case study: continuous co monitoring aids delivery...
TRANSCRIPT

I s sue No. 10, Spr ing 2010Q u a rter ly Review
c o ntinued on page 5
Case Study: Continuous CO Monitoring AidsDelivery in High-Risk Patient
Women who devel-oped peripartum cardiomyopathy duringor after one pregnancyare at high risk for arecurrence during sub-sequent pregnancies.Defined as a cardiomy-opathy of unknowncause that occurs inthe peripartum period(the last month ofpregnancy or withinfive months of delivery) in womenwithout preexisting heart disease, theincidence of this disorder in the UnitedStates is up to one in 2000 live births;it can be fatal.
In such patients, careful monitoringduring labor, delivery, and the immedi-ate postpartum period is essential tominimize morbidity and mortality. Atthe Society for Obstetric Anesthesia andPerinatology annual meeting, Dr. AlexPue presented his experience with onesuch patient at the Sharp/Mary BirchHospital for Women in San Diego, CA.
This 28-year-old woman had experi-enced postpartum cardiomyopathy twoyears earlier with her first pregnancy,with an ejection fraction (EF) of 25%.Following medical treatment, the EFimproved to 55% and her conditionstabilized. Two years later, she present-ed at 36 weeks' gestation; echocardio-graphy showed evidence of moderate
mitral regurgitationand an EF of 45%.
“We knew that therisk of cardiomyopa-thy is greatest duringlabor, delivery, and thefirst few postpartumdays due to increasesin cardiac output (CO)related to increasedmetabolism, straining,and fluid mobiliza-
tion,” Dr. Pue told CCContinuum.
Following consultation with perinatol-ogy, anesthesiology, cardiology, and thepatient, it was agreed that vaginaldelivery was the best option. The grouprejected a Cesarean section because itcarries its own risks and hemodynamicscan rapidly change during the proce-dure. “Vaginal delivery is preferred insuch situations,” noted Dr. Pue,
“because blood loss and large volumechanges are minimal. Overall, there isbetter hemodynamic stability and lesslikelihood of postoperative complica-tions.”
Experts ReviewEvolution of the ICU and Critical CareMedicine
Drs. Ake Grenvik and Michael Pinsky of the University of Pittsburgh havepublished a thoughtful review of thedevelopment of the critical care medi-cine discipline over the past 100+ years.Some of the points they cover are:
■ British nurse Florence Nightingale isconsidered to be the first to have usedan intensive care unit (ICU) in 1854 during the Crimean war.■ The first U.S. ICU was described in1929, a unit at Johns Hopkins Hospitalfor neurosurgical patients. Widespreadexpansion occurred during the polioepidemic in the early 1950s. Today,practically all acute-care hospitals haveat least one ICU.■ The development of mechanical ventilation led to the establishment ofrespiratory ICUs in many university medical centers. ■ The general medical-surgical ICUs ofearly years have changed, with separateunits for general surgery, cardiothoracics u rg e ry, trauma, neuro s u rg e ry, neonates,burns and transplantation. ■ Critical care nurses remain the mostimportant personnel category in ourICUs. With their special skills andknowledge, they are essential for continuous intensive care of critically illpatients.
c o ntinued on page 7
“Monitoring with the FloTrac system gave us confidence in managing this high-risk patient.”

2
Critical Care ContinuumAdvances in Critical Care MonitoringQuarterly ReviewIssue No.10, Spring 2010 Elaine Chen, Executive EditorJan M. Headley, RN, BS, EditorTim Patz, Managing Editor
Published by Edwards Lifesciences LLC One Edwards WayIrvine, CA 92614800-424-3278949-250-2500www.Edwards.com/CriticalCaree m a i l : C r i t i c a l C a re @ E d w a rd s . c o m
Although several studies have shown that goal-directedoptimization of hemodynamics and fluid management canlead to improved outcomes, the methods used in thosestudies were either invasive or had other limitations.
