cell inj 1
TRANSCRIPT

What is pathology ?
General Pathology
Systemic / Special Pathology

Any disease process will have:
1. Etiology 2. Pathogenesis3. Morphologic changes4. Signs & symptoms (clinical features)5. Diagnosis, prognosis, treatment & prevention
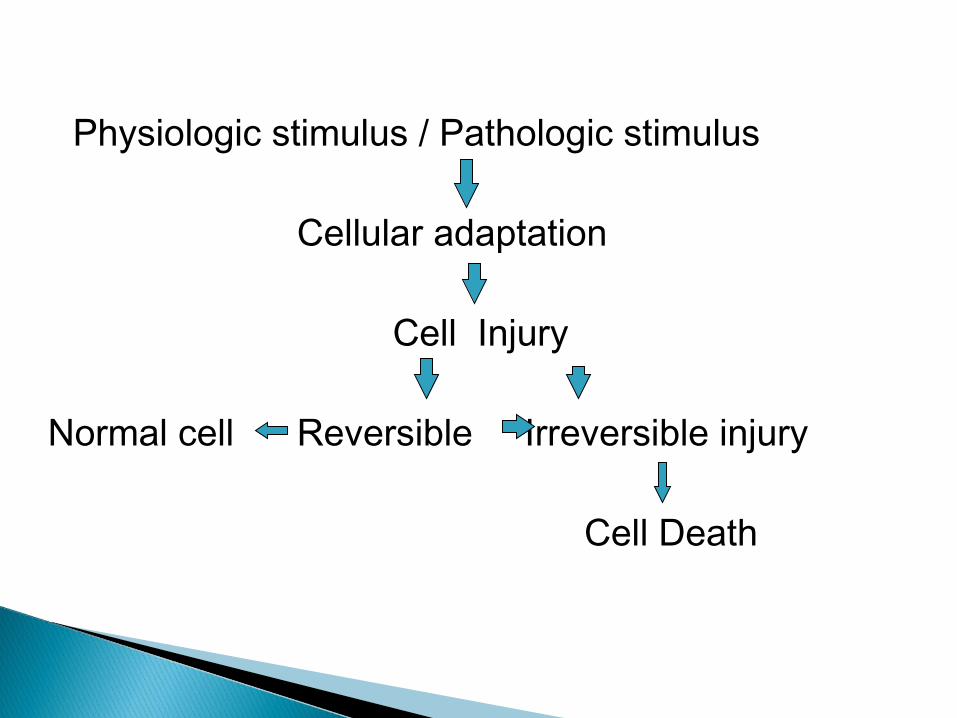
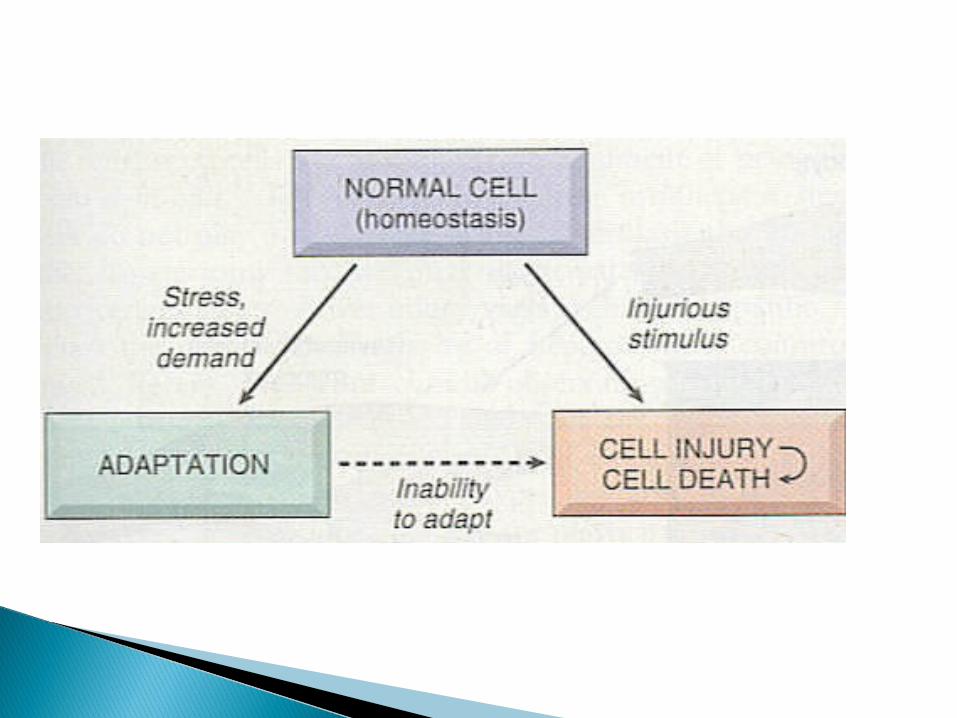
Physiologic stimulus / Pathologic stimulus
Cellular adaptation
Cell Injury
Normal cell Reversible Irreversible injury
Cell Death
Factors influencing cellular response to an
injurious stimulus:
1. Type of injurious agent
2. Duration of stimulus
3. Type of target cell
4. Status (nutritional & metabolic) of target cell
Response of a cell to injury can be in the form of:
