chemotherapy before liver resection of colorectal ...... friend or foe? abstract and introduction...
TRANSCRIPT

www.medscape.com
Friend or Foe?
Abstract and Introduction
Abstract
Objective: We conducted a systematic review of the published literature to critically assess benefits and risks of the use ofpreoperative chemotherapy in patients presenting with colorectal liver metastases.Background: In many centers, chemotherapy is used before hepatic resection of colorectal metastases, even in the presence ofa single lesion. Application of chemotherapy requires clear conceptual distinction between patients presenting with resectablelesions (neoadjuvant) versus patients presenting with unresectable lesions, for which chemotherapy is used to reach aresectable situation (downsizing).Methods: The literature (PubMed) was systematically reviewed for publications related to liver surgery and chemotherapyaccording to the methodology recommended by the Cochrane Collaboration.Results: For unresectable liver metastases, combination regimens result in enhanced tumor response and resectability rates upto 30%, although the additional benefit from targeted agents such as bevacizumab or cetuximab is marginal. For resectablelesions, studies on neoadjuvant chemotherapy failed to convincingly demonstrate a survival benefit. Most reports describedincreased postoperative complications in a subset of patients due to parenchymal alterations such as chemotherapy-associatedsteatohepatitis or sinusoidal obstruction syndrome.Conclusion: Preoperative standard chemotherapy can be recommended for downsizing unresectable liver metastases, but notfor resectable lesions, for which adjuvant chemotherapy is preferred.
Introduction
In patients with colorectal cancer (CRC), the liver is the most common site of hematogenous metastases. Synchronous livermetastases occur in about 15% of the patients, whereas the overall risk of developing metachronous metastases after resectionof the primary site is about 13%.[1] This risk increases to more than 30% in patients presenting with positive mesenteric lymphnodes (stage III disease).[1] In the absence of any treatment, the prognosis of patients with liver metastases is dismal with a5-year survival rate approaching zero.[2] Liver surgery with complete resection of the metastases has markedly improvedlong-term survival ranging from 36% to 58% and from 23% to 36% at 5 and 10 years, respectively.[3–9] In addition, the safety ofliver surgery has improved dramatically with current perioperative mortality rates of less than 5% in expert centers.[10–13]
The most significant advance regarding CRC over the past decade has been the introduction of several effective cytotoxic andtargeted agents (Table 1). Until the mid-1990s, 5-fluorouracil (5FU) was the only drug available for the treatment of metastaticCRC, yielding response rates below 20% without survival advantage. Then, two potent cytotoxic drugs, oxaliplatin and irinotecan,were introduced.[14] Irinotecan increased the response rates up to 39% in combination with 5FU therapy.[15,16] Similarly,oxaliplatin improved the response rate from 22% to 51% compared to 5FU alone.[17,18] Further benefits were achieved by theaddition of newly developed targeted agents such as the monoclonal antibodies cetuximab or panitumumab directed againstEGFR (Erbitux, Bristol-Myers Squibb, USA; Vectibix, Amgen, Netherlands, Avastin, Roche, Switzerland)[19] or bevacizumabdirected against VEGF (Avastin, Roche).[20] Combinations of oxaliplatin- or irinotecan-based chemotherapy with such antibodiesresulted in tumor response rates in up to 60% of the evaluated populations. Several large studies (Table 1) provide evidence thatin patients with metastatic CRC treated in a palliative intention, the combination of two cytotoxic drugs with an antibody increasedthe median overall survival from 20 to 22 months. In contrast to the palliative situation, there is much less evidence about theeffect of chemotherapy on survival in the perioperative setting. For example, there are only few studies looking at the use ofadjuvant chemotherapy after complete (R0) resection of liver metastases. One recently published multicenter RCT of 5FUmonotherapy demonstrated an increased disease-free survival and a trend toward increased overall survival compared toresection alone.[21] Although such a single agent regimen is currently obsolete, this unique RCT suggests that better results are
Chemotherapy Before Liver Resection of ColorectalMetastases
Kuno Lehmann, MD; Andreas Rickenbacher, MD; Achim Weber, MD; Bernhard C. Pestalozzi, MD;Pierre-Alain Clavien, MD, PhD, FACS
Posted: 02/22/2012; Annals of Surgery. 2012;255(2):237-247. © 2012 Lippincott Williams & Wilkins
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
1 de 23 24/02/12 01:17
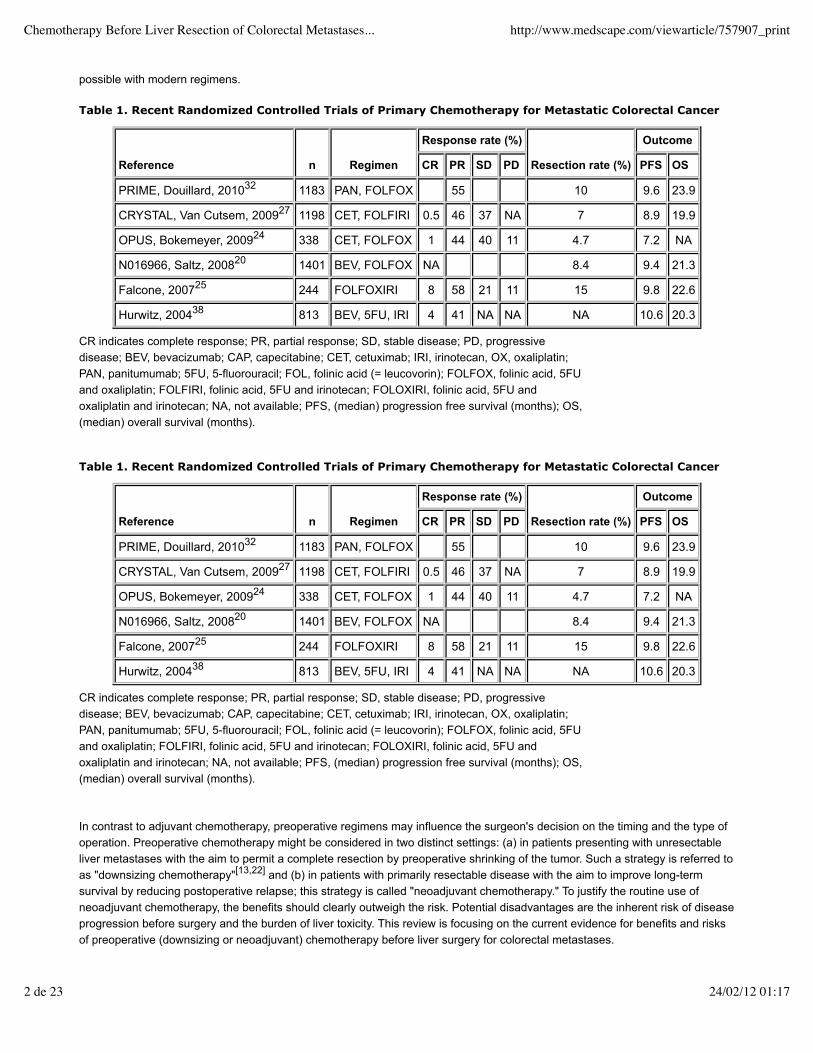
possible with modern regimens.
In contrast to adjuvant chemotherapy, preoperative regimens may influence the surgeon's decision on the timing and the type ofoperation. Preoperative chemotherapy might be considered in two distinct settings: (a) in patients presenting with unresectableliver metastases with the aim to permit a complete resection by preoperative shrinking of the tumor. Such a strategy is referred toas "downsizing chemotherapy"[13,22] and (b) in patients with primarily resectable disease with the aim to improve long-termsurvival by reducing postoperative relapse; this strategy is called "neoadjuvant chemotherapy." To justify the routine use ofneoadjuvant chemotherapy, the benefits should clearly outweigh the risk. Potential disadvantages are the inherent risk of diseaseprogression before surgery and the burden of liver toxicity. This review is focusing on the current evidence for benefits and risksof preoperative (downsizing or neoadjuvant) chemotherapy before liver surgery for colorectal metastases.
Table 1. Recent Randomized Controlled Trials of Primary Chemotherapy for Metastatic Colorectal Cancer
Reference n Regimen
Response rate (%)
Resection rate (%)
Outcome
CR PR SD PD PFS OS
PRIME, Douillard, 201032 1183 PAN, FOLFOX 55 10 9.6 23.9
CRYSTAL, Van Cutsem, 200927 1198 CET, FOLFIRI 0.5 46 37 NA 7 8.9 19.9
OPUS, Bokemeyer, 200924 338 CET, FOLFOX 1 44 40 11 4.7 7.2 NA
N016966, Saltz, 200820 1401 BEV, FOLFOX NA 8.4 9.4 21.3
Falcone, 200725 244 FOLFOXIRI 8 58 21 11 15 9.8 22.6
Hurwitz, 200438 813 BEV, 5FU, IRI 4 41 NA NA NA 10.6 20.3
CR indicates complete response; PR, partial response; SD, stable disease; PD, progressivedisease; BEV, bevacizumab; CAP, capecitabine; CET, cetuximab; IRI, irinotecan, OX, oxaliplatin;PAN, panitumumab; 5FU, 5-fluorouracil; FOL, folinic acid (= leucovorin); FOLFOX, folinic acid, 5FUand oxaliplatin; FOLFIRI, folinic acid, 5FU and irinotecan; FOLOXIRI, folinic acid, 5FU andoxaliplatin and irinotecan; NA, not available; PFS, (median) progression free survival (months); OS,(median) overall survival (months).
