central dopaminergic signaling agents
TRANSCRIPT
A. Michael Cridler, Marcelo J. Nieto, and Kenneth A
Witt
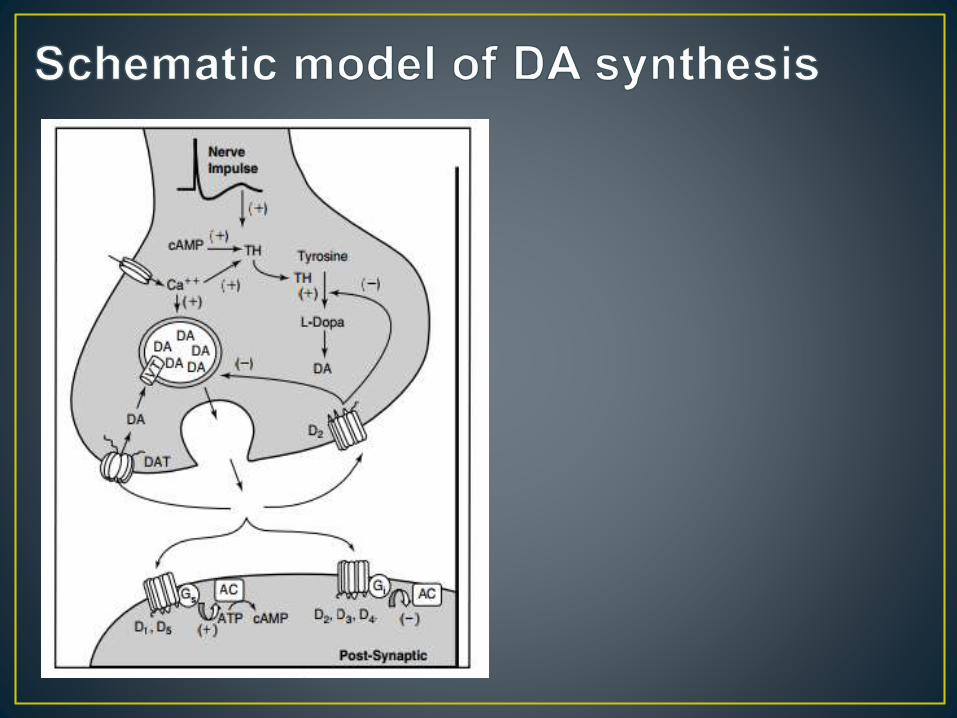
- CNS neurotransmitter controlling emotion, movement, reward mechanism, and metabolic precursor of norepinephrine and epinephrine
( C9H11NO3)
- is a nonessential amino acid the body makes fromanother amino acid called phenylalanine. It is a buildingblock for several important brain chemicals calledneurotransmitters, including epinephrine, norepinephrine,and dopamine. Neurotransmitters help nerve cellscommunicate and influence mood. Tyrosine also helpsproduce melanin, the pigment responsible for hair andskin color. It helps in the function of organs responsiblefor making and regulating hormones, including theadrenal, thyroid, and pituitary glands. It is involved in thestructure of almost every protein in the body.

1. NIGROSTRIAT PATHWAY
- involve in the production of movements
(tremors and muscle rigidity)
2. MESOCORTICAL PATHWAY
- motivation and emotional response
3. MESOLIMBIC PATHWAY
- pleasure and reward behaviour
- heavily implicated in addiction
4. TUBEROHYPOPHYSEAL PATHWAY
- regulation of prolactin
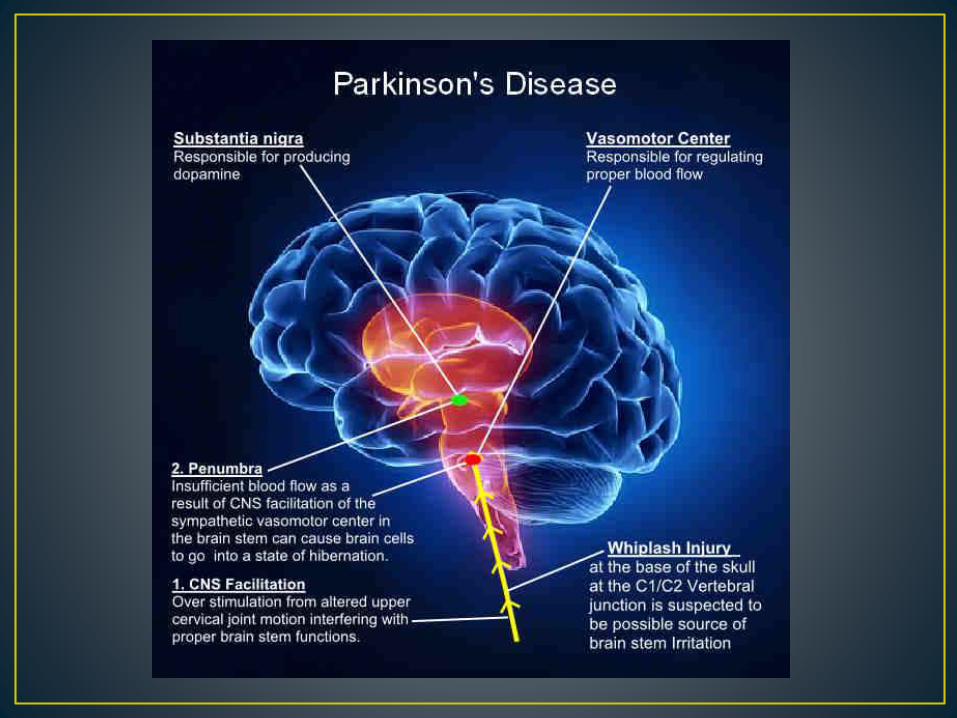
- it is a progressive neurodegenerative
illness characterized by tremor, muscular
rigidity, bradykinesia and postural imbalance.
LEVODOPA is a metabolic precursor of
dopamine. Dopamine itself does not cross the
blood-brain barrier, but its immediate
precursor, Levodopa, is actively transported
into the CNS and is converted to dopamine in
the brain. Large doses of levodopa are
required, because much of the drug is
decarboxylated to dopamine in periphery,
resulting nausea, vomiting, cardiac
arrhythmias and hypotension.
• CARBIDOPA diminishes the metabolism of
levodopa in the GI tract and peripheral
tissues; thus, increases the availability of
levodopa to the CNS.
• Addition of carbidopa lowers the dose of
levodopa needed by FOUR-TO-FIVE FOLD,
and decreases the side effects.
