chapter quality network (cqn) asthma pilot project team progress presentation
DESCRIPTION
State Name: Ohio Practice Name: Pediatric Associates of Mt. Carmel, Inc. Team Members: Jennifer Richard, MD; Maryjane Fee. Chapter Quality Network (CQN) Asthma Pilot Project Team Progress Presentation. Progress Summary Since Learning Session 1. Key Driver Engaging QI Team/Practice - PowerPoint PPT PresentationTRANSCRIPT
Chapter Quality Network (CQN)
Asthma Pilot Project Team Progress Presentation
State Name: OhioPractice Name: Pediatric Associates of Mt. Carmel, Inc.Team Members: Jennifer Richard, MD; Maryjane Fee

GLOBAL CQN AIMWe will build a sustainable quality improvement infrastructure within our practice to achieve measurable improvements in asthma outcomesSpecific Aim From fall 2009 to fall 2010, we will achieve measurable improvements in asthma outcomes by implementing the NHLBI guidelines and making CQN’s key practice changes
Measures/Goals
Outcome Measures: >90% of patients well controlled
Process Measures >90% of patients have “optimal” asthma care (all of the following) assessment of asthma control using a validated instrument stepwise approach to identify treatment options and adjust therapy written asthma action plan patients >6 mos. Of age with flu shot (or flu shot recommendation)
>90% of practice’s asthma patients have at least an annual assessment using a structured encounter form
Engaging Your QI Team and Your Practice*The QI team and practice is active and engaged in improving practice processes and patient outcomes
Using a Registry to Manage Your Asthma Population *Identify each asthma patient at every visit *Identify needed services for each patient *Recall patients for follow-up
Using a Planned Care Approach to Ensure Reliable Asthma Care in the Office * CQN Encounter Form * Care team is aware of patient needs and
work together to ensure all needed services are completed
Developing an Approach to Employing Protocols * Standardize Care Processes * Practice wide asthma guidelines
implemented
Providing Self management Support
* Realized patient and care team relationship
Key Drivers
Interventions
Form a 3-5 person interdisciplinary QI Team
Formally communicate to entire practice the importance and goal of this project
Meet regularly to work on improvement
All physicians and team members complete QI Basics on EQIPP
Collect and enter baseline data
Generate performance data monthly
Communicate with the state chapter and leaders within the organization
Turn in all necessary data and forms
Attend all necessary meetings and phone conferences
Select and install a registry tool
Determine staff workflow to support registry use
Populate registry with patient data
Routinely maintain registry data
Use registry to manage patient care & support population management
Select template tool from registry or create a flow sheet
Determine workflow to support use of encounter form at time of visit
Use encounter form with all asthma patients
Ensure registry updated each time encounter form used
Monitor use of encounter form
Select & customize evidence-based protocols for your office
Determine staff workflow to support protocol, including standing orders
Use protocols with all patients
Monitor use of protocols
Obtain patient education materials
Determine staff workflow to support SMS
Provide training to staff in SMS
Assess and set patient goals and degree of control collaboratively
Document & Monitor patient progress toward goals
Link with community resources
CQN Asthma Project Practice Key Driver Diagram Version 2.0

Progress Summary SinceLearning Session 1
• Key Driver– Engaging QI Team/Practice
• Very Good Progress– QI Team Established– All physicians completed QI Basics– Performance data reviewed– Meetings/Conferences attended
– Using a registry• Little Progress
– Practice wants to wait until EMR utilized– Planned Approach
• Good Progress– Encounter form used with all asthma patients– Established protocols (next slide)
– Self Management Approach• Fair Progress
– Education materials provided– Patient progress monitored

