chapter 26: the thorax and abdomen
TRANSCRIPT

Chapter 26: The Thorax and Abdomen








Assessment of the Thorax Abdomen
• Injuries to this region can produce life-threatening situations
• ATC’s evaluation should focus on signs and symptoms that indicate potentially life-threatening conditions
• Continually monitor breathing, circulation and any indication of internal bleeding or shock

• History– What happened to cause this injury?– Was there direct contact or a direct blow?– What position were you in?– What type of pain, was it immediate or gradual,
location(s)?– Difficulty breathing?– What positions are most comfortable?– Do you feel faint, light-headed or nauseous?– Chest pain?

– Hear or feel snap, crack or pop in your chest?– Muscle spasms?– Blood or pain during urination?– Was the bladder full or empty?– How long has it been since you last ate?– Is there a personal or family history of any
heart, abdominal problems or other diseases involving the abdomen and thorax?

• Observations– Is the athlete breathing? Are they having difficulty breathing? Does
breathing cause pain?– Is the athlete holding the chest wall?– Is there symmetry of the chest during breathing?– If the athlete’s wind was knocked out, is normal breathing returning?
How rapidly?– Body position
• Thorax injury - leaning towards side that is injured and splinting area w/ hand• Abdominal injury - lie on side w/ knees pulled to chest• Male external genitalia injury - lying on side holding scrotum

– Check for areas of discoloration, swelling or deformities• Around umbilicus = intra-abdominal bleed
• Flanks = swelling outside the abdomen
– Protrusion or swelling in any portion of abdomen (internal bleeding)
– Does the thorax appear to be symmetrical?– Are the abdominal muscles tight and guarding?– Is the athlete holding or splinting a particular part?– Blood -
• Bright red = lung injury
• Vomiting bright red and frothy = injury to esophagus and stomach although blood may be swallowed from mouth and nose

– Cyanosis - respiratory difficulty– Pale, cool, clammy skin indicates low BP– Monitor vital signs (pulse, respiration, BP)
• Rapid weak pulse or drop in BP is an indication of a serious internal injury (involves blood loss)
• Palpation– Thorax
• Check for symmetry of chest wall movement and search for areas of tenderness
• Palpate along ribs and intercostal spaces as well as costochondral junctions• AP pressure to rib cage to assess for fracture• Transverse pressure assesses costochondral junction• Semi-reclining position is useful if athlete is having difficulty breathing

– Abdomen• Patient should have arms at side, knees and hips flexed to relax abdomen• Four abdominopelvic quadrants (move clockwise starting from upper
right quadrant)• Feel for guarding and tenderness, rigidity (internal bleeding)• Rebound tenderness• Assess each organ (if possible)
• Auscultation– Heart Sounds
• “Lubbdupp” (may hear 3rd sound in children)• Listen for murmur (abnormal period due to valve insufficiency)
– Functional murmur versus pathogenic condition



The Auscultation Assistant.mht

– Breath sounds• Should be consistent
• Abnormal patterns– Cheyne-Stokes breathing (rate changes over 1-3 minutes)
– Biot’s breathing - normal rate followed by cessation
– Apneustic breathing - pauses in respiratory cycle at full inspiration
– Wheeze or rhonchi or rales
• Perform over apex, centrally and at base of each lung, both anteriorly and posteriorly
– Bowel sounds• Liquid-like gurgling due to peristalsis

• Percussion– Place fingers on abdomen and strike with other
hand– Solid organ = dull sound– Hollow organ = tympanic or resonant sound



Recognition and Management of Specific Injuries
• Rib Contusion– Etiology
• Blow to the rib cage can bruise ribs, musculature or result in fracture
– Signs and Symptoms• Painful breathing (particularly if muscles are involved)
• Point tenderness; pain with rib compression
– Management• RICE and NSAID’s
• Rest and decrease in activity

• Rib Fractures– Etiology
• Caused by a direct blow or the result of a violent muscular contraction
• Can be caused by violent coughing and sneezing
– Signs and Symptoms• History is critically important
• Pain with inspiration, point tenderness and possible deformity with palpation
– Management• Refer for X-rays
• Support and rest; brace

• Costochondral Separation– Etiology
• Result of a direct blow to the anterolateral aspect of the rib cage
– Signs and Symptoms• Localized pain in region of costochondral junctions
• Pain with movement; difficulty with breathing
• Point tenderness and possible deformity
– Management• Rest and immobilization
• Healing may take 1-2 months

