueThe procedure is performed using general anesthesia. A solu-tion of 50% saline serum and 50% lidocaine (1%) with epi-nephrine (1:10 000) is injected along the posterior portion ofthe pinna, subcutaneously and deep to the mastoid perios-teum. The skin is incised 2 to 4 mm from the postauricular sul-cus, with a small sole-shaped excision. Subperichondrial pos-terior dissection is performed up to 1 or 2 mm from the edge
IMPORTANCE Otoplasty procedures usually involve cartilage sparing, with stitches or cartilagescoring. These techniques have been widely reviewed in the literature. The techniquereported in this study requires neither stitches nor rasping but rather a complete separationof the helix and antihelix, with nontransfixing incisions to break the cartilaginous springs.
OBJECTIVES To evaluate the technical details, aesthetic results, and complications in a seriesof otoplasty procedures involving cartilage splitting without stitches.
DESIGN, SETTING, AND PARTICIPANTS We conducted a retrospective review of patients whounderwent otoplasty procedures between January 2004 and September 2010, by the samesenior surgeon.
MAIN OUTCOMES AND MEASURES File data on complications, recurrences, and revision rateswere collected. An aesthetic evaluation of the postoperative results was conducted by apanel of 3 plastic surgeons and 3 lay observers.
RESULTS Our series included 58 patients, with a mean age of 16 years. No recurrences werereported. Six patients (10%) experienced minor complications. No revisions were needed. Nochondritis or skin necrosis was noted. The aesthetic results were very good for 36 patients(62%) by the plastic surgeons and 39 patients (68%) by lay observers. The remainingaesthetic results were judged as good.
CONCLUSIONS AND RELEVANCE The Jost otoplasty procedure described herein requires nononabsorbable sutures to bend the cartilage, avoiding many complications. The technique issafe, reliable, and reproducible, with predictable and permanent outcomes. It is also usefulfor secondary otoplasty after failed Stenström or Mustarde otoplasty.
LEVEL OF EVIDENCE 4.
JAMA Facial Plast Surg. doi:10.1001/jamafacial.2013.326Published online August 29, 2013.
Video atjamafacialplasticsurgery.com
Author Affiliations: Department ofPlastic Surgery, Robert BallangerHospital, Aulnay-sous Bois, France(Obadia, Quilichini, Hunsinger,Leyder); Jean Verdier–AvicenneHospital, Paris XIII Bobigny MedicalSchool, Bobigny, France (Quilichini).
