chemonucleolysis for relief of sciatica due to a herniated
TRANSCRIPT

31. BONEN A, GARDNER J, PRIMROSE J, QUIGLEY R, SMITH D:An evaluation of the Canadian Home Fitness Test. Can JAppi Sport Sci 1977; 2: 133-136
32. ASTRAND I: Aerobic work capacity in men and womenwith special reference to age. Acta Physiol Scand 1960:49 (suppl 169): 1-92
33. JETT. M, CAMPBELL J, MONGEON J, ROUTHIER R: TheCanadian Home Fitness Test as a predictor of aerobiccapacity. Can Med Assoc J 1976; 114: 680-682
34. JETT. M: A comparison between predicted V02 max fromthe Astrand procedure and the Canadian Home FitnessTest. Can J Appi Sport Sci 1979; 4: 214-218
35. JErr. M, MONGEON J: A comparison between the effectsof a twelve-week programme of rope skipping and awalk/jog programme in males and females. Ibid: 268-273
36. SHEPHARD RJ, Cox M, COREY P, SMYTH R: Some factorsaffecting accuracy of Canadian Home Fitness Test scores.ibid: 205-209
37. COTTON FS, DILL DB: On the relation between the heartrate during exercise and that of the immediate post-exer-cise period. Am I Physiol 1935; 111: 554-556
38. DUNCAN WR, Ross WD, BANISTER EW: Heart rate mon-itoring as a guide to the intensity of an exercise pro-gramme. BC Med 1 1968; 10: 219-220
39. JETT. M: The Canadian Home Fitness Test as a Predictorof Maximal Oxygen Consumption. Report to RecreationCanada, Dept of National Health and Welfare, Ottawa,1975
40. BAILEY DA, MIRWALD RL: A Children's Test of Fitness.Report to Action British Columbia, Ministry of Health,British Columbia, Victoria, June 1975
41. THACKER J: A Project to Study the Relationship Betit'een
Questions A bout Physical Activity and Fitness Levels ciithe Canadian Home Fitness Test, MSc thesis, Temple U,Philadelphia, 1977
42. Standard Test of Occupational Fitness, Dept of NationalHealth and Welfare, Ottawa, 1979
43. Publi-Media, Inc.: The Canadian Home Fitness Test -Test Market Report to Recreatioti Canada, Dept of Na-tional Health and Welfare, Ottawa, 1975
44. LAUZON RRJ: The Canadian Home Fitness Test in thehealth environment. In SHEPHARD Ri, LAVALLfr H (eds):Physical Fitness A ssessment: Principles, Practice and A p-plication, CC Thomas, Springfield, Ill, 1978: 329-334
45. WILsoN JLG, JUNGNER G: The Principles and Practice ofScreening for Disease (Public Health Papers no 34), WorldHealth Organization, Geneva, 1968
46. SHEPHARD RJ, Cox M, SIMPNER K: Step test predictionsof maximum oxygen intake after an employee fitness pro-gramme. Can J A pp1 Sport Sci (in press)
47. M.ssw JF, SHEPHARD RJ: Physiological and psychologicaleffects of training. A comparison of individual and gymna-sium programs, with a characterization of the exercise"drop-out". Med Sci Sports 1971; 3: 110-117
48. SIDNEY KH, SHEPHARD RJ: Attitudes towards health andphysical activity in the elderly. Effects of a physical train-ing program. Med Sci Sports 1976; 8: 246-252
49. MEYER AJ, HENDERSON JB: Multiple risk factor reductionin the prevention of cardiovascular disease. Prei' Me.l1974; 3: 225-236
50. JACKSON ii: Diffusion of an innovation: Au ExploratoryStudy of the Consequences of Sport Participaction. Can-ada's Campaign at Saskatoon, 197 1-1974, PhD thesis,U of Alberta, Edmonton, 1975
Chemonucleolysis for relief of sciaticadue to a herniated intervertebral disc
JOHN A. MCCULLOCH,* MD, FRCS[C]
Chemonucleolysis is the nonoperative chemical removal ofdisplaced lumbar disc material. The enzyme chymopapain,which has a wide margin of safety between its effectivetherapeutic and toxic doses, is effective in the managementof sciatica due to a herniated intervertebral- disc. The pa-tient will have leg pain as the dominant symptom and a 500/creduction in straight-leg raising with or without bowstringdiscomfort and crossover pain. Neurologic symptoms andsigns are usual, as are abnormal results of contrast studies,which will verify the level of involvement.
