cerebrospinal fluid and intracranial pressure dr ifra ashraf
TRANSCRIPT
CEREBROSPINAL FLUID AND INTRACRANIAL
PRESSURE
DR IFRA ASHRAF

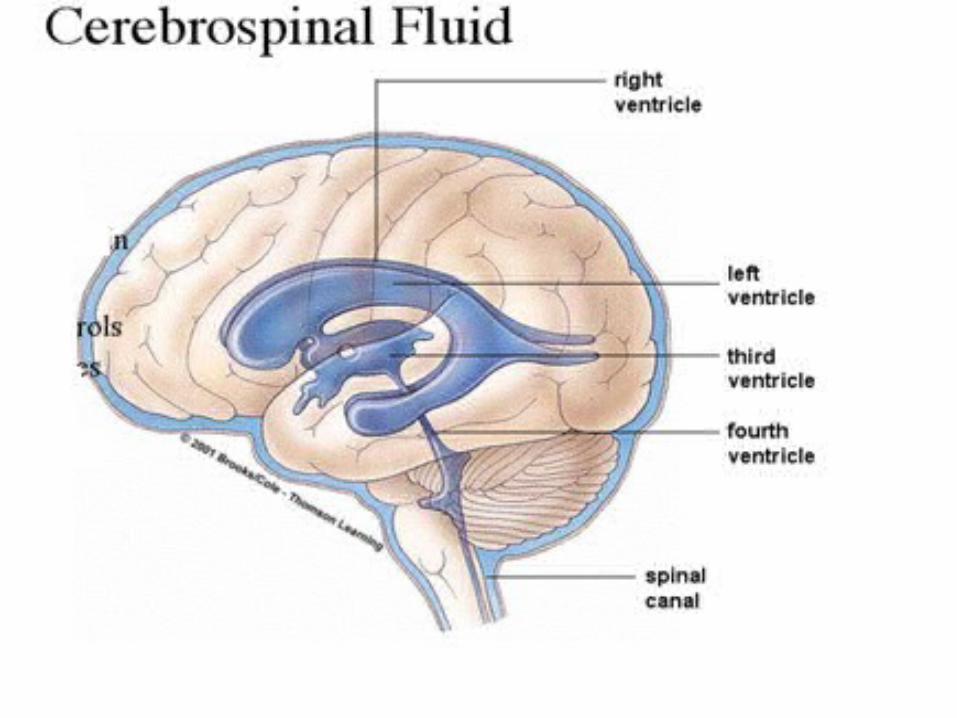
CEREBROSPINAL FLUIDThe cerebrospinal Fluid
[CSF] is a clear, colorless
transparent, tissue fluid
present in the cerebral
ventricles, spinal canal,
and subarachnoid spaces.
FORMATION
CSF is largely formed by the choroid plexus of the lateral
ventricle and remainder in the third and fourth ventricles.
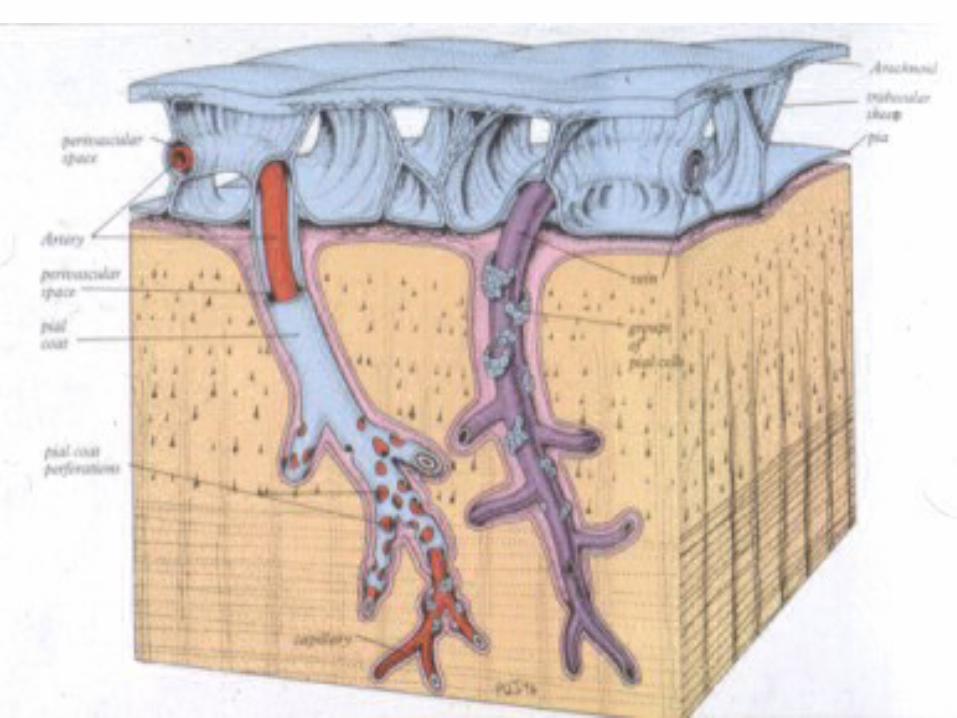
About 30%from the ependymal cells lining the ventricles and
other brain capillaries (perivascular space).
