cerebral malakoplakia associated with neonatal herpes ... · cerebral malakoplakia associated with...
TRANSCRIPT

ANNALS OF CLINICAL AND LABORATORY SCIENCE, Vol. 22, No. 5Copyright © 1992, Institute for Clinical Science, Inc.
Cerebral Malakoplakia Associated with Neonatal Herpes Virus Infection*
EMILY VOLK, M.S., JOSEPH C. PARKER, JR., M.D.,and SHELLEY TEPPER, M.D.
Department o f Pathology, University o f Missouri-Kansas City School o f Medicine,
Truman Medical Center, Kansas City, MO 64108
ABSTRACT
Cerebral malakoplakia has been recognized as a complication of probable neonatal herpes encephalitis and may be associated w ith persistent neurologic deficits including seizures. At autopsy, an eight-month-old boy had a discrete cystic gliotic lesion in his left inferior frontal lobe with malakoplakia. Perinatal herpetic cutaneous lesions were seen and were successfully treated with m edication at two weeks of age. Subsequent discontinuation of his anti-epileptic drugs was followed by sudden unexpected death. Im m unohistochem ical stains and electron microscopy of his brain failed to reveal herpes simplex virus.
Introduction
M alakoplakia was first described by Michaelis and Gutmann in 1902.10 The term, coined a year later by Von Hanse- mann, was derived from the Greek words ‘malakos’ (soft) and ‘plakos’ (plaque). I t is a rare, morphologically unique, chronic inflammatory process characterized by the accum ulation of large m ononuclear phagocytes term ed Von Hansem ann histiocytes, surrounded by and containing d iastase-resistan t period ic acid Schiff (PAS) positive inclusions and calcified, laminated, target-shaped bodies term ed M ichaelis-Gutmann bodies.1 W hen originally described, malakoplakia was thought
* Send reprint requests to Joseph C. Parker Jr., M.D., Department of Pathology, University of Louisville School of Medicine, Louisville, KY 40292.
to exist solely in the urinary tract, bu t in 1958 the first case of malakoplakia was d e sc r ib e d o u ts id e th e u rin a ry trac t. E x travesicu lar occurrence is in creasing.15,16 The most common sites include, in order of decreasing frequency, the urinary bladder, genital tract, gastrointestinal tract, and retroperitoneum .15,16 C erebral malakoplakia, however, is extremely rare and has been d esc rib ed in five infants, including neonates.1,5,7,11
M alakoplakia in the urinary b ladder has been linked to coliform infections, and bacteria have been dem onstrated in some diseased bladders.10 O ther possible agents have included staphylococci,13 e x t r a v a s a te d e r y t h r o c y t e s ,14 a n d viruses.15 To date, no virus has been isolated or identified from malakoplakic tissues. The process may result from imm un o lo g ic d y s fu n c tio n a n d h as b e e n
3000091-7370/92/0900-0300 $00.90 © Institute for Clinical Science, Inc.

CEREBRAL MALAKOPLAKIA WITH NEONATAL HERPES VIRUS INFECTION 301
associated with tuberculosis, sarcoidosis, malignancy, cachexia, and immune deficiency sta tes.15 The distinctive macrophage pattern of the Von Hansemann histiocytes suggests an altered macrophage response, secondary to an altered T-cell response. Lou and Teplitz9 suggested a d e fe c t in th e m acrophag ic lysosom e which could lead to incom plete cell degradation, resulting in deposition of products incom pletely d igested producing m alakop lak ia . H e rp e s sim plex virus (HSV) infecting the brain could lead to necrosis and histiocytic phagocytosis of cellu lar debris, which with an altered immune state, could cause malakoplakia.
Case Report
This 13-day-old black male weighing 3.9 kg (75th percentile) was bom after a gestation of 40 weeks. He was delivered vaginally by forceps without complications and admitted to Children’s Mercy Hospital in Kansas City, Missouri, for uncontrollable generalized myoclonic seizures. At birth, a small blister was noted on his scalp. At 11-days-old, his mother noted two small blisters on the baby’s subscapular region. Neurological exam revealed a lethargic infant with equal motion in all extremities and bilateral upgoing plantar reflexes. Moro and suck reflexes were intact. His neck was normal. The infant had tonic-clonic seizures beginning in his right arm becoming secondarily generalized in the Emergency Room. These seizures lasted only a few minutes, but occurred several times. The patient was treated with dilantin and hospitalized.
