center for the study of tobacco arkansas statewide tobacco ... · pdf filearkansas statewide...
TRANSCRIPT
Center for the Study of Tobacco
Arkansas Statewide Tobacco Programs and Services (AR Stops)
2005-2006 Fiscal Year Annual Report for the Arkansas Division of Health Tobacco Prevention and Education Program July 1, 2005 to June 30, 2006
• Smoke-free Workplace Assistance Program • Provider Education Program • Computerized Treatment Delivery Program • SOSWorks Fax-back Referral Program • Arkansas SOSQuitline • Arkansas Tobacco Cessation Network
Special Addendum Emerging Threats: Smokeless Tobacco, Bidis, Kreteks, Herbal Cigarettes, Betel Quid, and the Ariva Cigalette
Principal Investigator: Christine Sheffer, PhD
2
Center for the Study of Tobacco Arkansas Statewide Tobacco Programs and
Services (AR-Stops) Arkansas Division of Health Tobacco Prevention and Education 2005-2006 Fiscal Year Annual Report July 1, 2005 to June 30, 2006 Christine Sheffer, PhD, Principal Investigator 1. Smoke-free Workplace Assistance Program (SWAP)
Project Leader: Julie Harlan, CHES Project Consultant: John Wayne, DrPH
2. Provider Education Program (PEP)
Project Leader: Claudia Barone, RN, EdD 3. Computerized Treatment Delivery Program (YouCanQuit AR.net)
Project Leader: Alan Vanbiervliet, PhD 4. SOSWorks Fax-back Referral Program
Project Leader: Deidre Seker, MS 5. Arkansas SOSQuitline (QL) 6. Arkansas Tobacco Cessation Network (ATCN)
Project Coordinator: Jada Walker, MEd
3
List of Faculty and Staff Supported by AR Stops
Claudia Barone, EdD, RN Provider Education Coordinator & Dean, UAMS College of Nursing
Deborah Bledsoe ACADC, LADAC Interventionist Ted Brasfield Fiscal Administration Fran Butler, MS Interventionist Susan Caplener Interventionist Catherine Critz, BSW Interventionist Sherry Endres, BS Interventionist Eric Flowers, BS Interventionist Marilyn Fulton Administrative Assistant Nestor Garcia, MD, MPH Interventionist Mark Gilbert, MBS Interventionist Donny Graham Intake Interviewer Paul Greene, PhD Co-Director, Arkansas Tobacco Cessation Network Sharon Greene, MEd Interventionist Julie Harlan, CHES Smoke-free Workplace Assistance Coordinator Beverly Johnson Administrative Assistant William Lassiter, MS Interventionist Sharonda Love Administrative Assistant M. Camille Mack, MRC Interventionist Deborah Marple, RN Coordinator Alexandra Marshal Intake Interviewer Kenneth Mayes, CHES Interventionist Sherri Morris Follow-up Interviewer Charles Mullins, PhD Interventionist Mary Noble, BA,NCAC Interventionist Madilyn Nolen, MS Interventionist Sydney Rephan, BS Interventionist C. Annette Sanders Interventionist Deidre Seker, MS SOSWorks Coordinator Christine Sheffer, PhD Principal Investigator Jennifer Smart, BA Project Specialist YouCanQuit AR.net Shana Southard, MS Interventionist Blake Talbot, BS Intake Interviewer Charlie Stayton, AAS Intake Interviewer Alan VanBiervliet, PhD Project Leader YouCanQuitAR.net Shirley Vanderslice, CPC Intake Interviewer Merrie Vannucci, MA,ACADC Interventionist Daisy Wade, BS Interventionist Jada Walker, MEd Arkansas Tobacco Cessation Network Coordinator Tina Wall, MS Interventionist John Wayne, DrPH Smoke-free Workplace Consultant Rod West Fiscal Administration Amy Williams, BSW Interventionist Elaine Wooten, MS Coordinator
4
Executive Summary Consistent with the first six months of fiscal year 2005-2006, AR Stops continued to experience tremendous growth throughout the second half of the year. Most programs, such as the Arkansas SOSQuitline, SOSWorks, the Provider Education Program (PEP), and the Smoke-free Workplace Assistance Program (SWAP) greatly exceeded program goals as they rallied to meet an unexpected and immediate demand for services. The Arkansas SOSQuitline and SOSWorks, in particular, handled more callers and referrals than ever before. This resulted in more Arkansans receiving evidence-based treatment for tobacco dependence this year than ever before. The Arkansas Tobacco Cessation Network (ATCN) built a solid foundation of resources, personnel, and relationships in the community. YouCanQuit AR met its development goal this year and is ready for testing during the 2006-2007 fiscal year. As these programs continue to mature, we expect the demand for services to continue to increase as well, which, of course, bodes well for reducing the overall tobacco use prevalence rate in Arkansas and increasing the health and well-being of all Arkansans. As these programs grow, it is worth repeating that we are building what can be described as the most comprehensive and well-integrated tobacco treatment and assistance network in the country. Built on evidence-based methods and experience in the field, these programs have benefited from the ingenuity of numerous individuals at the College of Public Health and the Arkansas Division of Health as well as input and support from many dedicated legislators, especially those who serve on the Public Health and PEER Review committees. My sincere appreciation is extended to all who have contributed. We have accomplished a great deal this year and we look forward another record year next year! Sincerely, Christine Sheffer, PhD, Assistant Professor Department of Health Behavior and Health Education Fay W. Boozman College of Public Health University of Arkansas for Medical Sciences
5
Smoke-free Workplace Assistance Program (SWAP) Smoke-free workplace policies result in a 3.8% reduction in employee smoking prevalence.1 Federal figures indicate that employees who smoke cost $1,500 more per year in healthcare costs and $1,760 more per year in lost productivity. As part of the new Quitline contract with the Arkansas Division of Health, the COPH developed a program to assist Arkansas workplaces in implementing smoke-free policies. This program provided on-site evaluation and assistance to workplaces across the state. This component was a new addition to the Quitline contract and was not a part of Quitline activities prior to July 1, 2005. Funding for SWAP was allocated in August 2005. SWAP was expected to assist 15-20 worksites in fiscal year 2005-2006. From October 1 to June 30, 2006, SWAP assisted 36 worksites and affected the work environment of over 7440 employees in addition to numerous vendors, visitors, volunteers, customers, patients, and students. SWAP exceeded expectations by 16 workplaces or 80%. See Table below for details. SWAP is estimated to have motivated 283 employees to quit smoking this fiscal year resulting in continued yearly savings of $424,500 in healthcare costs and $498,080 in lost productivity for Arkansas employers. This program is estimated to have saved Arkansans $922,580 this year and every year that workplaces remain smoke-free. This is, of course, in addition to reducing numerous healthcare costs and hazards from reduced exposure to secondhand smoke in the workplace. 1. Fichtenberg CM. Glantz SA. Effect of smoke-free workplaces on smoking behaviour: systematic review. BMJ. 2002:325(7357):188.
6
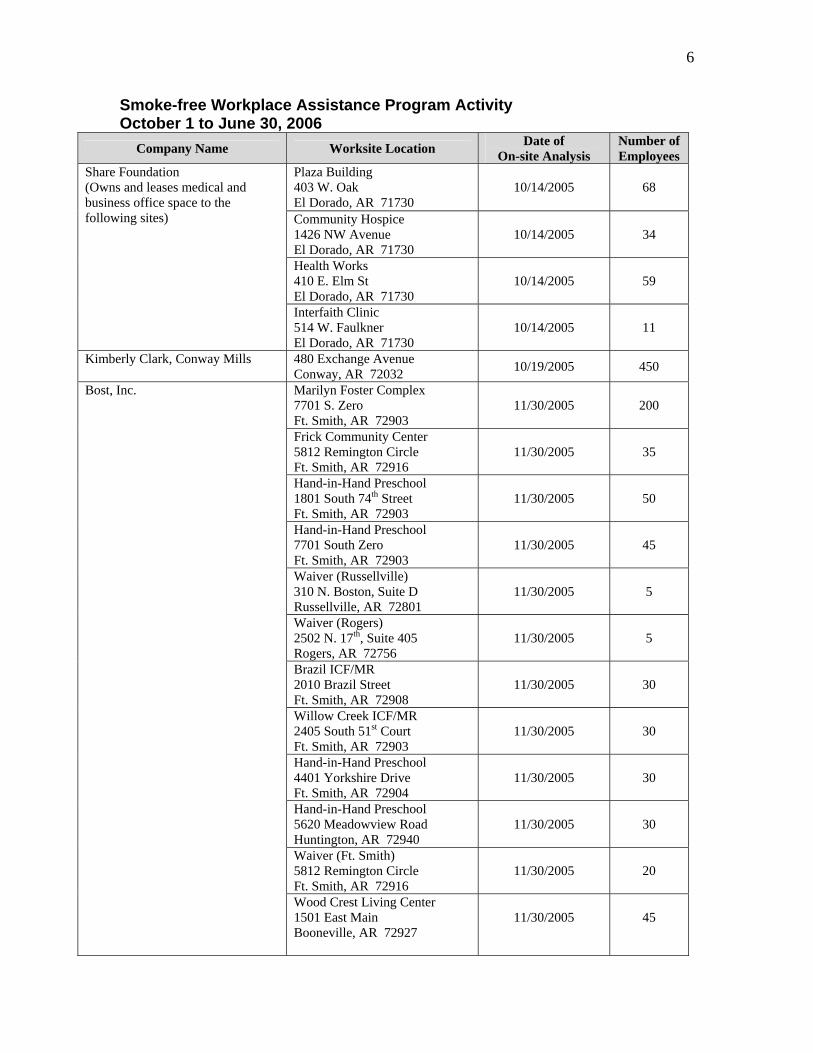
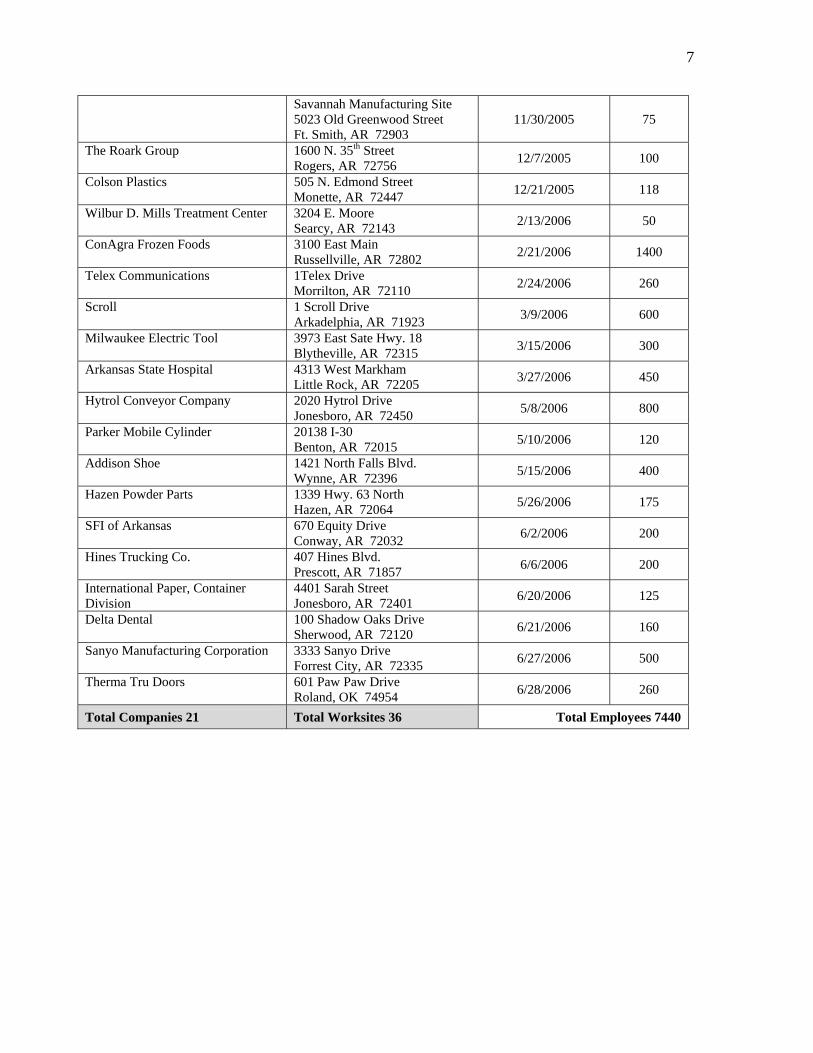
Smoke-free Workplace Assistance Program Activity October 1 to June 30, 2006
Company Name Worksite Location Date of On-site Analysis
Number of Employees
Plaza Building 403 W. Oak El Dorado, AR 71730
10/14/2005
68
Community Hospice 1426 NW Avenue El Dorado, AR 71730
10/14/2005
34
Health Works 410 E. Elm St El Dorado, AR 71730
10/14/2005
59
Share Foundation (Owns and leases medical and business office space to the following sites)
Interfaith Clinic 514 W. Faulkner El Dorado, AR 71730
10/14/2005
11
Kimberly Clark, Conway Mills 480 Exchange Avenue Conway, AR 72032 10/19/2005 450
Marilyn Foster Complex 7701 S. Zero Ft. Smith, AR 72903
11/30/2005
200
Frick Community Center 5812 Remington Circle Ft. Smith, AR 72916
11/30/2005
35
Hand-in-Hand Preschool 1801 South 74th Street Ft. Smith, AR 72903
11/30/2005
50
Hand-in-Hand Preschool 7701 South Zero Ft. Smith, AR 72903
11/30/2005
45
Waiver (Russellville) 310 N. Boston, Suite D Russellville, AR 72801
11/30/2005
5
Waiver (Rogers) 2502 N. 17th, Suite 405 Rogers, AR 72756
11/30/2005
5
Brazil ICF/MR 2010 Brazil Street Ft. Smith, AR 72908
11/30/2005
30
Willow Creek ICF/MR 2405 South 51st Court Ft. Smith, AR 72903
11/30/2005
30
Hand-in-Hand Preschool 4401 Yorkshire Drive Ft. Smith, AR 72904
11/30/2005
30
Hand-in-Hand Preschool 5620 Meadowview Road Huntington, AR 72940
11/30/2005
30
Waiver (Ft. Smith) 5812 Remington Circle Ft. Smith, AR 72916
11/30/2005
20
Bost, Inc.