• Sternum Fractures– Etiology
• Result of high impact blow to the chest• May also cause contusion to underlying cardiac muscle
– Signs and Symptoms• Point tenderness over the sternum• Pain with deep inspiration and forceful expiration• Signs of shock, or weak rapid pulse may indicate more severe
injuries
– Management• X-ray and monitor athlete for signs of trauma to the heart

• Muscle Injuries– Etiology
• Muscles are subject to contusions and strains• Occur most often from direct blows or sudden torsion of the trunk
– Signs and Symptoms• Pain occurs on active motions; pain with inspiration and expiration,
coughing, sneezing and laughing
– Management• Immediate pressure and application of cold for approximately one hour• After hemorrhaging is controlled, immobilize the injury to make the
athlete comfortable

• Breast Injury– Etiology
• Constant uncontrolled movement (particularly in large breasted women)• Stretching of Cooper’s ligament• Runner’s and cyclist’s nipple
– Management• Females should wear well-designed bra that has minimum elasticity and
allows for little movement• Special plastic cup-type brassieres may be required in sports with high
levels of physical contact• Use of an adhesive bandage can be used to prevent runner’s nipple• Wearing a windbreaker can prevent cyclist nipple

• Breast Cancer– Should be of great concern to all women– Most common cause of cancer in females– Females over 20 years old should perform breast
self-examinations every month and receive a clinical evaluation every 3 years
– Not all lumps are cancer -- may be benign fibrous cyst
– Mammograms are not recommended until age 40

• Lung Injuries– Etiology
• Pneumothorax - – pleural cavity becomes filled with air, negatively pressurizing the cavity, causing a
lung to collapse– Will produce pain, difficulty with breathing and anoxia
• Tension Pneumothorax– Pleural sac on one side fills with air displacing lung and heart, compressing the
opposite lung– May cause shortness of breath, chest pain, absence of breath sounds, cyanosis,
distention of neck veins, deviated trachea
• Hemothorax– Blood in pleural cavity causes tearing or puncturing of the lungs or pleural tissue– Painful breathing, dypsnea, coughing up frothy blood and signs of shock

• Traumatic Asphyxia– Result of a violent blow or compression of rib cage– Causes cessation of breathing– Signs include purple discoloration of the trunk and head,
conjunctivas of the eye– Condition requires immediate mouth to mouth resuscitation
– Management• Each of these conditions are medical emergencies and
require immediate attention
• Transport athlete to hospital immediately

• Hyperventilation– Etiology
• Rapid rate of ventilation due to anxiety induced stress or asthma• Develop a decreased amount of carbon dioxide relative to oxygen
– Signs and Symptoms• Athlete has difficulty getting air in and seems to struggle with breathing• Panic state with gasping and wheezing
– Management• Decrease rate of carbon dioxide loss• Slow respiration rate and alter respiration techniques• Breath into a bag• Normal respiration should return within 1-2 minutes, initial cause must be
determined
• Heart Contusion– Etiology
• Result of compression between sternum and spine• Most severe consequence would involve an aortic rupture
– Signs and Symptoms• Severe shock and heart pain• Heart may exhibit arrhythmias causing a decrease in cardiac output,
followed by death if medical attention is not administered
– Management• Immediate referral to an emergency room• Prepare to administer CPR and treat for shock

• Sudden Death Syndrome in Athletes– Etiology
• Hypertrophic cardiomyopathy- thickening of cardiac muscle w/ no increase in chamber size
• Anomalous origin of coronary arteries• Marfan’s syndrome- abnormality in connective tissue results in weakening of
aorta and cardiac vessels• Series of additional cardiac causes• Non-cardiac causes include drugs and alcohol, intracranial bleeding,
obstructive respiratory disease
– Signs and Symptoms• Most do not exhibit any signs prior to death• May exhibit chest pain, heart palpitations, syncope, nausea, profuse
sweating, shortness of breath, malaise and/or fever
– Management/Prevention• Counseling and screening are critical in early
identification and prevention of sudden death• Screening questions should address the following
– History of heart murmurs
– Chest pain during activity
– Periods of fainting during exercise
– Family history
– Thickening of heart or history of Marfan’s syndrome
• Cardiac screening - electrocardiograms and echocardiograms

• Kidney Contusion– Etiology
• Result of an external force (force and angle dependent)• Susceptible to injury due to normal distention of blood
– Signs and Symptoms• May display signs of shock, nausea, vomiting, rigidity of back muscles and
hematuria (blood in urine)• Referred pain (costovertebral angle posteriorly radiating forward around the trunk)
– Management• Monitor status of urine (hematuria) - refer if necessary• 24 hour hospitalization and observation with a gradual increase in fluid intake if an• Surgery may be required if hemorrhaging continues• 2 weeks of rest and close surveillance following initial return to activity is
necessary

