case 1 - clevelandclinicmeded.com€¦ · • on exam: pleasant but anxious teen who has normal bmi...
TRANSCRIPT

Case Studies in Psoriatic Arthritis
Christopher Ritchlin, MD, MPH
Professor of Medicine
Director, Translational Immunology Research Center
University of Rochester Medical Center
Rochester, NY
Case 1
The teen with psoriasis and psoriatic arthritis

History
• 17 yo female raised in Indonesia now living in the US referred for management of PsA.
• Diagnosed with psoriasis at age 12 and managed with topicals. One year later developed joint pain and swelling and started on MTX 20 mg per week continued to the present. She has persistent psoriasis and joint pain. C/O nausea and mouth sores. H/O generalized anxiety disorder
• On exam: Pleasant but anxious teen who has normal BMI and vitals. Psoriasis over 5% BSA and T, Sw 2nd, 3rd MCP, PIPs. X rays without erosions
• How would you proceed with this patient?
Anxiety and depression in psoriasis and psoriatic arthritis
• Challenges faced by a teen
– Social stigma
– Need for lab draws every 2 weeks
– Commitment to chronic medication

Depression and anxiety prevalent in PsA
C-S study 83 PsA and 199 RA pts 1. 22% PsA vs 25% RA but 37% PsA polyarthritis depressed and anxious 2. 10% PsA vs 34% RA on meds. 3. Body symptoms independent correlates of physical HRQOL in PsA 4. PsA pts more likely to attribute illness to psychological factors
Kotsis, K et al. Arthritis Care Res, May 2012
Psoriasis Center URMC Psoriasis Center

Followup 2 years later
• Patient has continued on MTX. Currently entering sophomore year at Cornell. Interested in switching to anti-TNF agent. Wants to drink socially and tired of persistent psoriasis, joint pain, nausea & fatigue and recurrent blood draws.
• On exam- psoriasis over 2% BSA and T, Sw, 2nd 3rd MCP and PIPs in the R hand. Remainder of exam normal.
• PPD strongly positive and IFN release assay negative. BCG was administered as an infant in Indonesia. She routinely travels back and forth between US and Indonesia. HIV neg.
• What is your next step?
Drug Regimens for LTBI
Drug Regimen Liver toxicity
Stop Drug %
INH 300/d X9 mo or 900 twice a week X 6 mo
3.8 3.7
RIF 600/d X 4 mo 0.7 2.1
RIF + INH 600 RIF/d + 300 INH/d X 3 mo ? 4.9
Rifapentine + INH 900 RIFA + 900 INH/wk X 3 mo 0.4 4.9*
Horsburgh CR et al, NEJM, April 2011 Sterling TR et al, NEJM, Dec 2011

Case #2
A 38 yo woman with psoriatic disease and UBOs
Case #2
38 yo WF who developed psoriasis 6 years ago. She had moderate plaques that did not respond to topicals. The psoriasis worsened and involved 40% BSA.
She then developed PsA of the peripheral joints. MTX was started but stopped due to increased LFTs in the setting of fatty liver.
She was started on etanercept and both the joints and skin responded. Recently, she noted a holocranial headache and numbness in the UEs.