1. Cellular adaptations2. Acute cell injury – reversible & irreversible3. Intra cellular accumulations (metabolic derangements)4. Pathologic calcification5. Aging
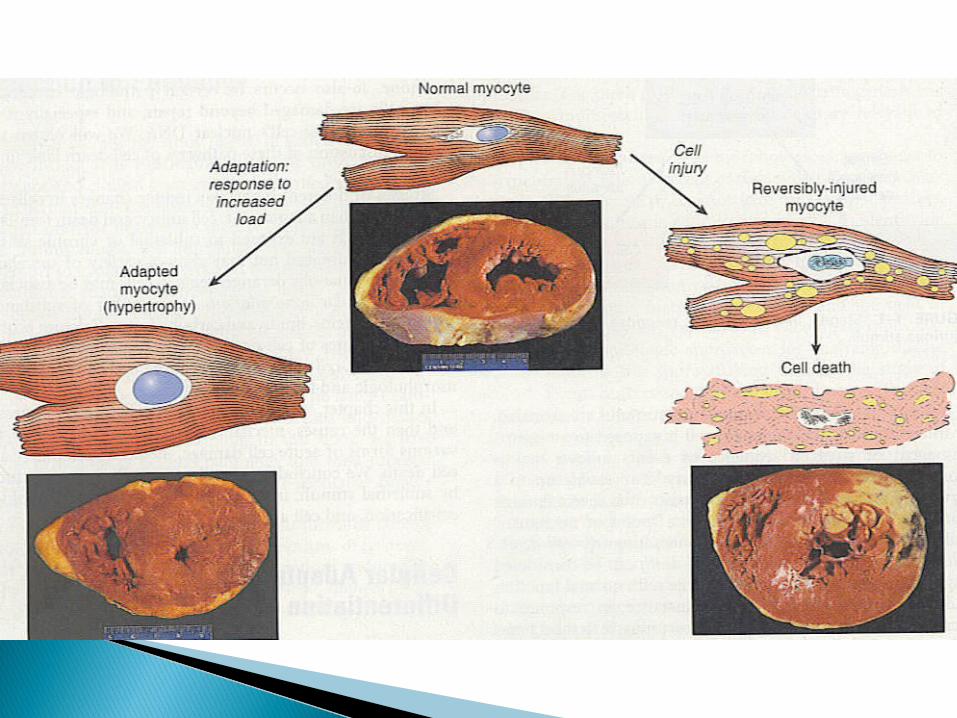
Atrophy Hypertrophy Hyperplasia Metaplasia
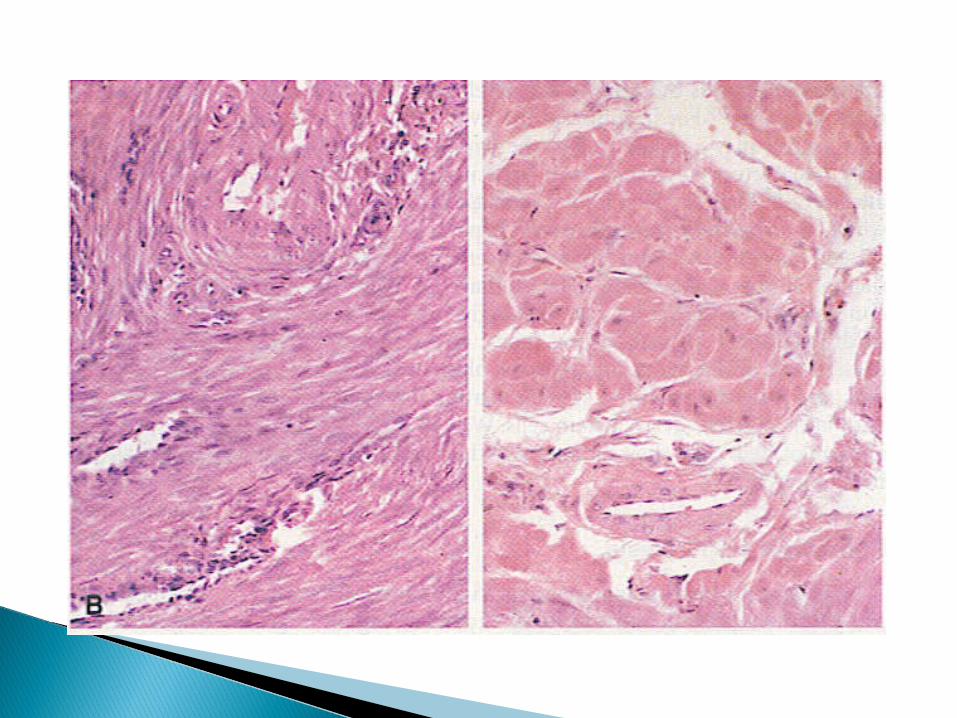
Defined as increase in cell size with concomitant increase in size of tissue or organs
Increased synthesis of structural proteins & organelles

Hypertrophy is usually associated with hyperplasia in stable cells
Pure hypertrophy occurs in heart & skeletal muscles (non-dividing permanent cells)
Physiologic hypertrophy occur in:
◦ Skeletal muscles (weight lifters) - Mechanical