Wood Crest Living Center 1501 East Main Booneville, AR 72927
11/30/2005
45
7
Savannah Manufacturing Site 5023 Old Greenwood Street Ft. Smith, AR 72903
11/30/2005
75
The Roark Group 1600 N. 35th Street Rogers, AR 72756 12/7/2005 100
Colson Plastics 505 N. Edmond Street Monette, AR 72447 12/21/2005 118
Wilbur D. Mills Treatment Center 3204 E. Moore Searcy, AR 72143 2/13/2006 50
ConAgra Frozen Foods 3100 East Main Russellville, AR 72802 2/21/2006 1400
Telex Communications 1Telex Drive Morrilton, AR 72110 2/24/2006 260
Scroll 1 Scroll Drive Arkadelphia, AR 71923 3/9/2006 600
Milwaukee Electric Tool 3973 East Sate Hwy. 18 Blytheville, AR 72315 3/15/2006 300
Arkansas State Hospital 4313 West Markham Little Rock, AR 72205 3/27/2006 450
Hytrol Conveyor Company 2020 Hytrol Drive Jonesboro, AR 72450 5/8/2006 800
Parker Mobile Cylinder 20138 I-30 Benton, AR 72015 5/10/2006 120
Addison Shoe 1421 North Falls Blvd. Wynne, AR 72396 5/15/2006 400
Hazen Powder Parts 1339 Hwy. 63 North Hazen, AR 72064 5/26/2006 175
SFI of Arkansas 670 Equity Drive Conway, AR 72032 6/2/2006 200
Hines Trucking Co. 407 Hines Blvd. Prescott, AR 71857 6/6/2006 200
International Paper, Container Division
4401 Sarah Street Jonesboro, AR 72401 6/20/2006 125
Delta Dental 100 Shadow Oaks Drive Sherwood, AR 72120 6/21/2006 160
Sanyo Manufacturing Corporation 3333 Sanyo Drive Forrest City, AR 72335 6/27/2006 500
Therma Tru Doors 601 Paw Paw Drive Roland, OK 74954 6/28/2006 260
Total Companies 21 Total Worksites 36 Total Employees 7440
8
Provider Education Program (PEP) Provider training in evidence-based, brief interventions has been shown to increase provider knowledge, awareness, and confidence in treating tobacco use and dependence as well as increase the frequency with which providers assist tobacco users with cessation.1
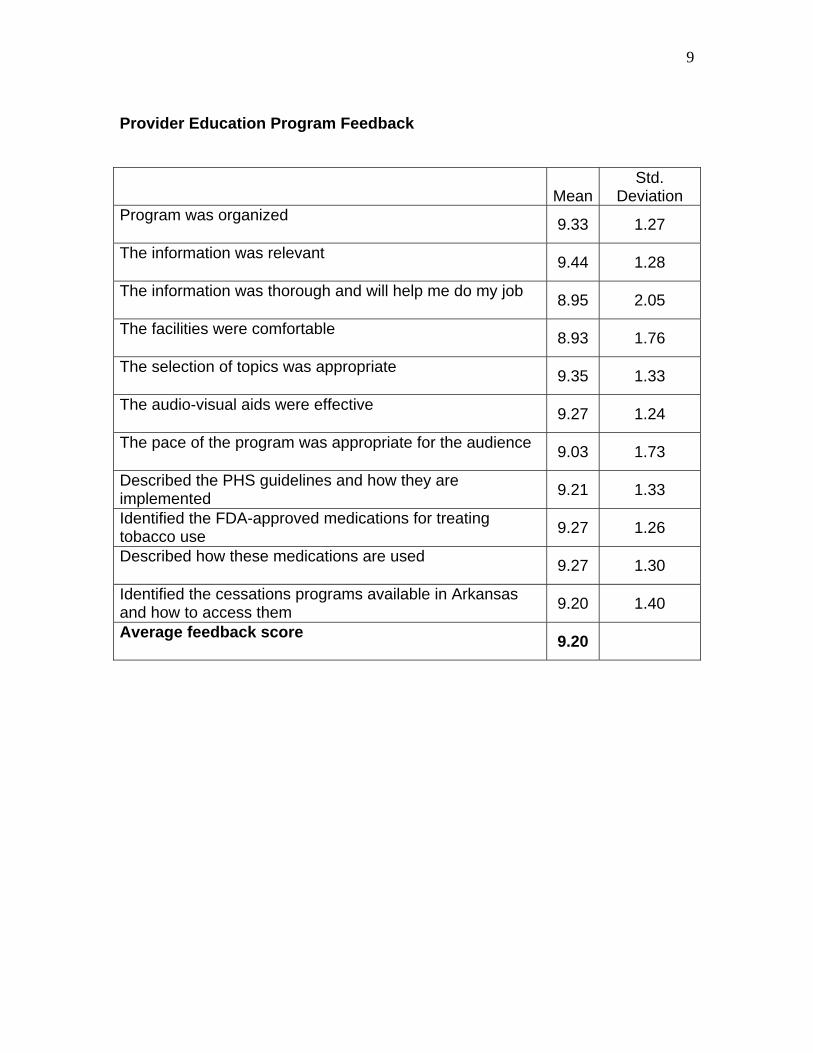
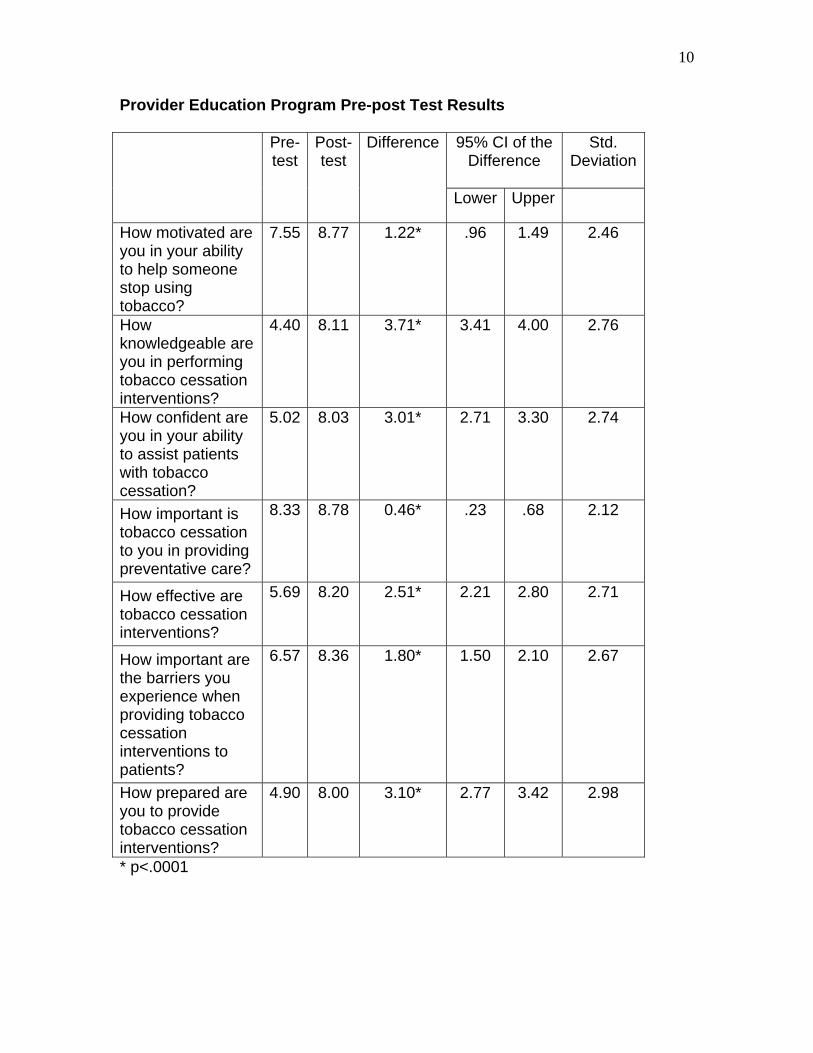
As part of the new Quitline contract with the Arkansas Division of Health, the COPH developed a CME- and CE- approved healthcare provider training program. This program provides on-site training to healthcare providers across the state in the evidence-based treatment of tobacco use and dependence using the Public Health Service Clinical Practice Guidelines, adapted motivational interviewing techniques, and practical instruction in how to utilize state-sponsored tobacco cessation services. This component was not a part of Quitline activities prior to July 1, 2005. Funding for the Provider Education Program (PEP) was allocated in August 2005. The initial program was tested by Dr. Sheffer and Dr. David Bourne in September 2005. The PEP coordinator position was filled in December 2005 by Dr. Claudia Barone. In fiscal year 2005-2006, PEP was expected to train 500 healthcare providers. PEP succeeded in training 606 Arkansas healthcare providers in 2005-2006 exceeding expectations by 106 providers or 21.2%. Evaluation results from the initial training with Dr. Bourne for 44 providers (34% physicians) were positive. On a scale of 1-5, with 1 being “poor” and 5 being “the best,” the average score for the training was 4.46, indicating strong acceptability. The program was further developed with feedback from the first training and pre- and post-testing for participants. Of the 606 providers trained, approximately 20% of those reporting held prescribing privileges (60 MD/DO, 1 DDS and 16 APN). Another 22% were registered nurses and 6% were registered dental hygienists. The pre- and post-tests questions were assessed on a 0-10 scale with 0 being “none or not at all” and 10 being “the most possible.” The overall program feedback averaged 9.20. Paired samples t-tests indicated that the training significantly increased provider motivation, knowledge, and confidence as well as perceived importance of treating tobacco use, perceived effectiveness of interventions for tobacco use, recognition of the importance of barriers, and perceived preparedness. See tables below for results. 1. Fiore MC, Bailey WC, Cohen SJ, Dorfman SF, Goldstein MG, Gritz ER, et al. Smoking cessation: Clinical practice guideline no. 18. Rockville, MD: US Dept of Health and Human Services, Public Health Service 2000.
9
Provider Education Program Feedback
Mean Std.
Deviation Program was organized 9.33 1.27
The information was relevant 9.44 1.28
The information was thorough and will help me do my job 8.95 2.05
The facilities were comfortable 8.93 1.76
The selection of topics was appropriate 9.35 1.33
The audio-visual aids were effective 9.27 1.24
The pace of the program was appropriate for the audience 9.03 1.73
Described the PHS guidelines and how they are implemented 9.21 1.33
Identified the FDA-approved medications for treating tobacco use 9.27 1.26
Described how these medications are used 9.27 1.30
Identified the cessations programs available in Arkansas and how to access them 9.20 1.40
Average feedback score 9.20
10
Provider Education Program Pre-post Test Results
95% CI of the Difference
Std. Deviation
Pre-test
Post-test
Difference
Lower Upper
How motivated are you in your ability to help someone stop using tobacco?
7.55 8.77 1.22* .96 1.49 2.46
How knowledgeable are you in performing tobacco cessation interventions?
4.40 8.11 3.71* 3.41 4.00 2.76
How confident are you in your ability to assist patients with tobacco cessation?
5.02 8.03 3.01* 2.71 3.30 2.74
How important is tobacco cessation to you in providing preventative care?
8.33 8.78 0.46* .23 .68 2.12
How effective are tobacco cessation interventions?
5.69 8.20 2.51* 2.21 2.80 2.71
How important are the barriers you experience when providing tobacco cessation interventions to patients?
6.57 8.36 1.80* 1.50 2.10 2.67
How prepared are you to provide tobacco cessation interventions?
4.90 8.00 3.10* 2.77 3.42 2.98
* p<.0001

11
Computerized Treatment Delivery (YouCanQuit AR.net ) As part of the Quitline contract, COPH initiated development of a digital program to compliment and expand treatment options for Arkansans. This component was not a part of previous Quitline activities. The program, entitled YouCanQuit AR.net, focuses on a positive approach to what you can do to quit smoking and maintain success. The program provides the key, evidence-based components of treatment in an alternate format designed to meet the access needs of a wide range of Arkansans. When released, the program will be available on CD-ROM, downloadable from the Web, and though a Web-based interface. The first version will be available on CD-ROM in the 2006-2007 fiscal year. Conversion to alternative tailored formats will begin following field testing and final revisions. There are several important differences between YouCanQuit and other digital programs. First, the intake, progress and follow-up data from YouCanQuit is fully integrated into the ARSTOPS follow-up and data collection system for evaluation purposes. Second, the YouCanQuit strategies compliment the evidence-based treatment options currently used in Arkansas. Finally, the images and video clips used in the program reflect the environment and people of Arkansas. This similarity and familiarity is likely to enhance the effectiveness of the program. When development is complete, YouCanQuit will consist of several related programs targeting different segments of the population. Although the basic quitting strategies are similar, the overall appearance and video examples will be tailored to particular groups to facilitate engagement. Middle aged males were selected as the first target group because data indicates that this group is underserved by the current cessation programs in Arkansas. Additionally, national data indicate that this group will utilize digital treatment programs. The software architecture of the current version will serve as a cost effective template for developing additional versions tailored for specific populations. Although complete development and testing is expected to require two full years, the initial version targeting middle age persons is scheduled for distribution in the 2006-2007 fiscal year. Throughout the development process the program has undergone iterative usability testing. YouCanQuit provides a tailored, guided path to developing and implementing an individualized plan for quitting tobacco. The program is organized into a 5 step process: 1. Identify your triggers; 2. Select strategies to manage your triggers; 3. Rate fading; 4. Set your Quit Date; and 5. Maintain your success. The steps are hierarchical with each step building on the therapeutic understanding and skill building developed in the previous step. The program guides the user through the steps using an onscreen counselor. Following is a brief description of program features. NOTE- Each component or Step in the program consists of several interactive tasks and educational units.