German researchers evaluated intraoperative goal-directedtherapy with the minimally invasive, easy-to-use FloTrac system (the GDT group) and a standard management protocol (the control group). They compared outcomes in terms of length of hospital stay (LOS) and incidence ofcomplications from the two approaches in 60 high-riskpatients undergoing major abdominal surgery.
As reported to the American Society of Anesthesiologistslast fall and summarized in the previous issue ofCCContinuum ( Issue #9, Winter 2009), this randomized,controlled trial showed reduced LOS for those in the GDTgroup (median duration of stay 15 days vs 19 days for control group, p=0.006).
Subsequent analysis showed that fewer patients in the GDT group experienced complications (6 patients/20% vs 15 patients/50%, p=0.03). Further, the total number ofcomplications was reduced in the GDT group (17 vs 49complications, p=0.001). Complications identified includedinfections (pneumonia, abdominal, urinary tract, wound);need for respiratory support for more than 24 hours;
cardiovascular (pulmonary edema, arrhythmia, hypoten-sion, acute myocardial infarction, stroke); abdominal(bowel obstruction, upper gastrointestinal bleeding, anastomotic leak); and renal (urine output < 500 ml/day,acute renal failure requiring dialysis).
Hence the authors concluded that “intraoperative GDTbased on minimally invasive, flow-related parametersobtained by autocalibrated arterial waveform analysisresulted in a significant reduction in LOS and significantlyless perioperative complications compared with a stan-dard management protocol with pressure-based targetparameters.”
Mayer J, Boldt J, Mengistu AM, et al. Goal-directed intraoperative therapy basedon autocalibrated arterial pressure waveform analysis reduces hospital stay inhigh-risk surgical patients: a randomized, controlled trial. Critical Care2010;14:R18
Fewer Complications Seen in Goal-Directed Therapy with FloTrac Sensor
“Shorter stays, fewer complications seen in GDT group.”
CorrectionIn Critical Care Continuum issue #9, there was an error in Table 1 onpage 4 in the ASA report on the presentation by Mayer, Boldt, et al.The NT-proBNP plasma level for the intervention group on postopday 1 was listed as 833 ± 675. It should have said 832 ± 675.

3
Report from ISICEM2 9T H I n t e rnational Symposium on Intensive Care and Emergency Medicine
B russels, Belgium, March 9 – 12 , 2010
SI and CI Affected by Obesity, ProducingMisleading Values
Stroke index (SI) and cardiac index (CI) are calculated bydividing stroke volume (SV) and cardiac output (CO) valuesby the patient’s body surface area (BSA). SI and CI (low, high,or normal) are used to determine appropriate interventionsin hemodynamic management. However, when morbidlyobese patients have their SV or CO indexed, high absolutevalues become low SI and CI - perhaps misleadingly low.This may then cause therapeutic interventions opposite totheir needs.
Clinicians at the Baystate Medical Center in Springfield, MA,calculated BSA thresholds and determined what BSA levelswould classify an SV or CO value as abnormal. As shown inTable 1, for example, the BSA threshold for an SV of 90 is2.72, and the BSA threshold for a CO of 7 is 2.80; i.e., at anSV of 90, a BSA higher than 2.72 would classify the patientas having a low SI, and at a CO of 7, a BSA higher than2.80 would classify the patient as having an abnormal CO.(See Table 1.)
With the current obesity epidemic, more patients withextreme BSAs are encountered in the ICU. “Normal” rangesfor SI and CI may be inappropriate for patients with extremeBSAs. Hence these investigators caution relying solely on SIand CI to assess hemodynamic perf o rmance and re c o m m e n dthat SV and CO be considered along with other physiologi-cal parameters before making therapeutic decisions in thesepatients.
McGee WT, Nathanson BH. Threshold levels of extreme body surface area that maycause a misrepresentation of cardiac performance. Crit Care 2010; 14(Suppl 1).Abstract P96.
