chapter 2 health in an urban context - who | world …€¦ · the dawn of an urban world hidden...
TRANSCRIPT

Since its inception in 1948, the World HealthOrganization has embraced a comprehensiveunderstanding of health as “not merely theabsence of disease or infirmity”, but rather “a state of complete physical, mental and socialwell-being.”29 Today, compelling scientificevidence shows that physical, mental and socialhealth and well-being are closely interwoven and deeply interdependent,30 and that health is influenced by a broad range of determinantsthat lie beyond the health sector. This chapterintroduces underlying drivers of health in urbanareas, and describes some of the common healthissues faced by people living in cities.
PART ONE. THE DAWN OF AN URBAN WORLDHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS 11
WHO/Anna Kari
CHAPTER 2
HEALTH IN AN URBAN CONTEXT
Determinants of health Determinants of health refer to the socioeconomic,cultural and environmental conditions thatinfluence the health of individuals and popula-tions. They include the conditions of daily life andthe broader influences upon them.
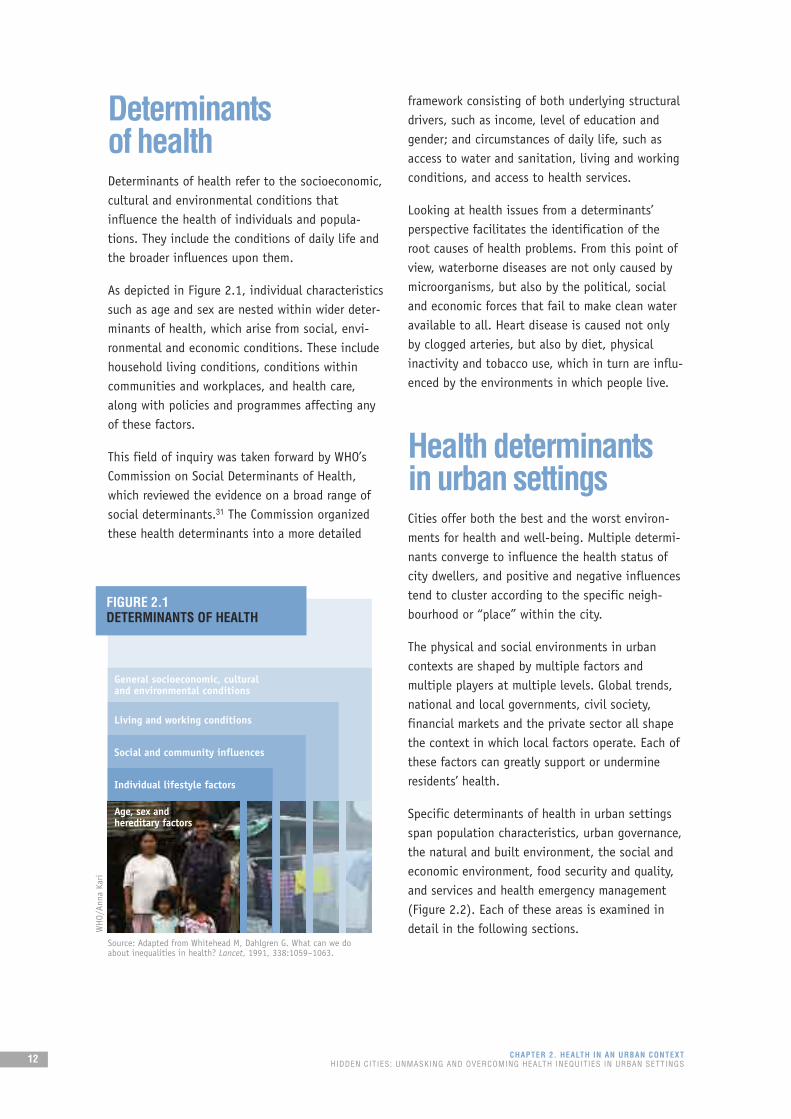
As depicted in Figure 2.1, individual characteristicssuch as age and sex are nested within wider deter-minants of health, which arise from social, envi-ronmental and economic conditions. These includehousehold living conditions, conditions withincommunities and workplaces, and health care,along with policies and programmes affecting anyof these factors.
This field of inquiry was taken forward by WHO’sCommission on Social Determinants of Health,which reviewed the evidence on a broad range ofsocial determinants.31 The Commission organizedthese health determinants into a more detailed
framework consisting of both underlying structuraldrivers, such as income, level of education andgender; and circumstances of daily life, such asaccess to water and sanitation, living and workingconditions, and access to health services.
Looking at health issues from a determinants’perspective facilitates the identification of theroot causes of health problems. From this point ofview, waterborne diseases are not only caused bymicroorganisms, but also by the political, socialand economic forces that fail to make clean wateravailable to all. Heart disease is caused not onlyby clogged arteries, but also by diet, physicalinactivity and tobacco use, which in turn are influ-enced by the environments in which people live.
Health determinants in urban settingsCities offer both the best and the worst environ-ments for health and well-being. Multiple determi-nants converge to influence the health status ofcity dwellers, and positive and negative influencestend to cluster according to the specific neigh-bourhood or “place” within the city.
The physical and social environments in urbancontexts are shaped by multiple factors andmultiple players at multiple levels. Global trends,national and local governments, civil society,financial markets and the private sector all shapethe context in which local factors operate. Each ofthese factors can greatly support or undermineresidents’ health.
Specific determinants of health in urban settingsspan population characteristics, urban governance,the natural and built environment, the social andeconomic environment, food security and quality,and services and health emergency management(Figure 2.2). Each of these areas is examined indetail in the following sections.
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS12
FIGURE 2.1DETERMINANTS OF HEALTH
General socioeconomic, cultural and environmental conditions
Living and working conditions
Social and community influences
Individual lifestyle factors
Age, sex and hereditary factors
Source: Adapted from Whitehead M, Dahlgren G. What can we doabout inequalities in health? Lancet, 1991, 338:1059–1063.
WHO/Anna Kari

Deaths of children in cities are often the directresult of contamination of water, inadequate sanitation and lack of solid waste disposal, which exacerbate the occurrence and severity ofdiarrhoeal and related diseases. Gastrointestinalillness can lead to malnutrition and death, espe-cially among younger and undernourished childrenwho still have poorly developed immune defences.
Pneumonia and diarrhoeal diseases are the leadingcauses of childhood death globally,34 and can be a particular problem in urban settings due tocrowding, indoor air pollution and poor access tohealth care in urban slums. For similar reasons,children in urban areas are susceptible to deathfrom malaria and vaccine-preventable illnessessuch as measles.
Road traffic injuries among children are of signifi-cant concern in urban areas. Lack of considerationto children in urban and transport planningcontributes to the problem.35 Globally in 2004,road traffic injuries were the leading cause of
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS 13
FIGURE 2.2FACTORS INFLUENCING THE HEALTH OF CITIES
POPULATION CHARACTERISTICS
The demographic characteristics of those living in a particular city or urban neighbourhood at aparticular time reflect historical trends, patterns of fertility and migration trends. The age, genderand disability status of city dwellers affect health,both at individual and populationwide levels.
Certain population groups require special consider-ation because they have particular health issues orneeds within urban environments. Withouttargeted attention, they are likely to be excludedfrom overall health development.
CHILDREN. Children comprise a major portion ofthe urban population: it is estimated that 60% of all city dwellers will be under the age of 18 by 2030.32 Although children living in urban areasare often regarded as better off than their ruralpeers, this is not always the case, considering that many children live in slums or other adverse environments.33
Social and economic environment
Services and health emergency management
Natural and built environment
Food security and quality
POPULATION CHARACTERISTICS
URBAN GOVERNANCE
1–3 from
left: WHO/Anna Kari; 4: UN Photo/Jawad Jalali