On his first day of hospitalization, he had recurrent seizures which began on the right side and became generalized. The baby was given more dilantin and had another seizure that day. Phénobarbital was added and was given intravenously until his 10th hospital day when it was administered orally. An electroencephalogram (EEG) and computerized tomographic scan of his head were normal. Laboratory studies on admission included white blood cell count of 10.2 thousand per mm3 with 38 percent segmented neutrophils, three percent bands, 44 percent lymphocytes, 11 percent monocytes, one percent eosinophil and one percent basophil. Hemoglobin was 13.1 g per dl with 756,000 per mm3 platelets. Serum electrolytes were normal. Cerebrospinal fluid showed no red blood cells, 66 per mm3 white blood cells with three segmented neutrophils, 28 lymphocytes, and 35 monocytes. Cerebrospinal fluid (CSF) protein was 64 mg per dl and glucose was 38 mg per dl. Urine analysis was normal. Blood cultures showed no growth after ten days.
During the first week of his hospital stay, the baby was irritable with periods of somnolence. He remained in a flexed posture and was given intravenous acyclovir for 14 days. Cultures of his skin lesions grew HSV 2. His cerebrospinal fluid (CSF) remained sterile. New skin lesions never developed, and his scalp and back lesions healed. An EEG prior to discharge was normal. About four months later, his mother brought him to the Emergency Room at Children’s Mercy Hospital for “seizures”, though no seizure activity was witnessed. The baby’s vital signs included 7.21 kg, 62 cm length, 37.8°C, pulse of 140 per sec, and respirations of 44 per sec. He was pink with capillary refill of less than two seconds. He was moving all extremities.
At six-months-old, CSF studies were repeated and failed to reveal HSV 1 and 2. His mother reported no recent seizures and stated that the baby’s doctor had discontinued seizure medication. At eight months old, without further seizures, according to the mother, he was found dead four hours following a feeding of diluted Coca-Cola. His death was attributed to chronic meningoencephalitis owing to HSV.
Postmortem Findings
Toxicologic tes tin g o f post-m ortem blood was negative for opiates, am phetamines, cocaine, and phenobarbital. Congestion and edem a of the lungs w ere observed, b u t no o ther abnorm alities were observed in the general autopsy.
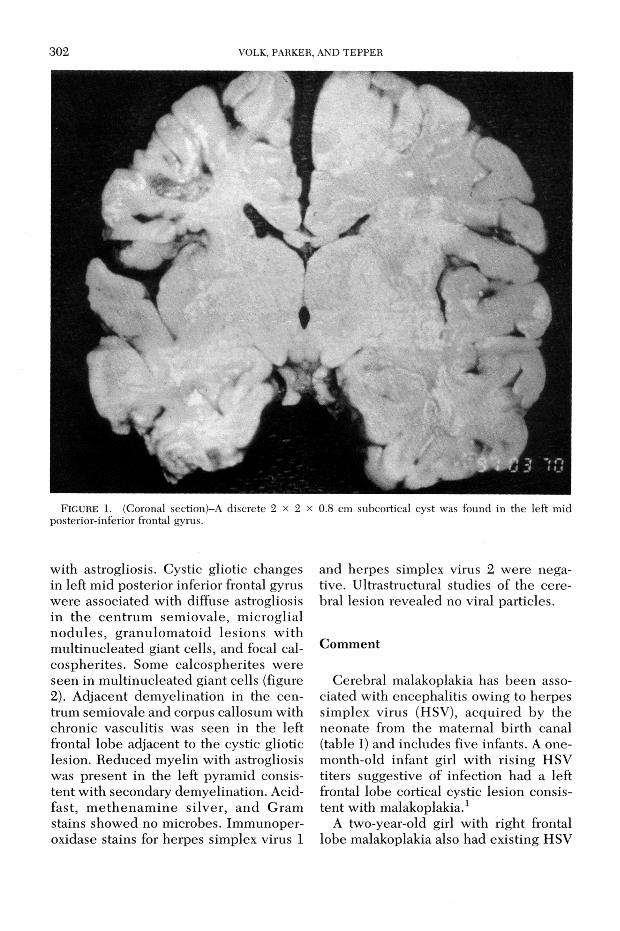
T he n e u ro p a th o lo g ic ex am in a tio n revea led a fixed b ra in w eigh ing 800 grams (normal 850 grams). The circle of Willis was intact. The right and left lateral ventricles were mildly dilated with the left lateral ventricle being slightly larger than the right. A discrete subcorti- cal cyst was seen in the left m id posterior inferior frontal gyrus and m easured 2 x 2 x 0.8 cm (figure 1). The corpus callosum was markedly th inned and varied from one to three mm in the maximal thickn e ss . T h e c e n tru m se m io v a le w as red u ced in the left frontal lobe, b u t appeared normal in the right frontal lobe. T he deep basal nuc le i and tem poral lobes w ere intact. T he brainstem and cerebellum were normal.
