checklist for enrollment packet - putnam edge high … for enrollment packet ... prior written...
TRANSCRIPT
Checklist For Enrollment Packet
Please ensure that you have included the following when you return your enrollment
packet:
___ Pupil Information Sheet (front and back)
___ Additional Information Sheet
___ Code of Conduct Form
___ Request for Records Form
___ Academic Interest Form
___ LEP/Occupational Survey
___ Race & Ethnicity Form
___ Chronic Disease Information Form
___ Exemption Notice
___ Student Technology Policy
___ Immunization Record
___ Physical Examination Form
___ Student Birth Certificate (homeschooled & private students)

Pupil Information Sheet
______________________________ Florida Student Number
Last Name: _______________________________ First: ________________________ Middle: _______________________ Lunch Number: ___________________ Age: ________ Grade: _____________ Sex: ____________ SOCIAL SECURITY NUMBER (optional)___________________ In compliance with Florida Statute 119.071(5)(a), the school district issues this notification regarding the purpose of the collection and use of social security numbers. The school district collects social security numbers for use in performance of district duties and responsibilities. To protect identity, the school district will secure social security numbers from unauthorized access. The school district will never release social security numbers to unauthorized parties. Date of Birth: __________________________ Place of Birth __________________________________________________
City County State Race: White ______ Black _______ Hispanic _______ Indian _______ Asian _______ MultiRacial _______ School Last Attended: _________________________________ City: ____________________________ State: _________ Address: _____________________________________________________ ____ Phone Number: (_____) _____________
(INCLUDE NAME OF ANY PUBLIC OR PRIVATE SCHOOL) Has the student ever attended a Florida Public School PreK or K12 grade? Yes _____ No _____ Is student in an exceptional education program? Yes ______ No ______ Speech Therapy? Yes _____ No _____ State any previous expulsions, arrests resulting in a charge, and Juvenile Justice actions: ___________________________________________________________________________________________________ ___________________________________________________________________________________________________ Name of Father/Guardian: ____________________________________ Occupation: _______________________ Driver’s Licence Number: _____________________________________________ Date of Birth: _____________________ Home Phone Number: (_____) _____________ Cell Number: (_____) _____________ Mailing Address: ____________________________________________ City: _______________________ ZIP: _______ 911 Address: _______________________________________________ City: _______________________ ZIP _______ Employer: ______________________________ Address: ____________________________________________________ Phone Number:(_____) _____________ City: ____________________________ State: ______ ZIP: _______ EMail Address: ______________________________________________________________________________________ Name of Mother/Guardian: ____________________________________ Occupation: _______________________ Driver’s Licence Number: _____________________________________________ Date of Birth: _____________________ Home Phone Number: (_____) _____________ Cell Number: (_____) _____________ Mailing Address: ____________________________________________ City: _______________________ ZIP: _______ 911 Address: _______________________________________________ City: _______________________ ZIP _______ Employer: ______________________________ Address: ____________________________________________________ Phone Number: (_____) _____________ City: ____________________________ State: ______ ZIP: _______ EMail Address: ______________________________________________________________________________________ Pupil Lives With: ____ Both Parents ____ Father ____ Mother ____ Other: __________________________ Give Directions to the Student’s 911 Address: ______________________________________________________________ ___________________________________________________________________________________________________ SIGNATURE ____________________________________________________________ DATE ______________________ SWORN TO AND SUBSCRIBED BEFORE ME THIS _______ DAY of ______________ 20 __
_________________________________________________________
(Signature of Notary Public State of Florida)
Personally Known ____ OR Produced Identification ___ _________________________________________________________ Type of Identification Produced ________________________ (Print, Type, or Stamp Commissioned Name of Notary Public)
Please continue on back.