death among youths aged 15–24 years, and thesecond leading cause of death for those aged 10–14 years.36
Children are also particularly vulnerable toexploitation and crime at the hands of olderchildren and adults. In deprived urban settings,children have higher rates of psychological andbehaviour problems37,38 and lower educational and occupational expectations39 than those fromrural areas.
OLDER ADULTS. Urbanization in low- and middle-income countries will concentrate an increasingproportion of the older population in cities. NewYork, London, Paris and Tokyo already have thelargest concentrations of older people in theirrespective countries. The “oldest old” – those 85and older – comprise the fastest-growing segmentof this population.40 In Africa and Asia, olderpeople still live predominantly in rural areas, but itis expected that this situation will be reversedbefore 2020.32
In cities, older people are often invisible orforgotten among other priorities. They may becomehousebound due to physical impairments combinedwith inadequate transportation systems. Pride maydiscourage them from seeking help. Specialattention is needed to ensure that older peoplecan preserve their autonomy and independentliving for as long as possible, and can accesshealth and other social services, including home-based care.
WOMEN. While cities open many possibilities forwomen to meet, work and form social supportnetworks, women living in cities also face uniquechallenges. These include heightened risk ofphysical, sexual and psychological violence;barriers in accessing health and social services dueto lack of control over family financial resources,child-care responsibilities, restricted mobility andlimited decision-making power; and lack ofeducation and economic security relative to men.41
Urban poverty has become highly feminized.Compared to their male counterparts, poor urbanwomen tend to have lower-paying jobs and higherilliteracy rates. They also are excluded from certaintypes of jobs because of lack of education ordiscriminatory practices. On top of this, women areoften excluded from land and home ownership andinheritance.42 All these factors place poor urbanwomen and their dependents at increased risk for arange of health problems.
MIGRANTS. Immigration is commonly characterizedas population movement from poor to richer locali-ties, as well as from rural to urban areas. Acomplex set of context-dependent factors –economic, political and social – explain why somecities have large migrant populations. Migrants areattracted by the possibilities that cities can offer.Frequently, they are searching for better employ-ment and economic opportunities, or fleeing frompersecution and violence.
Those who migrate to escape difficult circum-stances often experience a double jeopardy incities: pre-existing vulnerabilities combined withgreater exposure to migration-associated stressors.A social and economic gap often emerges betweenlong-time urban residents and migrants.43
PEOPLE WITH DISABILITIES. People with disabilitiesare strongly affected by the physical and socialenvironments of cities. Depending on their partic-ular characteristics, urban environments cangreatly facilitate or undermine the independenceand quality of life of people with disabilities.44
Cities’ physical environments and infrastructure areparticularly important for people with locomotor orsensory disabilities. Disability-friendly transportsystems, sidewalks, pedestrian crossings and building
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS14
WHO/Anna Kari

CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS 15
Dina lives with her father, mother,and little brother. She likes living inher neigbourhood because she knowseveryone and says that people arekind. Her uncles and aunts andgrandfather live next door.
“I got sick in 2009,” says Dina. “Ihad a headache, nausea, shivers andmy temperature was very high.” Shewent to the doctor but after a weekwas still very sick and so she went to
the hospital with her mother. “I wasadmitted to thehospital for four days.
I felt terrible and had a high fever.They did blood tests and the doctortold me it was dengue fever.”
“I was worried when the doctor toldme,” continues Dina, “because Iknew a girl my age who died a fewyears ago from dengue. I reallywanted to get well quickly.”
After Dina came out of the hospital,she noticed that people were
spraying in her neighbourhood.“Now they have been spraying thearea to kill the mosquitoes every fewmonths.” The community has alsostepped up its prevention efforts.“There are people in the communitywho monitor the larvae. They putpowder on the larvae they see whichkills them. Without larvae, there willbe no more mosquitoes.”
Still, Dina cautions, “People are notcareful enough. They leave opencontainers with water and there is alot of garbage dumped here.”
Dina, 16Jakarta, IndonesiaFIGHTING DISEASE AT THE SOURCE – LIVING CONDITIONS AND DENGUE
WHO/Anna Kari

entrances are but a few of the many factors thathave a major impact on the daily lives of thosewho use assistive devices such as canes, walkers orwheelchairs. People with hearing or visual impair-ments often benefit from additional accommoda-tions, such as the provision of key information inmultiple auditory and visual formats.
The social environment of cities influences thedegree of stigma and discrimination experiencedby people with disabilities. In particular, peoplewith chronic mental disorders or intellectualdisabilities can be adversely affected by hostileenvironments if they are not specifically addressedthrough public awareness campaigns and antidis-criminatory regulations.
The ability to access regular health services andcommunity support are particularly important forpeople with all types of disabilities.
URBAN GOVERNANCE
Urban governance refers to the mechanisms,processes and institutions through which residentsand groups articulate their interests, exercise theirlegal rights, meet their obligations and mediatetheir differences.45 It is important to note thatgovernance is broader than government. In manyformulations, governance includes government,and also the private sector, civil society andcommunity groups. Second, governance empha-sizes process. It recognizes that decisions aremade based on complex relationships betweenmany actors with different priorities.46
Urban governance is inextricably linked to thehealth and well-being of city dwellers. Good urbangovernance affirms that no one should be deniedaccess to the necessities of urban life, andprovides all city dwellers with the platform thatwill allow them to use their talents to improvetheir social and economic conditions.46 Withindeveloping countries, the best urban governancecan help produce 75 years or more of lifeexpectancy; with poor urban governance, lifeexpectancy can be as low as 35 years.47
Healthy urban governance is discussed in detail inPart Three of this report.
NATURAL AND BUILT ENVIRONMENT
The natural and built environment refers to naturaland human-made aspects of cities and their inter-action therein. Facets of the natural and builtenvironment that influence health include cities’geography and climate; housing conditions; accessto safe water and sanitation; transport systems;and air quality.
GEOGRAPHY AND CLIMATE. The geographicallocation and climate of cities are linked fundamen-tally to health. They influence residents’ vulnera-bility to natural disasters, including tornadoes,hurricanes or cyclones, floods, earthquakes, land-slides and fires. They also influence residents’health via heat waves, droughts and susceptibilityto illnesses carried by mosquitoes or other pests.
Climate change-related health impacts are alreadyhappening. A WHO assessment concluded that theeffects of climate change since the mid-1970s mayhave caused 150 000 additional deaths in 2000.48
This is probably an underestimate, consideringthat the study took into account only a subset ofpossible health impacts. It also concluded thatthese impacts are likely to increase in the future.The largest health risks are to children in thepoorest communities, the group that contributeleast to greenhouse gas emissions.49
The most adverse impacts of climate change arelikely to be in urban areas where people, resourcesand infrastructure are concentrated. In the future,climate change will increasingly multiply existingurban health risks through its impact on access towater and sanitation, food security and livingconditions, among other factors. Heat waves, airpollution, severe storms and infectious diseaseswill become more common (Box 2.1). Climatechange-related health risks will be greatest for theurban poor, who often lack adequate shelter oraccess to health services.23
Tropical mega-cities and coastal cities will beparticularly affected. Residents of these cities willbe exposed to a combination of health risks suchas heat waves, floods, infectious diseases and airpollution. The projected rise in sea level ofbetween 18 and 59 centimetres by the end of this
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS16

