challenges of new and emerging infections - jst · challenges of new and emerging infections...
TRANSCRIPT

Challenges of New and Challenges of New and emerging infectionsemerging infections
Prof.N.K.Ganguly,Director General, ICMR2nd Asian Science and Technology Forum,
Tokyo, Sept. 8th 2006

MRCIRMS
NICED
TRC
EVRC RMRC
RMRCCRME
NIE
VCRC
CJIL
RMRI
NARINIV
DMRCRMRC
RMRC
ICMR Institutes Researching in Communicable Diseases
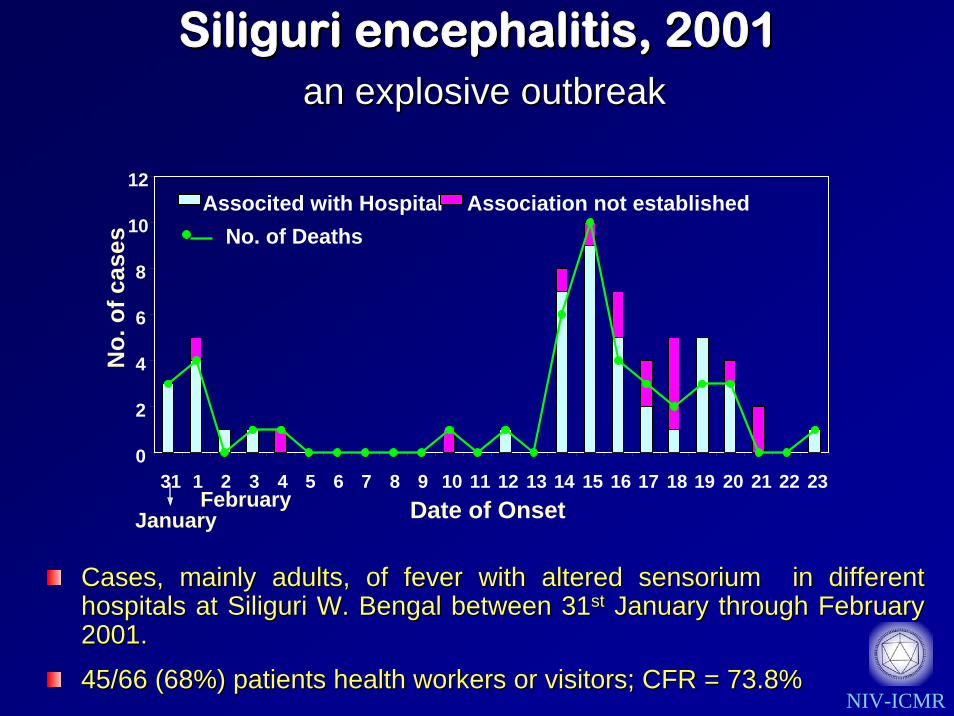
Siliguri encephalitis, 2001Siliguri encephalitis, 2001an explosive outbreakan explosive outbreak
Cases, mainly adults, of fever with altered sensorium in differCases, mainly adults, of fever with altered sensorium in different ent hospitals at Siliguri W. Bengal between 31hospitals at Siliguri W. Bengal between 31stst January through February January through February 2001.2001.
45/66 (68%) patients health workers or visitors; CFR = 73.8%45/66 (68%) patients health workers or visitors; CFR = 73.8%NIV-ICMR
0
2
4
6
8
10
12
31 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23Date of Onset
No.
of c
ases
Associted with Hospital Association not establishedNo. of Deaths
JanuaryFebruary

Nipah BanSILI-N2SILI-N1
SILI-N4SILI-N5
SILI-N3Nipah3 MalaysiaNipah6 Malaysia
Nipah1 MalaysiaNipah2 Malaysia33
3099
4562
88
0.005 Nipah2 Malaysia
NIPAH virus etiology
Nipah1 MalaysiaNipah3 Malaysia
Nipah1 BanNipah2 Ban
SILI-M177
100
0.005
• N gene amplified from 5/6 urine samples. (99.95%, & 97.11% homology) • M gene amplified in 3/6 samples (98.91% and 94.37% homology)
Nipah virus etiology confirmedChadha et al., 2005 EID
• Negative for antibodies to JE, WN, Den, Measles
CDC collaboration• 9/17 cases +ve IgM abs, 10/17 +ve for IgG abs for Nipah virus

Clinical featuresClinical features
Acute fever, mild to high grade (100Acute fever, mild to high grade (100--104 F)104 F)
Pediatric age group below 15 yrsPediatric age group below 15 yrs
Altered sensorium, Altered sensorium, camatosecamatose condition leading to death in condition leading to death in 11--2 days2 days
High mortality (CFR ~ 60%)High mortality (CFR ~ 60%)
No neck rigidity, No neck rigidity, KernigKernig’’ss sign absentsign absent
Malnourished children belonging to low socioMalnourished children belonging to low socio--economic economic class and poor hygieneclass and poor hygiene
Saharanpur outbreak 2002-04

A total of 40 cases with 25 deaths A total of 40 cases with 25 deaths (CFR (CFR 63%) 63%) reported from 12reported from 12--1010--02 to 1202 to 12--1212--0202
A total of 34 cases with A total of 34 cases with CFRCFR 80% 80% reported during Septreported during Sept--Oct 2003.Oct 2003.
During 2004, a total of 158 cases with 113 During 2004, a total of 158 cases with 113 deaths deaths (CFR 72%)(CFR 72%) reported between reported between OctoberOctober--December.December.
A few cases positive for viruses like A few cases positive for viruses like adenaden, , enteroentero etc.etc.
Saharanpur outbreak 2002-4
Negative for all viruses in culture and PCR
Diagnosis--Inconclusive
EM: Adeno-like particle from CSF