EMERGENCY INFORMATION: Name of Person to Contact in an Emergency Other Than Parents: ______________________________________________ Date of Birth: ________________________________ Relationship To Child: ______________________________________ Home Phone: (_____) _____________ Cell Phone: (_____) _____________ Work Phone: (_____) _____________ 911 Address: _______________________________________________ City: _______________________ ZIP _______ Second Person to Contact in an Emergency Other Than Parents: _______________________________________________ Date of Birth: ________________________________ Relationship To Child: ______________________________________ Home Phone: (_____) _____________ Cell Phone: (_____) _____________ Work Phone: (_____) _____________ 911 Address: _______________________________________________ City: _______________________ ZIP _______ Name of Brothers and Sisters living at Home AGE: GRADE: SCHOOL: _______________________________________________________ _______ ____________ ________________________ _______________________________________________________ _______ ____________ ________________________ _______________________________________________________ _______ ____________ ________________________ IF CHILD RIDES BUS: BUS NUMBER ________________________ DRIVER ____________________________________ IF CHILD DOES NOT RIDE BUS, HOW DOES HE OR SHE GET TO SCHOOL? ___________________________________
Parent’s Medical Authorization I do/do not (circle one) authorize the school to obtain necessary medical services for my son/daughter, ___________________________ in the event I cannot be located. My child’s doctor is: _____________________________ Phone number: ( ) ___________________. SIGNATURE ____________________________________________________________ DATE ______________________
Parent Consent for Health Screenings I hereby give consent for my child, _______________________________________ to participate in School Health Services Screenings conducted during the school year. Such screenings may include measurement of height, weight, vision, hearing, blood pressure, observation for scoliosis (spinal curvature), and nursing assessment for real or suspected health problems. It is understood no treatment will be administered without additional parental permission. Parents will be notified of any problems detected. Please list any problems, conditions or medications which might affect this child’s progress in school or participation in physical education, or other classes. ___________________________________________________________________________________________________ ___________________________________________________________________________________________________ SIGNATURE ____________________________________________________________ DATE ______________________ PCSB FORM #8330F1
* By typing your signature above you agree your electronic signature is the legal equivalent of your manual signature on this document.In doing this you also agree that you are the parent/legal guardian of the student on this form.
____ do ____ do not
______________________________________________________________ ________ ______________ ___________________________
______________________________________________________________ ________ ______________ ___________________________
If Child Rides Bus: Bus Number: ___________________ Driver: ____________________________________
If Child does not ride bus, How does he/she get to school: _________________________________________________
Additional Information Student Name: __________________________________ ☐ Enclose copy of student’s immunization records ☐ Enclose a copy of the student’s birth certificate (for private & home schooled students only) Transportation: ☐ Will ride the bus ☐ Will have private transportation ☐ Will walk to school ☐ Other: ________________________ Internet Access: ☐ Have at home ☐ Not at home If not at home, where will they have access after school: _____________________ Special Programs: ( i.e. 504, IEP, etc.) ☐ No ☐ Yes If yes, please explain: ____________________________________________________________________________________________________________________________________________

Code of Conduct
The Code of Conduct has been developed to help gain the greatest possible benefit from school experiences. It defines the responsibilities and rights of students attending Putnam County Schools. The consequences of student actions, which disrupt the learning process, are also clearly stated. Since parents/guardians can be held responsible for actions for their children, you should be involved in the education of your children. Students, parents, and schools working together will help maintain a safe atmosphere where students can learn. Putnam EDGE High School is in need of your cooperation. Parents and student please read and discuss this important booklet together. This form will be kept on file at the school and acknowledges your awareness of the contents. Failure to return this form will not relieve a student or parent(s)/guardian(s) from responsibility to know the contents of the Code of Conduct and will not excuse the student’s noncompliance with the Code of Student Conduct. The rules, regulations, and guidelines set out in this code of conduct are effective for the current school year and shall remain in effect until a new code of conduct is published.