◦ Uterine muscles (pregnancy) – Hormonal
◦ Mammary glands (pregnancy) – Hormonal
Pathologic hypertrophy occur in:
◦Heart (hypertension, post-MI) – Mechanical◦ Smooth muscle (achalasia in esophagus,
pyloric stenosis) – Mechanical◦ Kidney (following nephrectomy) –
Compensatory◦ Liver – Compensatory or drug-induced


Defined as an increase in number of cells with proportionate increase in size of tissue or organ
Occur in labile cells & stable cells
Usually associated with hypertrophy
Predisposition to cancer
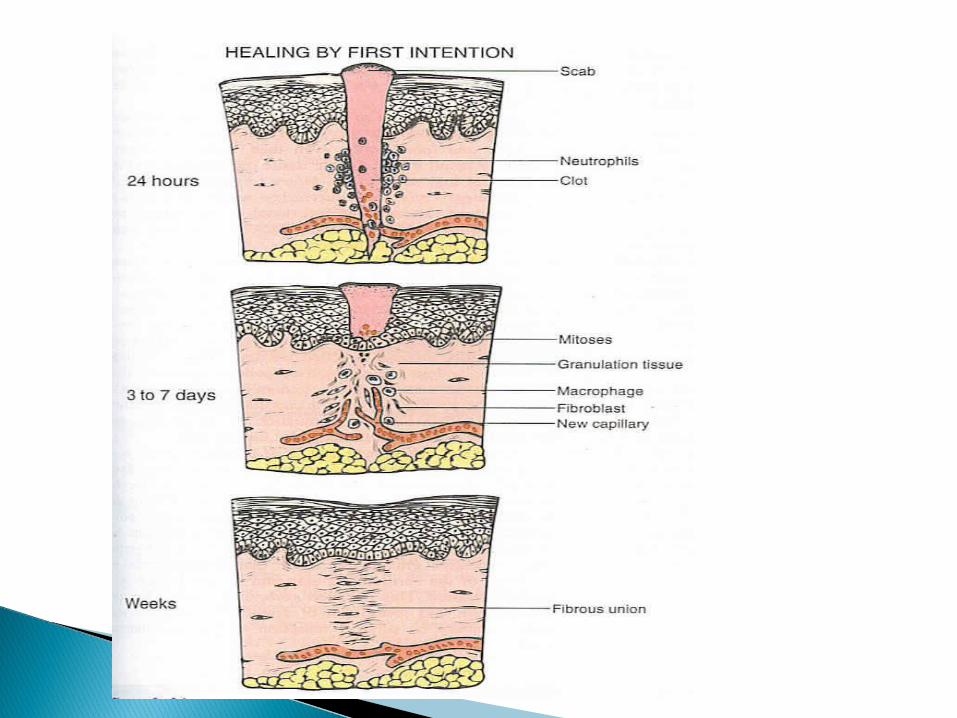
Physiologic hyperplasia:1. Hormonal e.g.i. Gravid uterusii. Female breast (pregnancy & puberty)2. Compensatory – Parenchymal e.g.i. Liver (influence of GF)3. Compensatory – Mesenchymal e.g.i. Fibroblasts & blood vessels (wound healing)

