chapter 19 immune disorders copyright © 2012 by saunders, an imprint of elsevier, inc
TRANSCRIPT

Chapter 19
Immune Disorders
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc.

The Immune System
• Protective processes eliminate foreign antigens through function of specific cells
• Antibodies fight infections– IgG is the only antibody that crosses the placenta
• Full-term infants receive adult levels, providing protection from bacterial infections
• Immune responses are humoral or cell-mediated– Humoral: B lymphocytes produce antibodies and memory
cells– Cell-mediated: Involves T lymphocyte cells
• Helper cells, killer cells, suppressor cells
• Autoimmune disorders: Abnormal, excessive response to self
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-2

Kawasaki Disease (KD)
• Description– Acute, severe vasculitis of all blood vessels
• Leading cause of acquired heart disease in children
• Signs and symptoms• Diagnosis: Clinical signs, lab tests, 2D echocardiogram
– Three stages• Acute: prolonged high fever, strawberry tongue, irritability• Subacute: Desquamation of hands/feet, arthritis, coronary aneurysms• Convalescent: All signs have disappeared
– Treatment and nursing care• Reduce inflammation via IV-IG and high-dose aspirin• Provide symptom-specific relief• Extreme irritability is the most challenging nursing issue
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-3

Stevens-Johnson Syndrome
• Description– A severe form of erythema multiforme involving
lesions of the skin and mucous membranes• Signs and symptoms
– Flu-like symptoms– Mucosal lesions in eyes, mouth, and GI tract
• Treatment and nursing care– Ophthalmologist monitors for corneal scarring– Care of topical and oral lesions as needed– Medication allergies should be noted in order to
prevent future incidents
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-4

Juvenile Idiopathic Arthritis (JIA)
• Description– JIA syndromes affect joints, connective tissue, viscera– Chronic, with remissions and exacerbations
• Signs and symptoms– Joint stiffness in the morning or after a period of inactivity– Osteopenia: low bone mass– Diagnosis: clinical manifestations, radiographs, lab tests– JIA is categorized by method of onset
• Systemic: acute febrile• Oligoarticular: involving five or fewer joints
– Risk for iridocyclitis, inflammation of the iris and ciliary body (risk of blindness)
• Polyarticular: involving more than five joints
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-5
Juvenile Idiopathic Arthritis
• Treatment and nursing care– Drug therapy and exercise to reduce pain and stiffness
• Continued monitoring of medications is important– Intra-articular long-acting corticosteroid injections preserve
joints• Home care
– Moist hot packs lessen stiffness– Firm mattresses prevent sagging joints– Encourage swimming– Avoid weight gain
• Facilitating school attendance– Provide unobtrusive access to the school health office– Excess absence may suggest preoccupation with illness
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-6

Juvenile Idiopathic Arthritis
• Meeting emotional needs– Parents should avoid overindulgence and
preferential treatment– Assist families in understanding the chronic
nature of the disease
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-7

Infectious Mononucleosis
• Description– A global disease caused by a herpes type of
Epstein-Barr virus (EBV)– Studies suggest that the organism is
transmitted by contact with saliva, either directly or from contaminated eating utensils; however, its communicability is considered low
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-8

Infectious Mononucleosis
• Signs and symptoms– Low-grade fever, sore throat, headache,
fatigue, skin rash, and general malaise– The lymph glands enlarge– Splenomegaly develops in approximately half
the patients – Liver involvement with mild jaundice occurs in
a small number of persons
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-9

Infectious Mononucleosis
• Treatment and nursing care– Acetaminophen or NSAIDs given as needed
– An antipyretic is given to reduce fever and discomfort
– An initial period of rest or restricted activities is usually needed; returning to usual activities is based on the child’s energy level
– Gargling with warm saline solution and sucking on throat lozenges can be helpful for pharyngitis
– Adequate fluid intake is necessary
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-10

Diabetes Mellitus (Type 1)
• Description– Failure to metabolize carbohydrates, fats, and
proteins properly due to lack of insulin
• Incidence– Frequency increases with age
• Highest rate of new cases among 5- to 7-year-old children
– Risk factors include history of Type1 DM in the family, psychosocial stress, obesity, viral infections
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-11