SARS Outbreak, 2003
MolecularPolymerase Chain Reaction (PCR)
Cell cultureElectron Microscopy
1 2 3 4 5 6 7 8 9 10 11
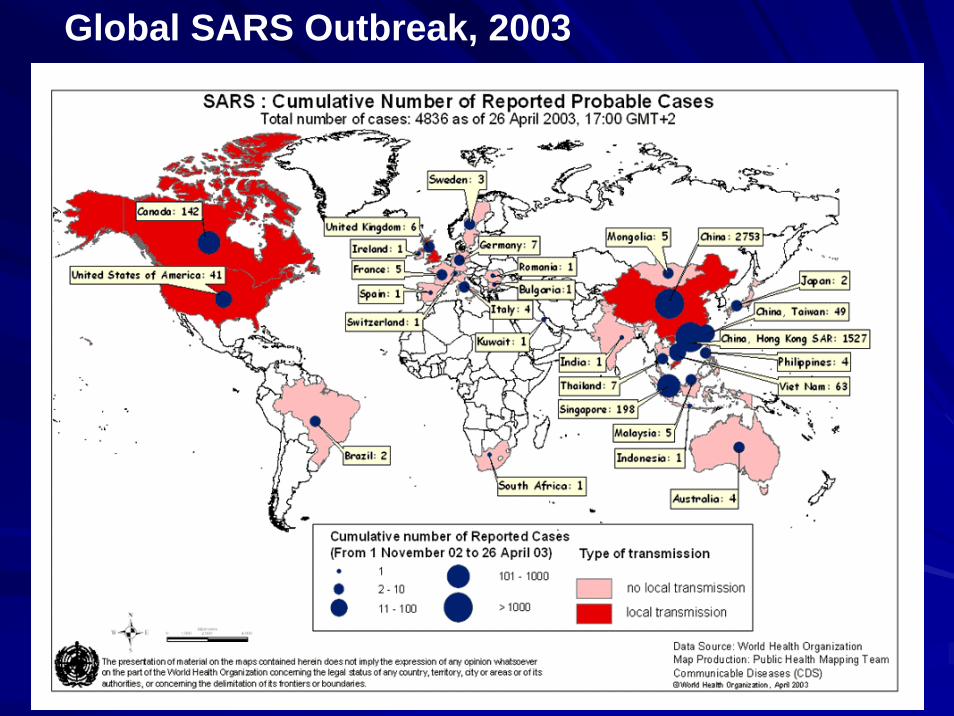
Global SARS Outbreak, 2003

June to September 2003, 319 cases of encephalitis with 174 deaths (CFR 54.5%) were reported from 11 districts of A. P.
Children below 14 years age, predominantly belonging to low socio-economic group, rural areas
Total chaos and panic as onset of disease was abrupt, 85% of deaths within 24 hours of hospitalization
All samples negative for known causes of encephalitis
Chandipura encephalitis outbreak, AP 2003

virus isolations:10strains in RD, Vero, MDCK cell lines and infant mice
Laboratory Studies
FA: CHP viral antigen in brain cells confirmed
PCR: CHP G gene primers amplified RNA from isolates and clinical samples. 98% homology with 1965 isolate.
Electron microscopy: Bullet shaped particles and helical nucleocapsid - typical Rhabdoviruse.
Identifications: Chandipura virus by CF and NT and PCR

Isolations, PCR and serology suggested involvement of CHP virus in these encephalitis cases
Subclinical infection recorded
Chandipura virus was found responsible for the outbreak in AP and adjoining districts of Maharashtra
Rao et al 2004; Lancet

An outbreak among tribals from Chotaudepur and Kawat Talukas in Vadodara dist and 1 taluka in Panchmahal district.
26 cases with 17 deaths (CFR 65%) between 9-6-04 to12-7-04.
80% of the deaths within 24 hours of hospitalization.
Chandipura encephalitis in Gujarat, 2004

CHP sequences: closely related to prototype strain (1965) and Andhra Pradesh (2003) isolates.
It was concluded that the etiological agent was Chandipura virus
Vadodara2Vadodara84
Vadodara125Vadodara103
Vadodara14Vadodara109
AP18RAP31M
Vadodara6Vadodara115AP27M
Vadodara112AP09R
AP60VMAH6514V96
5269
4943
76
4935
5033
55
31
0.01
Clinical samples –ve for JE, West Nile, Dengue and Paramyxovirus
Virus isolations : one in RD, PS Cell lines and in suckling mice.
PCR: CHP RNA in 9/20 (45%) acute serum samples.
ELISA: 2 patients +ve for CHP anti IgM abs.
Seroconversion: 1 case –ve for IgM in first sample turned +ve in second sample
Laboratory investigations
Chadha et al 2005; American J Trop Med Hyg

Chandipura encephalitis in A P, Chandipura encephalitis in A P, 20052005
PeriodPeriod 44thth May May –– 3131stst
AugustAugustTotal recorded Total recorded deaths/ casesdeaths/ cases
32/54 32/54 (59.3%)(59.3%)
Serum samples Serum samples from probable from probable cases cases ##
35 (65%)35 (65%)
Probable cases Probable cases deaths/casesdeaths/cases
21/35 (60%)21/35 (60%)
# encephalitis cases in age group < 15 yrs, fever of less than 5days at admission, and CNS involvement
Etiology was confirmed as Chandipura virus by isolation, seroconversion and PCR
Warangal, Karimnagar, Khamam and Adilabad districts