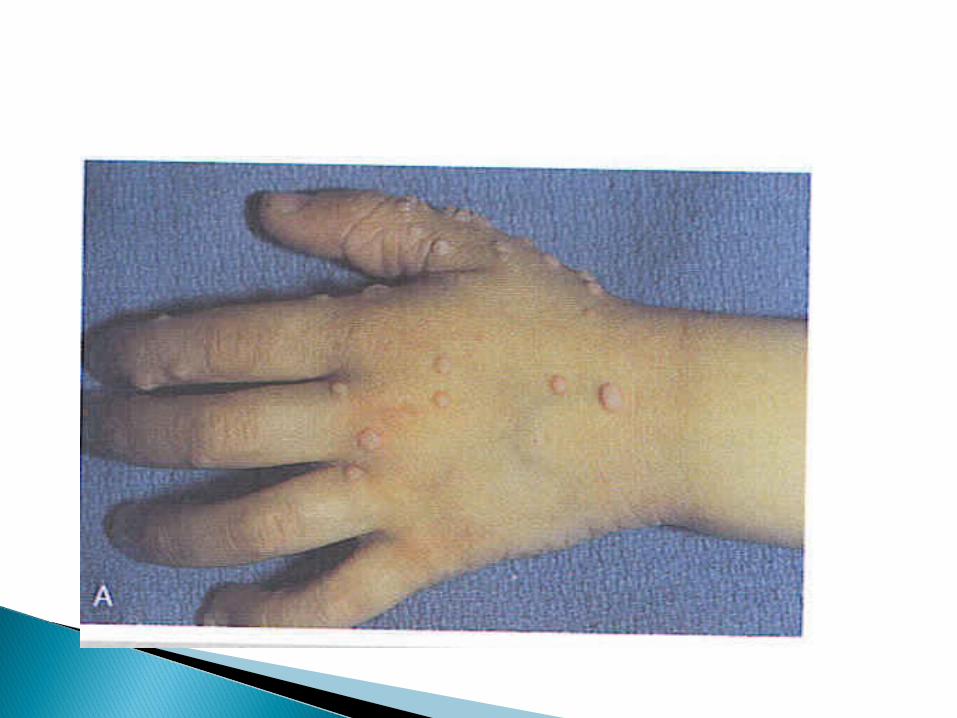
Pathologic Hyperplasia:
1. Endometrial hyperplasia (hormonal)2. Skin wart (HPV – GF)
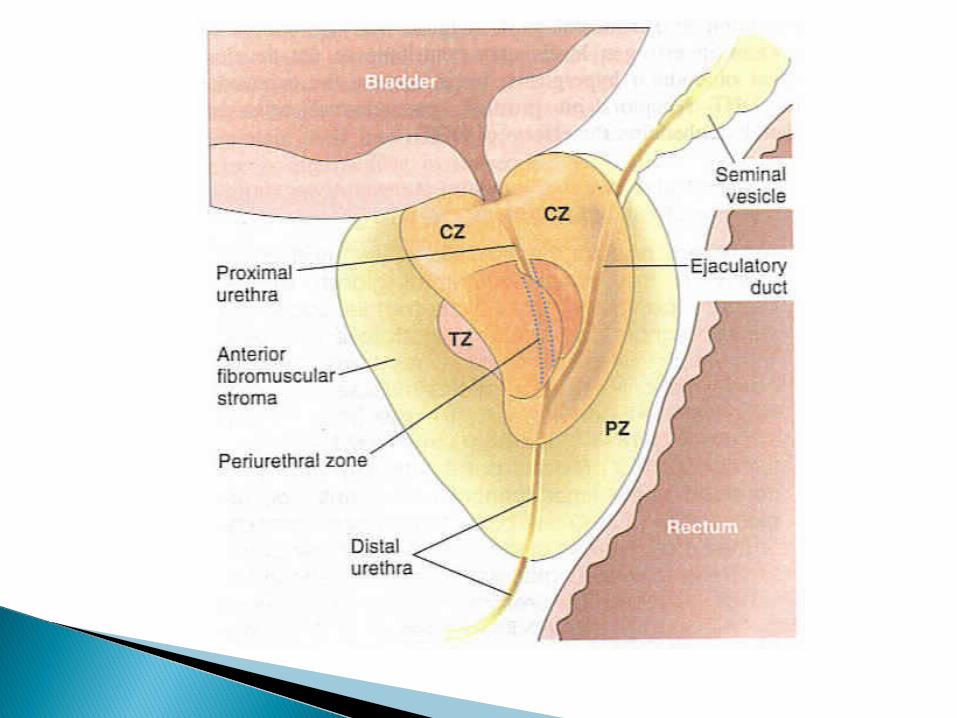
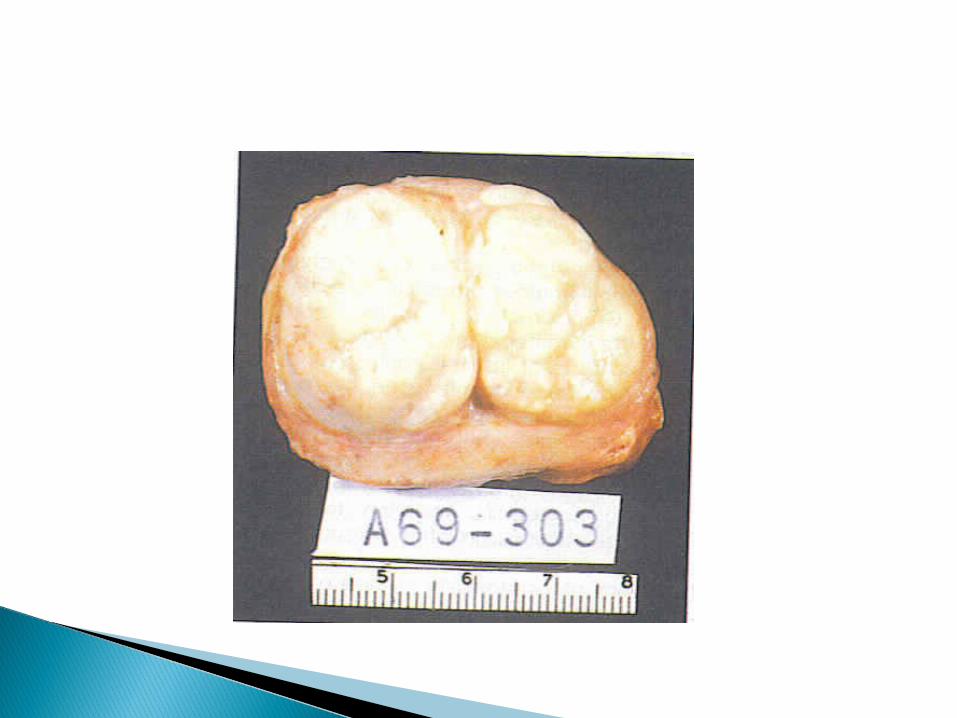
3. Prostate hyperplasia (hormonal)
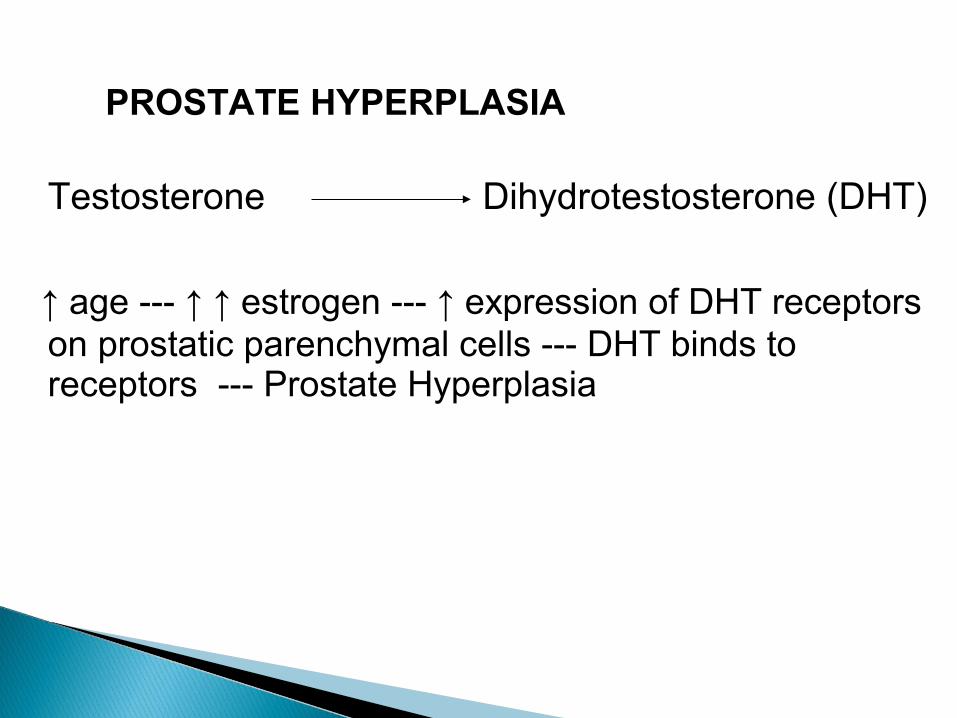
PROSTATE HYPERPLASIA
Testosterone Dihydrotestosterone (DHT)
↑ age --- ↑ ↑ estrogen --- ↑ expression of DHT receptors on prostatic parenchymal cells --- DHT binds to receptors --- Prostate Hyperplasia

Defined as replacement of one adult cell type (either epithelial or mesenchymal) by another adult cell type.