In 220 randomly selected patients who met criteria forthe diagnosis of sciatica due to a herniated intervertebraldisc and did not have psychogenic or nonorganic spinalpain, a spinal stenosis or a history of a previous, unsuccess-ful operation to relieve the sciatica, chemonucleolysis hada success rate of 800/0. The only complications were asevere anaphylactic reaction in two patients and lesser,delayed reactions in five others. All of the reactions weresuccessfully treated. Of the 45 patients in whom chemonu-cleolysis was unsuccessful, 38 underwent a laminectomy. In3 of the 38 the results of chemonucleolysis were initiallygood, but later the disc herniation recurred; thus, the long.term treatment failure rate was 1.40/c.
Assistant professor, departments of surgery and anatomy,University of TorontoReprint requests to: Dr. John A. McCulloch, CommerceCourt East, Box 37, Toronto, Ont. M5L IAI
La chimionucleolyse est l'extraction chimique non sanglanted'un disque lombaire deplace. L'enzyme utilise, Ia chymo-papaine, possede un large index therapeutique entre sa dosetherapeutique efficace et sa dose toxique, et elle est eff I-cace dans le traitement de Ia sciatique due A un disqueintervertebral herni6. Le patient presente comme symptAmesdominants des douleurs dans Ia jambe et une diminution de5O0/o de I'elevation de Ia jambe tendue du c8te douloureux,avec ou sans malaise en lacet ou douleur croisee. LessymptAmes et signes neurologiques sont courants, de mAineque les resultats anormaux des etudes radiologiques avecsubstance de contraste, qui sert a verifier le niveau delatteinte.Chez 220 patients choisis au hasard parmi ceux qul ren-
contraient les critAres diagnostiques d'une sciatique due Aun disque intervertAbral hernie, et qui n'avaient pas dedouleur spinale psychogene ou non organique, de st6nosespinale ou une histoire d'operation infructueuse pour lesoulagement de Ia sciatique, Ia chimionucleolyse a obtenuun taux de succes de 800/0. Les seules complications oh-servees ont ete une reaction anaphylactique grave chezdeux patients et des reactions retardees moms importanteschez cinq autres. Ces reactions furent traitees avec succes.Parmi les 45 patients chez qui Ia chimionucleolyse n'a pasreussi, 38 ont subi une laminectomie. Chez 3 des 38 lesr6sultats 6taient bons au dAbut, mais plus tard il y a eurecidive de Ia hernie discale. Donc, le taux dechec a longueecheance etait de 1.40/o.
