central line-associated bloodstream infections (clabsi) · bloodstream infections (bsis) and device...
TRANSCRIPT
Central Line-Associated
Bloodstream Infections
(CLABSI)
LEARNING OBJECTIVES:
• After this course, you should be able to:
• Describe the scope of the problem of CLABSI
• Review the structure of Device-associated Infections using NHSN criteria and the
surveillance methodology used for data collection
• Define key terms and protocol used for collecting CLABSIs and their corresponding
denominator data
• Become familiar with the different types of central lines and sources of contamination
• Differentiate between CLABSI and MBI-LCBI criteria
• Describe how to collect CLABSI data using the BSI form
• Describe how CLABSI rates, device utilization ratios, and standardized infection ratios
are calculated and reported to promote performance improvement
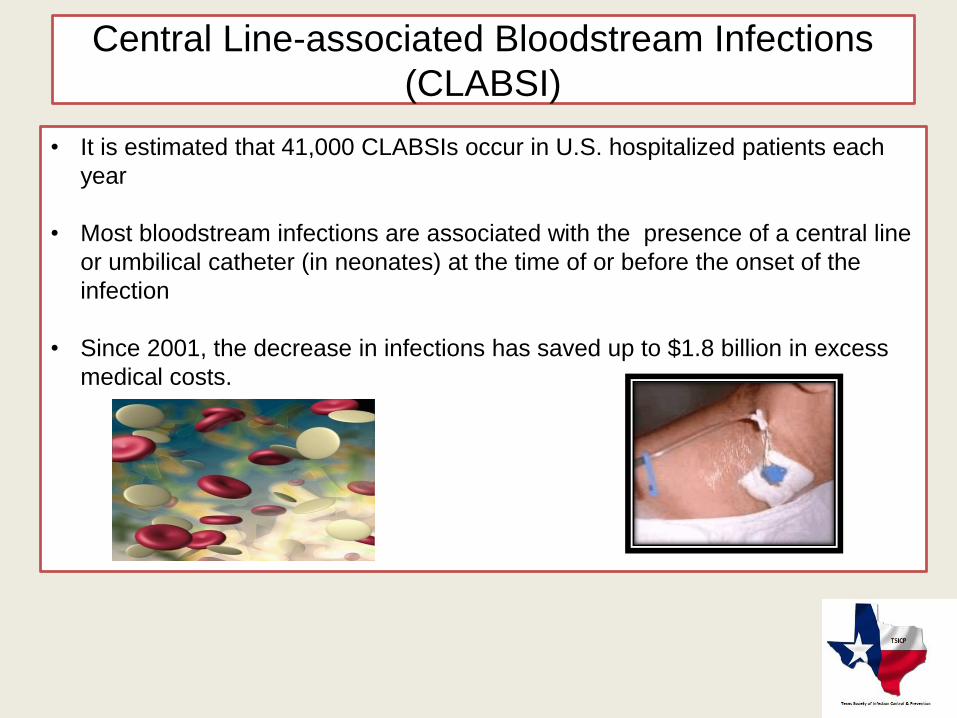
Central Line-associated Bloodstream Infections
(CLABSI)
• It is estimated that 41,000 CLABSIs occur in U.S. hospitalized patients each
year
• Most bloodstream infections are associated with the presence of a central line
or umbilical catheter (in neonates) at the time of or before the onset of the
infection
• Since 2001, the decrease in infections has saved up to $1.8 billion in excess
medical costs.
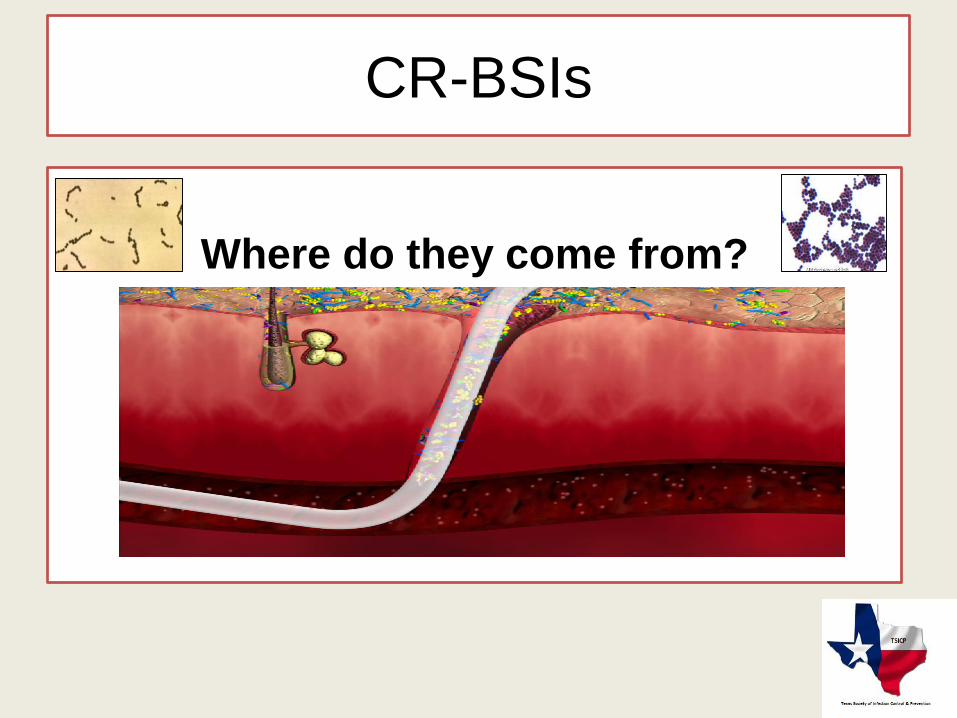
CR-BSIs
Where do they come from?
Bloodstream Infections (BSIs) and
Device Use
87% of BSIs are associated with device use1
Common devices:
– Central venous catheters (CVCs)– Arterial catheters– Peripherally inserted central catheters (PICCs)– Dialysis catheters and ports– Peritoneal dialysis catheters– Epidural catheters– External fixator pins
1. Richards M, Edwards J, Culver D, Gaynes R. Nosocomial infections in medical intensive care units in the United States. National Nosocomial Infections Surveillance System. Critical Care Medicine. 1999;27:853-854.
Evidence-based Choice for Catheter-related Bloodstream Infection (CR-BSI) Prevention- William R. Jarvis, M.D.
An intravascular catheter that terminates at or close to the heart or in one of the great
vessels which is used for infusion, withdrawal of blood, or hemodynamic monitoring
Examples of Central Lines includes the following:
• Aorta
• Pulmonary artery
• Superior vena cava Inferior vena cava
• Brachiocephalic veins Internal jugular veins
• Subclavian veins External iliac veins
• Common iliac veins
• Femoral veins
• In neonates, the umbilical artery/vein
REMINDER: Femoral Arteries are NOT great vessels.