In India, Isolated from sandflies in1970 in Aurangabad dist. of Maharashtra and 3 isolations from AP
Isolations from hedge hog in Nigeria, and sand flies in Senegal, West Africa,1992.
In sri Lanka, 2/115 monkeys positive for abs
Sandflies are probable vector & extra human reservoir may be present
CHP: Vector distribution, ecology
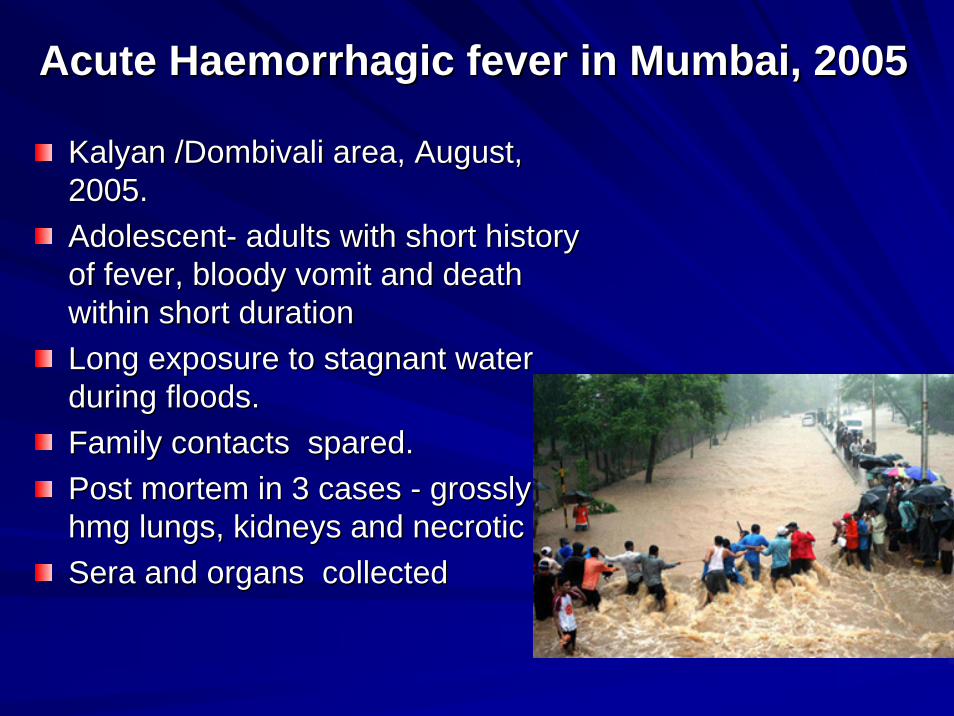
Acute Acute HaemorrhagicHaemorrhagic fever in Mumbai, 2005fever in Mumbai, 2005
KalyanKalyan //DombivaliDombivali area, August, area, August, 2005. 2005. AdolescentAdolescent-- adults with short history adults with short history of fever, bloody vomit and death of fever, bloody vomit and death within short duration within short duration Long exposure to stagnant water Long exposure to stagnant water during floods.during floods.Family contacts spared.Family contacts spared.Post mortem in 3 cases Post mortem in 3 cases -- grossly grossly hmghmg lungs, kidneys and necrotic liver. lungs, kidneys and necrotic liver. Sera and organs collectedSera and organs collected

Laboratory investigationsLaboratory investigations
Samples inoculated in suckling mice and cell culture Samples inoculated in suckling mice and cell culture -- no no isolations.isolations.
DengueDengue1of 51 sera samples positive 1of 51 sera samples positive All sera from 12 dead cases were All sera from 12 dead cases were negaivenegaive ..
LeptospiraLeptospira3/12 cases positive for 3/12 cases positive for LeptospiraLeptospira by MAT; PCR for by MAT; PCR for LeptospiraLeptospira negative. negative.
HantaanHantaanAll sera from 12 dead cases were negative.All sera from 12 dead cases were negative.PCR for Hantaan using PM organs were negative.PCR for Hantaan using PM organs were negative.Sera from contacts of dead cases +Sera from contacts of dead cases +veve for IgM abs for for IgM abs for Hantaan by commercial kits. Hantaan by commercial kits.
No viral etiology; Leptospirosis??

• Avian Influenza outbreak recorded in Maharashtra
• Poultry census, culling and tracing missing poultry
• Total destruction of backyard poultry
• Following outbreak in poultry >500 samples from handlers, cullers, contacts collectedOutbreak of Avian Influenza in Maharashtra, 2006

Rapid Molecular Tools in Virus Rapid Molecular Tools in Virus Identification: Avian FluIdentification: Avian Flu
NASBA results detecting very low amount of H5N1 RNA
Virus detection by Real time PCR
Real Time PCR System
State-of-artNASBA Platform
H5N1 gene of avian influenza virus detected by RT-PCR

Samples from suspected cases were processed for H5 and N1 PCR; all negative
All samples processed by Real-Time PCR/ NASBA –negative except 1 environmental sample that gave positive signal for N1 gene in NASBA
Samples were inoculated in eggs/ MDCK cell lines-no isolations
No sample met the criteria-hence all negative
Avian Influenza in Humans, 2006

Sudden onset of fever and crippling migrating arthralgias,which may last for a few days to months.
Papular or maculopapular skin rash may occur, typically on the trunk and limbs.
Normally, self resolving disease
Complications include-
Mild hemorrhagic manifestations
Meningo-encephalitis, Encephalitis
Maternal-foetal transmission
The relation between Chik and death is still under investigation.
Chikungunya outbreak, 2005-06