1. Levodopa, USP (S)-2-amino-3-(3,4-
dihydroxyphenyl) propanoic acid
- white/almost white crystalline powder
- slightly soluble in water, acidic and basic
solution
- insoluble in alcohol, chloroform, and
ether
- pKa=9.9 and 11.8
2. Carbidopa, USP (S)-3-(3,4-
dihydroxyphenyl)-2-hydrazyl-2
- white crystalline powder
- slightly soluble in water
- pKa = 7.8
- metabolized into a-methyl-3-methoxy-4-
hydroxyphenylpropionic acid and a-methyl-3,4-
dihydroxyphenylpropionic acid.
- Are utilized to prolong the plasma half-life of levodopa or block the striatal metabolism of DA.
Selegiline an irreversible MAO-B inhibitor potentiates levodopa by blocking its metabolism by MAO and improve the “wearing-off” effect of levodopa.
Rasagiline is five times more potent than selegiline.
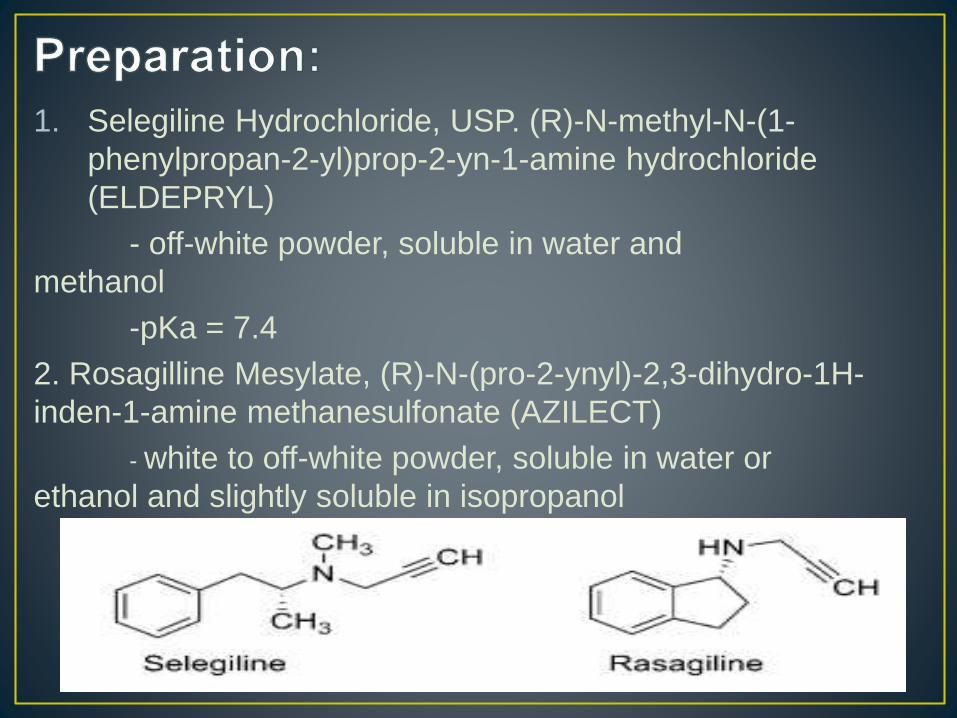
1. Selegiline Hydrochloride, USP. (R)-N-methyl-N-(1-
phenylpropan-2-yl)prop-2-yn-1-amine hydrochloride
(ELDEPRYL)
- off-white powder, soluble in water and
methanol
-pKa = 7.4
2. Rosagilline Mesylate, (R)-N-(pro-2-ynyl)-2,3-dihydro-1H-
inden-1-amine methanesulfonate (AZILECT)
- white to off-white powder, soluble in water or
ethanol and slightly soluble in isopropanol
a. Pergolide- binds at D2-type and 5-HT2B
receptor and is withdrawn in the market because
it induce valvular heart disease by acting 5-HT2B
receptor
b. Carbegoline- binds at D2-like receptors, 5-
HT2A and 5-HT2B receptors. In US, tx for
hyperprolactinemia and tx for PD in other
countries.
c. Bromocriptine- agonist at D2-like receptors,
antagonist in D1-like receptors and exhibits less
1. Bromocriptine Mesylate, USP (6aR,9R)-5-bromo-N-((2R,5S,10aS,10bS0-10b-hydroxy-5-isobutyl-2-isopropyl-3,6-dioxooctahydro-2H-oxazolo[3,2a]pyrrolo[2,1c]pyrazin-2-yl)-7-methyl-4,6,6a,7,8,9-hexahydroindolo[4,3-fg]quinoline-9-carboxamide methanesulfonate (PARLODEL)
- white solid, soluble in ethanol and water
- pKA = 6.6 and 15, half-life 0.3 hours
2. Carbigoline, (6aR,9R,10aR)-7-allyl-N-(3-(dimethylamino)propyl)-N-(ethylcarbomoyl)-4,6,6a, 7,8,9,10a-octahydroindolo[4,3-fg]quinoline-9-carboxamide (DOSTINEX)
- white powder, soluble in alcohol, chloroform, and N,N-dimethylformamide, insoluble in water
a. Pramipexole- D2 and D3 agonist but no
appreciable affinity for D1, D5, 5-HT2A, and 5-
HT2B
b. Ropinirole- low affinity to 5-HT2A, 5-HT2B, and
D1-like receptors.
Preparations:
1. Apomorphine Hydrochlorite, USP (6aR)-6-methyl-
5,6,6a,7-tetrahydro-4H-dibenzo[de,g]quinolone-
10,11-diol hydrochloride (APOKYN)
-white or off-white powder or crystal soluble in
hot water
- pKa = 8.92
2. Pramipexole Dihydrochloride, (S)-2-amino-6-propylamino-dihydrochloride (MIRAPEX)
- white to off-white powder soluble in water, slightly soluble in methanol and
ethanol, and insoluble in dichloromethane
-tx signs and symptoms of idiopathic PD and restless leg syndrome (RLS), alone or
with combination with levodopa.