Central Lines
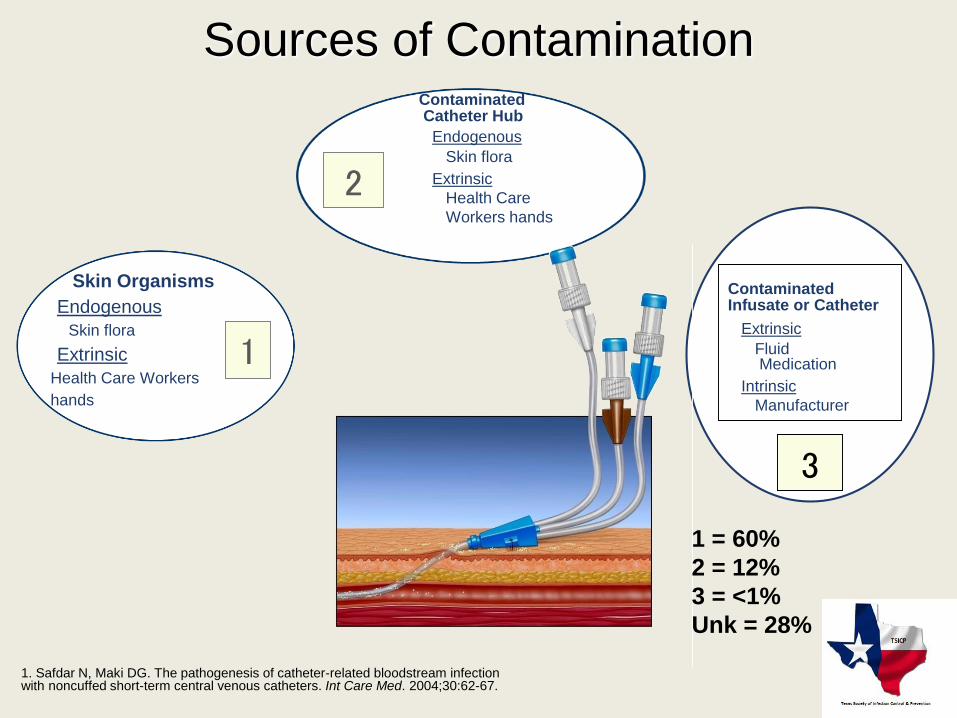
Sources of Contamination
1
Skin Organisms
Endogenous
Skin flora
Extrinsic
Health Care Workers
hands
ContaminatedCatheter Hub
Endogenous
Skin flora
Extrinsic
Health Care
Workers hands
2
3
ContaminatedInfusate or Catheter
Extrinsic
FluidMedication
Intrinsic
Manufacturer
1 = 60%
2 = 12%
3 = <1%
Unk = 28%
1. Safdar N, Maki DG. The pathogenesis of catheter-related bloodstream infection with noncuffed short-term central venous catheters. Int Care Med. 2004;30:62-67.
Biofilm
• Biofilm is a complex, highly organized community of microorganisms enclosed in a self-produced exopolysaccharide matrix attached to tissue or inanimate surfaces.1
• All medical-device-related infections originate as biofilm infections.
• Bacteria in a biofilm are chemically and physically protected by the biofilm structure and are also slow growing and are difficult to kill with antimicrobial therapies
1. Ryder, MA. Catheter-Related Infections: It's All About Biofilm. Topics in Advanced Practice Nursing eJournal. 2005;5(3) ©2005 Medscape
Posted 08/18/2005 . http://www.medscape.com/viewarticle/508109
What we can do to prevent CR-BSIs?
Site checks every shiftVisual inspection of the CVC insertion site
CVC dressing, and the CVC itself at the
start of each shift can help prevent future
complications.
WHAT TO LOOK FOR:
1- Is the dressing clean, dry, intact, & dated?
2- Is the dressing due to be changed?
3-How does the skin integrity under & around the dressing look?
4-Is the catheter in the same position as documented at time of insertion?
5-Are all ports of the CVC in working order? Do they flush easily and draw briskly?
What we can do to prevent CR-BSIs?
Good shift to shift communication
Communicate:
1-Your site check observations.
2-Dressing, tubing, or cap changes you may have performed.
3-Any patient complaints, questions, or concerns.
4-Any tests or procedures that may utilized the patient’s CVC.
5-Any interventions you may have performed, such as a CXR or line de-clot.
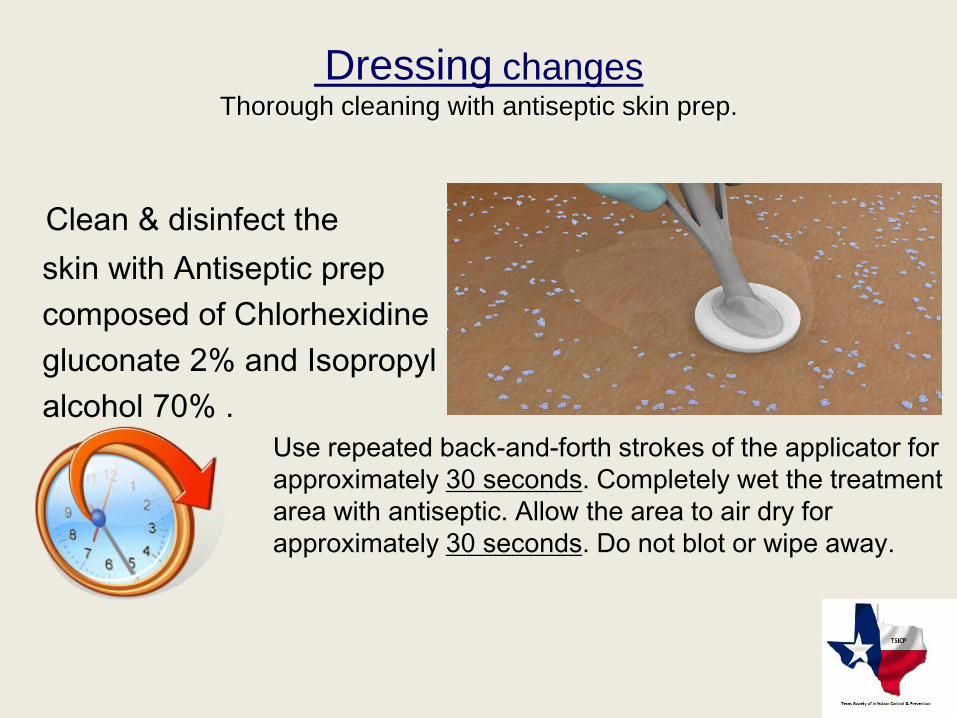
Dressing changesThorough cleaning with antiseptic skin prep.
Clean & disinfect the
skin with Antiseptic prep
composed of Chlorhexidine
gluconate 2% and Isopropyl
alcohol 70% .
Use repeated back-and-forth strokes of the applicator for
approximately 30 seconds. Completely wet the treatment
area with antiseptic. Allow the area to air dry for
approximately 30 seconds. Do not blot or wipe away.