Diabetes Mellitus (Type 1)
• Signs and symptoms– 3P’s: Polyuria (excretion of large amounts of urine),
polydipsia (excessive thirst), and polyphagia (constant hunger)
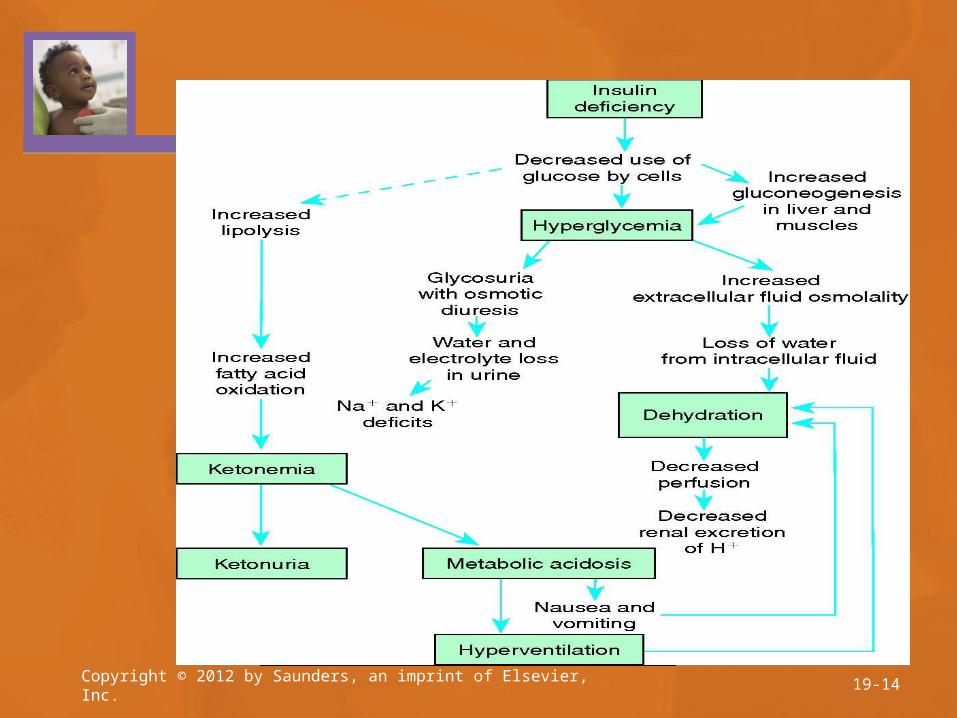
– Fatigue, anorexia, nausea, lethargy, weakness– Dry skin– Vaginal yeast infections– Urine accidents in a previously trained child– Hyperglycemia, glycosuria, ketoacidosis– Diabetic ketoacidosis (DKA) when conditions demand
an increase insulin to maintain blood sugar levels• Kussmaul breathing
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-12

Diabetes Mellitus (Type 1)
• Treatment and nursing care– Diabetic ketoacidosis
• Correction of depleted fluids, stabilization of vital signs• Low doses of IV insulin; check K+ levels• Response to treatment is gradual
– Long-term management• Promote normal growth and development through
metabolic control• Enable a happy childhood• Prevent complications• Planned educational programs provide a consistent
body of information to families
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-13
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-14

Diabetes Mellitus (Type 1)
• Treatment and nursing care (continued)– Insulin administration
• Goal: simulate the fluctuations in insulin levels normally seen in non-diabetic individuals
• Human insulin is frequently used; lesser incidence of allergies
• A 100-unit (U-100) insulin is standard in the United States
• Administered subcutaneously at a 90-degree angle
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-15

Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-16

Hypoglycemia
• Low blood glucose, also known as insulin shock• Symptoms appear suddenly• Immediate treatment consists of administering
sugar, such as orange juice, hard candy, or a commercial product such as Glutose PO
• If the child begins to feel better within a few minutes and blood glucose level exceeds 70 mg/dL, eat a small amount of protein or starch to prevent another reaction
• Severe hypoglycemia is treated with Glucagon IM
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-17