3. Ropinirole Hydrochloride, 4-(2-(dipropylamino) ethyl)indolin-2-one hydrochloride (REQUIP)
- white to pale greenish yellow powder, very soluble to water
- t1/2= 3 hrs , tx RLS
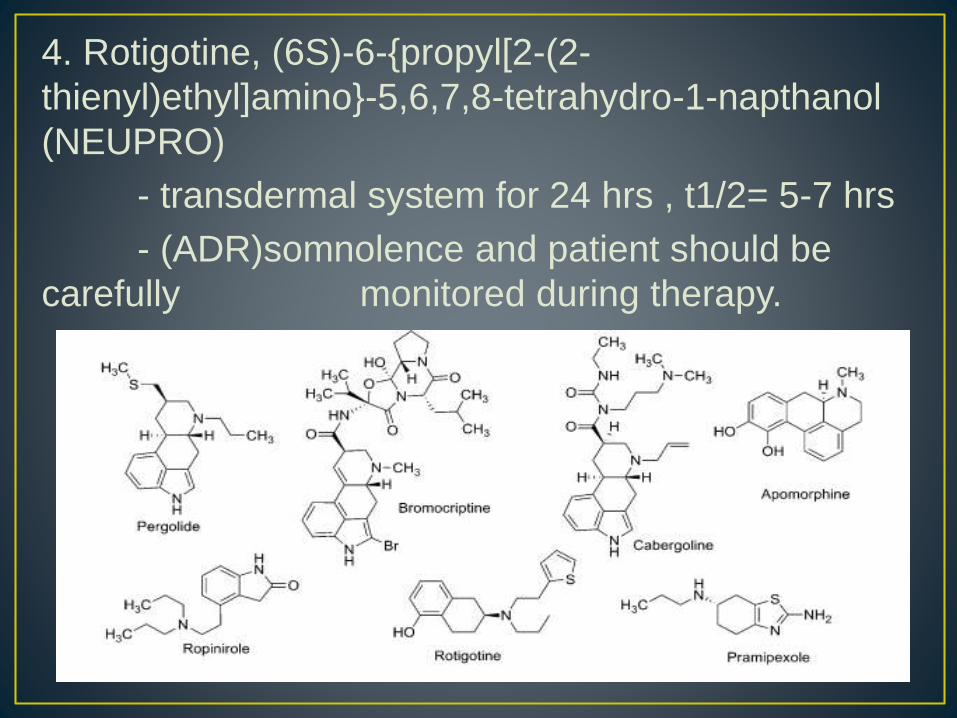
4. Rotigotine, (6S)-6-{propyl[2-(2-
thienyl)ethyl]amino}-5,6,7,8-tetrahydro-1-napthanol
(NEUPRO)
- transdermal system for 24 hrs , t1/2= 5-7 hrs
- (ADR)somnolence and patient should be
carefully monitored during therapy.
- Tx for early-stage PD
• Catechol O-methyltransferase (COMT) inhibitors allow a larger amount of levodopa to reach the brain, which raises dopamine levels there. They help provide a more stable, constant supply of levodopa, which makes its beneficial effects last longer.
• COMT inhibitors are always taken in combination with levodopa. They do not have any effect on Parkinson's disease symptoms by themselves.
Entacaptone- - does not penetrate BBB
- - only inhibits peripheral COMT
- - less motor fluctuations in combine with carbidopa
- - lack of toxicity

Preparation:
1. Tolcapone, 3,4-
dihydroxy-4’methyl-5-
nitrobenzophenone
(TASMAR)
- yellow, odorless,
nonhygroscopic,
crystalline
- pKA = 4.78
2. Entacapone, (E)-2-
cyano-3-(3,4-dihydroxy-5-
nitrophenyl)-N,N-diethyl-2-
propenamide (COMTAN)
- insoluble in water (pKA= 4.50)
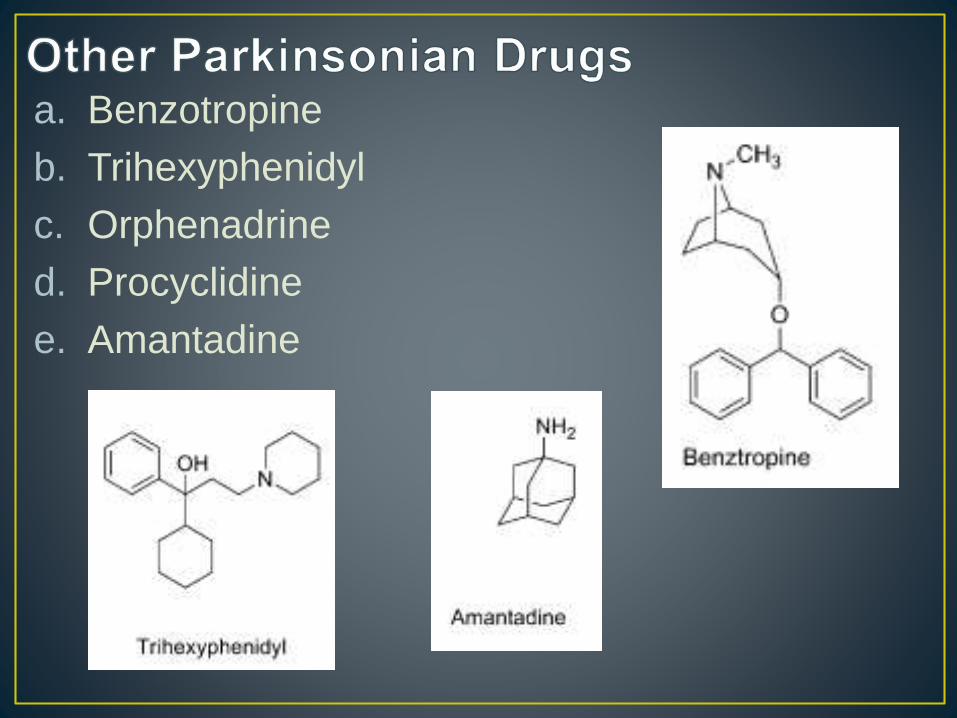
a. Benzotropine
b. Trihexyphenidyl
c. Orphenadrine
d. Procyclidine
e. Amantadine
Schizophrenia is a mental disorder caused by
some inherent dysfunction of the brain
characterized by delusions, abnormal behaviour,
hallucinations and thought disorders (positive
symptoms), as well as loss of normal emotions,
abilities, and motivation (negative symptoms).