Putnam EDGE High School Standard Artist Release
I hereby assign and authorize Putnam EDGE High School the right (all rights) in and to any picture, photograph, video, or similar data used for or related to a school purpose. I also authorize said producer, without limitation the right to reproduce, copy, cablecast, exhibit/publish, display on website, or distribute any such picture, expressly waive any rights or claims I may have against your FIRM and/or any of its affiliates, Subsidiaries, or Assigns except as outlined in this contract. _____________________________ ____________________________________________ ______________________ Parent/Guardian Name (Print) Parent/Guardian Signature Date _____________________________ ____________________________________________ ______________________ Student Name (Print) Student Signature Date
Putnam EDGE High School Parent/Guardian Internet Permission
PARENT OR GUARDIAN CONSENT (Required if student is under age 18) As the parent or guardian, I have read and understand the Guidelines for Telecommunications Use (including use of the school’s software, computer networks and the Internet) and have reviewed them with my child. I understand that this access is designed solely for educational purposes and Putnam EDGE High School has taken reasonable precautions to supervise Internet usage. However, I recognize that it is impossible for the School to control access to all information materials and I will not hold it responsible for materials acquired or contact made on the Internet. With that understanding, I hereby give permission for my child to utilize the school's Internet services. _____________________________ ____________________________________________ ______________________ Parent/Guardian Name (Print) Parent/Guardian Signature Date _____________________________ ____________________________________________ ______________________ Student Name (Print) Student Signature Date
Putnam EDGE High School Parent/Guardian Internet Permission
I (We) have received a copy and am (are) aware of the contents of the enclosed Putnam County Code of Conduct. Furthermore, I (we) are aware that supervision is provided 30 minutes before school begins and 30 minutes after school ends. _____________________________ ____________________________________________ ______________________ Parent/Guardian Name (Print) Parent/Guardian Signature Date _____________________________ ____________________________________________ ______________________ Student Name (Print) Student Signature Date * By typing your signatures above you agree your electronic signature is the legal equivalent of your manual signature on this document.In doing this you also agree that you are the student or parent/legal guardian of the student on this form.

Request for Records Student Name: __________________________________ Date of Birth: ___________ The student above has been enrolled at Putnam EDGE High School in grade: ____ Information to be released: ALL RECORDS, including Exceptional Education (IEP, all previous psychological reports). Florida Schools, please include recent FCAT Scores.
School last attended: __________________________ Phone #: (____)____________
School Address ______________________________ Fax #: (____)____________
City/State/Zip: __________________________________________________________
___________________________________________ ________________ Parent/Guardian Signature Date Federal law does not require prior written consent of the student or parent/guardian when releasing information to officials of the school to which the student intends to enroll.
* By typing your signature above you agree your electronic signature is the legal equivalent of your manual signatureon this document. In doing this you also agree that you are the parent/legal guardian of the student on this form.