Hypoglycemia
• Blood glucose self-monitoring– Home glucose monitoring should be taught to all
young patients and/or their caretakers– Blood specimen obtained with capillary blood-letting
devices– A drop of blood is put on a chemically treated reagent
strip, and a meter reads the blood glucose level• Nutritional management
– Elimination of concentrated carbohydrates (simple sugars) and refined sugars
– The two major approaches to nutritional management include the use of exchange lists and the constant carbohydrate monitoring diet
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-18

Hypoglycemia
• Exercise– Causes the body to use sugar and promotes
good circulation• Sick day rules –
• chart for controlling sugar on days you don’t feel well, so exercise less and eat less
• Infections raise the need for insulin• Skin care
– Bathe daily, dry well especially feet– The patient should be instructed to inspect skin
for cuts, rashes, abrasions, cysts, or boils
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-19

Hypoglycemia
• Foot care– Instruct the patient to wash and dry the feet well
each day– Instruct the patient to trim the nails straight across
• Infections– Obtain immunizations against communicable
diseases– Cystitis, subcutaneous nodules, and monilial
vulvitis occur with greater frequency in patients with diabetes
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-20

Hypoglycemia
• Urine checks– Routine urine checks for sugar are replaced by glucose
blood monitoring– May be used to test for acetone– Quantitative urine collection is sometimes ordered
• Glucose-insulin imbalances– Patient should recognize signs of insulin shock and
ketoacidosis– Carry a ready source of glucose for emergencies– Medic-Alert bracelets, wallet cards– Adults involved in caring for the child (i.e., coaches,
teachers) should have parent/physician phone numbers
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-21

Hypoglycemia
• Psychosocial aspects– Parents and patients must understand that although insulin
dose needs may vary, the child will need lifelong insulin administration
– Because children grow in spurts, dosing may be irregular– School-age children may use illness to gain attention or
avoid responsibilities– Rebellion against treatment regimen– Impact of disease on the rest of the family should be
considered• Other issues
– Planning is needed for travel– Surgery is typically well-tolerated– Regular eye and dental exams are especially important
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-22

Hypoglycemia
• Role of the nurse– Preparing the child for meals– Checking blood glucose– Observing the types and amounts of foods that
the patient refused and charting them in the nurse’s notes
– Reinforcing the interaction among nutrition, insulin requirements, and exercise and answering questions from the child or family
• The future of research on diabetes– Genetics, viruses, pancreas transplantation, beta
cell transplantation, and artificial pancreas
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-23

Type 2 Diabetes (T2DM)
• One-third to one-half of all newly diagnosed diabetes patients are younger than 18 years of age
• Insulin receptor resistance combined with insulin deficiency
• Symptoms similar to T1DM• Nutritional education and improved exercise• Insulin may be reduced or discontinued
within a few weeks of treatment if sugar is stable
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 19-24

Communicable Diseases
• Transmitted by direct/indirect contact, vector, or airborne
• Children’s immune systems are not fully developed until 6 years of age
• Nursing care focuses on disrupting the chain of infection to prevent disease– Reservoir: environment where organism exists and multiplies– Portal of exit: route by which organisms leave the reservoir– Portal of entry: route by which the organism enters the host– Prodromal symptoms indicate the onset of a disease
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 18-25

Immunizations
• Stimulate the body to produce antibodies in defense against weakened/killed microorganisms in the vaccine– Immunizations prevent epidemics
• Immunizations recommended in the U.S. by age 2:– Polio, diphtheria, tetanus, pertussis (whooping cough),
hepatitis A, hepatitis B, Haemophilus influenzae type b, mumps, measles, rubella, varicella (chickenpox), rotavirus, and Streptococcus pneumoniae (pneumococcus)
• Other vaccines with varying age groups are influenza, varicella, HPV/HPV4, rotavirus, meningococcal conjugate
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 18-26

Immunizations
• Contraindications to immunization– Acute febrile conditions– Some chronic diseases– Recent blood transfusion– Injection of immune serum globulin– Severe allergy to a vaccine component– Severe reaction after previous administration of
an immunization– Malignant disease– Chemotherapy– Steroid therapy
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 18-27

