challenges & solutions of setting up an anaesthesia assessment clinic anne kwan mbbs fhkca...
TRANSCRIPT
Challenges & Solutions of setting up an Anaesthesia Assessment Clinic
Anne Kwan
MBBS FHKCA FHKAM(Anaesthesiology)
FANZCA FFPM ANZCA Dip Pain Mgt (HKCA) Dip Acup M Pal Care
Chief of Service
Department of Anaesthesia, Pain Medicine and Operating Services
United Christian Hospital
HONG KONG
Anaesthesia Assessment Clinic
is not just
Day Surgery / Same Day Admission PAC
All elective cases

History
1909 - Nicole presented to BMA the results of 8988 operations on outpatients performed at the Glasgow Royal Hospital for Sick Children between 1899 and 1909
1916 - Waters opened the Down-Town Anaesthesia Clinic in Sioux City, Iowa for minor surgery and dental cases
1937 - Hertzfelt reported on more than 1000 outpatient paediatric hernia repairs performed with the use of GA
1962 - a formal ambulatory surgical programme was initiated at the University of California at LA
1974 - Federated Ambulatory Surgery Association was established
1989 - 1000 free standing ambulatory surgery centres in US
Aims of anaesthesia assessment
To assess & optimised patient’s medical condition To explain the different types of anaesthesia which can be
used for the operation To describe the relative risks and complications of the ana
esthesia chosen To briefly explain how the intended anaesthesia is conduc
ted To explain to patient the available clinical studies If patient is recruited in a clinical study, adequate explana
tion must be given and written consent must be obtained To ally patient’s anxiety by adequate explanation and pre
scription of premedications

Aims (cont)
To remind patient to take premedications if they have been prescribed
To remind patient of fasting time To select suitable form of postoperative a
nalgesia for the patient To educate patient in the use of postopera
tive analgesia To warn patient of possible postoperative
follow up call / visit
Benefits of Preoperative Assessment Clinic (PAC)
Ideal setting for anaesthetic assessment
Facilitate SOPD medical consultation
Decrease of inpatient length of stay (cost, hospital-acquired infection, psychological stress)
Facilitate operation scheduling
Ease immediate preoperative preparation
Reduce cancellation of operation
Essential ingredients
Anaesthetists Anaesthetic / PAC nurses Screening mechanism (patient/operation type, infectio
n) PAC protocols Physical set up Information technology smart Investigation facilities on site Fast tract consultation arrangements Review mechanism streamline Administrative guidelines Audit / review

The world trend
70-90% day surgery
Definition of day surgery
9 to 6 pm8 to 11 pm23 hoursRound the clock as long as < 24 hours
What is the situation in Hong Kong
90% of inpatient services provided by HA
20 operating theatre suites (230 Operating Rooms)
2 day centres as there is no inpatient facilities - TWEH, HKEH
Some have limited number of inpatient beds - AHNH, OLMH, TSKH, TWH, POH
2 centres only deal with high complexity cases - GH/QMH, PWH

HA has been monitoring day surgery or same day admission cases hoping to have benchmarking for healthcare efficiency
The following data are collected regularly and displayed at the MIPO site



For those hospitals or sites with suitable cases for day surgery or same day admit, what are the barriers?
Barriers:Poor education levelPoor home environment Patient staying alonePatient coming from old aged home
Culture
Hospital a safer placeSome changes after SARS
Incentives for patient / family
Hospital stay around HK$100 per day all inclusive
New case consultation at SOPD - HK$100
Old case consultation HK$60
Each drug item HK$10
Consultation at AED HK$100
Community Nurse visit HK$44
Incentives for surgeons
Funding based on number of inpatient beds
Casemix model not encouraging day surgery
Hard to streamline patient care path as day cases (admission, consultation, investigation, rescheduling)

Misunderstanding / fear
Patient screening not easy
Post operative complications attract complaints / medical legal issues
Hard to overcome old habits
Respect tradition