Compliance with Sepsis ResuscitationBundle Reduces Mortality, Even at 18Hours
The outcomes of implementation of severe sepsis resuscita-tion bundles (RB) within 6 hours have been reported; how-ever, researchers at Henry Ford Hospital (HFH) in Detroit, MI,studied outcomes when implementation is extended to 18h o u r s. Their prospective cohort study of 498 severe sepsisand septic shock patients over an 18-month period revealedthat mortality benefits are still significant with an extended compliance period. (See Table 2.)
In patients whose RBs were completed within 18 hours had a significantly lower hospital mortality of 10.2% (22%relative reduction). When adjusted for differences in baseline illness severity, the compliers had a greater reduction in predicted mortality of 26.8% vs 9.4% for non-compliers.The HFH Sepsis Collaborative Group concluded that the hospital-wide quality improvement initiative with emphasison the RB “significantly improved bundle compliance anddecreased hospital mortality.”
Coba V. Sepsis resuscitation bundle compliance in septic shock: improves survival andyet better late than never. Crit Care 2010; 14(Suppl 1). Abstract P398.
N o n - c o m p l i e r sC o m p l i e r s Significance
Within 18 hrs202 patients
At 18 hours296 patients
47.3% P < 0 . 0 33 7 . 1 %
Table 2. Hospital Mortality
Normal Values
SV60 –100
SI33 – 47
CO4 – 8
CI2.5 – 5
SV BSA CO BSA90 2.72 7 2.80
100 3.03 8 3.20110 3.33 9 3.60120 3.64 10 4.00130 3.94 11 4.40
Normal Values
Table 1. Critical BSA Thresholds
4
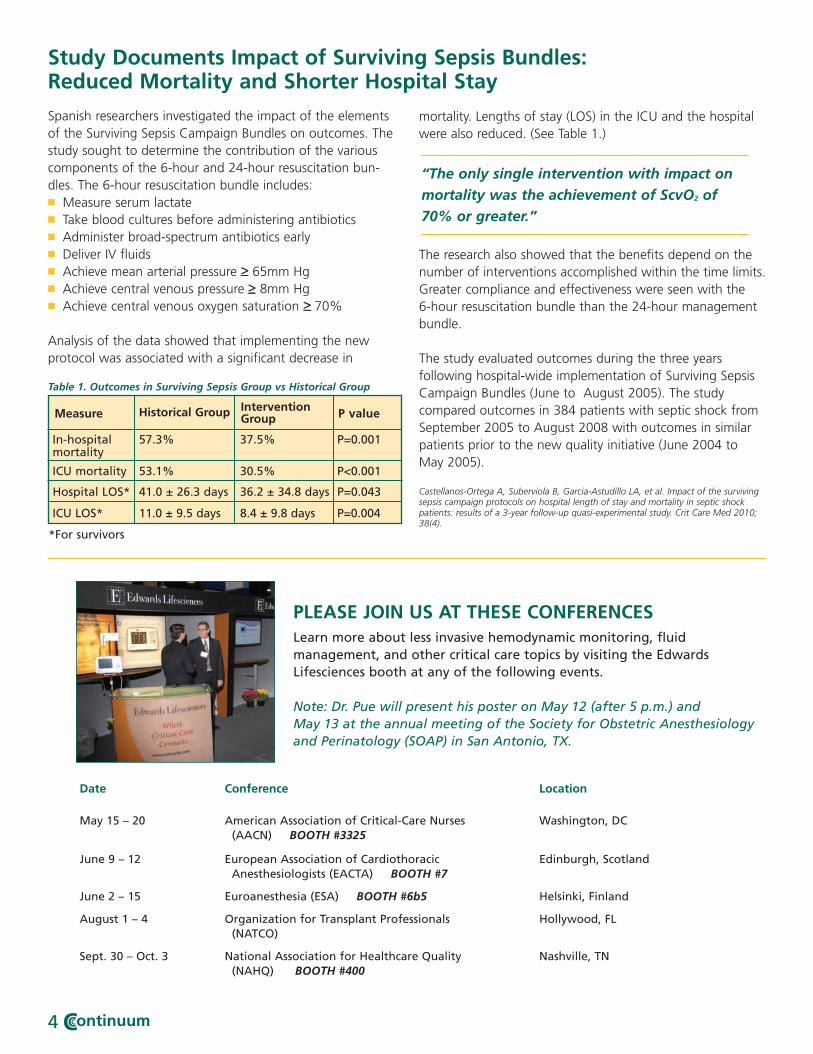
Spanish researchers investigated the impact of the elementsof the Surviving Sepsis Campaign Bundles on outcomes. Thestudy sought to determine the contribution of the variouscomponents of the 6-hour and 24-hour resuscitation bun-dles. The 6-hour resuscitation bundle includes: ■ Measure serum lactate■ Take blood cultures before administering antibiotics■ Administer broad-spectrum antibiotics early■ Deliver IV fluids■ Achieve mean arterial pressure ≥ 65mm Hg■ Achieve central venous pressure ≥ 8mm Hg■ Achieve central venous oxygen saturation ≥ 70%
Analysis of the data showed that implementing the newprotocol was associated with a significant decrease in
mortality. Lengths of stay (LOS) in the ICU and the hospitalwere also reduced. (See Table 1.)