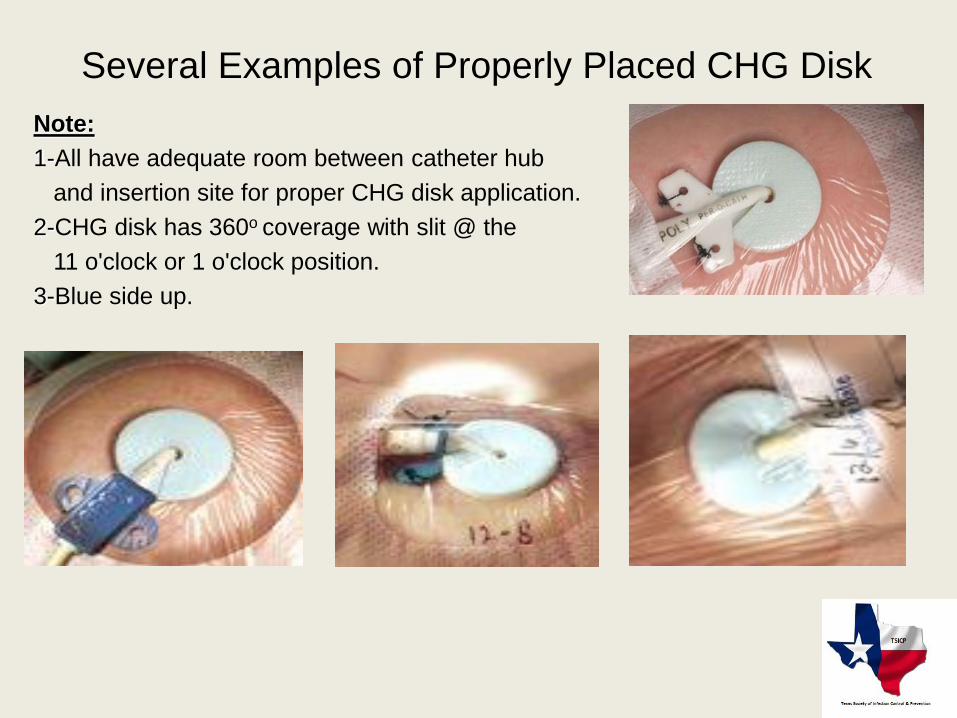
Several Examples of Properly Placed CHG Disk
Note:
1-All have adequate room between catheter hub
and insertion site for proper CHG disk application.
2-CHG disk has 360o coverage with slit @ the
11 o'clock or 1 o'clock position.
3-Blue side up.
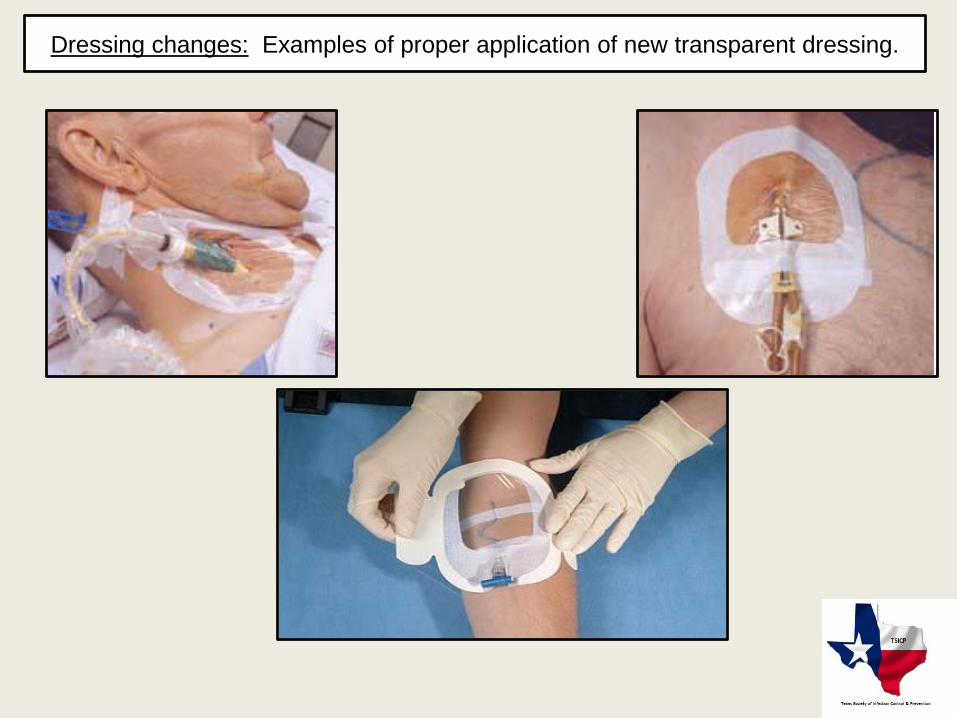
Dressing changes: Examples of proper application of new transparent dressing.
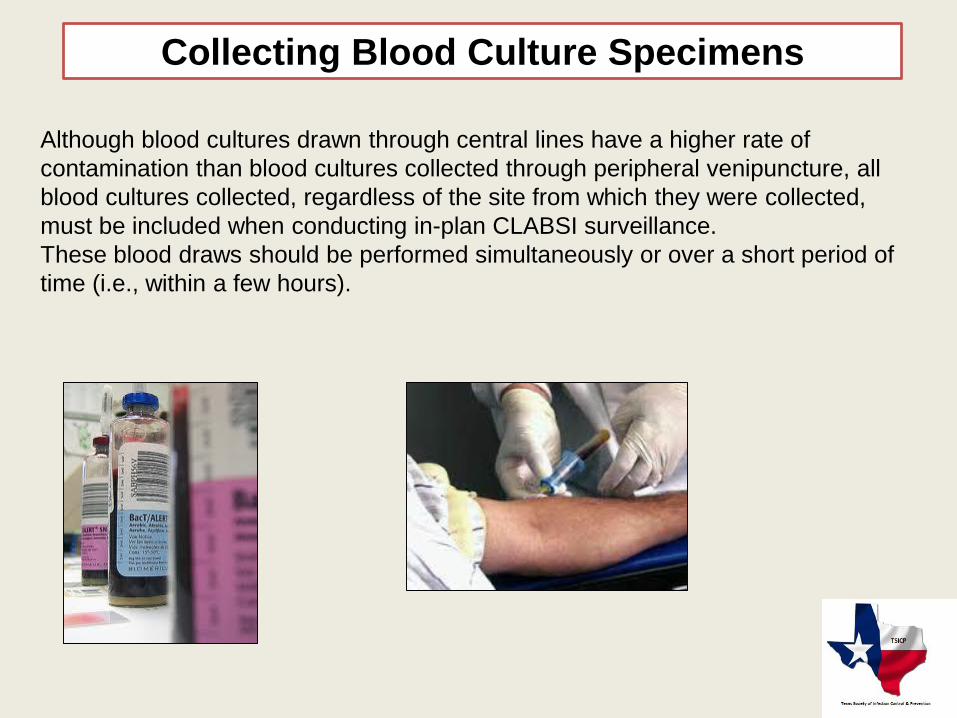
Collecting Blood Culture Specimens
Although blood cultures drawn through central lines have a higher rate of
contamination than blood cultures collected through peripheral venipuncture, all
blood cultures collected, regardless of the site from which they were collected,
must be included when conducting in-plan CLABSI surveillance.