• Kidney Stones– Etiology
• Unknown cause
– Signs and Symptoms• Calculus - stone composed of crystalline mineral salts that
forms in urinary tract
• Painful condition
– Management• Usually passes through the urethra and is excreted (very
painfully)

• Contusion of Ureters, Bladder and Urethra– Etiology
• Blunt force to the lower abdomen may avulse ureter or contuse/rupture bladder
• Hematuria is often associated with contusion of bladder during running (runner’s bladder)
• Injury to the urethra (more common in males) may produce severe perineal pain and swelling
– Signs and Symptoms• Pain, discomfort of lower abdominal region, abdominal rigidity, nausea,
vomiting, shock, bleeding from the urethra, increased quantity of bloody urine,
• Inability to urinate will present in case of ruptured bladder

• Contusion of Ureters, Bladder and Urethra– Signs and Symptoms (continued)
• Referred pain to low back and trunk as well as upper thigh region anteriorly and suprapubically
– Prevention• Check periodically for blood in urine
• Empty bladder prior to practice or competition
• Wear protective equipment

• Cystitis• Inflammation of the bladder associated with a urinary tract infection• May involve kidney, prostate, and urethra• Causes frequent, painful urination, chills and fever • Antibiotics are required for treatment
• Urinary Tract Infections• Caused by staphylococcus bacteria or chlamydia• Causes burning and painful urination and requires antibiotics for treatment• Can be prevented through increased fluid intake, practicing sanitary bowel
and bladder habits, washing genitals before intercourse, emptying the bladder after intercourse, removal of contraceptive diaphragms and sponges following intercourse

• Urethritis• Inflammation of the urethra -- generally caused by
gonorrhea or by other nongonococcal organisms
• Symptoms include pain on urination along with urethral discharge
• Treated with antibiotic therapy

• Gastrointestinal Bleeding– Etiology
• Distance running, gastritis, iron-deficiency anemia, ingestion of aspirin or NSAID’s, stress, bowel irritation, colitis
– Signs and symptoms• Blood in stool
• Abdominal pain, watery stool (w/pus) dehydration, intermittent fever (if colitis is involved)
– Management• Refer to physician is bleeding is occurring
• Liver Contusion– Etiology
• Blunt trauma - right side of rib cage• More susceptible if enlarged due to illness (hepatitis)
– Signs and Symptoms• Hemorrhaging and shock may present• May require immediate surgery• Presents with referred pain in right scapula, shoulder and substernal
area and occasionally in left anterior side of chest
– Management• Referral to a physician for diagnosis and treatment

• Pancreatitis– Etiology
• Inflammation of pancreas (acute or chronic) due to obstruction of pancreatic duct
• Acute conditions may lead to necrosis, suppuration, gangrene and hemorrhage
• Chronic cases may develop scar tissue, causing malfunction -- may develop due to chronic alcoholism
– Signs and Symptoms• Acute epigastric pain causing vomiting, belching, constipation and potentially
shock
• Tenderness and rigidity to palpation
• Chronic cases may result in jaundice, diarrhea and mild to moderate pain that radiates into the back

• Pancreatitis (continued)– Management
• In acute cases, re-hydration is necessary along with pain reduction, treatment of shock, reduction of pancreatic activity through medication
• Surgery if the duct is blocked
• Chronic cases require large doses of analgesics, pancreatic enzymes and modified diet

• Indigestion (Dyspepsia)– Etiology
• Some athletes develop food idiosyncrasies which cause them distress after eating• Reactions before competition• Emotional stress, esophageal and stomach spasms, or inflammation of mucous
linings in stomach and esophagus
– Signs and Symptoms• Increased HCl secretion, nausea, and flatulence
– Management• Elimination of irritating foods, development of regular eating habits, avoidance
of anxieties that cause gastric distress• If problems persist or athlete appears high strung and nervous -- follow-up with a
physician is needed

• Vomiting– Etiology
• Result of some irritation, most often in the stomach• Stimulates vomiting center of the brain, causing a series
of forceful diaphragm and abdominal contractions to compress stomach
– Management• Antinausea medications should be administered• Fluids to prevent dehydration (by mouth or
intravenously depending on the situation)