12
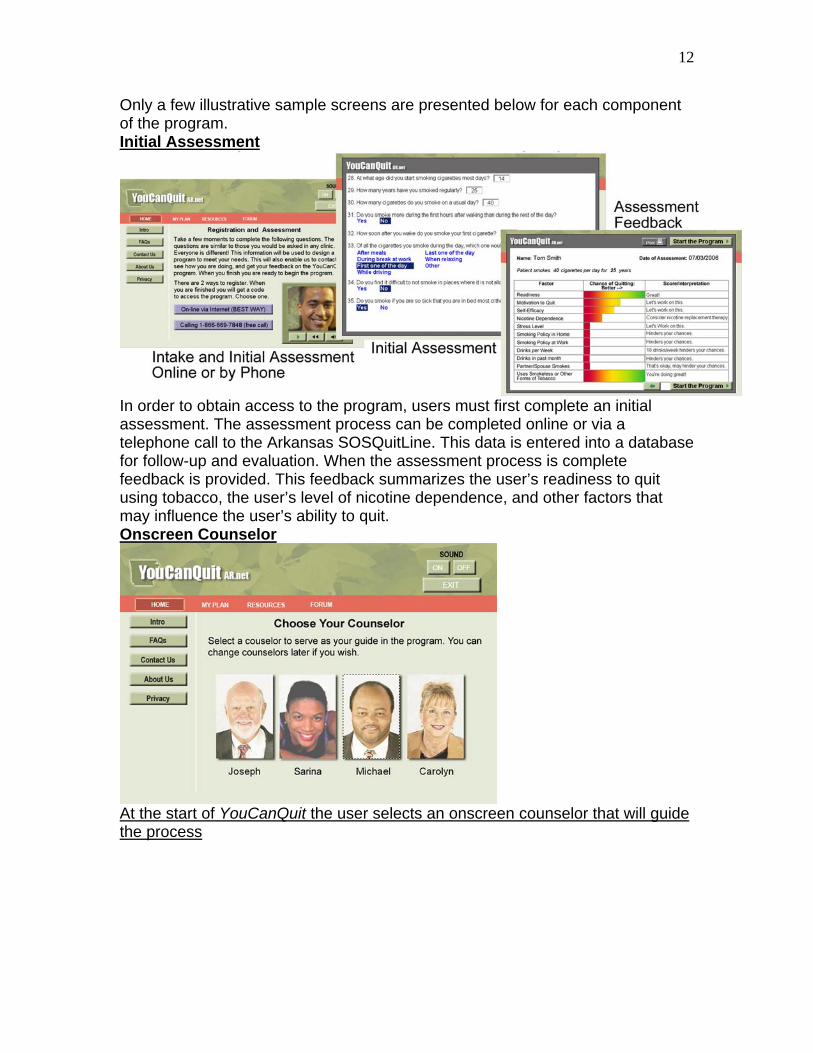
Only a few illustrative sample screens are presented below for each component of the program. Initial Assessment
In order to obtain access to the program, users must first complete an initial assessment. The assessment process can be completed online or via a telephone call to the Arkansas SOSQuitLine. This data is entered into a database for follow-up and evaluation. When the assessment process is complete feedback is provided. This feedback summarizes the user’s readiness to quit using tobacco, the user’s level of nicotine dependence, and other factors that may influence the user’s ability to quit. Onscreen Counselor
At the start of YouCanQuit the user selects an onscreen counselor that will guide the process
13
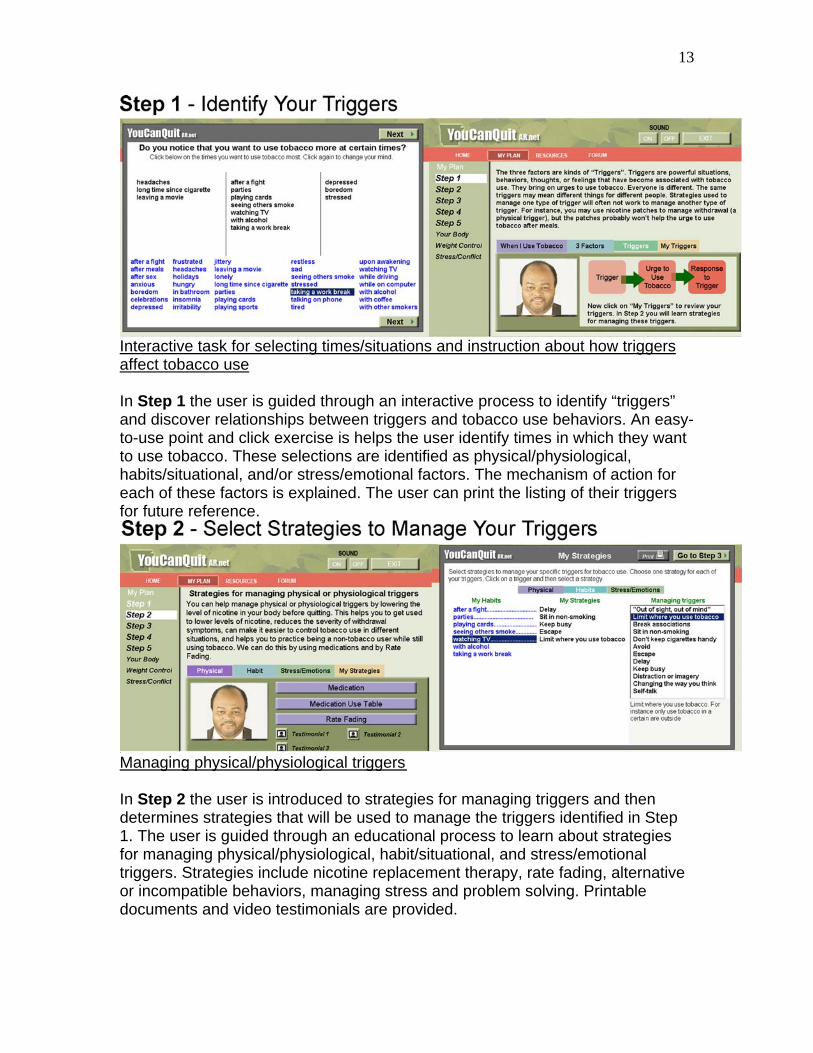
Interactive task for selecting times/situations and instruction about how triggers affect tobacco use In Step 1 the user is guided through an interactive process to identify “triggers” and discover relationships between triggers and tobacco use behaviors. An easy-to-use point and click exercise is helps the user identify times in which they want to use tobacco. These selections are identified as physical/physiological, habits/situational, and/or stress/emotional factors. The mechanism of action for each of these factors is explained. The user can print the listing of their triggers for future reference.
Managing physical/physiological triggers In Step 2 the user is introduced to strategies for managing triggers and then determines strategies that will be used to manage the triggers identified in Step 1. The user is guided through an educational process to learn about strategies for managing physical/physiological, habit/situational, and stress/emotional triggers. Strategies include nicotine replacement therapy, rate fading, alternative or incompatible behaviors, managing stress and problem solving. Printable documents and video testimonials are provided.
14
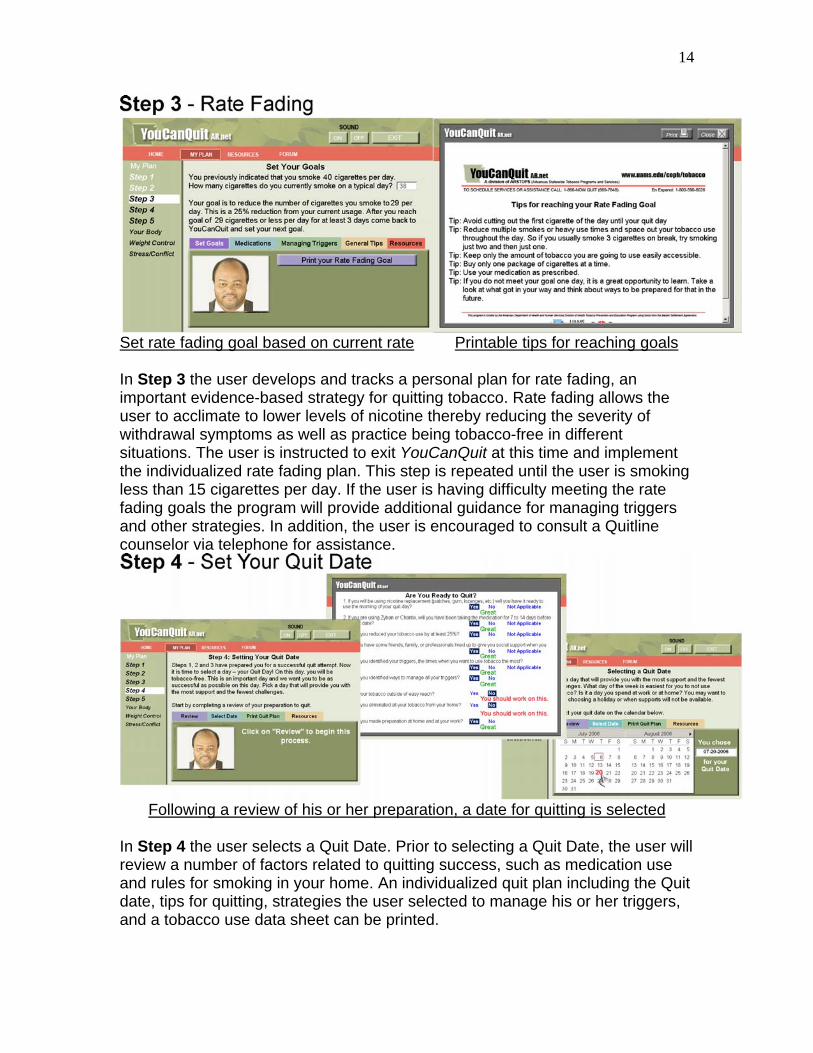
Set rate fading goal based on current rate Printable tips for reaching goals In Step 3 the user develops and tracks a personal plan for rate fading, an important evidence-based strategy for quitting tobacco. Rate fading allows the user to acclimate to lower levels of nicotine thereby reducing the severity of withdrawal symptoms as well as practice being tobacco-free in different situations. The user is instructed to exit YouCanQuit at this time and implement the individualized rate fading plan. This step is repeated until the user is smoking less than 15 cigarettes per day. If the user is having difficulty meeting the rate fading goals the program will provide additional guidance for managing triggers and other strategies. In addition, the user is encouraged to consult a Quitline counselor via telephone for assistance.
Following a review of his or her preparation, a date for quitting is selected In Step 4 the user selects a Quit Date. Prior to selecting a Quit Date, the user will review a number of factors related to quitting success, such as medication use and rules for smoking in your home. An individualized quit plan including the Quit date, tips for quitting, strategies the user selected to manage his or her triggers, and a tobacco use data sheet can be printed.
15
Screen views of two pages in Step 5
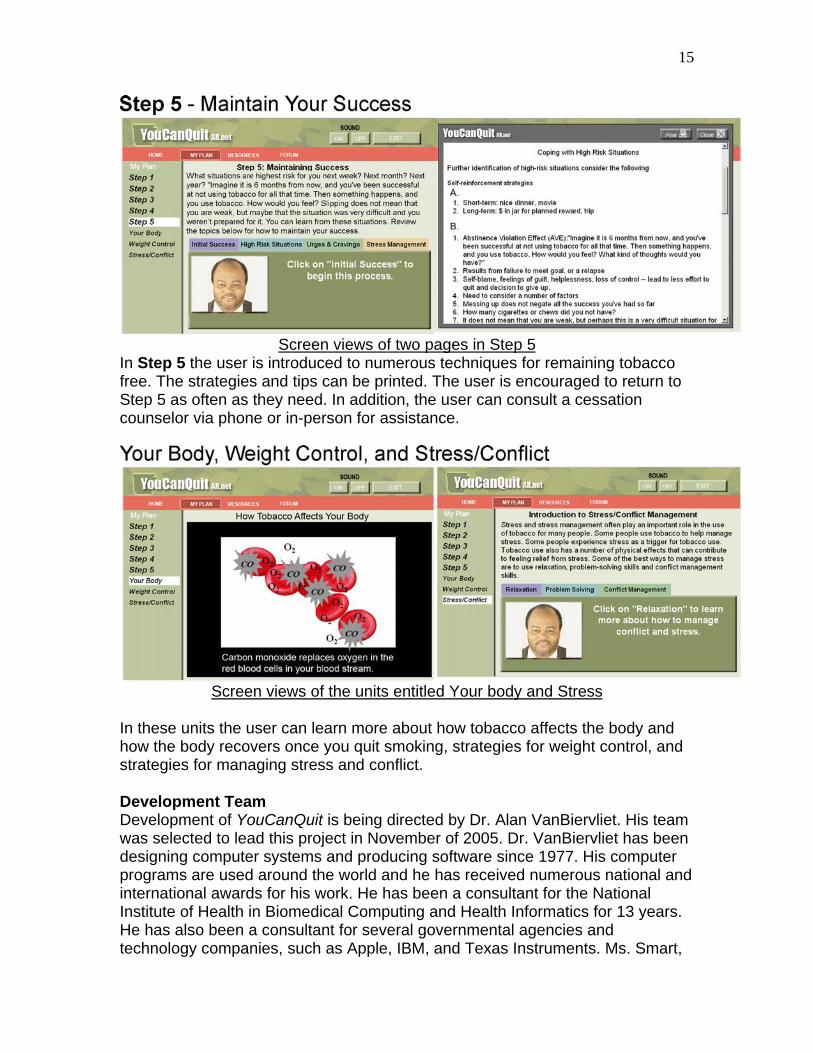
In Step 5 the user is introduced to numerous techniques for remaining tobacco free. The strategies and tips can be printed. The user is encouraged to return to Step 5 as often as they need. In addition, the user can consult a cessation counselor via phone or in-person for assistance.
Screen views of the units entitled Your body and Stress
In these units the user can learn more about how tobacco affects the body and how the body recovers once you quit smoking, strategies for weight control, and strategies for managing stress and conflict. Development Team Development of YouCanQuit is being directed by Dr. Alan VanBiervliet. His team was selected to lead this project in November of 2005. Dr. VanBiervliet has been designing computer systems and producing software since 1977. His computer programs are used around the world and he has received numerous national and international awards for his work. He has been a consultant for the National Institute of Health in Biomedical Computing and Health Informatics for 13 years. He has also been a consultant for several governmental agencies and technology companies, such as Apple, IBM, and Texas Instruments. Ms. Smart,

16
his associate, has worked on the team for the past 10 years and has developed considerable expertise in software development. Dr. VanBiervliet and Ms. Smart are using procedures they have developed over the years to successfully produce an effective, cost efficient program. The UAMS Creative Services Department has produced graphics, professional scripts, and video clips for use in YouCanQuit. Dr. Sheffer provided clinical guidance and contributed to the majority of the writing. Future Expectations and Directions Appropriate field testing must be accomplished in order to complete this project. We expect to test several versions of the product with the goal of continued refinement in order to maximize applicability and outcomes. We envision YouCanQuit AR to be available both as a treatment option and as an adjunct to other treatment modalities (i.e. over-the-phone or face-to-face treatment) in fiscal year 2006-2007. Additionally, once the initial program is developed and tested, tailored versions designed to attract and meet the needs of various population groups such as adolescents, young adults, ethnic groups, etc. will need to be developed.
17
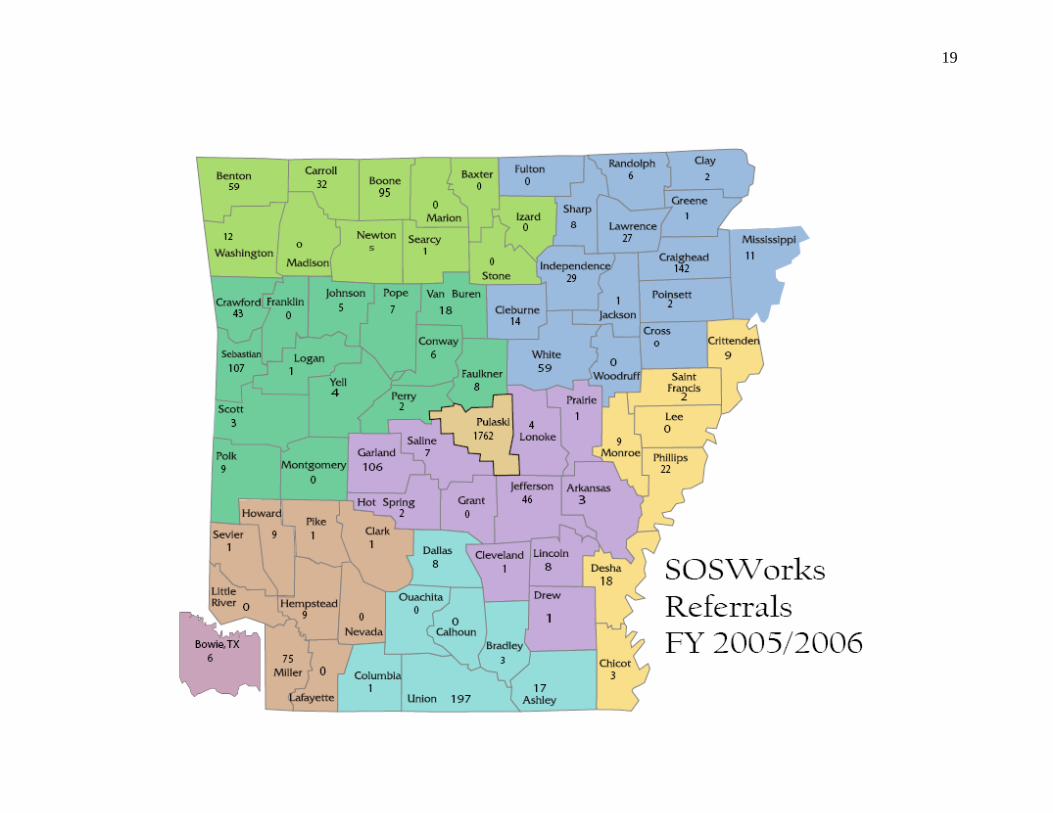
SOSWorks Fax-Back Referral Program Based on a model for the convergence of telephone-based treatment and health care services, SOSWorks is a free, proactive, centralized referral system that links tobacco users to the state-sponsored, evidence-based cessation services in Arkansas. The program targets all healthcare providers, i.e. primary care and specialists, dentists, hospitals, and third-party payers, and is also used by workplaces, individuals, chamber of commerce organizations, and others. Through SOSWorks, tobacco users are linked to state tobacco cessation services in a two simple steps:
• The HIPAA-compliant Treatment Referral Form is completed and faxed to
SOSWorks.