century50 will strain some of the largest andfastest-growing cities, located on coastlines ofdeveloping countries. Degraded natural protection(through deforestation and building on flood-plains), vast stretches of poor-quality housing, andextensive concrete ground cover without adequatedrainage will contribute to the vulnerability ofthese cities. Heavy rains will result in intense andsometimes lethal flash floods, such as those thatoccurred in and around Caracas, Bolivarian Republicof Venezuela, in 1999, and Mumbai, India, in 2005.51
HOUSING CONDITIONS. A roof over one’s head andan address in a habitable neighbourhood is a vitalstarting point for urban residents, from which theycan tap into what the city can offer them by way
of jobs, income, infrastructure and services. Decentshelter provides people with a home; security fortheir belongings; safety for their families; a placeto strengthen their social relations and networks; aplace for local trading and service provision; and ameans to access basic services.
Yet as described in Chapter 1, almost 900 millionurban residents live in slums and squatter settle-ments. Housing in these settings ranges fromhigh-rise tenements to shacks to plastic sheettents on sidewalks. These settings tend to beunregulated and overcrowded. They are oftenlocated in undesirable parts of the city, such assteep hillsides, riverbanks subject to flooding orindustrial areas.
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS 17
Climate change will exacerbate the impact of climate on urbanhealth, through heat waves, airpollution, severe storms and infectious diseases.51
The frequency and intensity of heatwaves will increase in the near future,causing particular problems in citiesdue to heat island effects. The urbanheat island effect is a phenomenonwhereby cities experience highertemperatures than surrounding ruralareas due to dense urban buildingsand lack of vegetation.
Increasingly severe and intenseflooding and storms will cause thedestruction of homes, health-carefacilities and other essentialservices, particularly in slums.Gradual sea level rise, coupled withstronger storm surges, will lead tomore frequent and severe coastalflooding and contamination of citywater supplies. The consequentdestruction of homes and communi-ties will eventually force unpro-tected populations to seek saferground, often increasing environ-mental and social pressures in theirnew locations.
Increasing temperatures and morevariable precipitation are alsoexpected to reduce crop yields inmany tropical developing regions.This is likely to worsen the burden of malnutrition in many cities ofthese areas.
Around the world, higher tempera-tures will endanger cities’ wateravailability and quality. Lack ofwater will compromise hygiene andincrease diarrhoea. Conversely,floods will cause contamination offreshwater supplies. In extremecases, water scarcity might result in famine.
The spread of illnesses carried by mosquitoes or other insects
and small animals is also expected to change as weather alters theirgeographical range, seasonal activityand breeding cycle. As such, climatechange may slow, halt or reverseprogress against infections such as diarrhoeal diseases, malaria and dengue.
Finally, rising temperatures willincrease levels of air pollutants suchas ground-level ozone. Urban outdoorair pollution caused more than 1.1 million deaths in 2004, mainlyfrom heart and lung diseases.52
A 1° Celsius rise in temperaturewould increase global deaths from air pollution by more than 20 000 people each year.53
BOX 2.1CLIMATE CHANGE: A MULTIPLIER OF HEALTH RISKS
UN Photo/Fardin Waezi
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS18
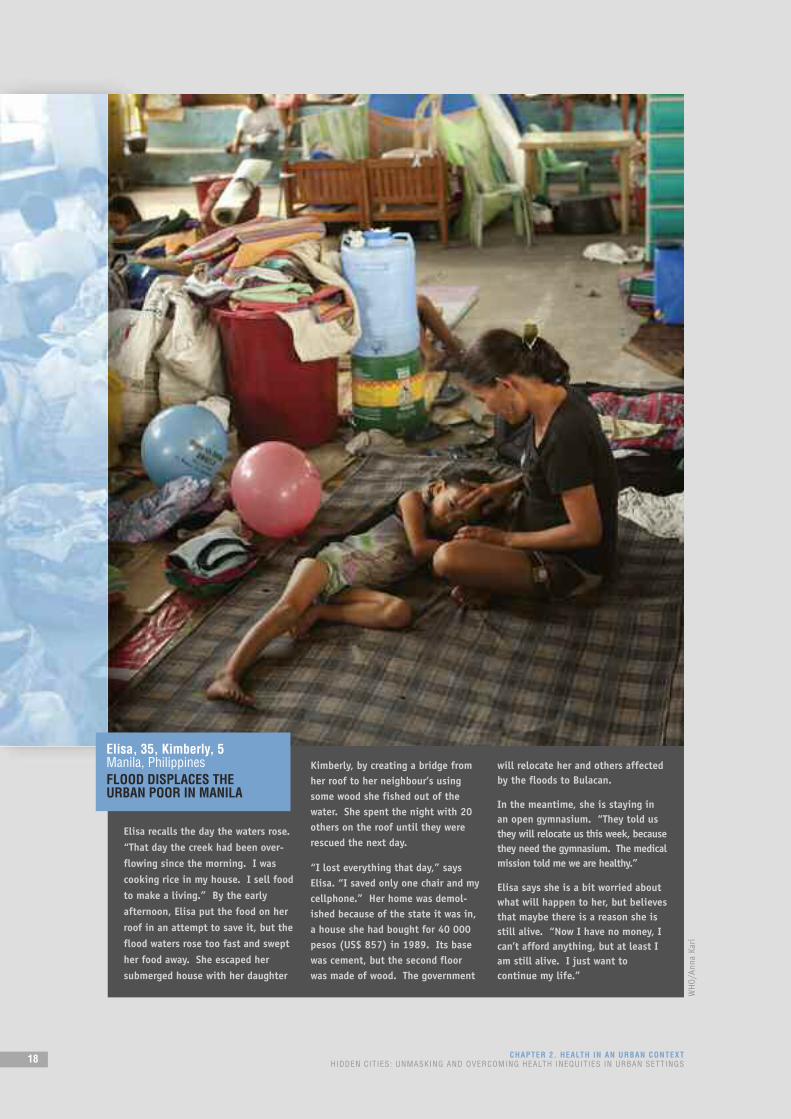
Elisa recalls the day the waters rose.“That day the creek had been over-flowing since the morning. I wascooking rice in my house. I sell foodto make a living.” By the earlyafternoon, Elisa put the food on herroof in an attempt to save it, but theflood waters rose too fast and swepther food away. She escaped hersubmerged house with her daughter
Kimberly, by creating a bridge fromher roof to her neighbour’s usingsome wood she fished out of thewater. She spent the night with 20others on the roof until they wererescued the next day.
“I lost everything that day,” saysElisa. “I saved only one chair and mycellphone.” Her home was demol-ished because of the state it was in,a house she had bought for 40 000pesos (US$ 857) in 1989. Its basewas cement, but the second floorwas made of wood. The government
will relocate her and others affectedby the floods to Bulacan.
In the meantime, she is staying inan open gymnasium. “They told usthey will relocate us this week, becausethey need the gymnasium. The medicalmission told me we are healthy.”
Elisa says she is a bit worried aboutwhat will happen to her, but believesthat maybe there is a reason she isstill alive. “Now I have no money, Ican’t afford anything, but at least Iam still alive. I just want tocontinue my life.”
Elisa, 35, Kimberly, 5Manila, PhilippinesFLOOD DISPLACES THE URBAN POOR IN MANILA
WHO/Anna Kari