• Food Poisoning (Gastroenteritis)– Etiology
• Ranges from mild to severe• Caused by infectious microorganisms that contaminate food particularly during
warm weather and periods of improper refrigeration
– Signs and Symptoms• Nausea, vomiting, cramps, diarrhea and anorexia• Usually subsides within 3-6 hours (staph. infection)• Salmonella infection may last 24-48 hours or more
– Management• Rapid replacement of fluids lost• Bed rest in all but mild cases• Nothing should be given by mouth if vomiting and nausea persist• Re-introduce easy food first

• Peptic Ulcer– Etiology
• Acids destroy mucous lining of stomach or small intestine
• Occurs in individuals with long periods of severe anxiety
– Signs and Symptoms• Gnawing pain, localized to gastric region
• Appears 1-3 hours following a meal
• Dyspepsia, heartburn, nausea, vomiting, w/ pain lasting minutes rather than hours
– Management• Antacids if pain persists
• If hemorrhaging or perforation occurs, surgery may be required

• Gastroesophageal Reflux– Etiology
• Reflux or backward flow of the acidic gastric contents into the esophagus (malfunctioning esophageal sphincter)
• Result of a hiatal hernia w/ incidence increased with activity
• Repeated bouts can result in inflammation of lower esophagus
– Signs and Symptoms• Heartburn-like retrosternal pain - similar to angina pectoris sensation
• Burning feeling with sour liquid taste in throat
– Management• Medication first, surgery if condition persists

• Diarrhea– Etiology
• Abnormal, loose stool or passage of fluid, unformed stool
• Acute or chronic
• Caused by a problem in diet, inflammation of the intestinal lining, GI infection, ingestion of certain drugs and psychogenic factors
– Signs and Symptoms• Abdominal cramps, nausea, vomiting and frequent elimination of
stools
• Loss of appetite, and a light brown or gray, foul-smelling stool
• Extreme weakness caused by dehydration

• Diarrhea (continued)– Management
• Determine cause (irritant, infection, or emotional upset)
• ATC can treat less severe cases by omitting certain foods from athlete’s diet
• Have athlete consume bland food that does not irritate system
• Provide pectins 2-3 times daily to absorb excess fluid

• Constipation– Etiology
• Failure of the bowels to evacuate feces• Causes include, lack of abdominal tone, insufficient moisture in the
feces, lack of roughage and bulk in diet to stimulate peristalsis, poor bowel habits, nervousness, anxiety, and overuse of laxatives and enemas
– Signs and Symptoms• Feeling of fullness, with occasional cramping and pain in lower
abdomen• If straining occurs during defecation, blood vessels may be ruptured
– Management• Regulate eating patterns (cereal, fruits, vegetables)• Deal with psychological aspects• Avoid medications unless prescribed by a physician

• Irritable Bowel Syndrome– Etiology
• Group of gastrointestinal tract disorders
– Signs and Symptoms• Abdominal pain that is relieved with defecation, irregular pattern of
defecation (at least 25% of the time), alterations in stool frequency, form, and passage, abdominal bloating and distension
– Management• Refer to physician for long-term management• Diet modification and antidiarrheal medications may be helpful
initially as well as psychological counseling• Long term prognosis -- good
• Appendicitis– Etiology
• Inflammation of the vermiform appendix (chronic or acute)• Result of blockage, lymph swelling, or carcinoid tumor• Early stages it presents as a gastric complaint, that gradually develops from red
swollen vessel to a gangrenous structure that can rupture into bowels causing peritonitis
– Signs and Symptoms• Mild to severe pain in lower abdomen, associated with nausea, vomiting and
low grade fever• Pain may localize in lower right abdomen (McBurney’s point)
– Management• Surgical intervention is often necessary (particularly if it is resulting in an
obstructed bowel = life threatening)
• Hemorrhoids (Piles)– Etiology
• Varicosities of the hemorrhoidal venous plexus of the anus
• Constant straining or constipation may result in stretching of anal vessels, protrusion and bleeding, or a thrombus forming in the external vessels
– Signs and Symptoms• Painful nodular swellings near the anal sphincter
• May cause slight bleeding and itching
– Management• Use of proper bowel habits, ingestion of mineral oil daily to assist in
lubricating a dry stool, application of suppository and anesthetic (for pain and itching)
• Surgery may be required if these measures fail

• Scrotal Contusion– Etiology
• Result of blunt trauma and contusion to the vulnerable and sensitive scrotum
– Signs and Symptoms• Hemorrhaging, fluid effusion, muscle spasm, severe
pain (disabling)
--Management•Reduction of testicular spasm Application of cold pack•Unresolved pain after 15-20 minutes requires referral to a physician

