case study 4 boy with attention deficit -...
TRANSCRIPT

Case Study 2: 1
Running head: CASE STUDY 2: BOY WITH ATTENTION DEFICIT
Case Study 2: Boy with Attention Deficit
Kim Bookout
Texas Woman's University

Case Study 2: 2
Case Study 2: Boy with Attention Deficit
Subjective Data
Patient Profile
Identifying Factors
The patient is an 8-year old white male who presents to 18 & Under MD with his mother
for evaluation of attention difficulties at school.
Background Information
Chief Complaint
Mom reports that the child is having difficulties at school with paying attention in class.
He has recently brought home several failing grades (20’s and 30’s) on work that he has
previously done very well.
History of Present Illness
The patient has had some failing grades during this school year unlike all other school
years. He has previously been a straight-A student. The patient was tested for LEAP (gifted-
talented program) because of his academic excellence. However, now, in second grade, he is
having more difficulties. The patient’s mother further reports that he has difficulty following
mulit-step instructions at home. Mom noticed some of the same tendencies in first grade but
because he did so well in class, no measures were taken. Despite the failing grades, the patient’s
teacher reports that he typically knows the answer to the questions missed but there is a
disconnect on getting it on paper. The patient’s teacher reports that his symptoms seem to have
worsened since the Christmas break. (Mom reports that the child’s older brother was home for 2
weeks during the break.)
Past Medical History
Case Study 2: 3
Illnesses
1. Strabismus (both eyes) 2. Amblyopia
Allergies
1. Latex 2. NKDA
Surgeries
1. Circumcision and Meatoplasty, March 2007 2. Strasbismus repair x 1
Medications
1. None
Birth History
The patient was born to a G1 P1→2, 31-year old female via spontaneous vaginal
delivery. He was term weighing 8 lb 13 oz. Mom’s pregnancy was uncomplicated and he had no
problems at delivery. He was breastfed initially and was discharged home with his mother from
the hospital.
Health Maintenance
1. Immunizations are up to date according to mom
2. Sick visits only in our office (4/16/07; 1/30/09; 6/8/09; 7/9/09; 7/13/09; 1/18/10)
3. Optometry exam 7/09, glasses
Social History
The patient is an 8-year old white male who lives at home with his mom, dad and 10-year
old brother. He attends public elementary school. He has no history of chronic disease. The
family lives in a single story home in a safe, suburban neighborhood. His father is a local realtor
and mom went back to work this year teaching 2nd grade. (Mom and dad elected to send the boys

Case Study 2: 4
to the elementary school in their neighborhood instead of the school where mom teaches.) The
family is privately insured but has experienced some financial challenges in the past year
according to the mother. The patient likes school and his teacher. He has several friends. He also
enjoys playing soccer in a local recreation league.
Family History
The patient’s father is 50 years old. He has a history of nasal allergies but no other
chronic disease. His mother is 39 years old and also has no chronic illness. The extended family
history is negative for diabetes, heart disease, kidney disease and lipid disorders. His paternal
grandfather has a history of alcohol abuse. The patient’s brother has a history of reactive airway
disease. He has one maternal uncle with ADHD. His father had nocturnal enuresis until an
advanced age. His mother suffers from sleepwalking including binge eating overnight. She now
has placed locks on the pantry and refrigerator to prevent this nightly overeating.
Review of Systems
General health: Good energy level. Reports difficulty in waking each morning. Does not wake feeling “refreshed”. No weight loss.
Skin/Hair/Nails: No excess sweating, rashes, or changes in skin color.
HEENT: No headaches. Wears glasses and is scheduled for a second surgery for strabismus in February, 2010. Positive history of amblyopia and strabismus. No drainage from eyes. Denies congestion or allergy symptoms. Does report snoring during sleep. No oral lesions. No untreated cavities. No hearing deficit. Neck/ Lymph: Anterior lymph nodes enlarged but non-tender.
Breast: Not discussed.
Chest/Lungs: No history of cough or reactive airway disease.
CV: No history of murmur, cyanosis. No dizziness or syncope. No edema to extremities.
Peripheral Vascular: No lower extremity pain, edema, or color changes.