Apart from those living in slums, countless otherurban residents suffer from unsuitable livingconditions, including building defects, poor ventilation of cooking and heating fuels, inade-quate or non-existent refrigeration or other foodstorage facilities, and hazardous locations such asproximity to highways or hazardous waste sites.47
Inadequate housing, especially where tenure isinsecure, is associated with injuries, respiratoryproblems, infectious diseases and mental health problems.54
Overcrowding is an additional health hazard. Whilerelatively rare in high-income countries, over-crowding is widespread in cities of low- andmiddle-income countries. The highest proportionsof urban residents without sufficient living spaceare in Africa and Asia; these are the same regionsthat have the most slums.1 The concentration ofpeople living in small, poorly ventilated livingareas increases the risk of disease transmissionand other health problems. Infectious diseasesthrive in overcrowded areas due to lack of ventila-tion, lack of hygiene and unhealthy environmentalexposures. Overcrowding also contributes to stressand family violence, including child maltreatment,intimate partner violence and sexual violence, andelder abuse.55,56
People with disabilities require accessible housingto live independently in their communities. Acces-sibility is dependent on the nature and extent ofpeople’s disabilities. For some, access may involvesmall modifications such as grab bars, whereas forwheelchair users, access may require ramps, widedoorways and low countertops.
ACCESS TO SAFE WATER AND SANITATION. Indeveloped countries, access to safe water andsanitation created the conditions for a dramaticreduction in deaths from infectious diseases in thelate 19th and early 20th centuries; now cities indeveloping countries are facing these same chal-lenges and opportunities.54
Almost half of city dwellers in Africa, Asia andLatin America suffer from at least one diseasecaused by lack of safe water and sanitation.57 Insub-Saharan Africa, poor people spend at least onethird of their incomes for treatment of waterborneand water-related diseases such as malaria,diarrhoea and worm infections.58
Although most official statistics reflect bettercoverage in urban areas than in rural areas, varioussurveys show that in many cities, the quantity andquality of water available to poor residents fallsshort of acceptable standards. Hundreds of millionsof people who supposedly have access to wateronly have access to communal pipes shared bydozens of people. For many urban families who arepoor, hours each day are lost just carrying waterfrom distant sources. Others use water from tankertrucks or bottles provided by private vendors, at prices often far higher than those paid bywealthier residents, who obtain their water frompublic water supply systems.
Proper sanitation is also important for preventinginfectious diseases. While a greater proportion ofthe urban population, compared with ruralresidents, has access to basic sanitation, overallrisk exposure is greater in cities due to denselypopulated living conditions. Most cities in low-and middle-income countries do not have sewers;as a result, one quarter to one half of these urbanresidents lack access to sanitation that signifi-cantly reduces their risk of illness.59 In many urbansettings, especially densely populated areas,latrines do not significantly reduce the risk ofdisease because of their unhealthy conditions.
TRANSPORT SYSTEMS. The modes of transport citydwellers use on a day-to-day basis have majorimplications for their health, and for the health ofthe broader population.60,61 Transport systemsinfluence health directly and indirectly, throughtheir impact on physical activity, road trafficsafety, air quality and psychosocial stress. Yetdespite the many ways in which transport systemsaffect health, the links are often unacknowledgedor overlooked.
Transport systems have an impact on levels ofregular physical activity among urban dwellers.Pedestrian- and bicycle-friendly cities, as well asthose with robust public transportation options,encourage physical activity. Conversely, overre-liance on private, motorized transport acts as abarrier to regular physical activity. Globally, insuf-ficient physical activity caused 3.2 million deathsin 2004.62
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS 19

Lack of proper urban planning can produce heavytraffic through residential areas, speeding andcompetition with pedestrians for limited roadspace.63 Poor planning also provides limitedcrossing points, poor pedestrian access toamenities and a lack of separation of people fromvehicle traffic, and inadequately regulated masstransit systems.64,65 All these factors contribute toroad traffic injuries.
Transport systems also influence health through airquality. Both the total number of motorizedvehicles and the level of traffic congestioncontribute substantially to air pollution in urbanareas. Air pollution is considered further in thefollowing section.
Social health and well-being also are affected.Transport systems can compromise mental andphysical health through noise pollution, chronicstress and social isolation. Lack of reliable trans-portation can be a barrier to accessing healthservices and generate opportunities for violence.
When transport systems are poorly designed, theurban poor suffer disproportionately. They areusually the most dependent on non-motorizedtransport and public transport, which can beneglected in transport development. Poor familiesoften work and live directly alongside congestedurban streets, and thus may be exposed most
directly to the health hazards of road traffic. In particular, underprivileged urban children,whose primary playground is often the street, are vulnerable to road traffic injury as well as tothe health and developmental effects of air andnoise pollution.
The urban poor are also at risk for other types ofroad traffic injury. At an early stage of urbaniza-tion, pedestrians and bicyclists are at much higherrisk of injury than those that can afford to usemotor vehicles.63 As economies develop, the urbanpoor tend to buy private motorcycles, while carsare purchased by wealthier city dwellers. Theinjury risk for motorcycles is much higher than forcars, so again a disparity develops between richand poor urban residents.
The poor, however, are not the only populationgroup to suffer the effects of poorly designedtransport systems. People with disabilities areparticularly affected by transport systems that donot accommodate the use of assistive devices orsensory impairments. Ultimately, traffic conges-tion, traffic-generated air pollution and trafficinjuries touch the lives of all city residents.
AIR QUALITY. All city dwellers are affected byindoor and outdoor air quality. Air pollutioncompromises lung function and increases heartattacks.66 In addition, high levels of air pollution
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS20
UND
P