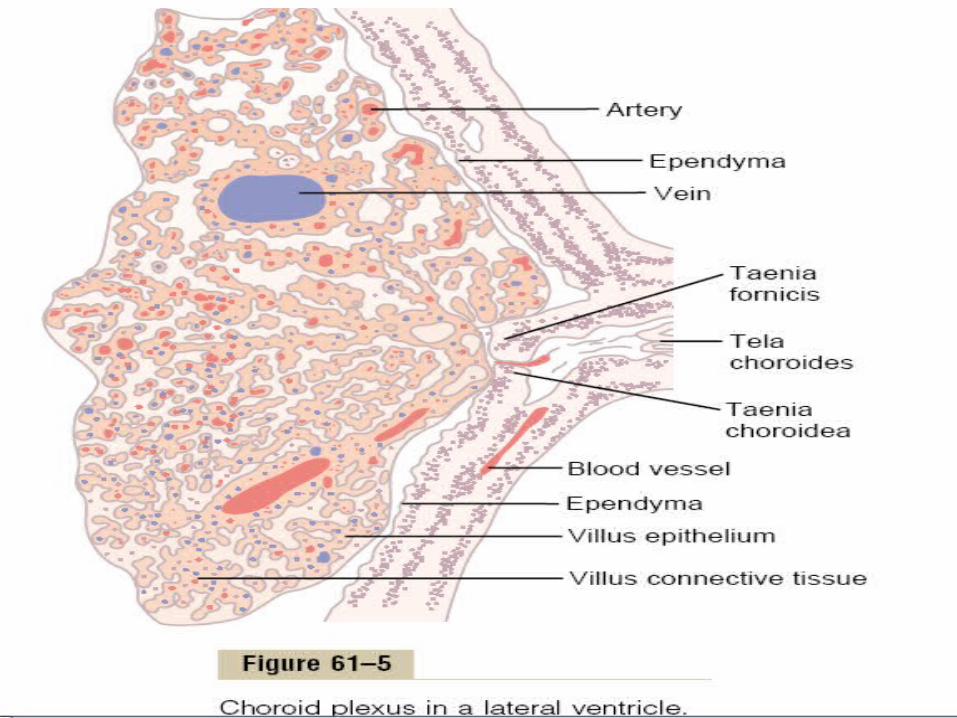
CHOROID PLEXUS• The choroid plexus consist of
highly vascularized, "cauliflower-like" masses of pia mater tissue that dip into pockets formed by ependymal cells.
• These ependymal cells have microvilli on the CSF side, form a continuous sheet around the choroid plexus.
MECHANISM OF FORMATION OF CSFCSF is formed primarily by
secretion (active
transportation) and by
filtration from the net works of
capillaries and ependymal cells
in the ventricles called choroid
plexus.
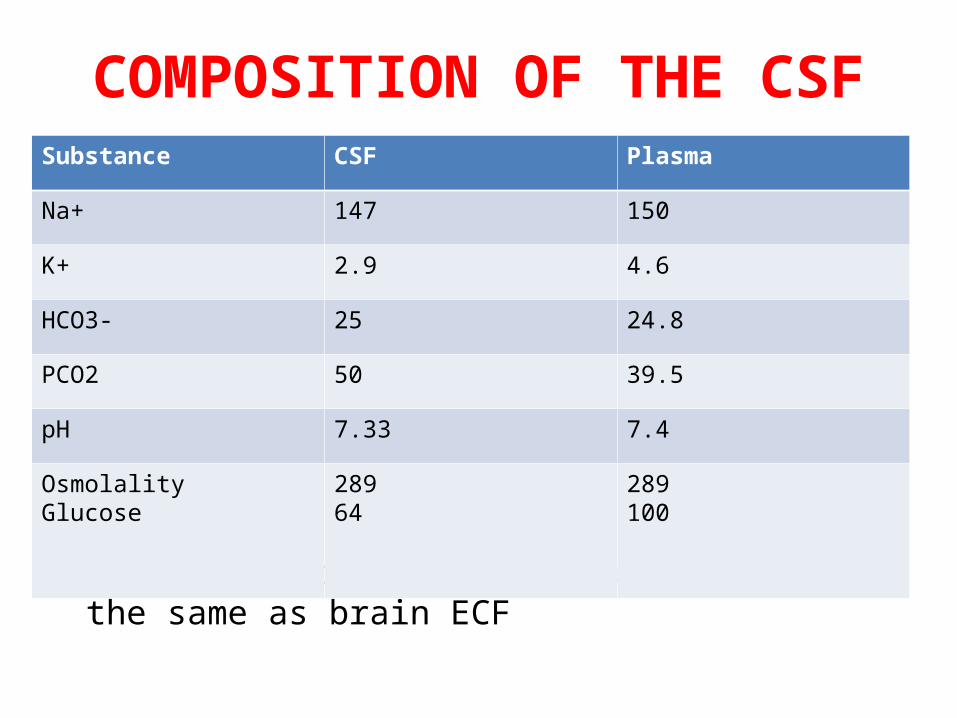
COMPOSITION OF THE CSF
• The composition of CSF is essentially the same as brain ECF
Substance CSF Plasma
Na+ 147 150
K+ 2.9 4.6
HCO3- 25 24.8
PCO2 50 39.5
pH 7.33 7.4
OsmolalityGlucose
28964
289100

CHARACTERISTICS OF CSF
Colour = Clear, transparent fluidSpecific gravity =1.004-1.007Reaction = Alkaline and does not coagulateCells = 0-3/ cmmPressure = 60-150 mm of H2O

Rate of formation:
About 20-25 ml/hour
550 ml/day in adults. Turns over 3.7 times a day
Total quantity: 150 ml:
30-40 ml within the ventricles
About 110-120 ml in the subarachnoid space [of which 75-80 ml in spinal part and 25-30 ml in the
cranial part].
