cell based model galila zaher, mrcpath assistant professor consultant hematologist kauh
TRANSCRIPT

Cell Based ModelGalila Zaher, MRCPath
Assistant ProfessorConsultant Hematologist
KAUH

VIIa
TF-BEARING CELL
ACTIVATED PLATELET
HEMOSTASIS
THROMBIN
FIBRIN HEMOSTATIC PLUG
INITIATION
OF HEMOSTASIS
PROPAGATIONOF HEMOSTASIS
TF
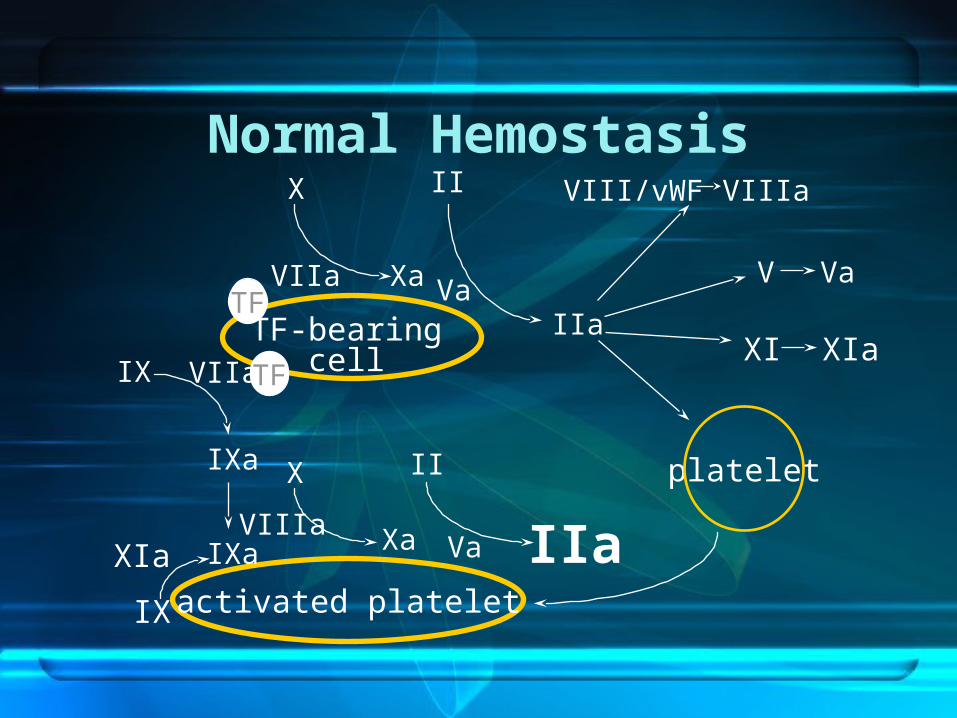
TF
X
Xa Va
II
IIaTF-bearingcell
VIII/vWF VIIIa
V Va
platelet
activated platelet
VIIa
VIIaIX
IXa
VIIIaVaIXa
X
Xa
II
IIa
TF
XIa
IX
XI XIa
Normal Hemostasis

IIa (THROMBIN)
FIBRINOGEN FIBRIN(SOLUBLE FIBRIN MONOMERS)
FXIIIa
FIBRINOLYSIS
TAFI
STABILIZED,CROSS-LINKED
FIBRIN(HEMOSTATIC
PLUG)
Thrombin FV FVIII
FVa FVIIa

0.60 U/mL
Fibrin Structure
0.10 U/mL
0.05 U/mL
0.03 U/mL
Blomback et al. 1994
(a)
(b)
(c)
(d)
Thrombin:

Thrombin Activity
0
0.005
0.01
0.015
0.02
0.025
0.03
0.035
0.04
0.045
0.05
0 20 40 60 80 100 120 140
Time (min)
Th
rom
bin
act
ivity
(dA
405
/min
)
With FVIII present(- FXI)
FVIII-deficiency
+ 50 nM FVIIa
+ 150 nM FVIIa
Kjalke et al. 1999

FACILITATE HEMOSTASIS • Enhance thrombin generation• Inhibit fibrinolysis• WHY FVIIa? • FVIIa not enzymatically active unless in
complex with TF• FVIIa not immediately inhibited by AT • FVII present in plasma • FVIIa added to hemophilia plasma with
inhibitors normalized APTT
Potential Use of rFVIIa• Increases thrombin generation • Hemophilia (FVIII/FIX deficiency)• Platelet disorders• Diffuse bleeding triggered by surgery and
trauma• Impaired initial hemostasis• FVII-deficiency• Liver disease (low levels of FVII)• OAC therapy (low levels of FVII)