directly affect people with asthma and other typesof lung or heart disease.
WHO estimates that urban outdoor air pollutioncaused approximately 1.1 million deaths worldwidein 2004.62 The air that city dwellers breathe isoften polluted from outdoor sources such asmotorized vehicles, industry and burning trash.People living in deprived neighbourhoods tend tohave higher levels of air pollution exposure thanthose living in higher-income areas.67 A surveyconducted in Rome, for example, showed thatpeople of low socioeconomic status were morelikely to live near busy roads and suffer thenegative effects of air pollution.68
Indoor sources of air pollution include smoke fromindoor stoves, machinery in small, poorly venti-lated workshops producing noxious fumes andsecond-hand tobacco smoke. WHO estimates thatin 2004, indoor smoke from solid fuels causedalmost 2 million deaths, while occupationalexposure to airborne particulates caused an addi-tional 457 000 deaths.62 The living conditionstypical of cities create the potential for substantialexposure to second-hand tobacco smoke,69 particu-larly for people in low-paid and insecure work.
SOCIAL AND ECONOMIC ENVIRONMENT
The social and economic environment has a majorimpact on the health of city dwellers. Influencesrange from local to global. For example, the 2007global financial crisis precipitated by the downturnin the United States housing market and thesubsequent collapse of major financial institutionsaffected the lives of countless urban residents,including many who previously thought that theyhad no connection to the workings of globalfinancial markets. In many cities around the world,unemployment has risen, social services and publicentitlements have been cut, wages have beenslashed and loans have become difficult to obtain.
Specific social and economic factors discussed in the next sections are access to economic andeducational opportunities, safety and security,social support and cohesion, and gender equality.
ECONOMIC AND EDUCATIONAL OPPORTUNITIES. City
dwellers’ access to economic opportunities –
whether employment or other income-generating
activities – has a major impact on their health
status. At a material level, access to economic
opportunities translates into access to good-
quality housing, water and sanitation, and other
daily necessities. Beyond helping to meet material
needs, access to economic opportunities provides
a means by which people can participate fully
within their communities and broader society.
Globalization – and in particular, trade liberaliza-
tion, cross-border financial flows and the
emergence of a global labour pool – has brought
both opportunities and risks for city dwellers. For
some, globalization has created job insecurity and
poverty; for others, it has opened new economic
opportunities.70
Informal economy workers constitute the majority
of workers in most countries and the number of
informally employed, unprotected and low-income
workers is increasing rapidly in both developing
and developed countries. The occupational health
and safety hazards they face are often added to
those of poor living environments, poor nutrition
and unsatisfactory housing. They are not covered
by social protection or comprehensive health care
and besides work-related injury and disease, they
are commonly affected by poverty-related diseases.71
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS 21
WHO/Anna Kari

At a local level, the economic environment also
influences health through the degree of wealth
disparity within a city. Relative poverty – often
defined as living on less than 60% of the national
median income – has been shown to relate to poor
health and risk of premature death, arguably
through the psychosocial stress of low socioeco-
nomic status and the poorer quality of social relations.
Access to educational opportunities provides the
foundation for future access to economic opportu-
nities. Education equips people with knowledge
and skills for daily living, increases opportunities
for income and job security, provides people with a
sense of control over life circumstances and
enables them to participate in society. Children
and adolescents who receive good-quality
education are set onto life pathways that affect
their health and well-being over time. Conversely,
children with low levels of education are more
likely to have poor health as adults.72
SAFETY AND SECURITY. Three major threats to the
safety and security of cities are urban crime and
violence, insecurity of tenure and forced evictions,
and natural and human-made disasters.73 The latter
two topics are discussed elsewhere in this report;
urban crime and violence are described below.
Crime and violence are typically most severe in
urban areas and are compounded by their rapid
growth. Sixty percent of urban dwellers in devel-
oping and transitional countries have been victims
of crime, over a five-year period, with victimiza-
tion rates reaching 70% in parts of Latin America
and Africa. In Latin America, the rapidly expanding
metropolitan areas of Rio de Janeiro, São Paulo,
Mexico City and Caracas account for more than half
of the violent crimes in their respective countries.
The homicide rate in Rio de Janeiro has tripled
since the 1970s, while the rate in São Paulo has
quadrupled. In Africa, cities such as Lagos, Johan-
nesburg, Cape Town, Durban and Nairobi account
for a sizeable proportion of their country’s crime.73
Both perceived and real levels of crime and
violence in urban areas influence health. Crime
directly affects the quality of life not only of
victims, but also of their friends, family and thegeneral community in which they live.72 Publicopinion surveys in the United Kingdom and theUnited States repeatedly show that people rankcrime among their top everyday concerns. InNairobi, Kenya, more than half of residents worryabout crime all the time or very often. Likewise, inLagos, Nigeria, 70% percent of surveyed residentsreport being fearful of becoming victims of crime,with 90% being fearful of the prospects of beingkilled in a criminal attack.73
Fear of crime isolates communities and has financialrepercussions for individuals, governments and theprivate sector.72 Concerns about violence isolatethe poor in their homes and the rich in theirsegregated spaces.74 For all, fear and insecuritypervade people’s lives, with serious implicationsfor trust and well-being among communities.47
Violence in urban areas takes a variety of forms,ranging from self-directed violence to interper-sonal violence and collective violence.75 Acts ofviolence have a devastating impact on people’shealth and livelihoods in many urban areas.76 Theyalso have many other costs, such as undermining acity’s economic prospects. The situation in somehigh-income countries is as bad as in many devel-oping countries, and the underlying social deter-minants are similar.47 Major contributors includesocial exclusion, poverty, unemployment and poorhousing conditions.
SOCIAL SUPPORT AND COHESION. The social environ-ment influences health in urban areas throughbuffering or enhancing the impact of stressors,and regulating access to the emotional andmaterial goods that influence health.54
High levels of social support have been shown tocontribute to a variety of positive health outcomes.Social support gives people the emotional andpractical resources they need, and can have apowerful protective effect on health. Conversely,social isolation and exclusion are associated withpoor health status and premature death.77
Social cohesion – the quality of social relation-ships and the existence of trust, mutual obliga-
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS22
tions and respect in communities or in the widercity – helps to protect people and their health.Societies with high levels of income inequalitytend to have less social cohesion and more violentcrime. High levels of mutual support will protecthealth, while the breakdown of social relationsreduces trust and increases violence.77
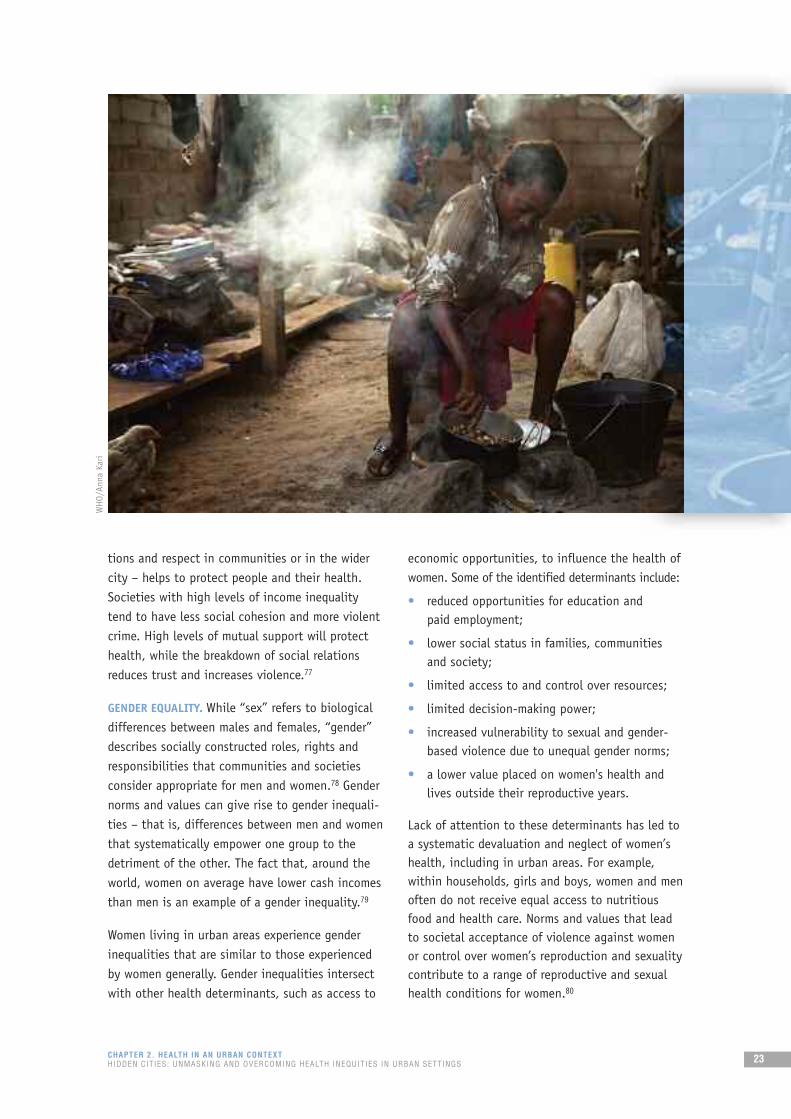
GENDER EQUALITY. While “sex” refers to biologicaldifferences between males and females, “gender”describes socially constructed roles, rights andresponsibilities that communities and societiesconsider appropriate for men and women.78 Gendernorms and values can give rise to gender inequali-ties – that is, differences between men and womenthat systematically empower one group to thedetriment of the other. The fact that, around theworld, women on average have lower cash incomesthan men is an example of a gender inequality.79
Women living in urban areas experience genderinequalities that are similar to those experiencedby women generally. Gender inequalities intersectwith other health determinants, such as access to
economic opportunities, to influence the health ofwomen. Some of the identified determinants include:
• reduced opportunities for education and paid employment;
• lower social status in families, communitiesand society;
• limited access to and control over resources;
• limited decision-making power;
• increased vulnerability to sexual and gender-based violence due to unequal gender norms;
• a lower value placed on women's health andlives outside their reproductive years.
Lack of attention to these determinants has led toa systematic devaluation and neglect of women’shealth, including in urban areas. For example,within households, girls and boys, women and menoften do not receive equal access to nutritiousfood and health care. Norms and values that leadto societal acceptance of violence against womenor control over women’s reproduction and sexualitycontribute to a range of reproductive and sexualhealth conditions for women.80
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS 23
WHO/Anna Kari

