chemical respiratory allergy - research institute for fragrance
TRANSCRIPT
a RIFM Workshop July 13-14, 2006
Langham Hotel London
TM
Chemical Respiratory
Allergy:definition, clinical observations,
and safety assessment

Results anticipated include:Reaching agreement on defining chemical respiratory allergens and chemical respiratory allergy. Answering the question, “Do contact allergens have the potential to elicit respiratory sensitization?”Identifying appropriate models to assess the potential for chemicals to induce respiratory sensitization. How a mechanistic understanding of chemical respiratory allergy can be incorporated into models for hazard and risk assessment.
AGENDADAY 1, Thursday, 13 JULY 06
8:00 – 9:00 am Registration and Continental Breakfast
Welcome & Introduction9:00 am RIFM Staff & Glenn Sipes
Clinical Aspects9:00 – 9:20 am Dr. Mark Utell, Prof. of Medicine and Environmental Medicine, University of Rochester School of
Medicine, USA. The Physiology And Pathology Of Respiratory Sensitization And Airway Inflammation: Immunological Versus Irritant Responses
9:20 – 9:40 am Dr. Paul Cullinan, Reader in Occupational and Environmental Medicine, Department of Occupational and Environmental Medicine, Imperial College (National Heart & Lung Institute), London and Honorary Consultant, Respiratory Medicine, Royal Brompton Hospital, London, UK Clinical Aspects Of Chemical Respiratory Allergy.
9:40 – 10:00 am Dr. David Bernstein, Professor of Clinical Medicine, University of Cincinnati, Division of Immunology/Allergy, Department of Medicine, USA Immunological Evaluation Of Chemical Respiratory Allergy
Research: 10:00 – 10:20 am Dr. Christina Herrick, Assistant Professor, Department of Dermatology, Yale University School of
Medicine, New Haven, USA. Animal Models Of Asthma: Comparison Of Skin Vs. Airway Routes Of Sensitization That Can Lead To Asthma-like Inflammation
10:20 – 10:40 am Dr. Frieke Kuper, Board-Certified Toxicological Pathologist, Department of Toxicology and Applied Pharmacology, TNO Quality of Life, NL Thelper1-mediated Allergic Reactions In The Respiratory Tract: Relevance For Hazard Identification Of Low Molecular Weight (Lmw) Allergens
10:40 - 11:00 am - Refreshment Break11:00 – 11:20 am Professor Ian Kimber BSc, MSc, PhD, Syngenta Principal Fellow, Company Health Assessment
Facility in Alderley Park, UK Relationships Between Skin and Respiratory Chemical Allergens
11:20 – 11:40 am Dr. Meryl Karol, Professor of Environmental and Occupational Health, and Civil and Environmental Engineering at the University of Pittsburgh, Associate Dean for Academic Affairs, USA Structure-activity Relationships And Models Of Chemicals Causing Respiratory Sensitization
Methodology:11:40 am – 12:00 pm Dr. Rebecca Dearman, Head of Immunology Research, Syngenta Central Toxicology Laboratory,
UK The Identification Of Chemical Respiratory Allergens: The Ctl Approach
••••
Tab 1
Tab 2
Tab 3
Tab 4
Tab 5
Tab 6
Tab 7
Tab 8
12:00 – 12:20 pm Dr. Josje Arts, Product Manager Inhalation Toxicology, Department of Toxicology and Applied Pharmacology, TNO Quality of Life, NL The Identification Of Chemical Respiratory Allergens: The Tno Approach
12:20 – 1:40 pm - BUFFET LUNCHMethodology (continued):1:40 – 2:00 pm Dr. Rob Vandebriel, Laboratory for Toxicology, Pathology & Genetics, National Institute for Public
Health & the Environment, (RIVM), NL The Identification Of Chemical Respiratory Allergens: The Rivm Approach
2:00 – 2:20 pm Dr. Kathy Sarlo, Principal Scientist, Central Product Safety, The Procter & Gamble Company, USA Evaluation Of Chemical Respiratory Allergy: An Industry View
Risk Assessment: 2:20 – 2:40 pm Dr. David Basketter, BSc, DSc, FIBiol, FRCPath, Eurotox Registered Toxicologist, Senior Scientist,
Safety and Environmental Assurance Centre, Unilever and Senior Lecturer, Dept of Dermatology, Guy’s, Kings and St Thomas Hospital School of Medicine, London, UK Hazard Identification, Characterisation And The Assessment Of Respiratory Sensitisation Risk For Consumer Products.
2:40 – 3:00 pm Dr. Marcel van Raaij, Centre for Substances and Integrated Risk Assessment, National Institute for Public Health and the Environment, (RIVM), NL Risk Assessment Aspects Of Respiratory Sensitization
3:00 - 3:20 pm - Refreshment Break:
Regulatory Perspective:3:20 – 3:40 pm Dr. Helen McGarry, Regulatory Scientist, Health and Safety Executive
Chemical Respiratory Hypersensitivity: UK Regulatory Perspectives
Summary and Conclusions:3:40 – 4:00 pm Dr. I. Glenn Sipes, Ph.D., Professor and Head Dept. of Pharmacology, College of Medicine,
University of Arizona, USA
General Questions & Answers, Closing:4:00 – 4:30 pm Presenters and Attendees
5:30 – 7:00 pm Meet the Presenters Reception (Hors d’oeuvres & open bar)
DAY 2, Friday, 14 JULY 06 Introduction:9:00 – 9:20 am Glenn Sipes
Review Of Previous Presentations And Goals For The Discussion, I.e. Definition Of A Chemical Respiratory Allergen, Role Of Ige And Cytokines, Other Mechanisms, Appropriate Models, Work That Needs To Be Done, Consensus.
Discussion:9:20 – 11:30 am Presenters and Attendees
Audience participation will be strongly encouraged.Summary & Closing:11:30 am – 12:00 pm Glenn Sipes & RIFM Staff
What outcomes were reached? What are the next steps?
12:00 – 1:30 pm - BUFFET LUNCH:
Tab 9
Tab 10
Tab 11
Tab 12
Tab 13
Tab 14
Tab 15

CHEMICAL CHEMICAL RESPIRATORY RESPIRATORY
ALLERGYALLERGYDefinition, Clinical Observations, Definition, Clinical Observations,
Safety AssessmentSafety Assessment
1313--14 July 200614 July 2006
London, EnglandLondon, England
Daniel IsolaDaniel IsolaProgram Manager, Respiratory ProgramProgram Manager, Respiratory Program
Research Institute for Fragrance Materials, Inc.Research Institute for Fragrance Materials, Inc.Woodcliff Lake, NJ USAWoodcliff Lake, NJ USA
[email protected]@rifm.org
DAI: WRKSHP CRA - 13 14 JUL 06 London 3
The Research Institute for The Research Institute for Fragrance Materials, Inc. (RIFM)Fragrance Materials, Inc. (RIFM)
Respiratory ProgramRespiratory ProgramConcerns regarding asthma and allergyConcerns regarding asthma and allergyStrategyStrategy●● QuantitateQuantitate human exposureshuman exposures●● Assess safety in useAssess safety in use
The International Scientific Authority for The International Scientific Authority for the Safe Use of Fragrance Materialsthe Safe Use of Fragrance Materials
DAI: WRKSHP CRA - 13 14 JUL 06 London 4
ANTICIPATED OUTCOMESANTICIPATED OUTCOMES
A better understanding of respiratory A better understanding of respiratory allergy, respiratory allergens, and the allergy, respiratory allergens, and the mechanisms involvedmechanisms involvedCommon grounds upon which to Common grounds upon which to build consensusbuild consensusIdentification of Identification of ““next stepsnext steps””regarding a valid animal model for regarding a valid animal model for respiratory sensitizationrespiratory sensitizationA sense of how to approach hazard A sense of how to approach hazard and risk assessmentand risk assessment
DAI: WRKSHP CRA - 13 14 JUL 06 London 5
ANTICIPATED OUTCOMESANTICIPATED OUTCOMES
A better understanding of respiratory allergy, A better understanding of respiratory allergy, respiratory allergens, and the mechanisms involvedrespiratory allergens, and the mechanisms involved●● RADS, EAARADS, EAA●● Th1, Th2 mediated, Th1, Th2 mediated, IgIg mediatedmediated●● Allergy: Allergy: ‘‘Allergy is a hypersensitivity reaction initiated Allergy is a hypersensitivity reaction initiated
by immunologic mechanismsby immunologic mechanisms’’ (according to EAACI, (according to EAACI, Johansson Johansson et alet al., 2001). ., 2001).
●● Respiratory allergy is a hypersensitivityRespiratory allergy is a hypersensitivity11 reaction in the reaction in the respiratory tract upon inhalation exposurerespiratory tract upon inhalation exposure22 with an with an antigen/allergen, which is initiatedantigen/allergen, which is initiated33 by immunologic by immunologic mechanisms induced by that specific antigen. mechanisms induced by that specific antigen.
11 (in toxicology terms: adverse, immune(in toxicology terms: adverse, immune--mediated)mediated)22 (challenge, local)(challenge, local)33 (sensitization; systemic, any route)(sensitization; systemic, any route)
●● Respiratory tract: including nasal and associated Respiratory tract: including nasal and associated structures, airways and lung parenchyma.structures, airways and lung parenchyma.
DAI: WRKSHP CRA - 13 14 JUL 06 London 6
ANTICIPATED OUTCOMESANTICIPATED OUTCOMES
A better understanding of respiratory allergy, A better understanding of respiratory allergy, respiratory allergens, and the mechanisms involved respiratory allergens, and the mechanisms involved (continued)(continued)●● Clinical picture Clinical picture -- symptomlesssymptomless changeschanges●● Consistent with immune mechanismsConsistent with immune mechanisms●● The The ““archtypearchtype””●● Occupational asthma Occupational asthma …… variable airflow limitation and/or variable airflow limitation and/or
hyperresponsivenesshyperresponsiveness and/or inflammation due to causes and/or inflammation due to causes and conditions attributable to and conditions attributable to ……. the workplace.. the workplace.””
●● A chronic lung disease characterized by:A chronic lung disease characterized by:Airway inflammation where many cells and cellular elements Airway inflammation where many cells and cellular elements play a roleplay a roleAirway obstruction (or narrowing) Airway obstruction (or narrowing) --Usually reversible, Usually reversible, either spontaneously or with treatment either spontaneously or with treatment Airway Airway hyperresponsivenesshyperresponsiveness to a variety of stimulito a variety of stimuliDifferent areas of the lungDifferent areas of the lung
DAI: WRKSHP CRA - 13 14 JUL 06 London 7
DISCUSSION TOPICSDISCUSSION TOPICS
Animal models (validation!)Animal models (validation!)●● Identify Identify ““potentialpotential”” respiratory respiratory
allergensallergens●● Cellular Cellular vsvs physiological changesphysiological changes●● Th1, Th2 biasTh1, Th2 bias●● Dermal, inhalationDermal, inhalation●● AsthmaAsthma●● LLNA + cytokine profilingLLNA + cytokine profiling
Pulmonary lymph nodesPulmonary lymph nodesInhalation challenge, Con. A Inhalation challenge, Con. A restimualtionrestimualtion
DAI: WRKSHP CRA - 13 14 JUL 06 London 8
DISCUSSION TOPICSDISCUSSION TOPICS
What is necessary informationWhat is necessary informationRoutes of exposureRoutes of exposureNegative controlsNegative controls●● Sensitivity & specificitySensitivity & specificityMechanisms of actions Mechanisms of actions –– necessary for necessary for appropriate risk/hazard assessmentappropriate risk/hazard assessment●● IgEIgE mediatedmediated●● Th1, Th2 mediatedTh1, Th2 mediated●● OtherOther
DAI: WRKSHP CRA - 13 14 JUL 06 London 9
ANTICIPATED OUTCOMESANTICIPATED OUTCOMES
Common grounds upon which to Common grounds upon which to build consensusbuild consensus
Identification of Identification of ““next stepsnext steps””regarding a valid animal model for regarding a valid animal model for respiratory sensitizationrespiratory sensitization
A sense of how to approach hazard A sense of how to approach hazard and risk assessmentand risk assessment
Mark J. Utell, MD
Bio
Dr. Mark J. Utell is Professor of Medicine and Environmental Medicine and Director of the Pulmonary/Critical Care and Occupational/Environmental Medicine Divisions at the University of Rochester Medical Center. He is also Associate Chairman of the Department of Environmental Medicine. Dr. Utell's research and teaching interests have focused primarily on the effects of inhaled particles, fibers and vapors on the respiratory system. Most recently, his laboratory has focused on clinical responses to ultrafine particles and mechanisms of response. His current research funding sources include the Environmental Protection Agency (Co-Director of a PM Center on ultrafine particles); the National Institutes of Health (NIEHS); New York State Energy Research and Development Authority (NYSERDA); and the Electric Power Research Institute (EPRI). Dr. Utell received his BA degree from Dartmouth College and his MD from Tufts University School of Medicine in 1972. Upon completion of a fellowship in Pulmonary Medicine, he joined the faculty at the University of Rochester in 1977. Dr. Utell has served as the Chairman of Workshops sponsored by the EPA, the American Petroleum Institute, the Health Effects Institute and the American Thoracic Society and had significant experience in developing national meetings. He has served on a number of national committees and review panels for federal, public and private agencies. Dr. Utell currently serves as Chair, Health Effects Institute’s Research Committee and has served as Chair of EPA’s Environmental Health Committee and on the Executive Committee of the EPA Science Advisory Board. Dr. Utell has been a member of the National Research Council’s (NRC) Committee on Research Priorities for Airborne Particulate Matter, and the Institute of Medicine's (IOM) Committee to Review the Health Consequences of Service during the Persian Gulf War. He is currently a member of the NRC Board on Environmental Studies and Toxicology (BEST) and IOM, Committee on Biodefense Analysis and Counter-measures. Dr. Utell is a former recipient of the NIEHS Academic Award in Environmental and Occupational Medicine. He is on the editorial boards of the Journal of Aerosol Medicine and Environmental Bioindicators having previously served on the editorial boards of Environmental Health Perspectives and the Annals of Internal Medicine. He has published extensively on the health effects of inhaled gases, particles and fibers in the workplace and environment and has over 100 publications as well as numerous presentations at professional meetings around the world.

RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006 The Physiology and Pathology of Respiratory Sensitization and Airway Inflammation: Immunological versus Irritant Responses Mark J. Utell, MD University of Rochester Medical Center, Rochester, NY USA
Each day we breathe 10.000 to 20, 000 liters, or approximately 35 lbs of air. Therefore, the
respiratory tract has an inevitable exposure to myriad gaseous and particulate toxicants contained
within this ambient air. Despite the chronicity of exposure, the respiratory defenses are generally
adequate to protect against significant injury. On occasion, acute or chronic inhalation of low-
level pollutants may cause airway inflammation, providing insights into mechanisms of lung
responses. In relating respiratory responses to specific exposures, it is recognized that penetration
of toxic gases and their retention can vary, depending on the physical properties of the gas (eg,
solubility), the concentration of the gas in the inspired air, the rate and depth of ventilation, and
the extent to which the material is reactive. Gases that are highly soluble are almost completely
extracted by the nose or upper airway, while removal of less water soluble gases (eg, ozone), is
much less complete, and these gases, therefore, penetrate deeper into the respiratory tract.
Similarly, the deposition of inhaled particles also depends on multiple factors, including the
aerodynamic properties of the particle (primarily its size), airway anatomy and breathing pattern.
Even the deposition of nanoparticles in the range of 1-50 nm differs greatly throughout the
respiratory tract.
A number of health outcomes have been associated with exposures to chemicals including
irritation, inflammation, bronchoconstriction and sensitization. Respiratory tract sensitizers range
from large molecular weight proteins of animal, plant and fungal origin to low molecular weight
organic and inorganic chemicals. The induced responses depend on genetic and other host-
specific factors, immunologic status of the host, agent-related factors such as the nature of the
pollutant, concentration and the length of exposure. Respiratory allergy results when airborne
allergens penetrate host defenses induce an immune response with T-lymphocytes and typically
elicit IgE antibodies (although not always). The IgE antibodies link to mast cells and, when
cross-linked, the mast cells release inflammatory mediators which cause bronchoconstriction.
Additional inflammatory cells are recruited, including eosinophils, which are responsible for

epithelial damage and increased airway reactivity. The demonstration of sensitization in an
individual case requires a clinical evaluation relating disease exacerbation to a specific exposure
and a positive skin or RAST test is often confirmatory. A significant health consequence of
respiratory sensitization is asthma, a disease characterized by inflammation, reversible airway
obstruction and increased airway responsiveness to various stimuli. Alternatively, an exposure
may result in non-immunologic or irritant-induced airway hyper-responsiveness. The term
reactive airways dysfunction syndrome (RADS) refers to onset of symptoms after a single
exposure to a high level of an irritant gas or fume in an individual without preceding respiratory
disease; however, a similar non-immunologic syndrome consistent with asthma, with symptoms
of cough, wheezing or dyspnea has occurred with more chronic low level exposure to irritants or
chemicals. Both immunological and irritant related airways disease are characterized by
nonspecific bronchial hyperresponsiveness assessed by methacholine or bronchodilators. Others
markers such as exhaled NO, exhaled breath pH, and cell counts and activation markers in
induced sputum, have been proposed as end-points for detecting and even distinguishing
immunologic from non-immunologic airway inflammation. Although bronchoscopy occasionally
provides cell counts, cytokines and other inflammatory markers from exposed individuals,
pathology is rarely available. In contrast to allergic airway inflammation, bronchial biopsies
from non-immunologic airways disease usually show only a mild inflammatory response, with
sparse lymphocytes and polymorpho-nuclear cells, and no eosinophils.
Distinguishing immunological responses from irritant responses can be difficult. In fact, recent
work with diesel exhaust particles provides an interesting example of an ambient exposure with
potential for causing both irritant. Nasal instillation of diesel particles plus ragweed versus
ragweed alone has been shown to result in increased IgE levels compared to the control;
furthermore, evidence of IgE switching has been demonstrated following instillation of diesel
particles alone. Inhalation of diesel particles has resulted in changes in lung function, airway
inflammation and increased cytokine levels—evidence of an irritant response. Studies are
underway to determine if inhalation of diesel particles can also cause increases in IgE levels as
seen with nasal instillation. Diesel exhaust could turn out to be a model chemical for studying
irritant and immunological airway responses.
Dr. Paul Cullinan
Bio Dr. Paul Cullinan is a pulmonologist and a Reader in Occupational and Environmental Medicine at Imperial College National Heart and Lung Institute and an Honorary Consultant Physician in Respiratory Medicine at Royal Brompton Hospital. The Royal Brompton's clinical service for the investigation of patients with suspected occupational lung disease is the largest of its kind in Europe. Both institutions are located in London. Dr. Cullinan earned his medical degree at the University of London. His academic and clinical interests are in occupational and environmental respiratory disease with an emphasis on occupational asthma, the epidemiology of occupational lung disease and other determinants of lung disease.
RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
ABSTRACT Clinical Aspects of Chemical Respiratory Allergy. Paul Cullinan ‘Allergy’ currently has a very high public profile, but the term is much misused. Strictly and originally it refers to the uncommitted immune response to an external (‘antigenic’) stimulus; if the response develops into a beneficial one then we speak of ‘immunity’; if it becomes harmful then we may talk of an ‘allergic disease’. Frequently however the term ‘allergy’ is used alone to describe an exaggerated immune response which may be associated with clinical (‘allergic’) disease. In lay language ‘allergy’ is often used to label a very wide variety of undesired responses to the outside world; this is unhelpful since it often leads to advice about avoidance and treatment that is at best useless and at worst severely handicapping. Respiratory allergic diseases are characterised by the clinical manifestations of local ‘allergic’ inflammation; this primarily is at the site of encounter between the antigen and the human host—the nose and the upper airways—although more widespread responses occur sometimes. Thus mucosal swelling and hyperirritability of the respiratory passages give rise to:
• nasal blockage and discharge • sneezing • cough with the production of generally clear sputum • airway narrowing with a sensation of tightness in the chest accompanied by wheeze and shortness
of breath. Some of these symptoms are not specific to respiratory allergy. In general however clinical allergic responses bear a close temporal relationship to antigen exposure. Thus allergic responses to grass pollens are largely confined to the flowering seasons of antigenic species and occupational allergies to relevant work-times. Where the antigen is ubiquitous—for example house dust mite antigens in Western Europe—then so may be the clinical manifestations of allergy. When an allergic response is sustained by frequent antigen exposure a state of ‘non-specific’ hyperresponsiveness may develop whereby symptoms are related also to non-antigenic, ‘irritant’ exposures. These are a common cause of misunderstanding. Four other features of an allergic response are relevant:
• they are, to some extent, governed by individual susceptibility although the details of this are poorly understood. The result is that allergic responses tend to be confined to a proportion only of the exposed population; the size of this proportion reflects also the intensity of antigenic stimulation. Thus not everybody develops hayfever; and not all workers exposed to a respiratory antigen develop occupational disease.
• an ‘immunological’ allergic response is more common than a clinical one. Thus at any time a proportion of any exposed population may have a ‘silent’ condition that is detectable only by immunological testing. Individuals with this condition can, under the right conditions of exposure, move to a more clinically apparent response.
• as with any immunogical response, a period of time, during which there are repeated antigen exposures, is required for the development of a clinical allergic response. Thus allergies do not become manifest on the first exposure to an antigen.

• once ‘fully’ developed and sustained a clinical allergy is a hyperimmune state. Thus clinical
erhaps the most important manifestation of respiratory allergy is asthma—another much abused term. A
his presentation offers a clinical description of classical respiratory allergy with particular reference to
responses tend to occur after increasingly small quantities of exposure to the causative antigen.
Pdefinition of ‘asthma’ is rather more difficult than a description. In its strictest sense the label refers to a state of non-infective bronchial inflammation that produces symptoms such as wheeze, cough and breathlessness accompanied by measurable and variable limitation to airflow. Frequently but not invariably these are associated with a state of bronchial hyperresponsiveness. Looser and less specific classifications often include any state where the above symptoms are reported; sometimes the label is qualified by reference to these as ‘asthma-like symptoms’. Unsurprisingly, the ascertainment of asthma in individuals (as patients) tends to be more specific than that used in large populations. Tthat which arises in the workplace from exposure to non-biological (‘chemical’) antigens. This state is compared with that reported from more widespread exposures to chemical agents. The certain implications of the former and the probable implications of the latter are discussed.
David I. Bernstein, MD
BIO
David I. Bernstein, MD is Professor of Clinical Medicine in the University of Cincinnati, Division of Immunology/Allergy in the Department of Medicine. Dr. Bernstein is director of the University of Cincinnati Allergy Laboratory and Co-director of the University of Cincinnati training program in Allergy-Immunology. He is board certified in Internal Medicine, Allergy-Immunology and Diagnostic Laboratory Immunology. His major research interests pertain to novel treatments for asthma, environmental causes of allergy and occupational lung diseases, specifically occupational asthma. Dr. Bernstein is currently conducting research in human genetics of Occupational Asthma caused by low molecular weight chemicals as well as a large birth cohort study examining environmental influences on development of childhood allergic disorders.
Dr. Bernstein is a graduate of the University of Cincinnati College of Medicine. He completed training in Internal Medicine at the Cleveland Clinic and served as an Allergy-Immunology fellow in training at Northwestern University (1980-82).
Dr. Bernstein has been active in many CME activities as a speaker at national meetings and served as the Chairperson of the Environmental and Occupational Disorder Interest Section and Immunotherapy Committee of the American Academy of Allergy, Asthma and Immunology.
He is co-editor of the authoritative text on Occupational Asthma, Asthma in the Workplace, now in its 3rd edition. Dr. Bernstein has authored or co-authored over 90 articles in peer-reviewed journals as well numerous reviews and book chapters.

RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006 Immunological Evaluation of Chemical Respiratory Allergy David I. Bernstein MD, U of Cincinnati, Division of Immunology-Allergy Occupational asthma has been defined as a condition of variable airflow limitation and/or hyperresponsiveness and/or inflammation due to causes and conditions attributable to the workplace. Two forms are included, those cases associated with a latency period of exposure involving IgE mediated sensitization and occupational asthma without a latency period, also referred to as irritant induced asthma. Both chemicals and proteins encountered in the workplace can act as respiratory sensitizers. However, reliable demonstration of immunologic sensitization to chemicals is often challenging and problematic. Much attention in this area has focused on in vitro serologic methods aimed at measuring specific IgE antibodies. However, development of clinically useful assay methods has been hindered by lack of standardization antigens and immunoassays. Most, if not all studies, have been performed with antigens prepared by conjugating chemicals with human serum albumin. For the majority of chemicals that cause OA, skin prick testing is not indicated with the exception of a few agents that are known to induce IgE mediated sensitization; these include acid anhydride compounds (e.g., trimellitic anhydride, phthalic anhydride), sulfonechloramide, persulfates, vinyl sulfone reactive dyes, and platinum salts. Because protocols for assays and conjugate preparation have not been standardized, results obtained in different laboratories are not comparable. Specific inhalation testing with chemical sensitizers is considered the gold standard for validating skin prick tests and serologic tests for chemical sensitizers. In this discussion, we will examine studies that have attempted to validate specific IgE and cellular assays for detecting clinical sensitization among worker exposed to diisocyanates, acid anhydrides and sulfone dyes. Methodologic variables that can affect test performance will be considered including conjugate preparation and characterization and well as assay methodology.
DR. CHRISTINA A. HERRICK
BIO
Dr. Christing A. Herrick is an Assistant Professor in the Department of Dermatology at the Yale University School of Medicine in New Haven, CT and an Attending Physician at Yale New Haven Hospital. She is a Board Certified Dermatologist. Dr. Herrick received her B.A. in 1986 from Rutgers College in New Brunswick, NJ. Her M.D., Ph.D. was conferred 1993 by the Department of Pathology, State University of New York – Downstate Medical Center, Brooklyn, NY. Her Doctoral Dissertation was titled "Regulation of Anamnestic IgE Responses." She was a Postdoctoral Fellow from 1997 to 1999 in the Departments of Dermatology and Immunobiology at Yale University School of Medicine in New Haven, CT and the Laboratories of Kim Bottomly, Ph.D., and Robert Tigelaar, M.D. During her postgraduate work she was awarded the Women’s Dermatologic Society Mentorship Award in 1997 for study of the treatment of atopic dermatitis patients with Dr. Jon Hanifin at The Oregon Health Sciences University, Portland, OR) Dr. Herrick’s professional associations include the American Academy of Dermatology, the Society for Investigative Dermatology, the Dermatology Foundation, and the Women’s Dermatologic Society among others. She also serves as a Medical Editor for Dermatology Focus (a publication of The Dermatology Foundation), and as a Member of the Scientific Advisory Board for a Novartis Study CASM981CUS09. Dr. Herrick reviews manuscripts for Immunology ,The Journal of Allergy and Clinical Immunology, The Journal of Clinical Investigation , The Journal of Experimental Medicine, The Journal of Immunology, The Journal of Investigative Dermatology among others and is a popular speaker and lecturer on immunology. She has been the recipient of 13 grants and fellowships and has authored more than 45 publications, book chapters and presentations.

RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
ABSTRACT
Animal Models of Asthma: Comparison of Skin versus Airway Routes of Sensitization that Can Lead to Asthma-Like Inflammation Christina Herrick, MD, PhD, Department of Dermatology Yale School of Medicine, New Haven, CT USA
Chronic inflammation of the airways is a feature common to all types of asthma and is thought to play a fundamental role in the clinical expression of disease. Specifically, Th2 type immune responses have been implicated in most forms of asthma. Despite this, it remains unclear why these Th2 responses develop in some individuals following exposure to certain environmental antigens, while the majority of exposed individuals remain disease-free. For this reason, we have aimed to establish mouse models of asthma that involve initial generation of Th2 responses at anatomic sites where allergens are normally encountered, namely the airway and skin. In models of atopic asthma, we have established sensitization protocols involving initial exposure of mice to the soluble protein ovalbumin (OVA), in the absence of adjuvant, either by inhalation or epicutaneously under an occlusive skin patch. Exposure of mice to OVA by either route induces strong Th2 responses, with high levels of IgE and IgG1 in serum. In addition, subsequent airway challenge of mice sensitized by either route leads to lung responses with characteristics of Th2 recruitment, including high numbers of eosinophils, mucus hypersecretion, and production of Th2 cytokines (IL-4, IL-5 and IL-13). We have also developed a mouse model of diisocyanate asthma which involves initial sensitization of mice to hexamethylene diisocyanate (HDI) through the skin. Subsequent inhaled antigen challenge of these mice results in lung inflammatory responses with characteristics of human disease, including eosinophilia and mucus hypersecretion. Interestingly, however, the response generated by epicutaneous exposure to HDI has characteristics of a mixed Th1/Th2 type response, with both Th1 (IgG2a) and Th2 (IgG1 and IgE) associated antibody isotypes in serum. In addition, both Th1 associated IFN-γ and Th2 type cytokines (IL-4, -5, and -13) are produced by lung inflammatory cells. Despite Th1 activation, however, the lung inflammation in HDI-sensitized mice was not dependent on IFN-γ, but appeared to be mediated primarily by Th2 cells. In summary, the data from the animal models described above suggest that both the skin and airway represent potentially important sites for generation of systemic Th2 type immune responses capable of mediating airway inflammatory responses upon subsequent inhaled antigen exposure.

RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
SUMMARY Animal Models of Asthma: Comparison of Skin versus Airway Routes of Sensitization that Can Lead to Asthma-Like Inflammation Christina Herrick, MD, PhD, Department of Dermatology Yale School of Medicine, New Haven, CT USA Asthma is a clinical syndrome characterized by reversible airway obstruction, bronchial
hyperresponsiveness and airway inflammation. Although distinct variants of asthma, such as atopic
versus non-atopic, may differ with regard to their etiology, chronic inflammation of the airways is a
feature common to all types of asthma and is thought to play a fundamental role in the clinical
expression of disease. It is clear that exuberant CD4 Th2 cell activation, a cardinal feature of all atopic
disease, including allergic rhinitis and atopic dermatitis, is also a driving force behind the
characteristic lung inflammatory response seen in allergic asthma (1). Similarly, Th2 type immune
responses have been implicated in other forms of asthma, such as the occupation-related asthma that
results from exposure to diisocyanates, a group of highly reactive, low molecular weight compounds
used in the manufacture of polyurethanes (2-4). However, despite the evidence that Th2 responses are
involved in many different forms of asthma, it remains unclear as to why these Th2 responses develop
in some individuals following exposure to certain environmental antigens, while the majority of
exposed individuals remain disease-free.
With the expanded use of polyurethane paints, foams and other products, diisocyanates have become
one of the most commonly identified causes of occupational asthma in industrialized countries (5,6).
Prevention can be difficult, in part because the exposure characteristics associated with risk of
developing asthma remain unclear. For instance, recent attention has been drawn to the possibility that
skin exposure, in addition to airway exposure, may contribute to sensitization of workers (4,7).
Similarly, the question of whether the skin may serve as an initial site for sensitization to aeroallergens
in atopic individuals has been raised, with the defective skin barrier and inflammation present in
children with atopic dermatitis contributing to development of systemic Th2 responses and upper
airway disease later in life.