Most progress in our office has been achieved in providing more consistent care by all physicians by establishing
standard office protocols.
• Protocols Established– Asthma patient follow-up visits:
• 24 hours of Urgent Care/ER visit • 72 hours of starting oral steroid in office• 2-4 weeks of starting controller medications• Six month follow-up from well child care visit
• Asthma Acton Plan Initiated– All well child visits all asthma patients– Instituted at first follow-up visit for asthma exacerbations
• Peak Flow Meter use for all age appropriate patients– Demonstrated at time of asthma action plan– RX given and PFM numbers reviewed at one or six month visits
• Educational Materials– Asthma “tool box” at each office to review inhaler use and written
educational materials– Given at initial visit

Follow-up Visit Recommended

Asthma Action Plan

Educational Materials Provided

Optimal Asthma Care

PDSA Cycles
PDSA Title:
Plan:
Do:
Study:
Act:

TEST 1What:Who (population):Who (executes):Where:When:
P D
S A
TEST 2What:Who (population):Who (executes):Where:When:
P D
S A
TEST 3What:Who (population):Who (executes):Where:When:
P D
S A
TEST 4What:Who (population):Who (executes):Where:When:
P D
S A
TEST 1What:Who (population):Who (executes):Where:When:
P D
S A
TEST 2What:Who (population):Who (executes):Where:When:
P D
S A
TEST 3What:Who (population):Who (executes):Where:When:
P D
S A
TEST 4What:Who (population):Who (executes):Where:When:
P D
S A
TEST 1What:Who (population):Who (executes):Where:When:
P D
S A
TEST 2What:Who (population):Who (executes):Where:When:
P D
S A
TEST 3What:Who (population):Who (executes):Where:When:
P D
S A
TEST 4What:Who (population):Who (executes):Where:When:
P D
S A
PDSA Title PDSA Title PDSA Title
PDSA Ramps

