ccih 2015 juli hedrick breakout 4c
TRANSCRIPT
Lessons learned from health systems strengthening in
fragile contexts
Juli Hedrick, MPH, Design and Development Officer with Dr. Dennis Cherian, BHMS, MPH, MA Senior Director, Health
and Jonathan Papoulidis, Executive Advisor, Fragile States World Vision
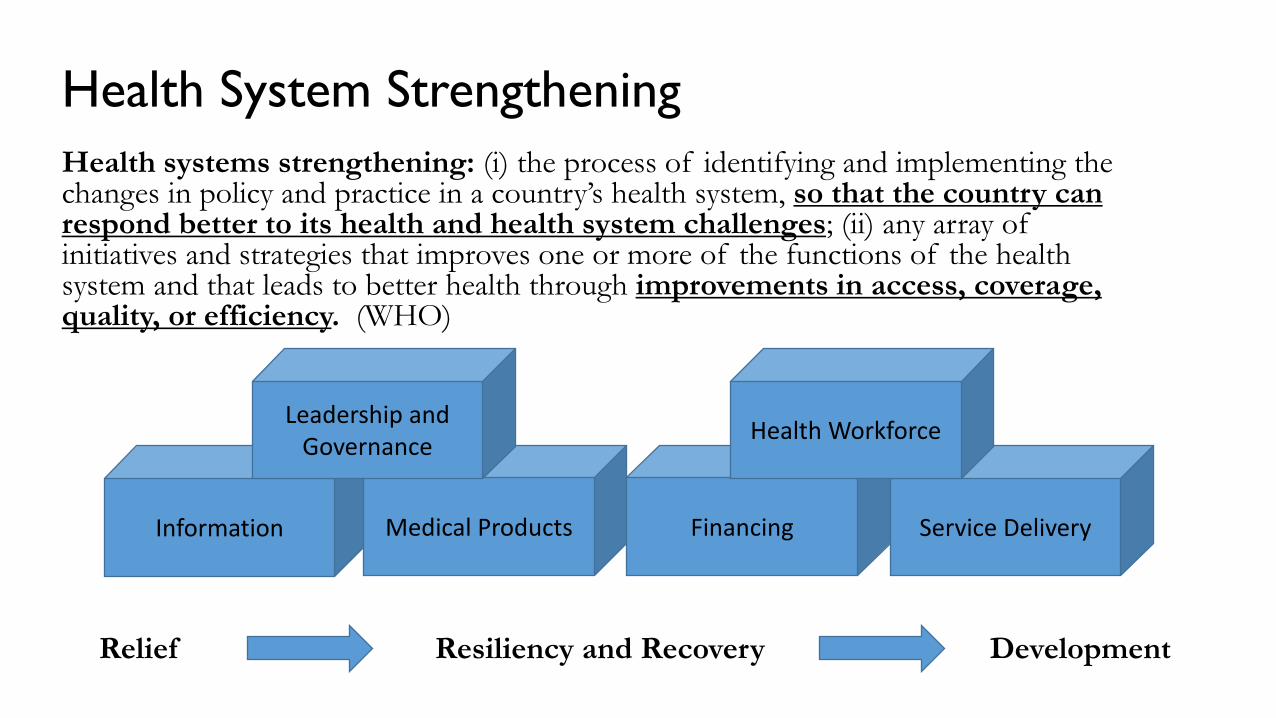
Health System Strengthening Health systems strengthening: (i) the process of identifying and implementing the changes in policy and practice in a country’s health system, so that the country can respond better to its health and health system challenges; (ii) any array of initiatives and strategies that improves one or more of the functions of the health system and that leads to better health through improvements in access, coverage, quality, or efficiency. (WHO)
Relief Resiliency and Recovery Development
Information Medical Products Financing Service Delivery
Health Workforce Leadership and Governance
Fragile States, Fragile Contexts Broken social contract between state and society, broken institutions, and low resilience to shock and stress
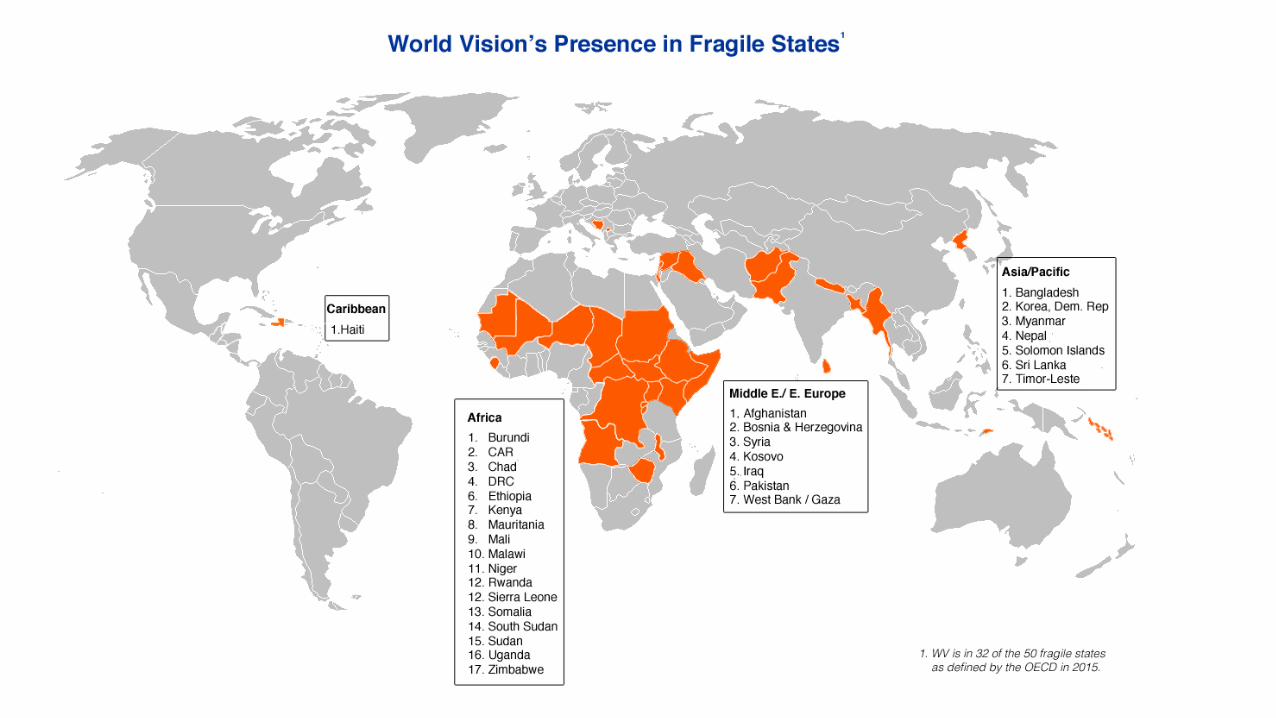
Fragile States Index: 50 most fragile states on a scored spectrum (World Bank, Fund for Peace)
WV is active in 32, with long term development programs in 17.