DYNAMICS OF CSF
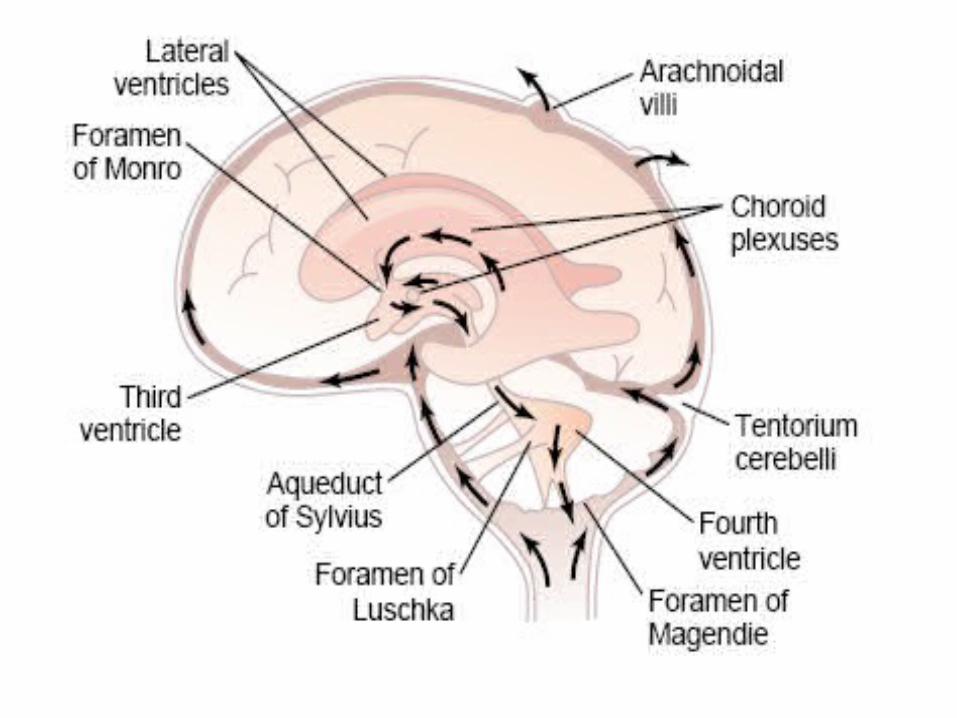
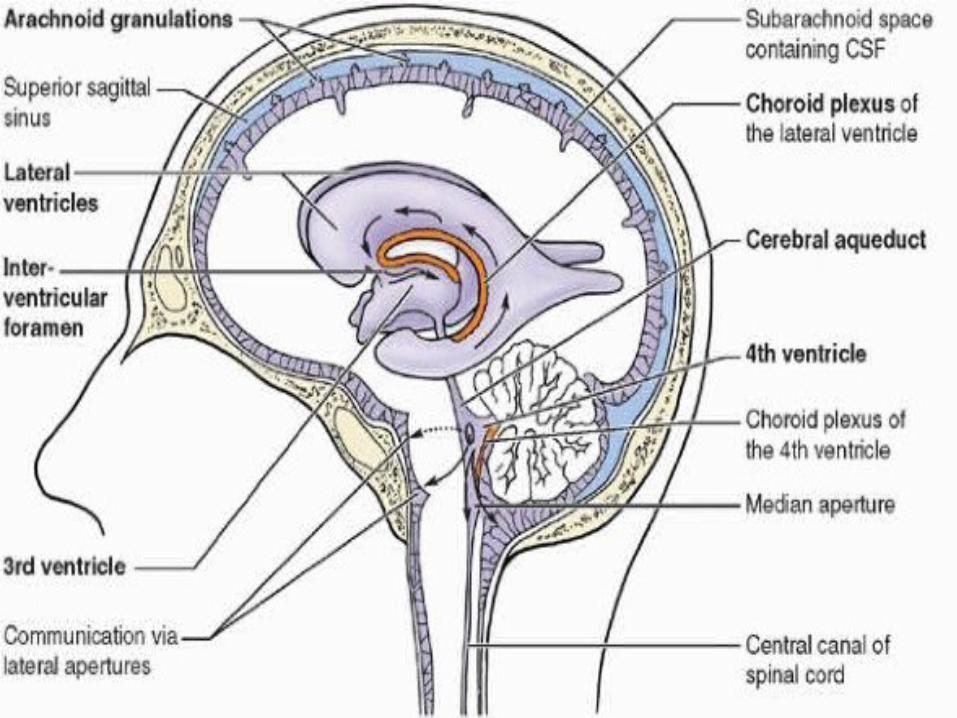
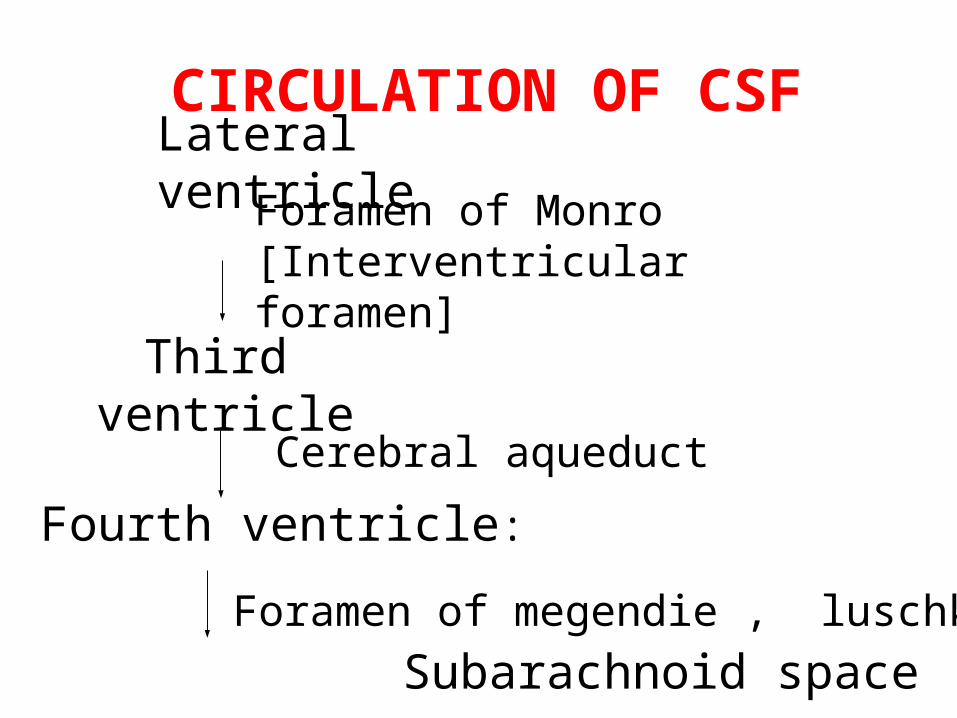
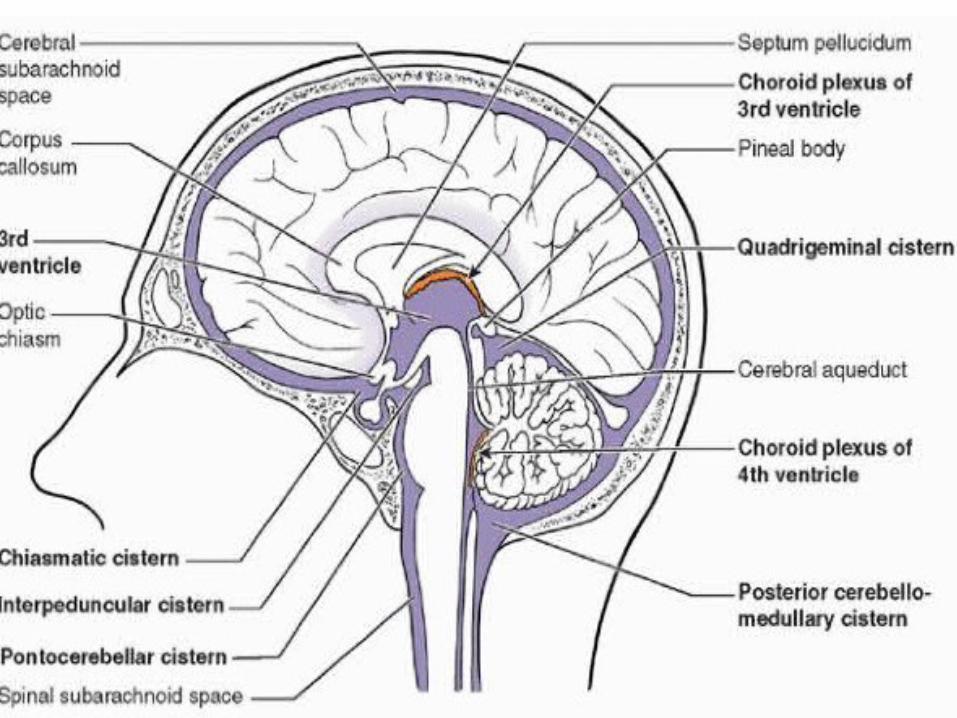
CIRCULATION OF CSFLateral ventricle
Foramen of Monro [Interventricular foramen]
Third ventricle
Subarachnoid space
Fourth ventricle:
Cerebral aqueduct
Foramen of megendie , luschka
ABSORPTION OF CSF
The arachnoidal villi are fingerlike inward projections of the arachnoidal membrane through the walls into venous sinuses.