- a.k.a First-generation, Conventional antipsychotics, Classical antipsychotics, Classical neuroleptics, Major tranquilizers
E.g
- Phenothiazines, Thioxanthenes, Butyrophenones, Diphenylbutylpiperidines, Dihydroindolones (MALDONE)
HIGH
- Haloperidol
- Fluphenazine
LOW
- Chlorpromazine
PHENOTHIAZINE
- (1876) by Badische Anilin und Soda Fabrik
(BASF) chemist, H. Caro and A Bernstein (1883)
High-Potency
Typical
Antipsychotics
- More EPS
- Less histaminic
(sedation),
alpha
adrenergic
(orthostasis),
and
anticholinergic
(dry mouth)
effect
Low-Potency Typical
Antipsychotics
- Less EPS but
more H1, a1, and
muscarinic side
effects
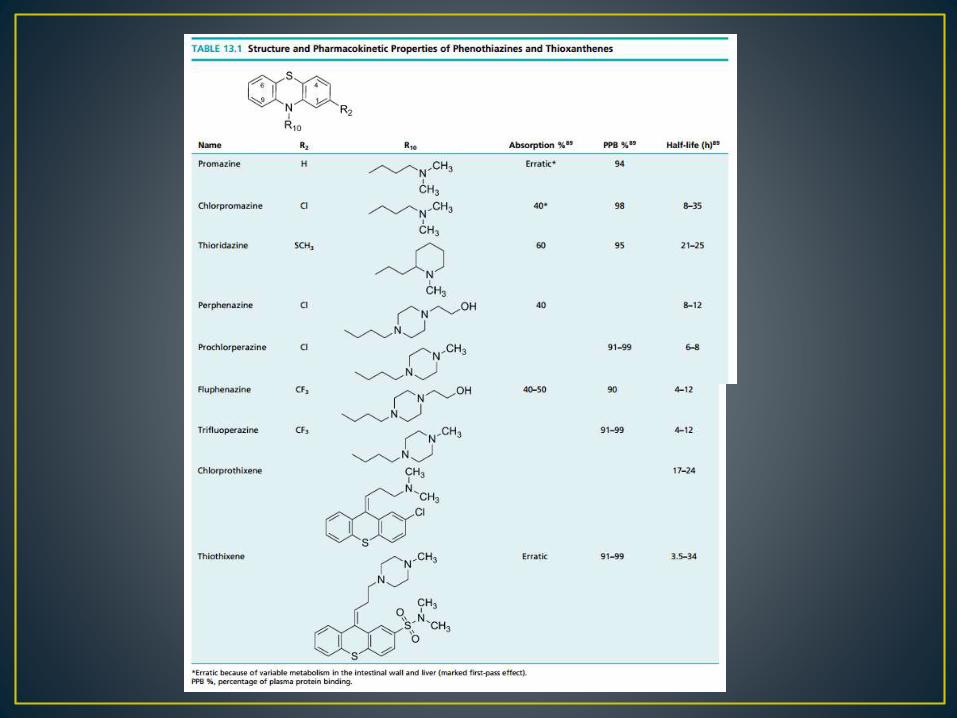
PHENOTHIAZINE
- Chlorpromazine
THIOXANTHENES
- Less likely to form
phenolic metabolites
1. Chlorpromazine Hydrochloride, USP 2-chloro-10-[3-(dimethylamino)propyl]phenothiazine (THORAZINE)
- White to slightly creamy white, odourless, bitter tasting, crystalline powder
- pKa= 9.43
- Minor substrate of CYP1A2 and 3A4, major CYP2D6
- Strong inhibitor of CYPD2D6 weak CYP2E1
- Strong anticholinergic, sedative and potent antiemetic
- EPS is low
- Tx nausea, vomiting, hiccups, porphyria, preoperative sedation, psychotic disorders