• Spermatic Cord Torsion– Etiology
• Result of testicle revolving in the scrotum following a direct blow or as the result of coughing or vomiting
– Signs and Symptoms• Acute testicular pain, nausea, vomiting and inflammation in
the area
– Management• Immediate medical care is required to prevent irreparable
complications
• Traumatic Hydrocele of the Tunica Vaginalis– Etiology
• Fluid accumulation caused by a severe blow to the testicular region (venous plexus on the posterior aspect of the testicle becomes engorged)
• Rupture of the plexus results in rapid accumulation of blood in the scrotum (hematocele)
– Signs and Symptoms• Pain and significant swelling in the scrotum
– Management• Cold pack application and referral to a physician

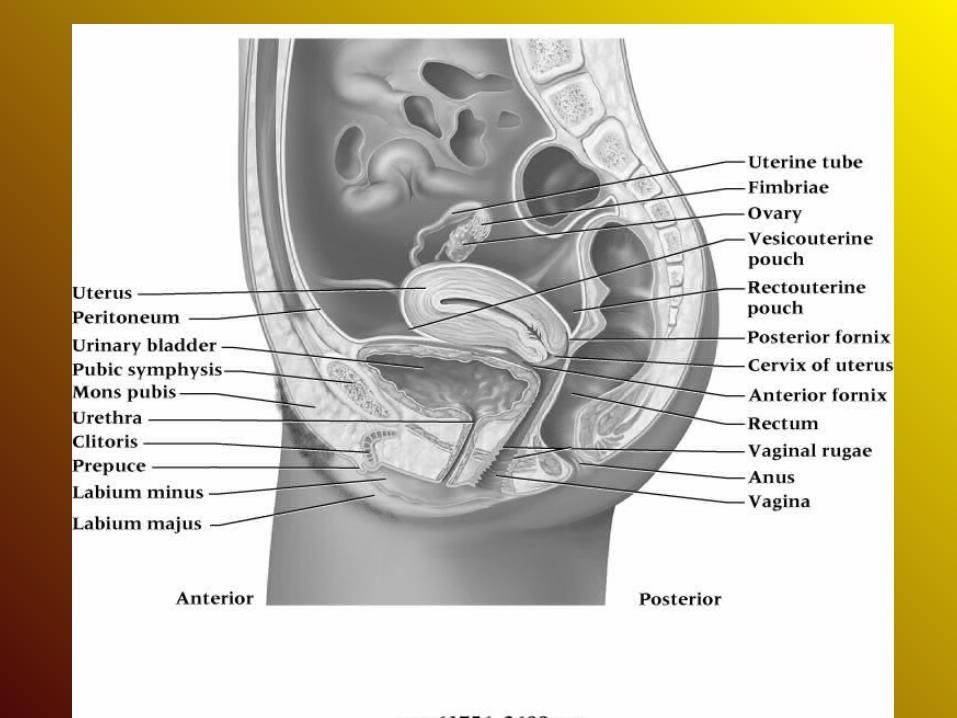
• Vaginitis– Etiology
• Inflammation of the vagina can be caused by a variety of microorganisms, bacterial infections, chemicals from douching, irritation from a tampon or poor hygiene habits
– Signs and Symptoms• Purulent and bloody vaginal discharge; strong odor with vaginal itching• Frequent and painful urination• Vagina is red and painful to the touch
– Management• Vaginitis caused by an STD will require appropriate antibiotic or
antifungal medication• Instruction on proper bladder and bowel hygiene as well as sexual
behavior may also be necessary

• Contusion of the Female Genitalia– Etiology
• Low incidence of injury in sports
• Most common occurrence involve contusion of external genitalia (vulva - including the labia, clitoris and the vaginal vestibule)
– Signs and Symptoms• Hematoma results from contusion - may also
involve pubic symphysis resulting in osteitis pubis

• Injury of the Spleen– Etiology
• Result of a direct blow, infectious mononucleosis (causing an enlarged spleen)
– Signs and Symptoms• Indications of a ruptured spleen involve history of a direct blow, signs of
shock, abdominal rigidity, nausea, vomiting• Kehr’s sign
– Management• Ability to splint self may produce delayed hemorrhaging - easily disrupted
resulting in internal bleeding• Conservative treatment involves 1 wk of hospitalization and a gradual
return to activity• Surgery will result in three months of recovery while removal of spleen
will result in a 6 month removal from activity

