challenging clinical cases cc8 noninvasive respiratory ... · challenging clinical cases : cc8...
TRANSCRIPT

ERS Annual Congress Milan
09–13 September 2017
Challenging clinical cases
CC8 Noninvasive respiratory aids for continuous
support in neuromuscular disorders
Tuesday, 12 September 2017
07:00-08:15
Blue 1 (North) MICO

You can access an electronic copy of these educational materials here:
http://www.ers-education.org/2017Tuesday
To access the educational materials on your tablet or smartphone please find below a list of apps to
access, annotate, store and share pdf documents.
iPhone / iPad
Adobe Reader - FREE
With the Adobe Reader app you can highlight, strikethrough, underline, draw (freehand), comment
(sticky notes) and add text to pdf documents using the typewriter tool. It can also be used to fill out
forms and electronically sign documents.
http://bit.ly/1sTSxn3
MetaMoJi Note Lite - FREE
MetaMoJi Note is a cross-platform note taking app, PDF annotation tool, and a digital scrapbook.
Sketch your ideas visually with stylish pens and ink, take notes, or annotate imported PDF documents.
MetaMoJi Note is a virtual whiteboard for sketching, annotation, scrapbooking or digital mashup.
http://apple.co/29o5Nw0
GoodReader - €4.99
GoodReader allows you to view, create and edit PDF annotations. It also provides advanced PDF files
organising, reading and editing functionalities, such as inserting or extracting pages, splitting or
merging files, etc.
http://apple.co/29gzrFy
Android
Adobe Reader - FREE
The Android version of Adobe Reader lets you view, annotate, comment, fill out, electronically sign
and share documents. It has all of the same features as the iOS app like freehand drawing,
highlighting, underlining, etc.
http://bit.ly/1deKmcL
Xodo - FREE
Xodo is an all-in-one PDF reader and PDF editor. With Xodo, you can read, annotate, sign, and share
PDFs and fill in PDF forms, plus syncing with Google Drive and Dropbox.
http://bit.ly/1kHNcFl
ez PDF Reader - €3.99
With ez PDF reader you can add text in text boxes and sticky notes; highlight, underline, or
strikethrough texts or add freehand drawings. Add memo & append images, change colour / thickness,
resize and move them around as you like.
http://bit.ly/1kdxZfT

Challenging clinical cases : CC8
Noninvasive respiratory aids for continuous support in neuromuscular
disorders
Aims : To describe how to set up non-invasive ventilation that is complemented by assisted cough
techniques, thereby safely extending the full-time non-invasive support of neuromuscular disease
patients and avoiding tracheostomy/invasive ventilation.
Tracks: Acute and chronic respiratory failure/sleep
Tags: Clinical
Target audience: Intensivist/critical care physician - Nurse - Physiotherapist - Pulmonologist -
Respiratory therapist
Chairs : João Carlos Winck (Vila Nova de Gaia, Portugal)
Chronic respiratory failure in a patient with ALS Capucine Morelot-Panzini (La Varenne St-Hilaire, France)
Chronic respiratory failure in a patient with chest wall deformity Collette Menadue (Leichhardt, NSW, Australia)
Th e ERS Practical Handbook of Noninvasive Ventilation provides a concise ‘why and how to’ guide to NIV from the basics of equipment and patient selection to discharge planning and community care.
Editor Anita K. Simonds has brought together leading clinicians and researchers in the fi eld to provide an easy-to-read guide to all aspects of NIV. Topics covered include: equipment, patient selection, paediatric indications, airway clearance and physiotherapy, acute NIV monitoring, NIV in the ICU, long-term NIV, indications for tracheostomy ventilation, symptom palliation, discharge planning and community care, and setting up an NIV service.
Th is Practical Handbook is a valuable reference and training resource for all NIV practitioners.
• User-friendly format with key point summaries• Focused on practical aspects and problem solving• Multiple choice questions to enable self-assessment
To buy printed copies, visit the ERS Bookshop in the World Village at the ERS International Congress 2017.
Electronic: WWW.ERSPUBLICATIONS.COMPrint: WWW.ERSBOOKSHOP.COM
ERS Practical Handbook of Noninvasive VentilationEdited by Anita K. Simonds
ISBN (print) 978-1-84984-075-0ISBN (ebook) 978-1-84984-076-7
€30 (ERS members)€40 (non-members)
NONINVASIVE VENTILATION...how to do it, why to do it,
when to do it and when to stop!
Thank you for viewing these presentations.
We would like to remind you that these
materials are the property of the authors.
It is provided to you by the ERS for your
personal use only, as submitted by the
authors.
2017 by the authors
Chronic respiratory failure in a patient with chest wall
deformity
Collette Menadue, PhD
Senior Physiotherapist
Respiratory Failure Service
Royal Prince Alfred Hospital
Sydney, Australia
CC8 Noninvasive respiratory aids for continuous support in neuromuscular disorders