The obvious limitations of the types of studies that can be performed with human subjects emphasize
the importance of relevant animal models for understanding the immunopathogenesis of the various
types of human asthma. For this reason, we have aimed to establish mouse models of asthma that
involve initial generation of Th2 responses at anatomic sites where environmental allergens are
normally encountered, namely the airway and skin. In models of atopic asthma, we have established
sensitization protocols involving initial exposure of mice to the soluble protein ovalbumin (OVA), in
the absence of adjuvant, either by inhalation or epicutaneously under an occlusive skin patch (8). In
our models, initial exposure of mice to OVA by either route induced strong Th2 responses. This was
demonstrated by a characteristic Th2-type antibody isotype profile in serum, with high levels of IgE
and IgG1, and little IgG2a. In addition, subsequent airway challenge of mice sensitized by either route
led to lung responses with characteristics of Th2 recruitment, including inflammatory infiltrates with
high numbers of eosinophils, mucus hypersecretion, and production of Th2 cytokines (IL-4, IL-5 and
IL-13) by lung inflammatory cells. Subsequent studies aimed at addressing the role of IL-4 in these
responses, however, revealed interesting differences between these two sites of sensitization. While
induction of Th2 inflammatory responses by primary exposure to inhaled antigen was significantly
impaired in IL-4 deficient mice, Th2 responses equivalent to those seen in wildtype mice were still
generated following epicutaneous antigen exposure in the absence of IL-4. Thus, there is an interesting
dichotomy in the IL-4 dependence of Th2 responses generated by exposure of two different anatomic
sites to soluble protein antigen. Taken together, the data implicate the skin of atopics as a potentially
important site of initial Th2 sensitization to environmental allergens, perhaps even more readily
allowing sensitization than through the airway.
While numerous studies have been performed in mouse models of atopic asthma, utilizing
sensitization to soluble protein antigens as described above, relatively few investigations of asthma
resulting from sensitization to a hapten, such as a diisocyanate, have been performed in mice. We have
developed a mouse model of diisocyanate asthma which, in contrast to previously reported models,
demonstrates antigen-specific lung inflammatory responses with characteristics of human disease,
including eosinophilia and mucus hypersecretion (9,10). Features of this model include induction of
both contact hypersensitivity and antigen-specific antibody responses following epicutaneous
sensitization with hexamethylene diisocyanate (HDI). Most importantly, however, challenge of
sensitized, but not unsensitized, mice with inhaled HDI results in the recruitment of high numbers of
eosinophils into the airway and mucus hypersecretion. Interestingly, the response generated by
epicutaneous exposure to HDI had characteristics of a mixed Th1/Th2 type response, with production
of both the Th1 associated cytokine IFN-γ and Th2 type cytokines (IL-4, -5, and -13) by lung
inflammatory cells. Similarly, both Th1 (IgG2a) and Th2 (IgG1 and IgE) associated antibody isotypes
were present in serum. This is in contrast to our mouse model of atopic asthma involving epicutaneous
sensitization to OVA, which results in a strongly biased Th2 immune response (8). Despite Th1
activation, however, the lung inflammation in HDI-sensitized mice was not dependent on IFN-γ. Thus,
despite a mixed response generated to HDI, airway eosinophilia induced by inhaled antigen exposure
appeared to be mediated primarily by Th2 cells, similar to that seen following epicutaneous protein
exposure.
In summary, the data from the animal models described above suggest that both the skin and
airway represent potentially important sites for generation of systemic Th2 type immune responses
capable of mediating airway inflammatory responses upon subsequent inhaled antigen exposure. This
supports the notion that asthmatic individuals may initially become sensitized to environmental
allergens via either skin or airway exposure.
References 1. Herrick, CA and K Bottomly. To respond or not to respond: T cells in allergic asthma. Nature
Reviews Immunology 2003;3:405.
2. Maestrelli P, Occari P, Turato G, et al. Expression of interleukin (IL)-4 and IL-5 proteins in asthma induced by toluene diisocyanate (TDI). Clinical & Experimental Allergy 1997;27(11):1292.
3. Baur X, Dewair M, Fruhmann G. Detection of immunologically sensitized isocyanate workers by RAST and intracutaneous skin tests. J. Allergy Clin. Immunol. 1984;73:610.
4. Petsonk EL, Wang ML, Lewis DM, Siegel PD, Husberg BJ. Asthma-like symptoms in wood product plant workers exposed to methylene diphenyl diisocyanate. Chest 2000;118(4):1183.
5. Chan-Yeung M, Malo JL. Occupational asthma. N Engl J Med 1995;333(2):107-12.
6. Bernstein JA. Overview of diisocyanate occupational asthma. Toxicology 1996;111(103):181.
7. Redlich CA, Stowe MH, Wisnewski AV, Eisen EA, Karol MH, Lemus R, et al. Subclinical immunologic and physiologic responses in hexamethylene diisocyanate-exposed auto body shop workers. Am J Ind Med 2001; 39:587.
8. Herrick, CA, H MacLeod, E Glusac, RE Tigelaar and K Bottomly. Th2 Responses Induced by Epicutaneous versus Inhalational Protein Exposure are Differentially Dependent on IL-4. J Clin Invest 2000;105:765.
9. Herrick, CA, L Xu, AV Wisnewski, J Das, CA Redlich, and K Bottomly. A novel mouse model of diisocyanate-induced asthma showing allergic-type inflammation in the lung after inhaled antigen challenge. J Allergy Clin Immunol 2002;109:873.
10. Herrick, CA, J Das, L Xu, AV Wisnewski, CA Redlich, and K Bottomly. Differential roles for CD4 and CD8 T cells following diisocyanate sensitization: Genetic control of Th2-induced lung inflammation. J Allergy Clin Immunol 2003;111:1087.
Dr. Frieke Kuper
BIO Dr. Frieke Kuper is a board-certified toxicological pathologist in the Department of Toxicology and Applied Pharmacology at TNO Quality of Life in the Netherlands. She is involved in guideline-driven toxicity studies that include studies into the safety of drugs and inhaled substances. Dr. Kuper obtained her Ph.D. at the Medical Faculty of the University of Utrecht. Before joining TNO, Dr. Kuper was external scientific advisor of the CEFIC-Long Range Initiative Toxicity programme and a member of the Education Committee of the Dutch Society of Pathologists. She participated in the ICICIS and NIEHS interlaboratory immunotoxicology studies. Dr. Kuper’s research areas are 'Respiratory allergy' and 'Immunopathology'. Projects sponsored by the Chemical Industries and the Dutch Ministries of Health, Welfare and Sport, and Social Affairs and Employement are on testing of the allergic potential of low molecular weight chemicals, the role of irritation in respiratory allergy and local inflammatory processes in respiratory allergy.

RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
ABSTRACT Thelper1-mediated allergic reactions in the respiratory tract: relevance for hazard identification of low molecular weight (LMW) allergens C. Frieke Kuper and Josje H. E. Arts TNO, Quality of Life, PO Box 360, 3700 AJ, the Netherlands Immune responses may be polarized toward either Thelper1 (Th1) or Thelper2 (Th2) production. Allergic contact dermatitis (mainly Th1) is the most common allergic disorder in the skin. Asthma and allergic rhinitis (mainly Th2), are most frequently encountered in the respiratory tract; asthma being so prominent that respiratory allergy has become almost synonymous to asthma. Thus, based on human evidence, the skin appears more prone to Thelper1 and the respiratory tract more prone to Thelper2 allergic disorders. This concept is in use to test chemicals for their potential to cause skin and/or respiratory allergy, although it is recognized that it is an oversimplification. Skin allergy also includes atopic dermatitis (mainly Th2) and respiratory allergy includes allergic alveolitis (hypersensitivity pneumonitis; mainly Th1). Moreover, LMW allergens examined today can activate both Th1- and Th2-cells, on the understanding that some of them preferentially induce either Th1 or Th2, whereas others do both almost equally well. The Th1-Th2 divergency between the skin and the respiratory tract may be less marked than it appears to be, due to an underestimation of Th1 disorders in the respiratory tract. To determine the relevance of Th1 allergic reactions for hazard identification of respiratory allergy induced by LMW compounds, the readiness to induce and the severity of Th1 responses in the respiratory tract should be known. Epidemiological studies have demonstrated the induction of allergic alveolitis (hypersensitivity pneumonitis), a serious, Th1-mediated respiratory disease by several anhydrides and diisocyanates, all of which are known respiratory LMW allergens. In addition, there is circumstantial (indirect) experimental evidence that predominantly Thelper1-mediated allergic inflammation in the nasal passages, larynx and/or lungs can be induced by trimellitic anhydride (TMA) and toluene diisocyanate (TDI), as well as by the typical contact allergens dinitrochlorobenzene (DNCB) and oxazolone (OXA); although OXA may not be such a typical contact allergen after all). It should be acknowledged that already upon a single challenge, TMA and, to a lesser extent, OXA induced a serious Th1-like allergic inflammation in sensitized animals whereas TDI and DNCB induced only a mild inflammatory cell infiltrate. The difference in severity of the response between the allergens can be explained partly by differences in challenge concentration, but it remains to be investigated if and how the mild infiltrate induced by TDI and DNCB progresses upon repeated/chronic exposure. It is concluded that Th1-mediated allergic inflammation need to be taken into consideration in the hazard identification for respiratory allergy.
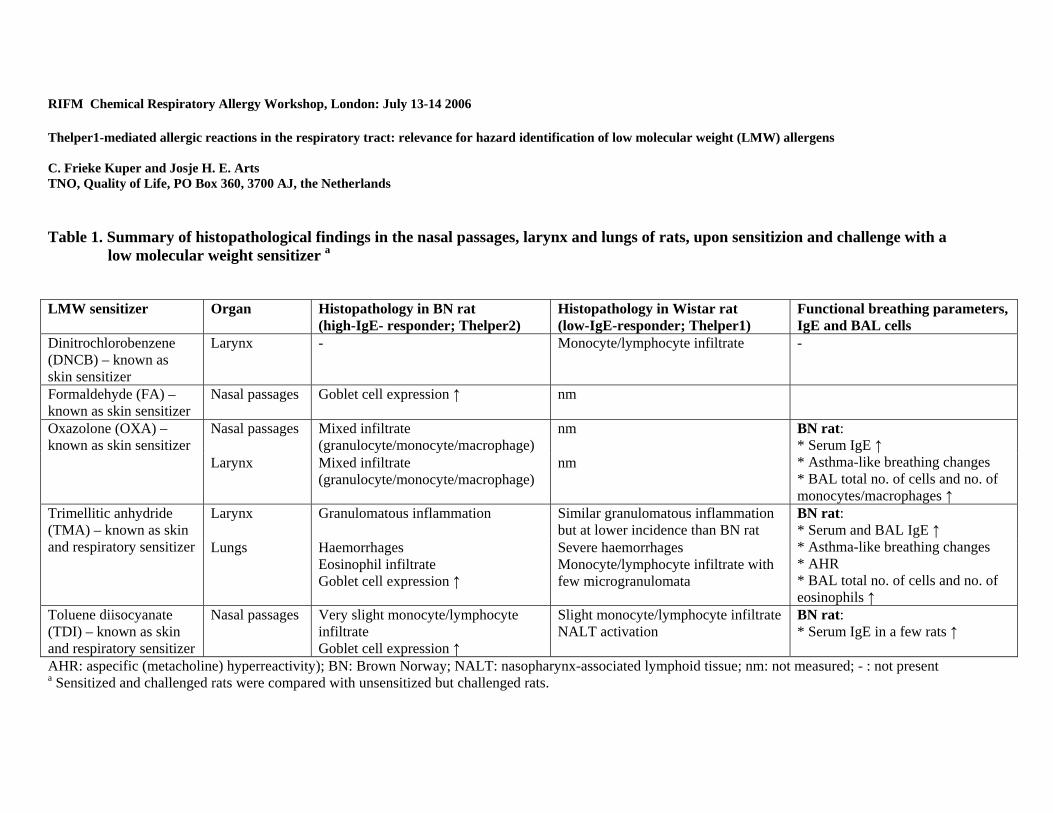
RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006 Thelper1-mediated allergic reactions in the respiratory tract: relevance for hazard identification of low molecular weight (LMW) allergens C. Frieke Kuper and Josje H. E. Arts TNO, Quality of Life, PO Box 360, 3700 AJ, the Netherlands Table 1. Summary of histopathological findings in the nasal passages, larynx and lungs of rats, upon sensitizion and challenge with a
low molecular weight sensitizer a
LMW sensitizer Organ Histopathology in BN rat (high-IgE- responder; Thelper2)
Histopathology in Wistar rat (low-IgE-responder; Thelper1)
Functional breathing parameters, IgE and BAL cells
Dinitrochlorobenzene (DNCB) – known as skin sensitizer
Larynx - Monocyte/lymphocyte infiltrate -
Formaldehyde (FA) – known as skin sensitizer
Nasal passages
Goblet cell expression ↑ nm
Nasal passages Mixed infiltrate (granulocyte/monocyte/macrophage)
nm Oxazolone (OXA) – known as skin sensitizer
Larynx Mixed infiltrate (granulocyte/monocyte/macrophage)
nm
BN rat: * Serum IgE ↑ * Asthma-like breathing changes * BAL total no. of cells and no. of monocytes/macrophages ↑
Larynx Granulomatous inflammation Similar granulomatous inflammation but at lower incidence than BN rat
Trimellitic anhydride (TMA) – known as skin and respiratory sensitizer Lungs Haemorrhages
Eosinophil infiltrate Goblet cell expression ↑
Severe haemorrhages Monocyte/lymphocyte infiltrate with few microgranulomata
BN rat: * Serum and BAL IgE ↑ * Asthma-like breathing changes * AHR * BAL total no. of cells and no. of eosinophils ↑
Toluene diisocyanate (TDI) – known as skin and respiratory sensitizer
Nasal passages Very slight monocyte/lymphocyte infiltrate Goblet cell expression ↑
Slight monocyte/lymphocyte infiltrate NALT activation
BN rat: * Serum IgE in a few rats ↑
AHR: aspecific (metacholine) hyperreactivity); BN: Brown Norway; NALT: nasopharynx-associated lymphoid tissue; nm: not measured; - : not present a Sensitized and challenged rats were compared with unsensitized but challenged rats.