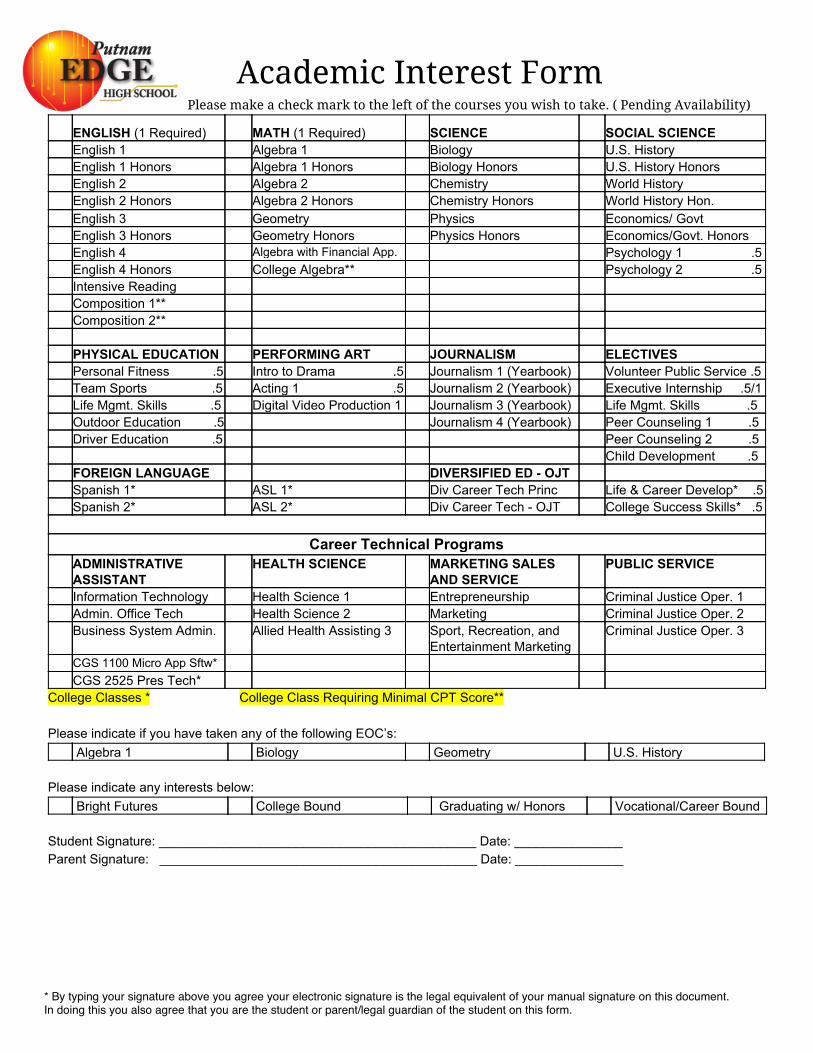
Academic Interest Form
Please make a check mark to the left of the courses you wish to take. ( Pending Availability)
ENGLISH (1 Required) MATH (1 Required) SCIENCE SOCIAL SCIENCE English 1 Algebra 1 Biology U.S. History English 1 Honors Algebra 1 Honors Biology Honors U.S. History Honors English 2 Algebra 2 Chemistry World History English 2 Honors Algebra 2 Honors Chemistry Honors World History Hon. English 3 Geometry Physics Economics/ Govt English 3 Honors Geometry Honors Physics Honors Economics/Govt. Honors English 4 Algebra with Financial App. Psychology 1 .5 English 4 Honors College Algebra** Psychology 2 .5 Intensive Reading Composition 1** Composition 2** PHYSICAL EDUCATION PERFORMING ART JOURNALISM ELECTIVES Personal Fitness .5 Intro to Drama .5 Journalism 1 (Yearbook) Volunteer Public Service .5 Team Sports .5 Acting 1 .5 Journalism 2 (Yearbook) Executive Internship .5/1 Life Mgmt. Skills .5 Digital Video Production 1 Journalism 3 (Yearbook) Life Mgmt. Skills .5 Outdoor Education .5 Journalism 4 (Yearbook) Peer Counseling 1 .5 Driver Education .5 Peer Counseling 2 .5 Child Development .5 FOREIGN LANGUAGE DIVERSIFIED ED OJT Spanish 1* ASL 1* Div Career Tech Princ Life & Career Develop* .5 Spanish 2* ASL 2* Div Career Tech OJT College Success Skills* .5
Career Technical Programs
ADMINISTRATIVE ASSISTANT
HEALTH SCIENCE MARKETING SALES AND SERVICE
PUBLIC SERVICE
Information Technology Health Science 1 Entrepreneurship Criminal Justice Oper. 1 Admin. Office Tech Health Science 2 Marketing Criminal Justice Oper. 2 Business System Admin. Allied Health Assisting 3 Sport, Recreation, and
Entertainment Marketing Criminal Justice Oper. 3
CGS 1100 Micro App Sftw* CGS 2525 Pres Tech* College Classes * College Class Requiring Minimal CPT Score** Please indicate if you have taken any of the following EOC’s: Algebra 1 Biology Geometry U.S. History Please indicate any interests below: Bright Futures College Bound Graduating w/ Honors Vocational/Career Bound Student Signature: ____________________________________________ Date: _______________ Parent Signature: ____________________________________________ Date: _______________
* By typing your signature above you agree your electronic signature is the legal equivalent of your manual signature on this document.In doing this you also agree that you are the student or parent/legal guardian of the student on this form.

LEP # 1 District School Board Of Putnam County
LEP and Occupational Survey
To Be Completed By the Parent, Guardian or Adult With The Student Upon Initial Enrollment
Student Name:________________________________School:_______________________________ Date entered United States School:_______________________ Part I HOME LANGUAGE SURVEY 1. Is a language other than English used in the home? ___Yes___No 2. Did the student above have a first language other than English? ___Yes___No 3. Does the student most frequently speak a language other than English? ___Yes ___No 4. What language is used in the home? _______________________________________________ 5. What is the national origin of the student? ___________________________________________ If you checked Yes to any of the questions on The Home Language Survey Part I, your child will be temporarily placed in the ELL program pending further assessment to determine if he or she meets criteria for entry into the program.