Conflict of interest disclosure
I have no real or perceived conflicts of interest that relate to this presentation.
I have the following real or perceived conflicts of interest that relate to this presentation:
Affiliation / Financial interest Commercial Company
Grants/research support:
Honoraria or consultation fees:
Participation in a company sponsored bureau:
Stock shareholder:
Spouse / partner:
Other support / potential conflict of interest:
This event is accredited for CME credits by EBAP and EACCME and speakers are required to disclose their potential conflict of interest. The intent of this disclosureis not to prevent a speaker with a conflict of interest (any significant financial relationship a speaker has with manufacturers or providers of any commercial productsor services relevant to the talk) from making a presentation, but rather to provide listeners with information on which they can make their own judgments. It remainsfor audience members to determine whether the speaker’s interests, or relationships may influence the presentation. The ERS does not view the existence of theseinterests or commitments as necessarily implying bias or decreasing the value of the speaker’s presentation. Drug or device advertisement is forbidden.
Introduction
AIMS:
1. Discuss timing and strategies to augment cough and airway
clearance in people with severe chest wall deformity and respiratory
muscle weakness
2. Discuss non-invasive ventilatory aids to avoid intubation and
improve outcomes during an acute respiratory illness
3. Discuss the role of non-invasive ventilation for long-term
continuous ventilatory support in patients with severe chest wall
deformity and respiratory muscle weakness
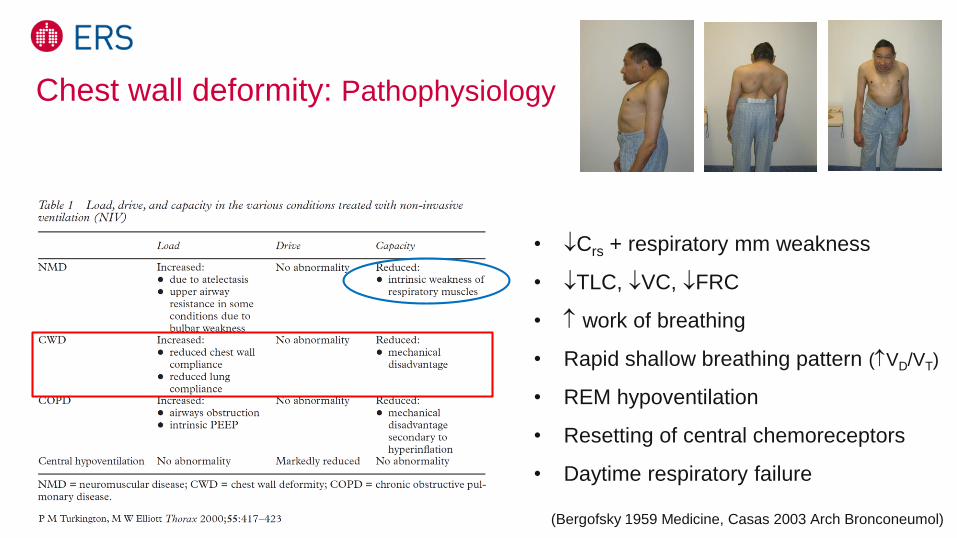
Chest wall deformity: Pathophysiology
• Crs + respiratory mm weakness
• TLC, VC, FRC
• work of breathing
• Rapid shallow breathing pattern (VD/VT)
• REM hypoventilation
• Resetting of central chemoreceptors
• Daytime respiratory failure
(Bergofsky 1959 Medicine, Casas 2003 Arch Bronconeumol)

Post polio syndrome (PPS)
• New or muscle weakness, occurs average 35yrs after acute polio
– Atrophy, pain, fatigue (Jubelt 2000 JAMA, Farbu 2006 Eur J Neurol)
• Prevalence 15-80% (Farbu 2006 Eur J Neurol)
• Sleep disordered breathing common (OSA/hypoventilation) (Hsu1998 Mayo Clin Proc)
• Chest wall deformity ’s risk of nocturnal hypoventilation (Howard 2003 Pract Neurol)
• Usually a slowly progressive neuromuscular disorder (Trojan 2005 Muscle Nerve)