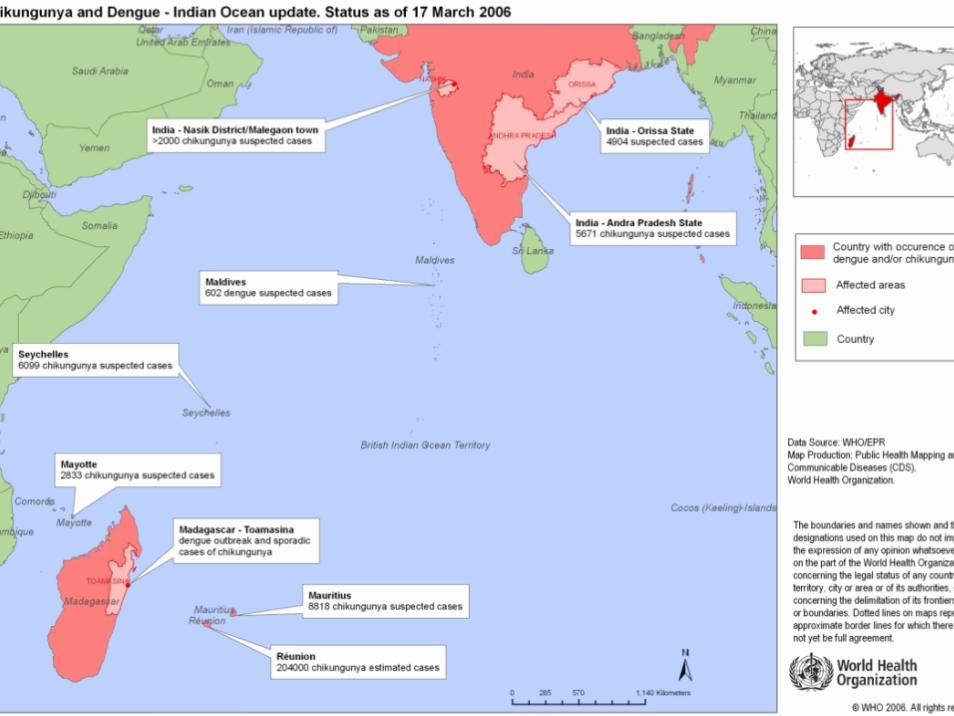

Chikungunya virus activity in India
60s to 80s 2005-06
Gujarat
Rajasthan
Madhya Pradesh
Maharashtra
Andhra Pradesh
Karnataka
TamilNaduKerala
Orissa

Chikungunya Laboratory Diagnosis
Virus isolationsImmunofluorescence Assay ( IFA )
RT-PCR for genomic detectionMAC ELISA
1.75 kb
2.0 kb
2.1 kb 1.3
kb
365 bp

Sporadic activity in India (2000-2004)
PlacePlace MACMAC--ELISAELISA--PositivePositive
HI PositiveHI Positive PCR PCR positipositiveve
KolhapurKolhapur 3/1203/120 2/112/11 ++
NandedNanded 2/112/11 1/161/16 --
GadchiroliGadchiroli 2/332/33 4/174/17 ++
PCMCPCMC 3/823/82 1/101/10 --
SuratSurat 1/1161/116 0/280/28 --
KeralaKerala 7/947/94 NDND NDND
HydrabadHydrabad 3/473/47 NDND NDND
Total no. of samples tested by MAC-ELISA for CHIK Infection [n=865]