These blood draws should be performed simultaneously or over a short period of
time (i.e., within a few hours).

Why is CVC care and maintenance so
crucial?
Cost
• Incremental cost per episode of CR-BSI ranges from $25,000 to $56,0001.
• Hospitals absorb the majority of these costs
• U.S. hospitals incur as much as $2.3 billion per year as a result of CR-BSI
• CMS will no longer reimburse for CR-BSIs due to recent changes.
1.Centers for Disease Control and Prevention. Guidelines for the prevention of intravascularcatheter-related infections. Morbidity Mortality Weekly Report. 2002;51:1-29.
CLABSI-POA
If all of the elements of an infection definition are present during the two calendar days
before the day of admission, the first day of admission (day 1) and/or the day after
admission (day 2) and are documented in the medical chart, the infection would be
considered POA.
NOTE: *Infections that are POA should not be reported as HAIs.
*Physician diagnosis is not an element for the BSI definition, so it
cannot be used to identify a BSI as POA.
Acceptable documentation does not include self-reported symptoms by the patient (e.g.,
patient reporting having a fever prior to arrival to the hospital). Instead, symptoms must
be documented in the chart by a healthcare professional during the POA time frame (e.g.,
nursing home documents fever prior to arrival to the hospital).
MD diagnosis can be accepted as evidence of an infection that is POA only when MD
diagnosis is an element of the specific infection definition.
HAI
An infection is considered an HAI if all elements of a CDC/NHSN site-specific infection
criterion were first present together on or after the 3rd calendar day of admission to the
facility (the day of hospital admission is Day 1).
For an HAI, an element of the infection criterion may be present during the first 2 hospital
days as long as it is also present on or after calendar day 3.
All elements used to meet the infection criterion must occur within a timeframe that does
not exceed a gap of 1 calendar day between any two elements.
If all elements of an infection are present within 2 calendar days of transfer from one
inpatient location to another in the same facility or a new facility (i.e. on the day of
transfer or the next day), the infection is attributed to the transferring location
CLABSI
A central line-associated bloodstream infection (CLABSI) is a laboratory-confirmed
primary bloodstream infection (LCBI) where central line (CL) or umbilical catheter (UC)
was in place for >2 calendar days when all elements of the LCBI infection criterion were
first present together, with day of device placement being Day 1,
AND
a CL or UC was in place on the date of event or the day before. If a CL or UC was in
place for >2 calendar days and then removed, the LCBI criteria must be fully met on the
day of device discontinuation or the next day. If the patient is admitted or transferred into
a facility with a central line in place (e.g., tunneled or implanted central line), day of first
access is considered Day 1.
Patient in MSICU has central line inserted/accessed on June 1.
On June 3, the central line is still in place and the patient has
positive blood culture with S. aureus. This is a CLABSI because
the central line was in place for >2 calendar days when all
elements of LCBI Criterion 1 were first present together
On Feb. 5, a patient has a CL discontinued which was in place for
17 days. On Feb. 6, the patient spikes a fever of 38.3°C. Two blood
culture sets collected on Feb. 7 are positive for S. epidermidis.
This is a healthcare-associated bloodstream infection but it is not a
CLABSI because the CL was not in place the day of or the day
before all elements of LCBI Criterion 2 were first present together
Central Line-associated Bloodstream Infections (CLABSI)
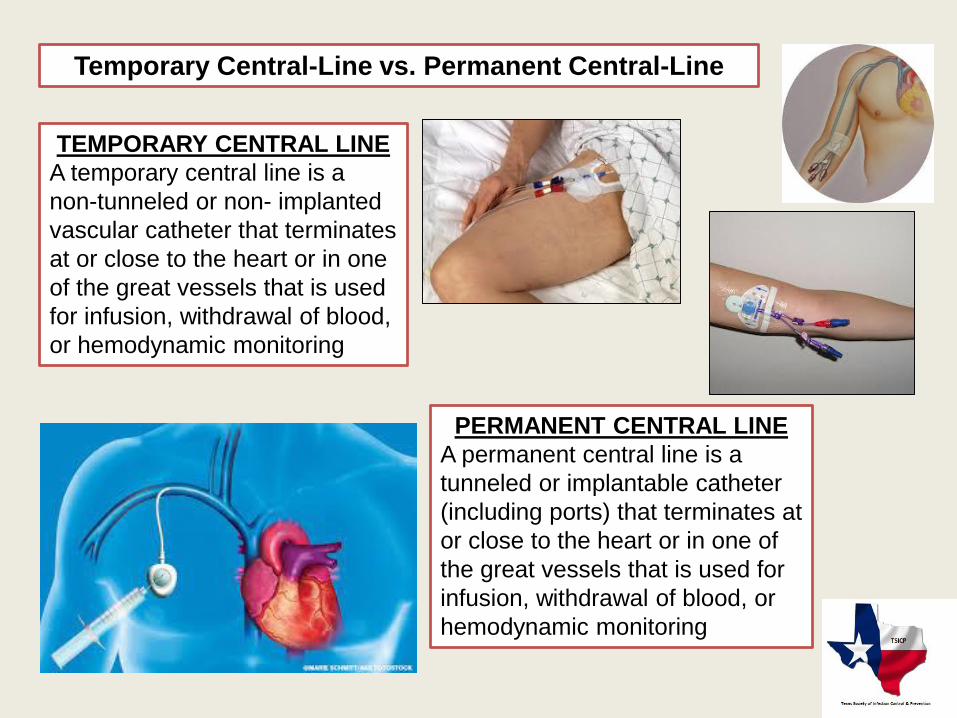
Temporary Central-Line vs. Permanent Central-Line
TEMPORARY CENTRAL LINE
A temporary central line is a
non-tunneled or non- implanted
vascular catheter that terminates
at or close to the heart or in one
of the great vessels that is used
for infusion, withdrawal of blood,
or hemodynamic monitoring
PERMANENT CENTRAL LINE
A permanent central line is a
tunneled or implantable catheter
(including ports) that terminates at
or close to the heart or in one of
the great vessels that is used for
infusion, withdrawal of blood, or
hemodynamic monitoring
INFUSION
Introduction of a solution through a blood vessel via a
catheter lumen.