REGULATION OF ABSORPTION
• Absorption of CSF occurs by bulk flow is proportionate to CSF pressure.:• At pressure of 112 mm (normal average): filtration and absorption are equal.• Below pressure of 68 mm CSF, absorption stops
FUNCTIONS OF CSFA shock absorberA mechanical bufferAct as cushion between the brain and craniumAct as a reservoir and regulates the contents of the craniumServes as a medium for nutritional exchange Transport hormones and hormone releasing factors
Count. Function Remove metabolic wastes from
CNS Serves as pathway for pineal
secretion to reach the pituitary gland.
it protects against acute changes in arterial and venous blood pressure;
it is involved in intra-cerebral transport, ex. hypothalamic releasing factors
BARRIERS IN BRAINThe brain tissue is separated from the plasma by two main barrier
(a) blood–brain barrier (BBB),
(b) blood–cerebral spinal fluid barrier (BCSFB)
.

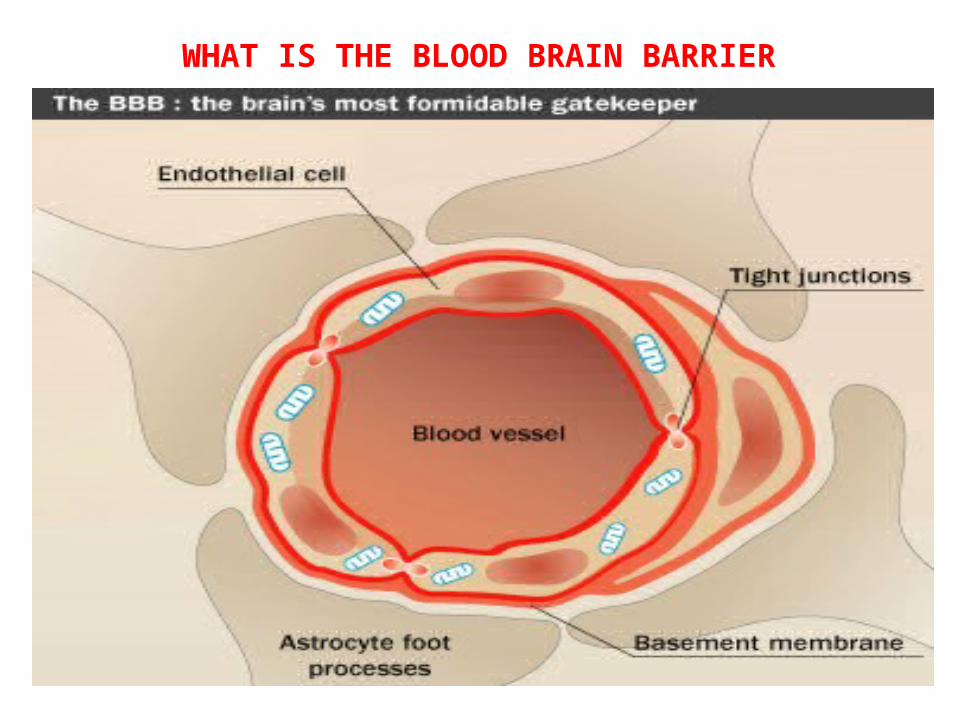
WHAT IS THE BLOOD BRAIN BARRIER