Table 1. Recent Randomized Controlled Trials of Primary Chemotherapy for Metastatic Colorectal Cancer
Reference n Regimen
Response rate (%)
Resection rate (%)
Outcome
CR PR SD PD PFS OS
PRIME, Douillard, 201032 1183 PAN, FOLFOX 55 10 9.6 23.9
CRYSTAL, Van Cutsem, 200927 1198 CET, FOLFIRI 0.5 46 37 NA 7 8.9 19.9
OPUS, Bokemeyer, 200924 338 CET, FOLFOX 1 44 40 11 4.7 7.2 NA
N016966, Saltz, 200820 1401 BEV, FOLFOX NA 8.4 9.4 21.3
Falcone, 200725 244 FOLFOXIRI 8 58 21 11 15 9.8 22.6
Hurwitz, 200438 813 BEV, 5FU, IRI 4 41 NA NA NA 10.6 20.3
CR indicates complete response; PR, partial response; SD, stable disease; PD, progressivedisease; BEV, bevacizumab; CAP, capecitabine; CET, cetuximab; IRI, irinotecan, OX, oxaliplatin;PAN, panitumumab; 5FU, 5-fluorouracil; FOL, folinic acid (= leucovorin); FOLFOX, folinic acid, 5FUand oxaliplatin; FOLFIRI, folinic acid, 5FU and irinotecan; FOLOXIRI, folinic acid, 5FU andoxaliplatin and irinotecan; NA, not available; PFS, (median) progression free survival (months); OS,(median) overall survival (months).
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
2 de 23 24/02/12 01:17
Methods
Search Strategy
The literature was scanned for publications related to liver surgery and chemotherapy according to the methodologyrecommended by the Cochrane Collaboration. The database (PubMed) was searched using exploded Medical Subject headings(MeSH) terms and specific text-word terms ("colorectal liver metastases," "liver surgery," "chemotherapy," "portal veinembolization," "portal vein ligation," "liver regeneration," "chemotherapy-associated steatohepatitis," "sinusoidal obstructionsyndrome," "downsizing," "liver injury," "complications," and "neoadjuvant"). All search results were stored in an EndNote file andduplicates were excluded. Two authors (KL and AR) independently assessed all the abstracts for eligibility with predefinedselection criteria (see below). The reference lists of retrieved papers were also screened for missing publications andpublications from a manual search were added to the list.
Selection Criteria
Publications reporting the use of chemotherapy in combination with liver surgery were included in this review. Exclusion criteriawere nonhuman studies, and articles not published in the English language. Only full original papers were retained, whereaseditorials, letters, practice guidelines, reviews, case reports, comments, and expert opinions were also excluded. Publicationsconcerning neoadjuvant chemotherapy were only considered if neoadjuvant chemotherapy was used preoperatively in patientswith resectable liver metastases, which had to be described in the publication.
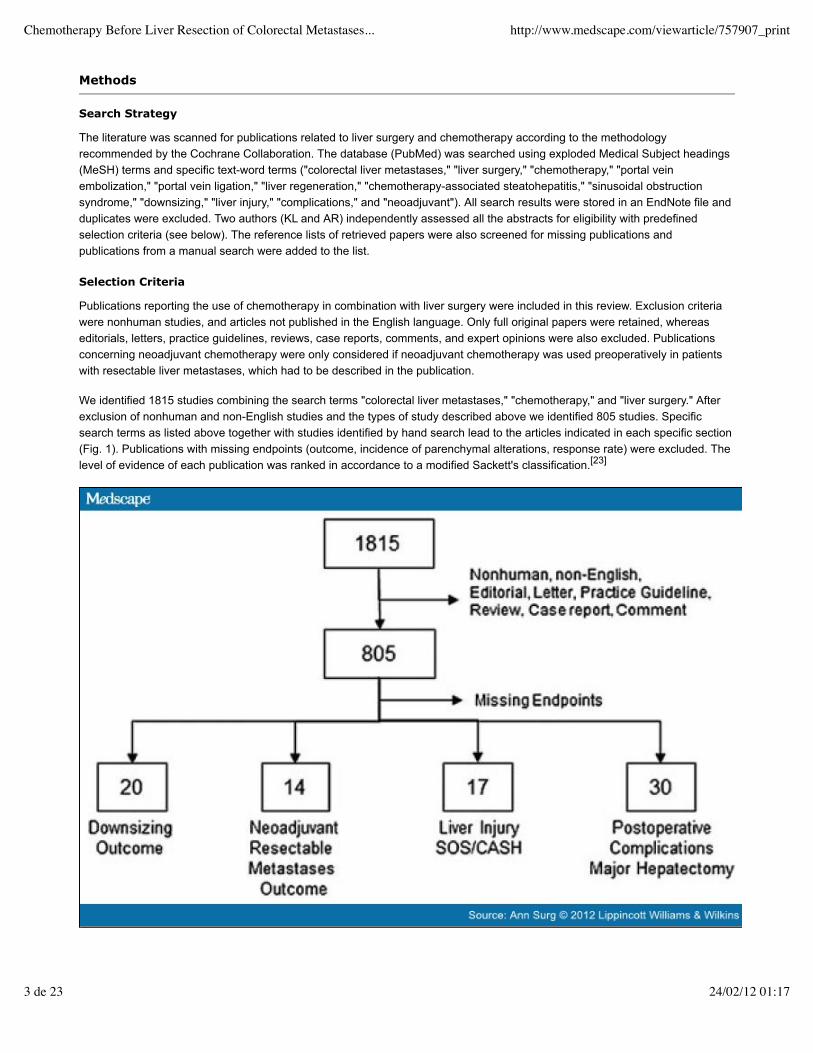
We identified 1815 studies combining the search terms "colorectal liver metastases," "chemotherapy," and "liver surgery." Afterexclusion of nonhuman and non-English studies and the types of study described above we identified 805 studies. Specificsearch terms as listed above together with studies identified by hand search lead to the articles indicated in each specific section(Fig. 1). Publications with missing endpoints (outcome, incidence of parenchymal alterations, response rate) were excluded. Thelevel of evidence of each publication was ranked in accordance to a modified Sackett's classification.[23]
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
3 de 23 24/02/12 01:17
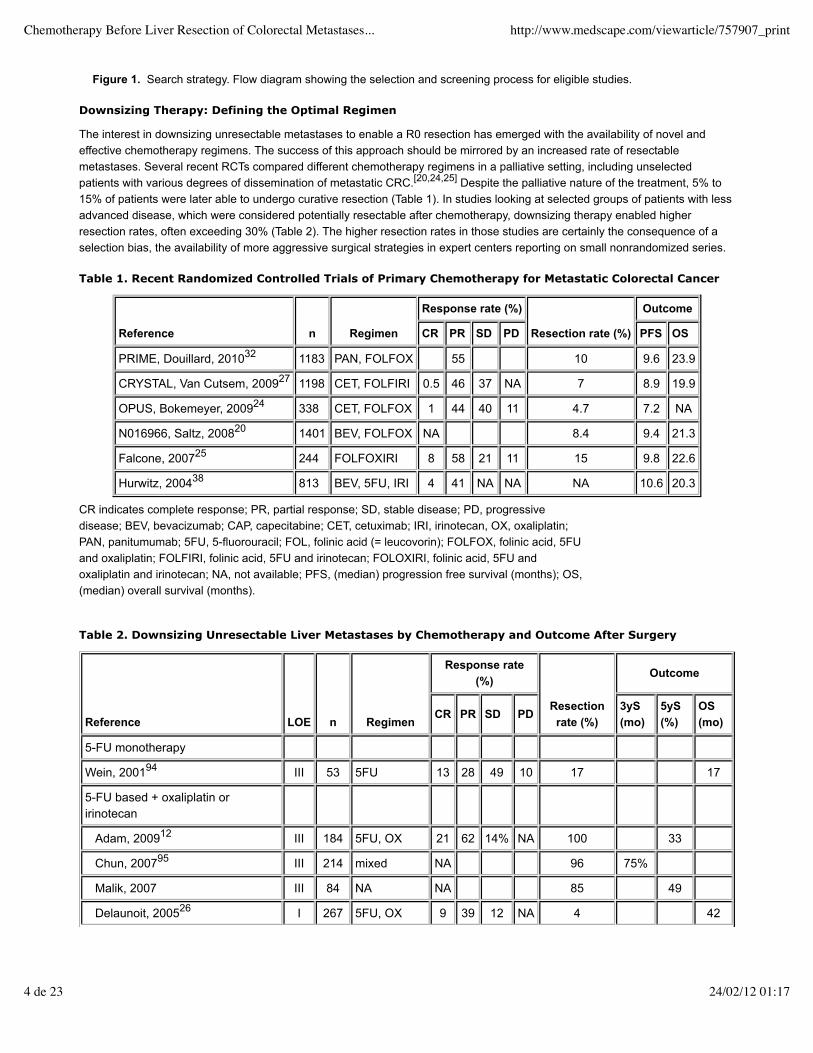
Figure 1. Search strategy. Flow diagram showing the selection and screening process for eligible studies.
Downsizing Therapy: Defining the Optimal Regimen
The interest in downsizing unresectable metastases to enable a R0 resection has emerged with the availability of novel andeffective chemotherapy regimens. The success of this approach should be mirrored by an increased rate of resectablemetastases. Several recent RCTs compared different chemotherapy regimens in a palliative setting, including unselectedpatients with various degrees of dissemination of metastatic CRC.[20,24,25] Despite the palliative nature of the treatment, 5% to15% of patients were later able to undergo curative resection (Table 1). In studies looking at selected groups of patients with lessadvanced disease, which were considered potentially resectable after chemotherapy, downsizing therapy enabled higherresection rates, often exceeding 30% (Table 2). The higher resection rates in those studies are certainly the consequence of aselection bias, the availability of more aggressive surgical strategies in expert centers reporting on small nonrandomized series.
Table 1. Recent Randomized Controlled Trials of Primary Chemotherapy for Metastatic Colorectal Cancer
Reference n Regimen
Response rate (%)
Resection rate (%)
Outcome
CR PR SD PD PFS OS
PRIME, Douillard, 201032 1183 PAN, FOLFOX 55 10 9.6 23.9
CRYSTAL, Van Cutsem, 200927 1198 CET, FOLFIRI 0.5 46 37 NA 7 8.9 19.9
OPUS, Bokemeyer, 200924 338 CET, FOLFOX 1 44 40 11 4.7 7.2 NA
N016966, Saltz, 200820 1401 BEV, FOLFOX NA 8.4 9.4 21.3
Falcone, 200725 244 FOLFOXIRI 8 58 21 11 15 9.8 22.6
Hurwitz, 200438 813 BEV, 5FU, IRI 4 41 NA NA NA 10.6 20.3
CR indicates complete response; PR, partial response; SD, stable disease; PD, progressivedisease; BEV, bevacizumab; CAP, capecitabine; CET, cetuximab; IRI, irinotecan, OX, oxaliplatin;PAN, panitumumab; 5FU, 5-fluorouracil; FOL, folinic acid (= leucovorin); FOLFOX, folinic acid, 5FUand oxaliplatin; FOLFIRI, folinic acid, 5FU and irinotecan; FOLOXIRI, folinic acid, 5FU andoxaliplatin and irinotecan; NA, not available; PFS, (median) progression free survival (months); OS,(median) overall survival (months).