Corresponding Author: JulienQuilichini, MD, Department of PlasticSurgery, Robert Ballanger Hospital,93602 Aulnay-sous-Bois, France( [email protected])
Research
Original Investigation
jamafacialplasticsurgery.com JAMA Facial Plastic Surgery Published online August 29, 2013 E1
Downloaded From: http://archfaci.jamanetwork.com/ by a Wegner Health Science Info Ctr & USD User on 09/05/2013
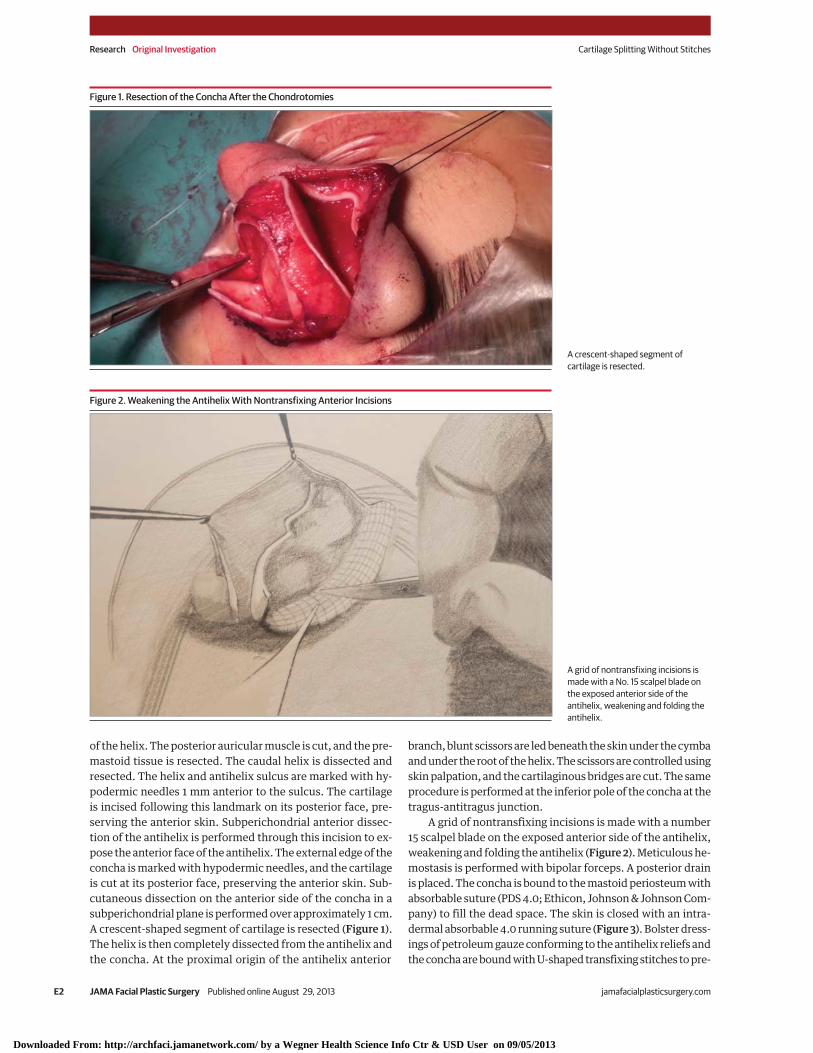
of the helix. The posterior auricular muscle is cut, and the pre-mastoid tissue is resected. The caudal helix is dissected andresected. The helix and antihelix sulcus are marked with hy-podermic needles 1 mm anterior to the sulcus. The cartilageis incised following this landmark on its posterior face, pre-serving the anterior skin. Subperichondrial anterior dissec-tion of the antihelix is performed through this incision to ex-pose the anterior face of the antihelix. The external edge of theconcha is marked with hypodermic needles, and the cartilageis cut at its posterior face, preserving the anterior skin. Sub-cutaneous dissection on the anterior side of the concha in asubperichondrial plane is performed over approximately 1 cm.A crescent-shaped segment of cartilage is resected (Figure 1).The helix is then completely dissected from the antihelix andthe concha. At the proximal origin of the antihelix anterior
branch, blunt scissors are led beneath the skin under the cymbaand under the root of the helix. The scissors are controlled usingskin palpation, and the cartilaginous bridges are cut. The sameprocedure is performed at the inferior pole of the concha at thetragus-antitragus junction.
A grid of nontransfixing incisions is made with a number15 scalpel blade on the exposed anterior side of the antihelix,weakening and folding the antihelix (Figure 2). Meticulous he-mostasis is performed with bipolar forceps. A posterior drainis placed. The concha is bound to the mastoid periosteum withabsorbable suture (PDS 4.0; Ethicon, Johnson & Johnson Com-pany) to fill the dead space. The skin is closed with an intra-dermal absorbable 4.0 running suture (Figure 3). Bolster dress-ings of petroleum gauze conforming to the antihelix reliefs andthe concha are bound with U-shaped transfixing stitches to pre-
Figure 1. Resection of the Concha After the Chondrotomies
A crescent-shaped segment ofcartilage is resected.
Figure 2. Weakening the Antihelix With Nontransfixing Anterior Incisions
A grid of nontransfixing incisions ismade with a No. 15 scalpel blade onthe exposed anterior side of theantihelix, weakening and folding theantihelix.