ChikChik-- vector in Indiavector in India
• Ae aegypti is the main vector
• Virus is transmitted by bite of female mosquitoes
• Primarily a daytime feeder• Lives around human
habitation• Breeds in artificial
containers
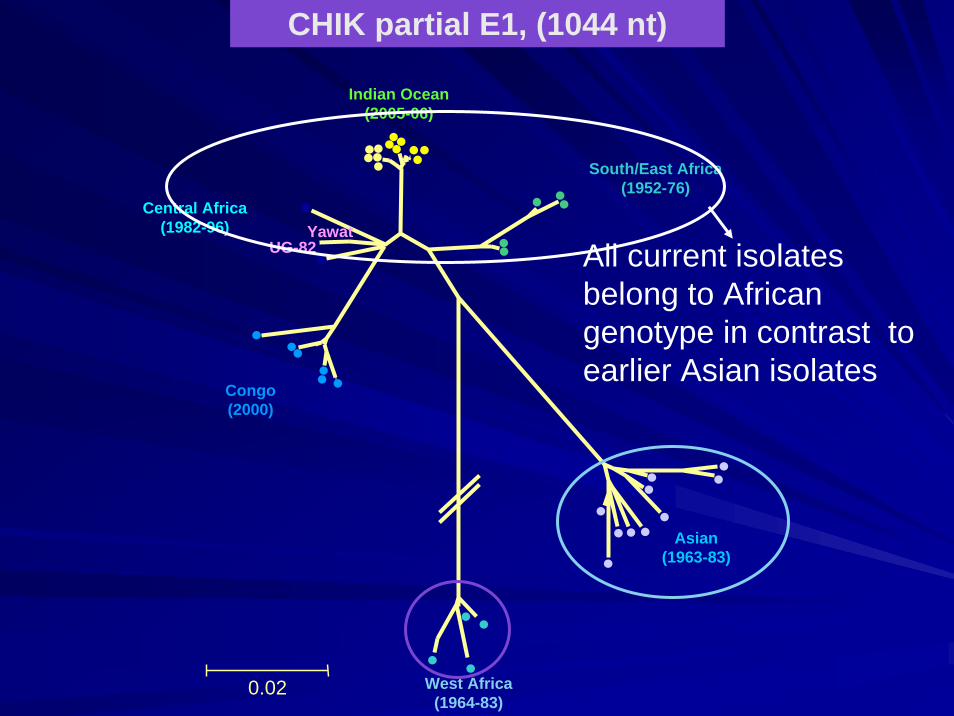
0.02
YawatCentral Africa
(1982-96)
Indian Ocean (2005-06)
South/East Africa(1952-76)
Asian(1963-83)
West Africa(1964-83)
Congo(2000)
UG-82
CHIK partial E1, (1044 nt)
All current isolates belong to African genotype in contrast to earlier Asian isolates
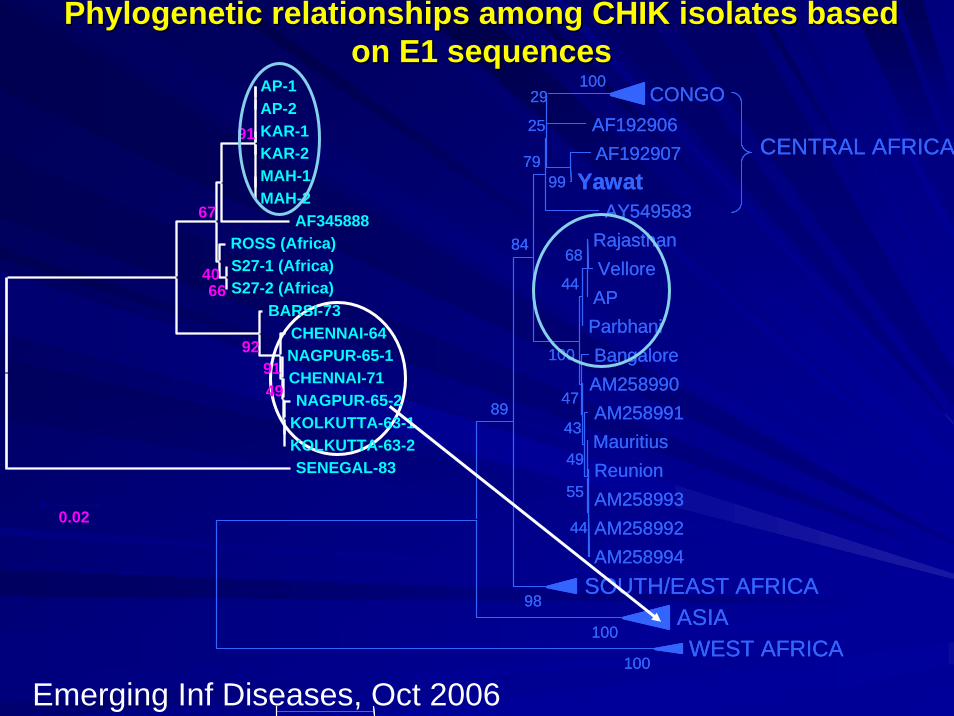
PhylogeneticPhylogenetic relationships among CHIK isolates based relationships among CHIK isolates based on E1 sequenceson E1 sequences
CONGOAF192906AF192907
YawatAY549583
CENTRAL AFRICA
RajasthanVelloreAPParbhaniBangaloreAM258990AM258991MauritiusReunionAM258993AM258992AM258994
SOUTH/EAST AFRICAASIAWEST AFRICA
100
100
100
98
99
89
29
25
79
8468
44
100
47
43
49
55
44
CONGOAF192906AF192907
YawatAY549583
CENTRAL AFRICA
RajasthanVelloreAPParbhaniBangaloreAM258990AM258991MauritiusReunionAM258993AM258992AM258994
SOUTH/EAST AFRICAASIAWEST AFRICA
100
100
100