Exam and Data
Exam Obese WF NAD Skin: plaques limited to the elbows MSK: fusion of the L 2-4 IP joints of the feet NEURO: no focal findings Data MRI: multiple enhancing demyelinating lesions CSF: normal EMGs/NCVs: normal The etanercept was stopped and she was treated with oral solumedrol 1 mg/kg and over 6 weeks her symptoms improved but the skin and joint disease returned after the steroid taper.
Case #2
How would you treat her skin and joint disease?
1. Resume etanercept
2. Adalimumab
3. MTX
4. LEF
5. Ustekinumab
6. Abatacept
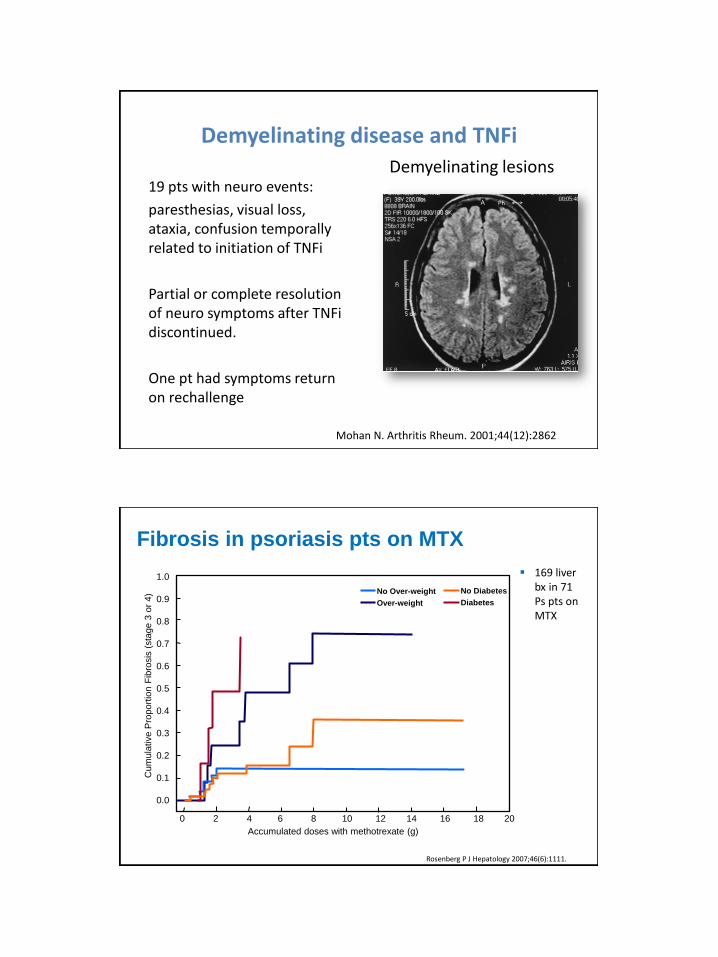
Demyelinating disease and TNFi
19 pts with neuro events:
paresthesias, visual loss, ataxia, confusion temporally related to initiation of TNFi
Partial or complete resolution of neuro symptoms after TNFi discontinued.
One pt had symptoms return on rechallenge
Demyelinating lesions
Mohan N. Arthritis Rheum. 2001;44(12):2862
Fibrosis in psoriasis pts on MTX
169 liver bx in 71 Ps pts on MTX
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Rosenberg P J Hepatology 2007;46(6):1111.
Cum
ula
tive P
roport
ion F
ibro
sis
(sta
ge 3
or
4)
0 2 4 6 8 10 12 14 16 18 20
Accumulated doses with methotrexate (g)
No Over-weight
Over-weight Diabetes
No Diabetes

Ustekinumab in PsA: Summit 1
• Phase III DBRPCT
• 409 PsA, 206 placebo
• 45 & 90 mg sc q12Wk
• DMARD failures
• 49% on MTX
Week 24
• Sig improvement in
dactylitis, enthesitis and
HAQ at Wk 24
• PASI75 = 60%
• AEs: 2 pts with
erythroderma and 1 CVA in
Rx group
• Radiographic data under
analysis
Ustekinumab effective for skin and MSK inflammation in PsA
23
9 2
42
25
12
50
28
14
0
20
40
60
80
100
ACR20 ACR50 ACR70
Perc
ent of
patie
nts
McInnes et al. EULAR 2012, Berlin
P<0.001
Ustekinumab is not effective for MS
Phase II RDBCT 249 pts with RRMS
Cumulative endpt was # gad enhancing MRI lesions at week 23
UST no decrease in primary endpoint and no exacerbation of demyelinating events.
Segal BM. Lancet Neurol 2008;7:796

Case #3
45 yo female with arthritis and psoriasis

45 y.o. female
Presents with pain and swelling in fingers & toes. She was diagnosed with psoriasis at 25 years of age. GP prescribed anti-inflammatories with mild benefit. She is a mother of 4 children and works fulltime as a shop
assistant.
Sister diagnosed with pulmonary TB x 1 yr previously, All family members screened for latent TB, however subject
declined.
Case 3
Before Wk 12 Post
Case 3

Case 3
Case 3

Case 3
Case 3
• What treatment would you consider next?

Therapeutic Options
• Corticosteroids (CS) alone
• CS + DMARD
• CS + DMARD + TNFi
• Other Biologics
MIPA: MTX is not a DMARD in PsA
• 6-month DBRCT of MTX 15 mg/wk vs
PBO
• 1° EP: PsARC
2° EPs: ACR20, DAS28, global
and skin scores
MTX PBO
Baseline 109 112
Completed 71 77
• No difference in SJC, TJC, CRP/ESR, PsARC, ACR20, DAS28 at 3 and 6 months
• Pt, MD global and skin scores significantly improved at 6 months (P=0.03, 0.02, 0.02)
Kingsley GH et al, Rheumatology 2012
OR with 95% CI for composite measures
PsARC
ACR20
DAS28
5.00 1.00 0.50 Log OR
Despite issues with study design, MTX does not have disease-remitting properties

Case 3
• Psoriasis
• + Synovitis DIPJ
• + Nail dystrophy
• + Dactylitis