FOOD SECURITY AND QUALITY
The surge in food prices since the end of 2006 hasled to increasing hunger in the world’s poorestcountries and made urban food security moreprecarious. Poor urban families use up to 70% oftheir income to purchase food, often neglectingeducation, child care and other costs. In countriesdeeply affected by famine or drought, families eatfewer meals, and children stop attending school tosave education fees in order to pay for food. Thedoubling of global food prices over the last threeyears could potentially push 100 million people in low-income countries deeper into poverty.81
Malnutrition and stunted development will become more common.
Paradoxically, urbanization has also been associ-ated with a shift towards calorie-dense diets, char-acterized by high levels of fat, sugar and salt.Processed foods, ready-to-eat meals and snackspurchased from street vendors, restaurants andfast food outlets have increased in most cities,
magnifying residents’ opportunities to consumehigh-fat, calorie-dense food. As a result, obesity ison the rise in cities around the world.
In middle- and high-income countries, it is thepoor who tend to be more obese than the wealthy,which has been viewed as something of a contra-diction. It is likely that several factors contributeto this relationship, but one explanation is thatcalorie-dense foods, such as fried or processedfoods, tend to cost less on a per-calorie basiswhen compared with fresh fruit and vegetables.82,83
SERVICES AND HEALTH EMERGENCY MANAGEMENT
A range of health and social services influenceurban health, including direct services such aseducation, health care and community-basedsupport, as well as governments’ capacity torespond to a wide range of public health threatsthat can strike urban centres. Key aspects of urbanhealth systems that can influence city dwellers’
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS24
UN Photo/Eskinder Debebe