Research Original Investigation Cartilage Splitting Without Stitches
E2 JAMA Facial Plastic Surgery Published online August 29, 2013 jamafacialplasticsurgery.com
Downloaded From: http://archfaci.jamanetwork.com/ by a Wegner Health Science Info Ctr & USD User on 09/05/2013

vent hematoma (Figure 4). A loose head dressing is placed. Af-ter surgery, antibiotic prophylaxis (cefuroxime) is given for 5days, for the duration of the bolster. Drains are removed at day1, and the bolster is removed at day 4 or 5. Technical high-lights are summarized in the Video footage.
PatientsIn this retrospective study, we included all patients who un-derwent a unilateral or bilateral otoplasty in our service by oneof us (P.L.) with the same surgical technique between Janu-ary 2004 and September 2010. Exclusion criteria included oto-plasties requiring a cartilaginous graft, otoplasties per-formed with other techniques, patients with less than 1 yearof follow-up data, and patients without preoperative and post-
operative photographs. Oral informed consent was obtainedfrom the study participants.
Data AnalysisWe reviewed 67 otoplasty files from January 2004 to Septem-ber 2010. Nine files were excluded. We included 58 patients andrecorded their age at the time of the intervention and any post-operative complications. The complications were categorizedas early complications (before postoperative day 15) or late com-plications (postoperative day 15 or later) and as major compli-cations (requiring reoperation or postoperative antibiotics) orminor complications (requiring conservative treatment).
Three external lay observers and 3 plastic surgeons whowere not involved in the operation reviewed the preopera-
Figure 3. Immediate Result Before Application of the Tied-Over Dressing
The skin is closed with an intradermalabsorbable 4.0 running suture.
Figure 4. Schematic View of the Tied-Over Dressing
Bolster dressings of petroleum gauzeconforming to the antihelix reliefsand the concha are bound withU-shaped transfixing stitches toprevent hematoma.
Cartilage Splitting Without Stitches Original Investigation Research
jamafacialplasticsurgery.com JAMA Facial Plastic Surgery Published online August 29, 2013 E3
Downloaded From: http://archfaci.jamanetwork.com/ by a Wegner Health Science Info Ctr & USD User on 09/05/2013

tive and postoperative photographs. They scored the globalmorphologic result of the intervention on a visual analog scaleranging from 1 (very poor) to 10 (excellent). These scores werethen categorized as unsatisfactory results (score range, 1-5), sat-isfactory results (score range, 6-7), or very satisfactory re-sults (score range, 8-10).
ResultsOur review included 58 patients. There were 28 women and30 men, with a mean age of 16 years (age range, 7-49 years).
ComplicationsThe only early complication was a small hematoma that waspunctured during consultation, without any aftermath. Thelate complications (postoperative day 15 or later) included onecase of external earache 2 months after the procedure, one caseof inflammatory reaction due to absorbable suture, one caseof delayed healing of the posterior incision (requiring a dress-ing >15 days), one case of painful unilateral syndrome at 3months but ending at 1 year after surgery, and one case of acompression wound on the anterior antihelical skin (requir-ing a dressing for 7 days). Altogether, 6 patients (10%) had acomplication. We observed no major complications (ex-tended necrosis or chondritis). No surgical revisions or recur-rences were reported. The results are summarized in the Table.
In this series, 3 patients had undergone a previous oto-plasty in a different institution to correct prominent ears. In 2patients, the recurrence was bilateral (with keloid scars in onecase) after Stenström otoplasty.8,9 In the third patient, the re-currence was unilateral after anterior blind rasping and Mus-tarde otoplasty.10 These 3 patients have no recurrence at 1 yearafter performance of the surgical technique described herein.The keloid scars were excised during the procedure and havenot recurred.
OutcomesNo global morphologic result score of less than 4 was re-ported by the 3 plastic surgeons or by the 3 lay observers. The
mean scores were 7.68 among the plastic surgeons, 8.24 amongthe lay observers, and 8.84 among the patients. The evalua-tions are summarized in Figure 5.