The ELL program services include:
● Teachers have state ELL endorsement training. ● Children will be taught using ELL strategies for effective instruction. ● Parents are invited to special LEP (Limited English Proficient) meetings concerning their child to discuss plans for the child’s academic
education. ● All ELL students participate in the same programs as regular students. ● Students are tested each year and will remain in the ELL program with an IPT score of NES or LES and will exit with a score FES. ● Students’ progress is monitored for two years after exiting the ELL program. ● Children that qualify for ESOL and Exceptional Education will receive both services.
_________________________________ ______________________________________ ____/____/____
Parent’s Signature Interpreter Date
Federal Definition of an Immigrant Student The term "immigrant children and youth," which is defined in section 3301(6) of Title III refers to individuals who: (A) are aged 3 through 21; (B) were not born in any State; and(C) have not been attending one or more schools in any one or more States for more than 3full academic years. Part II
Present occupation (s) of parent(s):_________________________________________________________________ 1. Have you or anyone in your family crossed state or county lines to work or seek work in one of the following occupations, either
full-time or part-time during the last six (6) years? Yes No ___ ___ FARMING (plowing, planting, cultivating, harvesting, or processing of farm crops) ___ ___ DAIRY WORK ___ ___ LIVESTOCK WORK (hoofing, cutting, branding, feeding, or rounding up) ___ ___ PLANTING, GROWING OR HARVESTING OF TREES ___ ___ POULTRY OR EGG WORK ___ ___ COMMERCIAL FISHING (fresh/salt water, crabbing and shrimping) ___ ___ WORKING ON A FISH FARM ___ ___ PROCESSING OR HAULING OF FARM/FISH PRODUCTS 2. If you checked Yes to any of the questions in part II, did your child move with you? ___Yes___No PCDSB Form E-29 Adopted 8-24-92 Revised 11-04-05 Amended 06-06-06
Dear Parent/Guardian: Every school district in Florida is required to report to the Florida Department of Education each year student data by race and ethnicity categories that are set by the federal government. The Department of Education does not report individual student data to the federal government, but does report the total number of students in various categories in each school. These reports help keep track of changes in student enrollment and ensures that all students receive the educational programs and services to which they are entitled. Please answer both questions on this form. All data collected will be entered into our database and reported to the Department of Education. Student Name: _____________________________ Grade Level: _____ 1. Is your child Hispanic or Latino: (Mark only one)
☐ No, my child is not Hispanic or Latino ☐ Yes, my child is Hispanic or Latino A person of Cuban, Mexican, Puerto Rican, South or Central America, or other spanish culture or origin, regardless of race.
2. What is your child’s race? ☐ American Indian or Alaska Native A person having origins in any of the Original peoples of North and South America (including Central America) and who maintains tribal affiliation or community attachment. ☐ Asian A person having origins in any of the original peoples of the far East, Southeast Asia, of the Indian subcontinent, e.g., Cambodia, China, India, Japan, Korea, Malaysia, Pakistan, the Philippine Islands, Thailand, and Vietnam. ☐ Black or African American A person having origins in any of the Black Racial groups of Africa. Terms such as “Haitian” or “Negro” can be used in addition to “Black or African American”. ☐ Native Hawaiian or Other Pacific Islander A person having origins in any of the original peoples of Hawaii, Guam, Samoa, or other Pacific Islands. ☐ White A person having origins in any of the original peoples of Europe, the Middle East, or North Africa.
___________________________________________ ________________ Parent/Guardian Signature Date * By typing your signature above you agree your electronic signature is the legal equivalent of your manual signature on this document.In doing this you also agree that you are the parent/legal guardian of the student on this form.
Chronic Disease Information Form Health Information
Student name: ____________________________________________ Date of Birth: ___________ School Name: ______________________________________________ School Year: ________
This form must be completed annually. The parent or guardian is responsible for keeping the school
informed of any changes in your child’s medical condition. Information will be shared with appropriate
school staff for your child’s best care.