• 30yo man with severe kyphoscoliosis and post polio syndrome referred
for sleep study
• Presents with:
– Dyspnoea, daytime sleepiness, sleep fragmentation, fatigue
• Past Medical Hx:
– Polio in Lebanon (age 2 ½), required short-term tracheostomy
– Wheelchair for mobility
– Severe muscle weakness lower limbs and trunk, weak upper limbs
– Obese (BMI 31.6)
– Snorer
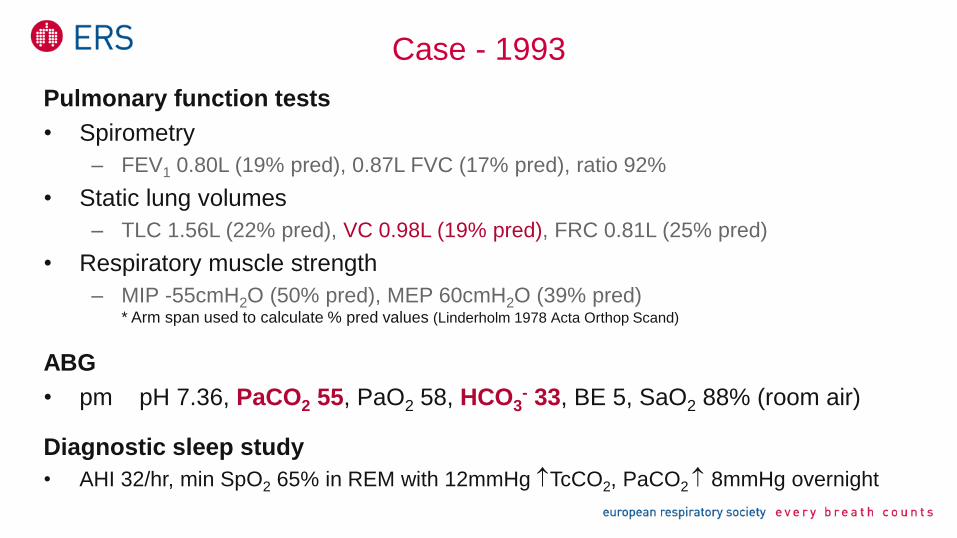
Case - 1993
Case - 1993
Pulmonary function tests
• Spirometry
– FEV1 0.80L (19% pred), 0.87L FVC (17% pred), ratio 92%
• Static lung volumes
– TLC 1.56L (22% pred), VC 0.98L (19% pred), FRC 0.81L (25% pred)
• Respiratory muscle strength
– MIP -55cmH2O (50% pred), MEP 60cmH2O (39% pred) * Arm span used to calculate % pred values (Linderholm 1978 Acta Orthop Scand)
ABG
• pm pH 7.36, PaCO2 55, PaO2 58, HCO3- 33, BE 5, SaO2 88% (room air)
Diagnostic sleep study
• AHI 32/hr, min SpO2 65% in REM with 12mmHg TcCO2, PaCO2 8mmHg overnight
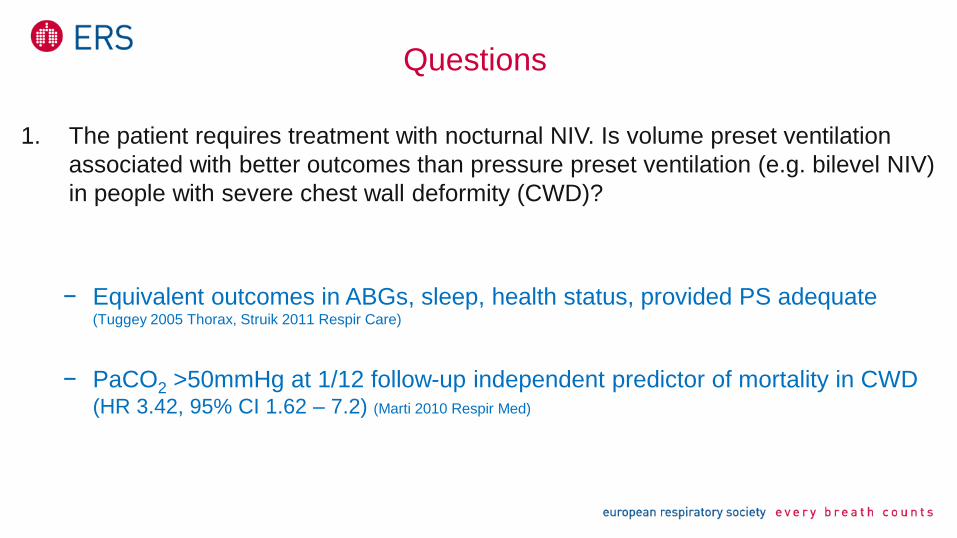
Questions
1. The patient requires treatment with nocturnal NIV. Is volume preset ventilation
associated with better outcomes than pressure preset ventilation (e.g. bilevel NIV)
in people with severe chest wall deformity (CWD)?
− Equivalent outcomes in ABGs, sleep, health status, provided PS adequate (Tuggey 2005 Thorax, Struik 2011 Respir Care)
− PaCO2 >50mmHg at 1/12 follow-up independent predictor of mortality in CWD (HR 3.42, 95% CI 1.62 – 7.2) (Marti 2010 Respir Med)
Case - 1993
• Bilevel (pressure preset) titration study performed:
– Spontaneous mode, IPAP 18 cmH2O, EPAP 6 cmH2O via nasal mask and
chin strap prevented OSA and hypoventilation