Case Study 2: 5
GI: Good appetite. Denies constipation, diarrhea, reflux.
GU: Nocturnal enuresis with episodes every night. No dysuria or daytime frequency/urgency.
Endocrine: No temperature intolerance. No weight loss with adequate weight gain.
M/S: Steady gait. No hypotonia. No back pain. Full ROM to all extremities.
Neurological: No dizziness, syncope, or seizure history. Has difficulty following multi-step instructions. Psychiatric: No obvious feelings of depression or sadness. No anxiety. No social isolation.
Objective Data
Physical Exam
Vital signs:
Ht: 52” Wt: 62.8 lbs BP: 97/59 Temp: 97.8 Pulse: 122 R: 20
General: 8 year old Caucasian, well-developed, well nourished, male in no acute distress. Well-groomed and dressed appropriately. Interactive with provider and parent. Skin/Hair/Nails: Skin warm, pink, and dry. No rashes or lesions.
Head: Atraumatic, normocephalic.
EENT: Pupils equal, round, and reactive to light. Extraocular movements intact in all 6 fields of gaze. No nystagmus. Mild strabismus. Vision 20/40 R eye; 20/25 L eye; 20/25 Both eyes while wearing correction. Hearing exam passed on R and L at 25 and 40 decibels. Tympanic membranes clear bilaterally. Nares patent. No erythema noted. Tonsils are 4+ with no exudates. Uvula midline. Soft and hard palate intact. No dental caries. Mild plaque buildup to lower teeth. Neck/Lymph: Supple. No lymphadenopathy.
Chest/Lungs: Lungs clear to auscultation bilaterally. No increased work of breathing.
Cardiovascular: Regular rate and rhythm. S1S2 noted with no murmur.
Abdomen: Soft, nontender. No distention. Bowel sounds normoactive. No hepatosplenomegaly. No masses. No CVA tenderness. Breasts: Not examined.
Musculoskeletal: Full range of motion all extremities. Muscle tone adequate.

Case Study 2: 6
Extremities: Warm and well perfused. Peripheral pulses 2+ bilaterally. No swelling.
Genetalia: Not examined.
Rectal: Not examined.
Neurological: Strength 5/5 all extremities. Normal tone. Steady gait. No mental status changes. DTRs intact. Psychiatric: Awake, alert and oriented to person, place, and time. The patient is interactive with provider and parent. He is able to describe the reason for his visit on this date. Previous Labs: None
Discussion of Findings:
This patient presents with persistent difficulties in school/academic activity with a recent
exacerbation of symptoms. Despite having a previous record of straight-A’s and meeting the
initial requirements for testing for the gifted-talented program, he is struggling with work that is
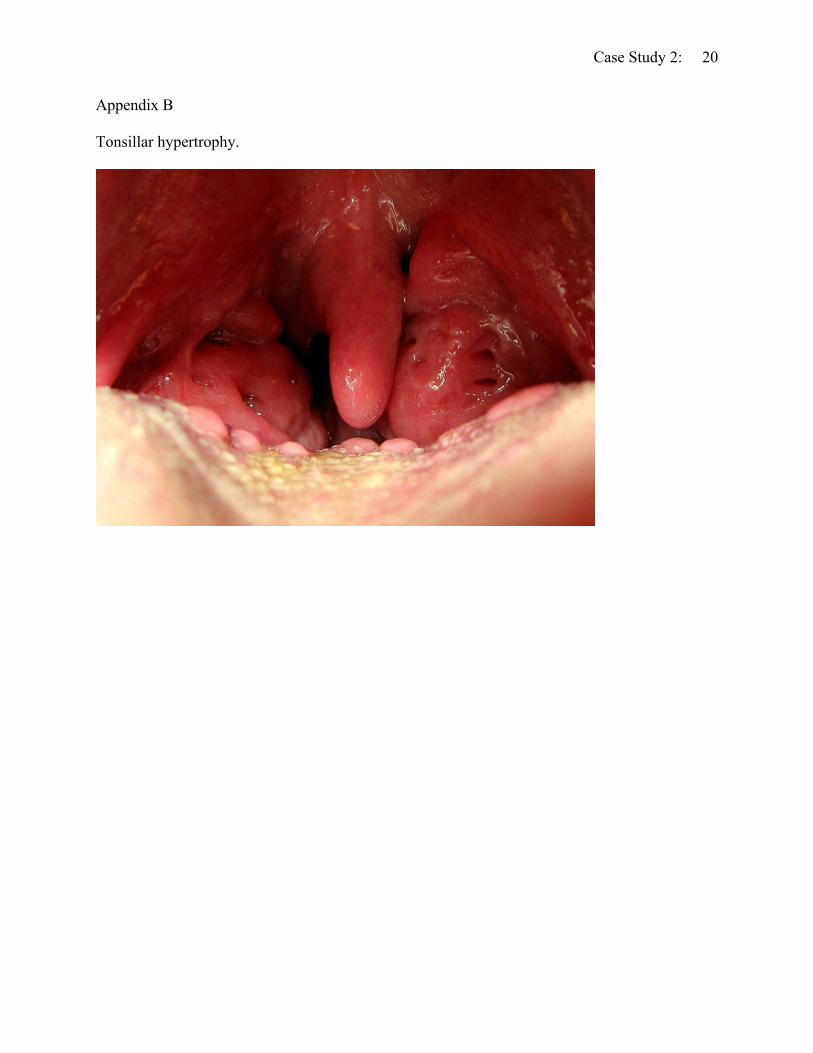
seemingly easy for him. Additionally, he presents with tonsillar hypertrophy, a history of snoring
and bedwetting. There is some evidence to suggest that tonsillar hypertrophy leads to snoring
which may be indicative of obstructive sleep apnea. He has never been evaluated for attention
deficit hyperactivity disorder (ADHD). He has a positive family history of ADHD (2nd degree
relative), nocturnal enuresis (father), and sleep disturbance (mother). His hearing and vision
exam are within normal limits.
Assessment/Impressions
1. Tonsillar hypertrophy 2. Nocturnal Enuresis 3. Attention Deficit/Hyperactivity Disorder (ADHD)
Attention deficit hyperactivity disorder is the most common psychiatric condition of
childhood and affects almost two million children in the United States (McGuinness, 2008).
Diagnosing ADHD can be a challenge as it is thought to be among a group of conditions instead