DiscussionMost otoplasty studies focus on techniques based on a poste-rior cartilage suture, occasionally associated with anterior car-tilage scoring. The postoperative result is generally good, andpatient satisfaction is usually high.11,12 However, complica-tions occur, and the recurrence rate is high, around 10%.11,13
In our series, we evaluated a technique that requires neitherstitches nor blind cartilage scoring, which has not been as-sessed to date in the literature.
Perioperative setting of cartilage suture may be difficultand uncertain. Complications with this technique usually in-clude extrusion of stitches or breaking, which can lead to re-currence in up to 24% of cases.10,14 With the Jost technique,no stitches are used to maintain the shape of the antihelicalfold; therefore, stitch-related complications (eg, palpation, ex-trusion, breaking) are avoided. The only stitches used are anabsorbable suture to fill the dead space behind the concha andskin suture.
With Stenström otoplasty, the cartilage is scored by a raspor microneedles that are blindly slipped through the poste-rior incision or by the use of an incision on the upper edge ofthe antihelix.12 Control of the intensity and the scoring area isdifficult because this procedure is led blindly. Hemostasis isnot possible, and the anterior skin can be injured, with bothleading to skin necrosis. In the Jost technique, the cartilage isscored on an area that is completely exposed; therefore, onecan easily set the depth and extent of the grid, depending onthe need for correction. In this way, we avoid a lack of scor-ing, which may lead to recurrence, as well as excess that may
Table. Study Results
VariableNo. (%)(n = 58)
Age, mean (range), y 16 (7-49)
Complications, No. (%)
Total 6 (10)
Early
Hematoma 1 (2)
Late 1 (2)
Painful unilateral syndrome 1 (2)
Delayed healing 1 (2)
External earache 1 (2)
Inflammatory reaction to absorbablesuture
1 (2)
Compression wound 1 (2)
Revision or recurrence, No. (%) 0
Figure 5. Outcome Evaluation
40
30
20
10
0
100
90
80
% R
epor
ting
the
Cosm
etic
Res
ult
Cosmetic Result
Very Satisfactory Satisfactory Unsatisfactory
70
60
50
Plastic surgeons
Lay observers
Patients
Thirty-six plastic surgeons (62%), 40 lay observers (69%), and 54 patients(93%) were very satisfied with the cosmetic result. Twenty plastic surgeons(34%), 18 lay observers (32%), and 2 patients (3%) were satisfied with thecosmetic result. Two plastic surgeons and 2 patients were dissatisfied with thecosmetic result.
Research Original Investigation Cartilage Splitting Without Stitches
E4 JAMA Facial Plastic Surgery Published online August 29, 2013 jamafacialplasticsurgery.com
Downloaded From: http://archfaci.jamanetwork.com/ by a Wegner Health Science Info Ctr & USD User on 09/05/2013

imply an overly marked antihelical fold, which would not ap-pear natural. Moreover, the rasping with the Stenström tech-nique is performed precisely on the desired antihelical fold.Morphologic outcomes can be disappointing if the rasping istoo extensive, leading to antihelical sharp edges. In the Josttechnique, there is no direct incision in the antihelical fold, pre-venting these complications.
The position chosen for the chondrotomies is not wherethe cartilage will be folded; the aim is to split helix-antihelixand antihelix-concha junctions. The anterior fibroelasticarch of the antihelix is broken with the anterior striation gridas a result of striations. Cartilage splitting and cartilage scor-ing allow spontaneous and natural placement of the antihe-lix fold.
The anterior faces of the antihelix and concha are dis-sected under the perichondrium, preserving the vasculariza-tion of the anterior skin during scoring. Ultimately, exhaustivehemostasis can be obtained because all undermined areas areaccessible. Moreover, the final bolster dressing fixed in the sul-cus helps prevent hematoma on elevated areas. However, thedressing must not be too tight to prevent any skin necrosis.