TF
X
Xa Va
II
IIaTF-bearingcell
VIII/vWF VIIIa
V Va
platelet
activated platelet
VIIa
VIIa
VIIa Va
X
Xa
II
IIa
TF
XI XIa
Hemophilia

Haemophilia• FDA-approved Hemophilia with inhibitors• Efficacy in major surgery 90-100% (90-100 µg/kg q2
for first 48 hs, q4 hours on D3-D4then to q6 hours for another week (Shapiro et al 1998; Ingerslev et al 1997)
• Efficacy in serious bleedings 83-95% (Lusher et al 1998)
• Efficacy in home treatment 92% (Key et al 1998) • Acute bleeds in hemophilia >5 BU• No good laboratory markers for monitoring efficacy • TEG or Trend of quantitative D-dimer levels as a blood
counts and fibrinogen level

COST-EFFECTIVENESS in mild-mod HA bleeding – UK study
Clinical effectiveness – • rFVIIa: mean 2.3 doses of 90 ug/kg
controlled 92% of all minor bleeds within 24 hrs (Key et al 1998).
• FEIBA (aPCC): mena 3 doses of 75 units/kg controlled 79% of minor bleeds within 36 hrs (Hilgartner)

COST EVALUATION MILD-MOD BLEEDINGS IN HAEMOPHILIA
Average cost
Time to resolve
Mean number doses/episode
Mean time to resolution
Effectiveness:
OVERALL COST
rFVIIa £11,794
30 hrs 3.6 17.3 hrs
89.3% 9,113US$
FEIBA £20,46 58 hrs 4.8 43.6 66.7% 12,542
rFVIIa is safe and has a higher efficacy relative to other treatment options”.

The FENOC study• FEIBA (activated prothrombin complex concentrate
(aPCC).• Test equivalence of products in treatment of ankle,
knee, and elbow joint bleeding. • A prospective, open-label, randomized,crossover• Data for 96 bleeding episodes contributed by 48
participants were analyzed. • FEIBA and NovoSeven appear to exhibit a similar
effect on joint bleeds, although the efficacy between products is rated differently by a substantial proportion of patients. 2007 ASH

FVII-DEFICIENCY• Autosomal recessive 1/500 000 persons• Genetic & clinical heterogeneity• FVII activity <1% severe• Prolonged PT; normal APTT • There is only small number of patients
available (case series) • FDA-approved dose 15 -30µ g per kg, q6 -12 hs• Monitored by PT & its correction correlate
well with achievement of clinical hemostasis

USE OF rFVIIa IN FVII-DEFICIENCY
• N=32 treated in Compassionate and ER between 1988- 1999.
• Treated at 28 sites in 6 countries (AUS, DK, I,Malaysia, USA)
• Non-surgical episodes: 43 joint bleeds • EFFECTIVE in 37/43 (86%) episodes independent on
location of bleed. • Surgical episodes: 26• EFFECTIVE in 25/26 (96%) episodes. • 10 adverse events 2 pt developed Abs against FVII• FDA-approved dose 15 to 30µ g per kg q 6-12
hours• Monitored by the PT.

Preliminary guidelines for off-label use proposed in 2004
• The consensus panel related use of rFVIIa as appropriate in :
• Cardiac, thoracic, aortic, and spinal surgery• Hepatic resection• Hysterectomy; postpartum bleeding • Severe, multiple trauma substantial blood replacement
ineffective.• Non traumatic ICH <4 hours since onset of symptoms• Anti-coagulated patients with expanding hematomas.• Doses of 41 to 90 µg / kg recommended in adults for all
scenarios.• Correction of the pH value >7.2 • Multitrauma patients is 100 - 140 µg/ kg repeat dose

European Recommendations on the use of rFVIIa as an adjunctive treatment for massive bleeding
–

Trauma.• Uncontrolled massive hemorrhage is 2nd
cause of death • Massive hemorrhage : surgical / vascular and
a coagulopathic component.• ‘Lethal triad‘: consumption , dilution and
metabolic disorders • In cases of injury, TF is brought into contact
with naturally occurring FVIIa, to initiate thrombin
• Pharmacological doses, rFVIIa bind activated platelets at the site of injury and activate FIX and X directly, leading to a thrombin burst