M icroscopically , focal p e riv ascu la r lymphoid cell infiltrates were seen in the midbrain, cerebellum , and frontal cortex
302 VOLK, PARKER, AND TEPPER
FIGURE 1. (Coronal section)-A discrete 2 x 2 x 0.8 cm subcortical cyst was found in the left mid posterior-inferior frontal gyrus.
with astrogliosis. Cystic gliotic changes in left mid posterior inferior frontal gyrus were associated with diffuse astrogliosis in the cen trum sem iovale, m icroglial no d u les , g ranu lom ato id lesions w ith m ultinucleated giant cells, and focal cal- cospherites. Some calcospherites were seen in m ultinucleated giant cells (figure2). Adjacent dem yelination in the centrum semiovale and corpus callosum with chronic vasculitis was seen in the left frontal lobe adjacent to the cystic gliotic lesion. Reduced myelin with astrogliosis was present in the left pyramid consistent with secondary demyelination. Acid- fast, m eth en am in e silver, and Gram stains showed no microbes. Immunoper- oxidase stains for herpes simplex virus 1
and herpes simplex virus 2 were negative. Ultrastructural studies of the cerebral lesion revealed no viral particles.
Comment
Cerebral malakoplakia has been associated with encephalitis owing to herpes sim plex virus (HSV), acquired by the neonate from the m aternal birth canal (table I) and includes five infants. A one- month-old infant girl with rising HSV titers suggestive of infection had a left frontal lobe cortical cystic lesion consistent with malakoplakia.1
A two-year-old girl with right frontal lobe malakoplakia also had existing HSV

CEREBRAL MALAKOPLAKIA W ITH NEONATAL HERPES VIRUS IN FECTIO N 303
J 'ft m m m B U —
■ M «
V # v
r'%| I m i
%’ » ,
I*- i '4 h ■ I P ’
* * i I Ÿ * '\ » , , 5♦ m ¡ÆLx-:
m , * 4
F igure 2. The cystic gliotic lesion in the left frontal lobe had a histiocytic reaction, with multi- nucleated giant cells and calcospherites consistent with cerebral m alako- plakia. (Hematoxylin and eosin x200.)
e n c ep h a litis .1 A th ree-m onth-o ld boy with malakoplakia of the brain and aortitis was observed w ith neonatal HSV infection.11 A three-month-old infant boy with cerebral malakoplakia of the brain had herpes simplex m eningoencephalitis diagnosed at two weeks.5 A three-week- old girl with right temporal lobe malakoplakia had rising serum HSV titers
and a m other w ith post-partum HSV 2 infection.7
Three major features in the curren t baby included (a) neonatal herpes simplex virus 2 infection, (b) cerebral malakoplakia, and (c) seizures. The HSV 2 infection seems to have damaged cerebral tissue leading to epilepsy. This virus is transmitted from person to person by

TABLE ICerebral Malakoplakia Associated with Probable Herpes Virus (HSV) Encephalitis
304 VOLK, PARKER, AND TEPPER
Reference Sex Age Location Course Comment
Chandra, & Kapur:Arch. Pathol. Lab. Med. .122:688-692, 1979.
F 1 month Left frontal lobe
2 Week hospital stay
Rising HSV titer
Chandra & Kapur:Arch. Pathol. Lab. Med. 103: 688-692,1979.
F 2 years Right frontal lobe
Encephalitis Severeneurologicalimpairment
Mirra:Am. J. Clin. Pathol. 56:104-110,1971.