CMA JOURNAL/APRIL 1, 1981/VOL. 124 879
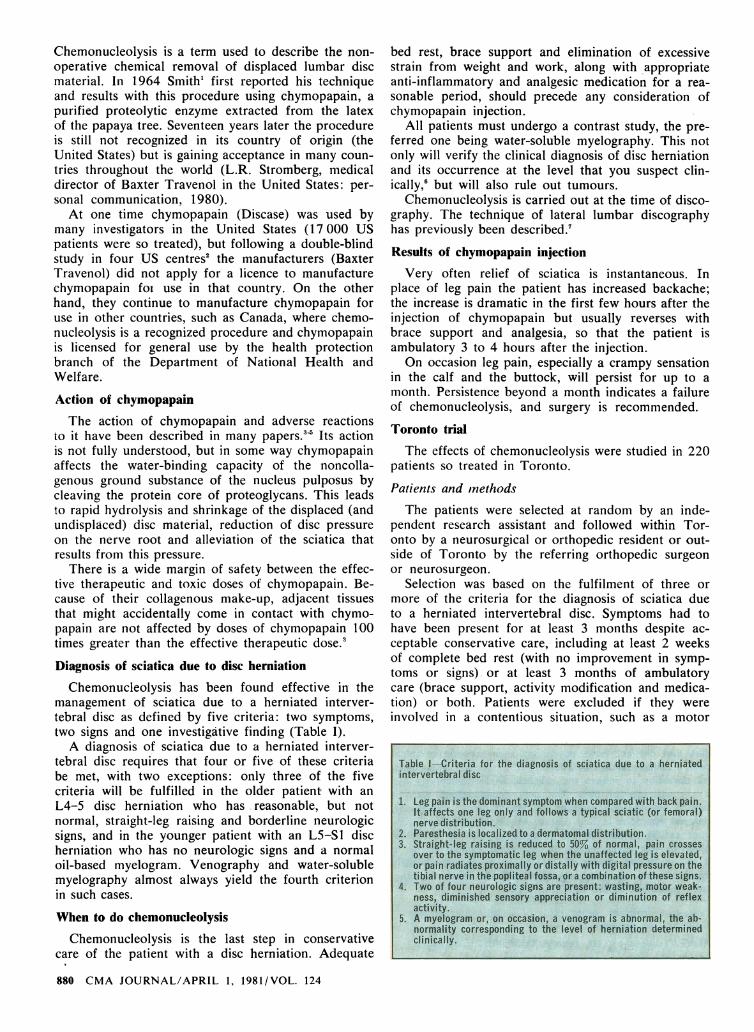
Table I-Criteria for the diagnosis of sciatica due to a herniatedintervertebral disc
I. Leg pain is the dominant symptom when cornpared with back pain.It affects one leg only and follows a typical sciatic (or femoral)nerve distribution.
2. Paresthesia Is localized to a dermatomaidistribution.3. Straight-leg raising is reduced to 50% of normal, pain crosses
over to the symptomatic leg when the unaffected leg is elevated,or pain radiates proximally or distally with digital pressure on thetibial nerve in the popflteal fosa, ova combination oftheseslgns.
4. Two of four neurologic signs are present: wasting, motor weak-ness, diminished sensory appreciation or diminution of reflexactivity.
5. A myelogram or, on occasion, a venogram is abnormal, the ab-normality corresponding to the level of herniation determinedclinically.

vehicle accident or compensation claim, had psycho-genic or nonorganic spinal pain or a spinal stenosis,or had previously undergone an unsuccessful operationto relieve the sciatica. Finally, only those who had asingle-disc herniation were selected for follow-up.On this basis 248 patients were selected at random,
with the assumption that this number would provideat least 200 patients for follow-up. In fact, only 28patients were not followed up, the reasons being dis-tance (for 7), refusal (for 8), unrelated death (for 1)and our inability to find them (for 12).The average age of the patients was 38 years, and
females formed 38% of the group. The average dura-tion of sciatica was 9.5 months, and the average timefrom injection to end of follow-up was 3.3 years(minimum 6 months, maximum 9 years). Three criteriawere fulfilled by 10% of the patients, four by 43%and five by 47%. Almost every patient had leg painas the dominant symptom, more than 65 % had neuro-logic signs only, and slightly more than 50% hadneurologic symptoms; 94% had either neurologic signsor a marked reduction in straight-leg raising. The con-trast study, showed an abnormality in 94% of thepatients.
Results
Chemonucleolysis was graded as either a success ora failure. Patients with a successful procedure werevirtually free of pain I month after the injection andwere functioning at a normal level in occupational andleisure activities. In those with continuing residualback or leg pain that interfered with a normal patternof living or required medication the procedure wasclassified as a failure.