• NIV is a standard of care
• No RCTs unethical
• Retrospective studies and prospective observational studies with long term
follow-up consistently showing:
– Good survival (Simonds 1995 Thorax, Duiverman 2006 Respir Med, Gustafson 2006 Chest, Laub 2007 Respir Med)
– Good HRQL
– Improvements in ABGs, hypoventilation symptoms, exercise tolerance
– Inconsistent effects on pulmonary function(Leger 1994 Chest, Chailleux 1996 Chest, Schonhofer 2001 Chest, Nauffal 2002 Respir Med, Gonzalez 2003 Chest)
• Restrictive pathologies <10% HMV Australia & New Zealand (Garner 2013 Eur Respir J)
NIV for chronic hypercapnia in chest wall deformity
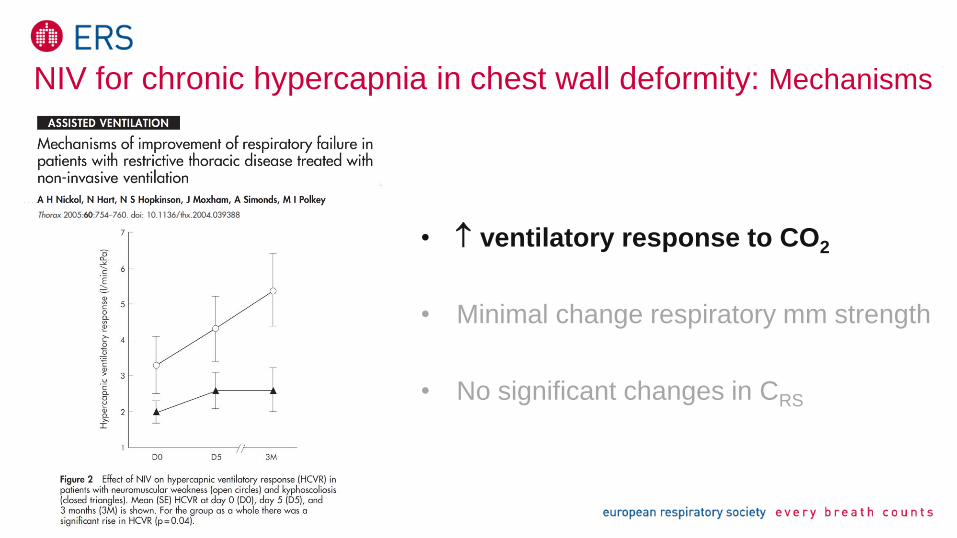
• ventilatory response to CO2
• Minimal change respiratory mm strength
• No significant changes in CRS
NIV for chronic hypercapnia in chest wall deformity: Mechanisms