Reversible initially
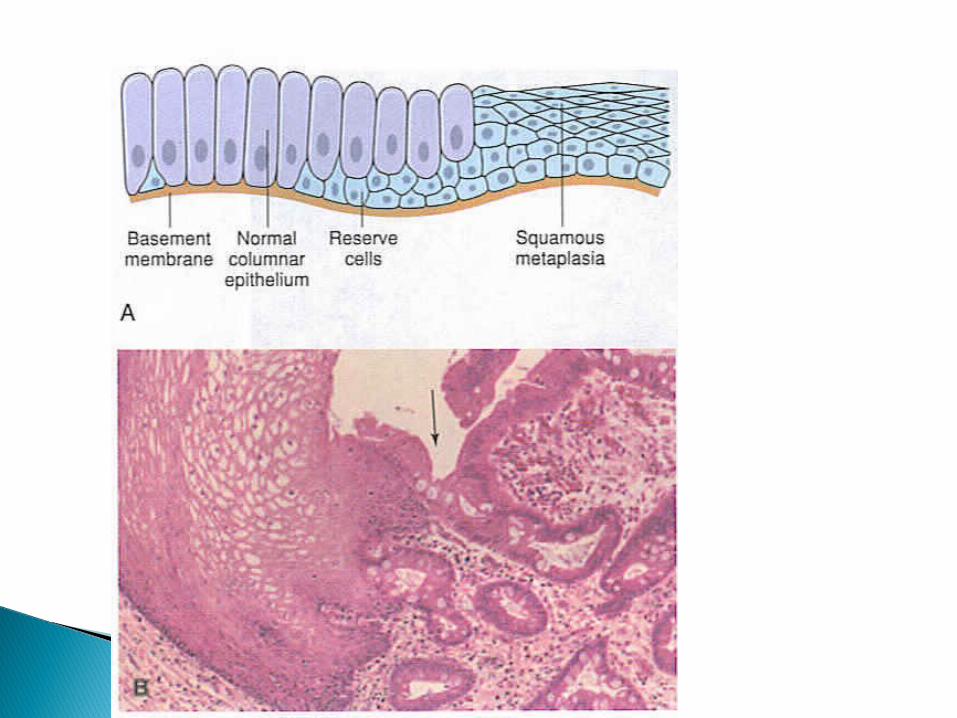
Epithelial metaplasia predispose to malignant transformation
Normal cell Metaplasia Cancer
Epithelial Metaplasia (columnar to squamous):
1. Cigarette smokers (trachea & bronchi)2. Vitamin A deficiency (respiratory epithelium)

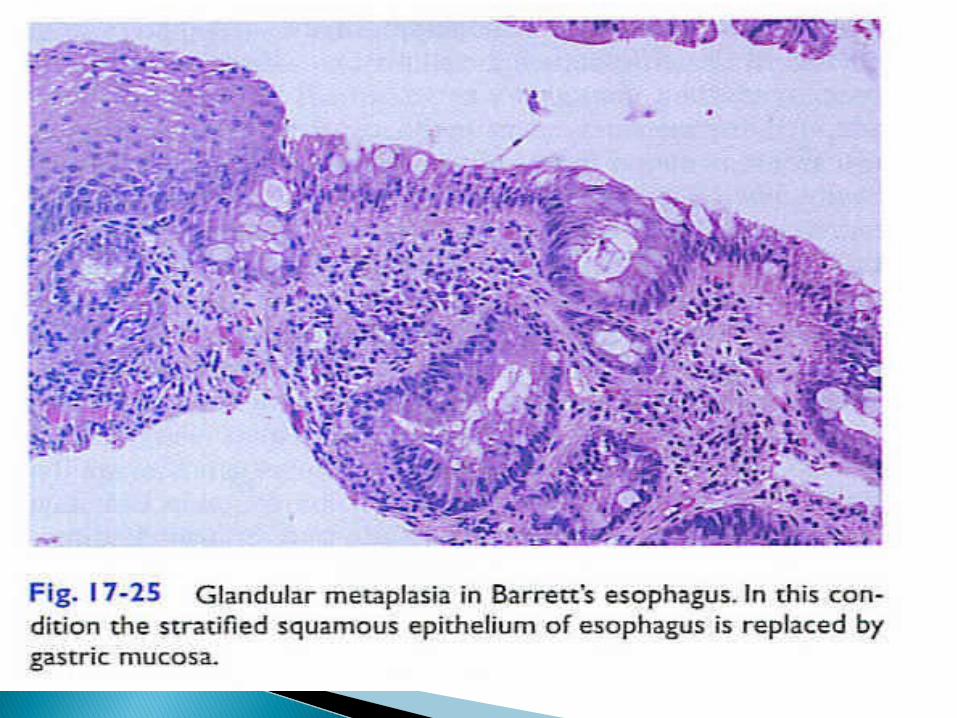
Epithelial Metaplasia (squamous to columnar):1. Barrett esophagus

Mesenchymal Metaplasia:
Osseous metaplasia in foci of injury

Decrease in size of cells, tissues or organs Both nucleus & cytoplasm reduced in size Causes include:
1. Disuse atrophy2. Denervation atrophy
3. Loss of hormonal stimulation4. Ischemia5. Malnutrition (PEM)6. Aging (senile atrophy) Mechanism – Decreased protein synthesis &
increased protein degradation

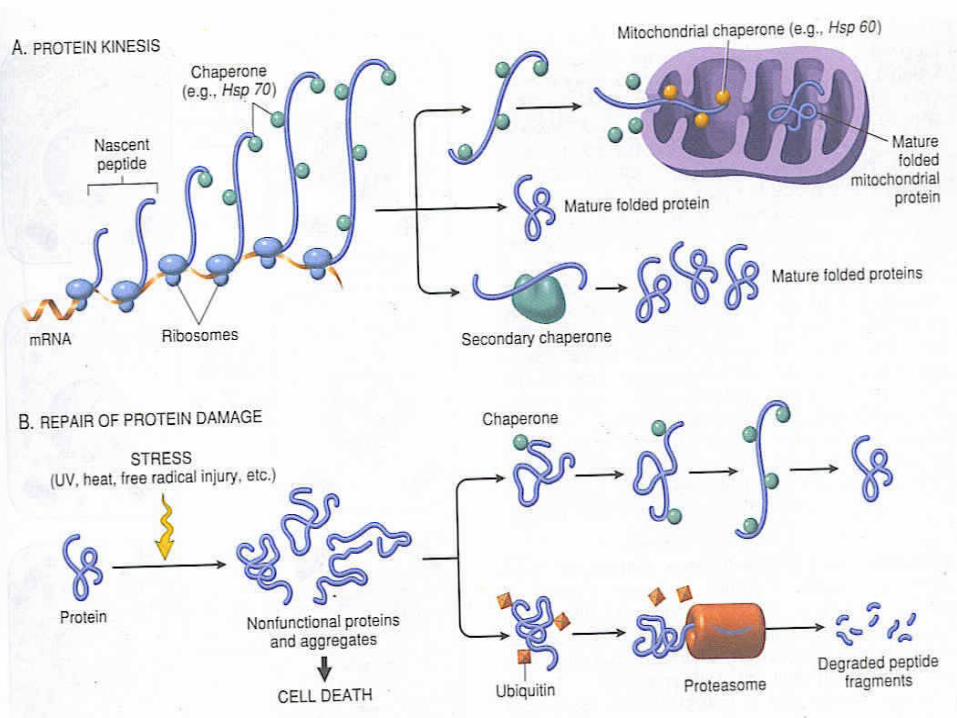
Protein degradation occurs through:
i. Ubiquitin - Proteasome pathway --- degrade cytosolic & nuclear proteins
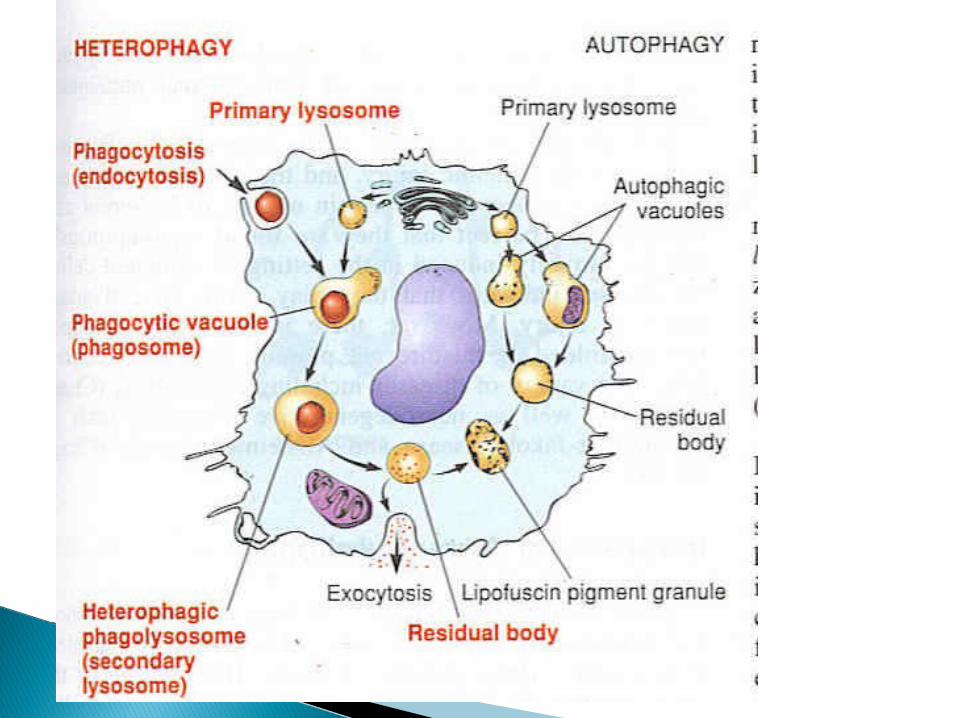
ii. Autophagy
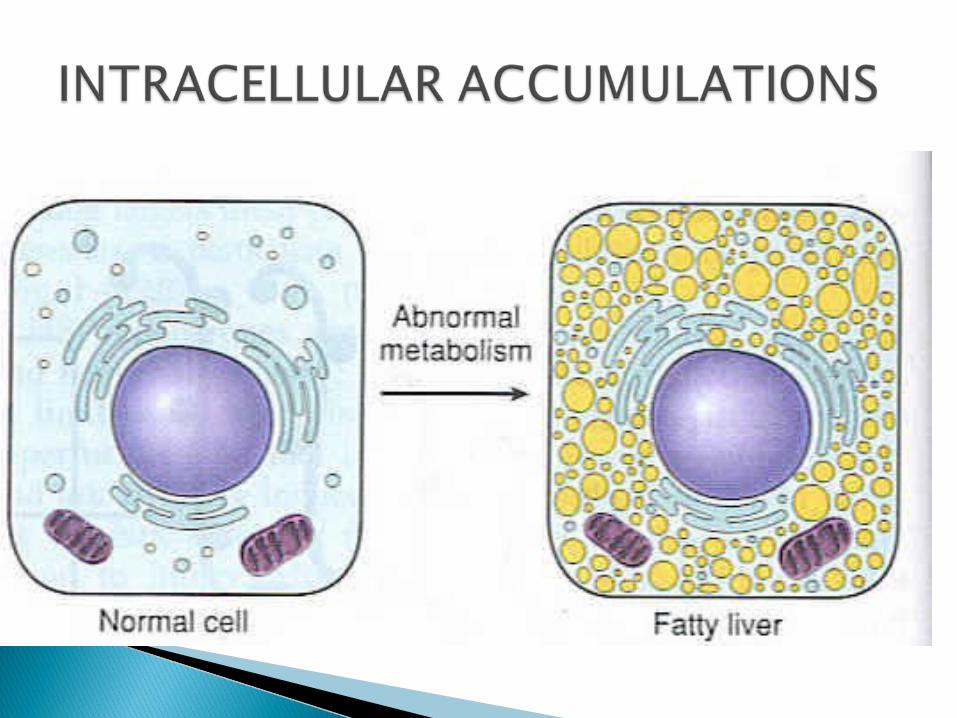


Abnormal accumulation of triglycerides in parenchymal cells
Seen in:1. Liver (mostly)2. Heart3. Skeletal muscles4. Kidney etc.