Table 2. Downsizing Unresectable Liver Metastases by Chemotherapy and Outcome After Surgery
Reference LOE n Regimen
Response rate(%)
Resectionrate (%)
Outcome
CR PR SD PD3yS(mo)
5yS(%)
OS(mo)
5-FU monotherapy
Wein, 200194 III 53 5FU 13 28 49 10 17 17
5-FU based + oxaliplatin oririnotecan
Adam, 200912 III 184 5FU, OX 21 62 14% NA 100 33
Chun, 200795 III 214 mixed NA 96 75%
Malik, 2007 III 84 NA NA 85 49
Delaunoit, 200526 I 267 5FU, OX 9 39 12 NA 4 42
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
4 de 23 24/02/12 01:17
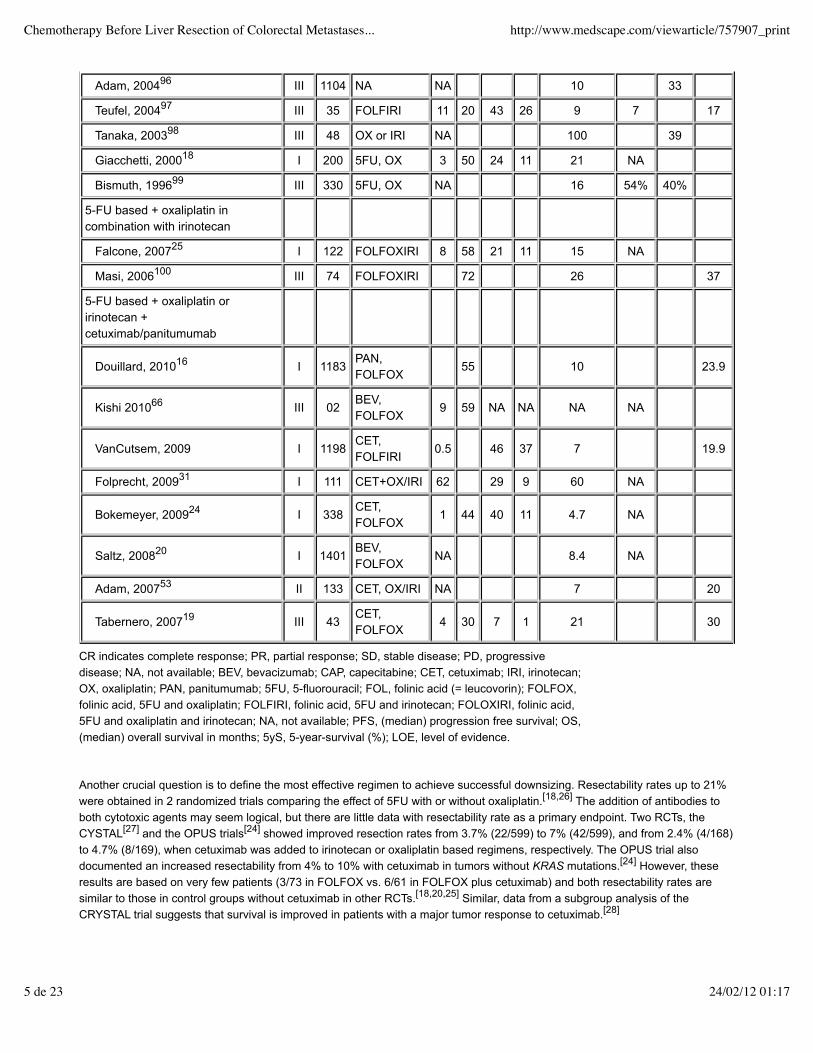
Another crucial question is to define the most effective regimen to achieve successful downsizing. Resectability rates up to 21%were obtained in 2 randomized trials comparing the effect of 5FU with or without oxaliplatin.[18,26] The addition of antibodies toboth cytotoxic agents may seem logical, but there are little data with resectability rate as a primary endpoint. Two RCTs, theCYSTAL[27] and the OPUS trials[24] showed improved resection rates from 3.7% (22/599) to 7% (42/599), and from 2.4% (4/168)to 4.7% (8/169), when cetuximab was added to irinotecan or oxaliplatin based regimens, respectively. The OPUS trial alsodocumented an increased resectability from 4% to 10% with cetuximab in tumors without KRAS mutations.[24] However, theseresults are based on very few patients (3/73 in FOLFOX vs. 6/61 in FOLFOX plus cetuximab) and both resectability rates aresimilar to those in control groups without cetuximab in other RCTs.[18,20,25] Similar, data from a subgroup analysis of theCRYSTAL trial suggests that survival is improved in patients with a major tumor response to cetuximab.[28]
Adam, 200496 III 1104 NA NA 10 33
Teufel, 200497 III 35 FOLFIRI 11 20 43 26 9 7 17
Tanaka, 200398 III 48 OX or IRI NA 100 39
Giacchetti, 200018 I 200 5FU, OX 3 50 24 11 21 NA
Bismuth, 199699 III 330 5FU, OX NA 16 54% 40%
5-FU based + oxaliplatin incombination with irinotecan
Falcone, 200725 I 122 FOLFOXIRI 8 58 21 11 15 NA
Masi, 2006100 III 74 FOLFOXIRI 72 26 37
5-FU based + oxaliplatin oririnotecan +cetuximab/panitumumab
Douillard, 201016 I 1183PAN,FOLFOX
55 10 23.9
Kishi 201066 III 02BEV,FOLFOX
9 59 NA NA NA NA
VanCutsem, 2009 I 1198CET,FOLFIRI
0.5 46 37 7 19.9
Folprecht, 200931 I 111 CET+OX/IRI 62 29 9 60 NA
Bokemeyer, 200924 I 338CET,FOLFOX
1 44 40 11 4.7 NA
Saltz, 200820 I 1401BEV,FOLFOX
NA 8.4 NA
Adam, 200753 II 133 CET, OX/IRI NA 7 20
Tabernero, 200719 III 43CET,FOLFOX
4 30 7 1 21 30
CR indicates complete response; PR, partial response; SD, stable disease; PD, progressivedisease; NA, not available; BEV, bevacizumab; CAP, capecitabine; CET, cetuximab; IRI, irinotecan;OX, oxaliplatin; PAN, panitumumab; 5FU, 5-fluorouracil; FOL, folinic acid (= leucovorin); FOLFOX,folinic acid, 5FU and oxaliplatin; FOLFIRI, folinic acid, 5FU and irinotecan; FOLOXIRI, folinic acid,5FU and oxaliplatin and irinotecan; NA, not available; PFS, (median) progression free survival; OS,(median) overall survival in months; 5yS, 5-year-survival (%); LOE, level of evidence.
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
5 de 23 24/02/12 01:17

This benefit of cetuximab in KRAS wild type tumors has been questioned by the COIN trial.[29] Survival of patients without KRASmutations was not improved when this antibody was added to an oxaliplatin-based neoadjuvant chemotherapy.[29] Recent datafrom genetic assessment of tumor tissues suggests that response rates and patient outcome may depend on other specificmutations of the EGFR signaling cascade.[30,31] Thus, a yet poorly defined subgroup of patients may profit from a therapy withcetuximab.
In the CELIM randomized phase II trial, cetuximab was added to both FOLFOX or FOLFIRI, resulting in a high overallresectability rate of 34% (23/68).[32] Of note, this study reported similar resection rates for patients with mutant and with wild typeKRAS.[32] Because the CELIM trial used cetuximab in both arms, it failed to provide clear evidence on the benefit of adding atargeted agent to a cytotoxic agent.
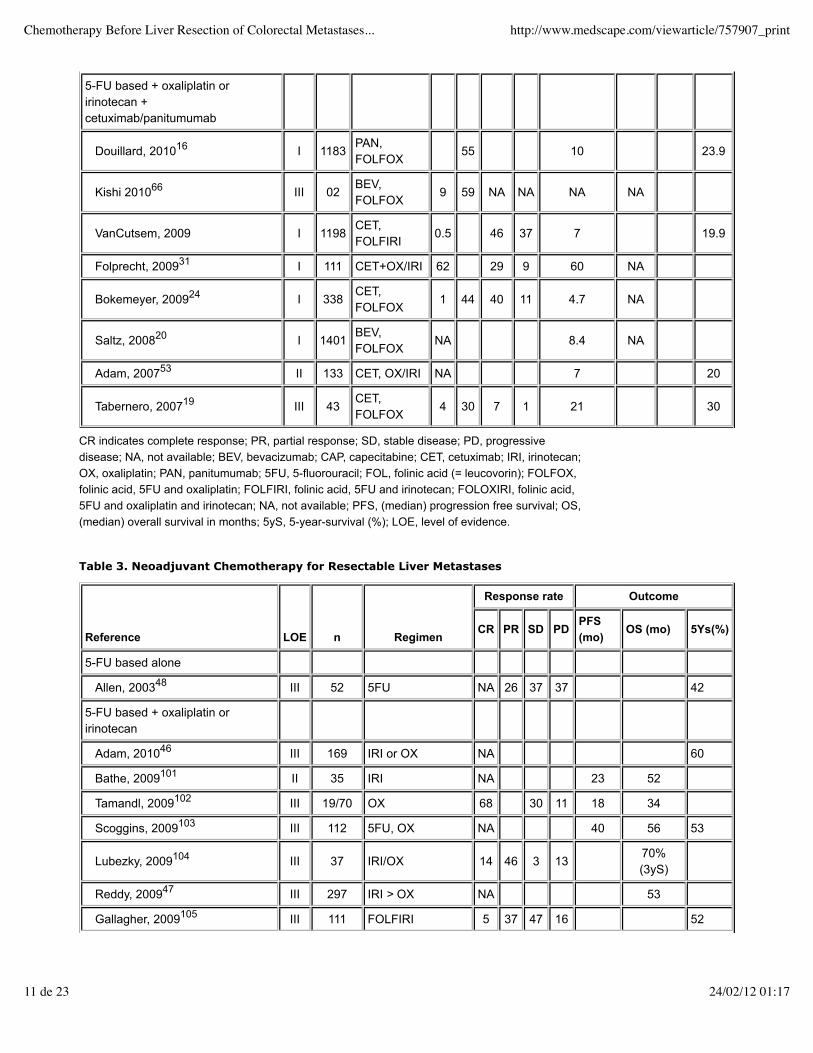
Panitumumab added to oxaliplatin was assessed in the PRIME trial, including only patients with KRAS wildtype tumors.[33] Thisregimen did not increase resectability. A similar finding was documented for bevacizumab, that only moderately improvedresectability rates from 6.1% (43/700) to 8.4% (59/700), when added to FOLFOX in a large RCT.[20] According to this study, only16 of 700 patients presenting with unresectable liver metastases could benefit from the addition of preoperative bevacizumab. Acombination of 2 antibodies, bevacizumab, and panitumumab, to cytotoxic regimens failed to add any benefit, as shown by thePACCE[34] and CAIRO-2[35] trials.