M 3 months Cerebralcortex
Died at 1.5 years
Associatedaortitis
Gorde, Borit, et al:Bull. Los Angeles Neurol. Soc. 42:6-11, 1978.
M 2 weeks Right frontal lobe
Recoveryover5 months
Siezures
Ho-Chang, Nigro, et al: Arch. Pathol. Lab. Med. 104:494-495. 1980.
F 3 weeks Right temporal lobe
Severepsychomotordelay
Rising HSV titer
Current: M 13 days Left frontal lobe
Died at 8 months
Seizures with scalp lesion whichyielded HSV
contact with infected cutaneous vesicles and can occur during the second stage of labor w ith fetal con tact w ith genita l herpes. Perinatal infectious risk is highest w hen the prim ary genital infection has occurred w ithin weeks of delivery.4 Neonatal death is usually due to dissem inated infection with HSV-2 which infects the liver, adrenals, and any other organs. Death occurs from infection of the brain, heart, and/or lungs.12 Neonatal herpes can in fec t the ce reb ra l h em ispheres, basal ganglia, b rainstem , cerebellum , spinal cord, or any combination. Microglial proliferation and intra-nuclear inclusion bodies in neurons and glial cells are seen. Perivascular inflammation occurs, bu t it is not as striking as in other affected organs. W idespread necrosis of the cerebrum can cause m ulticy stic cereb ral degeneration ,6 as seen in our patient.
According to Nahmias e t al,12 67 percent of symptomatic neonates have dissem inated disease and 33 percent have localized involvement to the brain, eye, skin, or mouth. Approximately 50 percent of symptomatic neonates with herpes virus show central nervous system involvement. Mortality rate is 62 percent. Among survivors, 50 percen t have perm anent sequelae.12 C hildren with HSV encephalitis rarely survive w ithout neurological deficits.3,4 Most neonates with dissem inated HSV infection are sym ptom atic within the first week after delivery, but they may show clinical manifestations as m uch as three weeks later.6 Vesicular cutaneous lesions usually appear on the scalp or buttocks in 30 percent.12
Herpes encephalitis is m anifested by irritability and seizures, which may be focal or generalized and often refractory

CEREBRAL MALAKOPLAKIA W ITH NEONATAL HERPES VIRUS IN FECTIO N 305
to therapy. The EEG is usually abnormal with slow waves or spike discharges. The CSF shows a leukocytosis with lymphocytic predom inance. Erythrocytes may be seen w h en hem orrhag ic necrosis develops. The CSF protein concentration is elevated.12 Patients with HSV-2 may d e v e lo p se v e re n e u ro lo g ic dam age. According to Corey et al,2 50 percent of infants w ith HSV-2 encephalitis treated w ith acyclovir w ere m icrocephalic; 57 percen t had ep ilepsy; 64 percen t had ophthalmic disease; 64 percent had cerebral palsy; and 57 percen t were m entally retarded.
Since cerebral malakoplakia is rare, its sequelae are not well defined. Mortality, in this condition, may exceed 50 percent.15 The extra-genitourinary involvem ent has been linked with imm unosuppression , in c lu d in g AIDS. A specific defec t in in trace llu la r k illing m echanisms may be the underlying cause.9 The HSV infection could cause incom plete histiocytic phagocytosis of necrotic cellular debris, resulting in subsequent mine ra liza tio n and m alak o p lak ia .16 This mechanism , which has been described with bacterial products, has not been recognized w ith viruses.
Epilepsy in our patient with chronic m eningoencephalitis was associated with sudden unexpected death (SUD), which varies from one in 500 to 1000 epileptic persons.8 The m echanism deals with connections be tw een the cerebral cortex, limbic system, and hypothalamus with the heart via the sympathetic autonomic nervous system. Abnormal cerebral discharges in seizures occur with potentially fatal cardiac dysrhythm ias, includ ing ven tricu la r f ib rilla tio n and asysto le.8 Although anticonvulsant m edication can abo lish th ese associated cardiac dysrhythm ias, m ost victim s of SUD show su b th e rap eu tic or no blood levels of an ticonvulsant m edication at autopsy. Transition from late sleep stage to wakefulness can also induce epileptic discharges.8
Our patient was infected w ith HSV 2 e ith e r th rough in trau te rin e rou tes or during labor. The virus colonized the baby’s skin, entered his blood stream and seems to have settled in the left frontal lobe following viremia. Necrosis in terfered w ith norm al cereb ral e lec trica l d isc h a rg e s , c re a tin g e p ile p s y . T h e a lte red im m une reaction in the baby resulted in malakoplakia. Months later, anticonvulsant m edication was discontinued. The baby experienced abnorm al electrical discharges from his damaged left frontal lobe, which stim ulated the sympathetic nervous system, resulting in a fatal cardiac dysrhythmia.