The research also showed that the benefits depend on thenumber of interventions accomplished within the time limits.Greater compliance and effectiveness were seen with the 6-hour resuscitation bundle than the 24-hour managementbundle.
The study evaluated outcomes during the three years following hospital-wide implementation of Surviving SepsisCampaign Bundles (June to August 2005). The study compared outcomes in 384 patients with septic shock fromSeptember 2005 to August 2008 with outcomes in similarpatients prior to the new quality initiative (June 2004 toMay 2005).
Castellanos-Ortega A, Suberviola B, Garcia-Astudillo LA, et al. Impact of the survivingsepsis campaign protocols on hospital length of stay and mortality in septic shockpatients: results of a 3-year follow-up quasi-experimental study. Crit Care Med 2010;38(4).
>>
>
Date Conference Location
May 15 – 20 American Association of Critical-Care Nurses Washington, DC(AACN) BOOTH #3325
June 9 – 12 European Association of Cardiothoracic Edinburgh, ScotlandAnesthesiologists (EACTA) BOOTH #7
June 2 – 15 Euroanesthesia (ESA) BOOTH #6b5 Helsinki, Finland
August 1 – 4 Organization for Transplant Professionals Hollywood, FL(NATCO)
Sept. 30 – Oct. 3 National Association for Healthcare Quality Nashville, TN(NAHQ) BOOTH #400
PLEASE JOIN US AT THESE CONFERENCESLearn more about less invasive hemodynamic monitoring, fluid management, and other critical care topics by visiting the EdwardsLifesciences booth at any of the following events.
Note: Dr. Pue will present his poster on May 12 (after 5 p.m.) and May 13 at the annual meeting of the Society for Obstetric Anesthesiologyand Perinatology (SOAP) in San Antonio, TX.
Table 1. Outcomes in Surviving Sepsis Group vs Historical Group
Study Documents Impact of Surviving Sepsis Bundles:Reduced Mortality and Shorter Hospital Stay
Measure Historical Group InterventionGroup P value
In-hospitalmortality
ICU mortality
Hospital LOS*
ICU LOS*
*For survivors
57.3%
53.1%
41.0 ± 26.3 days
11.0 ± 9.5 days
37.5%
30.5%
36.2 ± 34.8 days
8.4 ± 9.8 days
P=0.001
P<0.001
P=0.043
P=0.004
“The only single intervention with impact on
mortality was the achievement of ScvO2 of
70% or greater.”

What’s New on the Web
From SCCM: Prevention of Intravenous CatheterRelated Infections in the ICUFaculty: Naomi P. O’Grady, MD, FCCM
Peter J. Pronovost, MD, PhD, FCCM
Intended for physicians, nurses, pharmacists, and otherproviders who care for critically ill patients, this programfocuses on current best practices related to the insertion of a central line catheter in the adult ICU patient and for maintenance and patency of the central line catheter.