health are examined in greater detail below: accessto good-quality primary care services, universalcoverage and health emergency management.
ACCESS TO GOOD-QUALITY PRIMARY CARE SERVICES.Cities offer at least some opportunities foraccessing good-quality health care: health-carefacilities are overwhelmingly concentrated incities, and skilled health workers tend to flock tourban areas, especially those with teachinghospitals and higher incomes.
At the same time, many cities contain a complexcombination of public, private and non-profitproviders, with health facilities governed bydifferent authorities, from national ministries ofhealth to municipal authorities. Hospitals andspecialists have gained a pivotal role, often at theexpense of primary care services. Shortfalls inprimary care have resulted in the emergence of aninformal sector of unregulated, commercial healthcare in many cities. There are cities in Africa, forexample, where public primary care has almost orcompletely disappeared, and been replaced byunregulated, commercial providers.
Unregulated, commercial health care raises seriousquality concerns. It most often results in patientseither not getting the care they need, or gettingcare that they do not need, and in any eventpaying too much for it. Unregulated, commercialcare is often of substandard quality, and may beineffective and unsafe. Adverse effects or compli-cations put patients in a vicious cycle – needingmore care and becoming more impoverished.
Social factors, such as the lack of culturally appro-priate services, language barriers and prejudice onthe part of health workers can also prevent poorand marginalized city dwellers, especiallymigrants, from accessing care. These same groupsoften lack a basic understanding of how tonavigate the health system, and are thereforevulnerable to being preyed upon by unethical orincompetent health workers, providing poor-quality or even harmful care.
Good-quality primary care reduces exclusion and health disparities, and organizes healthservices around people's needs and expectations.When countries at the same level of economicdevelopment are compared, those where health
care is organized around the tenets of primaryhealth care produce a higher level of health for the same investment.84
UNIVERSAL COVERAGE. As defined by WHO MemberStates, universal coverage would require all peopleto have access to needed health services – preven-tion, promotion, treatment and rehabilitation –without the risk of financial hardship associatedwith accessing services. Universal coverage impliesnot only financial risk protection, but also primarycare networks (see previous section). It protectscity dwellers from foregoing essential health care because of financial costs, or facing severefinancial hardship and even impoverishment.85
In many cities, the urban poor face challenges inaccessing health services due to their inability topay out-of-pocket expenses for services. (This is incontrast to rural settings, where the main accessissue facing residents is that health facilities are farfrom their homes and communities.) Even at many“free” public clinics, patients are required to pay formedications and supplies, if not for consultations.
Many urban dwellers at some point will face a direchoice: either to go without essential treatment,or to seek treatment and go into poverty. Althoughthe first choice may seem more economicallyviable in the short term, over time it often leadsto even more severe impoverishment throughdisability, loss of income and premature death.86
Governments, typically at the national level, havea responsibility to ensure that all people canreceive the services they require and that they areprotected from the financial risks associated withusing them. Over the past century, a number ofcountries have achieved this level of protection.European countries began, for example, to putsocial health protection schemes in place in thelate 19th century, moving towards universalcoverage after the Second World War through tax-financed or social health insurance systems, ormore commonly, a blend of the two. More recently,Chile, Costa Rica, Cuba, the Republic of Korea,Thailand and Turkey have ensured access to coreservices with financial risk protection to theirentire populations. China, Colombia and Mexicoamong others are at various stages towards theimplementation of ambitious plans to achieveuniversal coverage in the near future.
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS 25
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS26
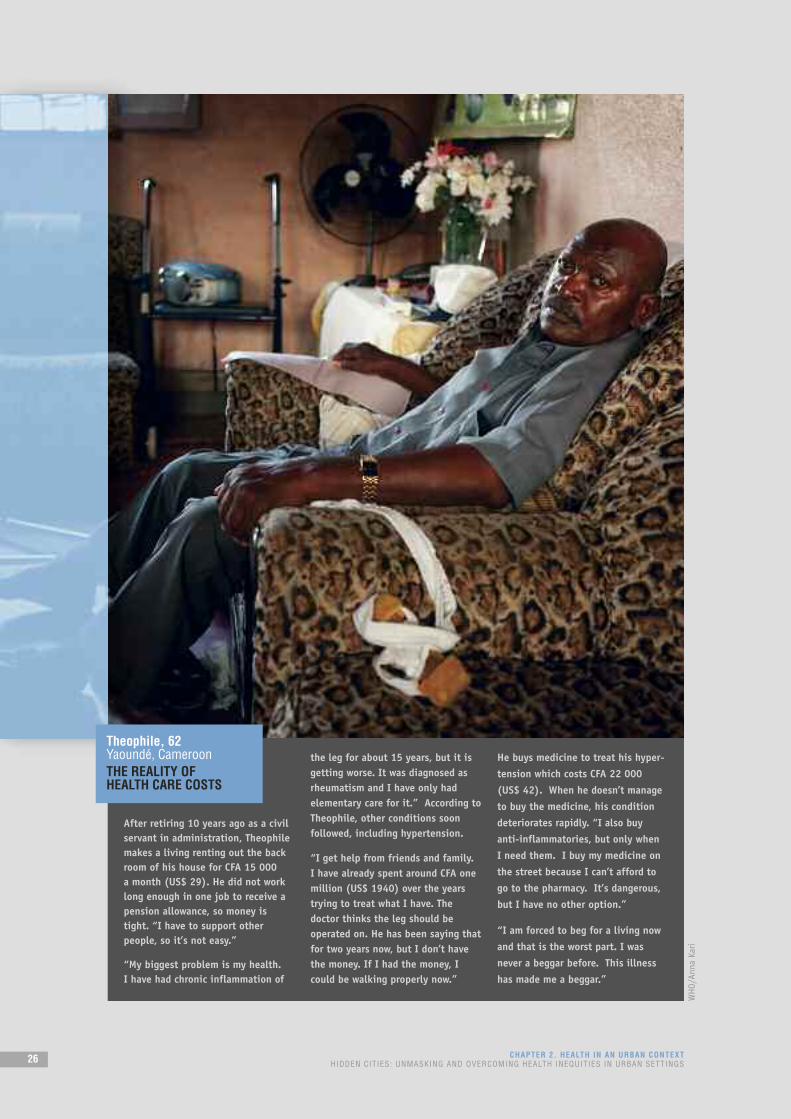
After retiring 10 years ago as a civilservant in administration, Theophilemakes a living renting out the backroom of his house for CFA 15 000 a month (US$ 29). He did not worklong enough in one job to receive apension allowance, so money istight. “I have to support otherpeople, so it’s not easy.”
“My biggest problem is my health. I have had chronic inflammation of
the leg for about 15 years, but it isgetting worse. It was diagnosed asrheumatism and I have only hadelementary care for it.” According toTheophile, other conditions soonfollowed, including hypertension.
“I get help from friends and family. I have already spent around CFA onemillion (US$ 1940) over the yearstrying to treat what I have. Thedoctor thinks the leg should beoperated on. He has been saying thatfor two years now, but I don’t havethe money. If I had the money, Icould be walking properly now.”
He buys medicine to treat his hyper-
tension which costs CFA 22 000
(US$ 42). When he doesn’t manage
to buy the medicine, his condition
deteriorates rapidly. “I also buy
anti-inflammatories, but only when
I need them. I buy my medicine on
the street because I can’t afford to
go to the pharmacy. It’s dangerous,
but I have no other option.”
“I am forced to beg for a living now
and that is the worst part. I was
never a beggar before. This illness
has made me a beggar.”
Theophile, 62Yaoundé, CameroonTHE REALITY OF HEALTH CARE COSTS
WHO/Anna Kari

HEALTH EMERGENCY PREPAREDNESS AND RESPONSE.
A city’s degree of health emergency preparednessand community resilience has a major influence onthe health of its residents when disaster strikes.The impact of natural disasters (such as extremeweather events and earthquakes), chemical andradiological hazards, fires, transport crashes andepidemics is amplified by both the populationdensity and built environment of urban areas.Health facilities might be damaged, destroyed oroverwhelmed, and the health workforce might belost, leaving people with limited access to healthand emergency services when they are mostneeded (see Box 2.2 for example of response toHaiti earthquake, January 2010).87
In today’s interconnected world, cities are proneto the import of infectious diseases. Business and
leisure travellers, migrants, and imported animals
and animal products are all potential carriers of
infectious agents. Cities also are the places to
which people with new and unusual illnesses are
brought, because they are beyond the scope of
rural clinics. Once an infectious pathogen arrives,
cities become an efficient engine for its rapid
national and international spread, due to their
population density and multiple transport links
through bus and train stations, large international
airports and seaports (Box 2.3 on the next page).
Biosafety and biosecurity also are important
because large cities not only host major research
laboratories and biotechnology companies, but
also constitute targets of choice for deliberate
epidemics and malicious poisoning.
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS 27
Urban areas in Haiti sufferedimmense devastation by the earth-quake that struck on 12 January2010. Thirty percent of buildingswere destroyed in the capital, Port-au-Prince, and other cities wereseverely damaged. The earthquakedisrupted Haiti’s services that weredesigned to save lives and treat thewounded. Many government buildingsand hospitals were destroyed, andcountless government officials andhealth workers were killed. Evenbefore the earthquake, the country’shealth status was already the lowestin the western hemisphere, andmore than 70% of Haitians survivedon less than US$ 2 a day.
The large international response was beset by numerous logisticaland infrastructure challenges,including how to receive anddistribute large amounts of aid to 3 million people in a setting whereairports and seaports were damagedand roads were blocked by rubble.Working with their bare hands,ordinary Haitians saved tens ofthousands of people from the rubblein the first hours of the earthquake,before any international teamarrived in the country.
Despite great damage caused to key government buildings,national authorities were keen to reclaim control of the overallcoordination of the humanitarianresponse, which United Nations and other international partnerssupported. Local organizations, such as the Haitian Red Cross, wereinstrumental in delivering servicesto affected people, and the survivorsthemselves were greatly responsiblefor providing shelter, support andcare to their fellow Haitians.
Among other pressing issues, Haitiansmust now consider ways in which themany thousands of people who under-went amputations can access reha-bilitative care and ongoing supportin their communities. Urban plannerswill need to determine how they canenable people with amputations to liveand travel easily within cities. Morebroadly, the challenge for Haiti andits partners will be to move from thehumanitarian response phase to a realdevelopment strategy that may ensurea better future for generations to come.
BOX 2.2SPOTLIGHT ON HAITI’S EARTHQUAKE
UN Photo/Sophia Paris