2. Thioridazine Hydrochloride, USP 10-[2-(1-methyl-2-piperidyl)ethyl]-2-(methylthio)phenothiazine (MELLARIL)
- White to slightly yellow, crystalline or micronized powder, odourless, insoluble in H2O and dehydrated alcohol.
- pKa= 9.66
- Low EPS and less antiemetic activity
- Tx of schizophrenic patients who fail to respond adequately to treatment with other antipsychotic drugs
3. Perphenizine, USP 2-[4-[3-(2-chloro-10H-phenothiazin-10-yl)propyl]piperazin-1-yl]ethanol
- Control of severe nausea and vomiting in adults
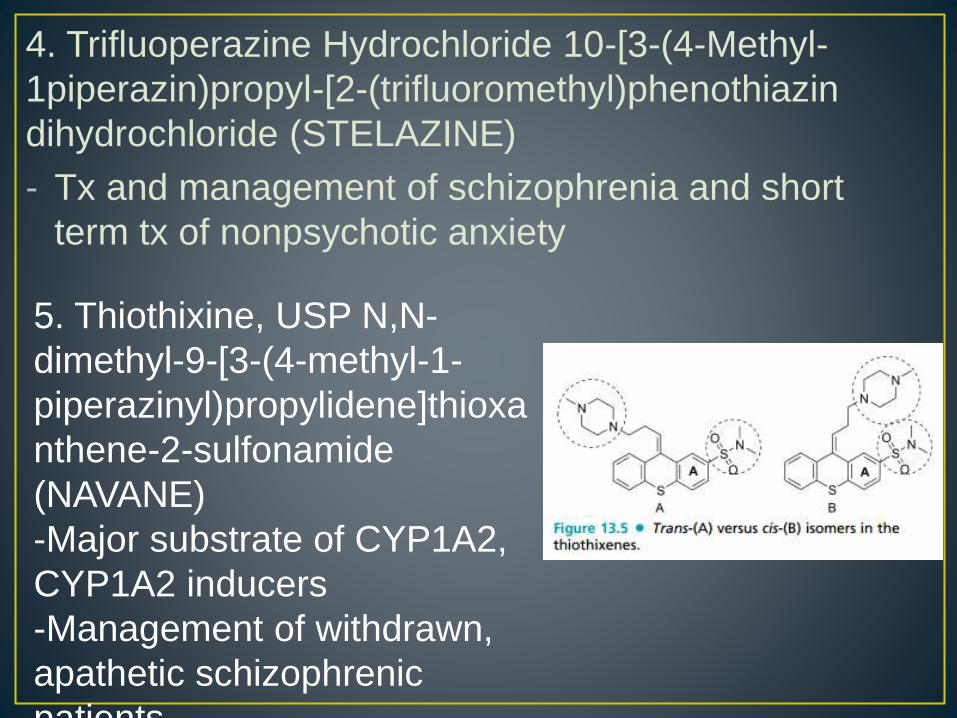
4. Trifluoperazine Hydrochloride 10-[3-(4-Methyl-
1piperazin)propyl-[2-(trifluoromethyl)phenothiazin
dihydrochloride (STELAZINE)
- Tx and management of schizophrenia and short
term tx of nonpsychotic anxiety
5. Thiothixine, USP N,N-
dimethyl-9-[3-(4-methyl-1-
piperazinyl)propylidene]thioxa
nthene-2-sulfonamide
(NAVANE)
-Major substrate of CYP1A2,
CYP1A2 inducers
-Management of withdrawn,
apathetic schizophrenic
patients
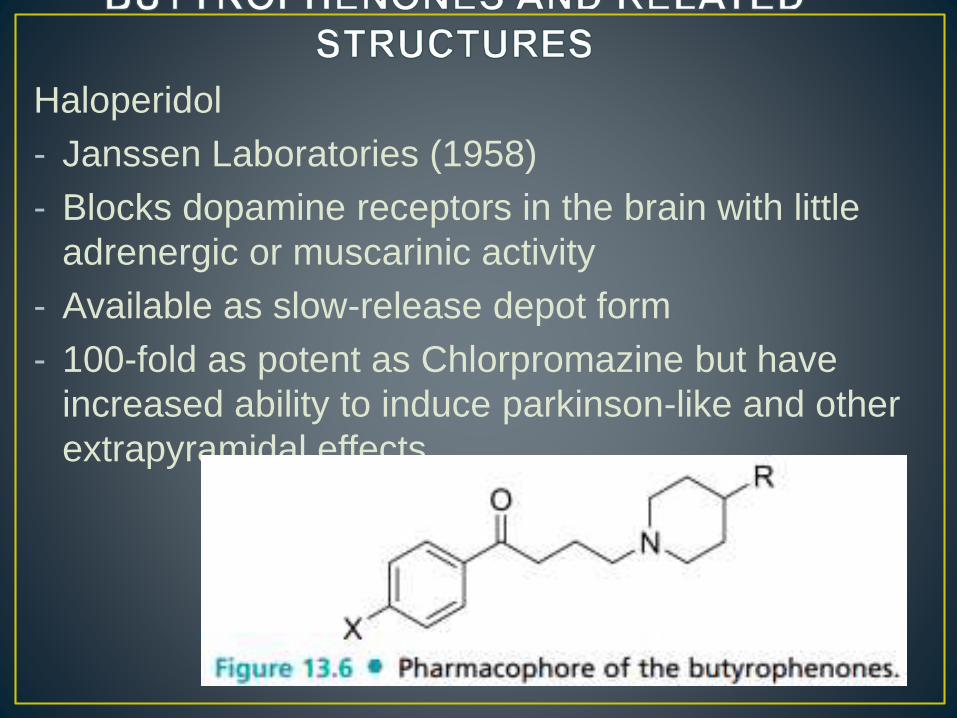
Haloperidol
- Janssen Laboratories (1958)
- Blocks dopamine receptors in the brain with little
adrenergic or muscarinic activity
- Available as slow-release depot form