98
99
89
29
25
79
8468
44
100
47
43
49
55
44
AP-1AP-2KAR-1KAR-2MAH-1MAH-2
AF345888ROSS (Africa)S27-1 (Africa)S27-2 (Africa)
BARSI-73CHENNAI-64NAGPUR-65-1CHENNAI-71NAGPUR-65-2
KOLKUTTA-63-1KOLKUTTA-63-2SENEGAL-83
4991
92
6640
67
91
0.02
Emerging Inf Diseases, Oct 2006
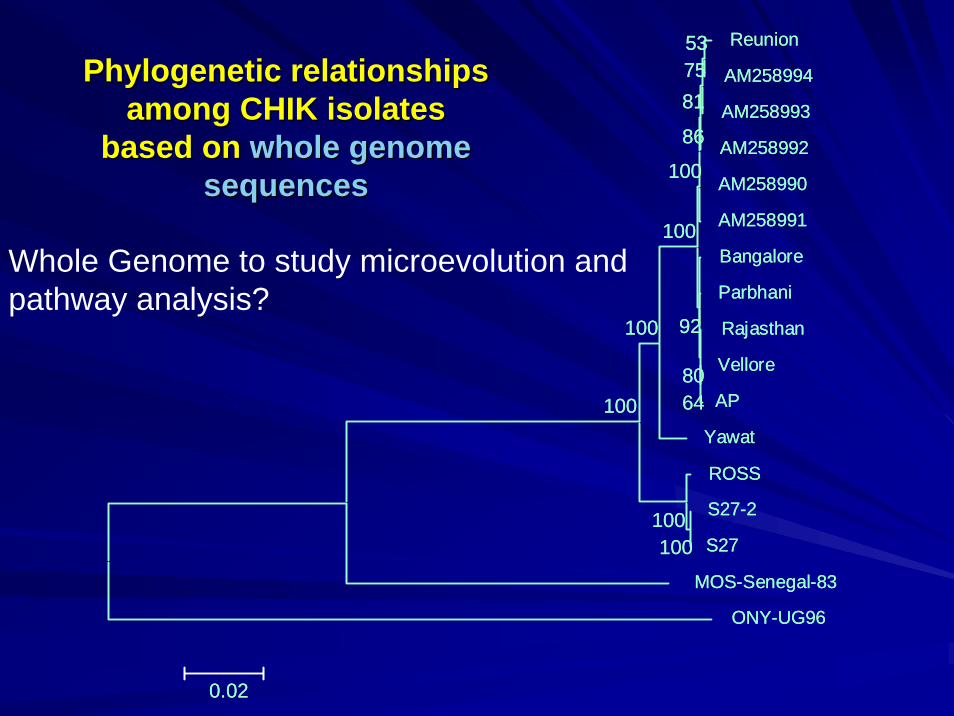
Reunion
AM258994
AM258993
AM258992
AM258990
AM258991
Bangalore
Parbhani
Rajasthan
Vellore
AP
Yawat
ROSS
S27-2
S27
MOS-Senegal-83
ONY-UG96
100100
100
100
537581
86
100
100
6480
92
0.02
Reunion
AM258994
AM258993
AM258992
AM258990
AM258991
Bangalore
Parbhani
Rajasthan
Vellore
AP
Yawat
ROSS
S27-2
S27
MOS-Senegal-83
ONY-UG96
100100
100
100
537581
86
100
100
6480
92
0.02
PhylogeneticPhylogenetic relationships relationships among CHIK isolates among CHIK isolates
based on based on whole genome whole genome sequencessequences
Whole Genome to study microevolution and pathway analysis?
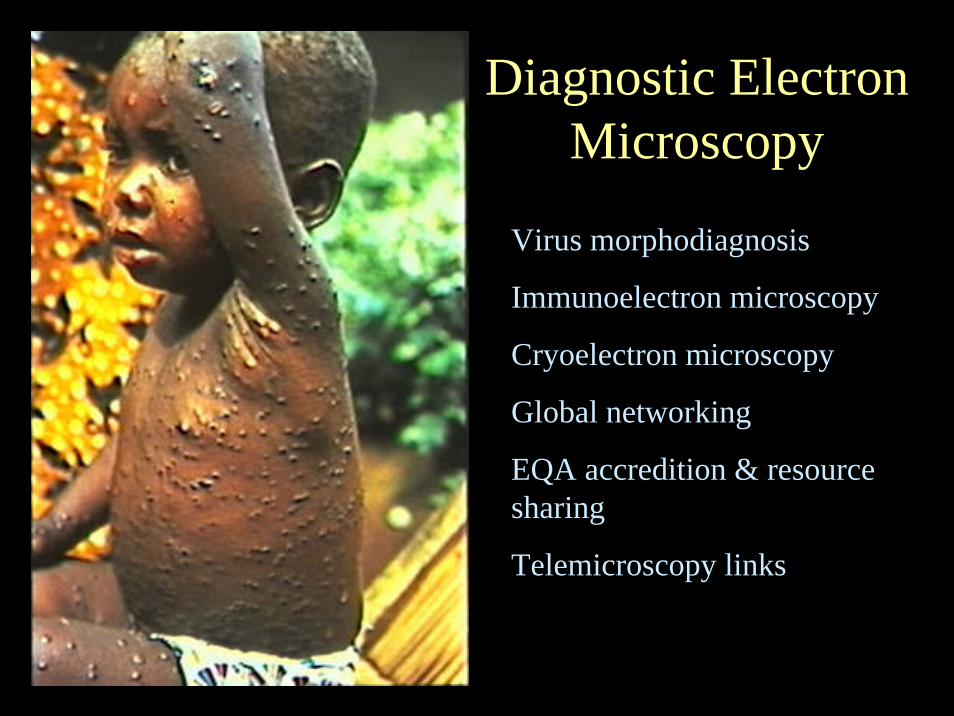
Diagnostic Electron Microscopy
Virus morphodiagnosis
Immunoelectron microscopy
Cryoelectron microscopy
Global networking
EQA accredition & resource sharing
Telemicroscopy links