Immunizations
• Precautions/side Effects– Benefits of protection greatly outweigh the
risks– Notify a health care provider if the child
experiences• Persistent high fever• Continued crying• Decreased responsiveness• Seizure activity
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 18-28

Immunizations
• Hepatitis B (Hep B) vaccine– Intramuscular– Given to newborns before discharge– Three doses total
• HBIG also, if mother has a positive surface antigen for Hep B– Injection site tenderness/mild temperature common
• Rotavirus vaccine– Oral– Not recommended with previous history of
intussusception, or if antibody-containing blood products have been administered in the past 42 days
– Irritability, mild diarrhea/vomiting
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 18-29

Immunizations
• Diphtheria-tetanus-pertussis vaccine (DTP) and diphtheria-tetanus-acellular pertussis vaccine (DTaP)– Requires excellent intramuscular injection technique– Contraindications
• Encephalopathy within 7 days of administering a previous dose
– Side effects: mild fever, swelling at injection site, fussiness, decreased appetite
– Tdap: Licensed in 2005, recommended as a once-only booster for adolescents
• Haemophilus influenzae type b (Hib) vaccine– Intramuscular– Side effects are usually mildCopyright © 2012 by Saunders, an imprint of Elsevier, Inc. 18-30

Immunizations
• Pneumococcal vaccine (PCV)– Intramuscular– Can cause fever, fussiness, local erythema
• Polio vaccine– Oral in the past; now subcutaneous or
intramuscular– Contraindications: anaphylactic reaction to
neomycin/streptomycin/polymyxin B, pregnancy– Side effects are rare
• Mild soreness at injection site
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 18-31

Immunizations
• Influenza vaccine– Intramuscular
• Live attenuated influenza vaccine (LAIV) intranasal alternative for persons aged 5-49 years
– Contraindication: anaphylactic hypersensitivity to eggs• Mumps, measles, and rubella vaccine (MMR)
– Subcutaneous– Contraindications: pregnancy, anaphylactoid reaction to neomycin or
gelatin, immunodeficiency– Precautions: administration of antibody-containing blood products,
thrombocytopenia– Possible side effects
• Measels vaccine: fever/rash 7-12 days after vaccination• Rubella vaccine: rash within a few days, joint pain/swelling 2 weeks after
vaccination• Combination MMR: mild fever, rash, mild swelling of cheek/neck glands
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 18-32

Immunizations
• Varicella vaccine– Subcutaneous– Contraindications: immunocompromised, pregnancy, children
receiving steroids, previous anaphylactic reaction to neomycin or gelatin
– Precautions: recent administration of antibody-containing blood products
– Reactions: Mild vaccine-associated maculopapular or varicella rash, soreness/edema at the injection site, mild fever
• Hepatitis A vaccine– Intramuscular– Contraindication: Sensitivity to alum or 2-phenoxyethanol – Possible side effect: Local redness may occur
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 18-33

Immunizations
• Meningococcal vaccine (MCV)– Intramuscular– Contraindications: hypersensitivity to any
component of the vaccine– Possible side effect: Pain/redness at injection site
• Human papillomavirus (HPV)– Possible side effects: Pain, redness, swelling at
injection site• Because syncope can occur, children should be
observed for 15-20 minutes after administration
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 18-34

Health Problems and Immunizations
• Children with asthma, lung/heart/kidney disease, metabolic/blood disorders should not receive LAIV– Administer inactivated influenza vaccine
• Children with cancer, leukemia, AIDS, or other immune system problems should not receive live-virus vaccines– LAIV, MMR, varicella, rotavirus
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 18-35

Importance
• Community outreach projects sponsored by the Public Health Department provide immunizations for children
• Accurate records are important• Administration of multiple vaccines in one
visit does not increase intensity or number of side effects
• EMLA cream or topical vapocoolant sprays may decrease pain at injection site
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 18-36

Concerns
• Thimerosal, a mercury-containing preservative, has been eliminated from childhood immunizations
• Some investigators believe that MMR vaccine is associated with autism– Multiple studies fail to support an association
between MMR vaccine and autism• See Price et al. (2010)
Copyright © 2012 by Saunders, an imprint of Elsevier, Inc. 18-37