This webcast is supported, in part, by medical educationgrants from Edwards Lifesciences, LLC, and BaxterHealthcare Corporation. It was aired on February 17, 2010, and is now archived at the SCCM site:h t t p : //w w w. s c c m . o rg / C o n f e re n c es/We b c a s ts/P a g e s /d e f a u l t y. asp x; click on the title of this program. It is accred-ited by ACCME and offers 1.5 contract hours for nurses, 1.5 AMA PRA category 1 credits for physicians, and 1.5 CEhours for pharmacists.
Register online for the annual CVT Critical CareC o n f e re n c e
The 7th annual Cardiovascular-Thoracic (CVT) Critical CareConference will take place in Washington, DC, September30 – October 2, 2010. This multidisciplinary CME confere n c ei n c l u d e s faculty presentations, symposia, audience-panel discussions and workshops addressing the major issues inCVT care. The latest management strategies for challengingclinical problems will be discussed as well.
Register online at http://www.facts-care.org /annual-details.html or via the OACCM site - www.oaccm.org.
Organization for Advancing Critical Care Monitoringwww.OACCM.org
Dr. Pue chose to use a minimally invasive cardiac functionmonitoring system (FloTrac system, Edwards Lifesciences)that continuously calculates CO, stroke volume (SV) and SVR (with a central venous line) based on radial arterialwaveform analysis. “Without the FloTrac system to monitorthe patient during labor and delivery, we probably wouldhave elected to deliver via C-section, even with its increasedrisks,” said Dr. Pue.
Continuous CO Monitoring continued from page 1
“This elevated level of monitoring helped give us confidence when walking the tightrope ofkeeping her comfortable without overdoing thephysiological response.”
OACCM has initiated a forum for critical care providers todiscuss current issues, to poll others on specific topics andneeds, to suggest areas for CME programs - just about anysubject pertinent to critical care. Go to “My Forum” atwww.OACCM.org to see what your colleagues are saying.
Check out the continuing education programs on the website of the Organization for Advancing Critical CareMonitoring. It’s free!
OACCM Accreditation Information
CME activity on the OACCM website has been planned andimplemented in accordance with the Essential Areas andPolicies of the Accreditation Council for Continuing MedicalEducation (ACCME) through the joint sponsorship of theInstitute for Medical Studies (IMS) and Med-CE-online.com.
Physicians: The Institute for Medical Studies is accredited bythe ACCME to provide CME for physicians. Please refer toindividual programs on the website for the maximum numberof category 1 credits that can be received toward the AMAPhysician’s Recognition Award. Each participant should claimonly those hours of credit that he/she actually spent in theeducational activity.
Nurses may claim credit for activities approved for AMA PRACategory 1 Credits™ in most states, for up to 50% of the nursing requirement for recertification.
As planned, the patient was admitted at 37 weeks’ gestationfor induction. The team’s goal was to achieve vaginal deliverywith minimal pushing, excellent pain control, and hemody-namic stability. Seven hours after induction, with a single pullof the vacuum and no pushing, a 2745-gram infant wasdelivered, with good APGAR scores. All hemodynamicparameters were stable and pain was well controlled. Thepatient was transferred to the surgical ICU three hours afterdelivery and to a monitored bed the following day. She wasdischarged at noon the next day. At three-month follow-up,she was asymptomatic with an EF of 45% to 50%.
Pue AF. Continuous cardiac output monitoring in a laboring patient with peripartumcardiomyopathy. Presented at 42nd annual meeting of the Society for ObstetricAnesthesia and Perinatology, May 2010; and interview with CCContinuum in October2009.
5

6
A number of speakers addressed the issue of fluid management in surgical patients during the Euroanaesthesiameeting in Milan.