- 100-fold as potent as Chlorpromazine but have
increased ability to induce parkinson-like and other
extrapyramidal effects
1. Haloperidol, USP 4-[4-(p-chlorophenyl)-4-
hydroxypiperidinol]-4-flourobutyrophenone
(HALDOL)
- Odorless white to yellow crystalline powder
- Rapidly absorbed with high bioavailability
- Excreted slowly in urine and feces
- Long term tx of psychosis and specially useful to
patients who are noncompliant with their drug
treatment
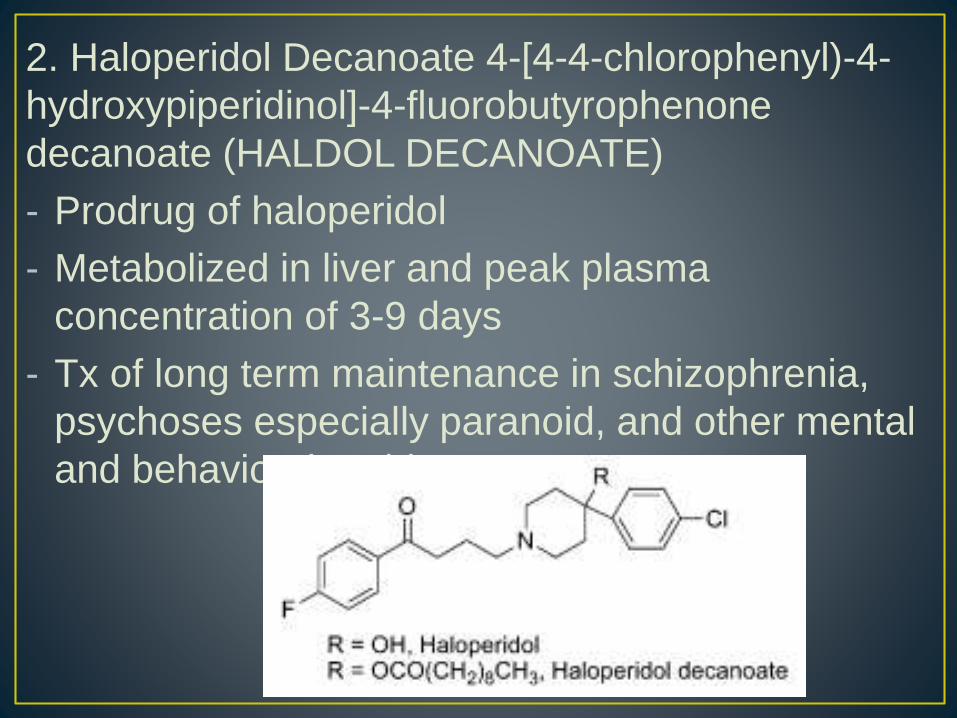
2. Haloperidol Decanoate 4-[4-4-chlorophenyl)-4-
hydroxypiperidinol]-4-fluorobutyrophenone
decanoate (HALDOL DECANOATE)
- Prodrug of haloperidol
- Metabolized in liver and peak plasma
concentration of 3-9 days
- Tx of long term maintenance in schizophrenia,
psychoses especially paranoid, and other mental
and behavioral problems
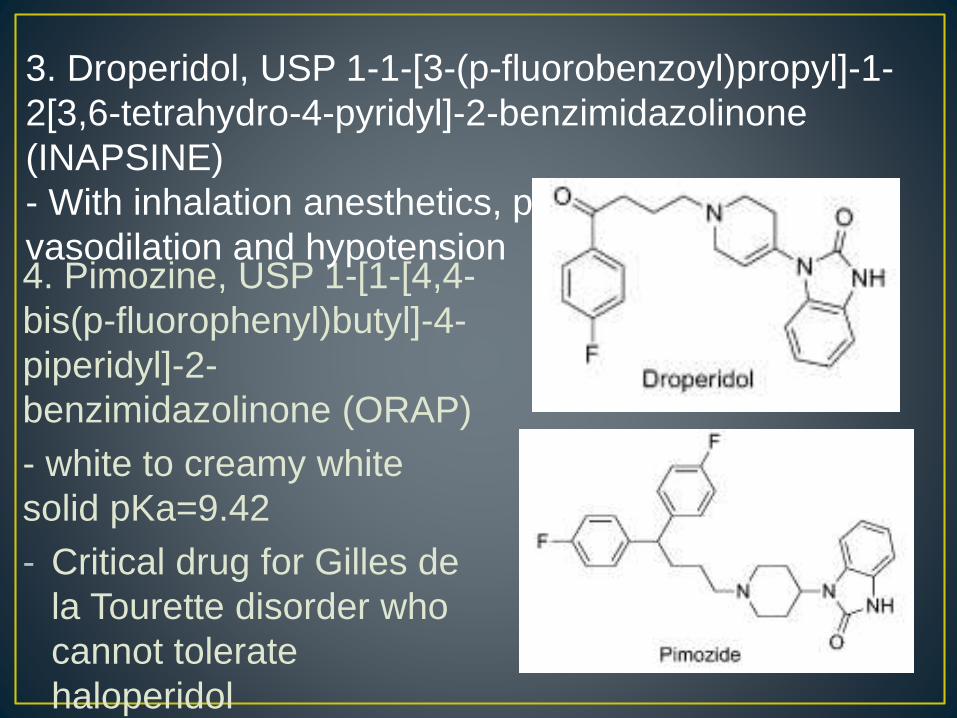
4. Pimozine, USP 1-[1-[4,4-
bis(p-fluorophenyl)butyl]-4-
piperidyl]-2-
benzimidazolinone (ORAP)
- white to creamy white
solid pKa=9.42
- Critical drug for Gilles de
la Tourette disorder who
cannot tolerate
haloperidol
3. Droperidol, USP 1-1-[3-(p-fluorobenzoyl)propyl]-1-
2[3,6-tetrahydro-4-pyridyl]-2-benzimidazolinone
(INAPSINE)
- With inhalation anesthetics, produce peripheral