Structural and functional barrier which impedes and regulates the influx of most compounds from blood to brain
Formed by • endothelial cells (BMEC) of
capillary• Basement membrane• Foot process of astrocytes
WHAT IS THE BLOOD BRAIN BARRIER
WHAT IS BLOOD CSF BARRIER
Lumen of blood capillaries separated by ventricle
Endothelial cell of capillaries Basement membrane Choroid epithelial cell with
tight junction
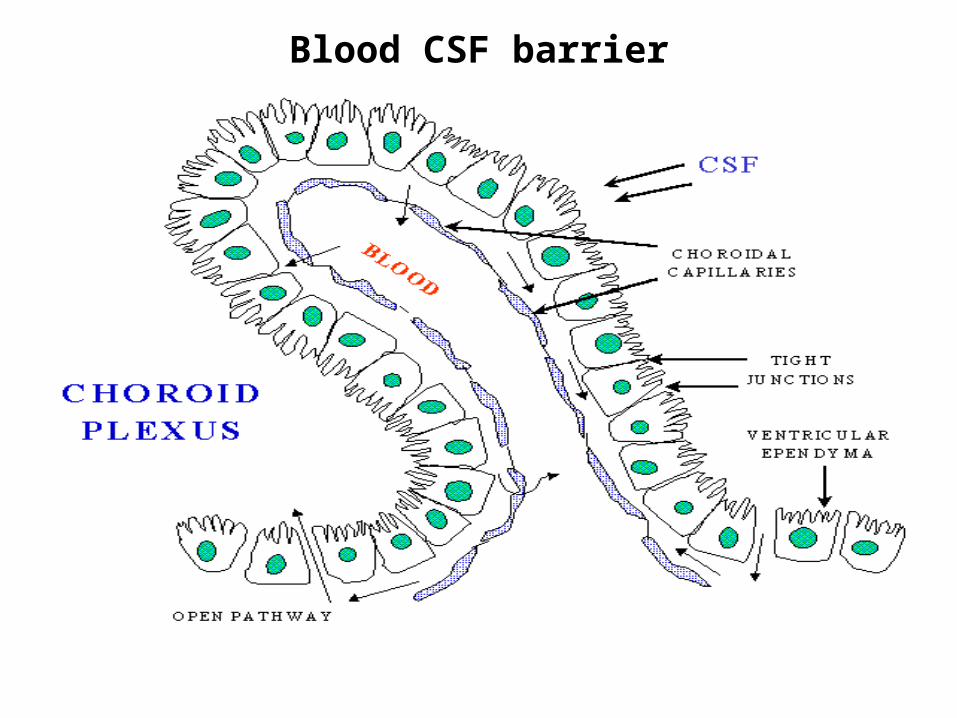
Blood CSF barrier


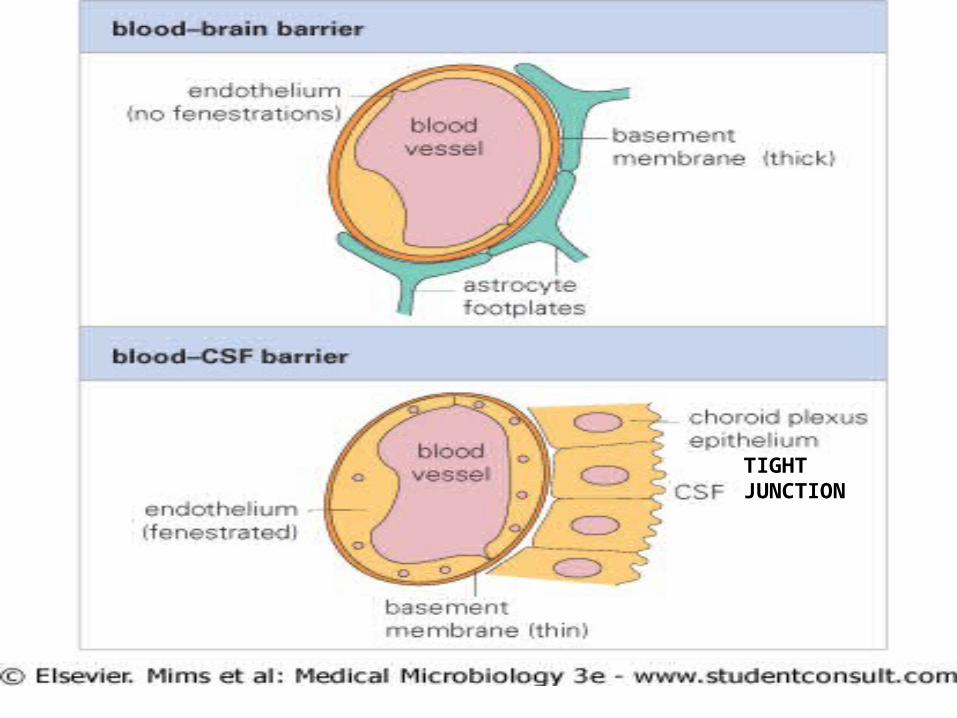
TIGHT JUNCTION
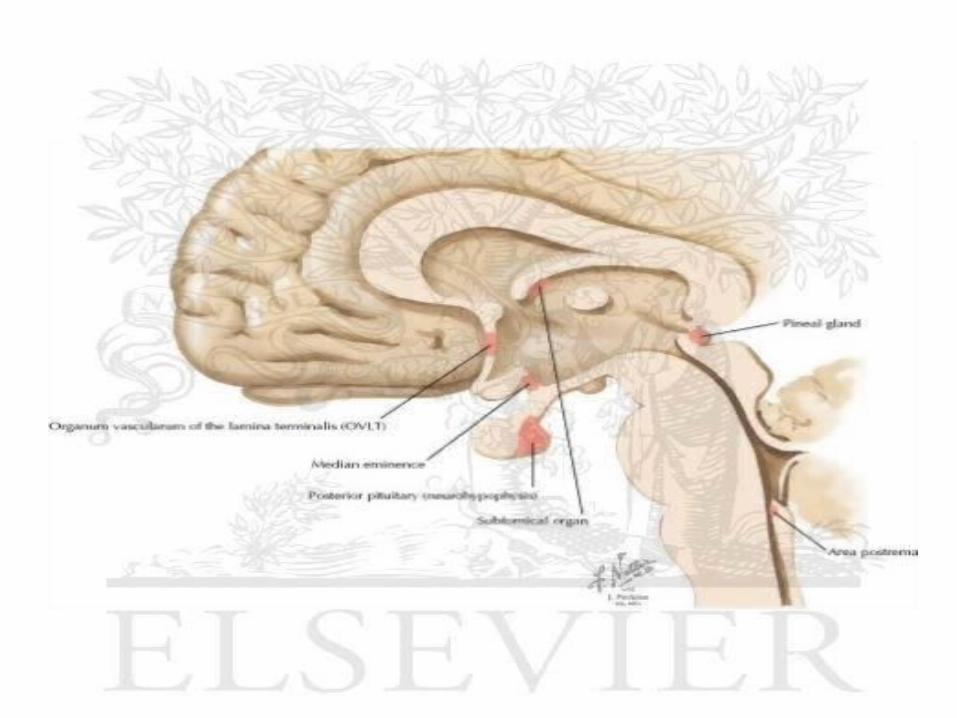
REGIONS OF BRAIN NOT ENCLOSED BY BBB
• Circumventricular organs –area postrema, –median eminence, –neurohypophysis, –pineal gland, –subfornical organ and –lamina terminalis
HYDROCEPHALLUS:• External hydrocephallus or communicating: Large amounts of CSF accumulates when the reabsorptive capacity of arachnoid villi decreases.
• Internal hydrocephallusr or non communicating : occurs when foramina of Luschka & Magendie are blocked or obstruction within ventricular system, resulting in distention of the ventricles.
INTRACRANIAL PRESSURE
• ICP typically means the supratentorial CSF pressure measured in the lateral ventricles or over the cerebral cortex.
• Normal ICP value is 10 mm Hg or130 mm of H2O
• Intracranial hypertension is defined as a sustained increase above 37 mm Hg or 300mm of H2O
Intracranial compartment is a rigid container and consists of three components•a. brain-80% of total volume •b. blood-10% of total volume •c. CSF-10% of total volume An increase in one of these components must be accompanied by an equivalent reduction in another to avoid a rise in ICP
MONRO-KELLIE HYPOTESIS
to maintain a normal ICP, a change in the volume of one compartment must be offset by a reciprocal change in the volume of another compartmentpressure is normally well-controlled through alterations in the volume of blood and CSF
• Initially, an increase in volume is met with little or no change in ICP. Ultimately, there is a point where minute increases in volume can result in a dramatic rise in ICP.