Case – 1993 to 2007 (14yrs)
• Responded well to NIV- ABGs normal
- Symptoms resolved
- Using NIV 7-8hr/night
• Back to work- Disability Advocate
- Teacher Disability Services
- After hours emergency care coordinator
• Wheelchair sports
• Married with 2 children
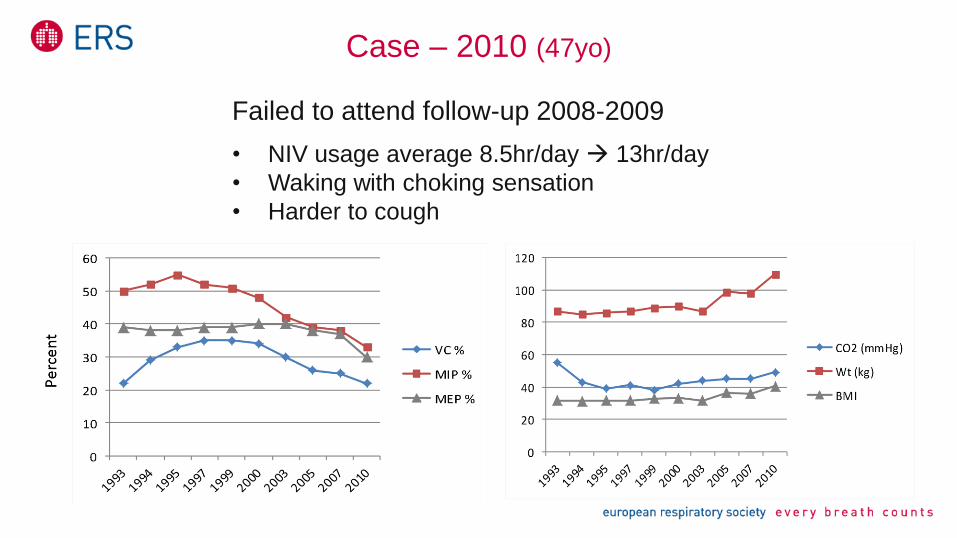
Case – 2010 (47yo)
Failed to attend follow-up 2008-2009
• NIV usage average 8.5hr/day 13hr/day
• Waking with choking sensation
• Harder to cough
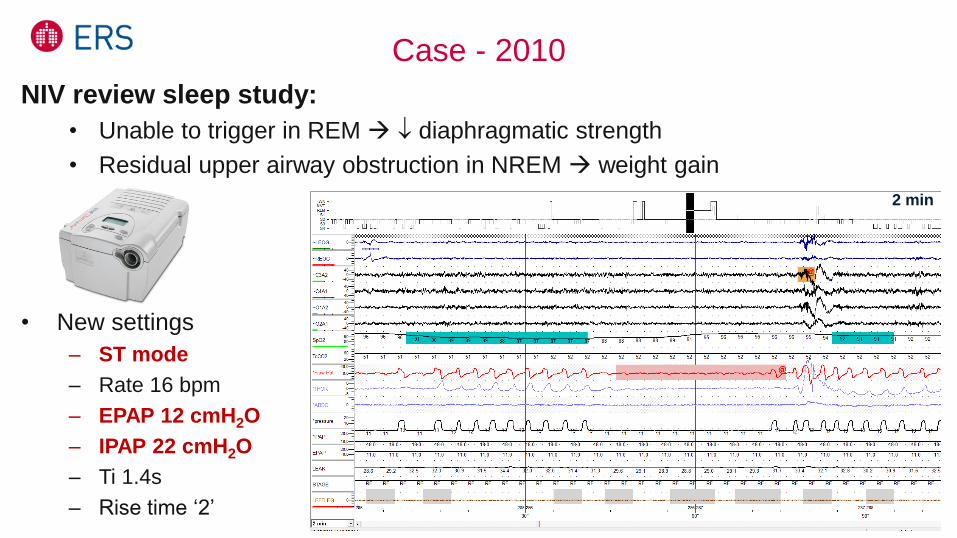
Case - 2010
NIV review sleep study:
• Unable to trigger in REM diaphragmatic strength
• Residual upper airway obstruction in NREM weight gain
• New settings
– ST mode
– Rate 16 bpm
– EPAP 12 cmH2O
– IPAP 22 cmH2O
– Ti 1.4s
– Rise time ‘2’
2 min

Case - 2010
• Discussed Advanced Care Plan
– For trial of full active Rx, including I+V
• Referral to dietician
• Cough assessment peak cough flow (PCF) 180L/min
Questions
2. PCF 160L/min = minimum threshold for an effective cough (Bach 1996 Chest).
Should strategies to augment cough be introduced now (PCF 180L/min)?
– Yes, respiratory mm strength ’s during URTI PCF (Poponick 1997 Am J Respir Crit Care Med)
– PCF <270L/min threshold for starting techniques (Tzeng 2000 Chest, McKim 2011 Can Respir J)
3. What strategies can be used to PCF?
– Manually Assisted Cough (MAC)
– Lung Volume Recruitment (LVR) +/- MAC
– Mechanical in-exsufflation (MI-E) +/- MAC
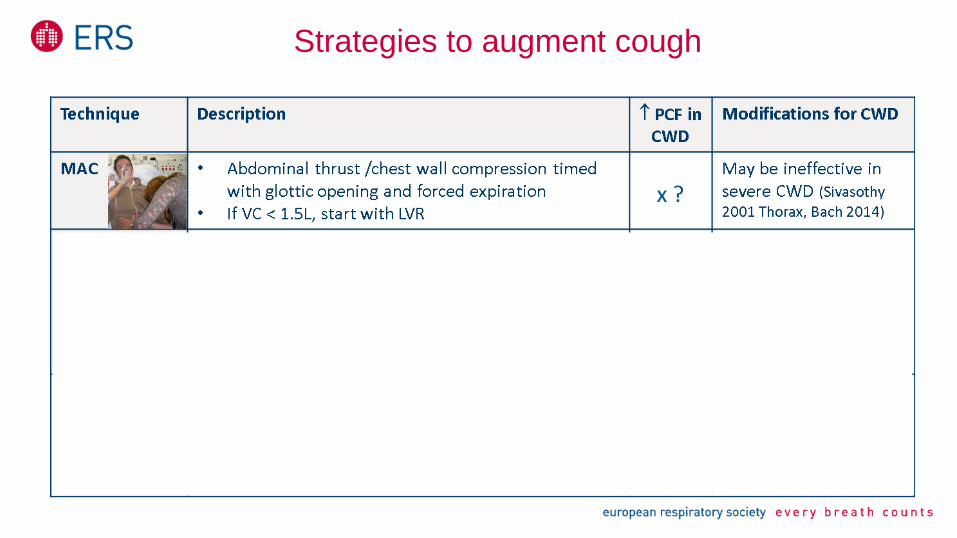
Strategies to augment cough