1
RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
SUMMARY Thelper1-mediated allergic reactions in the respiratory tract: relevance for hazard identification of low molecular weight (LMW) allergens
C. Frieke Kuper and Josje H. E. Arts TNO, Quality of Life, the Netherlands
Immune responses may be polarized toward either Thelper1 (Th1) or Thelper2 (Th2) production. This
polarization may be advantageous as in certain parasitic infections but can be deleterious also as in
allergic disorders. Allergic contact dermatitis (mainly Th1) is the most common allergic disorder in
the skin. Asthma and allergic rhinitis (mainly Th2), are most frequently encountered in the respiratory
tract; asthma being so prominent that respiratory allergy has become almost synonymous to asthma.
Thus, based on human evidence, the skin appears more prone to Thelper1 and the respiratory tract
more prone to Thelper2 allergic disorders. This concept is in use to test chemicals for their potential to
cause skin and/or respiratory allergy, although it is recognized that it is an oversimplification. Skin
allergy also includes atopic dermatitis (mainly Th2) and respiratory allergy includes allergic alveolitis
(hypersensitivity pneumonitis; mainly Th1; Belenky and Fuhrman, 2006). Moreover, LMW allergens
examined today (metals excluded) can activate both Th1- and Th2-cells, on the understanding that
some of them preferentially induce either Th1 or Th2, whereas others do both almost equally well
(Dearman et al., 2003; Van Och et al., 2002; Ulrich et al., 2001). Their action may depend on tissue
factors, e.g. different manners of antigen presentation during sensitization, but if Th1-Th2 divergency
is tissue-dependent it is not so easy to understand why the skin can be such an effective route to
sensitize the respiratory tract for Th2-mediated allergic reactions by LMW allergens (Arts and Kuper,
2003; Warbrick et al., 2002). Finally, the Th1-Th2 paradigm does not take into account the role of
regulatory T cells, which may explain some of the conflicting experimental data (Oosterhout and
Bloksma, 2005).
The Th1-Th2 divergency between the skin and the respiratory tract may be less marked than it appears
to be, due to an underestimation of Th1 disorders in the respiratory tract. In contrast to allergic asthma,
which is considered to be predominantly Th2, Th1 reactions in the respiratory tract may be less
clinically manifest, or rather unspecific and thus not readily related to exposure. Moreover, the local
dose of airborne allergens in the respiratory tract depends not only on the concentration of the allergen
in the air but also strongly on the physicochemical characteristics of the compound (particulate versus
gaseous; size of particles; chemical reactivity) and the anatomy of the respiratory tract. Asthma is a
2
disease with a distinct functional abnormality. To come to expression, it might not matter much where
the main impact of the compound is, as long as it is somewhere in the bronchial tree where there is
muscle tissue to contract. Th1-mediated allergic inflammations, on the other hand, may also occur
everywhere in the respiratory tract and the lung parenchyma but may present as various different
entities.
The nature of an individual’s response to inhalation of an allergens is determined not only by the
characteristics of the allergen but also to a significant extent by his or her basic immunological
reactivity. Indeed, an individual with a prevalence for Th1 responses is more prone to develop allergic
alveolitis, while an individual with a prevalence for Th2 likely may develop asthma (Belenky and
Fuhrman, 2006). Experimental studies with TMA (Th1 and Th2) and DNCB (Th1) confirmed the
importance of host factors: firstly, Brown Norway (BN; high-IgE responding, Th2-prone) rats were
immunized to DNCB on the basis of a positive LLNA (Arts et al., 1997), but the respiratory tract did
not exhibit an allergic response despite the relatively large challenge concentration (Table 1;
unpublished observations) and secondly TMA-sensitized Wistar rats (low-IgE responding, Th1-prone)
did not exhibit asthma-like breathing changes upon TMA challenge despite a wide range of challenge
concentrations (Arts et al., 2004).
To determine the relevance of Th1 allergic reactions for hazard identification of respiratory allergy
induced by LMW compounds, the readiness to induce and the severity of Th1 responses in the
respiratory tract should be known. If relevant, should LMW contact allergens also be regarded as
potential respiratory allergens? Anhydride and diisocyanate allergens are classified as both
contact/skin (Th1) and respiratory (Th2) allergens. Occupational exposure to diisocyanates and
anhydrides is associated with asthma as well as allergic alveolitis (Merget et al., 2002; Grammer,
1999; Bauer, 1995). In addition, experimental work provided the following circumstantial (indirect)
evidence for the induction of Th1 responses in the respiratory tract by TMA and TDI (Table 1). TMA
induced a haemorrhagic pneumonitis (haemorrhages, lymphocytes and microgranulomata in the lungs)
in Wistar (Th1) rats, resembling allergic alveolitis in man. Pulmonary haemorrhages have also been
found with TMA in Sprague Dawley (Th1-prone) rats in a 4-week inhalation study at a very low
concentration (Leach et al., 1987). Moreover, a granulomatous inflammation was induced in the larynx
in both TMA-sensitized and -challenged Wistar (Th1) and BN (Th2) rats but not in unsensitized,
challenged rats. If this granulomatous laryngitis is truly a Th1 allergic inflammation, BN rats
expressed asthma-like (Th2?) breathing changes as well as granulomatous (Th1?) inflammation in the
larynx. The latter finding is somewhat unexpected because it appears to be in contrast with the
observation that the respiratory tract of BN rats was quite insensitive to the contact sensitizer DNCB
(Th1). TDI induced a predominantly lymphocytic infiltrate in the nasal passages of sensitized and

3
challenged BN and Wistar rats, independent of elevated serum IgE and in the absence of asthma-like
breathing changes. Since TDI is a reactive volatile substance, a response in the nasal passages was
expected but the similarity in response between Wistar and BN rats was not. It is unclear if the
lymphocytic infiltrate has any diagnostic value in identification of allergic rhinitis/asthma in BN rats.
These confusing results are in line with the indication that, especially diisocyanate allergens may
induce asthma by allergic, but non-IgE-mediated mechanisms (Maestrelli et al., 1997). Most evidence
points to involvement of a Th1 response. Surprisingly, AHR, one of the hallmarks of asthma, may be a
Th1-related phenomenon in TDI-induced asthma (Matheson et al., 2005).
The above data with diisocyanates and anhydrides support the notion that respiratory allergic disorders
are multifactorial and complex disorders, involving a spectrum of immune (and non-immune)
reactions. More straightforward responses may be expected with the LMW compounds DNCB,
DNFB, picrylchloride (TNCB), FA and OXA (Table 1), which have been recognized as contact
allergens but not as respiratory allergens in epidemiology studies. However, epidemiology data are
restricted because they are based on exposure. The very low vapour pressure and/or large particle size
of these allergens may preclude the generation of sufficiently high airborne concentrations.
Experimental studies with skin-sensitized and respiratory tract-challenged animals revealed an almost
pure lymphocytic infiltrate in the larynx of Wistar but not BN rats with DNCB (inhalatory challenge;
Zwart et al., 1994) and a comparable infiltrate in the lungs of Wistar rats and BalB/c mice with DNFB
and picrylchloride (intranasal challenge; Satoh et al., 1995; Garssen et al., 1989). The observations
lead to the following questions: Is a lymphocytic infiltrate in the larynx and lungs of sensitized and
challenged animals but not in unsensitized, challenged animals an indication of a Th1, delayed type
hypersensitivity response in the respiratory tract, like it would be in the skin? Can such an infiltrate
progress to a serious allergic disease upon repeated or chronic exposure? FA induced increased goblet
cell hyperplasia in the nasal passages of BN rats, which may be the result of an immune-mediated
response, because it was observed in sensitized and challenged animals only, or of neurological
stimulation (Fujimaka et al., 2004). The contact allergen OXA induced inflammatory cell infiltrates in
the nasal passages and larynx of sensitized and challenged BN rats, although it should be noted that
serum IgE levels were increased in these rats and they showed asthma-like breathing changes during
the challenge. Elevated serum IgE levels and expression of Th2 cytokines with OXA have been
observed before, especially upon repeated or chronic exposure (Webb et al., 1998). However, most test
systems are short-term, with few contacts with the allergens. The few repeated or chronic experiments
available showed that the immune response may change in the course of repeated or chronic exposure.
In summary, epidemiological studies have demonstrated the induction of a serious, Th1-mediated
respiratory allergy (allergic alveolitis or hypersensitivity pneumonitis) by several anhydrides and

4
diisocyanates, all of which are known respiratory LMW allergens. In addition, there is circumstantial
(indirect) experimental evidence that predominantly Thelper1-mediated allergic inflammation in the
nasal passages, larynx and/or lungs can be induced by respiratory allergens like TMA and TDI, as well
as by the typical contact allergens DNCB and OXA (although OXA may not be such a typical contact
allergen after all). It should be acknowledged that already upon a single challenge, TMA and, to a
lesser extent, OXA induced a serious Th1-like allergic inflammation in sensitized animals whereas
TDI and DNCB induced only a mild inflammatory cell infiltrate. The difference in severity of the
response between the allergens can be explained partly by differences in challenge concentration, but
it remains to be investigated if and how the mild infiltrate induced by TDI and DNCB progresses upon
repeated/chronic exposure. It is concluded that Th1-mediated allergic inflammation need to be taken
into consideration in the hazard identification for respiratory allergy.
References Arts JHE, Droge SCM, Spanhaak S, Bloksma N, Penninks AH, Kuper CF (1997) Local lymph node activation and IgE responses in Brown Norway and Wistar rats after dermal applciation of sensitizing and non-sensitizing chemicals. Toxicol 117:229-237
Arts JHE, Kuper CF (2003) Approaches to induce and elicit respiratory allergy : impact of route and intensity of exposure. Toxicology Letters 140-141:213-222
Arts JHE, De Koning MW, Bloksma N, Kuper CF (2004) Respiratory allergy to trimellitic anhydride in rats: concentration-response realtionships during elicitation. Inhalation Toxicol 16:1-11
Bauer X (1995) Hypersensitivity pneumonitis (extrinsic allergic alveolitis) induced by isocyanates. J Allergy Clin Immunol 95:1004-1010
Belenky SN, Fuhrman CR (2006) Hypersensitivity pneumonitis. In: P Fireman (ed) Atlas of Allergies and Clinical Immunology. 3rd Ed. Mosby, Elsevier, Philadelphia. pp 125-137
Dearman RJ, Skinner RA, Humphreys NE, Kimber I (2003) Methods for the identification of chemical respiratory allergens in rodents: comparisons of cytokine profiling with induced changes in serum IgE. J Appl Toxicol 23:199-207
Fujimaka H, Kurokawa Y, Kunugita N, Kikuchi M, Sato F, Arashidani K (2004) Differential immunogenic and neurogenic inflammatory responses in an allergic mouse model exposed to low levels of formaldehyde. Toxicology 197:1-13
Garssen J, Nijkamp FP, Wagenaar S Sc, Zwart A, Askenase P, Van Loveren H (1989) Regulation of delayed type hypersensitivity-like responses in the mouse lung, determined with histological procedures: serotonin, T cell suppressor-induced factor and high antigen dose tolerance regulate the magnitude of T cell dependent inflammatory reactions. Immunol 68:51-5558
Grammer LC (1999) Occupational allergic alveolitis. Ann Allergy Asthma Immunol 83:602-606
Leach CL, Hatoum NS, Ratajczak HV, Zeiss CR, Roger JC, Garvin PJ (1987) The pathologic and immunologic response to inhaled trimellitc anhydride in rats. Toxicol Appl Pharmacol 87:67-80
Maestrelli et al., 1997
Matheson JM, Johnson VJ, Luster MI (2005) Immune mediators in a murine model for occupational asthma: Studies with toluene diisocyanate. Txocol Sci 84(1):99-109
5
Merget R, Marczynski B, Chen Z, Remberger K, Raulf-Heimsoth M, Willrot PO, Baur X (2002) Haemorrhagic hypersensitivity pneumonitis due to naphtylene-1,5-diisocyanate. Eur Respir J 19:377-380
Oosterhout AJM, Bloksma N (2005) Regulatory T-lymphocytes in asthma. Eur Respir J 26:918-932
Satoh T, Kramarik JA, Tollerud DJ, Karol MH (1995) A murine model for assessing the respiratory hypersensitivity potential of chemical allergens.
Ulrich P, Grenet O, Bluemel J, Vohr HW, Wiemann C, Grundler O, Suter W (2001) Cytokine expression profiles during murine contact allergy: T helper 2 cytokines are expressed irrespective of the type of contact allergen. Arch Toxicol 75(8):470-479
Van Och FM, Van Loveren H, De Jong WH, Vandebriel RJ (2002) Cytokine production induced by low-molecular-weight chemicals as a function of the stimulation index in a modified local lymph node assay: an approach to discriminate contact sensitizers from respiratory sensitizers. Toxicol Appl Pharmacol 184:46-56
Warbrick EV, Dearman RJ, Kimber I (2002) IgG and IgE antibody responses following exposure of Brown Norway rats to trimellitic anhydride: comparison of inhalation and topical exposure. Toxicology 172:157-168
Webb EF, Tzimas MN, Newsholme SE, Grishold DE (1998) Intralesional cytokines in chronic oxazolone-induced contact sensitivity suggest roles for tumor necrosis factor alpha and interleukin-4. J Invest Dermatol. 111:86-92
Zwart A, Arts JHE, Kuper CF (1994) Wave propagation: a new parameter in the description of mechanical airway impedance. Eur Respir Rev. 4:203-209
Professor Ian Kimber BSc, MSc, PhD
BIO
Ian Kimber is currently a Syngenta Principal Fellow based at the Company Health Assessment Facility in Alderley Park, UK. He has broad research interests in all forms of allergy and immunmotoxicity, and in the initiation and regulation of cellular immune function. Professor Kimber has honorary appointments at several British Universities (Manchester, Birmingham, Liverpool, Central Lancashire and Aberdeen), sits on a variety of editorial boards (immunology, toxicology, dermatology and pathology journals) and serves, and has served, on many national and international expert and advisory committees. He has published approximately 500 research articles, review papers and book chapters

RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
ABSTRACT Relationships between Skin and Respiratory Chemical Allergens Ian Kimber1, David A Basketter2 and Rebecca Dearman3 1Syngenta Central Toxicology Laboratory, Macclesfield, UK; 2 Unilever Safety and Environmental Assurance Centre, Sharnbrook, UK. Chemical allergy may take a variety of forms; those of greatest significant within the context of occupational medicine being skin sensitisation resulting in allergic contact dermatitis, and sensitisation of the respiratory tract associated with asthma. There is a need to identify and characterise the potential of chemicals to induce allergic sensitisation. Although robust and validated methods are now in place for the toxicological evaluation of skin sensitising activity, approaches for the identification of chemical respiratory allergens are less mature, and as yet there are available no widely applied or validated methods for this purpose. Here we explore one aspect of chemical allergy that is of some interest; the fact that experience to date indicates that all chemicals that are known to induce sensitisation of the respiratory tract in humans elicit positive responses in the local lymph node assay, or in other standard tests for skin sensitisation potential. The utility of this activity with respect to integrated approaches to safety assessment will be discussed.
RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
SUMMARY Relationships between Skin and Respiratory Chemical Allergens Ian Kimber1, David A Basketter2 and Rebecca J Dearman11Syngenta Central Toxicology Laboratory, Macclesfield, UK; 2Unilever Safety and Environmental Assurance Centre, Sharnbrook, UK Within the context of occupational and environmental health there are two main forms that chemical
allergy may take. The first of these is skin sensitisation resulting in allergic contact dermatitis. The second
is allergic sensitisation of the respiratory tract resulting pulmonary hypersensitivity, asthma and/or rhinitis.
These allergic diseases pose toxicologists with important, but different, challenges. Skin sensitisation is a
common occupational health problem, with many hundreds of chemicals having been implicated as
contact allergens, and is without doubt the most common manifestation of immunotoxicity among
humans. In contrast, allergic sensitisation of the respiratory tract is less prevalent and fewer chemicals
have been found to case respiratory allergic disease. This is, however, an important manifestation of
chemical allergy, not least because occupational asthma is associated with high levels of morbidity, and
can be fatal. Moreover, there are as yet no validated or widely accepted methods available for the
identification of chemicals that have the potential to cause respiratory allergy.
It is intriguing that some chemical allergens (the majority) preferentially induce in humans skin
sensitisation, whereas others (much fewer in number) selectively cause sensitisation of the respiratory
tract. The bases for these differences have been the investigated for some time and current understanding
of the relevant immunological processes has informed the development of proposed approaches to the
prospective identification of chemical respiratory allergens. However, irrespective of the mechanisms
underlying the development of divergent allergic responses in man, there is evidence that in animal
models for the assessment of skin sensitising activity respiratory allergens (as well as contact allergens)
elicit positive responses. To some extent this is unexpected because despite opportunities for dermal
exposure those chemical respiratory allergens for which sufficient data are available appear to cause skin
sensitisation only rarely.
Although this represents something of a paradox the fact remains that chemical respiratory allergens will
normally elicit positive responses in the local lymph node assay (LLNA), even when they are only rarely
associated with skin sensitisation in human subjects. In fact, our view currently is that most if not all
identified chemical respiratory allergens test positive in the LLNA. The practical implication of this with
respect to hazard identification is that one can draw from these observations the conclusion that chemicals
1
that test negative in the LLNA not only lack the potential to cause skin sensitisation, but will fail also to
induce allergic sensitisation of the respiratory tract.
From this arises the proposal that in an integrated testing strategy for sensitising activity a first step would
be to test chemicals in the LLNA.Those eliciting a positive response would naturally be identified on this
basis as having skin sensitising activity. A potential also to cause sensitisation of the respiratory tract
would not be excluded on this basis and if necessary additional investigations – such as those that will be
discussed during this workshop – might be deployed if there were concerns about the potential for
respiratory sensitisation. In this context, and with respect to managing such a strategy effectively, it is
important to emphasise that although all chemical respiratory allergens are though to elicit positive
responses in the LLNA, only a small fraction of chemicals that test positive in the LLNA are respiratory
allergens.
The corollary is that chemicals that fail to elicit a positive response in the LLNA can be considered to
lack both skin and respiratory sensitising activity.
2