Case Study 2: 7
of a distinct process and is frequently seen with other behavior disorders such as oppositional
defiant disorder, anxiety disorder and depression (Spencer, 2006). It is also seen with other
genetic disorders such as fragile X, Williams syndrome, Angelman syndrome, Kleinfelter’s
syndrome and Turner’s syndrome (Hay, Levin, Sondheimer, & Deterding, 2009). Thus, organic
causes for ADHD must be ruled out.
ADHD has a definite genetic component with several different genes identified as
candidates. It is thought, however, that multiple genes are responsible for the disorder.
ADHD is expressed with great variability among children. There is a triad of symptoms
associated with ADHD: impulsivity, inattention, and hyperactivity. Some children experience
more inattentiveness without hyperactivity while others express inattentiveness, defiance, and
hyperactivity. In order to meet the diagnostic criteria for ADHD, symptoms must be present for
at least six months, appear prior to the age of seven years, and impair the child’s academic,
social, and familial environments (National Institute of Mental Health, 2008).
Differential Diagnoses:
1. Obstructive sleep apnea 2. Learning disability
Chronic Diagnoses:
1. Strabismus 2. Amblyopia
Plan
Laboratory Tests:
None.
Diagnostic Tests:
1. NICHQ ADHD Primary Care Initial Evaluation

Case Study 2: 8
2. NICHQ ADHD Teacher Informant Evaluation 3. NICHQ ADHD Parent Informant Evaluation 4. Hearing Screen 5. Vision Screen 6. Sleep Study
Health Maintenance:
Up to date
Medications:
1. Omega 3 vitamin chews x 2 po daily
Education:
During the visit, mom was instructed regarding possible diagnoses as all co-morbid
factors were discussed (snoring, bedwetting, fatigue, and behavior problems). Education was
also provided with regard to medical management of ADHD as well as sleep-disordered
breathing or obstructive sleep apnea. The patient’s mom and dad are both in favor of medication
for ADHD should the diagnosis be made. A review of the role of the ENT physician was
provided specifically regarding tonsillectomy and adenoidectomy. In addition, a brief overview
of a sleep study was given along with its purpose in determining the presence of obstructive
sleep apnea. It is important to maintain open communication with families who are dealing with
ADHD so that they are comfortable with alternative plans, medications, and adjuvant care or
therapies available.
Referral:
1. ENT
2. Pulmonolgy—Sleep study
Follow-up and Continuity of Care:

Case Study 2: 9
The patient’s mother was provided with forms for completion (NICHQ ADHD Parent &
Teacher Informant) to determine the presence of Attention Deficit Disorder. She was instructed
to proceed with scheduling an appointment with the ENT specialist and the pulmonology sleep
study specialist. Once the forms are complete, they will be returned to the office for scoring and
determination for the need for medication.
Update:
The patient’s mother and teacher completed the NICHQ forms. See Appendix A. The
forms were scored to reveal low scores in all categories. Thus, a diagnosis of ADHD was not
made. The family proceeded with consultation with the ENT for tonsillar hypertrophy. On exam,
the ENT explained to parents that he was 50/50 regarding surgery
(tonsillectomy/adenoidectomy) and was guarded in terms of whether or not the surgical
intervention would eliminate his symptoms of attention deficit and bedwetting. The ENT
encouraged the parents to proceed with the sleep study. A sleep study is scheduled for mid-
February.
Discussion
In the United States almost 60% of children diagnosed with ADHD are treated with
pharmacotherapy as opposed to only 1% of Finnish youth with ADHD being medicated
(McGuinness, 2008). In a study of 457 children in Finland, researchers found that by late
adolescence, children who had been treated with medications for ADHD were on track to
perform as well as those who did not receive medications both academically and socially
(Smalley et al., 2007). In the United States, researchers with the National Institute of Mental
Health Collaborative Multisite Multimodal Treatment Study of Children With Attention-
Deficit/Hyperactivity Disorder evaluated 579 children with ADHD. The children were randomly

Case Study 2: 10
assigned to four treatment groups with medication only, intensive behavior therapy, combination
medication and behavior therapy, and a community treatment control group. While all groups in
the study improved, the most improvement was seen in the children receiving a combination of
medical management and behavioral therapy with regard to social skills, aggressive behaviors,
and parent-child relationships. Thus, the role of behavioral management for children with ADHD
is further established.
Parents of children with ADHD often struggle with the decisions regarding treatment.
This is especially true for the first child in the family being diagnosed with the disorder.
Stimulant medications have been used for many years and are effective for 70-90% of the
children who take them (Hay et al., 2009). The side effects of stimulant medications are often
what concern parents the most. The most common side effects are insomnia and anorexia or
appetite suppression. Less common side effects are tics, seizures, and sudden cardiac death. It is
for the latter that the recommendation for a pre-treatment EKG was made by the American
Academy of Pediatrics (American Academy of Pediatrics, 2001).
Long-acting stimulants and short-acting forms of stimulants are available to use with
ADHD. Often the long-acting dose will allow symptom control through mid- to late-afternoon. If
parents find that children are unable to complete homework or are unable to pay attention during
afternoon sports practices, they may find it necessary to administer a short-acting dose in the
early afternoon (from noon to two o’clock). Alternative medications such as clonidine and
guanfacine (α2-adrenergic presynaptic agonists) may be used to decrease norepinepherine levels
which can be helpful in decreasing motor tics in children with Tourette syndrome and help those
children who are hyper-reactive to certain stimuli (Hay et al., 2009). Non-stimulant medications

Case Study 2: 11
(e.g., Strattera®) are also available but with mixed results regarding efficacy and control of
symptoms.
Sleep disordered breathing represents a group of diagnoses that includes primary snoring,
obstructive sleep apnea, and upper airway resistance. Obstructive sleep apnea is the most severe
of the disorders. It is estimated that the prevalence of sleep disordered breathing and primary
snoring is around 11% while obstructive sleep apnea is only around 3% of children (Wei, Mayo,
Smith, Reese, & Weatherly, 2007). The American Academy of Pediatrics issued clinical
practice guidelines for diagnosis and management of uncomplicated sleep apnea in children in
2002. The three signs and symptoms most indicative of sleep apnea are habitual snoring with
gasping or struggling to breathe, enlarged tonsils (see Appendix B), and daytime symptoms
including unrefreshed sleep, attention deficit, daytime fatigue, emotional lability, and
hyperactivity. When all three signs are present, it is not unreasonable for clinicians to proceed
with surgical intervention without having sleep study results (Hay et al., 2009). Many surgeons,
however, will obtain the gold standard polysomnography (sleep study) prior to any surgical
intervention.
Nocturnal enuresis is a condition that is common in childhood with an unclear etiology. It
affects boys three times more frequently than girls. Additionally, a family history reveals a
parent (usually the father) with prolonged night time bedwetting (Hay et al., 2009). It is
important to determine whether or not the child has neurological impairment, structural
abnormalities, urinary tract infection or diabetes that could contribute to or cause nocturnal
enuresis. (In this patient’s case, a previous provider completed a workup for organic causes of
his enuresis and all findings were negative.) The treatment for nocturnal enuresis places
emphasis on the fact that time and maturation often are the “cure” for enuresis. If, however,