Questions
4. Are LVR and MI-E safe to perform in people with severe CWD?
– Extremely low complication rates (Bach 2008 Am J Phys Med Rehab, Bach 2014 J Neurorestoratology)
– Case reports of pneumothorax
• LVR: 72yo woman with PPS, scoliosis, asthma after 3yrs of LVR(Westermann 2013 J Bras Pneumol)
• MI-E: 26yo man with DMD, scoliosis on CNVS; 58yo man SCI + COPD on noct NIV (Suri 2008 Am J Phys Rehab)
– Avoid if previous/current pneumothorax, bullous emphysema, hypotension
• Transient MAP 10mmHg (50cmH2O) (Molgat-Seon 2017 ERJ Open Res)
– Urgent medical r/v if sudden chest pain/dyspnoea following LVR or MI-E

• LVR
– Dose: Recommended 10-15 insufflation cycles, x2-3/day (Kang 2000 Chest)
• Short trial of MI-E 45cmH2O
• Missed follow-up in 2011
Case - 2010

Case - 2012
• Admitted to hospital with URTI
• High-flow O2 in ambulance drowsy (GCS 14)
• For full active treatment
• ABG: pH 7.27, PaCO2 65, PaO2 110, HCO3- 31, SaO2 99% (8L/min O2 mask)
• Placed on NIV via BiPAP Vision in the Emergency Dept:
- IPAP 12, EPAP 6, FiO2 .35 via an oronasal mask
- Audible mask leak, intermittent trigger failure
- Audible upper airway noises, weak non-productive cough
• Repeat ABG (1hr): pH 7.27, PaCO2 67, PaO2 63, HCO3- 31, SaO2 89%
Questions
5. Would you continue with NIV or intubate the patient?
NIV is not currently optimised and signs of secretion retention, continue NIV but:
a) Manage pt in location where intubation is readily available (Ambrosino 2009 Eur Respir J)
b) Optimise NIV and trial for finite period
• Back-up rate
• PS (and EPAP for sleep)
• Minimise leak and reduce PVAs (Vignaux 2009 ICM, Davidson 2016 Thorax)
c) Airway clearance using mechanical in-exsufflation (MI-E) (Bach 1993 Arch Phys Med Rehab )
d) Target SpO2 88-92% (O’Driscoll 2011 Clin Med)
e) Humidification

Case – 2012
• Transferred to HDU
• NIV dependent (STx16bpm, IPAP 25, EPAP 12)
• Regular chest PT + MI-E (E70) at 50 cmH2O PCF 300L/min
• Able to clear sputum
• Supplemental O2 weaned to 1L/min
• Repeat ABG (1hr):
- pH 7.32, PaCO2 58, PaO2 65, HCO3- 30, SaO2 91%
• Plan: continue NIV + regular chest PT with MI-E

Case - 2012
Progress next day:
• pH 7.36, PaCO2 54, PaO2 67, HCO3- 30
• Still NIV dependent + ongoing MI-E
• Reddened nasal bridge
– Alternative interfaces, pressures daytime
• Download of home BiPAP machine
Case
• NIV usage past 6/12 >19 hr/day ventilator dependent (Tzeng 2000 Chest)
• Using NIV for breathlessness
– Stopped regular LVR, thought daytime NIV was adequate
• Stopped work, housebound
• Implications for weaning and d/c planning (equipment and safety)