Another approach is the upfront use of all 3 effective cytotoxic drugs, ie, 5FU, irinotecan plus oxaliplatin. In a large RCT, such aregimen has led to improved progression free survival, and an improved overall resection rate of 15%, and 36% for liver-onlymetastases.[25] This regimen was associated with many side effects, such as diarrhea and fatigue.
We conclude that preoperative downsizing chemotherapy with oxaliplatin or irinotecan-based combinations for nonresectablemetastases enables subsequent radical resections in about a third of selected groups of patients. The addition of a singletargeted agent such as cetuximab or panitumumab (for KRAS wildtype tumors) or bevacizumab to cytotoxic combinations mayoffer a benefit for selected patients in the downsizing scenario. Given the additional costs of about 40,000 $ per patient(cetuximab for 16 weeks), the routine use of combination chemotherapy such as FOLFOX (or XELOX) or FOLFIRI incombination with cetuximab, panitumumab, or bevacizumab for downsizing liver metastases is currently not warranted. In thefuture, additional genotyping may help to select those patients that will respond well to a therapy with cetuximab. In young andhealthy patients, the triple combination FOLFOXIRI is an appealing alternative, although the side effects are higher.
Can Response and Resectability Rates be Further Increased by Selective Hepatic IntraarterialChemotherapy (HAI)?
HAI was designed to selectively deliver chemotherapeutic drugs to the target site. It aims at reducing side effects by reducing theoverall systemic exposure to the drugs. Selective HAI may offer superior efficacy along with reduced systemic toxicity, comparedto systemic chemotherapy.[36] Furthermore, placement of HAI catheters during open surgery can be combined with otherprocedures, such as portal vein ligation to induce hypertrophy of the contralateral liver lobe.[37,38] To avoid disease progression,the future remnant part of the liver, usually the left hemiliver or just segments II to III, can be concomitantly cleared frommetastases.[13,39] After an interval of about 4 weeks, a curative hepatectomy can be attempted.[37]
Most studies on HAI have used continuous infusion of floxuridine (FUDR), a pyrimidine antimetabolite considered superior to5FU because of its short half-life and high hepatic extraction rate. A recent meta-analysis has suggested a higher response rateto HAI than to systemic 5FU-based therapy (43% vs. 18%, respectively). However, there was no benefit on survival.[40] Theevidence on the benefit of the use of the second generation of drugs is more limited for HAI, although promising data areemerging. In a recent phase II study, HAI with oxaliplatin was used in combination with systemic treatment, resulting in animpressive response rate of 64%.[41] The same regimen enabled successful downsizing and resection in 18% (8/44) of patientswith metastases refractory to aggressive systemic oxaliplatin or irinotecan treatment.[42] HAI with oxaliplatin resulted in animpressive 5-year-survival of 56% in patients that were downsized and resected, compared to 0% in the nonsurgical group.[43] Inaddition to improved resectability, HAI might reduce relapse rates, as liver metastases, that become undetectable after HAI, werereported to remain silent in nearly two thirds of the cases.[44] This benefit of HAI is supported by a recent study that identified HAIwith FUDR as a significant predictor for a complete pathologic response.[45]
We conclude that hepatic intraarterial chemotherapy may achieve more complete responses, and higher resectability rates thansystemic chemotherapy. HAI should be considered in situations with a high tumor load, and in lesions refractory to systemic
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
6 de 23 24/02/12 01:17
chemotherapy.
Is Neoadjuvant Chemotherapy Justified for Resectable Lesions?
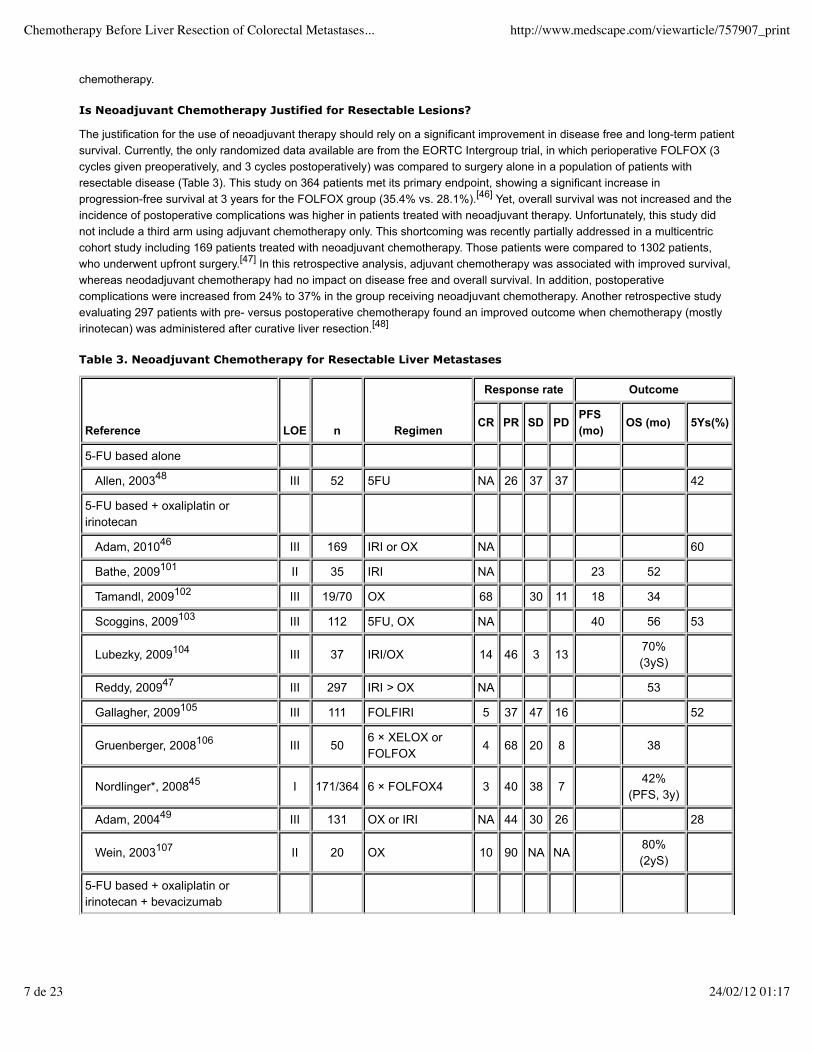
The justification for the use of neoadjuvant therapy should rely on a significant improvement in disease free and long-term patientsurvival. Currently, the only randomized data available are from the EORTC Intergroup trial, in which perioperative FOLFOX (3cycles given preoperatively, and 3 cycles postoperatively) was compared to surgery alone in a population of patients withresectable disease (Table 3). This study on 364 patients met its primary endpoint, showing a significant increase inprogression-free survival at 3 years for the FOLFOX group (35.4% vs. 28.1%).[46] Yet, overall survival was not increased and theincidence of postoperative complications was higher in patients treated with neoadjuvant therapy. Unfortunately, this study didnot include a third arm using adjuvant chemotherapy only. This shortcoming was recently partially addressed in a multicentriccohort study including 169 patients treated with neoadjuvant chemotherapy. Those patients were compared to 1302 patients,who underwent upfront surgery.[47] In this retrospective analysis, adjuvant chemotherapy was associated with improved survival,whereas neodadjuvant chemotherapy had no impact on disease free and overall survival. In addition, postoperativecomplications were increased from 24% to 37% in the group receiving neoadjuvant chemotherapy. Another retrospective studyevaluating 297 patients with pre- versus postoperative chemotherapy found an improved outcome when chemotherapy (mostlyirinotecan) was administered after curative liver resection.[48]
Table 3. Neoadjuvant Chemotherapy for Resectable Liver Metastases
Reference LOE n Regimen
Response rate Outcome
CR PR SD PDPFS(mo)
OS (mo) 5Ys(%)
5-FU based alone
Allen, 200348 III 52 5FU NA 26 37 37 42
5-FU based + oxaliplatin oririnotecan
Adam, 201046 III 169 IRI or OX NA 60
Bathe, 2009101 II 35 IRI NA 23 52
Tamandl, 2009102 III 19/70 OX 68 30 11 18 34