INFUSIONS CAN INCLUDE:
• Continuous infusions such as nutritious fluids or medications
• Intermittent infusions such as flushes or IV antimicrobial administration
• Administration of blood or blood products in the case of transfusion or hemodialysis
An introducer is considered an intravascular
catheter, and depending on the location of its tip and
use, may be a central line
In neonates, catheters in the umbilical artery and
vein are considered central lines
Neither the location of the insertion site nor the type
of device may be used to determine if a line qualifies
as a central line
Pacemaker wires and other non-lumened devices
inserted into central blood vessels or the heart are
not considered central lines because fluids are not
infused, pushed, or withdrawn through such devices
Central Line-associated Bloodstream Infections (CLABSI)
The inpatient location where the patient
was assigned on the date of the BSI
event, which is further defined as the
date when the last element used to
meet the LCBI criterion occurred
Location of attribution
If all elements of an LCBI are present within 2 calendar days of transfer from one inpatient
location to another in the same facility or a new facility (i.e., on the day of transfer or the
next day), the infection is attributed to the transferring location or facility. Receiving facilities
should share information about such HAIs with the transferring facility to enable reporting
Example: Patient with a central line in place for 6 days in the SICU is transferred to the
surgical ward. On the next day, all elements of LCBI are first present together. This is
reported to NHSN as a CLABSI for the SICU.
TRANSFER RULE
Identifying Central Line-associated Bloodstream Infections
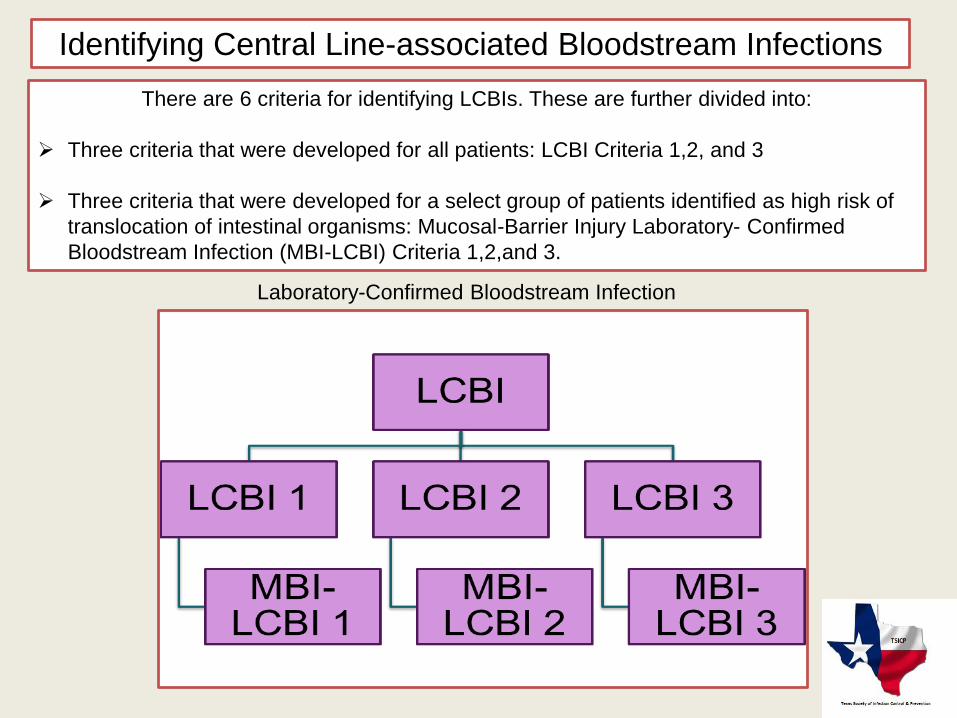
Laboratory-Confirmed Bloodstream Infection
There are 6 criteria for identifying LCBIs. These are further divided into:
Three criteria that were developed for all patients: LCBI Criteria 1,2, and 3
Three criteria that were developed for a select group of patients identified as high risk of
translocation of intestinal organisms: Mucosal-Barrier Injury Laboratory- Confirmed
Bloodstream Infection (MBI-LCBI) Criteria 1,2,and 3.

Central Line-associated Bloodstream Infections (CLABSI) LCBI
Criterion 1
Example: Jon Smith had a PICC line inserted on admission (June 1). On hospital day 4, he became
confused and experienced chills. Blood cultures were drawn which grew E. faecalis. No other source of
E. faecalis infection could be identified.
Mr. Smith meets the criteria for LCBI Criterion #1.
Patient has a recognized pathogen cultured from one or more blood cultures
AND
Organism cultured from blood is not related to an infection at another site.
IMPORTANT NOTES TO REMEMBER
One or more blood cultures means that at least one bottle from a blood draw is reported by the
laboratory as having grown organisms (i.e., is a positive blood culture).
"Recognized pathogen" does not include organisms considered common commensals. A few of the
recognized pathogens are Staph aureus, Enterococcus spp., E. coli, Pseudomonas spp., Klebsiella
spp., Candida spp., etc
Central Line-associated Bloodstream Infections (CLABSI)
LCBI Criterion 2
Criterion 2: Patient has at least one of the following signs or symptoms: fever (>38.0°C), chills,
or hypotension
and
positive laboratory results are not related to an infection at another site
and
the same common commensal (i.e., diphtheroids [Corynebacterium spp. not C. diphtheriae],
Bacillus spp. [not B. anthracis], Propionibacterium spp.,
coagulase-negative staphylococci [including S. epidermidis], viridans group
streptococci, Aerococcus spp., Micrococcus spp.) is cultured from two or more blood cultures
drawn on separate occasions. Criterion elements must occur within a timeframe that does not
exceed a gap of 1 calendar day between any two elements.
Central Line-associated Bloodstream Infections (CLABSI)
LCBI Criterion 2 and 3
The phrase “two or more blood cultures drawn on separate occasions” means:
1. That blood from at least 2 blood draws were collected within two calendar
days of each other, and
2. That at least one bottle from each blood draw is reported by the laboratory
as having grown the same common commensal (i.e., is a positive blood
culture).
Note: If special pediatric blood culture bottles are used, only one bottle may be
inoculated per blood draw. Therefore, to meet this part of the criterion, two
would have to be culture-positive.
Central Line-associated Bloodstream Infections (CLABSI)
Examples
A neonate has blood drawn for culture
on Tuesday and again on Thursday and
both grow the same common
commensal. Because the time between
these blood cultures exceed the two-
day period for blood draws, this part of
the criteria is not met.
An adult patient has blood drawn at 8
a.m. and again at 8:15 a.m. of the same
day. Blood from each blood draw is
inoculated into two bottles and
incubated (four bottles total). If one
bottle from each blood draw set is
positive for coagulase negative
staphylococci, this part of the criteria is
met.
Central Line-associated Bloodstream Infections (CLABSI)
LCBI Criterion 2: Examples
Example 1:
Mr. Smith developed a fever (38.6°C) on day 6 of his admission. Blood cultures
drawn 2 hours apart both grew coagulase-negative staphylococci. Mr. Smith had
no signs or symptoms or laboratory evidence of infection at the time of blood
cultures.
Mr. Smith meets Criterion 2 for LCBI.
Example 2:
Mrs. Green was admitted to the MICU for a myocardial infarction. A subclavian
central line was inserted on admission. She developed chills and a fever
(38.8°C) on day 4. One blood culture grew Staph epidermidis and the physician
ordered vancomycin to be given IV.