History of Day Surgery at UCH
April 1992 - general surgical cases
Nov 1992 - eye cases
July 1993 - orthopaedic cases
Oct 93 - ENT cases
April 96 - O&G, dental cases
April 98 - pain cases
Same Day Admission Programme from July 97
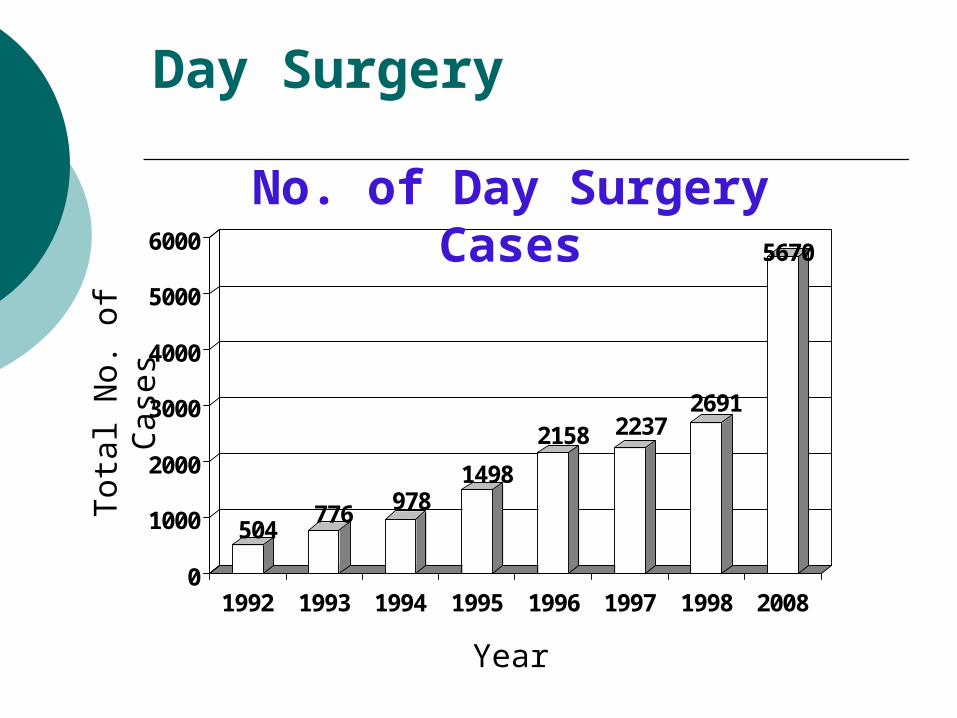
Day Surgery
504776 978
1498
2158 22372691
5670
0
1000
2000
3000
4000
5000
6000
1992 1993 1994 1995 1996 1997 1998 2008
Tot
al N
o. o
f C
ases
Year
No. of Day Surgery Cases
The UCH model - One stop approach
Surgeon consultation - anaesthesia assessment all on one day
Nurse screening and patient education before anaesthetist’s assessment
Written instruction (with DSC hotline) to take home
Patient to confirm operation within 2 weeks of operation
DSC staff to remind patient the day before
Surgeon and anaesthetist to review before operation
Challenges
Undiagnosed or unstable medical conditions: IHD, HT, DM, asthma or COADAnaesthetist as peri-operative physician
Fast track consultationCardiac - IHD - EchocardiographyCOAD - Resp function test and optimizationDM, HT, Asthma - specialist anaesthetist review
Team in-charge to follow up patient until ready for operation
Others
Type and screened blood / products for every indicated cases
Bowel preparation CMS enables communication and tracking of actions OR Manager to approach all surgeons to promote benefits of day surgery or SDA
KPI
Cancellation rate <2%
Medical condition - URTI, menstruation; surgical condition changed - lump disappearedChange of mind (not wanting surgery)Social issues (family member was sick, urgent visit to Mainland)
Admission rate (<2%)
Readmission rate (<0.2%)

Nurse
Call patient on day after discharge for satisfaction score and feedback
Others
In houses physician to deal with consultation
Anaesthetist or nurse manager to schedule operations (DS, SDA, IP)
Casemix funding incentives
Pain & symptom relief
Case manager to follow patient thru
ASA 1/2 Nurse Assessment Clinic
Physical facilities
Purpose built Peri-operative Centre
IT smart environment
Seamless support
100%