■ German researchers evaluated the use of the FloTrac/Vigileo system (Edwards Lifesciences) to guide intraoperativefluid and catecholamine therapy in patients undergoingmajor abdominal surgery. Forty high-risk patients were ran-domized to standard care or an intervention group whosetreatment was guided by a protocol based on stroke volumevariation and cardiac index. They found that patients in theintervention group received significantly more colloid volumereplacement and more dobutamine; crystalloid volume re-placement and norepinephrine use was not diff e rent betweenthe two groups. The mean hospital stay was significantlyreduced in the intervention group; reduction in the meanICU stay was not statistically significant. (See Table below.)
Mayer J, Boldt J, Beschmann R, et al. Individualized intraoperative patient optimizationusing uncalibrated arterial pressure waveform analysis in high risk patients undergoingmajor abdominal surgery. Abstract 3AP4-3.
■ The reliability of urine output (UO) as a predictor of bloodvolume variations during surgery was examined by cliniciansin Cantabria, Spain. They compared UO to measures ofheart rate (HR), invasive mean arterial pressure (MAP), cardiac index (CI), stroke volume index (SVI), stroke volume
variation (SVV) using the FloTrac sensor (Edwards Lifesciences),central venous pressure (CVP) and ScvO2 using the PreSepcentral oximetry catheter (Edwards Lifesciences). Measure-ments were recorded before and after surgery and everyhour during the procedure in 23 consecutive patients under-going major surgical procedures. Normovolemia was main-tained using the institution’s algorithm. Statistical analysisrevealed no relation between UO and CVP, CI, SVI, SVV orScvO2; there was a relationship between UO and MAP. Theresearchers concluded that “UO should not be used as anintraoperative guide of blood volume loss/restitution duringmajor surgery.”
Solares G, Perez L, Rabanal M, et al. Urine output does not predict intraoperativeblood volume variations during major surgery. Abstract 4AP9-6.
■ Clinicians in Japan addressed the issue of blood loss duringhepatic surgery, which can be reduced by lowering centralvenous pressure (CVP). Noting that CVP is a poor indicatorof blood volume, they investigated the potential role ofstroke volume variation (SVV) to predict fluid responsiveness.Hemodynamic variables were assessed retrospectively in 14patients undergoing hepatic resection; all received mechani-cal ventilation. SVV, stroke volume index, and cardiac indexw e re measured with the FloTrac sensor (Edwards Lifesciences).Analysis of 1330 data points before and during the Pringletechnique showed that SVV correlated significantly to SVI(r=0.65, p<0.01), whereas CVP was not significantly corre-lated to other hemodynamic variables. They concluded thatSVV is “a useful predictor to evaluate preload” in hepaticsurgery.
Tateda T, Morita S, Sakamoto M. Stroke volume variation as a predictor of preload inpatients undergoing hepatic surgery. Abstract 3AP4-1.
Report from Euroanaesthesia 2009E u ropean Society of Anesthesiology
Milan, Italy, June 6 – 9, 2009
Standard Care Intervention P value
Mean hospital stay(days)Mean ICU stay(hours)
20.6 ± 8.1
49.2
14.8 ± 4.7
41.0
P=0.009
P>0.05
Reductions in SVV-guided group

7
Up to one-third of patients experience extubation failure,even after they have met the criteria of a two-step weaningprotocol. Clinicians in the ICU at Moinhos de Vento Hospitalin Porto Alegre, Brazil, evaluated the predictive value of cen-tral venous saturation (ScvO2) as a more accurate parameterfor detecting extubation failure in difficult-to-wean patients.
The six-month study enrolled 73 “difficult-to-wean” patients,defined as patients who had been mechanically ventilatedfor more than 48 hours and failed to tolerate their firstspontaneous breathing trial even after passing the two-stepweaning protocol. Extubation failure was defined as a needfor reintubation within 48 hours after extubation. The studyincluded assessment of ventilatory, blood gas, and hemody-namic parameters during mechanical ventilation and at the30th minute of spontaneous breathing.