Poxviruses
UAcUAc AMdateAMdate PTAPTA
Lesion from farmer’s hand direct TEM imaging of vesicular fluid
Parapoxirus
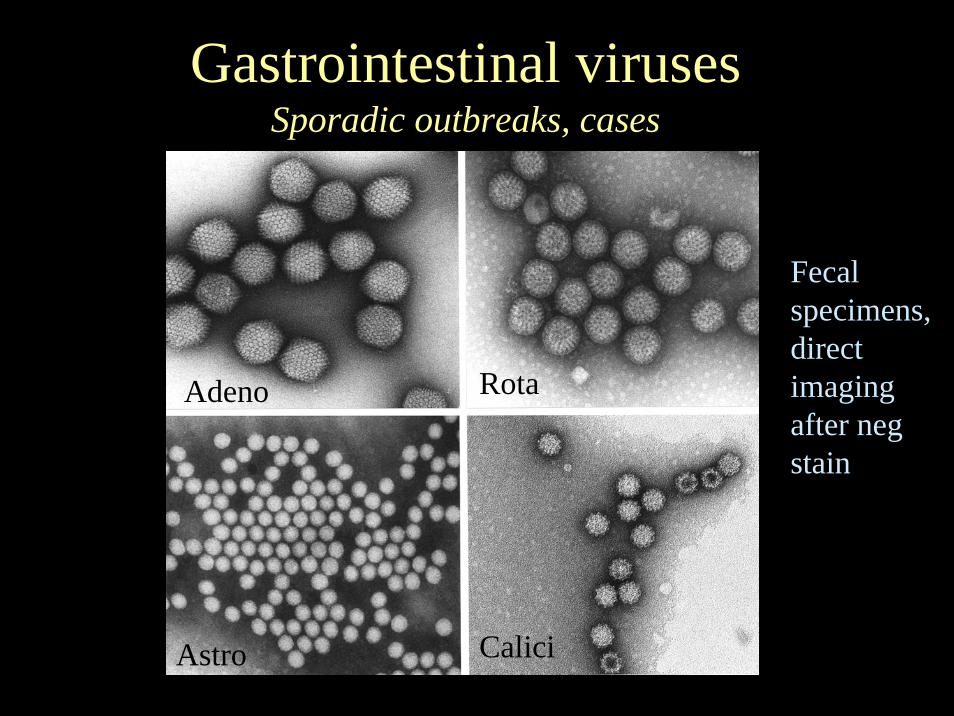
Gastrointestinal virusesSporadic outbreaks, cases
Adeno Rota
Astro Calici
Fecal specimens, direct imaging after negstain