Reversible injury
Causes:
Toxins (CCl4, chloroform, aflatoxins, poisons) Protein malnutrition Diabetes mellitus Obesity Pregnancy Alcohol abuse Starvation Anemia (hypoxia) Reye syndrome
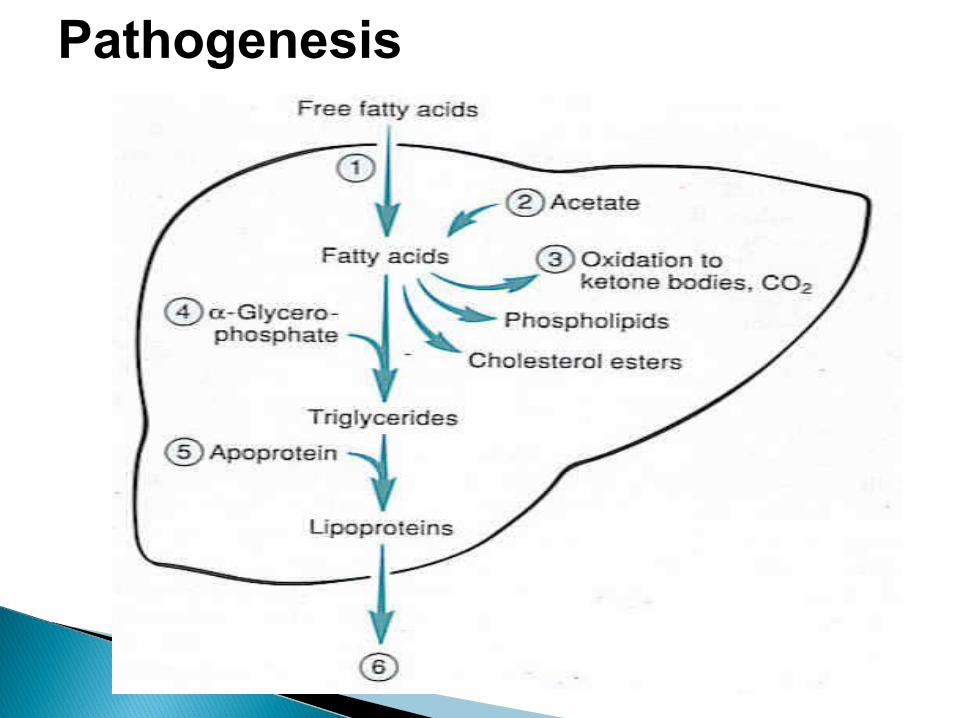
Pathogenesis
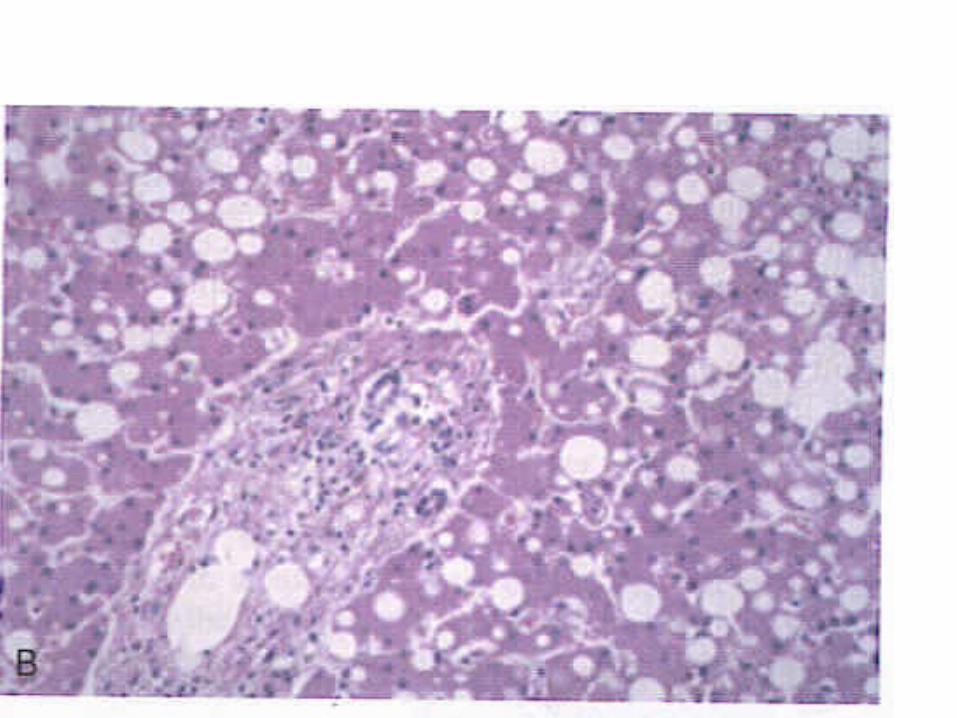
Morphology:
Liver:
◦Gross --Enlarged, yellow, soft & greasy
◦M/s --- Microvesicular change
Macrovesicular change Fatty cysts


Heart:◦Gross --- In anemia --- “tigered effect” In diphtheria --- uniform effect
◦M/s features --- same as above
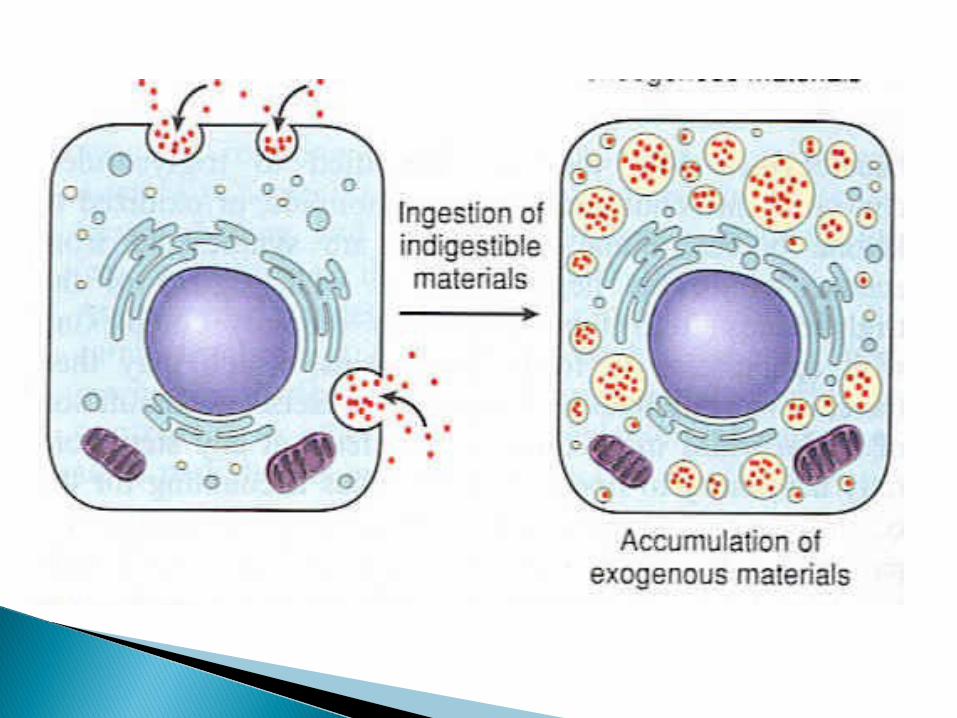
Phagocytic cells engulf cholesterol --- foam cells e.g.