Extubation failure occurred in 42.5% of the patients. Twovariables measured at the 30th minute of spontaneousbreathing that successfully predicted extubation failure wereScvO2 and oxygen extraction ratio (O2ER). Reduction ofScvO2 by 4.5% or more was an independent predictor ofreintubation (95% confidence interval 12.1-201.5lp<0.0001). A reduction of 17% or more predicted 100% of extubation failure.
The authors concluded, “Central venous saturation was anearly and independent predictor of extubation failure.” Theyhypothesized that this effect may be due to the increasedoxygen demand of the respiratory muscles during sponta-neous breathing. They also suggested that ScvO2 be includedin weaning protocols of difficult-to-wean patients, whichmay make the protocol a more useful and accurate tool forpredicting extubation outcomes.
Teixeira C, da Silva NB, Savi A, et al. Central venous saturation is a predictor of reintu-bation in difficult-to-wean patients. Crit Care Med 2010;38(2):491-6.
Experts Review continued from page 1
June 9 – 11: PediaSat Catheter Clinician Education Program Irvine, CA
July 8 – 9:FloTrac Sensor Clinician Education ProgramChicago, IL
July 15 – 16:Sepsis Clinician Education ProgramDallas, TX
September 22 – 24:FloTrac SensorSepsis Clinician EducationProgram Atlanta, GA
December 2 – 3:FloTrac Sensor Clinician Education ProgramIrvine, CA
UPCOMING EDUCATIONAL EVENTS SPONSORED BY EDWARDS
Drop in Central Venous SaturationCan Predict Extubation Failure
“Reduction of ScvO2 by 4.5% or more was anindependent predictor of reintubation.”
■ After AACN certification of critical care nurses was recog-nized, protocols have been developed that not only permit but actually require ICU nurses to intervene in various crisis situations, particularly cardiac arrest.
■ Respiratory therapists are another important category in American ICUs. The growth of a strong respiratory therapy arm in critical care medicine in North America has helped advance the development of artificial ventilation worldwide.
■ Fellowships in critical care medicine were first offered in the late 1960s and certification was begun in four specialties (anesthesiology, internal medicine, pediatrics and surgery) in 1986.
The authors also describe the professional societies and publica-tions dedicated to critical care medicine and the educationalopportunities that are available to allow practicing intensivists toremain abreast of the most recent advances and best practicesin the field.
“Critical care medicine has become the epicenter of acute-caremedicine,” the authors conclude.
Grenvik A, Pinsky MR. Evolution of the intensive care unit as a clinical center and criticalcare medicine as a discipline. Crit Care Clin 2009;25:239-50.
Edwards Lifesciences
One Edwards WayIrvine, California 92614
Any quotes used in this material are taken from independent third - p a rty publications and are not intended to imply that such third party reviewed or endorsed any of the products of Edwards Lifesciences. Rx only. See instructions for use for full prescribing information. Edwards Lifesciences, the stylized E logo, FloTrac, Vigileo and PreSep are trademarks of Edwards Lifesciences Corporation and are re g i s t e red in the United States Patent and Trademark Office. Early Goal-Directed Therapy is a trademark of Dr. Emanuel Rivers. ©2010 Edwards Lifesciences LLC. All rights re s e rved. AR05123
Q u a r ter ly Rev iew Spr ing 2010
We welcome your feedback. Please provide any input or suggestions to: [email protected]
E-mail option available
Would you prefer to receive via e-mail? It is available in a user-friendly “reader version.”
___ Yes ___ No If yes, please provide your e-mail
address here:_______________@__________________________
FAX this form to us at 949-250-5010. Or e-mail us at [email protected]. Thank you for your input.
What Do YOU Think?
How would you handlethe challenges of post-p a rtum cardiomyopathy? See page 1.
Pg. 1 Continuous CO monitoring in high-risk pregnancies.
Pg. 2 G o a l - D i rected Therapy with F l o Trac Sensor
Pg. 3 R e p o rt from ISICEM
Pg. 4 Impact of Surviving Sepsis Guidelines
Pg. 6 R e p o rt from Euroanaesthesia 2009
Inside this Issue