Six of our patients (10%) had postoperative complica-tions. This is consistent with the literature.2 However, our cri-teria may have been overinclusive because any postoperativeneed for nursing care was considered a complication. In fact,all of the complications were minor postoperative events, withno bearing on the morphologic outcome.
We observed no chondritis or skin necrosis, although theskin elevation was extensive. However, a superficial compres-sion wound occurred on a limited area (<3-mm diameter), mostlikely due to a tight dressing. The only infection was a Cory-nebacterium external otitis, occurring 2 months after the pro-cedure, and may have been caused by a small wound on theexternal auditory canal. No keloid scars have occurred, prob-ably because the skin resection is moderate and the suture istension free.
Two cases of persistent swelling at postoperative month3 were reported. Although we did not classify these as com-plications, it is important to point them out because they maybe linked to the technique and the inflammatory reactioncaused by extensive dissection. In all cases, swelling had dis-appeared after 4 months.
Figure 6. Preoperative and Postoperative Views
A B C
D E F
A-C, Preoperative view; D-F, result after 1 year.
Cartilage Splitting Without Stitches Original Investigation Research
jamafacialplasticsurgery.com JAMA Facial Plastic Surgery Published online August 29, 2013 E5
Downloaded From: http://archfaci.jamanetwork.com/ by a Wegner Health Science Info Ctr & USD User on 09/05/2013

Regarding the other complications (delayed woundhealing, a persistent painful syndrome, and a cutaneousreaction to absorbable suture), none were specific to theJost procedure. These complications may occur with anysurgical procedure.
The Jost technique can also be used for secondary oto-plasty after failed procedures. Because the surgical steps aredifferent from those of the Mustarde and Stenström tech-niques, the Jost procedure can be performed regardless of theinitial operation. Therefore, this technique is a helpful life-boat in case of recurrence for surgeons who usually performanother procedure.
The duration of the Jost technique is longer than others,requiring approximately 80 minutes compared with 45 min-utes for the anterior scoring techniques and 60 minutes forthe posterior sutures.13 Moreover, the Jost technique mayseem more complicated than the other procedures becauseit combines extensive skin undermining and transfixing car-tilage splitting. However, the learning curve is rapid, and ajunior surgeon can operate autonomously after approxi-mately 3 procedures.
Because extensive skin elevation is performed, one mayfear skin necrosis or hematoma and an infection, but noneoccurred in this series. The patients were young nonsmokers,ensuring optimal skin vascularization, and the ear is a well-vascularized area. Moreover, meticulous hemostasis and theuse of a bolster dressing help avoid those complications. The
drain usually collects less than 3 mL of blood, and our team isdebating whether to use one at all.
Antibiotic prophylaxis for the duration of the dressing canbe justified because of the use of transfixing stitches on the bol-ster toward the skin and the cartilage. To our knowledge, no sci-entific evidence exists on the use of antibiotics after otoplas-ties; therefore, this practice may vary among operating teams.
Ultimately, the level of patient satisfaction is high. The sur-geons are also satisfied with the global morphologic result,which is described as very natural, without a vertical antihe-lix or an unpleasing acute angle (Figure 6). The rare cases thatare less satisfactory involve asymmetry, a “telephone ear” de-formity, or an uncorrected lobule protrusion. These findingsare consistent with other series.2,12,15,16 Therefore, the Jost tech-nique results in a natural shape, without any hypercorrectionor recurrence, and is positively perceived by the patient andthe surgical team.
In conclusion, the Jost technique of cartilage splitting with-out stitches leads to excellent outcomes. The ear spontane-ously assumes a natural shape after the cartilage scoring. Weobserved no instances of recurrence and few complications,all of which were minor. This procedure requires no use of non-absorbable sutures to bend the cartilage, avoiding many com-plications. The learning curve is rapid. Jost otoplasty is safe,reliable, and reproducible, with long-lasting outcomes. The Josttechnique can also be useful for secondary otoplasty after failedStenström or Mustarde procedures.