Meryl H. Karol, PhD
BIO
Meryl H. Karol, PhD is a Professor of Environmental and Occupational Health, and Civil and Environmental Engineering at the University of Pittsburgh, and Associate Dean for Academic Affairs. She is recognized for her innovative animal models of respiratory diseases, including byssinosis, hypersensitivity pneumonitis, respiratory irritancy and chemically-induced asthma, and for development of novel radioimmunoassay to detect immunologic responses to chemical allergens. She is credited with identifying the dose-dependency for induction of chemically-induced respiratory sensitization. Her current research is focused on the effect of chemicals on the developing immune system, and health effects from indoor air pollutants. She holds three patents related to design of novel test antigens to detect immunologic responses. Her teaching includes classes on immunotoxicology, dermal toxicology, air pollution, environmental epidemiology and environmental science.
Dr. Karol received her BS from Cornell University (Ithaca, NY), a Ph.D. in immunochemistry from Columbia University (NY), and undertook postdoctoral studies in biochemistry at the State University of New York (Stony Brook)
Dr. Karol has been active in numerous scientific and professional societies. She was elected the first female President of the Society of Toxicology (1994-5), and was elected Director of the International Union of Toxicology (IUTOX) (1995-98), and Secretary-General of IUTOX (1998-2004). Dr. Karol serves on the Scientific Advisory Board of the EPA, and the Advisory Committee for Pharmaceutical Science of the FDA Center for Drug Evaluation Research. She currently chairs the National Research Council’s Committee on Toxicologic and Radiologic Effects from Exposures to Depleted Uranium During and After Combat. She is a Fellow of the American Toxicology Society and has served on its Board of Directors.
Dr. Karol is the recipient of numerous national awards including the Rachel Carson Award, the Frederick Sperling Memorial Award, Women in Science Award, the Frank R. Blood Award, among others. She has published extensively on structure-activity and molecular modeling of chemically-induced asthma and allergic contact dermatitis.
RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
ABSTRACT Structure-Activity Relationships and Models of Chemicals Causing Respiratory Sensitization Meryl H. Karol, PhD Structure-activity relationship (SAR) models are important in chemical sensitization since they have both the potential to contribute mechanistic insight into this airway disease and to predict the sensitization activity of new drugs and chemicals. The most important factor influencing sensitization is the structure of the chemical. Other contributory factors relate to genetics and characteristics of the exposure, including the dose, route, duration, and frequency of exposure. For a chemical to be biologically active, it first must be transported from its site of contact to its site of action, and then interact with receptors or targets. Accordingly, active chemicals must possess appropriate partition and reactivity values. Because of the hydrophilic environment of the respiratory tract, as compared with the hydrophobic environment of the skin, it is expected that chemicals causing respiratory sensitization would differ considerably from skin sensitizing chemicals in transport factors. This presentation will highlight developments in structure-activity models of chemically-induced respiratory hypersensitivity, and describe the databases, types of models developed, (ie, those based on physical-chemical considerations and those based on mechanistic understanding of respiratory sensitization), as well as structural alerts of respiratory sensitizers, and predictions and limitations of the models. Lastly, the importance of rigorous validation of SAR models will be discussed.
DR. REBECCA J. DEARMAN
BIO Dr Rebecca J. Dearman is Head of Immunology Research at the Syngenta Central Toxicology Laboratory. Her active research interests include all aspects of allergy, particularly the cellular and molecular regulation of food allergy, chemical respiratory sensitization and contact allergy. Dr. Dearman joined the Syngenta Central Toxicology Laboratory in 1988 after completing a Biochemistry degree at the University of Bath and a PhD in Immunochemistry at the University of Southampton. Dr Dearman is a member of the British Toxicology Society, the US Society of Toxicology and the British Society of Immunology. She is a member of the Committee on Toxicity of Chemicals in Food, Consumer Products and the Environment and is on the editorial board of the journals Toxicological Sciences and Food and Chemical Toxicology. Dr. Dearman has over 200 peer reviewed publications and has made over 700 presentations at national and international scientific meetings.
RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
ABSTRACT The Identification of Chemical Respiratory Allergens: the CTL Approach Rebecca J Dearman and Ian Kimber Syngenta Central Toxicology Laboratory, Macclesfield, UK Chemical respiratory allergy is an important occupational health problem, but there are currently available no validated methods for hazard identification. There is now increasing evidence that respiratory sensitisation is associated with the preferential activation of type 2 T lymphocytes and the expression of type 2 cytokines interleukin (IL)-4, IL-5, IL-10 and IL-13. Respiratory sensitizing potential has been explored as a function of induced cytokine secretion profiles in Brown Norway (BN) rats and BALB/c strain mice. Animals have been exposed topically to the reference contact allergen 2,4-dinitrochlorobenzene (DNCB), which lacks respiratory sensitizing potential, or to the reference respiratory allergen trimellitic anhydride (TMA). Exposure of BALB/c strain mice or BN rats resulted in Th1- and Th2-type cytokine secretion patterns being induced by DNCB and TMA, respectively. Cytokine expression patterns by BN lymph node cells (LNC) were considerably more variable than those observed for LNC derived from BALB/c strain mice. To date, 7 contact allergens and 14 respiratory allergens from different chemical classes have been shown to stimulate type 1 and type 2 cytokine profiles, respectively, in the BALB/c strain mouse. These data suggest that the measurement of induced cytokine secretion profiles in the BALB/c strain mouse provides a robust method for hazard identification and characterization of chemical respiratory allergens.
RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
SUMMARY The Identification of Chemical Respiratory Allergens: the CTL Approach Rebecca J Dearman and Ian Kimber Syngenta Central Toxicology Laboratory Macclesfield, UK Chemical respiratory allergy is an important occupational health problem, but there are currently available
no validated methods for hazard identification. This is due in part to the fact that the relevant cellular and
molecular mechanisms of sensitisation of the respiratory tract have been unclear, with particular
controversy regarding the role of IgE. There is now increasing evidence that respiratory sensitisation is
associated with the preferential activation of type 2 T lymphocytes and the expression of type 2 cytokines
interleukin (IL)-4, IL-5, IL-10 and IL-13. Type 2 cell products favour immediate type hypersensitivity
reactions, serving as growth and differentiation factors for mast cells and eosinophils, the cellular
effectors of the clinical manifestations of the allergic responses, and promoting IgE antibody production.
In contrast, type 1 cell products, such as interferon-γ (IFN-γ), down-regulate IgE antibody production and
favour delayed type hypersensitivity reactions such as contact sensitisation.
Immune responses have been characterised in BALB/c strain mice following topical exposure to the
reference respiratory allergen trimellitic anhydride (TMA), or to 2,4-dinitrochlorobenzene (DNCB) a
contact allergen that apparently lacks potential to cause sensitisation of the respiratory tract. Under
conditions of exposure of equivalent immunogenicity with respect to lymphocyte proliferation and IgG
antibody responses, treatment only with TMA provoked increases in serum IgE concentration and a
preferential type 2 cytokine profile in lymph node cells draining the site of exposure. The converse type 1
cytokine secretion profile was provoked by topical exposure to DNCB. These polarised cytokine

phenotypes take time to develop (measured usually 13 days after initiation of exposure), with LNC
isolated 3 days after the start of exposure displaying a mixed phenotype with both type 1 and type 2
cytokines expressed following treatment with both chemical contact and respiratory allergens. The ability
of DNCB and TMA to provoke divergent cytokine expression patterns (“cytokine fingerprinting”) has
been confirmed using the Brown Norway strain rat, although more inter-experimental variation in
cytokine secretion was observed in the latter species. These data suggest that chemical contact allergens
such as DNCB and respiratory sensitizers such as TMA exhibit an innate ability to stimulate type 1 and
type 2 cytokine production profiles, respectively, which is species independent.
Subsequent applications of cytokine fingerprinting in the BALB/c strain mouse conducted with a range of
additional chemical respiratory allergens, including diisocyanates, platinum salts, glutaraldehyde, and
various acid anhydrides, have confirmed that the expression of a preferential type 2 cytokine expression
profile is a general property of respiratory sensitising chemicals. Using the same exposure protocol,
treatment with allergens such as 2,4-dinitrofluorobenzene (DNFB), isoeugenol and hexyl cinnamic
aldehyde (contact allergens that apparently lack respiratory sensitizing activity) stimulates instead a
selective type 1 cytokine secretion pattern. These data suggest that the measurement of induced cytokine
secretion profiles in the BALB/c strain mouse shows real promise as a method for hazard identification
and characterisation of chemical respiratory allergens.
Dr. Josje Arts Bio
Dr. Josje Arts is Product Manager Inhalation Toxicology, Toxicology and Applied Pharmacology Department at TNO. She started with TNO in 1986 as an inhalation toxicologist. In 1993 she started to work on respiratory allergy. Her specialties are: Inhalation Toxicology, Respiratory Irritation and Respiratory Allergy.
Dr. Arts studied Human Nutrition at the Wageningen University NL, with toxicology as the main subject. Her work with TNO on respiratory allergy resulted in her 2001 PhD thesis entitled ‘Respiratory allergy induced by low molecular weight chemicals in rats.’
Dr. Arts advises both government and industry on her specialty topics and she has obtained research projects from both sectors on respiratory allergy and toxicity of nanoparticles.
RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
ABSTRACT THE IDENTIFICATION OF CHEMICAL RESPIRATORY ALLERGENS: THE TNO APPROACH Josje Arts and Frieke Kuper. TNO Quality of Life, Zeist, the Netherlands. Human experience seems to have taught us that not all contact allergens have shown respiratory allergenic potential, whereas on the contrary, all respiratory LMW chemicals tested have shown contact allergenic potential, or in other words, were positive in one or more contact allergy tests. In addition, there is a growing body of evidence that effective sensitisation of the respiratory tract by defined chemical respiratory allergens can occur in response to dermal contact.
Contact allergens have not shown respiratory allergenic potential but this might be just a matter of exposure because all LMW respiratory allergens known to date have been classified based on human experience (exposure), and not on hazard, due to the lack of validated test methods. Experimental studies with typical contact sensitizers like DNCB, DNFB, picrylchloride and oxazolone have shown aspecific airway hyperreactivity, and allergic pulmonary inflammation in sensitized and challenged rats and mice (and not in challenged-only animals).
A recently carried out LLNA by the inhalation route in BALB/c mice, together with our colleagues from RIVM, NL, (W.H. de Jong and R.J. Vandebriel), has not only shown positive results for the acid anhydrides TMA and phthalic anhydride and for the diisocyanates TDI and HDI, but also for the typical contact allergens DNCB and oxazolone, indicating that all these compounds should receive the label ‘sensitisation by inhalation’.
The following tiered approach is proposed for the identification of respiratory LMW allergens:
- Stage 0: Examination of the risk of inhalatory exposure on the basis of physical characteristics and/or use of the chemical.
- Stage 1: When inhalation exposure is likely, assessment of sensitising potential by the LLNA in mice or rats.
- Stage 2: In case further studies into the positive result in stage 1 are required, assessment of the capacity to increase total serum IgE in BN rats.
- Stage 3: In case of a positive result in stage 2, assessment of functional and morphological airway changes in the sensitised BN rat upon an inhalative provocation at the time that total serum IgE levels are high.
Overall, using this tiered approach, a large part of the responses of humans to inhaled TMA have been reproduced in the high IgE-responding BN rat and this approach has been found to clearly distinguish a respiratory allergen (TMA) from a typical skin allergen (DNCB), and from a non-sensitiser (methyl salicylate). With TMA, positive results were obtained in both the LLNA and IgE-test, and inhalation challenge indeed resulted in asthma-like functional and morphological reactions, and non-specific airway hyperreactivity in sensitised BN rats only. In sensitised low IgE-responding Wistar rats, reactions were limited to non IgE-associated morphological airway changes. Moreover, immune-mediated functional airway reactions in BN rats induced by TMA could be distinguished from irritation reactions induced by the same compound. With DNCB and oxazolone, it has been shown that LMW chemicals capable of inducing skin sensitisation may also represent a risk of respiratory allergy when inhaled.
Testing of other (respiratory) sensitizers will have to prove the usefulness of the tiered approach in the rat as described here.
RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
SUMMARY THE IDENTIFICATION OF CHEMICAL RESPIRATORY ALLERGENS: THE TNO APPROACH Josje Arts and Frieke Kuper. TNO Quality of Life, Zeist, the Netherlands. Human experience seems to have taught us that not all contact allergens have shown respiratory allergenic
potential, whereas on the contrary, all respiratory LMW chemicals tested have shown contact allergenic
potential, or in other words, were positive in one or more contact allergy tests. In addition, there is a growing
body of evidence that effective sensitisation of the respiratory tract by defined chemical respiratory allergens
(such as for instance the acid anhydrides) can and does occur in response to dermal contact.
Contact allergens have not shown respiratory allergenic potential but this might be just a matter of exposure
because all LMW respiratory allergens known to date have been classified based on human experience
(exposure), and not on hazard, due to the lack of validated test methods. Experimental studies with typical
contact sensitizers like DNCB, DNFB, picrylchloride and oxazolone have shown aspecific airway
hyperreactivity, and allergic pulmonary inflammation in sensitized and challenged rats and mice (and not in
challenged-only animals; see for an overview Arts and Kuper, 2006). Therefore, it is not unlikely that people
who are sensitized might suffer adverse pulmonary reactions if they were to inhale sufficient amounts of the
contact allergen to which they were sensitized. Therefore, the absence of diseases like extrinsic allergic
alveolitis in a substantial number of individuals exposed to contact allergens is in our view more a matter of risk
(on inhalation exposure but dermal exposure only) rather than hazard. It should, however, be noted that it has
been indicated in literature that extrinsic allergic alveolitis is considered being overlooked to a large extent.
A recently carried out LLNA by the inhalation route in BALB/c mice, together with our colleagues from
RIVM, NL (W.H. de Jong and R.J. Vandebriel), has not only shown positive results for the acid anhydrides
TMA and phthalic anhydride and for the diisocyanates TDI and HDI, but also for the typical contact
allergens DNCB and oxazolone, indicating that all these compounds should receive the label ‘sensitisation
by inhalation’.
The following tiered approach is proposed for the identification of respiratory LMW allergens (see Figure 1;
Arts, 2001):
- Stage 0: Examination of the risk of inhalatory exposure on the basis of physical characteristics and/or use
of the chemical.