• SOSWorks contacts the tobacco user by telephone at their convenience and discusses cessation options, provides motivational counseling, and refers them to either face-to-face or telephone-based treatment. If a referral is refused, they are mailed self-help and/or motivational and tailored materials.
Healthcare providers are given feedback on all referrals:
• Seven days after the initial contact, SOSWorks contacts the patient to follow-up on the status of the referral. A report is faxed to the healthcare provider.
• Three months after the initial contact, SOSWorks again contacts the
patient to follow-up on the status of the referral and satisfaction with treatment. A report is faxed to the healthcare provider.
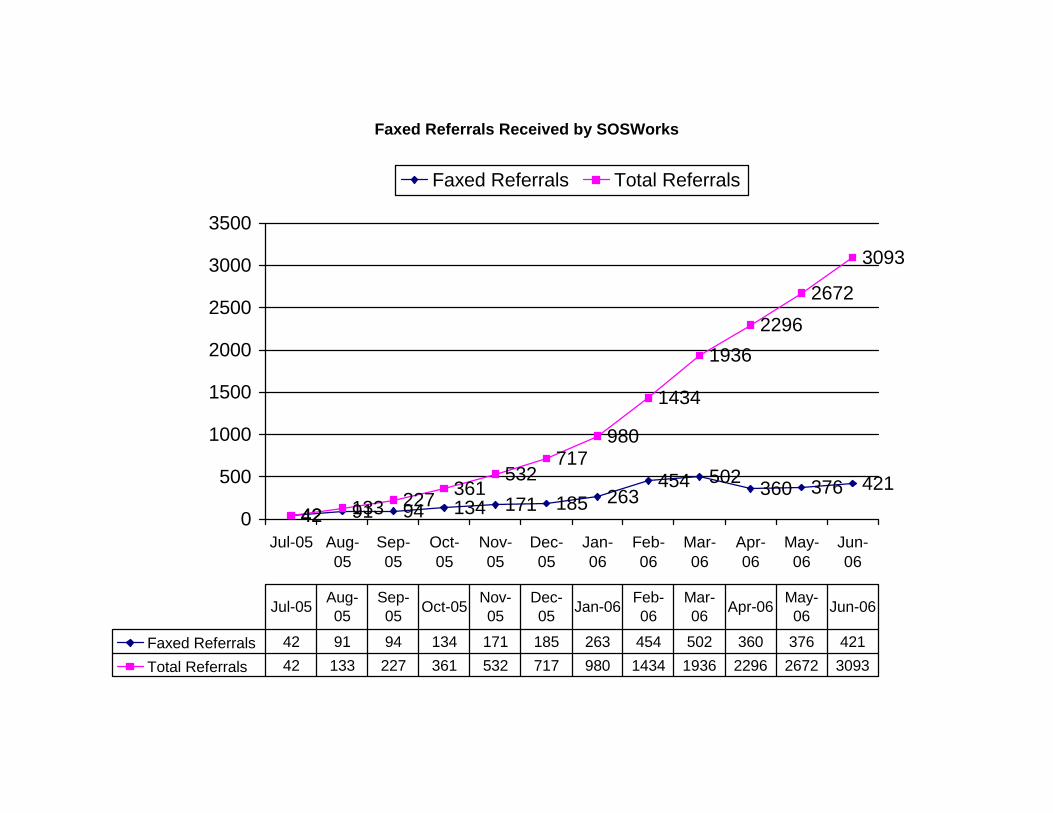
SOSWorks was developed by Christine Sheffer, PhD in February 2004. The contract to provide these services was awarded to COPH beginning July 1, 2005. SOSWorks expected to serve 100 referrals per month or 1200 referrals in the 2005-2006 fiscal year. SOSWorks actually served 3093 referrals from 438 healthcare providers in 216 clinics and workplaces exceeding expectations by 1893 referrals or 157%. See the following tables for more information. 1. Pacific Center on Tobacco and Health. Linking a network: Integrate quitlines with healthcare systems.2003.http://www.paccenter.org/public/reports
Faxed Referrals Received by SOSWorks
42 91 94 134 171 185 263454 502 360 376 421
42 133 227 361532
717980
1434
19362296
2672
3093
0
500
1000
1500
2000
2500
3000
3500
Jul-05 Aug-05
Sep-05
Oct-05
Nov-05
Dec-05
Jan-06
Feb-06
Mar-06
Apr-06
May-06
Jun-06
Faxed Referrals Total Referrals
Faxed Referrals 42 91 94 134 171 185 263 454 502 360 376 421Total Referrals 42 133 227 361 532 717 980 1434 1936 2296 2672 3093
Jul-05 Aug-05
Sep-05 Oct-05 Nov-
05Dec-05 Jan-06 Feb-
06Mar-06 Apr-06 May-
06 Jun-06
19
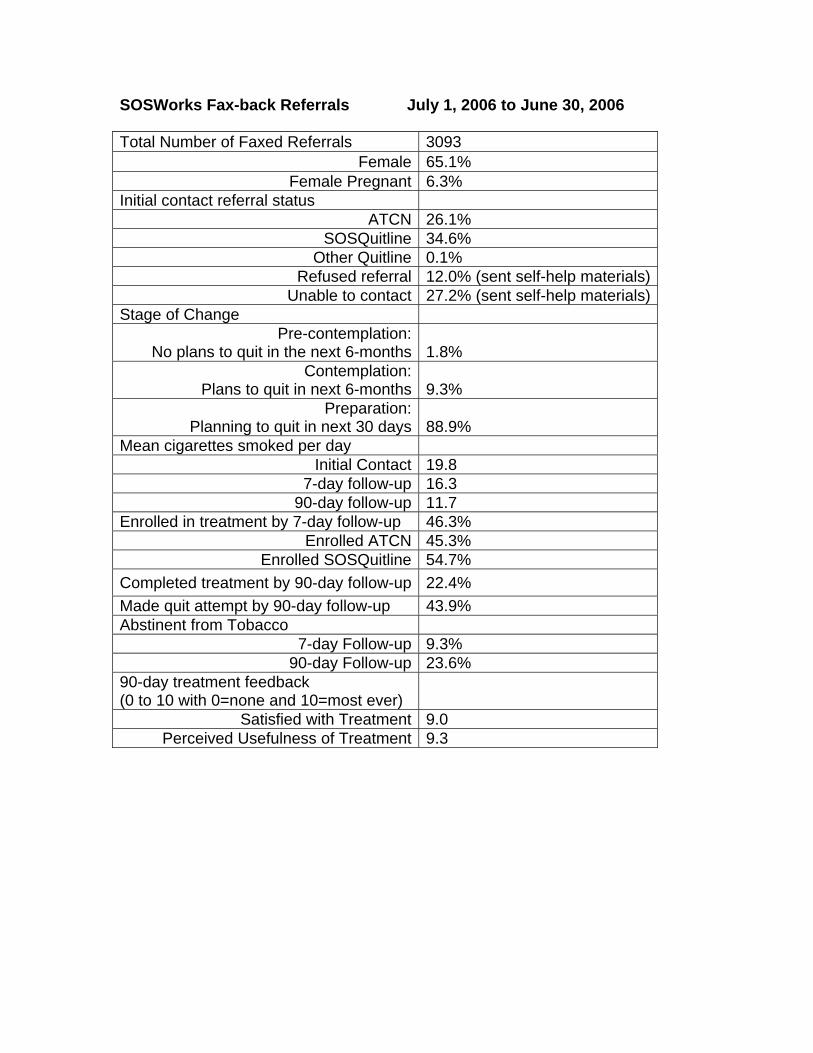
SOSWorks Fax-back Referrals July 1, 2006 to June 30, 2006
Total Number of Faxed Referrals 3093 Female 65.1%
Female Pregnant 6.3% Initial contact referral status
ATCN 26.1% SOSQuitline 34.6%
Other Quitline 0.1% Refused referral 12.0% (sent self-help materials)
Unable to contact 27.2% (sent self-help materials) Stage of Change
Pre-contemplation: No plans to quit in the next 6-months
1.8%
Contemplation: Plans to quit in next 6-months
9.3%
Preparation: Planning to quit in next 30 days
88.9%
Mean cigarettes smoked per day Initial Contact 19.8
7-day follow-up 16.3 90-day follow-up 11.7
Enrolled in treatment by 7-day follow-up 46.3% Enrolled ATCN 45.3%
Enrolled SOSQuitline 54.7% Completed treatment by 90-day follow-up 22.4% Made quit attempt by 90-day follow-up 43.9% Abstinent from Tobacco
7-day Follow-up 9.3% 90-day Follow-up 23.6%
90-day treatment feedback (0 to 10 with 0=none and 10=most ever)
Satisfied with Treatment 9.0 Perceived Usefulness of Treatment 9.3

21
Future Directions for SOSWorks SOSWorks will continue to expand the program to healthcare settings and workplaces while adding efforts to engage churches and ministries in fiscal year 2006-2007. The PEP and SWAP programs are key for disseminating this convenient and popular method of linking tobacco users with treatment. Also key is presenting the programs at local and regional professional meetings. We expect SOSWorks to continue to grow as healthcare providers, workplaces, and others throughout the state become more aware of and confident with making referrals to for treating tobacco use and dependence.
22
The Tobacco Dependence Treatment Programs: The Arkansas SOSQuitline (QL)
and Arkansas Tobacco Cessation Network (ATCN)
The AR Stops programs currently include two evidence-based, statewide tobacco dependence treatment programs – The Arkansas SOSQuitline and the Arkansas Tobacco Cessation Network. Each of these programs delivers intensive, evidence-based, cognitive-behavioral treatment for tobacco dependence in a different modality. Outcome assessments are conducted at 3-, 6-, and 12-months post-discharge. Treatment is based on a bio-psycho-social model and manualized to ensure consistency. Delivery is highly individualized, highly interactive, and does not require literacy. The programs offer numerous treatment contacts and a wide variety of tailored materials provided to participants as needed. Treatment is delivered by specially trained Tobacco Interventionists, all of whom have completed a 4-day Tobacco Interventionist workshop and are clinically supervised. Follow-up training sessions for Tobacco Interventionists are delivered periodically. Services include medication assistance, including nicotine patches for those patients who are attending treatment sessions and have the permission of their healthcare providers. Self-help and motivational materials are provided to all contacts who are not interested in treatment as well as those who do not keep their treatment appointments. Treatment is available in Spanish. The website (www.uams.edu/coph/tobacco) enables participants to contact a Tobacco Interventionist by e-mail. Future Directions for the Treatment Programs These programs will be expected to reach 1-2% of the estimated 492,438 tobacco users in Arkansas over the next year with high-quality, standardized services. Congruent with the goals and objectives of the Arkansas Division of Health Tobacco Prevention and Education Program for each of these programs, future focus will be to develop referrals from the healthcare community, increase enrollment, and provide for the continued growth, training, and proficiency of the new Interventionists.