Mrs. Green does not meet either criteria for LCBI.
If Mrs. Green had another blood culture from day 4 or day 5 that was positive for
Staph epidermidis, she would meet the criteria for LBCI.
Criterion 3:
Patient <1 year of age has at least one of the following signs or symptoms : fever
(>38.0°C, core) hypothermia (<36°C, core), apnea, or bradycardia
and
positive laboratory results are not related to an infection at another site
and
the same common commensal (i.e., diphtheroids [Corynebacterium spp. not C.
diphtheriae], Bacillus spp. [not B. anthracis], Propionibacterium spp.,
coagulase-negative staphylococci [including S. epidermidis], viridans group
streptococci, Aerococcus spp., Micrococcus spp.) is cultured from two or more blood
cultures drawn on separate occasions. Criterion elements must occur within a
timeframe that does not exceed a gap of 1 calendar day between any two elements.
A Note About Neonates/Infants
• Criterion 3 only applies to patients who are 1 year of age or less (before or on
their birthday).
• Although LCBI Criterion 3 can only be used for infants and neonates, Criteria 1 or
2 can also be used in this population
Example:
Baby Boy Jones was afebrile at birth and had
no signs/symptoms of an infection. At 4 days
of age, the infant became very fussy and
irritable. A blood culture was drawn which
grew Pseudomonas aeruginosa, and no
other sources of infection were identified
Baby Boy Jones met Criterion 1 for LCBI.
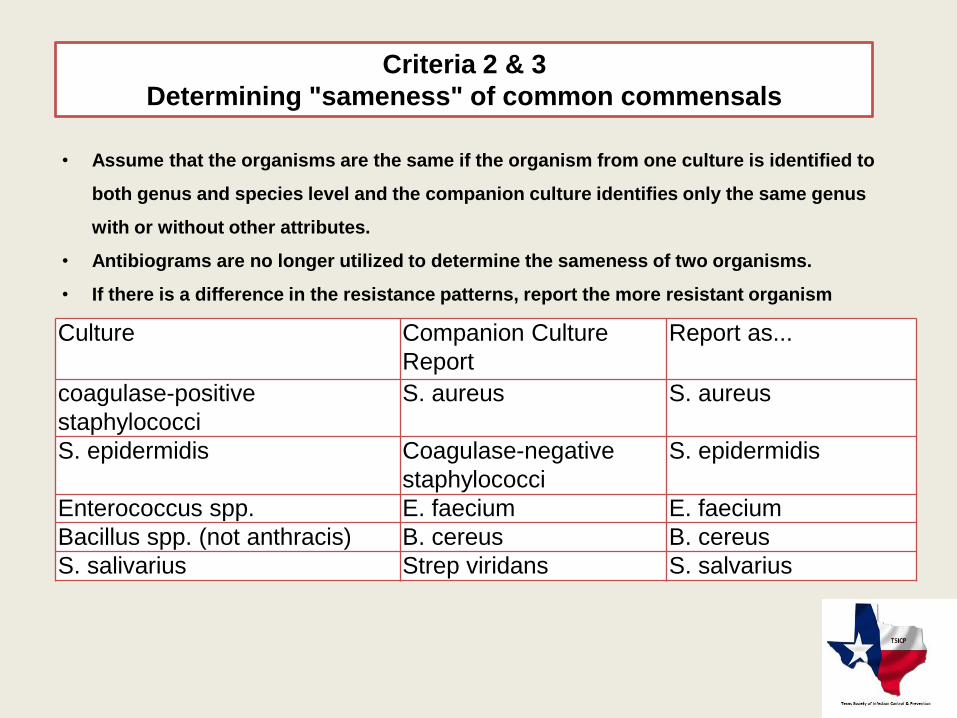
Culture Companion Culture
Report
Report as...
coagulase-positive
staphylococci
S. aureus S. aureus
S. epidermidis Coagulase-negative
staphylococci
S. epidermidis
Enterococcus spp. E. faecium E. faecium
Bacillus spp. (not anthracis) B. cereus B. cereus
S. salivarius Strep viridans S. salvarius
• Assume that the organisms are the same if the organism from one culture is identified to
both genus and species level and the companion culture identifies only the same genus
with or without other attributes.
• Antibiograms are no longer utilized to determine the sameness of two organisms.
• If there is a difference in the resistance patterns, report the more resistant organism
Criteria 2 & 3
Determining "sameness" of common commensals
If these are the results from two blood draws, we would assume that they are
the same organisms.
Indicate which result would be reported:
- Coagulase-negative staphylococci
- Staph epidermidis
Central Line-associated Bloodstream Infections (CLABSI)
Mucosal Barrier Injury Laboratory-Confirmed Bloodstream Infection
(MBI-LCBI)
PURPOSE:
To address need more specific BSI definition in oncology
• To reduce misclassification of BSI resulting from translocation of intestinal
organisms as BSI associated with the central line
• These BSIs are not impacted by CLABSI prevention measures
• Are aimed at patients with mucosal barrier injury at high risk for translocation
of intestinal organisms
• Development was led by CDC with input from external subject matter experts
• Considerations given to data collection, burden, use of objective criteria,
availability of data components, clinical credibility
MBI-LCBI Criterion 1
Patient of any age meets criterion 1 for LCBI with at least one blood culture growing any of the
following intestinal organisms with no other organisms isolated: Bacteroides spp., Candida spp.,
Clostridium spp., Enterococcus spp., Fusobacterium spp., Peptostreptococcus spp., Prevotella
spp., Veillonella spp., or Enterobacteriaceae
AND
Patient meets at least one of the following:
Is an allogeneic hematopoietic stem cell transplant recipient within the past year with one of the
following documented during same hospitalization as positive blood culture:
• Grade III or IV gastrointestinal graft versus host disease (GI GVHD)
• ≥1 liter diarrhea in a 24 hour period (or ≥20 mL/kg in a 24 hour period for patients <18 years of age) with
onset on or within 7 calendar days before the date the positive blood culture is collected.
Is neutropenic, defined as at least 2 separate days with values of absolute neutrophil count (ANC)
or total white blood cell count (WBC) <500 cells/mm3 on or within 3 calendar days before the date
the positive blood culture was collected (Day 1).
MBI-LCBI Criterion 2
Patient of any age meets criterion 2 for LCBI when the blood cultures are growing only
viridans group streptococci with no other organisms isolated:
AND
Patient meets at least one of the following:
Is an allogeneic hematopoietic stem cell transplant recipient within the past year with one
of the following documented during same hospitalization as positive blood culture:
• Grade III or IV gastrointestinal graft versus host disease (GI GVHD)
• ≥1 liter diarrhea in a 24 hour period (or ≥20 mL/kg in a 24 hour period for patients <18 years of
age) with onset on or within 7 calendar days before the date the positive blood culture is
collected.
Is neutropenic, defined as at least 2 separate days with values of absolute neutrophil
count (ANC) or total white blood cell count (WBC) <500 cells/mm3 on or within 3 calendar
days before the date the positive blood culture was collected (Day 1).