ARTICLE INFORMATION
Accepted for Publication: February 4, 2013.
Published Online: August 29, 2013.doi:10.1001/jamafacial.2013.326.
Author Contributions: Drs Obadia and Quilichinicontributed equally to this work.Study concept and design: Obadia, Quilichini,Leyder.Acquisition of data: Obadia, Quilichini, Hunsinger.Analysis and interpretation of data: Obadia,Quilichini.Drafting of the manuscript: Quilichini, Hunsinger.Critical revision of the manuscript for importantintellectual content: Obadia, Quilichini, Leyder.Statistical analysis: Obadia, Quilichini, Hunsinger.Obtained funding: Obadia.Administrative, technical, and material support:Obadia, Quilichini, Leyder.Study supervision: Obadia, Quilichini.
Conflict of Interest Disclosures: None reported.
Previous Presentation: This study was presentedat the Société Française de Chirurgie PlastiqueReconstructrice et Esthétique (SOFCPRE)—Day ofYoung Plastic & Reconstructive Surgeons; March 10,2012; Paris, France.
REFERENCES
1. Dieffenbach JF. Die Operative chirurgie. Leipzig,Germany: F. A. Brockhaus; 1845.
2. Richards SD, Jebreel A, Capper R. Otoplasty:a review of the surgical techniques. ClinOtolaryngol. 2005;30(1):2-8.
3. Chongchet V. A method of antihelixreconstruction. Br J Plast Surg. 1963;16:268-272.
4. Becker OJ. Surgical correction of the abnormallyprotruding ear. Arch Otolaryngol.1949;50(5):541-560.
5. Stenström SJ, Heftner J. The Stenströmotoplasty. Clin Plast Surg. 1978;5(3):465-470.
6. Farrior RT. A method of otoplasty: normalcontour of the antihelix and scaphoid fossa. AMAArch Otolaryngol. 1959;69(4):400-408.
7. Furnas DW. Otoplasty for prominent ears. ClinPlast Surg. 2002;29(2):273-288; viii.
8. Jost G. Atlas of Aesthetic Plastic Surgery. Paris,France: Masson; 1975.
9. Stenström SJ. A “natural” technique forcorrection of congenitally prominent ears. PlastReconstr Surg. 1963;32:509-518.
10. Mustarde JC. Correction of prominent earsusing buried mattress sutures. Clin Plast Surg.1978;5(3):459-464.
11. Schlegel-Wagner C, Pabst G, Müller W, Linder T.Otoplasty using a modified anterior scoringtechnique. Arch Facial Plast Surg.2010;12(3):143-148.
12. de la Fuente A, Sordo G. Minimally invasiveotoplasty. Aesthetic Plast Surg. 2012;36(1):77-82.
13. Mandal A, Bahia H, Ahmad T, Stewart KJ.Comparison of cartilage scoring and cartilagesparing otoplasty: a study of 203 cases. J PlastReconstr Aesthet Surg. 2006;59(11):1170-1176.
14. Scharer SA, Farrior EH, Farrior RT. Retrospectiveanalysis of the Farrior technique for otoplasty. ArchFacial Plast Surg. 2007;9(3):167-173.
15. Schwentner I, Schmutzhard J, Deibl M, SprinzlGM. Health-related quality of life outcome of adultpatients after otoplasty. J Craniofac Surg.2006;17(4):629-635.
16. Braun T, Hainzinger T, Stelter K, Krause E,Berghaus A, Hempel JM. Health-related quality oflife, patient benefit, and clinical outcome afterotoplasty using suture techniques in 62 childrenand adults. Plast Reconstr Surg.2010;126(6):2115-2124.
Research Original Investigation Cartilage Splitting Without Stitches
E6 JAMA Facial Plastic Surgery Published online August 29, 2013 jamafacialplasticsurgery.com
Downloaded From: http://archfaci.jamanetwork.com/ by a Wegner Health Science Info Ctr & USD User on 09/05/2013