Questions
6. As the patient will remain ventilator dependent (>16-18hr/day) long term, would
you change to tracheal ventilation or continue with NIV to prepare for d/c?
– No RCTs
– Continuous NIV (including mouthpiece ventilation) in NMD and CWD:
• Safe, good survival (Bach 1987 Chest, Bach 1993 Chest, Bach1993 Arch Phys Med Rehab, Toussaint 2006 Eur
Respir J, McKim 2013 Can Respir J, Nicolini 2016 Rev Port Pneumol)
• complications, chest infections (Bach 1993 Chest, Bach 1998 Am J Phys Med Rehabil, Souden 2008 Chron Resp Dis)
• complex care, live at home, cost (Souden 2008 Chron Resp Dis, Bach 2015 Am J Phys Med Rehab)
• Preferred by patients (Bach 1993 Chest (vol 103), Bach 1993 Chest (vol 104), McKim 2013 Can Respir J)
Case: Life support ventilator (Trilogy 100), weaned to usual nocturnal settings
Trial of daytime mouthpiece ventilation (MPV)

Open-circuit mouthpiece ventilation (MPV)
(Bach 1987 Chest, Bach 1993 Chest, McKim 2013 Can Respir J, Garuti 2014 Rev Port Pneumol, Khirani 2014 Respir Care)
Limitations to MPV/continuous NIV: • Severe bulbar dysfunction
• Inability to protect the airway
• PCF <160L/min despite LVR and MI-E
• Uncooperative
Advantages Disadvantages
Speech Limited to daytime (awake) use
Eating/drinking easier Aerophagia (ACV mode)
Avoid pressure areas Orthodontic deformity
Breath stacking (ACV mode) Hypersalivation
Little dead space Nuisance alarms*
Aesthetics
Role for tracheal ventilation in
selected individuals
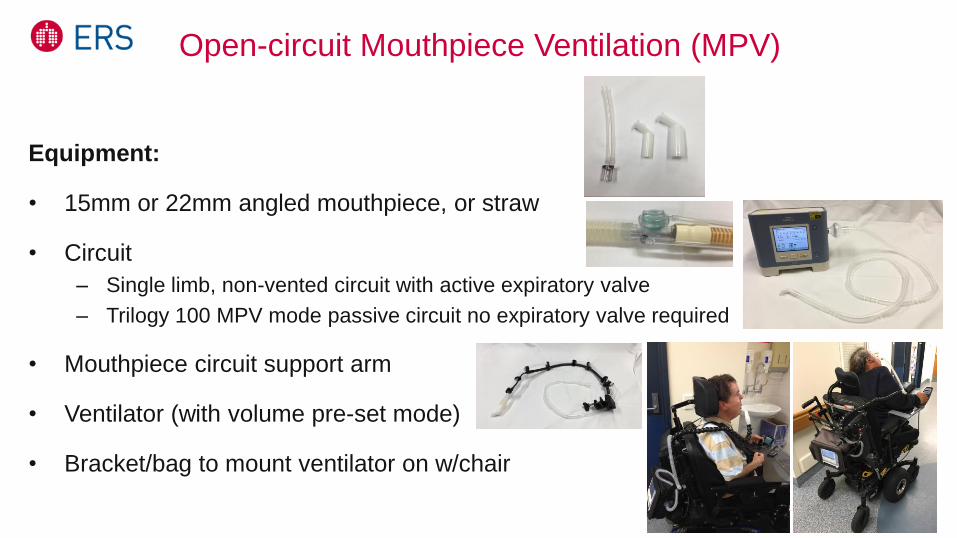
Open-circuit Mouthpiece Ventilation (MPV)
Equipment:
• 15mm or 22mm angled mouthpiece, or straw
• Circuit
– Single limb, non-vented circuit with active expiratory valve
– Trilogy 100 MPV mode passive circuit no expiratory valve required
• Mouthpiece circuit support arm
• Ventilator (with volume pre-set mode)
• Bracket/bag to mount ventilator on w/chair

Mouthpiece ventilation (MPV)
Settings
• Mode: predominantly volume controlled ventilation (ACV mode) (Khirani 2014 Respir Care)
– Can also use pressure controlled ventilation/PACV (cannot breath stack)
• VT: adults 700-1500mL (Hess 2012 Respir Care, Bach 2014 J Neurorestoratology)
• PEEP/EPAP: zero (Nicolini 2014 Phys Med Rehabil Int)
• Rate: zero/lowest if can spontaneously trigger, otherwise set as needed*
*Trilogy 100 MPV mode ‘kiss’ trigger (reverse flow trigger) no rate required (doesn’t blow on face)
• Ti, Flow shape, Trigger sensitivity
Alarms
• Low pressure alarm: off or minimum
– Angled mouthpiece/straw provides resistance to maintain pressure in circuit (15mm > 22mm)
• Apnea alarm and Disconnect alarm: off or maximum duration