MBI-LCBI Criterion 3
Patient < 1 year of age meets criterion 3 for LCBI when the blood cultures are growing only
viridans group streptococci with no other organisms isolated:
AND
Patient meets at least one of the following:
Is an allogeneic hematopoietic stem cell transplant recipient within the past year with one of
the following documented during same hospitalization as positive blood culture:
• Grade III or IV gastrointestinal graft versus host disease (GI GVHD)
• ≥20mL/kg diarrhea in a 24 hour period for patients with onset on or within 7
calendar days before the date the positive blood culture is collected.
Is neutropenic, defined as at least 2 separate days with values of absolute neutrophil count
(ANC) or total white blood cell count (WBC) <500 cells/mm3 on or within 3 calendar days
before the date the positive blood culture was collected (Day 1).
Important Information Regarding MBI-LCBI
"no other organisms isolated" means there is not isolation in a blood
culture of another recognized pathogen (e.g., S. aureus) or common
commensal (e.g., coagulase-negative staphylococci) other than listed
in MBI criterion 1,2, or 3 that would otherwise meet LCBI criteria*.
If this occurs, the infection should not be classified as MBI-LCBI.
Grade III/IV GI GVHD is defined as follows:
• In adults: > 1 L diarrhea/day or ileus with abdominal pain
• In pediatric patients: > 20mL/kg/day of diarrhea
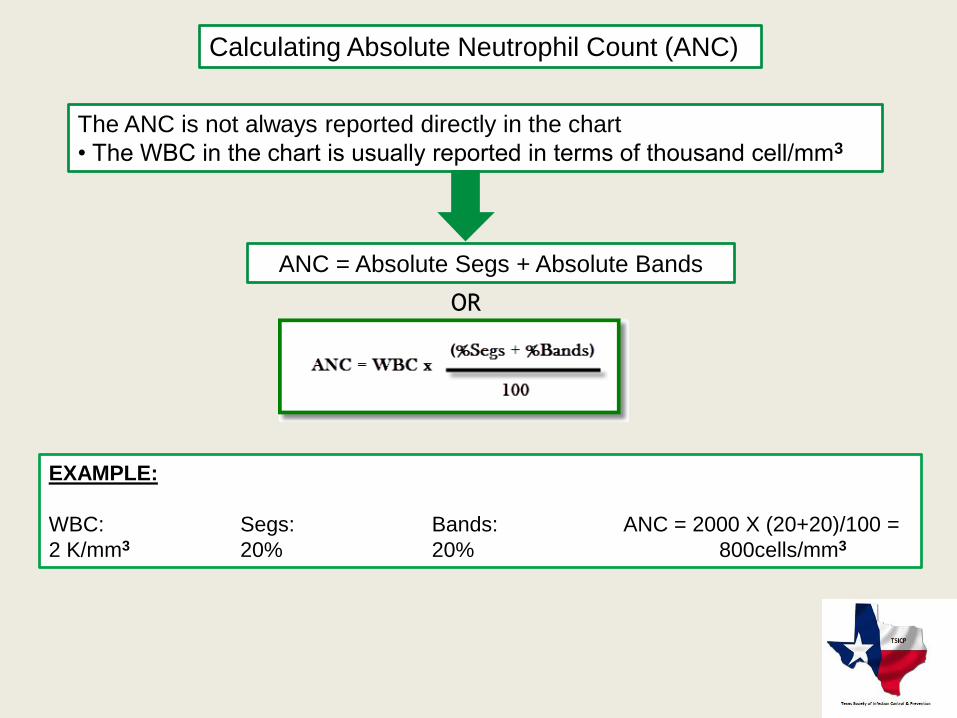
Calculating Absolute Neutrophil Count (ANC)
The ANC is not always reported directly in the chart
• The WBC in the chart is usually reported in terms of thousand cell/mm3
ANC = Absolute Segs + Absolute Bands
EXAMPLE:
WBC: Segs: Bands: ANC = 2000 X (20+20)/100 =
2 K/mm3 20% 20% 800cells/mm3
OR
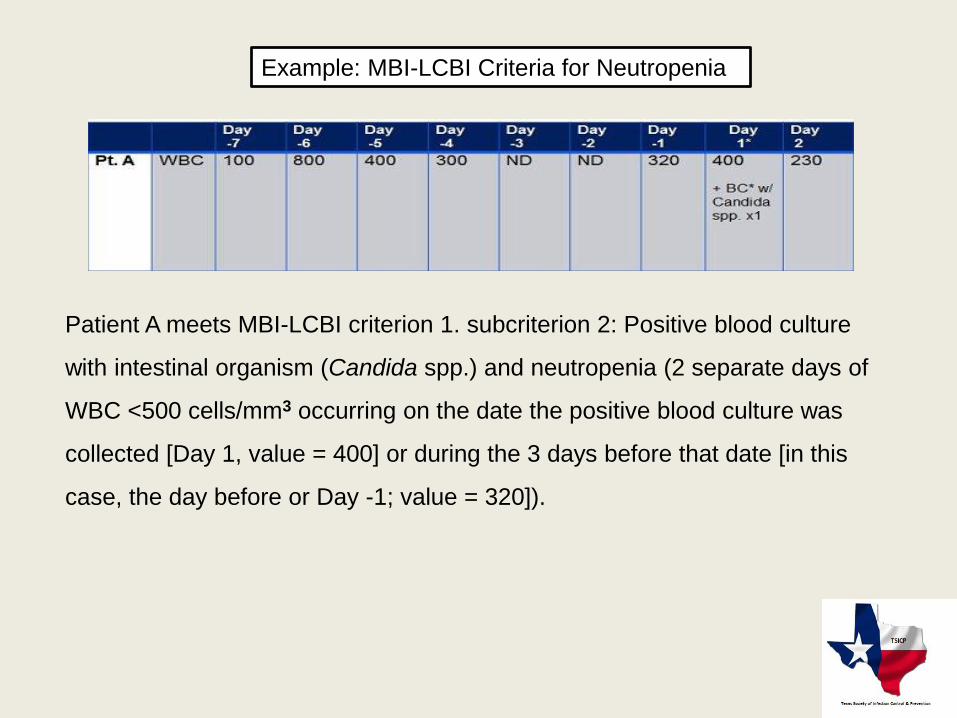
Example: MBI-LCBI Criteria for Neutropenia
Patient A meets MBI-LCBI criterion 1. subcriterion 2: Positive blood culture
with intestinal organism (Candida spp.) and neutropenia (2 separate days of
WBC <500 cells/mm3 occurring on the date the positive blood culture was
collected [Day 1, value = 400] or during the 3 days before that date [in this
case, the day before or Day -1; value = 320]).