1. Atherosclerosis 2. Xanthomas (Hyperlipidemic syndrome)

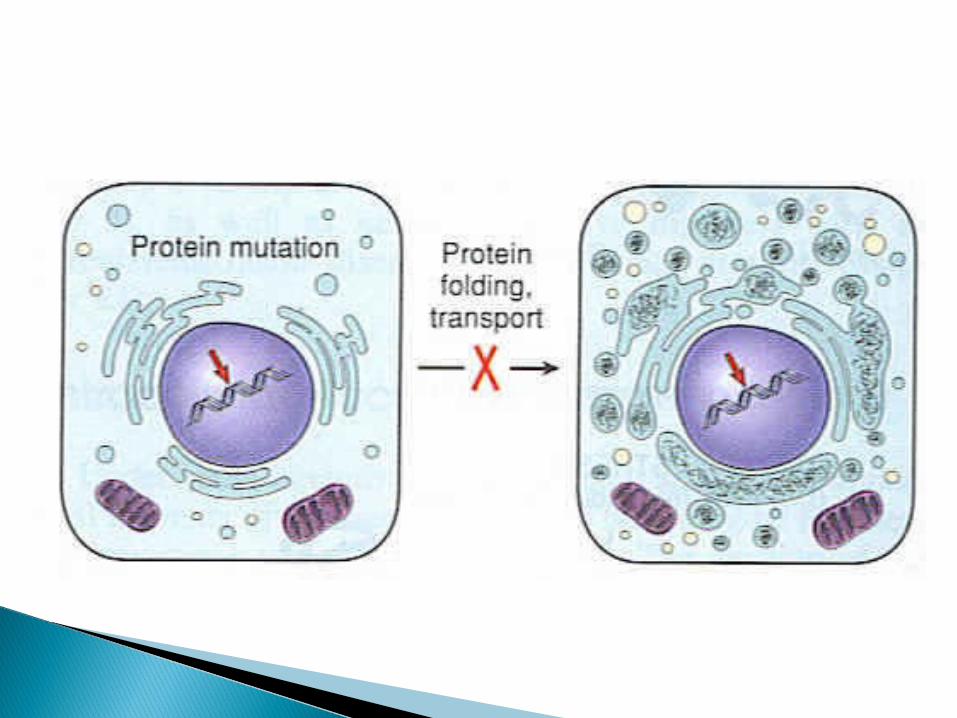
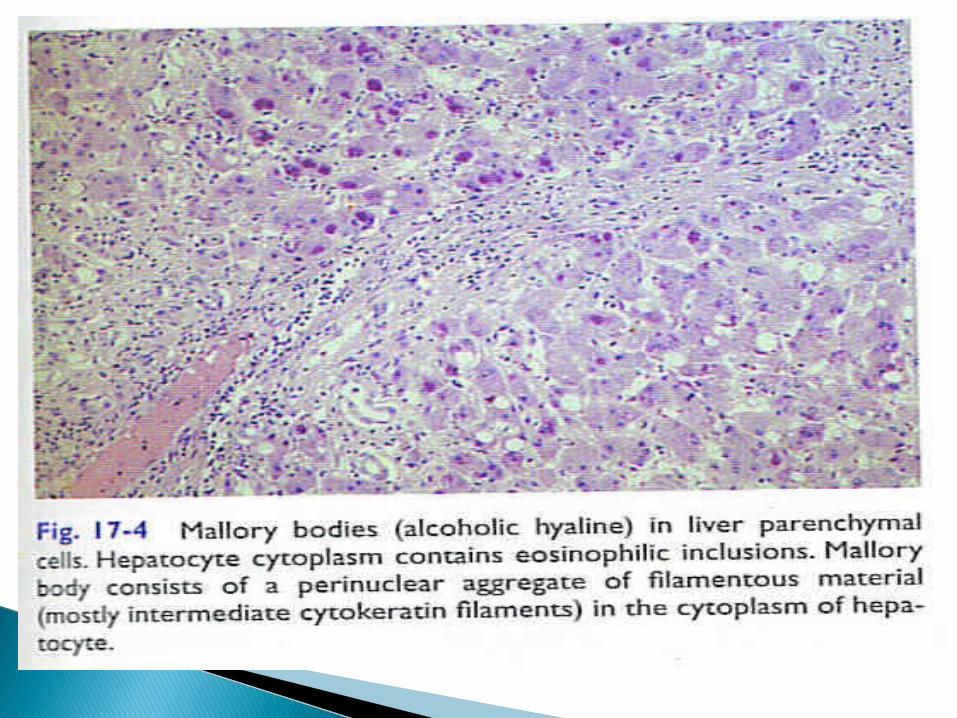
Causes of protein deposition include:
1. Nephrotic syndrome2. Russell bodies 3. Mallory bodies (alcohol )4. Neurofibrillary tangles in Alzheimer disease
Causes of glycogen deposition include:1. Diabetes mellitus2. Glycogen storage diseases hepatic type --- Von Gierke’s disease
(deficiency of glucose-6-phosphatase) myopathic type --- McArdle’s disease
(deficiency of muscle phosphorylase) Pompe disease --- deficiency of lysosomal
acid maltase