Scoggins, 2009103 III 112 5FU, OX NA 40 56 53
Lubezky, 2009104 III 37 IRI/OX 14 46 3 1370%(3yS)
Reddy, 200947 III 297 IRI > OX NA 53
Gallagher, 2009105 III 111 FOLFIRI 5 37 47 16 52
Gruenberger, 2008106 III 506 × XELOX orFOLFOX
4 68 20 8 38
Nordlinger*, 200845 I 171/364 6 × FOLFOX4 3 40 38 742%
(PFS, 3y)
Adam, 200449 III 131 OX or IRI NA 44 30 26 28
Wein, 2003107 II 20 OX 10 90 NA NA80%(2yS)
5-FU based + oxaliplatin oririnotecan + bevacizumab
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
7 de 23 24/02/12 01:17
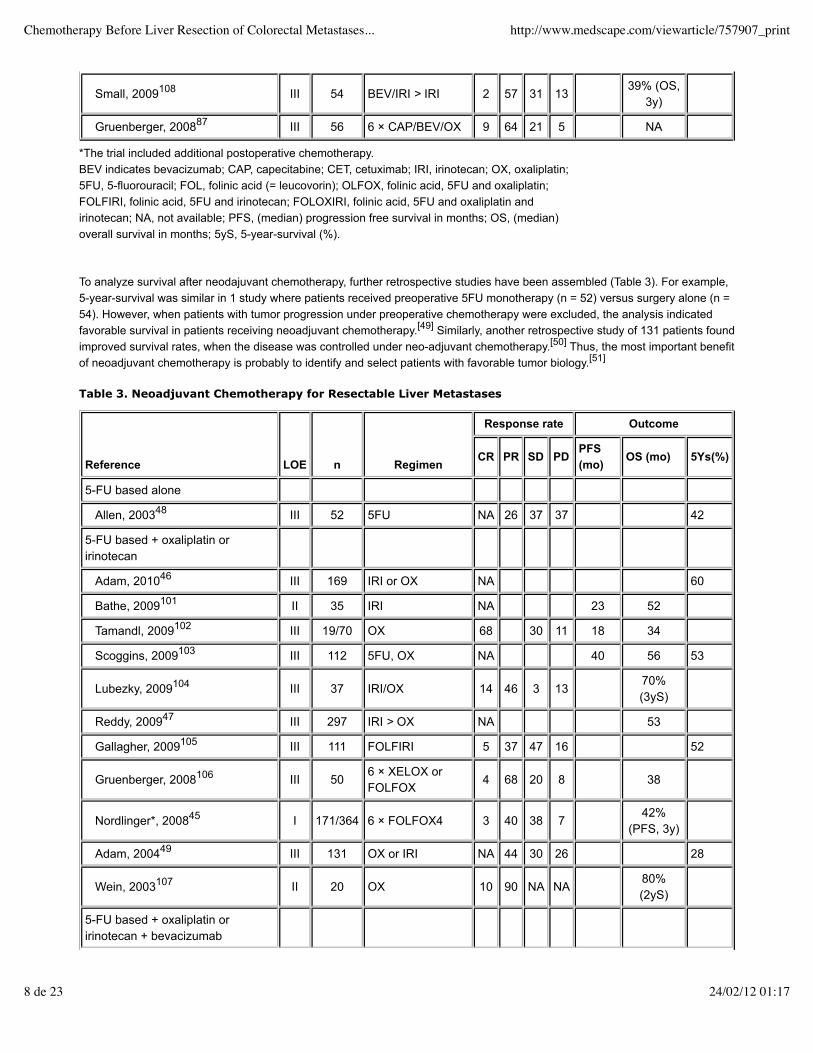
To analyze survival after neodajuvant chemotherapy, further retrospective studies have been assembled (Table 3). For example,5-year-survival was similar in 1 study where patients received preoperative 5FU monotherapy (n = 52) versus surgery alone (n =54). However, when patients with tumor progression under preoperative chemotherapy were excluded, the analysis indicatedfavorable survival in patients receiving neoadjuvant chemotherapy.[49] Similarly, another retrospective study of 131 patients foundimproved survival rates, when the disease was controlled under neo-adjuvant chemotherapy.[50] Thus, the most important benefitof neoadjuvant chemotherapy is probably to identify and select patients with favorable tumor biology.[51]
Small, 2009108 III 54 BEV/IRI > IRI 2 57 31 1339% (OS,
3y)
Gruenberger, 200887 III 56 6 × CAP/BEV/OX 9 64 21 5 NA
*The trial included additional postoperative chemotherapy.BEV indicates bevacizumab; CAP, capecitabine; CET, cetuximab; IRI, irinotecan; OX, oxaliplatin;5FU, 5-fluorouracil; FOL, folinic acid (= leucovorin); OLFOX, folinic acid, 5FU and oxaliplatin;FOLFIRI, folinic acid, 5FU and irinotecan; FOLOXIRI, folinic acid, 5FU and oxaliplatin andirinotecan; NA, not available; PFS, (median) progression free survival in months; OS, (median)overall survival in months; 5yS, 5-year-survival (%).
Table 3. Neoadjuvant Chemotherapy for Resectable Liver Metastases
Reference LOE n Regimen
Response rate Outcome
CR PR SD PDPFS(mo)
OS (mo) 5Ys(%)
5-FU based alone
Allen, 200348 III 52 5FU NA 26 37 37 42
5-FU based + oxaliplatin oririnotecan
Adam, 201046 III 169 IRI or OX NA 60
Bathe, 2009101 II 35 IRI NA 23 52
Tamandl, 2009102 III 19/70 OX 68 30 11 18 34
Scoggins, 2009103 III 112 5FU, OX NA 40 56 53
Lubezky, 2009104 III 37 IRI/OX 14 46 3 1370%(3yS)
Reddy, 200947 III 297 IRI > OX NA 53
Gallagher, 2009105 III 111 FOLFIRI 5 37 47 16 52
Gruenberger, 2008106 III 506 × XELOX orFOLFOX
4 68 20 8 38
Nordlinger*, 200845 I 171/364 6 × FOLFOX4 3 40 38 742%
(PFS, 3y)
Adam, 200449 III 131 OX or IRI NA 44 30 26 28
Wein, 2003107 II 20 OX 10 90 NA NA80%(2yS)
5-FU based + oxaliplatin oririnotecan + bevacizumab
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
8 de 23 24/02/12 01:17

Complete tumor response, occurring in 2% to 14% of patients after neoadjuvant treatment (Table 3) is unwanted for resectablelesions, and may even be detrimental due to undetectable remnant tumor cells. Careful histological examination afterpreoperative chemotherapy has revealed the presence of vital cancer cells in surrounding halos of former tumor nodules in mostcases.[52] For example in one study, 80% of metastases that had disappeared radiologically after chemotherapy contained viabletumor cells at the time of resection.[53] Together with the difficulty to localize the tumor during surgery, undetectable tumornodules may predispose to incomplete resections and early recurrence.[53]
Small, 2009108 III 54 BEV/IRI > IRI 2 57 31 1339% (OS,
3y)
Gruenberger, 200887 III 56 6 × CAP/BEV/OX 9 64 21 5 NA
*The trial included additional postoperative chemotherapy.BEV indicates bevacizumab; CAP, capecitabine; CET, cetuximab; IRI, irinotecan; OX, oxaliplatin;5FU, 5-fluorouracil; FOL, folinic acid (= leucovorin); OLFOX, folinic acid, 5FU and oxaliplatin;FOLFIRI, folinic acid, 5FU and irinotecan; FOLOXIRI, folinic acid, 5FU and oxaliplatin andirinotecan; NA, not available; PFS, (median) progression free survival in months; OS, (median)overall survival in months; 5yS, 5-year-survival (%).
Table 3. Neoadjuvant Chemotherapy for Resectable Liver Metastases
Reference LOE n Regimen
Response rate Outcome
CR PR SD PDPFS(mo)
OS (mo) 5Ys(%)
5-FU based alone
Allen, 200348 III 52 5FU NA 26 37 37 42
5-FU based + oxaliplatin oririnotecan
Adam, 201046 III 169 IRI or OX NA 60
Bathe, 2009101 II 35 IRI NA 23 52
Tamandl, 2009102 III 19/70 OX 68 30 11 18 34
Scoggins, 2009103 III 112 5FU, OX NA 40 56 53
Lubezky, 2009104 III 37 IRI/OX 14 46 3 1370%(3yS)
Reddy, 200947 III 297 IRI > OX NA 53
Gallagher, 2009105 III 111 FOLFIRI 5 37 47 16 52
Gruenberger, 2008106 III 506 × XELOX orFOLFOX
4 68 20 8 38
Nordlinger*, 200845 I 171/364 6 × FOLFOX4 3 40 38 742%
(PFS, 3y)
Adam, 200449 III 131 OX or IRI NA 44 30 26 28
Wein, 2003107 II 20 OX 10 90 NA NA80%(2yS)
5-FU based + oxaliplatin oririnotecan + bevacizumab
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
9 de 23 24/02/12 01:17
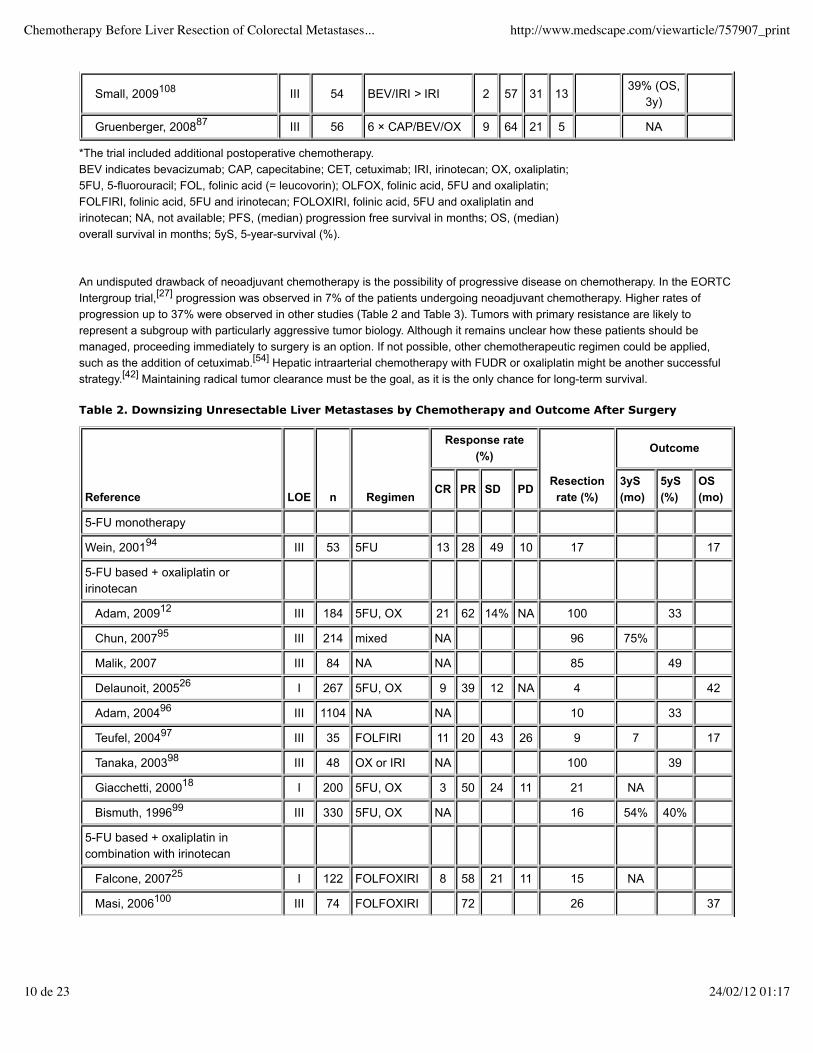
An undisputed drawback of neoadjuvant chemotherapy is the possibility of progressive disease on chemotherapy. In the EORTCIntergroup trial,[27] progression was observed in 7% of the patients undergoing neoadjuvant chemotherapy. Higher rates ofprogression up to 37% were observed in other studies (Table 2 and Table 3). Tumors with primary resistance are likely torepresent a subgroup with particularly aggressive tumor biology. Although it remains unclear how these patients should bemanaged, proceeding immediately to surgery is an option. If not possible, other chemotherapeutic regimen could be applied,such as the addition of cetuximab.[54] Hepatic intraarterial chemotherapy with FUDR or oxaliplatin might be another successfulstrategy.[42] Maintaining radical tumor clearance must be the goal, as it is the only chance for long-term survival.