___ My child does not have a medical condition.
List medical conditions your child has now
List all of the medicine(s) your child takes now (home and school)
List any medication(s) to be given at school. A medications authorization form is required.
ADD ____ ADHD ____
A2 ____ Allergy - Insects Epipen ____
A4 ____ Allergy - Medications Name of Medications
Epipen ____
A5 ____ Allergy - Latex Epipen ____
A7 ____ Allergy - Food List the food
Physician order is needed for special diet.
Epipen ____
A9 ____ Allergy - Other Specify Allergy
Epipen ____
AS ____ Asthma How frequent are the episodes?
Inhaler at School ____ Inhaler at Home ____ Nebulizer at School ____ Nebulizer at Home ____
CA ____ Cancer
CP ____ Cerebral Palsy
CYF ____ Cystic Fibrosis
DB ____ Diabetes Hypoglycemia or Hyperglycemia?
Diet ____ Oral Medication ____ Insulin ____ Pump ____ Carb counting ____
EA ____ Ear Problems (describe) Hearing aide ____ (left/right/both FM System ____ Deaf ____ (left/right/both)

Will any medication be taken at school for any of the illnesses listed above? Yes ____ No ____ If yes, Dr. _____________________________ Doctor’s Phone Number: (_____) _____-________
Medication cannot be given at the school until an authorization form is completed. Health Room Staff will contact you to set up a care conference for certain conditions listed above.
Does your child use an adaptive equiptment? Wheelchair ____ Walker ____ Brace ____ Other (Please specify): __________________________________
Please print clearly persons to call in case of emergency Name: ___________________________ Phone: (_____) _____-________ Cell: (_____) _____-________
Name: ___________________________ Phone: (_____) _____-________ Cell: (_____) _____-________
PARENT SIGNATURE: ________________________________________________ DATE ________________
EP ____ Epilepsy/Seizures List known triggers
Last Seizure _______
GA ____ Gastrointestinal ____ Reflux ____ IBS ____ Crohn’s ____ Other
HD ____ Heart Disease HM ____ Heart Murmur
HE ____ Hemophilia
HP ____ Hypertension
KD ____ Kidney Disease
MD ____ Muscular Dystrophy
MG ____ Migraines
NO ____ Nosebleeds Occasional ____ Frequent ____ Medical condition ____
PC ____ Psychiatric Conditions Please list
SC ____ Sickle Cell Anemia Trait Only ____
Last Crisis _______
VP ____ Vision Problems (describe) Glasses ____ Contacts ____ Visually Impaired ____ Blind ____ (left/right/both)
Any Medical Condition not covered above, please list:
* By typing your signature above you agree your electronic signature is the legal equivalent of your manual signature on this document.In doing this you also agree that you are the parent/legal guardian of the child on this form.

ThirtyDay Exemption Notice
Physical Examination Form FloridaLaw authorizes school officials to grant up to a thirty (30) day exemption for any student who is entitled to admittance to Kindergarten or any other initial entrance into any Florida School. I understand that ___________________________ is granted this temporary exemption
(Name of Student) in order to be admitted to class until the Student Physical Examination Form is presented to the school. I also understand that my child will be temporarily excluded from school after thirty (30) days until the Student Physical Examination Form is presented to the school. This exemption will expire in thirty (30) days. ____________ _____________ ___________________________________________ Date Issued Expiration Date Parent/Guardian Signature Immunization Records FloridaLaw authorizes school officials to grant up to a thirty (30) day exemption for any student who is entitled to admittance to Kindergarten or any other initial entrance into any Florida School. I understand that ___________________________ is granted this temporary exemption
(Name of Student) in order to be admitted to class until the his/her Immunization Record can be obtained from the previous school. I also understand that my child will be temporarily excluded from school after thirty (30) days until his/her Immunization Record can be obtained from the previous school. This exemption will expire in thirty (30) days. ____________ _____________ ___________________________________________ Date Issued Expiration Date Parent/Guardian Signature
* By typing your signature above you agree your electronic signature is the legal equivalent of your manual signature on this document.In doing this you also agree that you are the parent/legal guardian of the student on this form.