Yes Yes
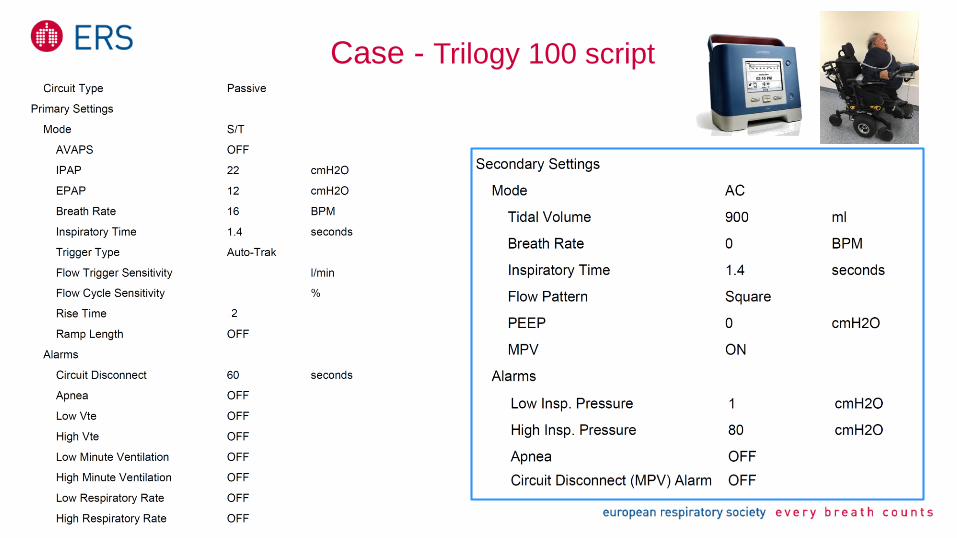
Case - Trilogy 100 script

LVR (breath stacking) with mouthpiece ventilation

Safety
considerations for
NIV dependent
patients
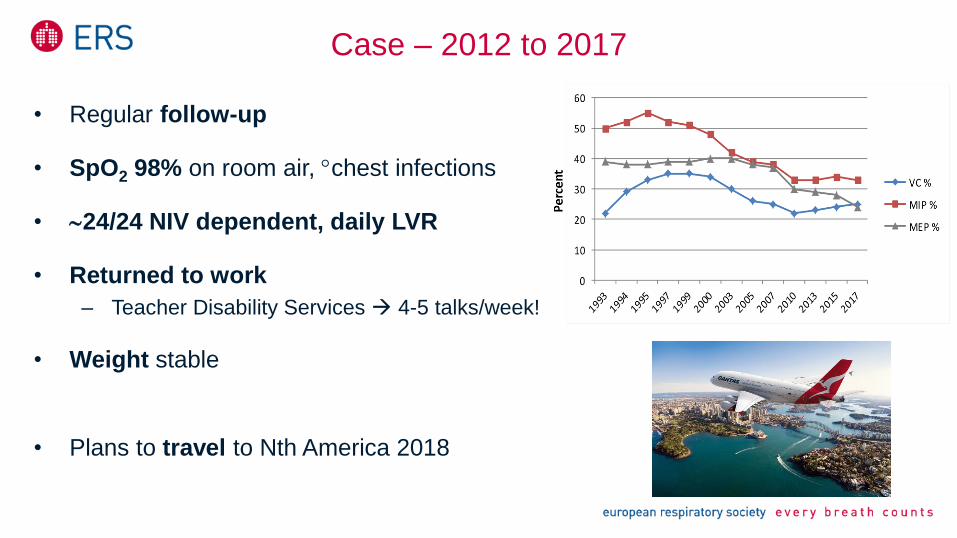
• Regular follow-up
• SpO2 98% on room air, chest infections
• 24/24 NIV dependent, daily LVR
• Returned to work
– Teacher Disability Services 4-5 talks/week!
• Weight stable
• Plans to travel to Nth America 2018
Case – 2012 to 2017

Conclusion
• Regular follow-up and monitoring is important to allow timely introduction of
non-invasive respiratory aids
• Strategies to augment cough and facilitate airway clearance are integral to
the success of NIV in patients with severe CWD and respiratory muscle
weakness
• Non-invasive ventilation and assisted cough strategies may be used to avoid
intubation in selected individuals with acute on chronic hypercapnic
respiratory failure
• Individuals with severe CWD and respiratory muscle weakness can be
successfully managed with continuous NIV with good long term survival
and quality of life

Questions?