Small, 2009108 III 54 BEV/IRI > IRI 2 57 31 1339% (OS,
3y)
Gruenberger, 200887 III 56 6 × CAP/BEV/OX 9 64 21 5 NA
*The trial included additional postoperative chemotherapy.BEV indicates bevacizumab; CAP, capecitabine; CET, cetuximab; IRI, irinotecan; OX, oxaliplatin;5FU, 5-fluorouracil; FOL, folinic acid (= leucovorin); OLFOX, folinic acid, 5FU and oxaliplatin;FOLFIRI, folinic acid, 5FU and irinotecan; FOLOXIRI, folinic acid, 5FU and oxaliplatin andirinotecan; NA, not available; PFS, (median) progression free survival in months; OS, (median)overall survival in months; 5yS, 5-year-survival (%).
Table 2. Downsizing Unresectable Liver Metastases by Chemotherapy and Outcome After Surgery
Reference LOE n Regimen
Response rate(%)
Resectionrate (%)
Outcome
CR PR SD PD3yS(mo)
5yS(%)
OS(mo)
5-FU monotherapy
Wein, 200194 III 53 5FU 13 28 49 10 17 17
5-FU based + oxaliplatin oririnotecan
Adam, 200912 III 184 5FU, OX 21 62 14% NA 100 33
Chun, 200795 III 214 mixed NA 96 75%
Malik, 2007 III 84 NA NA 85 49
Delaunoit, 200526 I 267 5FU, OX 9 39 12 NA 4 42
Adam, 200496 III 1104 NA NA 10 33
Teufel, 200497 III 35 FOLFIRI 11 20 43 26 9 7 17
Tanaka, 200398 III 48 OX or IRI NA 100 39
Giacchetti, 200018 I 200 5FU, OX 3 50 24 11 21 NA
Bismuth, 199699 III 330 5FU, OX NA 16 54% 40%
5-FU based + oxaliplatin incombination with irinotecan
Falcone, 200725 I 122 FOLFOXIRI 8 58 21 11 15 NA
Masi, 2006100 III 74 FOLFOXIRI 72 26 37
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
10 de 23 24/02/12 01:17
5-FU based + oxaliplatin oririnotecan +cetuximab/panitumumab
Douillard, 201016 I 1183PAN,FOLFOX
55 10 23.9
Kishi 201066 III 02BEV,FOLFOX
9 59 NA NA NA NA
VanCutsem, 2009 I 1198CET,FOLFIRI
0.5 46 37 7 19.9
Folprecht, 200931 I 111 CET+OX/IRI 62 29 9 60 NA
Bokemeyer, 200924 I 338CET,FOLFOX
1 44 40 11 4.7 NA
Saltz, 200820 I 1401BEV,FOLFOX
NA 8.4 NA
Adam, 200753 II 133 CET, OX/IRI NA 7 20
Tabernero, 200719 III 43CET,FOLFOX
4 30 7 1 21 30
CR indicates complete response; PR, partial response; SD, stable disease; PD, progressivedisease; NA, not available; BEV, bevacizumab; CAP, capecitabine; CET, cetuximab; IRI, irinotecan;OX, oxaliplatin; PAN, panitumumab; 5FU, 5-fluorouracil; FOL, folinic acid (= leucovorin); FOLFOX,folinic acid, 5FU and oxaliplatin; FOLFIRI, folinic acid, 5FU and irinotecan; FOLOXIRI, folinic acid,5FU and oxaliplatin and irinotecan; NA, not available; PFS, (median) progression free survival; OS,(median) overall survival in months; 5yS, 5-year-survival (%); LOE, level of evidence.
Table 3. Neoadjuvant Chemotherapy for Resectable Liver Metastases
Reference LOE n Regimen
Response rate Outcome
CR PR SD PDPFS(mo)
OS (mo) 5Ys(%)
5-FU based alone
Allen, 200348 III 52 5FU NA 26 37 37 42
5-FU based + oxaliplatin oririnotecan
Adam, 201046 III 169 IRI or OX NA 60
Bathe, 2009101 II 35 IRI NA 23 52
Tamandl, 2009102 III 19/70 OX 68 30 11 18 34
Scoggins, 2009103 III 112 5FU, OX NA 40 56 53
Lubezky, 2009104 III 37 IRI/OX 14 46 3 1370%(3yS)
Reddy, 200947 III 297 IRI > OX NA 53
Gallagher, 2009105 III 111 FOLFIRI 5 37 47 16 52
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
11 de 23 24/02/12 01:17
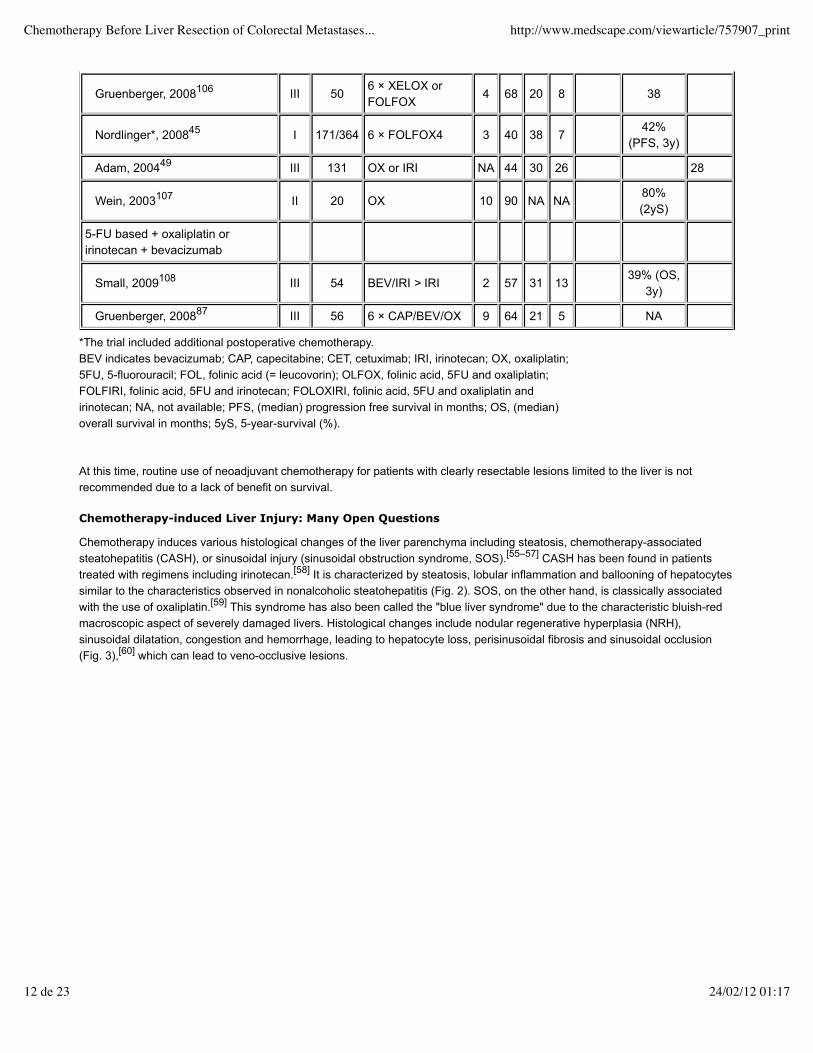
At this time, routine use of neoadjuvant chemotherapy for patients with clearly resectable lesions limited to the liver is notrecommended due to a lack of benefit on survival.
Chemotherapy-induced Liver Injury: Many Open Questions
Chemotherapy induces various histological changes of the liver parenchyma including steatosis, chemotherapy-associatedsteatohepatitis (CASH), or sinusoidal injury (sinusoidal obstruction syndrome, SOS).[55–57] CASH has been found in patientstreated with regimens including irinotecan.[58] It is characterized by steatosis, lobular inflammation and ballooning of hepatocytessimilar to the characteristics observed in nonalcoholic steatohepatitis (Fig. 2). SOS, on the other hand, is classically associatedwith the use of oxaliplatin.[59] This syndrome has also been called the "blue liver syndrome" due to the characteristic bluish-redmacroscopic aspect of severely damaged livers. Histological changes include nodular regenerative hyperplasia (NRH),sinusoidal dilatation, congestion and hemorrhage, leading to hepatocyte loss, perisinusoidal fibrosis and sinusoidal occlusion(Fig. 3),[60] which can lead to veno-occlusive lesions.