vasodilation and hypotension
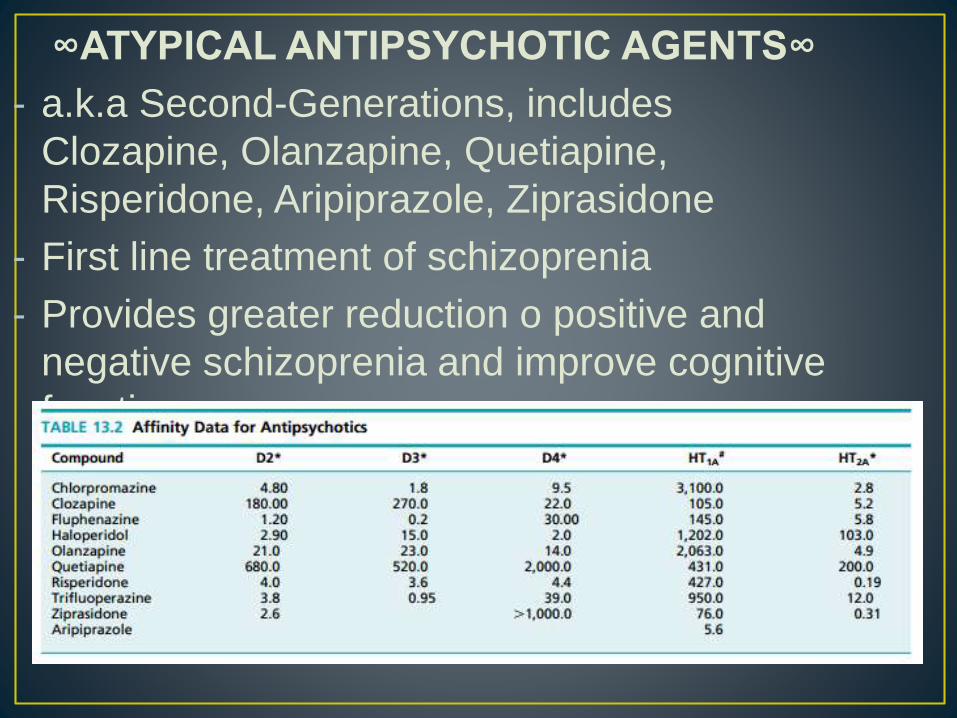
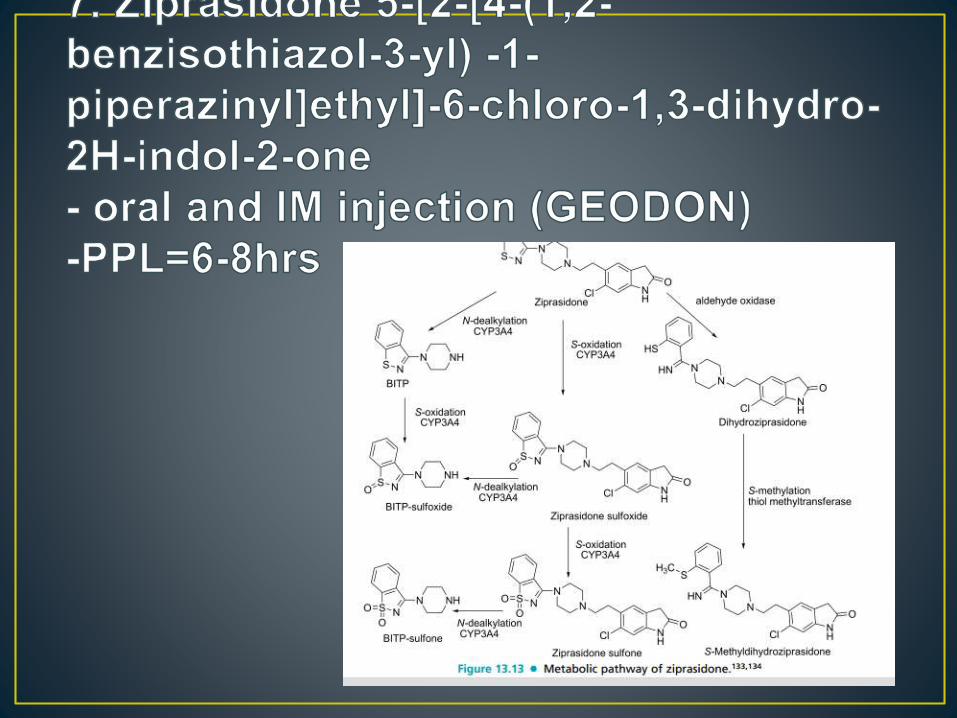
∞ATYPICAL ANTIPSYCHOTIC AGENTS∞
- a.k.a Second-Generations, includes
Clozapine, Olanzapine, Quetiapine,
Risperidone, Aripiprazole, Ziprasidone
- First line treatment of schizoprenia
- Provides greater reduction o positive and
negative schizoprenia and improve cognitive
function
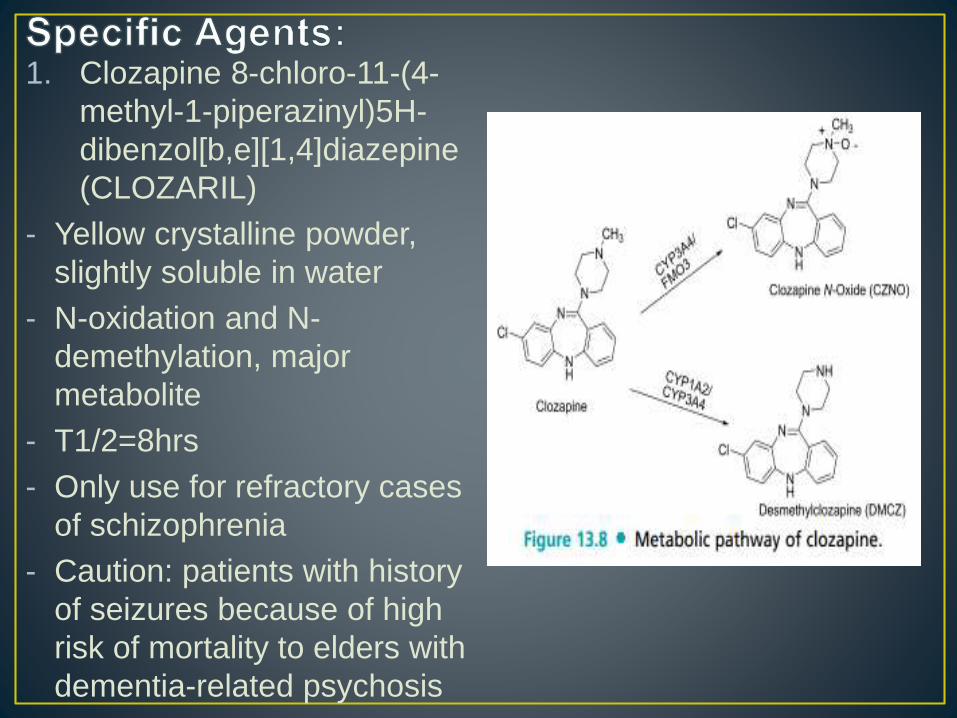
1. Clozapine 8-chloro-11-(4-
methyl-1-piperazinyl)5H-
dibenzol[b,e][1,4]diazepine
(CLOZARIL)
- Yellow crystalline powder,
slightly soluble in water
- N-oxidation and N-
demethylation, major
metabolite
- T1/2=8hrs
- Only use for refractory cases
of schizophrenia
- Caution: patients with history
of seizures because of high
risk of mortality to elders with
dementia-related psychosis
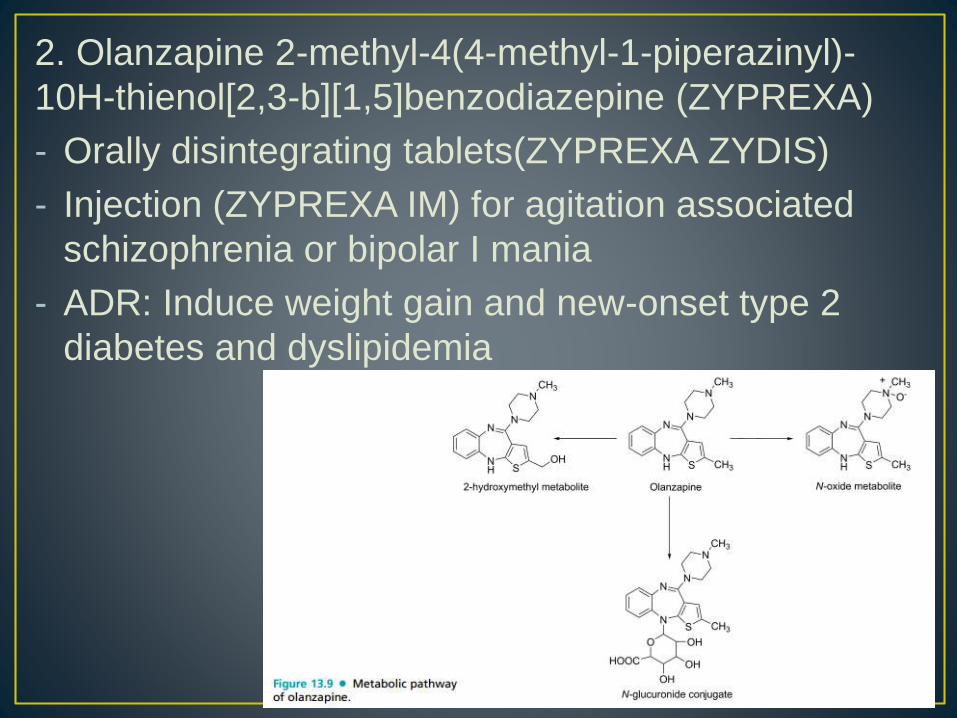
2. Olanzapine 2-methyl-4(4-methyl-1-piperazinyl)-
10H-thienol[2,3-b][1,5]benzodiazepine (ZYPREXA)
- Orally disintegrating tablets(ZYPREXA ZYDIS)
- Injection (ZYPREXA IM) for agitation associated
schizophrenia or bipolar I mania
- ADR: Induce weight gain and new-onset type 2
diabetes and dyslipidemia
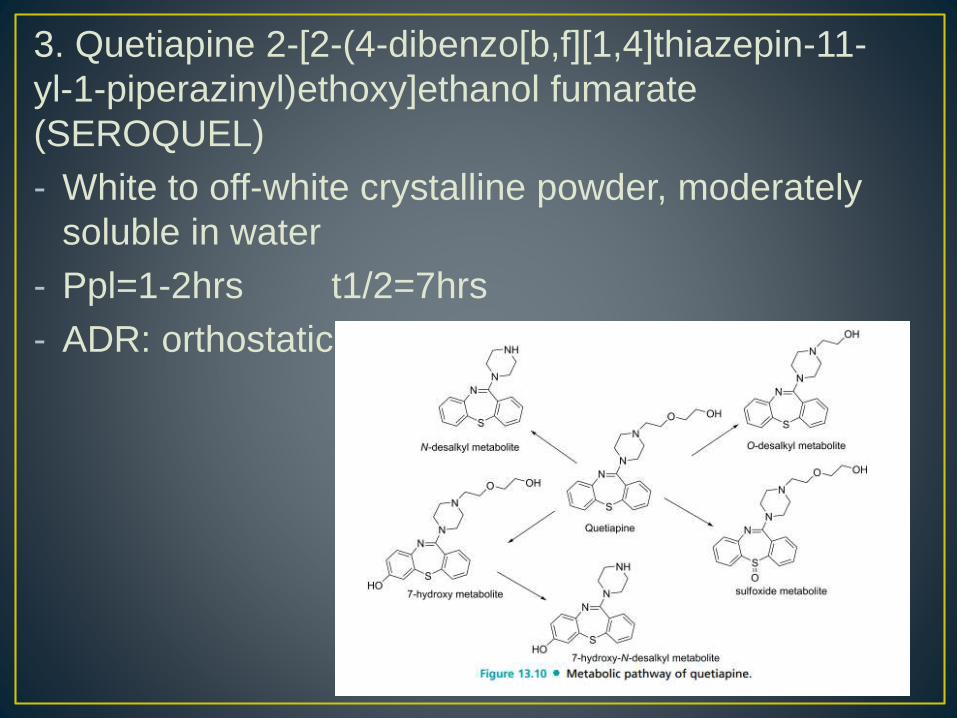