Conflict and insecurity in urban environments and the movement of people from crises in ruralareas to cities pose other significant humanitarianchallenges. Slums – and their associated healthhazards – can proliferate as large numbers ofdisplaced people seek refuge at the margin ofurban areas.
The degree to which governments are prepared tomanage these kinds of circumstances affects notonly city dwellers, but also the country as a whole.When urban areas, which are countries’ mostconcentrated sources of health, logistic and otherresources, are affected by emergencies, assistanceto the rest of the country becomes restricted.
Health consequencesof living in citiesAs outlined in the previous section, good-qualityhousing and living conditions, social and economicopportunities, and access to services such aseducation and health care contribute to the healthand well-being of city dwellers. The higher levelsof social support and greater social cohesiontypically found in urban areas are also linked to anumber of positive health outcomes. Good urbangovernance underpins the realization of these andother determinants of health.
At the same time, cities present a number of healthrisks, especially when they are poorly governed orfail to sufficiently prioritize health in all policies.Many are confronted by a triple threat: infectiousdiseases exacerbated by poor living conditions;noncommunicable diseases and conditions (such asheart disease, cancer and diabetes) and conditionsfuelled by tobacco use, unhealthy diets, physicalinactivity and harmful use of alcohol; and injuries(including road traffic accidents) and violence.89
INFECTIOUS DISEASES
Infectious diseases are a major threat in many citiesdue to population density, overcrowding, lack of safewater and sanitation systems, international travel andcommerce, and poor health-care access, particularly in urban slums. The 2003 outbreak of SARS (seeBox 2.3) is a case in point. Other infectious condi-tions, such as the human immunodeficiency virus(HIV), tuberculosis, pneumonia and diarrhoealinfections, have an ongoing presence in cities.
Frequently, it is the urban poor who suffer thegreatest burden. Slums are productive breedinggrounds for tuberculosis, hepatitis, dengue,pneumonia, cholera and diarrhoeal diseases, whichspread easily in highly concentrated populations.
Women face particular vulnerability to HIVinfection, stemming from a combination of biolog-ical factors and gender inequality. Female drugusers and sex workers are particularly at risk;stigma, discrimination and punitive policies onlyincrease their vulnerability.90
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS28
In 2003, severe acute respiratory syndrome (SARS)– the first severe new disease of the 21st century –highlighted the fact that no city is automaticallyprotected by virtue of its wealth or its standards ofliving and health care from either the arrival of anew disease or the subsequent disruption it cancause. SARS was, to a large extent, a disease ofprosperous urban centres. Contrary to expectations,it spread most efficiently in sophisticated cityhospitals. Fortunately, the spread of SARS washalted less than four months after it was firstrecognized as an international threat. Had SARSbeen allowed to establish a foothold in a resource-poor setting, it is doubtful whether the demandingmeasures, facilities and technologies needed tostop it could have been fully deployed.88
BOX 2.3SPREAD OF SARS VIA URBAN CENTRES
Jelle Boontje/SXC.com

NONCOMMUNICABLE DISEASES
Noncommunicable diseases and conditions, such asasthma, heart disease and diabetes, are a significantproblem in urban centres. Most of this heightenedrisk can be traced back to changes in diet andphysical activity as a consequence of urbanization,as well as exposure to air pollutants, includingtobacco smoke. As mentioned in the subsection on “food security and quality”, urbanization isassociated with a shift towards calorie-dense diets, characterized by high levels of fat, sugar and salt.As a result, obesity is on the rise in cities aroundthe world. On top of this, people in cities tend tohave physically inactive types of employment, andurban sprawl further discourages physical activity.Other factors that inhibit regular physical activityinclude overcrowding, high-volume traffic, overre-liance on motorized transportation, crime and poorair quality. Air pollution, including tobacco smoke, isa risk factor for asthma and other respiratory diseases.
Rapid urbanization also threatens mental health.Poor housing conditions, overcrowding, noisepollution, unemployment, poverty and culturaldislocation can cause or exacerbate a range ofmental health problems, including anxiety, depres-sion, insomnia and substance abuse.91,92,93
INJURIES AND VIOLENCE
About 16 000 people die every day as a result ofinjuries – about 10% of all deaths. The principalcauses of death from injury are road trafficaccidents (22%), suicide (15%) and homicide(10%), with war accounting for another 3%.94
Road traffic injuries alone are responsible for 1.3 million deaths per year globally. In manydeveloping countries, urbanization and theincreased number of motorized vehicles have not been accompanied by adequate transportinfrastructure, enforcement of traffic regulations or implementation of measures to ensure improved road safety. Low- and middle-incomecountries have higher road traffic fatality rates(20.1 and 22.1 per 100 000 population, respec-tively) than high-income countries (11.9 per 100 000).97 And, more than 90% of the world’sroad fatalities occur in low- and middle-incomecountries, which have only 48% of the world’sregistered vehicles.95
Worldwide, over 1.6 million people lose their lives to violence each year.76 Suicide accounts for 844 000 deaths, homicide for 600 000 deathsand collective violence for 184 000 deaths.96,97
For every person who dies from violence, manymore are injured and suffer a range of physical,mental and other consequences.76 Child maltreat-ment, youth violence, intimate partner violence,sexual violence and elder abuse, although unlikelyto result in death, are other highly prevalent forms of violence with significant behavioural and health consequences. Major contributors tourban violence include social exclusion, poverty,unemployment and poor housing conditions. The fear of such violence further contributes to the fragmentation of cities, socially, economicallyand politically.74 Young people are particularlyaffected by urban violence. In urban areas, peopleaged 15 to 24 commit the largest number ofviolent acts, and are also the principal victims of violence.32
CHAPTER 2. HEALTH IN AN URBAN CONTEXTHIDDEN CITIES: UNMASKING AND OVERCOMING HEALTH INEQUITIES IN URBAN SETTINGS 29
CHAPTER SUMMARY
This chapter has explained how broad physical, social and economic determinants influence the health
of people, and looked at some key determinants in urban areas. Health determinants in cities span the
domains of the natural and built environment, the social and economic environment, food security and
quality, services and health emergency management, and urban governance. n In practice, many
cities offer both the best and worst environments for health and well-being. This dichotomy will be
explored in detail in Part Two of this report.