23
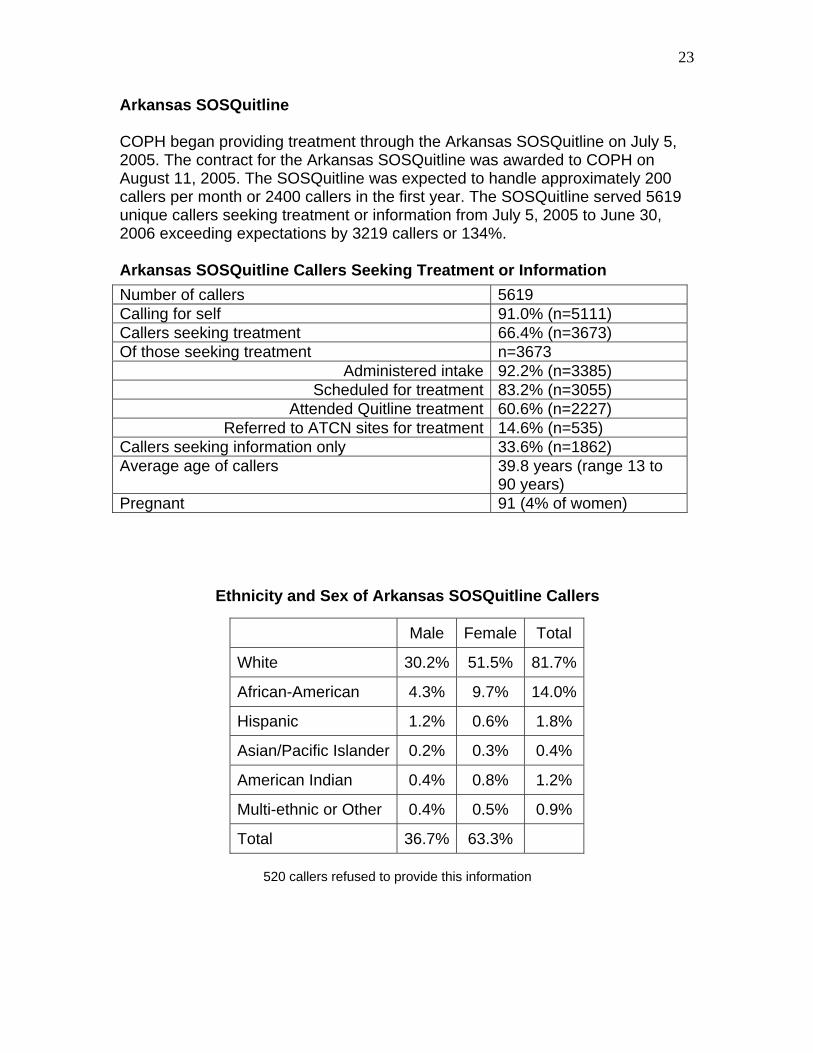
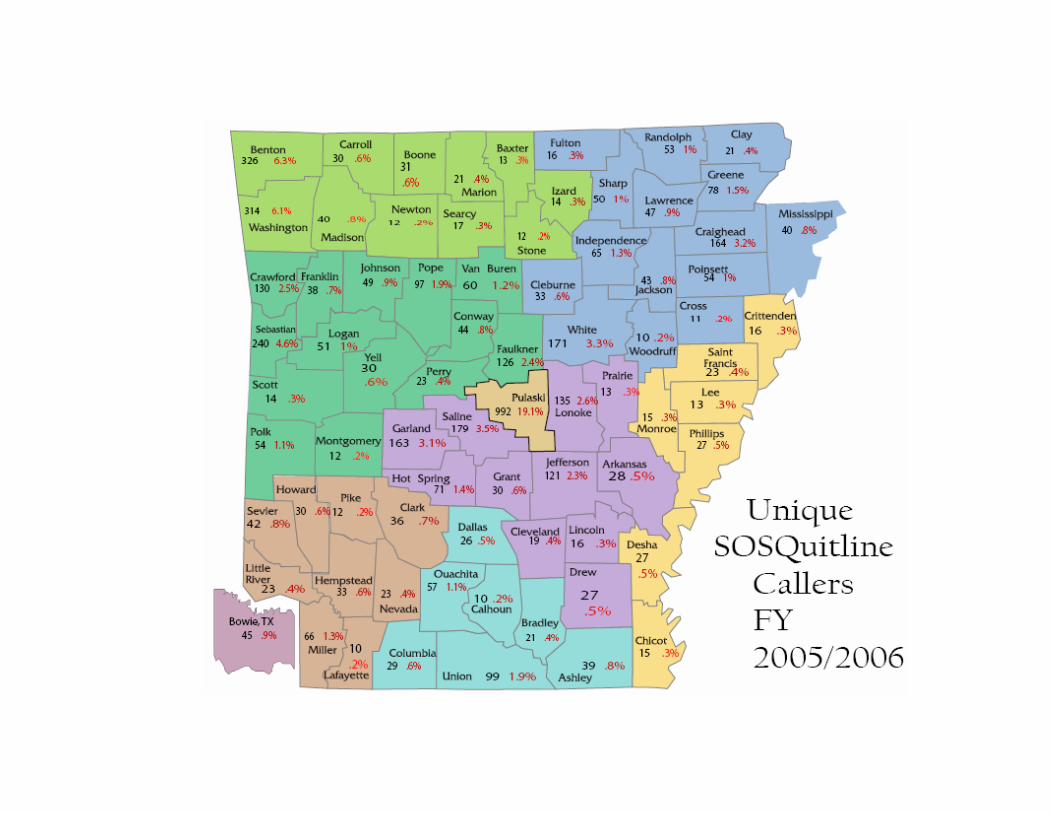
Arkansas SOSQuitline COPH began providing treatment through the Arkansas SOSQuitline on July 5, 2005. The contract for the Arkansas SOSQuitline was awarded to COPH on August 11, 2005. The SOSQuitline was expected to handle approximately 200 callers per month or 2400 callers in the first year. The SOSQuitline served 5619 unique callers seeking treatment or information from July 5, 2005 to June 30, 2006 exceeding expectations by 3219 callers or 134%. Arkansas SOSQuitline Callers Seeking Treatment or Information
Ethnicity and Sex of Arkansas SOSQuitline Callers
520 callers refused to provide this information
Number of callers 5619 Calling for self 91.0% (n=5111) Callers seeking treatment 66.4% (n=3673) Of those seeking treatment n=3673
Administered intake 92.2% (n=3385) Scheduled for treatment 83.2% (n=3055)
Attended Quitline treatment 60.6% (n=2227) Referred to ATCN sites for treatment 14.6% (n=535)
Callers seeking information only 33.6% (n=1862) Average age of callers 39.8 years (range 13 to
90 years) Pregnant 91 (4% of women)
Male Female Total
White 30.2% 51.5% 81.7%
African-American 4.3% 9.7% 14.0%
Hispanic 1.2% 0.6% 1.8%
Asian/Pacific Islander 0.2% 0.3% 0.4%
American Indian 0.4% 0.8% 1.2%
Multi-ethnic or Other 0.4% 0.5% 0.9%
Total 36.7% 63.3%
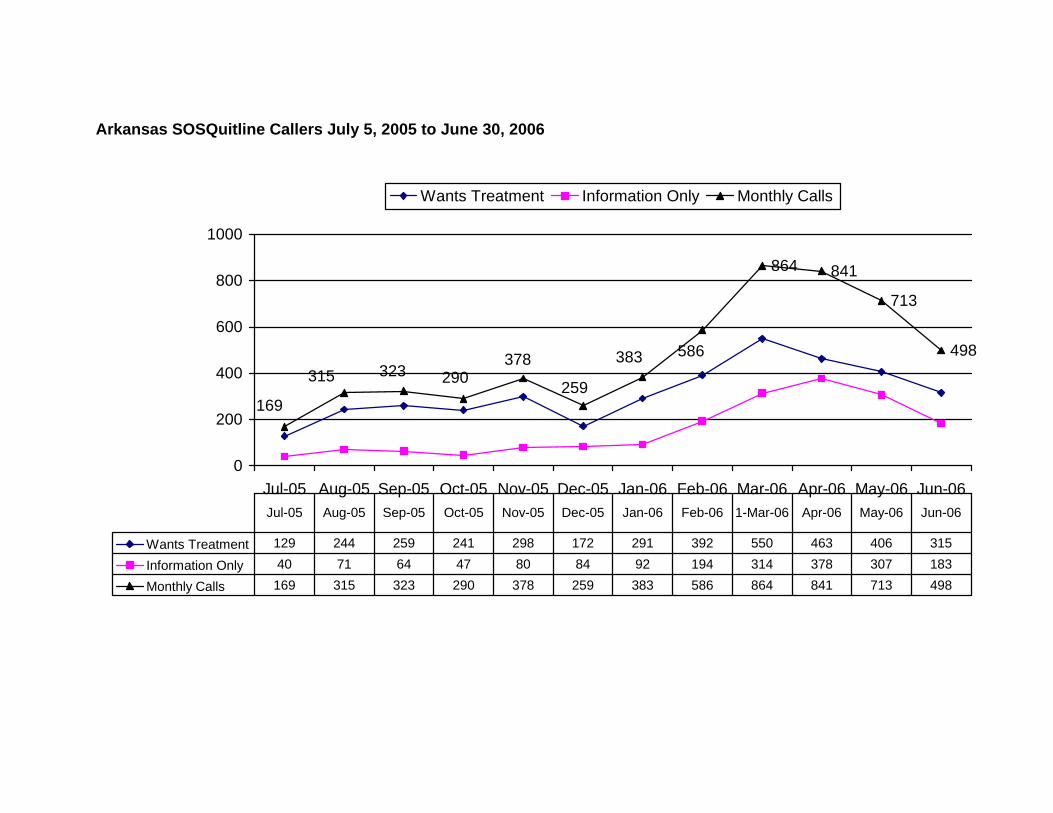
Arkansas SOSQuitline Callers July 5, 2005 to June 30, 2006
864 841
713
498
169
586378290315 323
383
259
0
200
400
600
800
1000
Jul-05 Aug-05 Sep-05 Oct-05 Nov-05 Dec-05 Jan-06 Feb-06 Mar-06 Apr-06 May-06 Jun-06
Wants Treatment Information Only Monthly Calls
Wants Treatment 129 244 259 241 298 172 291 392 550 463 406 315
Information Only 40 71 64 47 80 84 92 194 314 378 307 183
Monthly Calls 169 315 323 290 378 259 383 586 864 841 713 498
Jul-05 Aug-05 Sep-05 Oct-05 Nov-05 Dec-05 Jan-06 Feb-06 1-Mar-06 Apr-06 May-06 Jun-06
26
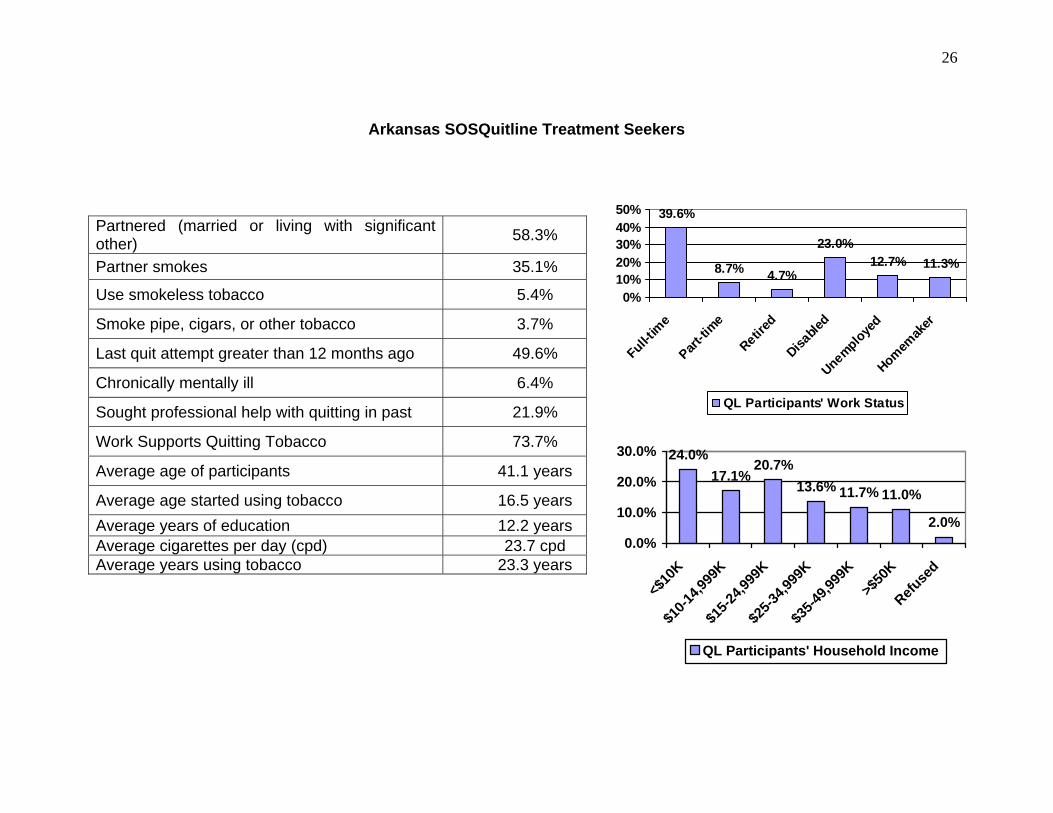
Arkansas SOSQuitline Treatment Seekers
39.6%
8.7% 4.7%
23.0%12.7% 11.3%
0%10%20%30%40%50%
Full-tim
ePart
-time
Retired
Disable
dUnemploye
dHomem
aker
QL Participants' Work Status
24.0%17.1%
20.7%13.6% 11.7% 11.0%
2.0%0.0%
10.0%
20.0%
30.0%
<$10
K$1
0-14,9
99K
$15-2
4,999
K$2
5-34,9
99K
$35-4
9,999
K>$
50K
Refuse
d
QL Participants' Household Income
Partnered (married or living with significant other) 58.3%
Partner smokes 35.1%
Use smokeless tobacco 5.4%
Smoke pipe, cigars, or other tobacco 3.7%
Last quit attempt greater than 12 months ago 49.6%
Chronically mentally ill 6.4%
Sought professional help with quitting in past 21.9%
Work Supports Quitting Tobacco 73.7%
Average age of participants 41.1 years
Average age started using tobacco 16.5 years Average years of education 12.2 years Average cigarettes per day (cpd) 23.7 cpd Average years using tobacco 23.3 years
27
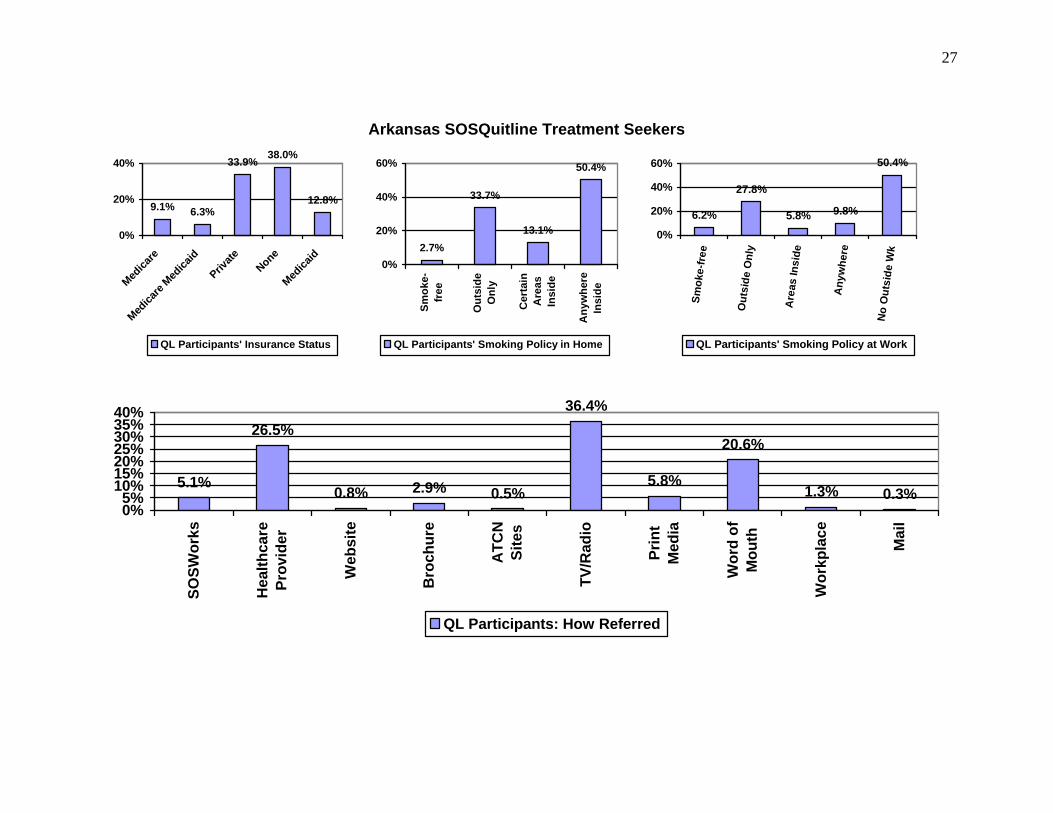
Arkansas SOSQuitline Treatment Seekers
9.1% 6.3%
33.9% 38.0%
12.8%
0%
20%
40%
Medica
re
Medica
re Med
icaid
Private
NoneMed
icaid
QL Participants' Insurance Status
2.7%
33.7%
13.1%
50.4%
0%
20%
40%
60%
Smok
e-fr
ee
Out
side
Onl
y
Cer
tain
Are
asIn
side
Any
whe
reIn
side
QL Participants' Smoking Policy in Home
6.2%
27.8%
5.8% 9.8%
50.4%
0%
20%
40%
60%
Smok
e-fr
ee
Out
side
Onl
y
Are
as In
side
Any
whe
re
No
Out
side
Wk
QL Participants' Smoking Policy at Work
5.1%
26.5%
0.8% 2.9% 0.5%
36.4%
5.8%
20.6%
1.3% 0.3%0%5%
10%15%20%25%30%35%40%
SOSW
orks
Hea
lthca
rePr
ovid
er
Web
site
Bro
chur
e
ATC
NSi
tes
TV/R
adio
Prin
tM
edia
Wor
d of
Mou
th
Wor
kpla
ce
Mai
l
QL Participants: How Referred
28
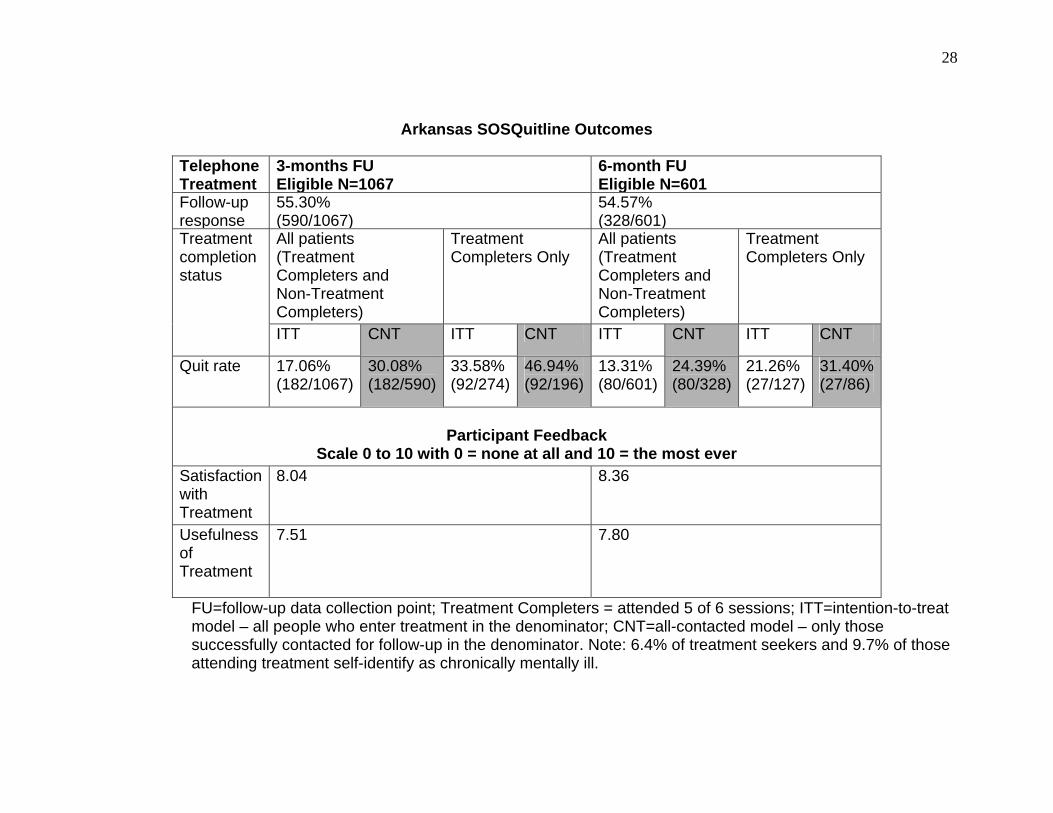
Arkansas SOSQuitline Outcomes
FU=follow-up data collection point; Treatment Completers = attended 5 of 6 sessions; ITT=intention-to-treat model – all people who enter treatment in the denominator; CNT=all-contacted model – only those successfully contacted for follow-up in the denominator. Note: 6.4% of treatment seekers and 9.7% of those attending treatment self-identify as chronically mentally ill.