BluntTrauma• Successful report for trauma in an Israeli soldier • Case series of 36 patients stopped bleeding in 72% of
cases • Several case studies ,case series , retrospective cohort• Conventional hemostatic measures have failed. • Promising addition to thrapeutic armamentarium • Multicenter, randomized, double-blind, placebo controlled
study by Boffard• Initial dose of 200 µg/kg , then 100 µg/kg, at 1 and 3
hours • Produced a significant reduction in the primary endpoint
RBC transfusion requirements , need for massive transfusion, and incidence of respiratory failure Grade B
• Penetrating trauma are uncertain, no recommendations can be made for this indication. Grade B

0
5
10
15
20
25
30
35
Blunt Penentrating
Trauma: % Patients Requiring > 20 Units RBC
rFVIIaPlacebo
%Pts
P=0.03
P=0.08
PenetratingBoffard et al.: J Trauma 2005


Recommendations on the use of rFVIIa as an adjunctive treatment for massive bleeding – a
European perspective• Not be used in prophylactically in elective surgery (grade A) • Use of rFVIIa in blunt trauma (grade B). • Not be recommended for use in penetrating trauma (grade B)• Not be recommended for use in liver surgery (grade B)• Not be recommended for use in or in bleeding episodes in
patients with Child–Pugh A cirrhosis (grade B). Bleeding after cardiac surgery (grade D).
• Postpartum hemorrhage (grade E)• Uncontrolled bleeding in surgical patients (grade E)• Monitoring of rFVIIa efficacy should be performed visually and
by assessment of transfusion requirements (grade E), • Critical Care 2006, 10:R120
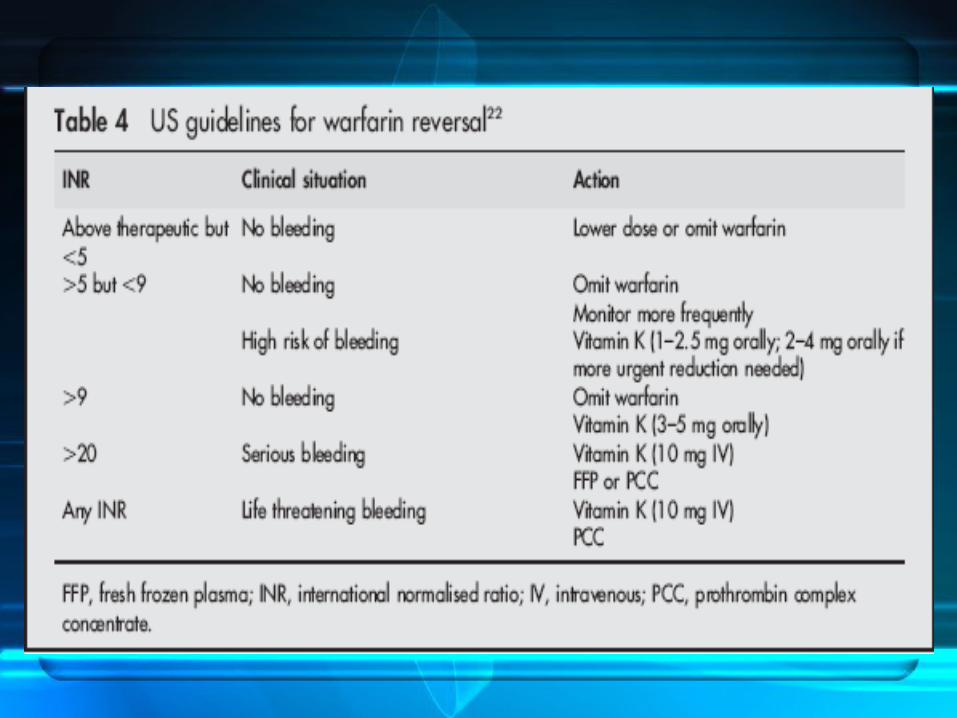
Warfarin Reversal• Dramatic increase in number of patients receiving
OAC• Interindividual variation (environmental and genetic) • Incidence of fatal haemorrhage :1%/Y. • Increased risk of ICH > 50 y compared with non-
anticoagulated 10x• Reversal :seriousness of bleeding , thrombotic risk
and speed and completeness of reversal• Options : dose omission ,vit K & factors replacement • FFP or PCCs