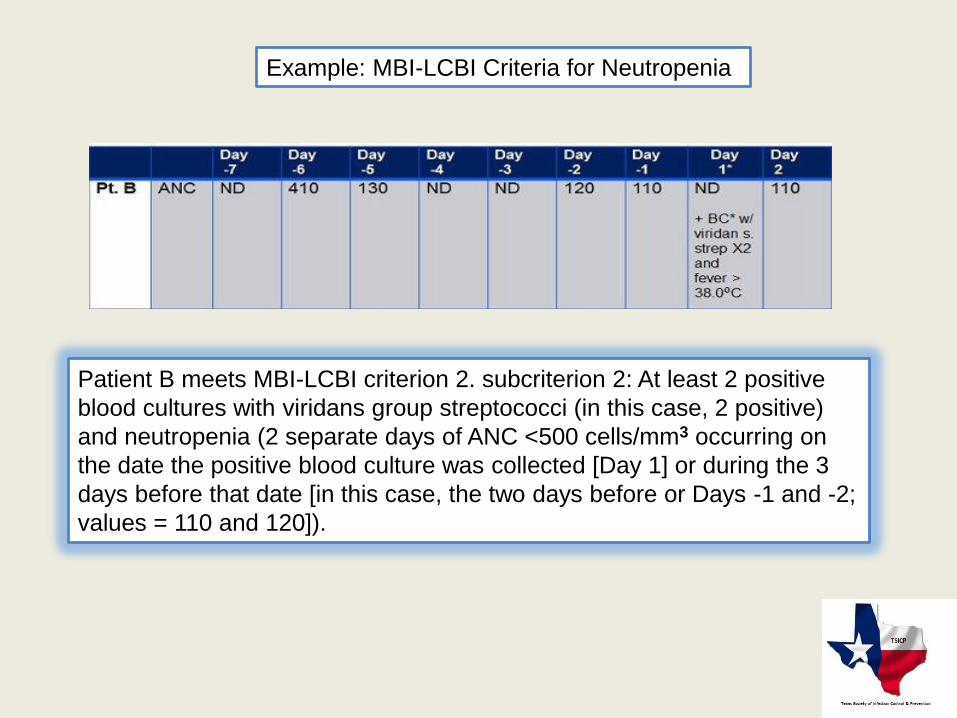
Patient B meets MBI-LCBI criterion 2. subcriterion 2: At least 2 positive
blood cultures with viridans group streptococci (in this case, 2 positive)
and neutropenia (2 separate days of ANC <500 cells/mm3 occurring on
the date the positive blood culture was collected [Day 1] or during the 3
days before that date [in this case, the two days before or Days -1 and -2;
values = 110 and 120]).
Example: MBI-LCBI Criteria for Neutropenia
Primary BSI vs. Secondary BSI
Primary BSI
("not related to an infection at another site")
• A primary BSI is identified by ruling out all non-blood sites as the source of the
bloodstream infection
• A BSI that is associated with an infection at another site is referred to as a Secondary
BSI and never reported as a BSI or CLABSI
Secondary BSI
• A culture-confirmed BSI associated with a documented infection at another site
AND
• Primary infection must meet one of the CDC/NHSN infection definitions (Chapter 17)
AND
• BSI and other sites must be related according to the culture guidelines provided in the
next few slides
Forms used for CLABSI
Calculating the CLABSI Rate
CLABSI rate equals the number of CLABSIs identified* divided by the number of central line
days*, multiplied by 1000.
* Stratify by --
• Type of ICU or other location
• Specialty Care Area (SCA)/Oncology
• Temporary line
• Permanent line
• NICU
• Birthweight category

NOTE: There is no multiplier for the DU Ratio
The DU Ratio measures the proportion of patient days in which central lines were used. It is a
measure of the patient's exposure to risk in this location.
Device Utilization (DU) Ratio
CLABSI Standardized Infection Ratio (SIR)
While the CLABSI SIR can be calculated for single locations, the measure
also allows you to summarize your data across multiple locations,
adjusting for differences in the incidence of infection among the location
types.
Note: The SIR will be calculated only if the number of expected
HAIs (numExp) is > 1.
Analysis
In NHSN, you can generate:
• Line listings
• Rate tables• Frequency tables
• Bar charts
• Pie charts
• Control charts
Click on each button to the right
to see an example of CLABSI
output
CLABSI
Line Listing
CLABSI Rate
Table & DU Ratios
CLABSI
Pie Chart
CLABSI
SIR
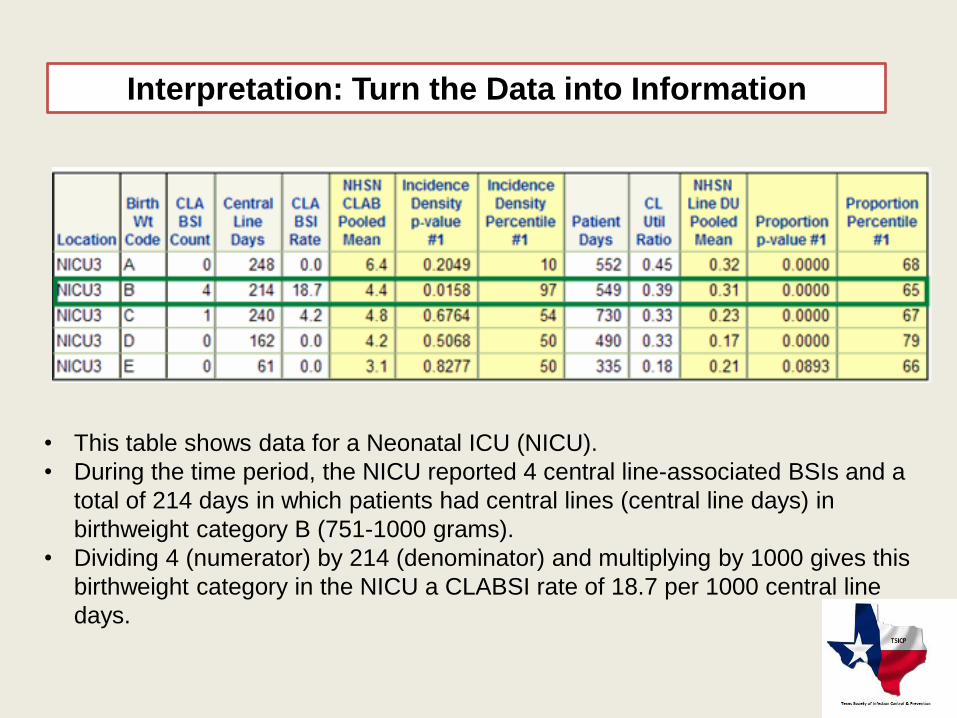
Interpretation: Turn the Data into Information
• This table shows data for a Neonatal ICU (NICU).
• During the time period, the NICU reported 4 central line-associated BSIs and a
total of 214 days in which patients had central lines (central line days) in
birthweight category B (751-1000 grams).
• Dividing 4 (numerator) by 214 (denominator) and multiplying by 1000 gives this
birthweight category in the NICU a CLABSI rate of 18.7 per 1000 central line
days.

QUESTIONS??