Telephone Treatment
3-months FU Eligible N=1067
6-month FU Eligible N=601
Follow-up response
55.30% (590/1067)
54.57% (328/601)
All patients (Treatment Completers and Non-Treatment Completers)
Treatment Completers Only
All patients (Treatment Completers and Non-Treatment Completers)
Treatment Completers Only
Treatment completion status
ITT CNT ITT CNT ITT CNT ITT CNT
Quit rate 17.06% (182/1067)
30.08% (182/590)
33.58% (92/274)
46.94% (92/196)
13.31% (80/601)
24.39% (80/328)
21.26% (27/127)
31.40%(27/86)
Participant Feedback
Scale 0 to 10 with 0 = none at all and 10 = the most ever Satisfaction with Treatment
8.04 8.36
Usefulness of Treatment
7.51 7.80
29
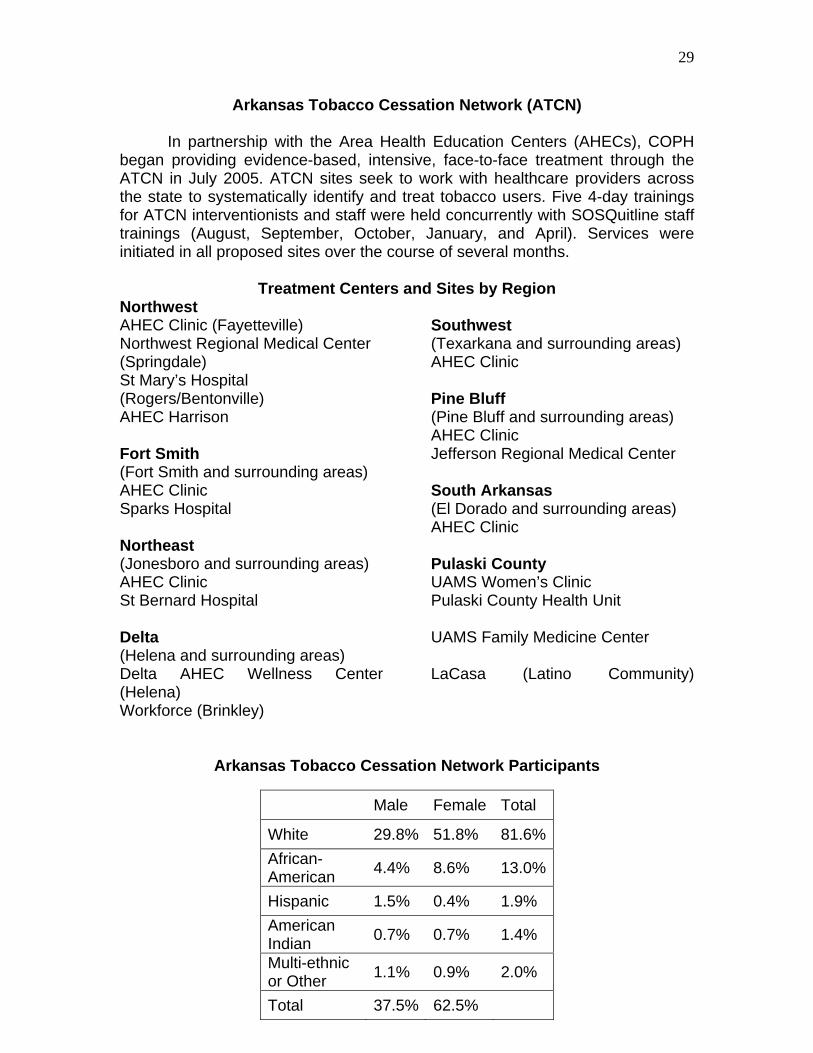
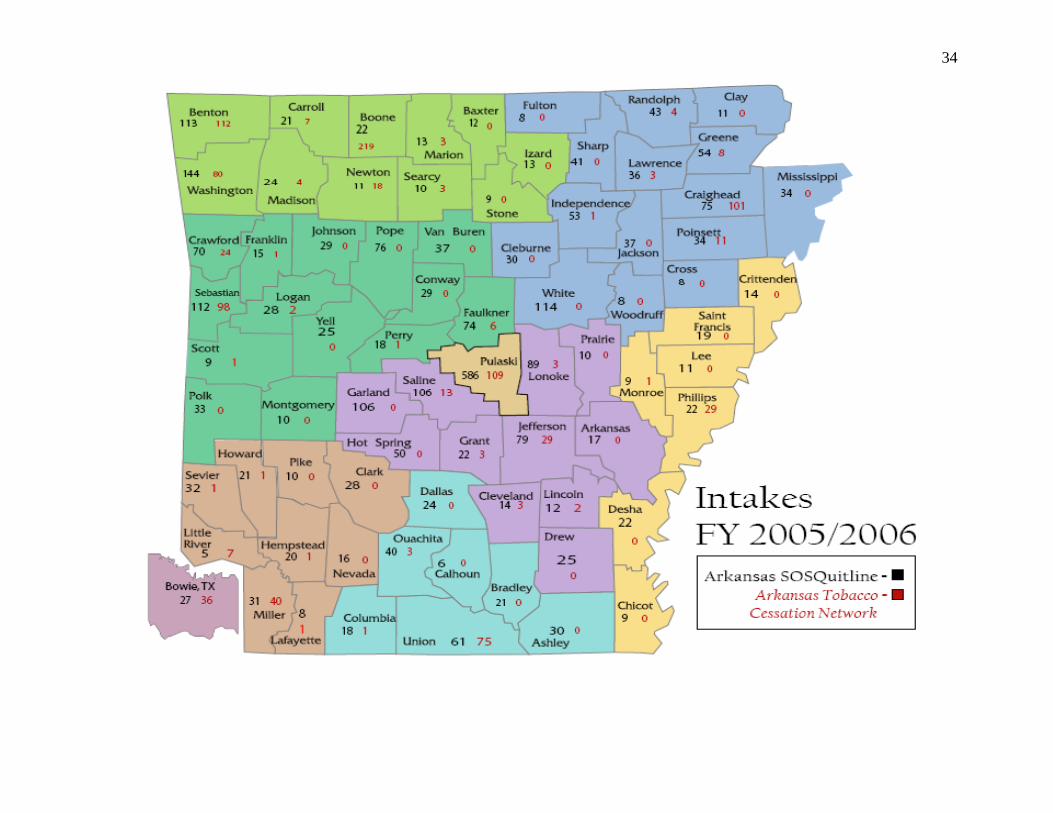
Arkansas Tobacco Cessation Network (ATCN)
In partnership with the Area Health Education Centers (AHECs), COPH began providing evidence-based, intensive, face-to-face treatment through the ATCN in July 2005. ATCN sites seek to work with healthcare providers across the state to systematically identify and treat tobacco users. Five 4-day trainings for ATCN interventionists and staff were held concurrently with SOSQuitline staff trainings (August, September, October, January, and April). Services were initiated in all proposed sites over the course of several months.
Treatment Centers and Sites by Region
Northwest AHEC Clinic (Fayetteville) Northwest Regional Medical Center (Springdale) St Mary’s Hospital (Rogers/Bentonville) AHEC Harrison Fort Smith (Fort Smith and surrounding areas) AHEC Clinic Sparks Hospital Northeast (Jonesboro and surrounding areas) AHEC Clinic St Bernard Hospital Delta (Helena and surrounding areas) Delta AHEC Wellness Center (Helena) Workforce (Brinkley)
Southwest (Texarkana and surrounding areas) AHEC Clinic Pine Bluff (Pine Bluff and surrounding areas) AHEC Clinic Jefferson Regional Medical Center South Arkansas (El Dorado and surrounding areas) AHEC Clinic Pulaski County UAMS Women’s Clinic Pulaski County Health Unit UAMS Family Medicine Center LaCasa (Latino Community)
Arkansas Tobacco Cessation Network Participants
Male Female Total
White 29.8% 51.8% 81.6%African-American 4.4% 8.6% 13.0%
Hispanic 1.5% 0.4% 1.9% American Indian 0.7% 0.7% 1.4%
Multi-ethnic or Other 1.1% 0.9% 2.0%
Total 37.5% 62.5%
26 25 37 45 56 49 5126 5188
133189
238
336387
566
691
818
933
115179
98 127125
0
100
200
300
400
500
600
700
800
900
1000
1100
Monthly Enrollment Total Enrolled
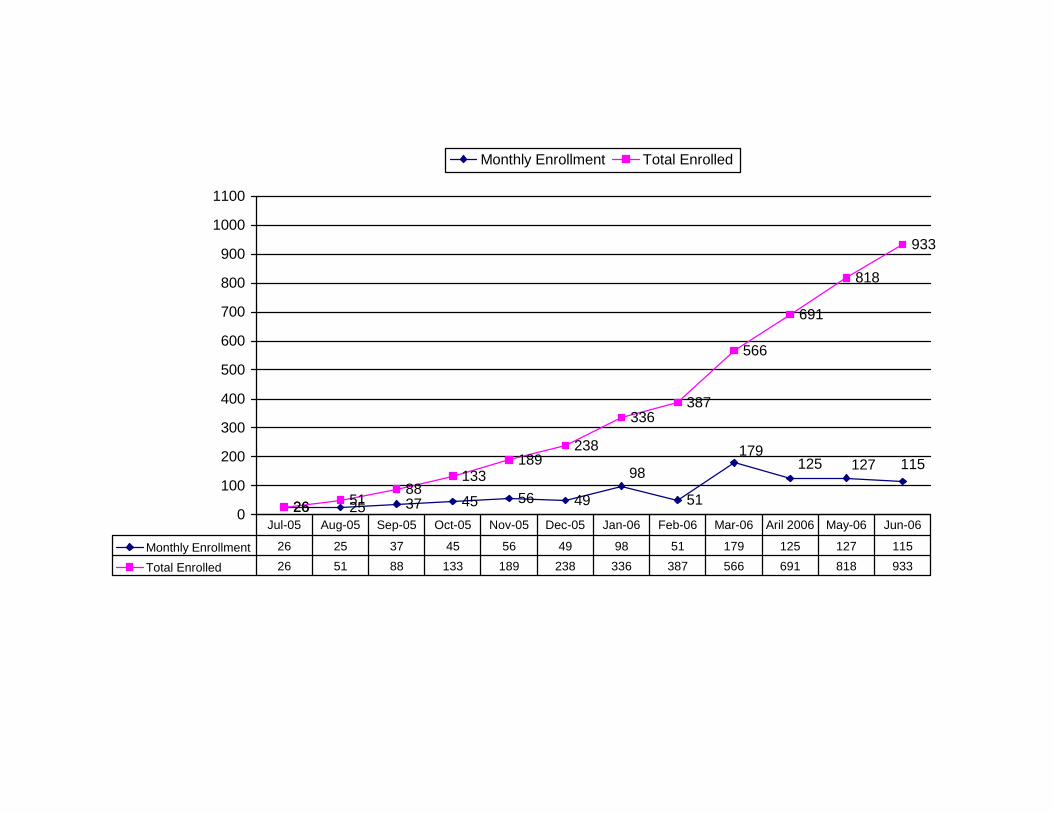
Monthly Enrollment 26 25 37 45 56 49 98 51 179 125 127 115
Total Enrolled 26 51 88 133 189 238 336 387 566 691 818 933
Jul-05 Aug-05 Sep-05 Oct-05 Nov-05 Dec-05 Jan-06 Feb-06 Mar-06 Aril 2006 May-06 Jun-06
31
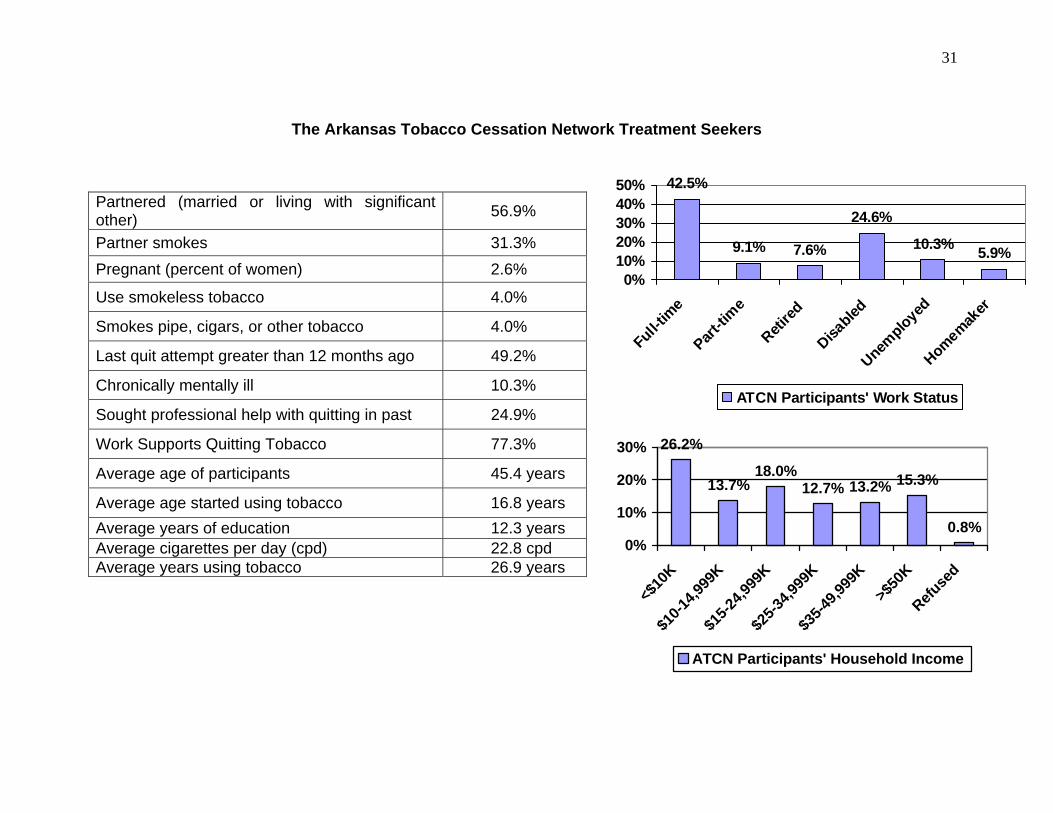
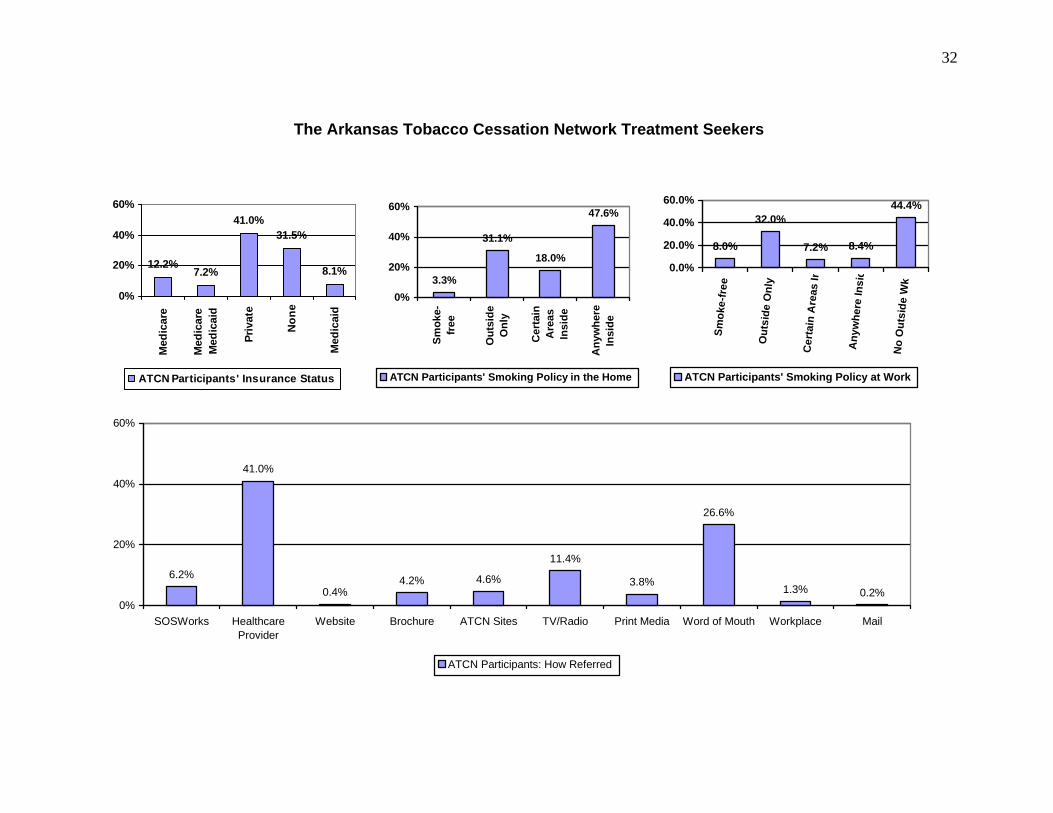
The Arkansas Tobacco Cessation Network Treatment Seekers
42.5%
9.1% 7.6%
24.6%
10.3% 5.9%
0%10%20%30%40%50%
Full-tim
ePart
-time
Retired
Disabled
Unemployed
Homemaker
ATCN Participants' Work Status
26.2%
13.7%18.0%
12.7% 13.2% 15.3%
0.8%0%
10%
20%
30%
<$10
K$1
0-14,9
99K
$15-2
4,999
K$2
5-34,9
99K
$35-4
9,999
K>$
50K
Refuse
d
ATCN Participants' Household Income
Partnered (married or living with significant other) 56.9%
Partner smokes 31.3% Pregnant (percent of women) 2.6%
Use smokeless tobacco 4.0%
Smokes pipe, cigars, or other tobacco 4.0%
Last quit attempt greater than 12 months ago 49.2%
Chronically mentally ill 10.3%
Sought professional help with quitting in past 24.9%
Work Supports Quitting Tobacco 77.3%
Average age of participants 45.4 years
Average age started using tobacco 16.8 years Average years of education 12.3 years Average cigarettes per day (cpd) 22.8 cpd Average years using tobacco 26.9 years
32
The Arkansas Tobacco Cessation Network Treatment Seekers
12.2%7.2%
41.0%31.5%
8.1%
0%
20%
40%
60%
Med
icar
e
Med
icar
eM
edic
aid
Priv
ate
Non
e
Med
icai
d
ATCN Participants' Insurance Status
3.3%
31.1%
18.0%
47.6%
0%
20%
40%
60%
Smok
e-fr
ee
Out
side
Onl
y
Cer
tain
Are
asIn
side
Any
whe
reIn
side
ATCN Participants' Smoking Policy in the Home
8.0%
32.0%
7.2% 8.4%
44.4%
0.0%
20.0%
40.0%
60.0%
Smok
e-fr
ee
Out
side
Onl
y
Cer
tain
Are
as In
Any
whe
re In
sid
No
Out
side
Wk
ATCN Participants' Smoking Policy at Work
6.2%
41.0%
0.4%4.2% 4.6%
11.4%
3.8%
26.6%
1.3% 0.2%0%
20%
40%
60%
SOSWorks HealthcareProvider
Website Brochure ATCN Sites TV/Radio Print Media Word of Mouth Workplace Mail
ATCN Participants: How Referred
33
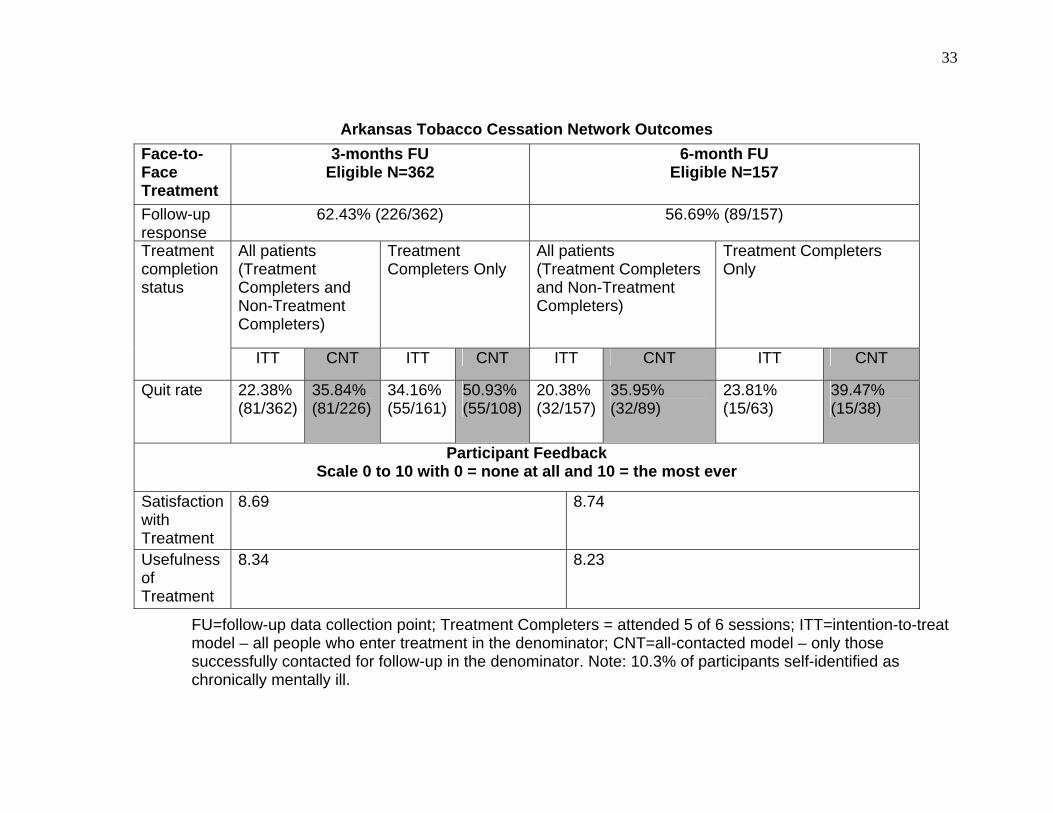
Arkansas Tobacco Cessation Network Outcomes
FU=follow-up data collection point; Treatment Completers = attended 5 of 6 sessions; ITT=intention-to-treat model – all people who enter treatment in the denominator; CNT=all-contacted model – only those successfully contacted for follow-up in the denominator. Note: 10.3% of participants self-identified as chronically mentally ill.
Face-to-Face Treatment
3-months FU Eligible N=362