Warfarin Reversal PCCs
• Intermediate purity plasma products • Only HTDEFIX is licensed in UK for warfarin reversal• PCCs, (‘‘4 factor concentrates’’), OR low VII (3 ) • Amounts of protein C and S• Optimum dose not established.• Thrombogenicity, exacerbation of DIC are dose
related• Current cost in UK (single treatment for a 70 kg
individual £437 -£875). • More expensive > FFP. ( unit of produced from UK
plasma costs about £30). • FFP that is methylene blue treated or produced from
non-UK plasma is more expensive.)
Warfarin Reversal rFVIIa
• Advocated in the management of bleeding• Studied in a small number of studies • Normalises the INR in anticoagulated • Dose range, 15–90 mg/kg• Small numbers of patients with ICH successfully
treated with rFVIIa have been reported recently.54–56
• Lin J, J Neurosurg 2003;98:737–40.• Sorensen B, Blood Coagul Fibrinolysis 2003;14:469–77 • On the basis of this limited data, the role of rFVIIa in
warfarin reversal remains unclear.

Use in intracranial hemorrhage.
• A recent report in ICH in adults • Control the expansion of intracranial hematomas in
elderly patients, improving neurologic outcome and significantly decreasing mortality.
• Serious thromboembolic events were higher in the treated groups (7% vs. 2% for placebo).
• Bijsterveld NR, Circulation 2002;106:2550-4.
SAFETY PROFILE• Theoretical increased risk of thrombotic events• rFVIIa bind to active PLTs , hemostatic activity
should be restricted to vessel injury (TF is exposed & PLTs are locally activated)
• Experimental evidence for localized effect in rabbit model
• Dec 1995 -Jan 2005,total amount of rFVIIa released 680,245 standard doses :approved or “off-label” use,
• Over this postmarketing period, 123 thrombotic corresponding to a mean of 1/10000 thrombotic
• Review in patients with acquired and congenital hemophilia with inhibitors, incidence of thrombotic events was low

SAFETY PROFILE• Review of 13 controlled clinical trials, 1178 patients
with coagulopathy No significant association was found between exposure to rFVIIa and incidence of thrombotic events????.
• No inhibitors reported neither in HA nor off-label use.• Two patients with FVII-DEFICIENCY (no FVII protein)
developed transient inhibitors against FVII.• Thrombotic complication: elderly with existing
atherosclerotic disease. • FDA report :Arterial and venous thromboembolic
events .Half occurred in first 24 hours after last rFVIIa dose.
• Underlying medical conditions existed in some. • Lack sufficient information dosage ,concomitant
medications, pre-existing medical conditions and the confounding indication;
Advantages DisadvantagesAdvantages • Rapid onset of action• Low-volume dosing• Recombinant nature alleviating infectious disease
transmission • Low risk of thrombogenicity :increasing cases being
reported of thromboembolic manifestationsDisadvantages • Substantial cost $1000 per milligram• Risk of thrombosis• Variability of current recommended dose and dosing
intervals• Short half-life • Limited data pertaining to safety and efficacy,• Problems with monitoring its efficacy.

SUMMARY• Great potential in achieving hemostasis in patients
refractory to traditional treatments.• Significant cost and uncertain benefit in many clinical
situations, it should not be used indiscriminately. • Transfusion service , pharmacy OR content expert in
hemostasis are appropriate gatekeepers • The ordering physician must demonstrate to a
gatekeeper that the patient meets established criteria • For off-label use a maximum of two doses • Further doses given only after additional expert
consultation. • FDA-approved indication :Hemophilia patients with
inhibitors & Congenital FVII deficiency

Thanks

Hemostatic DefectsMost common are:- Low platelet counts- Low levels of vit K-depandent
coagulation factors (FVII, FX, FIX, FII, ProtC)
- lowered fibrinogen- lowered FVIII and FV - increased fibrinolysis
Use in qualitative PLT disorders.• Ability of pharmacologic doses to enhance rate of
thrombin generation on activated PLTs• Midlevel evidence and case reports exist.• Glanzmann’s thrombasthenia :reports with good
results.• A report of 33 episodes in 7children 60% excellent
response if treated within 12 hours of onset of bleeding.
• Surgical prophylaxis and excessive menstrual bleeding
• Doses of 90 to 120µ g per kg • Approved for use in Europe • Poon MC, international survey. J Thromb Haemost 2004;2:1096-
103.