Case Study 2: 12
children and parents would like to proceed with therapy, several options exist. The first is to
reduce fluid intake prior to bedtime. The second is to employ strategies to improve bladder
capacity by having the child hold his urine as long as possible during the day. Prompted voiding
is another option for children with bedwetting but has mixed results. In fact, using any of these
options may result in a disappointing outcome with less than 60% success rate (Hay et al.).
Another option is the bedwetting alarm. Anecdotal reports from parents state the child who is
using the alarm is typically the last family member to wake when the alarm sounds. In other
words, the sound sleeper is likely not to benefit from the alarm. Desmopressin (DDAVP) is a
pharmacologic option that may be given intranasal or oral. It is an antidiuretic hormone analog
that prevents urination. (Intranasal preparations have been unavailable for the past two years
(personal communication, D. Naylor, February 4, 2010)). Its use can result in complete remission
of bedwetting in as much as 50% of children for the duration of using the product. This is an
excellent option for use with children attending summer camp and sleepovers. Counseling for
parents should emphasize the need to allow the child time to outgrow the behavior. There is
some discussion in the literature discussing the relationship between nocturnal enuresis and
attention deficit (Elia et al., 2009). The frequent co-occurrence of the two conditions is
suggestive of genetic crossover in children.
Ultimately, clinicians must consider several factors in the diagnosis and management of
attention deficit/hyperactivity disorder. The presence of comorbid symptoms such as sleep
apnea, tonsillar hypertrophy, daytime fatigue, and nocturnal enuresis, may prompt parents and
clinicians to proceed with surgical intervention (tonsillectomy and adenoidectomy) to decrease
problems associated with tonsillar hypertrophy and sleep disordered breathing. If, however,

Case Study 2: 13
surgical intervention is not recommended, parents and clinicians may wish to proceed with
pharmacologic treatment for attention deficit/hyperactivity disorder.

Case Study 2: 14
References
American Academy of Pediatrics (2001). Clinical practice guideline: Treatment of the school
aged child with attention-deficit/hyperactivity disorder. Pediatrics, 108, 1033
Elia, J., Takida, T., Daberadinis, R., Burke, J., Accardo, J., & Ambrosini, P. et al. (2009).
Nocturnal enuresis: A suggestive endophenotype marker for a subgroup of attention
deficity/hyperactivity disorder. The Journal of Pediatrics, 155, 239-245.
Hay, W. W., Levin, M. J., Sondheimer, J. M., & Deterding, R. R. (Eds.). (2009). Current
diagnosis & treatment: Pediatrics (19th ed.). New York: McGraw Hill.
McGuinness, T. M. (2008). Helping parents decide on ADHD treatment for their child. Journal
of Psychosocial Nursing, 46(8), 23-27.
National Institute of Mental Health. (2008). Attention deficit hyperactivity disorder [Fact sheet].
Retrieved from http://www.nimh.nih.gov/health/publications/adhd/complete-
publication.shtml
Smalley, S. L., McGough, J. J., Moilanen, I. K., Loo, S. K., Taanila, A., & Ebeling, H. et al.
(2007). Prevalence and psychiatric comorbidity of attention-deficit/hyperactivity disorder
in an adolescent Finnish population. Journal of the American Academy of Child and
Adolescent Psychiatry, 46, 1575-1583.
Spencer, T. J. (2006). ADHD and comorbidity in childhood. Journal of Clinical Psychiatry,
67(Suppl. 8), 27-31.
Wei, J., Mayo, M., Smith, H., Reese, M., & Weatherly, R. (2007). Improved behavior and sleep
after adenotonsillectomy in children with sleep disordered breathing. Archives of
Otolaryngology Head & Neck Surgery, 133, 974-979.

Case Study 2: 15
Appendix A
NICHQ forms.

Case Study 2: 16

Case Study 2: 17

Case Study 2: 18

Case Study 2: 19
Case Study 2: 20
Appendix B
Tonsillar hypertrophy.