Front office receptionist
identifies asthma patient
through problem list or chief complaint
CQN encounter from given to parent to complete
MA/Nurse reviews chart before patient in room parent
given encounter form if not already
done
Encounter not always completed by time physician in room
Well VisitPhysician review questionnaire
In room. Reviews medications and anyconcerns. Asthma action plan
completed or revised.Education materials
given.
CQN encounter form given to Front Office
Coordinator to be entered into EQIPP
Follow up visit scheduled to have Asthma action Plan completed
Educational Materials Reviewed
Office Flow Diagram
Asthma Sick VisitSymptoms and medications reviewed
Appropriate RX givenEducational Materials given
Encounter may be put on chart not given to parent
Parent may not stop to
schedule follow-up visit
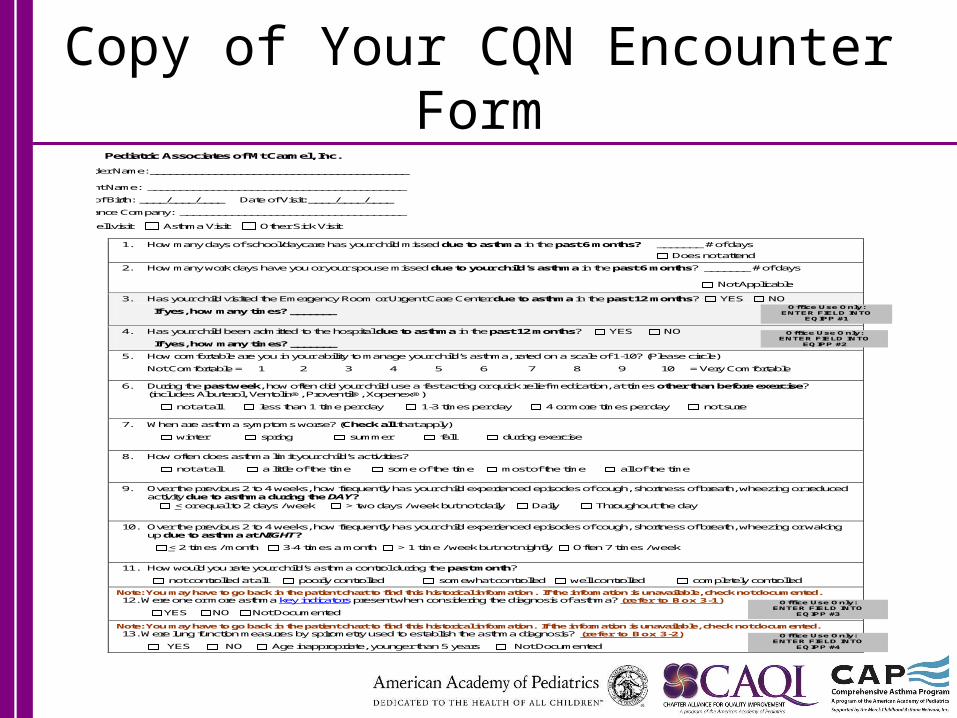
Copy of Your CQN Encounter Form
Pediatric Associates of Mt Carmel, Inc.
Provider Name: ________________________________________ Patient Name: ________________________________________ Date of Birth: ____/____/____ Date of Visit: ____/____/____
Insurance Company: ___________________________________
Well visit Asthma Visit Other Sick Visit
1. How many days of school/daycare has your child missed due to asthma in the past 6 months? _______ # of days
Does not attend
2. How many work days have you or your spouse missed due to your child’s asthma in the past 6 months? _______ # of days Not Applicable
3. Has your child visited the Emergency Room or Urgent Care Center due to asthma in the past 12 months? YES NO
If yes, how many times? _______
4. Has your child been admitted to the hospital due to asthma in the past 12 months? YES NO
If yes, how many times? _______
5. How comfortable are you in your ability to manage your child’s asthma, rated on a scale of 1 -10? (Please circle)
Not Comfortable = 1 2 3 4 5 6 7 8 9 10 = Very Comfortable
6. During the past week, how often did your child use a fast acting or quick relief medication, at times other than before exercise? (includes Albuterol, Ventolin®, Proventil®, Xopenex®)
not at all less than 1 time per day 1-3 times per day 4 or more times per day not sure
7. When are asthma symptoms worse? (Check all that apply)
winter spring summer fall during exercise
8. How often does asthma limit your child’s activities?
not at all a little of the time some of the time most of the time all of the time
9. Over the previous 2 to 4 weeks, how frequently has your child experienced episodes of cough , shortness of breath, wheezing or reduced activity due to asthma during the DAY?
1. < or equal to 2 days / week > two days / week but not daily Daily Throughout the day
10. Over the previous 2 to 4 weeks, how frequently has your child experienced episodes of cough, shortness of breath, wheezing or waking up due to asthma at NIGHT?
2. < 2 times / month 3-4 times a month > 1 time / week but not nightly Often 7 times / week
11. How would you rate your child’s asthma control during the past month?
not controlled at all poorly controlled somewhat controlled well controlled completely controlled
Note: You may have to go back in the patient chart to find this historical information. If the information is unavailable, check not documented. 12. Were one or more asthma key indicators present when considering the diagnosis of asthma? (refer to Box 3-1)
YES NO Not Documented
Note: You may have to go back in the patient chart to find this historical information. If the information is unavailable, check not documented. 13. Were lung function measures by spirometry used to establish the asthma diagnosis? (refer to Box 3-2)
YES NO Age inappropriate, younger than 5 years Not Documented
Office Use Only: ENTER FIELD INTO
EQIPP #1
Office Use Only: ENTER FIELD INTO
EQIPP #2
Office Use Only: ENTER FIELD INTO
EQIPP #3
Office Use Only: ENTER FIELD INTO
EQIPP #4