- Stage 1: When inhalation exposure is likely, assessment of sensitising potential by the LLNA in mice or
rats. For hazard assessment, regardless whether exposure is likely or not, a LLNA should always be
performed. In case of a negative result, the substance is considered a non-sensitising chemical provided
that skin absorption has taken place. In case of a positive result, further testing may be considered
unnecessary when, for classification purposes, one is interested in sensitising potential only. As such the
chemical should be classified (hazard) for both skin and respiratory allergy.
- Stage 2: In case further studies into the positive result in stage 1 are required, assessment of the capacity
to increase total serum IgE in BN rats. Such a test is also recommended for existing chemicals which
have already been identified as skin sensitizers and for which inhalation exposure is likely to occur.
- Stage 3: In case of a positive result in stage 2, assessment of functional and morphological airway
changes in the sensitised BN rat upon an inhalative provocation at the time that total serum IgE levels are
high. Concentration levels below which adverse effects are unlikely to occur can be established. Further,
histopathological examination should confirm Th2 allergy and/or provide information on other types of
inflammatory airway reactions.
Overall, using this tiered approach, a large part of the responses of humans to inhaled TMA have been
reproduced in the high IgE-responding BN rat and this approach has been found to clearly distinguish a
respiratory allergen (TMA) from a typical skin allergen (DNCB), and from a non-sensitiser (methyl
salicylate). With TMA, positive results were obtained in both the LLNA and IgE-test, and inhalation
challenge indeed resulted in asthma-like functional and morphological reactions, and non-specific airway
hyperreactivity in sensitised BN rats only. In sensitised low IgE-responding Wistar rats, reactions were
limited to non IgE-associated morphological airway changes. Moreover, immune-mediated functional airway
reactions in BN rats induced by TMA could be distinguished from irritation reactions induced by the same
compound. With DNCB and oxazolone, it has been shown that LMW chemicals capable of inducing skin
sensitisation may also represent a risk of respiratory allergy when inhaled.
Testing of other (respiratory) sensitizers will have to prove the usefulness of the tiered approach in the rat as
described here.
References Arts J.H.E. (2001) Respiratory allergy induced by low molecular weight chemicals in rats. PhD thesis, Utrecht University, NL
Arts J.H.E. and Kuper C.F. (2006) Animal models to test respiratory allergy of low molecular weight chemicals: a guidance. Methods (accepted)
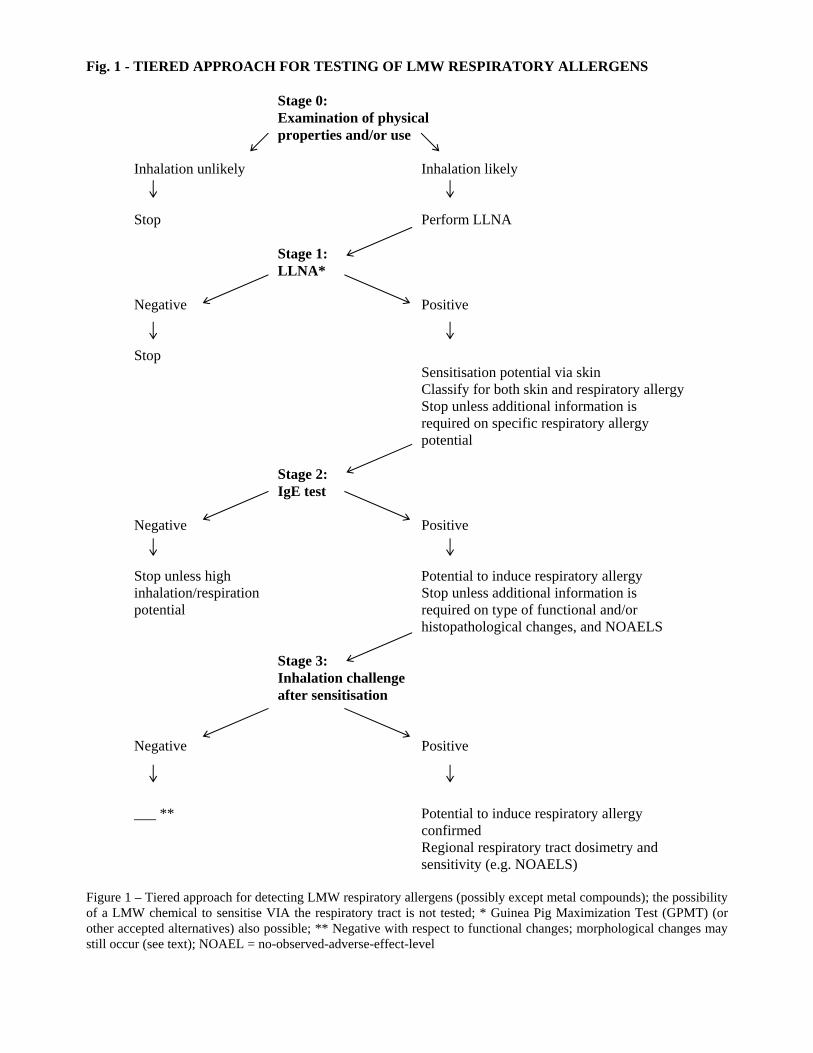
Fig. 1 - TIERED APPROACH FOR TESTING OF LMW RESPIRATORY ALLERGENS
Stage 0: Examination of physical properties and/or use Inhalation unlikely Inhalation likely Stop Perform LLNA Stage 1: LLNA* Negative Positive Stop Sensitisation potential via skin Classify for both skin and respiratory allergy
Stop unless additional information is required on specific respiratory allergy
potential Stage 2: IgE test Negative Positive Stop unless high Potential to induce respiratory allergy inhalation/respiration Stop unless additional information is potential required on type of functional and/or histopathological changes, and NOAELS Stage 3: Inhalation challenge after sensitisation Negative Positive ___ ** Potential to induce respiratory allergy confirmed Regional respiratory tract dosimetry and sensitivity (e.g. NOAELS) Figure 1 – Tiered approach for detecting LMW respiratory allergens (possibly except metal compounds); the possibility of a LMW chemical to sensitise VIA the respiratory tract is not tested; * Guinea Pig Maximization Test (GPMT) (or other accepted alternatives) also possible; ** Negative with respect to functional changes; morphological changes may still occur (see text); NOAEL = no-observed-adverse-effect-level

Dr. Rob Vandebriel
Bio
Dr. R;ob Vandebriel is with the Netherlands National Institute for Public Health & the Environment
(RIVM) in the Laboratory for Toxicology, Pathology & Genetics. His research focuses on the areas of
long-term adverse effects of vaccination, expressed as allergy and autoimmunity, with special
emphasis on the role of the innate immune system and in vivo and in vitro methods to assess
immunotoxicity, with special emphasis on sensitization and genomics approaches.
Dr. Vandebriel was granted a MSc in 1984 from Wageningen University, Netherlands where he
studied Virology, Molecular Biology, and Biochemistry. He received his Ph.D. in 1991 from Utrecht
University in the Netherlands. His thesis was titled “Initiation of the cellular immune response against
murine tumor allografts.”
Dr. Vandebriel’s work includes the publications:
Vandebriel, R.J., W.H. De Jong, S.W. Spiekstra, M. Van Dijk, A. Fluitman, J. Garssen & H. Van
Loveren. Assessment of preferential T-helper 1 or T-helper 2 induction by low molecular weight
compounds using the local lymph node assay in conjunction with RT-PCR and ELISA for Interferon-γ
and Interleukin-4. Toxicol. Appl. Pharmacol. 162, 77-85 (2000).
Banus, H.A., R.J. Vandebriel, H. de Ruiter, J.A.M.A. Dormans, N.J. Nagelkerke, F.R. Mooi, B.
Hoebee, H.J. van Kranen & T.G. Kimman. Host genetics of Bordetella pertussis infection in mice; the
significance of Tlr4 in genetic susceptibility and pathobiology. Infect. Immun. 74, 2596-2605 (2006).

RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
ABSTRACT CYTOKINE PRODUCTION INDUCED BY LOW- MOLECULAR-WEIGHT CHEMICALS AFTER INHALATORY EXPOSURE RJ Vandebriel1 , JHE Arts2 , A de Klerk1, CF Kuper2 ,H van Loveren1 and WH de Jong1. 1RIVM, Bilthoven, the Netherlands, and 2TNO Quality of Life, Zeist, the Netherlands. The LLNA is used to test the potential of low molecular weight (LMW) compounds to induce sensitization via the skin. A stimulation rate of 3 times the control value is used as cut off point to designate a compound a sensitizer. The dose inducing a stimulation index of 3 (EC3 value) can be used to compare potency between compounds and was found to correlate with human skin sensitization thresholds. To date all known LMW respiratory allergens tested were found positive in this dermal assay. It is unknown whether the potency as determined by the dermal route is comparable to the potency after inhalation exposure.
In general, contact sensitizers have been shown to selectively induce Th1 immune responses, such as IFN-γ production, whereas Th2 responses, such as interleukin (IL)-4 production, were seen after exposure to respiratory allergens. In the present study we investigated whether inhalation exposure would result in similar lymph node stimulation as observed after skin exposure. In addition cytokine profiling was used to characterize the response.
The contact allergens 2,4- dinitrochlorobenzene (DNCB), hexyl cinnamic aldehyde (HCA) and oxazolone (OXA, 4-ethoxymethylene 2- phenyloxazol-5-one), as well as the respiratory allergens fluorescein 5-isothiocyanate, phthalic anhydride (PA), toluene diisocyanate (TDI), and trimellitic anhydride (TMA) were tested after dermal exposure. For a range of concentrations, both proliferative responses and cytokine production were established. From the estimated concentrations, IFN-γ, IL-4, and IL-10 production as a function of stimulation indices were plotted. All four respiratory allergens showed significantly higher IL-4 and IL-10 production patterns compared to the contact allergens. Positive identification of DNCB, HCA, and OXA as contact allergens on the basis of IFN-γ production, was observed only at very high stimulation indices (SI≥35) for DNCB and OXA and already at low SI’s (SI≤7) for HCA. In subsequent studies mice were exposed inhalatory to the contact sensitizer DNCB and respiratory allergen TMA. Different exposure doses were obtained by exposing the animals for various times (45, 90, 180 or 360 min/day) for three consecutive days to the same concentration. Dermal application was used as a positive control for the induction of immune responses. Lymph nodes in the nasopharyngeal region showed an increase in weight and cell number, and positive (i.e. SI > 3) proliferation responses, although these responses were in general lower than the positive controls observed in lymph nodes draining the skin exposed sites (ear). Induction of cytokines was determined after in vitro stimulation of the lymph node cells with concanavalin A for 24 hours. Preliminary results of these experiments will be presented.
This research is funded by the Dutch Ministry of Public Health, Welfare and Sports (VWS).

RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
SUMMARY CYTOKINE PRODUCTION INDUCED BY LOW- MOLECULAR-WEIGHT CHEMICALS AFTER DERMAL AND INHALATION EXPOSURE RJ Vandebriel1 , JHE Arts2 , A de Klerk1, CF Kuper2 , H van Loveren1 and WH de Jong1 . 1RIVM, Bilthoven, the Netherlands, and 2TNO Quality of Life, Zeist, the Netherlands. Chemical sensitizers can be identified in the local lymph node assay (LLNA) in which the potential of low
molecular weight (LMW) compounds to induce lymph node cell proliferation is measured as a marker for
sensitization after skin exposure. A stimulation rate of 3 times the control value is used as cut off point to
designate a compound a sensitizer. The dose inducing a stimulation index of 3 (EC3 value) can be used to
compare potency between compounds (Basketter et al 1999, 2005, Van Och et al 2000, De Jong et al 2002),
and was found to correlate with human skin sensitization thresholds (Griem et al 2003, Schneider and Akkan
2004, Basketter et al 2005). To date all known LMW respiratory allergens tested were found positive in this
dermal assay. It is unknown if the potency as determined by the dermal route is comparable to the potency
after inhalation exposure.
The term respiratory hypersensitivity is used to describe asthma and other related respiratory conditions
irrespective of the underlying immunological (or non-immunological) mechanism. Respiratory allergy or
asthma, when caused by protein allergens is accompanied by IgE production which ultimately may result in
an anaphylactic shock after secondary exposure. For chemically induced respiratory allergy there might be a
role for IgE, but IgE induction is not always obvious. In patients IgE may be absent in chemically induced
respiratory allergy. So, other (immunological) mechanisms may be partly responsible for the expression of
respiratory hypersensitivity. One of these might be the Thelper1 response, as several skin sensitizers known
to induce Thelper1 reactions were able to induce allergic responses in the lungs (Arts and Kuper 2006),
including hyperreactivity to non-specific stimuli (Garssen et al 1991). In a recent paper by Vanoirbeek et al
(2006) a difference was observed between DNCB and TMA responses in the lung at a secondary inhalatory
challenge after previous skin sensitization. TMA but not DNCB induced ventilatory changes, while both
compounds induced similar inflammatory responses as indicated by evaluation of bronchial lavage fluids.
Also lymph node responses in terms of cytokine production were qualitatively similar, but IL-4 induction
was quantitatively different. IgE levels were increased only after TMA treatment. So, irrespective of the
immunological mechanisms both compounds induced an immunological response after inhalation challenge.
One of the methods proposed for the distinction between contact and respiratory sensitizers is the
determination of cytokine production in the draining lymph node after skin exposure (Dearman et al 1995,
1996, Vandebriel et al 2000, 2003). Lymph node cells can be harvested and either used with or without in
vitro (re)stimulation with concanavalin A (Con A). Both mRNA expression and cytokine production of IFNγ

and Il-4 could be used for discrimination between DNCB and TMA (Vandebriel et al 2000, 2003). Only
TMA could be positively identified as respiratory sensitizer by the IL-4 production. In a study comparing a
short exposure and a longer exposure (Dearman et al 1995), both in the short (5 days) and in the longer (17
days) protocol similar results were obtained (Vandebriel et al 2003). There were no differences between
DNCB and TMA, or between culture with and without Con A for the production of the Thelper1 cytokine
IFNγ, although cultures terminated at 5 days generally reached higher levels of IFNγ production. DNCB
treatment induced after Con A stimulation of the lymph node cells only low levels of IL-4 in both exposure
scenarios, while TMA induced IL-4 in both exposure scenarios both with and without Con A stimulation.
However, Con A simulation resulted in much higher (>10 fold) IL-4 levels. So, especially for the induction
of IL-4 in vitro (re)stimulation of the lymph node cells with Con A is necessary in order to obtain IL-4 levels
which can be used to distinguish between contact and respiratory sensitizers. As both DNCB and TMA were
found to induce almost equal levels of IFNγ, IFNγ can not be used to positively discriminate these two
compounds.
Although a stimulation index of 3 is used as cut off point for designating a compound a sensitizer, much
higher stimulation indices can be found for strong allergens like DNCB and TMA. We investigated how the
strength of the immunization as measured by the stimulation index after dermal exposure would influence
cytokine production, and thus would influence the outcome of the test (Van Och et al 2002). The contact
allergens 2,4- dinitrochlorobenzene (DNCB), hexyl cinnamic aldehyde (HCA) and oxazolone (OXA, 4-
ethoxymethylene 2- phenyloxazol-5-one), as well as the respiratory allergens fluorescein 5-isothiocyanate
(FITC), phthalic anhydride (PA), toluene diisocyanate (TDI), and trimellitic anhydride (TMA) were tested.
For a range of concentrations, both proliferative responses and cytokine production were established.
Estimated concentrations were derived at several stimulation indices (SIs). From the estimated
concentrations, IFN-γ, IL-4, and IL-10 production as a function of stimulation indices were plotted. All four
respiratory allergens showed significantly higher IL-4 and IL-10 production patterns compared to the contact
allergens. Positive identification of DNCB, HCA, and OXA as contact allergens on the basis of IFN-γ
production, was observed only at very high stimulation indices (SI≥35) for DNCB and OXA and already at
low SI’s (SI≤7) for HCA.
To investigate whether the dermal route is sufficient for the identification of respiratory sensitizers or
whether for a more reliable identification inhalation exposure would be needed, similar experiments were
performed with DNCB and TMA after inhalation exposure. Different exposure doses were obtained by
exposing the animals for various times (45, 90, 180 or 360 min/day) to the same concentration. Dermal
application was used as a positive control for the induction of immune responses. Lymph nodes in the
nasopharyngeal region showed an increase in weight and cell number, and positive (i.e. SI > 3) proliferation
responses, although these responses were in general lower than the positive controls observed in lymph
nodes draining skin exposed sites (ear). Induction of cytokines was determined after in vitro stimulation of
the lymph node cells with Con A for 24 hours.
References Arts JHE and Kuper CF. (2006) Animal models to test respiratory allergy of low molecular weight chemicals: a guidance. Methods (accepted for publication)
Basketter DA, Andersen KE, Liden C, Van Loveren H, Boman A, Kimber I, Alanko K, Berggren E (2005). Evaluation of the skin sensitizing potency of chemicals by using the existing methods and considerations of relevance for elicitation. Contact Dermatitis 52, 39-42.
Basketter DA, Clapp C, Jefferies D, Safford RJ, Ryan CA, Gerberick GF, Dearman RJ and Kimber I. (2005) Predictive identification of human skin sensitisation thresholds. Contact Dermatitis, 53, 260 - 267.
Basketter DA, Lea LJ, Dickens A, Briggs D, Pate I, Dearman RJ, Kimber I (1999). A comparison of statistical approaches to the derivation of EC3 values from local lymph node assay dose responses. J Appl Toxicol 19, 261-266.
Dearman RJ, Basketter DA, Kimber I. (1995) Differential cytokine production following chronic exposure of mice to chemical respiratory and contact allergens. Immunology 86, 545-550.
Dearman RJ, Smith S, Basketter DA, Kimber I (1996). Classification of chemical allergens according to cytokine profiles of murine lymph node cells. J Appl Toxicol 17, 53-62.
De Jong WH, Van Och FMM, Den Hartog JAger CF, Spiekstra SW, Slob W, Vandebriel RJ, Van Loveren H (2002). Ranking of allergic potency of rubber chemicals in a modified local lymph node assay. Toxicol Sc 66, 226-232.
Garssen J, Nijkamp FP, Van Der Vliet H, Van Loveren H (1991). T cell mediated induction of airway hyperreactivity in mice. Am Rev Resp Dis 144, 931-938.
Griem, P., Goebel, C., and Scheffler, H. (2003). Proposal for a risk assessment methodology for skin sensitization potency data. Reg. Tox. Pharmacol. 38: 269-290.
Schneider, K and Akkan, Z. (2004). Quantitative relationship between the local lymph node assay and human skin sensitization assays. Reg. Tox. Pharmacol. 39: 245-255.
Vandebriel RJ, De Jong WH, Hendriks JJA, Van Loveren H.( 2003) Impact of exposure duration by low molecular weight compounds on interferon-γ and interleukin-4 mRNA expression and production in the draining lymph nodes of mice. Toxicology 188, 1-13.
Vandebriel RJ, De Jong WH, Spiekstra SW, Van Dijk M, Fluitman A, Garssen J, Van Loveren (2000). Assessment of preferential T-helper 1 or T-helper 2 induction by low molecular weight compounds using the local lymph node assay in conjunction with RT-PCR and ELISA for interferon-G and inyterleukin-4. Toxicol Appl Pharmacol 162, 77-85.
Van Och FMM, Van Loveren H, De Jong WH, Vandebriel RJ (2002). Cytokine production induced by low molecular weight chemicals as a function of the stimulation index an a modified local lymph node assay: an approach to discrminate contact sensitizers from respiratory sensitizers. Toxicol Apll Pharmacol 184, 46-56.
Van Och FMM, Slob W, De Jong WH, Vandebriel RJ Van Loveren H (2000). A quantitative method for assessing the sensitizing potency of low molecular weight chemicals using a local lymph node assay: employment of a regression method that includes determination of the uncertainty margins. Toxicology 146, 49-59.
Vanoirbeek JAJ, Tarkowski M, Vanhooren HM, De Vooght V, Nemery B, Hoet PHM (2006). Validation of a mouse model of chemically induced asthma using trimellitic anhydride, a respiratory sensitizer, and dinitrochlorobenzene, a dermal sensitizer. J Allergy Clin Immunol 117, 1090-1097.
DR. KATHERINE SARLO
BIO
Dr. Katherine Sarlo joined The Procter & Gamble Company in 1985 and is a principal scientist in the Central Product Safety organization. Dr. Sarlo directs both internal and external pre-clinical and clinical research in the area of type 1 allergy and nanotoxicology. She is also responsible for developing approaches to risk assessment that incorporate exposure and outcome as it relates to allergy and to nanotoxicology. Dr. Sarlo received a BS in Biology at the State University of New York at StonyBrook in 1980. She received her Ph.D. in Microbiology and Immunology at Ohio State University in 1985.

RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
ABSTRACT Evaluation of Chemical Respiratory Allergy: An Industry View Katherine Sarlo, PhD The Procter & Gamble Company Having models to predict whether a new compound can cause immune mediated respiratory allergy is important so that the risk to populations exposed to these compounds can be minimized. Much can be learned about respiratory allergy by studying occupational cohorts. Among the tens of thousands of compounds used in a variety of workplaces only a few hundred have been described as causes of allergic occupational asthma. The majority of these compounds are high molecular weight materials such as proteins and only a handful of high and low molecular weight compounds are responsible for the majority of cases of allergic occupational asthma. The clinical experience indicates that those chemicals that induce respiratory allergy are distinct from chemicals shown to induce other forms of hypersensitivity such as contact dermatitis. If contact allergens can induce responses on the skin and in the airways and if respiratory allergens can do the same, then this should be apparent among humans exposed and symptomatic to these chemicals. Examples from industry (platinum workers, dye workers) indicate that this is not the case. Several laboratories are testing variations of a “modified” local lymph node assay (LLNA) to assess its potential for hazard identification of chemical respiratory allergens. The methods used to assess respiratory reactivity in the model have been subject to great controversy among pulmonary specialists, claiming that these endpoints are not indicative of experimental asthma or bronchoconstriction. In addition, measures of total IgE and possibly cytokine profiles may be too non-specific to correlate with bronchoconstriction. Whether any of these endpoints are predictive for specific immune respiratory allergic responses is open for debate. A measure of immunogenicity in the LLNA does not equate to a blanket classification of all chemicals as respiratory allergens. Work needs to be done to understand whether any aspect of the LLNA can be used to predict the potential of a chemical to function as a respiratory allergen. Measurements of specific immune reactivity in an animal model that are consistent with respiratory allergy and correlate with the clinical observations is needed. Validation of such methods across laboratories is key to demonstrate that the methods are robust and predictive.

RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
SUMMARY Evaluation of Chemical Respiratory Allergy: An Industry View Katherine Sarlo, PhD The Procter & Gamble Company Low molecular weight reactive chemicals, metals and drugs and larger sized molecules such as proteins
can cause respiratory allergy (hypersensitivity) in a portion of an exposed population. Respiratory allergy
can encompass hypersensitivity induced asthma including classic IgE allergic antibody mediated events
or the less common conditions such as allergic alveolitis and chronic beryllium disease. These diseases
are defined by an adaptive immune response since there is specificity and memory that result in damage
to the host. Workplace exposure to a variety of low and high molecular weight agents is a leading cause
of asthma among adults. Much can be learned about respiratory allergy by studying occupational cohorts
since work can be done to characterize the population exposed and the population at risk along with the
exposure(s) associated with expression of the disease. Among the tens of thousands of compounds used in
a variety of workplaces only a few hundred have been described as causes of allergic occupational
asthma. The majority of these compounds are high molecular weight materials such as proteins. Only a
handful of high and low molecular weight compounds are responsible for the majority of cases of allergic
occupational asthma. Recent surveys conducted in the UK show that isocyanates are the leading cause of
occupational asthma, followed by flours and grains and laboratory animals. A survey in France showed
that the leading causes were flours and grains, isocyanates and latex.
Having the ability to predict whether a chemical or high molecular weight compound can cause immune
mediated respiratory allergy is important so that the risk to populations exposed to these compounds can
be minimized. However, respiratory allergy and asthma is a complex disease where personal risk factors
(genetics, smoking status, atopy) in combination with environmental factors (exposure to agent, presence
of “adjuvants) plus the innate properties of the compound to function as an allergen must be “in synch” in
order to get the expression of the disease. For some chemicals such as platinum salts, reactive dyes and
acid anhydrides there is a clear role for chemical specific IgE antibody in the manifestation of respiratory
allergy. For certain other chemicals such as the isocyanates and plicatic acid, IgE antibody can only be
found in a small portion of effected individuals suggesting that other less understood mechanism(s) of
immune mediated respiratory allergy may be in play. This makes it difficult to develop predictive in
silico, in vitro and animal models for chemical induced immune mediated respiratory allergy.
The clinical experience shows that those chemicals that induce respiratory allergy are distinct from
chemicals shown to induce other forms of hypersensitivity such as contact dermatitis. With the exception
of isocyanates, it is rare to see clinically confirmed contact dermatitis among a population of workers
where respiratory allergy exists to the same chemical. Conversely, it is rare to see clinically confirmed
chemical respiratory allergy among a population of workers where contact dermatitis exists. In these
environments there are opportunities for both airway and skin exposures. Therefore, if contact allergens
can induce responses on the skin and in the airways and if respiratory allergens can do the same, then this
should be apparent among humans exposed and symptomatic to these chemicals. To illustrate, an
assessment of platinum salt exposed workers showed that 14% had occupational respiratory allergy and
asthma; 95% of the symptomatic workers that were skin prick test positive to the metal were patch test
negative. Only 1 worker (0.5%) had symptoms of eczema and was skin prick test positive and patch test
positive to platinum. In another example, only 0.3% of dye process workers (crush, mix, dry, transport)
had skin symptoms of urticaria and pruritis (no eczema) while 25% had respiratory symptoms. Nearly
one-third of the workers with respiratory symptoms had IgE antibody to several dyes (using dye-protein
conjugates as antigens). Such clinical follow-ups are important since they suggest that chemicals that
cause respiratory allergy are different from those that cause contact dermatitis.
Several investigators have been using rodents (mice, rats, guinea pigs) to investigate the immune response
to chemical allergens to identify appropriate immune endpoints that can be used in hazard and risk
assessment. A “modified” local lymph node assay (LLNA) is being tested by several laboratories as a
potential model for hazard identification of chemical respiratory allergens. Total IgE serum levels,
cytokine profile in lymph nodes from exposed animals and respiratory reactivity assessed in a whole body
plethysmograph with or without measures of air flow (Penh) have been proposed as a way to distinguish
chemical contact allergens from chemical respiratory allergens. Unfortunately, use of non-specific
measures of immunity such as total IgE levels and potentially cytokine profiles may not be appropriate for
the following reasons:
1. changes in total serum IgE can be driven by chemical toxicity (e.g., mercuric chloride) or by non-specific elevation of cytokines such as IL-18,
2. interlaboratory assessment of total IgE levels from Balb/c mice treated with standard TMA or DNCB reagents showed lab to lab variability and differences in basal IgE levels in mice obtained in the UK and in the US,
3. changes in cytokine profiles vary based on the protocol used; differences in time of assessment and stimulation of cells (e.g., antigen vs. mitogen) may impact the profile,
4. different laboratories have reported different results for total IgE and cytokine profiles using the classic contact allergen DNCB; this may be related to choice of species and strain and small differences in protocol,
5. the human response to allergens is heterogenous involving CD4+ and CD8+ cells and a mix of Th2 and Th1 cytokines; the rodent response is predominantly Th2, illustrating the complexity of the response in man.

In addition, several laboratories have reported poor correlations among total IgE levels, cytokine profile
and airway reactivity measured as changes in breathing pattern or Penh. The methods used to assess
respiratory reactivity in these rodent models have been subject to great controversy among pulmonary
specialists, claiming that these endpoints are not indicative of experimental asthma or
bronchoconstriction. Likewise, measures of total IgE and cytokine profiles may be too non-specific to
correlate with respiratory allergy. Whether any of these endpoints are predictive for specific immune
respiratory allergic responses is open for debate.
Observations and measurements made from the clinical experience should drive the development of
predictive models for chemical induced respiratory allergy. It is clear from the clinical experience that
those chemicals that cause respiratory allergy are distinct from chemicals that cause contact dermatitis.
While one would expect that chemicals that cause both contact dermatitis and respiratory allergy could be
positive in the LLNA (as long as they penetrate thru the skin), a measure of immunogenicity does not
equate to a blanket classification of all chemicals as respiratory allergens. Following this path would lead
to a greater use of animals to understand if the chemical is truly a respiratory allergen and can lead to
unintended disruption in manufacturing with increase in costs and medical monitoring when this is not
warranted. Additional work must be done to understand whether any aspect of the LLNA can be used to
predict the potential of a chemical to function as a respiratory allergen. Measurements of specific immune
reactivity in an animal model that are consistent with respiratory allergy and correlate with the clinical
observations is needed.Validation of such methods across laboratories is key to demonstrate that the
methods are robust and predictive.
Selected References: McDonald, J.C., Keynes, H.L., and Meredith, S.K., Reported incidence of occupational asthma in the United Kingdom, 1989-97, Occup. Environ. Med., 57, 823, 2000.
Van Kampen, V., Merget, R., and Baur, X. Occupational airway sensitizers: an overview of the respective literature, Am. J. Ind. Med., 38, 164, 20002.
Ameille, J., Pauli, G., Calastreng-Crinquand, A., Vervloet, D., Iwatsubo, Y., Popin, E., Bayeux-Dunglas, M.C., Kopferschmitt-Kubler, M.C. Reported incidence of occupational asthma in France, 1996-1999: the ONAP program. Occup. Environ. Med., 60, 136, 2003.
Cristaudo, A., Sera, F., Severino, V., De Rocco, M., Di Lella, E., Picardo, M., Occupational hypersensitivity to metal salts, including platinum in the secondary industry, Allergy, 60, 159, 2005.
Park, H.S., Lee, M.K., Kim, B.O., Lee, K.J., Roh, J.H., Moon, Y.H., Hong, C. Clinical and immunological evaluations of reactive-dye exposed workers, J Allergy Clin Immunol, 87, 639, 1991.

Dr. David Basketter BSc, DSc, FIBiol, FRCPath, Eurotox Registered Toxicologist BIO
Dr Basketter originates from Manchester, UK and attended London University where he graduated in Physiology in 1973 and later earned a DSc in 1997. He was admitted to fellowship of the Institute of Biology in 1998 and made a Fellow of the Royal College of Pathology in 2004. In 1979, Dr. Basketter moved to the Unilever Laboratory in Sharnbrook, UK. Here, Dr Basketter’s toxicology career developed, focusing on allergy and irritation. Dr Basketter is a Eurotox Registered Toxicologist and is currently Senior Scientist in the Unilever Safety and Environmental Assurance Centre with responsibility for allergy and irritation. He also holds the position of Senior Lecturer in the Dept of Dermatology of Guy’s, Kings and St Thomas Hospital School of Medicine in London, UK. His particular interests/responsibilities include the development of non-animal methods for the identification and assessment of irritants and allergens, and the establishment of safe exposure limits for both skin and respiratory allergens. His research activities in this general area have resulted in over 300 publications. Dr Basketter chairs several committees on irritation/sensitisation topics, and is, or has been, a member of EU/OECD/WHO expert groups on this subject, including those involved with development of in vitro alternatives. He is toxicology/risk assessment section editor of the journal Contact Dermatitis and is a past president of the European Society of Contact Dermatitis.

RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
ABSTRACT Hazard identification, characterisation and the assessment of respiratory sensitisation risk for consumer products David A Basketter Safety and Environmental Assurance Centre, Unilever, Bedfordshire, UK
Sensitisation of the respiratory tract, a type of immediate hypersensitivity mediated by IgE, is a serious health endpoint, having the potential lead to bronchoconstriction, asthma and consequently even death. A limited set of chemicals, often from specific groups (eg isocyanates, acid anhydrides) has been associated with this endpoint, but to date, no prescribed method for the predictive identification of chemicals with this property exists. Additionally, where such chemicals have been identified, by whatever means, their fuller characterisation and risk assessment presents a challenge. In practice, chemical respiratory sensitisation is managed by a combination of hazard identification in standard skin sensitisation assays and where appropriate, further analysis, eg by cytokine fingerprinting. This is followed by an assessment of the extent of exposure of the respiratory tract and comparison of that exposure with known benchmarks. These benchmarks normally will be drawn from clinically well known occupational chemical respiratory sensitisers, for which occupational airborne limits have been established and proven to be of practical value in the elimination of clinical risk. In the present work, these matters are discussed and practical examples given of hazard identification, characterisation and risk assessment.