Gruenberger, 2008106 III 506 × XELOX orFOLFOX
4 68 20 8 38
Nordlinger*, 200845 I 171/364 6 × FOLFOX4 3 40 38 742%
(PFS, 3y)
Adam, 200449 III 131 OX or IRI NA 44 30 26 28
Wein, 2003107 II 20 OX 10 90 NA NA80%(2yS)
5-FU based + oxaliplatin oririnotecan + bevacizumab
Small, 2009108 III 54 BEV/IRI > IRI 2 57 31 1339% (OS,
3y)
Gruenberger, 200887 III 56 6 × CAP/BEV/OX 9 64 21 5 NA
*The trial included additional postoperative chemotherapy.BEV indicates bevacizumab; CAP, capecitabine; CET, cetuximab; IRI, irinotecan; OX, oxaliplatin;5FU, 5-fluorouracil; FOL, folinic acid (= leucovorin); OLFOX, folinic acid, 5FU and oxaliplatin;FOLFIRI, folinic acid, 5FU and irinotecan; FOLOXIRI, folinic acid, 5FU and oxaliplatin andirinotecan; NA, not available; PFS, (median) progression free survival in months; OS, (median)overall survival in months; 5yS, 5-year-survival (%).
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
12 de 23 24/02/12 01:17

Figure 2. Chemotherapy-associated steatohepatitis (CASH). A, Low power view revealing severe steatosis accentuated incentrilobular zone (H&E, scale bar: 200 µm). B, High power view showing hepatocellular steatosis and hepatocellulardegeneration (ballooning, arrowhead) as well as an inflammatory infiltrate with polymorphonuclear cells (arrow) (H&E, scalebar: 50 µm).
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
13 de 23 24/02/12 01:17
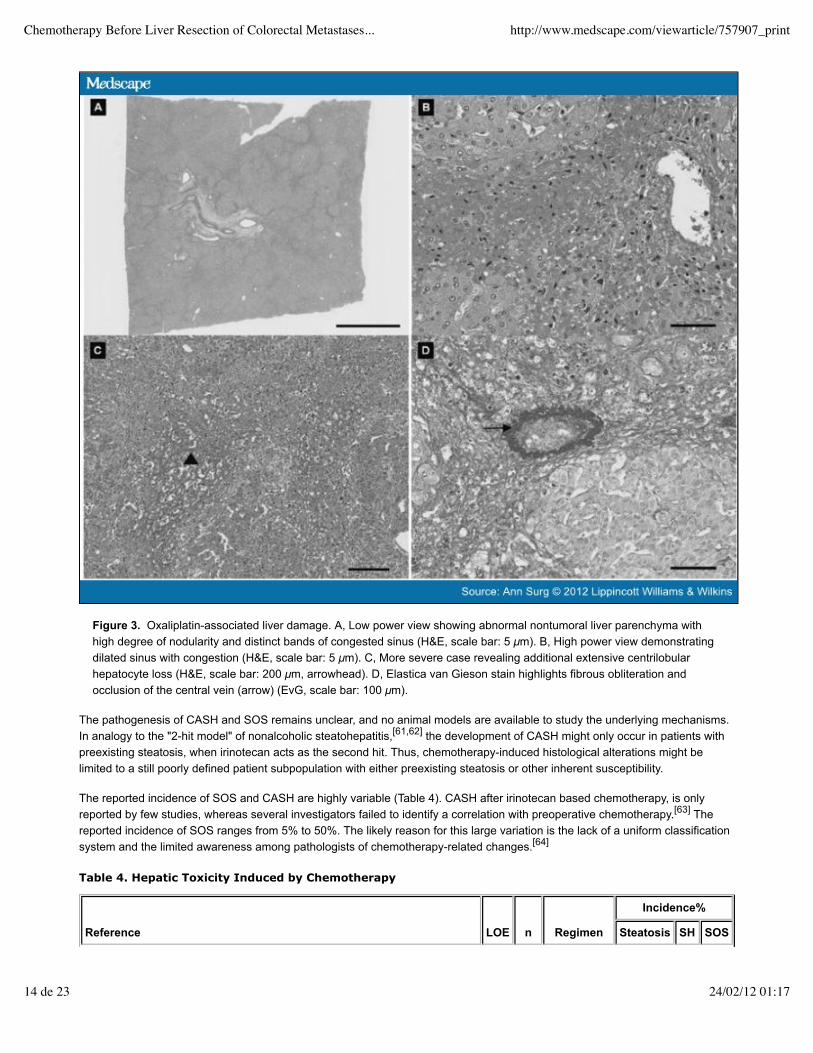
Figure 3. Oxaliplatin-associated liver damage. A, Low power view showing abnormal nontumoral liver parenchyma withhigh degree of nodularity and distinct bands of congested sinus (H&E, scale bar: 5 µm). B, High power view demonstratingdilated sinus with congestion (H&E, scale bar: 5 µm). C, More severe case revealing additional extensive centrilobularhepatocyte loss (H&E, scale bar: 200 µm, arrowhead). D, Elastica van Gieson stain highlights fibrous obliteration andocclusion of the central vein (arrow) (EvG, scale bar: 100 µm).
The pathogenesis of CASH and SOS remains unclear, and no animal models are available to study the underlying mechanisms.In analogy to the "2-hit model" of nonalcoholic steatohepatitis,[61,62] the development of CASH might only occur in patients withpreexisting steatosis, when irinotecan acts as the second hit. Thus, chemotherapy-induced histological alterations might belimited to a still poorly defined patient subpopulation with either preexisting steatosis or other inherent susceptibility.
The reported incidence of SOS and CASH are highly variable (Table 4). CASH after irinotecan based chemotherapy, is onlyreported by few studies, whereas several investigators failed to identify a correlation with preoperative chemotherapy.[63] Thereported incidence of SOS ranges from 5% to 50%. The likely reason for this large variation is the lack of a uniform classificationsystem and the limited awareness among pathologists of chemotherapy-related changes.[64]
Table 4. Hepatic Toxicity Induced by Chemotherapy
Reference LOE n Regimen
Incidence%
Steatosis SH SOS
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
14 de 23 24/02/12 01:17

Does Preoperative Chemotherapy Increase the Morbidity/Mortality After Surgery?
The association of CASH and SOS with postoperative outcome has been addressed in several recent reviews.[55,56] Briefly,agreement exists on a link between the chemotherapy-associated changes and poor postoperative outcomes. A subgroupanalysis of a large study on 167 major liver resections identified irinotecan-induced CASH as an independent risk factor forpostoperative mortality including death from liver failure.[58] Others have identified oxaliplatin-mediated SOS as a risk factor forpostoperative complications and prolonged hospital stay (Table 5). Administration of more than 6 cycles of oxaliplatin increasedthe risk of developing SOS and was associated with a poorer outcome.[65] Further observations suggest that prolongedadministration of chemotherapy over more than 9 to 12 cycles increases the rate of reoperations and prolonged hospitalstay.[66,67] An alternative to prolonged administration of chemotherapy may be the addition of cetuximab. In selected patients, arapid tumor response after cetuximab may reduce the number of cycles required for tumor downsizing.[28]
5-FU based alone
Sahajpal, 2007109 III 53 5FU 10 NA NA
5-FU based + oxaliplatin or irinotecan
Adam, 201046 III 169 IRI, OX 29 NA 11
Hubert, 2010110 III 100 FOLFOX 21 3 49
Nakano, 200864 III 90 OX, IRI 98 NA 73
Pawlik, 2007111 III 153 IRI, OX 27 4 10
Hewes, 2007112 III 25 OX 13 0 NA
Karoui, 2006113 III 45 OX 42 58 49
Vauthey, 200657 III 158 IRI, OX 9 8 5
Aloia, 200665 III 75 OX 13 NA 23
Yedibela, 2005114 III 32 OX 6 NA NA
Rubbia-Brandt, 200458 III 153 OX 49 NA 51
Adam, 200496 III 138 OX 38 NA 8
Parikh 2003115 III 61 IRI 13 NA NA
5-FU based + oxaliplatin in combination with irinotecan
Masi76 II 196 FOLFOXIRI 76 5 48
5-FU based + oxaliplatin or irinotecan + antibodies (bevacizumab orcetuximab/panitumumab)
Kishi, 201066 III 102 BEV, OX NA NA 5
Scoggins, 2009103 III 112 BEV, OX 17 15 NA
Adam, 200753 III 25 CET 16 NA 20
LOE indicates level of evidence; CX, chemotherapy; SH, steatohepatitis; SOS, sinusoidalobstruction syndrome; BEV, bevacizumab; CAP, capecitabine; CET, cetuximab; IRI, irinotecan; OX,oxaliplatin; 5FU, 5-fluorouracil; FOL, folinic acid (= leucovorin); FOLFOX, folinic acid, 5FU andoxaliplatin; FOLFIRI, folinic acid, 5FU and irinotecan; FOLOXIRI, folinic acid, 5FU and oxaliplatinand irinotecan; NA, not available.