Fragile contexts: pockets of fragility that can occur in any state (consider Indonesia, Jordan, Lebanon)
Factors:
• Insecurity: war, conflict, drought, famine, flooding
• Instability: political, economic,
• Vulnerability: geographic or social access, extreme poverty, culture, gender, caste, tribe, religion
One-third of those living on less than one dollar per day currently live in fragile states; two-thirds will be in fragile states by 2030. (G7+)
USAID Child Survival and Health Grants Program
Afghanistan Better Health for Mothers and Children Project 2008-2013 Goal: To achieve sustained improvements in the survival and health of mothers, newborns and children Partners: The Herat Department of Public Health (DOPH) Afghanistan Ministry of Public Health (MOPH), Bakhtar Development Network, USAID Mission, Kabul Dimagi, Inc.
South Sudan Mother and Child Health Transformation Project 2010-2014 Goal: To reduce maternal, neonatal, infant and child mortality in Gogrial East and West counties of Warrap state through three strategic objectives that aim to 1) increase use of high impact low cost and feasible interventions for better maternal, neonatal, infant and child health (MNCH) outcomes, 2) strengthen capacity of the health system to deliver essential health services and 3) build and strengthen local and national partnerships to sustain improvements in MNCH. Partners: South Sudan Ministry of Health (all levels) Gogrial Women’s Network, USAID, Juba Mission
Keep the design as simple as possible
• Get a thorough situational analysis of fundamental health issues but also cultural and gender issues. Identify one or two most vital barriers to knowledge, behavior, health care seeking, distance, no provider, etc?
• Access (geographic, religious/ social, etc), quality, coverage. physical or social. Gender, inequity, mobility. Population dispersion. Caste, ethnic divisions. View every technical intervention – immunization, HBLSS, etc. through equity lens.
• Use operations research to dig deeper on other interventions • Design social interventions in addition to clinical care. • Simplify the staffing and the budget
Build human resources for health
• Assess availability and local capacity. Likely extremely limited – use short term volunteers, North/South or South/South collaborations, training programs.
• CHWs bridge the gap between community and facility. Work with low-level illiterate/ low literate frontline health workers Communicate visually, tools, counting beads
• Plan for high staff turnover • Explore the potential of mission hospitals as an extension
of the gov’t health facilities, pairing/ mentoring of staff, motivation, commitment, areas of growth.
Use mobile technologies where possible • Consistency in programming and reporting • Allows for continuation in tenuous security situations • In Afghanistan, WV taught frontline health workers to use
algorithms loaded onto mobile phones for improved maternal health outcomes
• Not an option in South Sudan – won’t work everywhere
Work with the formal health system
• Find the conduit that works: may be technical vs. political
• Link into or create coordination mechanisms: projects vs. system strengthening
• Use accountability measures: Citizen Voice and Action In Bangladesh: a network of mother-led savings groups improved health and nutrition outcomes by advocating for service delivery In DRC, WV has an MOU with the government to use CVA as the preferred method of social accountability. Over 500 officials from various ministries have been trained to use the scorecard.
Informal: Community health workers and community health systems – the best conduit of actual service delivery Shura in Afghanistan, former TBAs in South Sudan Literacy – counting beads, tools
Supervision: provide local support In an operations research embedded in a child survival grant in northern South Sudan, WV used a supportive supervision model to build capacity of illiterate frontline health workers.
Use mobile technologies where possible consistency in programming and reporting
allows for continuation in tenuous security situations
In Afghanistan, WV taught frontline health workers to use algorithms loaded onto mobile phones for improved maternal health outcomes
Work with informal health systems
Merge the formal and informal Joint meetings – rebuild relationships
Reports
High profile project visits
Monitoring and evaluation
Mandates and policies
Input from and reporting to all stakeholders
North/South collaboration
Security
• Be adaptable. • Identify local stakeholders/ organizations, strong decision
makers • Cultivate local ownership through use of advisory groups
– informed, equipped, aware of local situation. Best advocates.
In Afghanistan, the shura (local health committee) In South Sudan, the HHPs
Thank You