• Compensatory mechanisms that prevent the initial rise in ICP include:a) displacement of CSF from the cranial to spinal compartment,
b) decrease in production of CSF c) increase in absorption of CSF d) decrease in total cerebral blood
volume

Clinical signs and symptoms that suggest increased ICP include:
1) Headache2) Nausea/vomiting3) Blurre vision4) Papilledema 5) Somnolence alter level of
consciousness6) Pupillary dilatation7) Cushing triad• Bradycardia• Hypertension• Irregular respiration
CAUSES• mass effect such as brain tumor, hematoma,
or abscesses • generalized brain swelling , acute liver
failure, heart failure• increase in venous pressure can be due
to venous sinus thrombosis, heart failure, or obstruction of veins
• obstruction to CSF flow and/or absorption can occur in hydrocephalus , , infection, carcinoma, granuloma, hemorrhage or obstruction in sinus
• increased CSF production occurin meningitis, hemorrhage, or choroid plexus tumor
disrupt structural integrity
local edema
increased component in cranium
change in volume of other
brain has limited space to expand
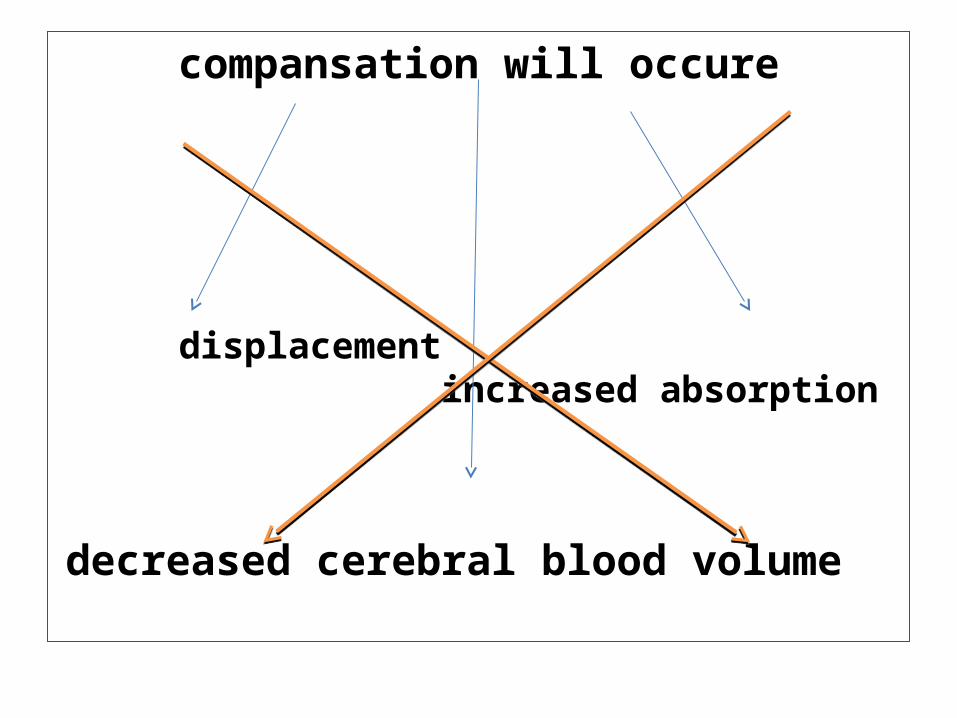
compansation will occure
displacement increased absorption
decreased cerebral blood volume

ICP began to rise
change in level of consciousness
reduce cerebral further blood flow swelling

ischemia cushing reflex vasomotor center
increased arterial pressure to
compensate increased ICP
bradycardia irregular respiration hypertension
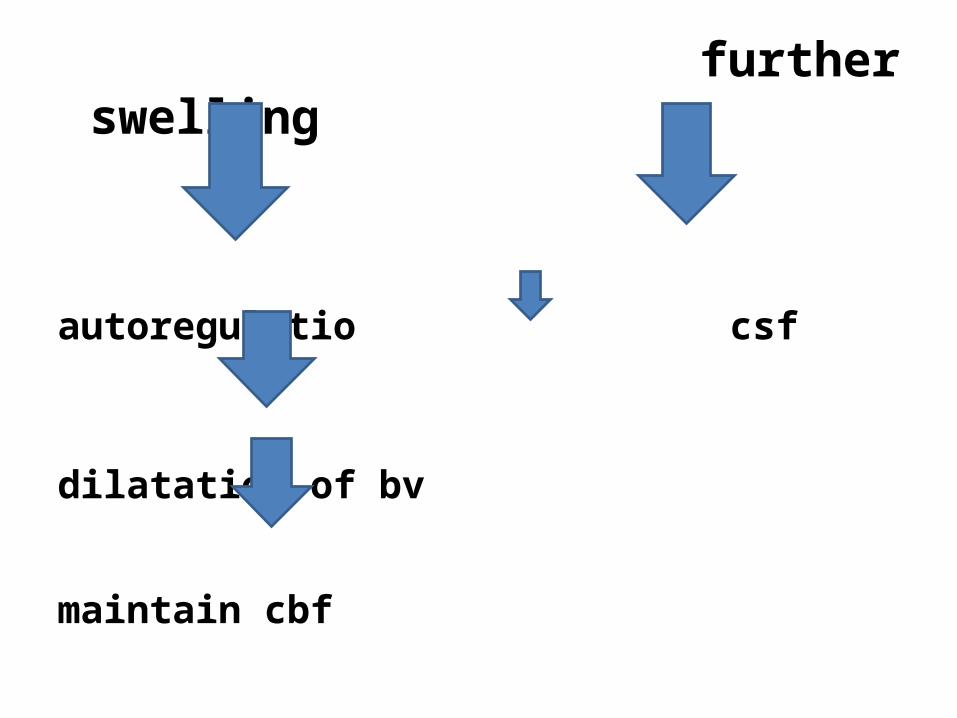
further swelling
autoregulatio csf
dilatation of bv
maintain cbf

ineffective decompansationautoregulation
shifting of brain tissue from heigher pressure to low pressure
herniation

ISCHEMIA DISTURBE VITAL CENTER
CESSATION OF CBF COMA
PERMENANT NEUROLOGICAL DEATH