Marcel T.M. van Raaij, Ph.D.
Bio
Marcel van Raaij is a project leader for the Center of Substances and Risk Assessment at the National Institute of Public Health and Environment (RIVM) in the Netherlands. He joined RIVM in 1994 where he worked on the combination effects of environmental stressors such as noise and inhalation toxicity on the hormonal- and immune system. In 1997, he began his work on toxicological risk assessments of pesticides and biocides. In addition, he worked on the setting and use of intervention values for chemical incidents, the use of uncertainty factors in risk assessment, methodological issues, and exposure scenarios for chemicals in consumer products. He was/is responsible for projects, e.g. on cumulative and chemical risk assessment, and scientific aspects of risk assessment during acute exposures.
In 2003, Dr. van Raaij was appointed head of the department ‘Toxicology and Risk Assessment’ of the Center of Substances and Integrated Risk Assessment. This department focuses on risk assessments and methodological developments for many chemical frameworks (pesticides, biocides, industrial chemicals, food additives, cosmetics, veterinary products and others). Before working at RIVM, he was appointed as assistant investigator in the department of Animal Physiology of the University of Leiden. His research focuses on the hormonal regulation of metabolic processes.
Dr. Van Raaij did his basic training in medical biology at the State University of Leiden in the Netherlands. He received his Ph.D. in 1994.
RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
ABSTRACT Risk assessment aspects of respiratory sensitization Dr. Marcel T.M. van Raaij Center of Substances and Integrated Risk Assessment (SIR), National Institute of Public Health and Environment (RIVM), Bilthoven, The Netherlands In cosmetic products a wide range of fragrance chemicals are being used. A range of fragrance chemicals have been shown to possess sensitizing properties when in contact with the skin. Within the EU a list of 26 fragrance chemicals has been formulated to have skin sensitization properties. Most of the scientific basis was provided by human patch testing.
In addition to the use of cosmetics, these fragrance chemicals are also used in a rnage of scented products. Scented products are compiled of a broad variety of product types including passive room perfumes, sprays, fragrance candles, ethereal oils, iron and vacuum cleaner perfumes, and even toys. In recent years a substantial increase in the use of scented products has been noted. Scented products are now being used widely in homes (living rooms, toilets), offices, shopping centres, and even in cars. There seems to be a tendency towards increased spreading of fragrance materials leading to potential inhalation exposures over the day. The Dutch Food and Non Food authority (VWA) has requested RIVM to evaluate this increased use of scented products because concern exists whether this may lead to an increased risk for respiratory sensitization. In addition, RIVM was requested to investigate the possibility to design a methodology to assess the safety of scented products.
In 2005, RIVM has produced a report on the use of scented products in which an inventory of products and uses was made. Special consideration was given to categorization of product types and (default) exposure scenarios for these product types. Although there is a lack of data on exposure to fragrance materials, it appeared possible to propose exposure scenarios for input in consumer exposure models such ConsExpo (www.rivm.nl/consexpo).
The toxicological endpoint of sensitization, however, is problematic to handle in risk assessment. For reasons of transparency, a quantitative approach is preferred when designing a methodology for assessing the safety of scented products. For skin sensitization, some proposals have been published for a quantitative risk assessment. However, these approaches are still under scientific development. For respiratory sensitization the situation is more complex. At present, no harmonized test systems are available and discussion exists on the specific endpoints to use in testing of respiratory sensitization.
From a general risk assessment view, the following questions can be posed. Why would a chemical that is able to induce sensitization by skin contact not be able to induce sensitization by inhalation exposure? Is it only a matter of dose? Is there a qualitative or quantitative difference between exposure of the immune system through the dermal or inhalation routes? Is there a relation between the potency of a substance to induce skin sensitization and its potency to induce respiratory sensitization? If so, can dermal tests be used to assess the potency of substances for inhalation thereby avoiding extensive animal testing by inhalation exposure and filling the gap of data on this subject? From the perspective of public health prevention, what effects should be preventing to occur?
Because of all of these questions, and the interest of Dutch policy in this matter, RIVM was requested to perform some pilot experiments on the issue of respiratory sensitization. See the contribution of Rob Vandebriel for further information on this subject.
Dr. Helen McGarry
BIO
Dr. Helen McGarry is a regulatory toxicologist at the Health and Safety Executive (HSE) in the UK.
Since joining the HSE, Dr. McGarry has become the UK’s competent authority representative on the
REACH Implementation Project (RIP) endpoint working group for skin and respiratory sensitization,
which is charged with producing guidance for the industry on meeting the information requirements under
REACH.
Dr. McGarry studied pharmacy at the University of Manchester and after which she worked in
community pharmacy for a short while. She then completed an MSc and a PhD in tropical medicine at the
University of Liverpool, followed by several years of postdoctoral research at the Liverpool School of
Tropical Medicine.
Dr. McGarry is also currently part of the planning group for a World Health Organization workshop
entitled ‘Skin Sensitization in Chemical Risk Assessment’, to be held in October 2006.

RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
ABSTRACT Chemical Respiratory Hypersensitivity: UK Regulatory Perspectives Dr Helen McGarry, Regulatory Scientist, Health and Safety Executive Occupational asthma is the major cause of work-related respiratory ill health in the UK. The recognition
of this fact, combined with the seriousness of the disease, led in the 1990s to an increased regulatory drive
within the UK to try to improve the control of chemicals that cause asthma at work. One important
activity was the development within the EU of revised criteria for the classification of substances as
respiratory sensitizers (R42). In refining these criteria, many areas of uncertainty had to be addressed, not
least the terminology used to define respiratory hypersensitivity and respiratory sensitizers. Another such
area was the toxicological mechanisms that underlie the disease state, particularly the involvement or
otherwise of the immune system. Additionally, the reported ability of dermal exposure to induce
sensitization of the respiratory tract had to be considered. The adopted regulatory approach focuses on the
occurrence of the disease, not on the underlying mechanism, and in making a classification decision, a
balanced view of all available information is taken (which is usually human evidence). Animal tests may
be used as screens but, currently, they have only a limited regulatory use. An emerging issue is the
suggestion that low molecular weight chemicals that test positive in animal predictive tests for skin
sensitization also have the potential to be respiratory allergens. Thus it is clear that, although it is ten
years since the EU criteria for classification and labelling of respiratory sensitizers were agreed, there are
still significant areas of uncertainty that have yet to be resolved.
RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
SUMMARY Chemical Respiratory Hypersensitivity: UK Regulatory Perspectives Dr Helen McGarry, Regulatory Scientist, Health and Safety Executive Occupational asthma is the major cause of work-related respiratory ill health in the UK [1]. The
recognition of this fact, combined with the seriousness of the disease, led in the 1990s to an increased
regulatory drive within the UK to try to improve the control of chemicals that cause asthma at work. One
consequence of this was the publication of a compendium of critical appraisals of agents implicated in
occupational asthma [2]. Another important activity was the development within the EU of revised
criteria for the classification of substances as respiratory sensitizers, since the existing criteria were not
detailed enough to deal with complex databases, and required that (unless the chemical under
consideration was an isocyanate) there was evidence that the substance or preparation was ‘capable of
inducing a sensitization reaction in humans by inhalation.’ In revising the criteria, many areas of
uncertainty had to be addressed, not least the terminology used to define respiratory hypersensitivity and
respiratory sensitizers. Another such area was the toxicological mechanisms that underlie the disease
state, particularly the involvement or otherwise of the immune system. Additionally, some issues of
exposure, such as the reported ability of dermal exposure to induce sensitization of the respiratory tract
and the relevance of peak exposures, had to be considered.
The Health and Safety Executive (HSE) took the approach of concentrating on the induction phase of
sensitization, which was defined as the process of rendering the airways unusually sensitive
(hypersensitive) such that, following subsequent inhalation exposure, a response may be elicited that is
associated with the classical symptoms of an asthmatic reaction [2]. However, because it is not always
possible to define the mechanism of such induction, the involvement of the immune system did not have
to be demonstrated. For this reason, the term ‘respiratory hypersensitivity’ was preferred to ones such as
‘respiratory sensitization’ or ‘respiratory allergy’, and the term ‘asthmagen’ was coined to encompass all
agents that induce asthma-like symptoms, including those for which non-immunological mechanisms
appear to be involved. Two such mechanism are reactive airways dysfunction syndrome (RADS) [3,4]
and repeated low-level irritation, both of which have been associated with occupational asthma [5-7].
Therefore, the adopted regulatory approach focuses on the occurrence of the disease, not on the
underlying mechanism, and in making a classification decision, a balanced view of all available
information is taken. Unfortunately, this, currently, is usually human evidence following occupational
exposure. Animal tests may be used as screens, and the HSE has actively encouraged the development of
such tests. However, at the moment this approach has only a limited regulatory use, with positive results
being acceptable as ‘weight-of-evidence’, but negatives not being considered in making a classification
decision. In the absence of such tests, an emerging, controversial issue is the suggestion that low
molecular weight chemicals that test positive in animal predictive tests for skin sensitization should also
be classified as respiratory allergens. Since around 33% of substances notified to the HSE under the
Notification of New Substances regulations are positive in the murine local lymph node assay [8], the
adoption of this approach would have a huge regulatory and socio-economic impact. A more generally
accepted view is that dermal exposure to some respiratory allergens can induce respiratory
hypersensitivity, mainly demonstrated in animals [9,10], although the regulatory view is that further
evidence for its relevance to humans is required before this route of exposure can be considered for
hazard identification.
The evaluation of data relating to human evidence for a substance being a respiratory allergen also raises
uncertainties. For example, clinical investigations are often aimed at the diagnosis of asthma in a single
patient, and there is no particular need to unequivocally identify the inducing agent. There is also often a
lack of exposure data for the suspected agent and for previous and/or concurrent exposures to other
chemicals. The quality of key tests needs to be carefully assessed, particularly the bronchial challenge test
in terms of whether or not the test was conducted blinded; if a control substance was included; if control
(non-asthmatic/asthmatic) subjects were tested; and if confounding factors were controlled.
Unfortunately, few tests meet all these criteria, so in making a classification decision, the regulatory
approach is to take a balanced view of all the available information.
In revising the EU classification criteria, the aim was, in addition to trying to address some of the above-
mentioned uncertainties, to make the assignment of the classification phrase ‘May cause sensitisation by
inhalation’ (R42) more consistent, transparent and scientifically-based. The new classification criteria,
which were adopted by EU Member States in 1996, were as follows:
1. If there is evidence that the substance or preparation can induce specific respiratory
hypersensitivity; or
2. where there are positive results from appropriate animal tests; or
3. if the substance is an isocyanate, unless there is evidence that the substance does not cause
respiratory hypersensitivity.
Guidance on the nature of the human evidence required is provided, which, if based on exposure, should
take into consideration the size of the population exposed and the extent of exposure. There is a statement
that ‘immunological mechanisms do not have to be demonstrated’, with two examples of non-
immunological mechanisms of action being given as repeated low-level irritation and pharmacologically-
mediated effects; the former is different from the irritation that may lead to the classification of ‘Irritating
to respiratory system’ (R37), which is ‘reversible and usually limited to the upper airways’.
Risk assessment often raises further uncertainties. For example, the data available for identifying
respiratory allergens are generally not sufficient to set occupational exposure limits, and, in the absence of
a suitable test method, it is not possible to define no-observed-adverse-effect-levels for new substances. It
is also not clear which groups of workers the limits should protect. For example, should an occupational
exposure limit for a reactive chemical protect particularly susceptible individuals, such as those with
mild/unrecognised asthma, and if not, would screening for bronchial hyper-reactivity be advisable before
exposure?
Thus it is clear that, although it is ten years since the EU criteria for classification and labelling of
respiratory sensitizers were produced, there are still areas of uncertainty that have yet to be resolved.
Additionally, it is probable that any future revisions to the classification and labelling criteria will take
place in the context of the Global Harmonisation Scheme and not just within the EU.
References 1. Ross D.J., Sallie B.A., McDonald J.C. SWORD '94: surveillance of work-related and occupational
respiratory disease in the UK. Occupational Medicine 1995; 45: 175-8.
2. Health and Safety Executive. Asthmagen? Critical assessments of the evidence for agents implicated in occupational asthma. Sudbury, Suffolk, U.K.: HSE Books, 1997.
3. Brooks S.M., Weiss M.A., Bernstein I.L. Reactive airways dysfunction syndrome (RADS). Persistent asthma syndrome after high level irritant exposures. Chest 1985; 88: 376-84.
4. Brooks S.M., Weiss M.A., Bernstein I.L. Reactive airways dysfunction syndrome. Case reports of persistent airways hyperreactivity following high-level irritant exposures. Journal of Occupational Medicine 1985; 27: 473-6.
5. Kipen H.M., Blume R., Hutt D. Asthma experience in an occupational and environmental medicine clinic. Low-dose reactive airways dysfunction syndrome. Journal of Occupational Medicine 1994; 36: 1133-7.
6. Leroyer C., Perfetti L., Cartier A., Malo J.L. Can reactive airways dysfunction syndrome (RADS) transform into occupational asthma due to "sensitisation" to isocyanates? Thorax 1998; 53: 152-3.
7. Gautrin D., Leroyer C., Infante-Rivard C., Ghezzo H., Dufour J.G., Girard D., Malo J.L. Longitudinal assessment of airway caliber and responsiveness in workers exposed to chlorine. American Journal of Respiratory and Critical Care Medicine 1999; 160: 1232-7.
8. Cockshott A., Evans P., Ryan C.A., Gerberick G.F., Betts C.J., Dearman R.J., Kimber I., Basketter D.A. The local lymph node assay in practice: a current regulatory perspective. Human and Experimental Toxicology 2006; in press.
9. Kimber I., Dearman R.J. Chemical respiratory allergy: role of IgE antibody and relevance of route of exposure. Toxicology 2002; 27: 311-5.
10. Scheerens H., Buckley T.L., Muis T.L., Garssen J., Dormans J., Nijkamp F.P., Van Loveren H. Long-term topical exposure to toluene diisocyanate in mice leads to antibody production and in vivo airway hyperresponsiveness three hours after intranasal challenge. American Journal of Respiratory and Critical Care Medicine 1999; 159: 1074-80.
RIFM Chemical Respiratory Allergy Workshop, London: July 13-14 2006
Glenn Sipes, Ph.D.
BIO
Dr. I. Glenn Sipes is Professor and Head of the Department of Pharmacology, College of Medicine at the University of Arizona. He is also Professor of Pharmacology and Toxicology and Anesthesiology. For 19 years he served as Head of the Department of Pharmacology and Toxicology in the College of Pharmacy and was the founding Director of the Center for Toxicology. As an academic scientist, Dr. Sipes has trained 32 MS and 26 PhD students and mentored 25 postdoctoral fellows.
Dr. Sipes earned a B.S. in Pharmacy from the University of Cincinnati (1965) and the Ph.D. in Pharmacology from the University of Pittsburgh (1969). After three years as a staff fellow at NIH, with Drs. B. Brodie and J. Gillette, he joined the faculty at the University of Arizona as an assistant professor in 1973. He developed a research program with emphasis on the biotransformation of drugs and environmental chemicals and on mechanisms of chemical-induced liver and ovarian injury.
Dr. Sipes is active in the Society of Toxicology (SOT) having served as a Councilor, Secretary, Vice President and President. Other professional activities include serving as a Councilor for the International Society for the Study of Xenobiotics; as a Councilor and as Chair of the Pharmaceutical Sciences section for the American Association for the Advancement of Science, of which he is also a Fellow; as a member of the NAS/NRC Committee of Toxicology and Board of Environmental Studies and Toxicology and as Chairperson of the NIH Toxicology Study Section. He is a member of the National Advisory Environmental Health Sciences Council. He was a Burroughs Wellcome Toxicology Scholar from 1985-1990 and was elected a Fellow of the Academy of Toxicological Sciences. From 1998-2004, Dr. Sipes served as President of the International Union of Toxicology and after that as Past President. He is a technical advisor (currently chair) to the Joint Expert Committee on Food Additives for the United Nations/WHO and a member of Research Institute for Fragrance Material’s Expert Panel. In addition he has served as a consultant and/or on advisory committees for several pharmaceutical and chemical companies.
Dr. Sipes served as Editor of Toxicology and Applied Pharmacology, an official journal of the SOT for seven years and was an associate editor of Life Sciences and on the editorial boards of Quality Assurance and Annual Review of Pharmacology and Toxicology, and Molecular Interventions. He served as Editor-in-Chief of the 13 volume series entitled, Comprehensive Toxicology. Dr. Sipes is the author of over 200 research publications and several review articles and book chapters.