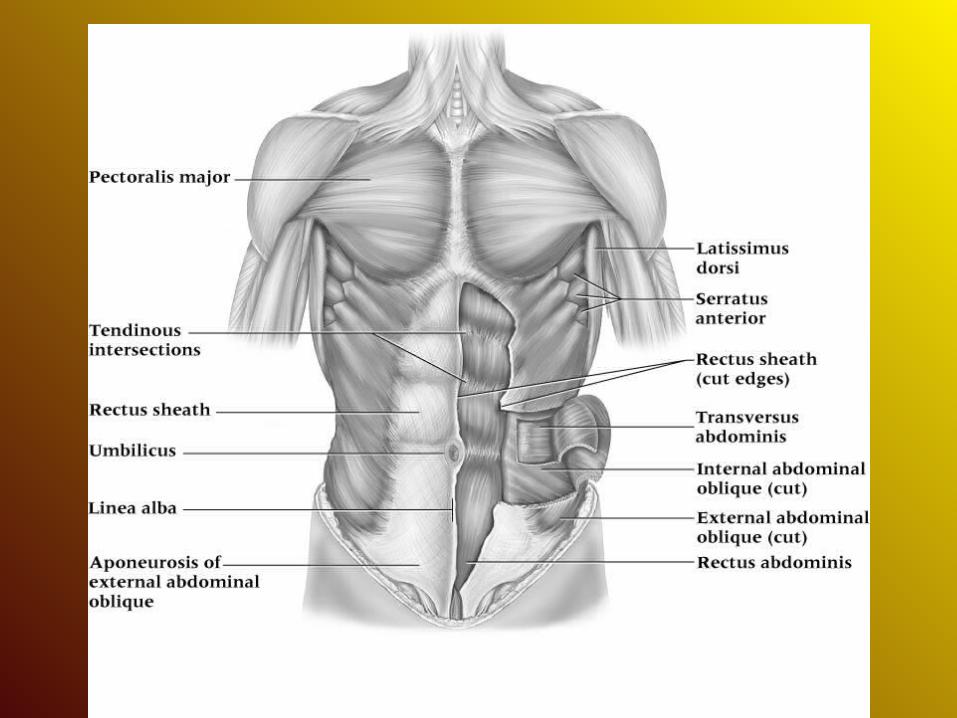
• Abdominal Muscle Strain– Etiology
• Result of sudden twisting or reaching of trunk, tearing abdominal musculature
– Signs and Symptoms• Severe pain and hematoma formation• Generally involves rectus abdominus
– Management• Ice and compression with conservative treatment• Exercise within pain free limits

• Contusions of Abdominal Wall– Etiology
• Caused by a compressive force - generally occurring in collision sports• Extent of injury depends on whether force is blunt or penetrating
– Signs and Symptoms• May cause a hematoma to develop under fascia of surrounding muscle
tissue• Swelling may cause pain and tightness w/in the region
– Management• Cold pack and compression• Be sure to check for signs of internal injuries

• Hernia– Etiology
• Protrusion of abdominal viscera through portion of abdominal wall (congenital or acquired)
• Inguinal vs. femoral hernias • Complications and strangulated hernias
– Signs and Symptoms• Acquired hernia occur when natural weakness is further aggravated by a direct blow or
strain– History of direct blow to groin area, pain and prolonged discomfort, superficial protrusion with pain
increasing with coughing & reported pulling sensation in groin area
– Management• Surgery is preferred by most physicians• Mechanical devices are not suitable for athletics due to friction and irritation they
produce

• Blow to Solar Plexus– Etiology
• Transitory paralysis of the diaphragm
– Signs and Symptoms• Stops respiration and leads to anoxia
• Generally transitory
– Management• Must help athlete overcome apprehension
• Use short inspirations and long expirations
• Calm athlete, prevent hyperventilation
• ATC should question possibility of internal injury

• Stitch in the Side– Etiology
• Idiopathic condition with obscure cause and several hypotheses– Constipation, intestinal gas, overeating, diaphragmatic spasm, poor conditioning, lack of
visceral support and weak abdominals, distended spleen, breathing techniques resulting in lack of oxygen, ischemia of diaphragm or intercostal muscles
– Signs and Symptoms• Cramp-like pain that develops on either the right or left costal angle during
hard physical activity
– Management• Relaxation of the spasm
– Stretch arm on affected side as high as possible– Flex trunk forward on the thighs
• Additional problems may warrant further study