Encounter form page 2
14. Asthma severity level: (refer to the EPR3 Control Tables 4-2a, 4-2b, and 4-6)
Severe Persistent Moderate Persistent Mild Persistent Intermittent
15. Is the patient on a controller medication? YES NO Started this visit
If YES, does the patient/parent report using controller medications daily? YES NO
16. For patients who use rescue/controller inhalers, is a spacer utilized? YES NO NA (Maxair® and dry powder inhalers do not require spacer)
17. Has the patient received oral steroids for bronchospasm within the past 12 months? YES NO 18. Has the patient been seen by an allergist or pulmonologist during the last 12 months for assistance with asthma management due to
severity of illness? (refer to specialist referral criteria) Specialist: ___________________________________ YES NO Referred this visit
19. Were validated questions used to determine the current level of asthma control (if validated tool used or parent completed entire parent section, check “yes”)? YES NO
20 a. Physician assessment of control: What is the patient’s current level of control during the past month? (review the National Heart, Lung, and Blood Institute (NHLBI) Expert Panel Report 3 (EPR-3) control tables (refer to the EPR-3 Control Tables 3-5a, 3-5b, 3-5c, 4-2a, 4-2b, 4-6, 4-3a, 4-3b, 4-7)
Well Controlled Not Well Controlled Very Poorly Controlled 20 b. If “not well controlled” or “very poorly controlled”:
Did you identify reasons for lack of control? (Examples: exposure to allergens, tobacco smoke, indoor or outdoor pollutants and irritants, nonadherence to medication regimen) YES NO
21. For patients age 5 years and older, is spirometry currently scheduled, or have results been obtained within the last 1 year? (refer to Box 3-2)
YES date____/____/_____ NO Younger than 5 years 22. Have you used the age –appropriate NHLBI EPR-3 stepwise table to identify treatment options or to adjust therapy based on asthma
control? (refer to the Stepwise Tables 4-1a, 4-1b, 4-5)
YES NO
23a. If in active flu season (Sept.-March), was the flu shot administered? YES shot date: ___/___/_____
NO-reason: _______________________________________ Patient younger than 6 months, other contraindications, or vaccine unavailable
23 b. If patient has not yet received a flu shot during the current season (Sept.-March), or if between seasons, was the flu shot recommended? YES NO
24a. Does the patient have a written asthma action plan? YES NO
24 b. If yes, was the plan updated as needed and reviewed with the patient and/or family at this visit? YES NO
25. Were asthma self-management education and materials (other than or in addition to the asthma action plan) provided and explained to the patient and family at this visit? (Examples include correct medication techniques, avoiding environmental triggers, and getting help to quit smoking. See Figure 3–13 in EQIPP, Delivery of Asthma Education by Clinicians During Patient Care Visits for more information.)
YES NO
26. Follow Up Visit: Return in: _____ weeks, or _____ months Return visit date (Optional): _____ / _____ / _____
This form was developed specifically for the AAP Chapter Quality Network Asthma Pilot Project and originally developed by the Physicians
Hospital Organization at Cincinnati Children’s Hospital Medical Center
Office Use Only: ENTER FIELD INTO
EQIPP #5
Office Use Only: ENTER FIELDS INTO
EQIPP #6A and 6B
Office Use Only: ENTER FIELD INTO
EQIPP #8
Office Use Only: ENTER FIELD INTO
EQIPP #7
Office Use Only: IF “YES” IN EITHER 12A
or 12B ENTER FIELD INTO EQIPP #9
Office Use Only: If a follow-up visit was
scheduled ENTER FIELD INTO EQIPP #12
Office Use Only: ENTER FIELD INTO
EQIPP #10
Office Use Only: ENTER FIELD INTO
EQIPP #11

Key Learnings Establishing protocols increased consistency among doctors
Scheduling follow-up visit at time encounter increased compliance
Short term follow-up (ie. 3-7 days) increased compliance with medication/asthma regimens
Providing educational materials facilitated discussions at follow-up visit
Testing small changes in office procedure easier to track progress
Challenging to sustain interest in long term projects

Barriers and Successes
• Barriers– Large group practice– Communications– Time Constraints– Sustaining interest– Delegating PDSA Cycles
• Successes– Data collections– Asthma action plans

Future Plans
• Choose another validated instrument to assess asthma control ie. ACT
• Investigate use of spirometry in office• Investigate registry options with EMR