Sapporo and Noroviruses

Rapid ultrathin sectioning K4M
CPE+ cultures BHK21 cells
TEM characterization of some unclassified viruses from India
A Bunyavirus
Chittoor virus

0.1
SAB1VP1KEKZK00018
KAGBG00024KABLK00002
KAGBG00022KAKPP00004
UPMRT01029UPMRT02021
UPMRT01041UPMRT01038
UPMTR02012UPMRT02017
UPMRT02056UPPIL02044
UPMZN02103UPMZN02076
UPMZN02055UPMZN02044UPMZN02084
UPMRT02016UPMRT02002
UPMZN02035UPMRT01037
UPMRT01108KABLY03006
UPMRT02038
Introduction of wild poliovirus type 1 from UP to Karnataka, 2003
Enterovirus Research Centre, Mumbai ICMR, New Delhi
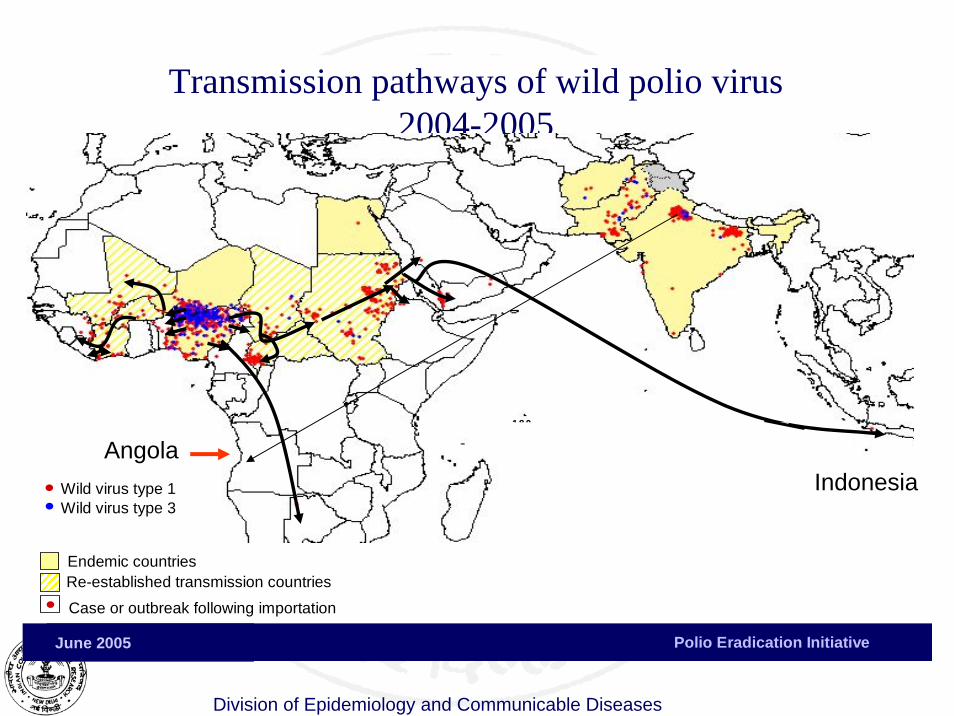
Division of Epidemiology and Communicable Diseases
Polio Eradication Initiative June 2005
Transmission pathways of wild polio virus 2004-2005
Case or outbreak following importation
Endemic countries
Wild virus type 1Wild virus type 3
Re-established transmission countries2 0 0 2
11
162
45
0 0 0 114
5
0
20
40
60
80
100
120
140
160
180
04
-De
c
05
-Ja
n
05
-Fe
b
05
-Ma
r
05
-Ap
r
05
-Ma
y
SAA
YEMINO
AngolaIndonesia
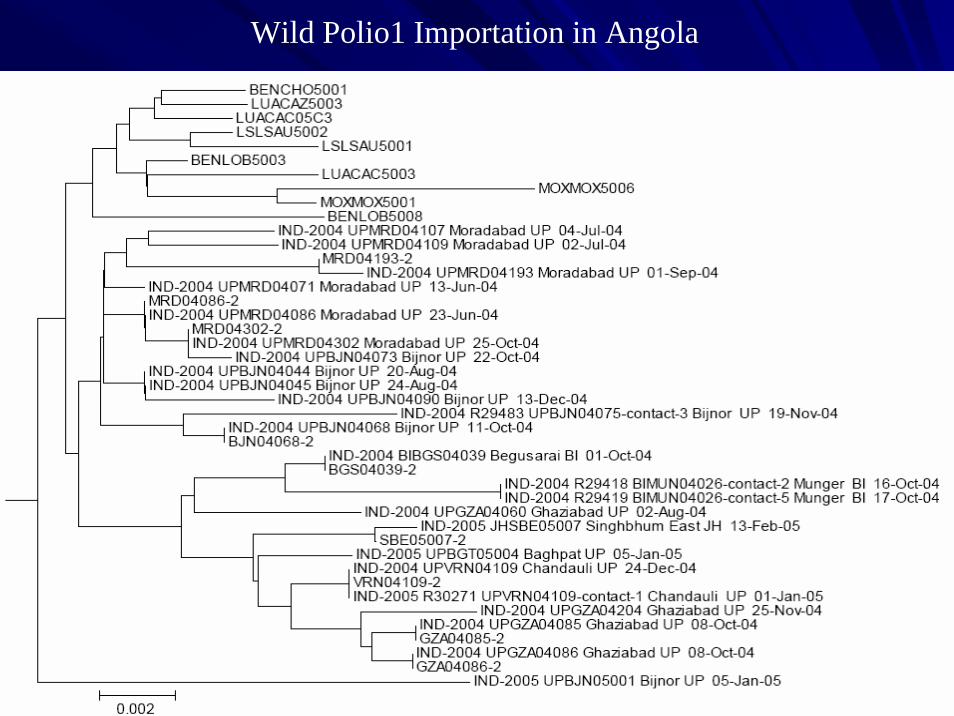
Wild Polio1 Importation in Angola
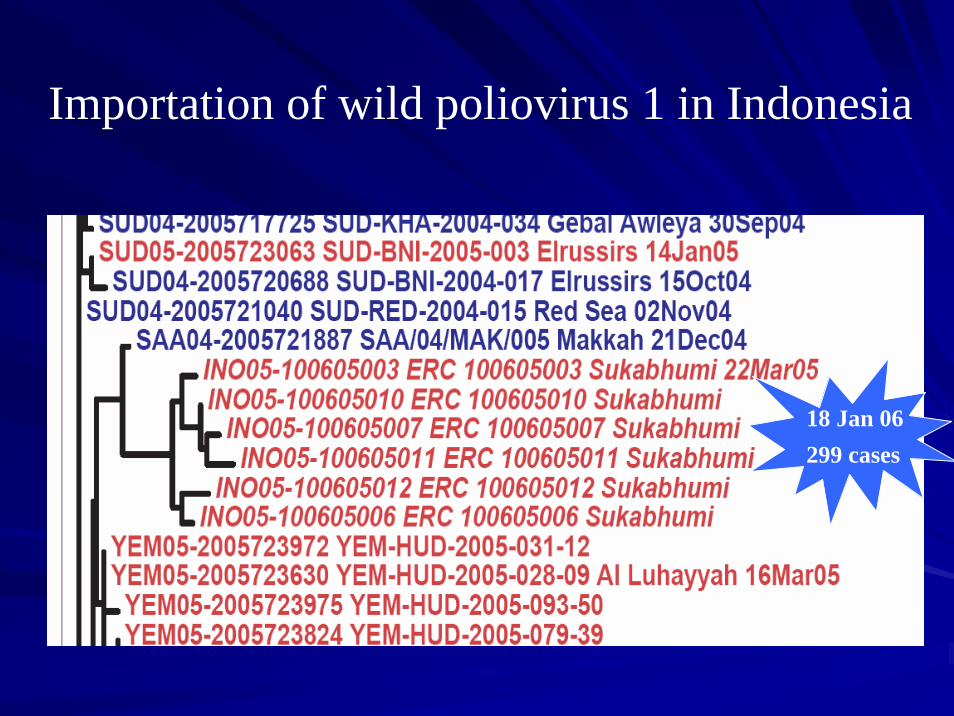
Importation of wild poliovirus 1 in Indonesia
18 Jan 06299 cases

M
F
G
14
16 G ward
M warda

International collaboration in Emerging International collaboration in Emerging Infectious Diseases and Disease Infectious Diseases and Disease
SurveillanceSurveillance
Sharing of informationSharing of informationBiological Material for R&DBiological Material for R&DCollaborative researchCollaborative researchSite preparation for clinical trialsSite preparation for clinical trialsInvestigation of outbreaksInvestigation of outbreaksInfrastructure strengthening esp. for labs of Infrastructure strengthening esp. for labs of appropriate appropriate biosafetybiosafety levelslevelsTraining for managing outbreaks and Training for managing outbreaks and biosecuritybiosecuritylevelslevelsWorkshopsWorkshops
RecommendationsRecommendationsIncreasing research capacities and capabilities of Increasing research capacities and capabilities of developing countries to deal with emerging infections.developing countries to deal with emerging infections.Human networking as important as technology based Human networking as important as technology based networking to address emerging infections.networking to address emerging infections.Need to develop networking between research Need to develop networking between research organizations and institutions involved in emerging organizations and institutions involved in emerging infectionsinfectionsA regional network of networks would help in sharing of A regional network of networks would help in sharing of informationinformationICMR to be nodal agency for emerging and reICMR to be nodal agency for emerging and re--emerging emerging infections in Indiainfections in India