6-month FU Eligible N=157
Follow-up response
62.43% (226/362) 56.69% (89/157)
All patients (Treatment Completers and Non-Treatment Completers)
Treatment Completers Only
All patients (Treatment Completers and Non-Treatment Completers)
Treatment Completers Only
Treatment completion status
ITT CNT ITT CNT ITT CNT ITT CNT
Quit rate 22.38% (81/362)
35.84% (81/226)
34.16% (55/161)
50.93% (55/108)
20.38% (32/157)
35.95% (32/89)
23.81% (15/63)
39.47% (15/38)
Participant Feedback Scale 0 to 10 with 0 = none at all and 10 = the most ever
Satisfaction with Treatment
8.69 8.74
Usefulness of Treatment
8.34 8.23
34
Emerging Threats: Smokeless Tobacco, Bidis, Kreteks, Herbal Cigarettes, Betel Quid, and the Ariva
Cigalette
All tobacco products are nicotine delivery devices. Inhalation is not necessary for nicotine to be absorbed into the body and for nicotine dependence to develop. All tobacco products also introduce a number of known carcinogens into the body as well as a number of other compounds. All tobacco products are potentially addictive. Cigarettes are currently the most popular form of tobacco used today. Engineered with specially cured tobacco-leaf and other additives, designed to be inhaled into the lungs, and rolled in flame–retardant paper, this product is the most effective method for administering nicotine today. Note: Smoking light cigarettes does not reduce risk.
Image obtained from www.trinketsandtrash.org
Other forms of smoked tobacco popular today include cigars, pipe tobacco, bidis, kreteks, herbal cigarettes, and betel quid. Cigars are tobacco rolled in tobacco leaf and engineered for absorption in the mouth. Large cigars can deliver as much nicotine as 20 or more cigarettes. Pipe tobacco is usually flavored, high in nicotine, and also engineered for absorption in the mouth. Although pipe tobacco and cigars are not intended for inhalation, users generally inhale some of the tobacco smoke and a significant amount of carbon monoxide. Less well known, but increasingly popular with young people are bidis, kreteks, and herbal cigarettes all of which are flavored cigarettes and/or tobacco mixed with
36
cloves and/or other herbs. Bidis are wrapped in temburni leaf instead of paper. Many of these products deliver significantly more nicotine and carcinogens than mainstream cigarettes.
Betel quid is most often a mixture of betel leaf, areca nut, slaked lime (calcium hydroxide), tobacco, and flavoring agents. Chewing or smoking
this product causes oral submucous fibrosis, a precancerous debilitating and progressive disease marked by stiffening of the oral mucosa and restriction of the mouth opening. Submucous fibrosis is not reversible, has no cure, and frequently results in oral cancer.
Forms of smokeless tobacco popular today are chew, wet snuff, dry snuff, snus, and finally the Ariva Cigalette. Chew is sometimes called plug and was the most popular form of tobacco until the mass production of the cigarette. Both chew and wet snuff, often called dip, are moist, chopped tobacco engineered to be held in the mouth. Dry snuff is a scented fine powder that can be snorted into the nose or held in the mouth. Snus is Swedish wet snuff. Snus from Sweden is often produced differently than the American wet snuff, but the industry is not regulated so there is no definitive evidence that all snus is produced similarly.
The Ariva Cigalette is a lozenge made from compressed tobacco and should not be confused with the Commit lozenge, a nicotine replacement product.
37
Although most of the tobacco users who sought treatment from the AR Stops tobacco treatment programs used cigarettes as their sole source of tobacco, 3-4% of treatment seekers this year smoked other forms of tobacco and 4-5% used smokeless tobacco. There was also considerable overlap among these two groups. Worth noting is the fact that tobacco users who use multiple forms of tobacco are more difficult to treat and have more difficulty quitting.
Of considerable interest of late is the increase in the sales of smokeless tobacco products in the US and elsewhere. The industry has reported an increase in
sales of smokeless tobacco of about 4% per year for the past several years. The tobacco industry has increased the variety and availability of smokeless products as well as introduced a number of dynamic advertising campaigns designed to attract new sectors of the potential tobacco using market such as youth and women. In Arkansas, there has been an increase in the prevalence of smokeless tobacco use among youth from 1999 to 2005. This increase is not, as yet, evident in the prevalence rates for adults, but clearly, the prevalence of smokeless tobacco use in Arkansas is not decreasing. The chart below illustrates the
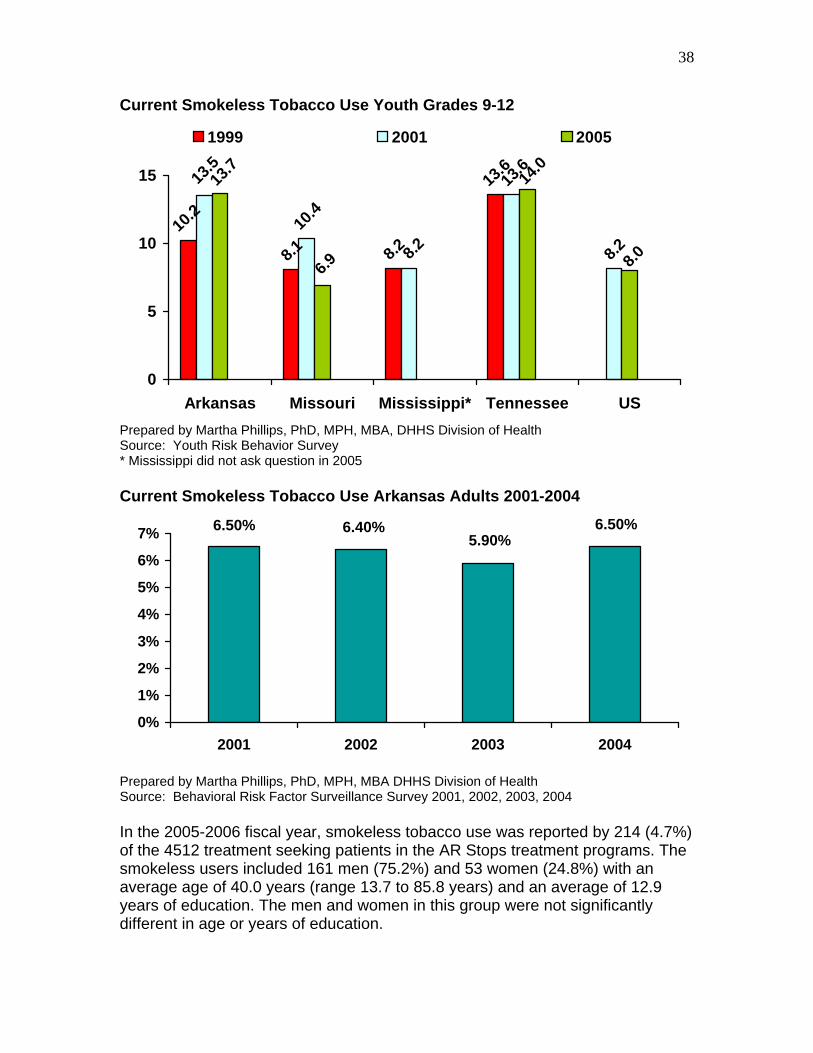
increase in prevalence among youth in Arkansas and compares the prevalence in Arkansas with that of three adjoining states.