The average stay in hospital was 4.5 days, and 50%of the patients returned to full work within 50 days.While 85% of the patients considered their chemonu-cleolysis a success, 93% of the entire group statedthat if the circumstances that prompted their consulta-tion arose again they would opt for chemonucleolysis.
The examiners felt that only 80% of the patientshad a successful result (Table II), and within thatgroup 22 patients had minor residual symptoms thatdid not require medication or medical attention andonly slight modification of activity. A more criticalobserver, however, would classify the results in thesepatients as failures. Of the 45 patients with a clearly
unsuccessful result, 38 underwent a laminectomy, usu-ally immediately after chemonucleolysis; 50% werefound to have a sequestered disc, 25 % lateral recessstenosis and 25 % a variety of problems, such as amildly bulging disc or mechanical back pain. Three ofthe 38 patients initially had a good result with chemo-nucleolysis but later required surgery because the discherniation recurred.
Complications
Of the 220 patients 2 had a severe anaphylactic re-action and 5 had a delayed reaction, usually a rash.The seven reactions (which yield a short-term com-plication rate of 3.2%) were successfully managedand there were no long-term effects. No other com-plications occurred at the time of injection. In thosewho underwent surgery no adverse effects of thechymopapain injection were noted.
Discussion
As the last step in conservative care, chemonucleol-ysis has a role to play in the management of sciaticadue to a herniated intervertebral disc. Using the diag-nostic criteria outlined in Table I we can expect ex-cellent results in about 80% of patients, a figurethat compares favourably with the success rate re-ported from any study of surgical intervention for thesame problem.8 In addition, the short-term complica-tion rate of 3.2% in this series compares favourablywith that of any reported series of laminectomy/dis-cectomy procedures.8 Long-term permanent complica-tions were absent from this series, and in this respectthe results were better than those of any reportedsurgical series.8My previous experience with chymopapain in treat-
ing a broad spectrum of back disabilities, as describedin l977,. had defined the type of patient who respondsto this method of treatment. For example, it had sug-gested that chemonucleolysis is best reserved for thesingle-disc herniation; hence, only patients with such aherniation were selected for follow-up in this study.Equally important was the exclusion of patients thatwere in contentious situations, had psychogenic ornonorganic spinal pain or a spinal stenosis, or hadpreviously undergone an unsuccessful operation torelieve the sciatica. Thus, the success rate of 80%in this series of carefully selected candidates representsa rate in "ideal" patients. Obviously, on occasion apatient with less than ideal indications will be selectedfor chemonucleolysis, but less than ideal results willensue.
The mechanism of action of chymopapain is notclearly understood. This enzyme is thought to inter-fere with the water-binding capacity of noncollagenousground substance in the nucleus pulposus. How thisaffects the pain of sciatica is not clear, and the drama-tic relief of leg pain that so often occurs immediatelyafter the injection remains an enigma.
Initially needle placement is difficult, but after treat-ing 50 to 100 patients one can achieve the skill neces-sary to do this procedure most effectively. It is im-portant that the tip of the needle be observed between
CMA JOURNAL/APRIL 1, 1981/VOL. 124 881

the inside edges of the pedicles on an anteroposteriorroentgenogram and in the centre of the disc on alateral film. Equally important is the use of very smallamounts of contrast material to verify the position ofthe needle tip and to allow for injection of chymo-papain into a relatively "clear" disc space. Adequateamounts (2 ml or 4000 U) of chymopapain need tobe injected into each disc space. Leakage of the en-zyme into the extradural space has not concerned me,and the findings at subsequent laminectomy whenchemonucleolysis has failed have supported this posi-tion.
Chemonucleolysis is considered a failure if the pa-tient has continuing leg pain 1 month after the injec-tion of chymopapain. It is common for the patientto have continuing back pain at this stage, but in mostpatients this pain subsides over the ensuing weeks ormonths to the point where it is negligible, and by thistime there is virtually no leg pain either.