3. Quetiapine 2-[2-(4-dibenzo[b,f][1,4]thiazepin-11-
yl-1-piperazinyl)ethoxy]ethanol fumarate
(SEROQUEL)
- White to off-white crystalline powder, moderately
soluble in water
- Ppl=1-2hrs t1/2=7hrs
- ADR: orthostatic hypotension and somnolence
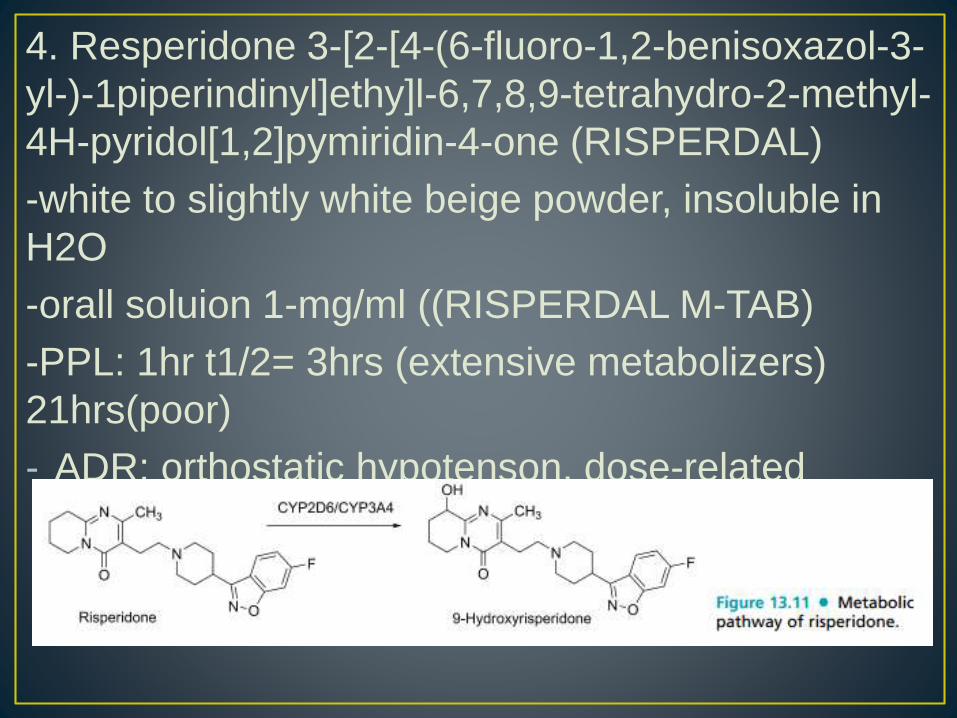
4. Resperidone 3-[2-[4-(6-fluoro-1,2-benisoxazol-3-
yl-)-1piperindinyl]ethy]l-6,7,8,9-tetrahydro-2-methyl-
4H-pyridol[1,2]pymiridin-4-one (RISPERDAL)
-white to slightly white beige powder, insoluble in
H2O
-orall soluion 1-mg/ml ((RISPERDAL M-TAB)
-PPL: 1hr t1/2= 3hrs (extensive metabolizers)
21hrs(poor)
- ADR: orthostatic hypotenson, dose-related
hyperprolactinemia, mild weight gain, EPS,
insomia
5. Paliperidone (±)-3-[2-[4-(6-fluoro-1,2-
benzisoxazol-3-yl)-1piperidinyl]ethyl]-6,7,8,9-
tetrahydro-9-hydroxy-2-methyl,4H-pyridol[1,2-
a]pyrimidin-4-one (INVEGA)
- Insoluble in water, extended release tablet
- T1/2= 23hrs
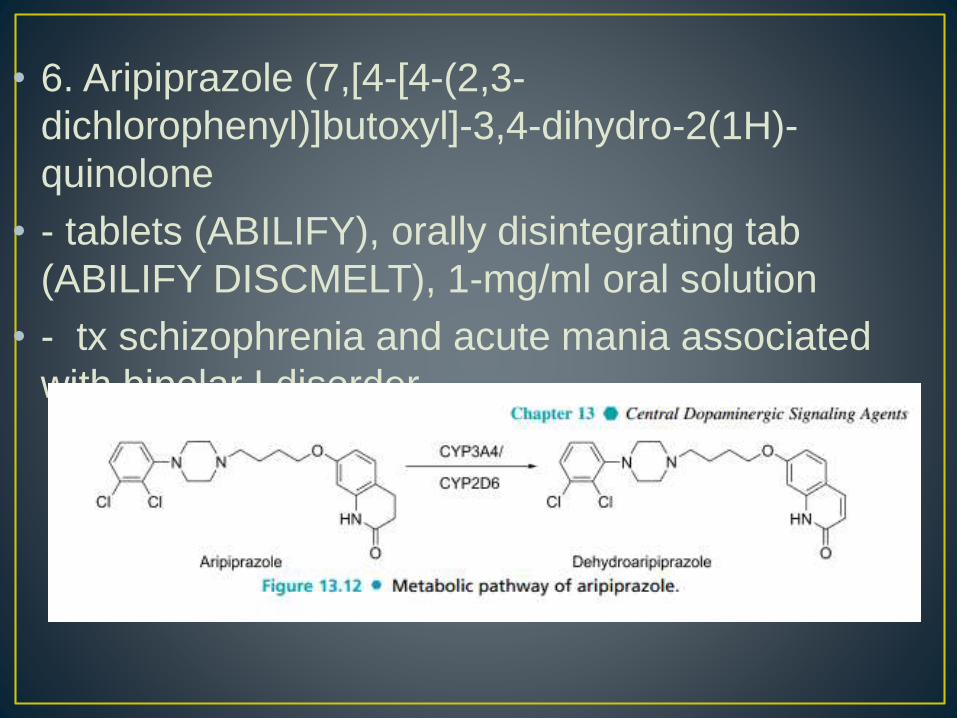
• 6. Aripiprazole (7,[4-[4-(2,3-
dichlorophenyl)]butoxyl]-3,4-dihydro-2(1H)-
quinolone
• - tablets (ABILIFY), orally disintegrating tab
(ABILIFY DISCMELT), 1-mg/ml oral solution
• - tx schizophrenia and acute mania associated
with bipolar I disorder