Technology Policy Putnam EDGE High School
Technology Policy Professional Conduct Guidelines and Acceptable Use Policy regarding technical systems at Putnam EDGE High School Policy Statement Students and staff are expected to maintain a professional approach to all actions performed in the classroom and while using the information systems/network. The following serves as general guidelines and should not be considered allinclusive. It is our expectation that students will make good choices while using the information systems at Putnam EDGE High School. Acceptable Use Policy (AUP)
● Treat school property with respect. ● Provide a protective sleeve and/or backpack or case that will secure/protect the
computer. ● Limit recreational use of workstations and network infrastructure. ● Use the Echo Help Desk database to request help or information. ● Report any system problems or misuse to network management. ● If you are not sure about the acceptability of use, ask the staff. ● Make primary use of workstations and network infrastructure for educational purposes.
Uses NOT allowed without permission, arrangements, or approval from technical managers, instructors, or staff: General Directly contacting equipment, applications, or software vendors with intent to solicit material Inappropriate use of EDGE devices (Including but not limited to cameras, laptops, tablets, etc.) Printing any document or file (without permission) Use of Email, website or network equipment for personal and/or commercial gain Workstation (i.e. EDGE computers, laptops, tablets, etc.) Changing configurations and/or settings (ONLY APPROPRIATE DESKTOPS and Screen Savers are allowed.) Downloading to equipment (i.e. programs or apps, freeware, files, MP3s, etc.) Playing MP3s over the network Playing music CD without headphones Playing unapproved games at any time Storing unauthorized files on local drive (i.e. MP3s, Pictures, documents, etc.) Using any username and/or password other than your account Borrowing Equipment ONLY with permission from administration (While borrowing equipment you must comply with all school policies.) Email/Discussion Accessing or impersonating another user through using their account Inappropriate content and/or profanity (Including but not limited to text, images, and files) Inappropriate or unprofessional signatures or stationery in Email Sending chain messages Sending Emails with malicious intent Sending to groups larger than classroom and/or workgroups

Hacking Intentional introduction, and/or distribution, of any files containing a virus to a system and/or network Infiltration of computer systems and/or security for testing or troubleshooting without network management supervision Possession of destructive or invasive programs Remotely controlling another computer or server Viewing, modifying, or tampering with information and/or files accessed by hacking Hardware Using outside (nonEDGE) equipment (i.e. personal computer, iPad, iPod, cell phones, storage devices) Internet Accessing noneducational sites during class time (e.g. inappropriate, pornographic, gambling, gaming, etc.) Accessing communication websites (e.g. chat rooms, games, messaging services, nonschoolrelated Email) Accessing social networking websites (e.g. Facebook, Tumblr, Twitter, Instagram, Vine, Google+, blogs, etc.) Software Copying software licensed (Including but not limited to software, applications, or freeware) Downloading files (i.e. software, freeware, files, MP3s, etc.) *Putnam EDGE High School reserves the right to revise the Technology Policy. Such revisions and additions shall be communicated and rendered effective immediately upon notice. Consequences of violations: First Offense: Handled and documented by person observing the infraction in Echo. Student will be reminded of the policy regarding network/technology use on campus. Second Offense: Handled and documented by person observing the infraction. Referral to Director with a behavior contract/review of Student Contract. Third Offense: Meeting with student, Director and parent about appropriate behavior and assignment of community service. Fourth Offense: Enforcement of Behavior Contract Improper behavior regarding the technology systems at Putnam EDGE High School may result in restricted and/or limited network access. Restrictions will be given at the discretion of the Director. Severe infractions will be swiftly dealt with independently of the above consequences. PARENT NAME: __________________________________ STUDENT NAME: __________________________________
STUDENT SIGNATURE: _______________________________________________ DATE: _______________________
PARENT SIGNATURE: ________________________________________________ DATE: _______________________
* By typing your signature above you agree your electronic signature is the legal equivalent of your manual signature on this document.In doing this you also agree that you are the parent/legal guardian of the studenton this form.