It is my impression that the long-term result withthis procedure will be superior to that with laminec-tomy because of the absence of dissection of any ofthe very important midline ligamentous structures andthe absence of opening of the extradural space andconsequent entry of blood into it, which are naturalaspects of the operation. Of the patients undergoingsurgery during the follow-up period, three had a re-currence of disc herniation; this represents a long-term treatment failure rate of 1.4%. Again, this fig-ure compares favourably with those reported fromlong-term follow-up studies of laminectomy/discec-tomy.8No article about chymopapain would be complete
without discussion of the double-blind study done inthe United States.2 That work ultimately led to aban-donment of the technique in that country. The studycan be criticized on a number of grounds. The pa-tients were few (104) and were spread over fourcentres, and a substantial proportion were veterans,which concentrated the study in a segment of societythat was not representative of the general population.Further, the diagnostic criteria used to select patientsfor chymopapain injection were far less stringent thanthose used in this study. Most important, the US studywas not truly double-blind, because the placebo solu-tion contained enzyme activators. In spite of theseshortcomings the double-blind study is still seen asthe most scientific paper published on chemonucleol-ysis. It can be verified or invalidated only by anotherdouble-blind study. Such a study is currently underway in Australia (R. Fraser, Flinders Medical Centre,Bedford Park, South Australia: personal communica-tion, 1980).
Conclusion
The relief of sciatica due to a herniated interver-tebral disc by a simple, safe, nonsurgical procedurerequiring a brief hospital stay should represent a majoradvance to all those concerned with delivering andfinancing medical care. Instead chemonucleolysis re-mains controversial, banned from use by one of theworld's major governments and viewed with scepticismby many doctors.
I believe that this procedure is a valuable clinicaltool: in the randomly selected group of ideal patientsI have described, chemonucleolysis had an 80% suc-cess rate. The issue remains unresolved, but in myopinion history will view Smith's contribution to thetreatment of a herniated intervertebral disc with thesame importance and respect granted Mixter and Barr10for initially describing the condition.
I thank Mary Hogan, MSW for the many hours of re-search assistance. In addition, Dr. Eng Lee (orthopedicresident in the department of surgery, University ofToronto) and Dr. Nasser Khoury (neurosurgical residentin the same department) assisted in the follow-up of manyof the patients. Further, I thank the many surgeons inmany areas of North America who assisted me by seeingpatients. Dr. D.F. Andrews, director of statistical services.and his staff in the department of statistics, Universityof Toronto were very helpful in assembling and analysingthe data.
References1. SMITH L: Enzyme dissolution of the nucleus pulposus in
humans. JAMA 1964; 187: 137-1402. MARTINS AN, RAMIREZ A, JOHNSTON J, SCHWET5CHENAU
PR: Double-blind evaluation of chemonucleolysis for her-niated lumbar discs. Late results. J Neurosurg 1978; 49:8 16-827
3. MACNAB I, MCCULLOCH JA, WEINER DS, HUGO EP, GAL-WAY RD, DALL D: Chemonucleolysis. Can J Surg 1971;14: 280-289
4. FORD LT: Experimental study of chymopapain in cats.C/in Orthop 1969; 67: 68-71
5. STERN IJ, SMITH L: Dissolution by chymopapain in vitroof tissue from normal or prolapsed intervertebral disks.C/in Orthop 1967; 50: 269-277
6. MCCULLOCH JA, WADDELL G: Variation of the lumbo-sacral myotomes with bony segmental anomalies. J Bonebull Surg [Br] 1980; 62: 475-480
7. Idem: Lateral lumbar discography. Br J Radiol 1978; 51:498-502
8. HIRSCH C, NACHEMSON A: The reliability of lumbar discsurgery. C/in Orhop 1963; 29: 189-195
9. MCCULLOCH JA: Chemonucleolysis. J Bone Joint Surg [Br]1977; 59: 45-52
10. MIXTER WJ, BARR JS: Rupture of the intervertebral discwith involvement of the spinal canal. N Dig/ J Med 1934;211: 210-215
882 CMA JOURNAL/APRIL 1, 1981/VOL. 124