Acknowledgment
Thanks are extended to John J. Kepes, M.D. of the Department of Pathology at the University of Kansas Medical Center in Kansas City, Kansas, for his assistance in identifying and classifying the lesion in the current case report.
References
1. C h a n d r a , R. S. and Ka p u r S.: Malakoplakia of the Brain. Arch. Pathol. Lab. Med. 103:688— 692, 1979.
2. C o r e y , L., W h it l e y , R. J ., and St o n e , T.: Difference between HSV 1 and HSV 2 neonatal encephalitis in neurological outcome. Lancet I : 1-4, 1988.
3. F r e n t z , J. M., G o h d , R. S., and W o o d y , N. C.: Untreated neonatal herpes simplex meningitis without apparent neurological damage. J. Pediat. 85:77-79, 1974.
4. G e r s h o n , A. A., F is h , I., and Br u n e l l , P. A.: Herpes simplex infection of the newborn. Am. J. Dis. Child. 224:739-741, 1972.
5. G r o d e , M. L., B o r i t , A., V a n D e V e l d e , R. L., W e i n e r , L., and C a r t o n , C . A.: Cerebral Malakoplakia. Bull. Los Angeles Neurological Soc. 43:6-11, 1978.
6. Haynes, R. E.: The spectrum of herpes simplex virus infections in children. Southern Med. J. 69:1069-1078, 1976.
7. H o -C h a n g C ., N ig r o , M. A., and P e r r i n , E. V.: Cerebral malakoplakia and neonatal herpes simplex infection. Arch. Pathol. Lab. Med. 204:494-495, 1980.
8. J a y , G . and L e e s t m a , J.: Sudden death in epilepsy, a comprehensive review of literature and

306 VOLK, PARKER, AND TEPPER
proposed mechanisms. Acta Neurologica Scand. 63 Suppl 82:5-59, 1981.
9. LOU, T. Y. and T e PLITZ, C.: Malakoplakia: pathogenesis and ultrastructural morphogenesis, a problem of altered macrophage response. Human Pathol. 5:191-207, 1974.
10. MlCHAELIS L. a n d GUTMANN C.: U e b e r e in - s c h lu s se in b la s e n tu m o re n . Z . K lin ic h e M ed . 47:208—215, 1902.
11. MlRRA, J. M .: Aoritis and malakoplakia-like lesion of the brain in association with neonatal herpes simplex infection. Am. J. Clin. Pathol. 56:104-110, 1971.
12. N a h m ia s , A. J., A l f o r d , C. A ., and Ko r o n e s ,S. B.: Infections of newborn with herpesvirus hominus. Adv. Pediat. 27:185—226, 1970.
13. P r ic e , H. M., H a m r a h a n , J. B., and F il ir id a , R. G.: Morphogenesis of calcium laden cytoplasmic bodies in malakoplakia of the skin: an electron microscopic study. Human Pathol. 4: 381-394, 1973.
14. Sm it h -S in c l a ir , C ., Ka h n , L. B., and C y r v e s ,C .: Malakoplakia in childhood; A case report with ultrastructural observation and review of literature. Arch. Pathol. 99:198-203, 1975.
15. S t a n t o n , M . J. a n d M a x t e d M .: M a la k o p la k ia , a s tu d y o f th e l i te ra tu re a n d c u r re n t c o n c e p ts o f p a th o g e n e s is , d ia g n o s is a n d t re a tm e n t. J. U ro l. 225:129-146, 1981.
16. TE R N E R J. Y. and LA T TE S, R.: Malakoplakia of colon and retroperitoneum. Am. J. Clin. Pathol. 44:20-31, 1965.