38
Current Smokeless Tobacco Use Youth Grades 9-12
8.2
13.6
10.4
8.210
.2
8.1 8.2
13.613
.5
8.0
14.0
6.9
13.7
0
5
10
15
Arkansas Missouri Mississippi* Tennessee US
1999 2001 2005
Prepared by Martha Phillips, PhD, MPH, MBA, DHHS Division of Health Source: Youth Risk Behavior Survey * Mississippi did not ask question in 2005 Current Smokeless Tobacco Use Arkansas Adults 2001-2004
6.50%5.90%
6.40%6.50%
0%
1%
2%
3%
4%
5%
6%
7%
2001 2002 2003 2004
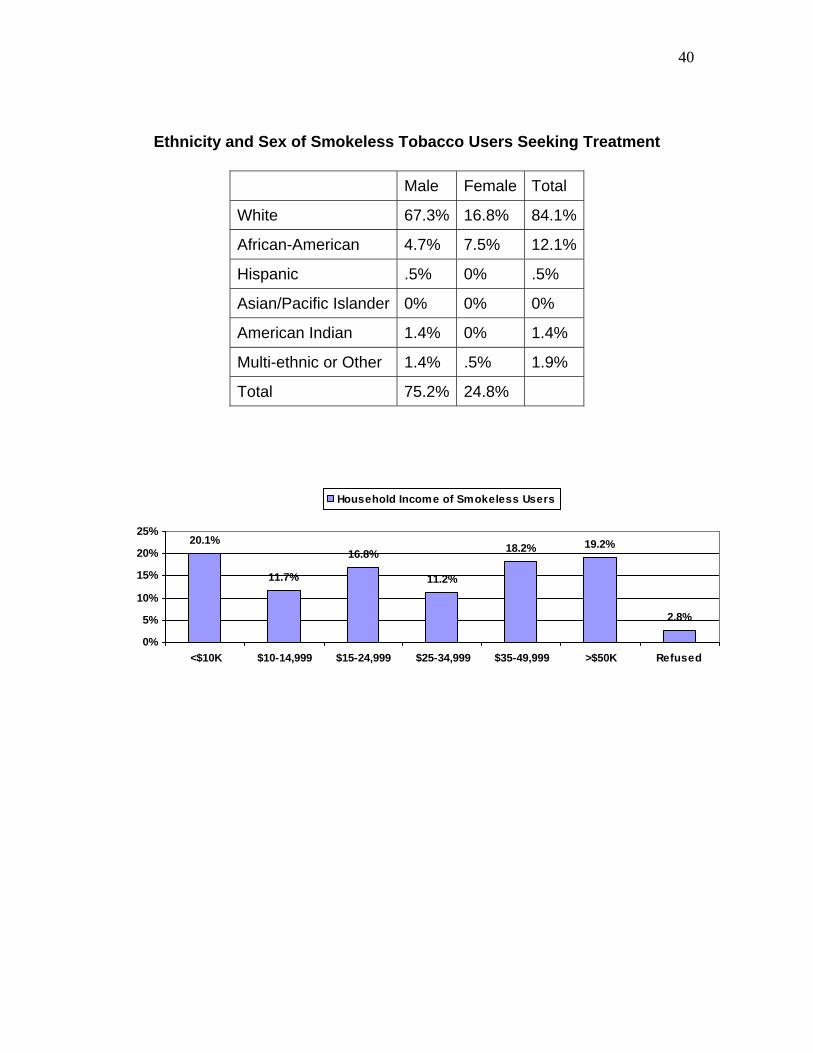
Prepared by Martha Phillips, PhD, MPH, MBA DHHS Division of Health Source: Behavioral Risk Factor Surveillance Survey 2001, 2002, 2003, 2004 In the 2005-2006 fiscal year, smokeless tobacco use was reported by 214 (4.7%) of the 4512 treatment seeking patients in the AR Stops treatment programs. The smokeless users included 161 men (75.2%) and 53 women (24.8%) with an average age of 40.0 years (range 13.7 to 85.8 years) and an average of 12.9 years of education. The men and women in this group were not significantly different in age or years of education.
39
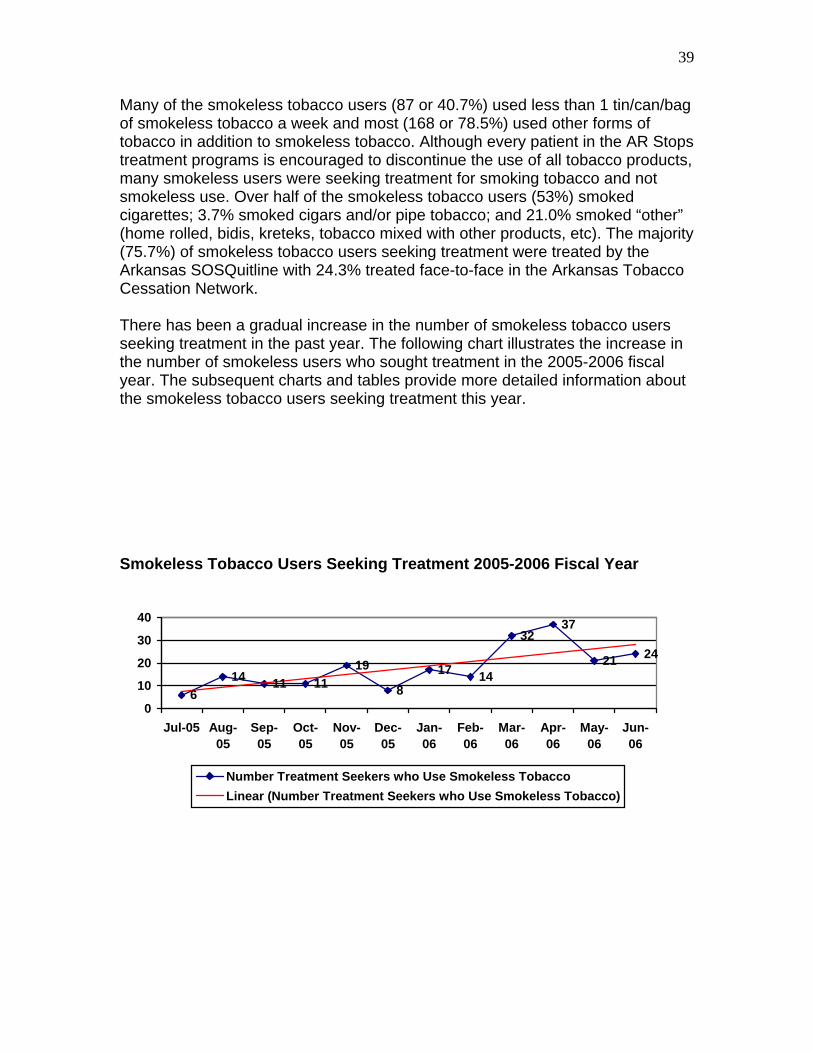
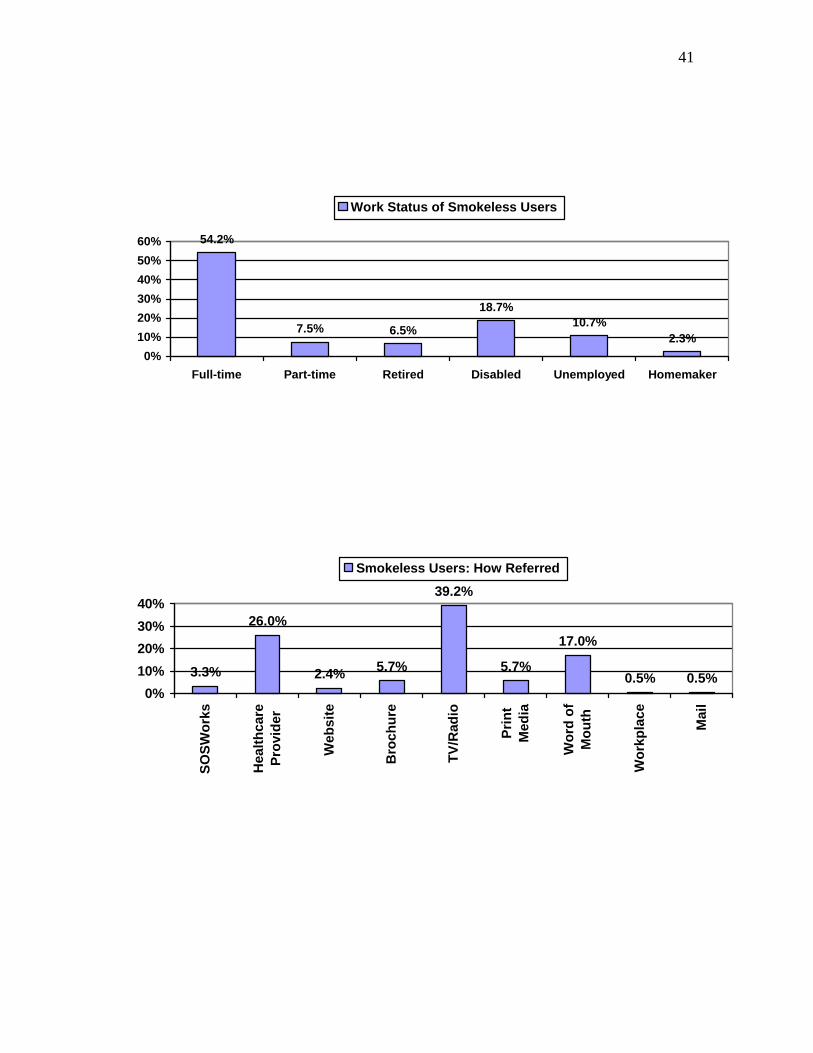
Many of the smokeless tobacco users (87 or 40.7%) used less than 1 tin/can/bag of smokeless tobacco a week and most (168 or 78.5%) used other forms of tobacco in addition to smokeless tobacco. Although every patient in the AR Stops treatment programs is encouraged to discontinue the use of all tobacco products, many smokeless users were seeking treatment for smoking tobacco and not smokeless use. Over half of the smokeless tobacco users (53%) smoked cigarettes; 3.7% smoked cigars and/or pipe tobacco; and 21.0% smoked “other” (home rolled, bidis, kreteks, tobacco mixed with other products, etc). The majority (75.7%) of smokeless tobacco users seeking treatment were treated by the Arkansas SOSQuitline with 24.3% treated face-to-face in the Arkansas Tobacco Cessation Network. There has been a gradual increase in the number of smokeless tobacco users seeking treatment in the past year. The following chart illustrates the increase in the number of smokeless users who sought treatment in the 2005-2006 fiscal year. The subsequent charts and tables provide more detailed information about the smokeless tobacco users seeking treatment this year. Smokeless Tobacco Users Seeking Treatment 2005-2006 Fiscal Year
614 11 11
19
817 14
3237
21 24
0
10
20
30
40
Jul-05 Aug-05
Sep-05
Oct-05
Nov-05
Dec-05
Jan-06
Feb-06
Mar-06
Apr-06
May-06
Jun-06
Number Treatment Seekers who Use Smokeless TobaccoLinear (Number Treatment Seekers who Use Smokeless Tobacco)
40
Ethnicity and Sex of Smokeless Tobacco Users Seeking Treatment
20.1%
11.7%
16.8%
11.2%
18.2% 19.2%
2.8%
0%
5%
10%
15%
20%
25%
<$10K $10-14,999 $15-24,999 $25-34,999 $35-49,999 >$50K Refused
Household Income of Smokeless Users
Male Female Total
White 67.3% 16.8% 84.1%
African-American 4.7% 7.5% 12.1%
Hispanic .5% 0% .5%
Asian/Pacific Islander 0% 0% 0%
American Indian 1.4% 0% 1.4%
Multi-ethnic or Other 1.4% .5% 1.9%
Total 75.2% 24.8%
41
54.2%
7.5% 6.5%
18.7%10.7%
2.3%0%
10%20%30%40%50%60%
Full-time Part-time Retired Disabled Unemployed Homemaker
Work Status of Smokeless Users
3.3%
26.0%
2.4% 5.7%
39.2%
5.7%
17.0%
0.5% 0.5%0%
10%20%30%40%
SOSW
orks
Hea
lthca
rePr
ovid
er
Web
site
Bro
chur
e
TV/R
adio
Prin
tM
edia
Wor
d of
Mou
th
Wor
kpla
ce
Mai
l
Smokeless Users: How Referred

42
AR Stops Treatment Outcomes for Smokeless Users
Of the 214 smokeless users that presented for treatment, as mentioned previously, most (78.2%) used other forms of tobacco. Abstinence 3-months and 6-months post-treatment was assessed for all forms of tobacco use. Of the 214 smokeless users, 126 were discharged during the 2005-2006 fiscal year; 29.3% had completed 5 out of the 6 sessions of treatment; and 41.1% were abstinent from tobacco at discharge. One-year follow-up data will be collected and reported, but too few have reached the one-year follow-up point at present since AR Stops began in July 2005. However, sufficient numbers have reached the 3-month and 6-month follow-up points to report the data below. 3-Month Follow-up Of the 126 discharged, 66 had been discharged for at least 3-months and were thus eligible for the 3-month follow-up assessment. Of those reached for follow-up, 18.2% were abstinent from all tobacco, 51.2% were abstinent from cigarettes, 69.0% were abstinent from smokeless tobacco, and 100% were abstinent from pipes, cigars, and other forms of tobacco. 6-Month Follow-up Of the 126 discharged, 36 were eligible for the 6-month follow-up assessment. Of those reached for follow-up, 11.1% were abstinent from all tobacco, 57.1% were abstinent from cigarettes, 60.0% were abstinent from smokeless tobacco, and 85.7% were abstinent from pipes, cigars, and other forms of tobacco. Conclusions The epidemiological evidence indicates that there has been an increase in the number of youth using smokeless tobacco products in Arkansas. Although the evidence to date has not shown an increase in regular use among adults, market data indicate that more smokeless products are being consumed. This may herald an increase in occasional usage that has not, as yet, developed into regular usage. In any event, the prevalence of smokeless tobacco use has not decreased while there is evidence to suggest that it will increase in the near future. Interestingly, the smokeless users who have presented for treatment are often those who experiment with other forms of tobacco as well, making treatment and the quitting process more complex. The AR Stops treatment programs treat all forms of tobacco use and see the use of smokeless tobacco and other forms of tobacco as important emerging threats. No quantity or form of tobacco use is without risk.