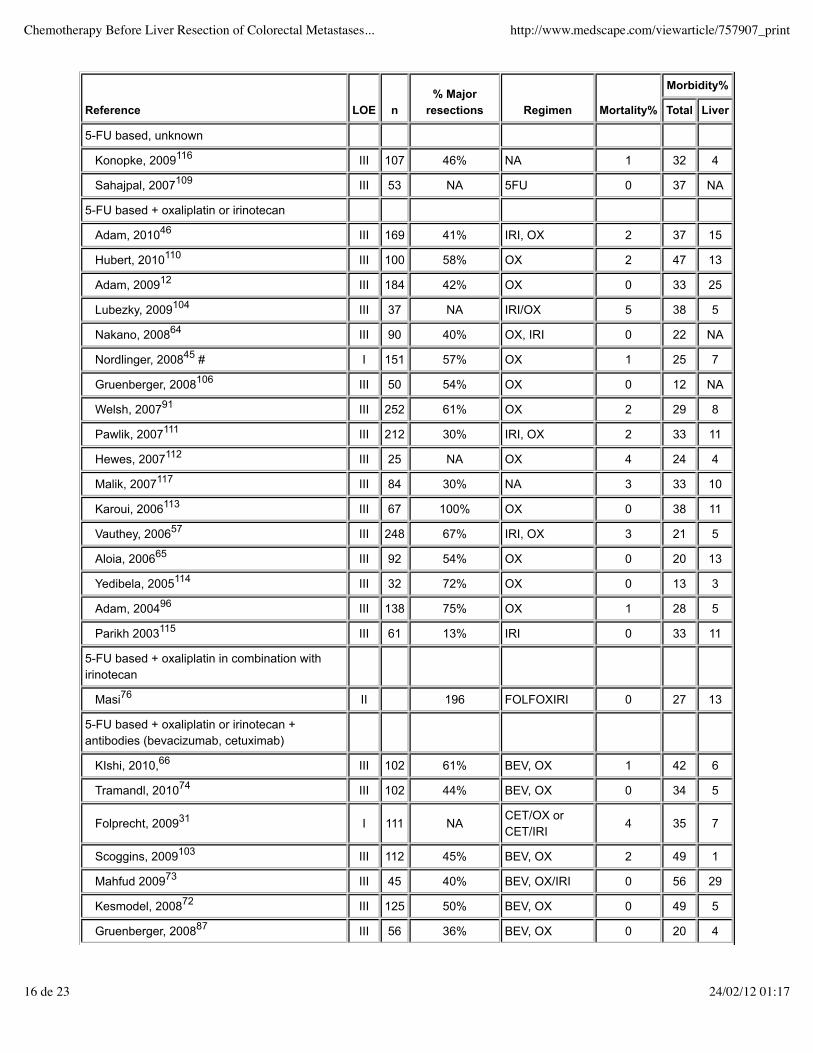
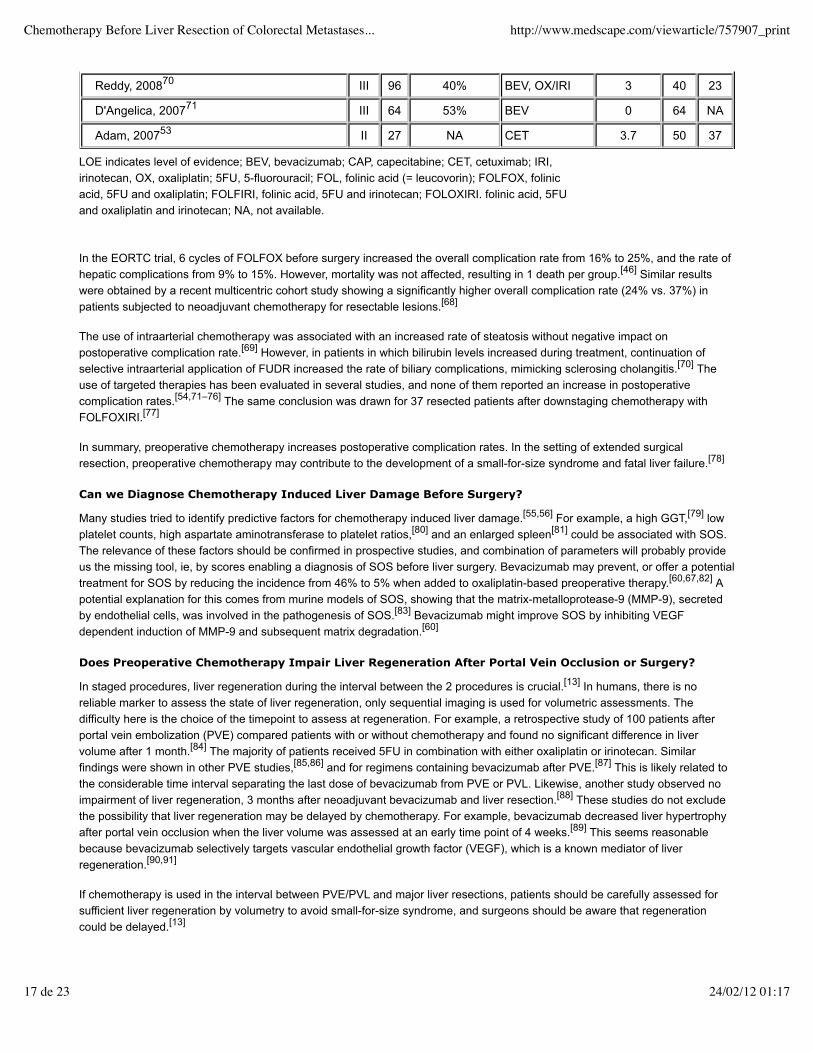
Table 5. Complications After Hepatectomy With Preoperative Chemotherapy
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
15 de 23 24/02/12 01:17
Reference LOE n% Major
resections Regimen Mortality%
Morbidity%
Total Liver
5-FU based, unknown
Konopke, 2009116 III 107 46% NA 1 32 4
Sahajpal, 2007109 III 53 NA 5FU 0 37 NA
5-FU based + oxaliplatin or irinotecan
Adam, 201046 III 169 41% IRI, OX 2 37 15
Hubert, 2010110 III 100 58% OX 2 47 13
Adam, 200912 III 184 42% OX 0 33 25
Lubezky, 2009104 III 37 NA IRI/OX 5 38 5
Nakano, 200864 III 90 40% OX, IRI 0 22 NA
Nordlinger, 200845 # I 151 57% OX 1 25 7
Gruenberger, 2008106 III 50 54% OX 0 12 NA
Welsh, 200791 III 252 61% OX 2 29 8
Pawlik, 2007111 III 212 30% IRI, OX 2 33 11
Hewes, 2007112 III 25 NA OX 4 24 4
Malik, 2007117 III 84 30% NA 3 33 10
Karoui, 2006113 III 67 100% OX 0 38 11
Vauthey, 200657 III 248 67% IRI, OX 3 21 5
Aloia, 200665 III 92 54% OX 0 20 13
Yedibela, 2005114 III 32 72% OX 0 13 3
Adam, 200496 III 138 75% OX 1 28 5
Parikh 2003115 III 61 13% IRI 0 33 11
5-FU based + oxaliplatin in combination withirinotecan
Masi76 II 196 FOLFOXIRI 0 27 13
5-FU based + oxaliplatin or irinotecan +antibodies (bevacizumab, cetuximab)
KIshi, 2010,66 III 102 61% BEV, OX 1 42 6
Tramandl, 201074 III 102 44% BEV, OX 0 34 5
Folprecht, 200931 I 111 NACET/OX orCET/IRI
4 35 7
Scoggins, 2009103 III 112 45% BEV, OX 2 49 1
Mahfud 200973 III 45 40% BEV, OX/IRI 0 56 29
Kesmodel, 200872 III 125 50% BEV, OX 0 49 5
Gruenberger, 200887 III 56 36% BEV, OX 0 20 4
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
16 de 23 24/02/12 01:17
In the EORTC trial, 6 cycles of FOLFOX before surgery increased the overall complication rate from 16% to 25%, and the rate ofhepatic complications from 9% to 15%. However, mortality was not affected, resulting in 1 death per group.[46] Similar resultswere obtained by a recent multicentric cohort study showing a significantly higher overall complication rate (24% vs. 37%) inpatients subjected to neoadjuvant chemotherapy for resectable lesions.[68]
The use of intraarterial chemotherapy was associated with an increased rate of steatosis without negative impact onpostoperative complication rate.[69] However, in patients in which bilirubin levels increased during treatment, continuation ofselective intraarterial application of FUDR increased the rate of biliary complications, mimicking sclerosing cholangitis.[70] Theuse of targeted therapies has been evaluated in several studies, and none of them reported an increase in postoperativecomplication rates.[54,71–76] The same conclusion was drawn for 37 resected patients after downstaging chemotherapy withFOLFOXIRI.[77]
In summary, preoperative chemotherapy increases postoperative complication rates. In the setting of extended surgicalresection, preoperative chemotherapy may contribute to the development of a small-for-size syndrome and fatal liver failure.[78]
Can we Diagnose Chemotherapy Induced Liver Damage Before Surgery?
Many studies tried to identify predictive factors for chemotherapy induced liver damage.[55,56] For example, a high GGT,[79] lowplatelet counts, high aspartate aminotransferase to platelet ratios,[80] and an enlarged spleen[81] could be associated with SOS.The relevance of these factors should be confirmed in prospective studies, and combination of parameters will probably provideus the missing tool, ie, by scores enabling a diagnosis of SOS before liver surgery. Bevacizumab may prevent, or offer a potentialtreatment for SOS by reducing the incidence from 46% to 5% when added to oxaliplatin-based preoperative therapy.[60,67,82] Apotential explanation for this comes from murine models of SOS, showing that the matrix-metalloprotease-9 (MMP-9), secretedby endothelial cells, was involved in the pathogenesis of SOS.[83] Bevacizumab might improve SOS by inhibiting VEGFdependent induction of MMP-9 and subsequent matrix degradation.[60]
Does Preoperative Chemotherapy Impair Liver Regeneration After Portal Vein Occlusion or Surgery?
In staged procedures, liver regeneration during the interval between the 2 procedures is crucial.[13] In humans, there is noreliable marker to assess the state of liver regeneration, only sequential imaging is used for volumetric assessments. Thedifficulty here is the choice of the timepoint to assess at regeneration. For example, a retrospective study of 100 patients afterportal vein embolization (PVE) compared patients with or without chemotherapy and found no significant difference in livervolume after 1 month.[84] The majority of patients received 5FU in combination with either oxaliplatin or irinotecan. Similarfindings were shown in other PVE studies,[85,86] and for regimens containing bevacizumab after PVE.[87] This is likely related tothe considerable time interval separating the last dose of bevacizumab from PVE or PVL. Likewise, another study observed noimpairment of liver regeneration, 3 months after neoadjuvant bevacizumab and liver resection.[88] These studies do not excludethe possibility that liver regeneration may be delayed by chemotherapy. For example, bevacizumab decreased liver hypertrophyafter portal vein occlusion when the liver volume was assessed at an early time point of 4 weeks.[89] This seems reasonablebecause bevacizumab selectively targets vascular endothelial growth factor (VEGF), which is a known mediator of liverregeneration.[90,91]
If chemotherapy is used in the interval between PVE/PVL and major liver resections, patients should be carefully assessed forsufficient liver regeneration by volumetry to avoid small-for-size syndrome, and surgeons should be aware that regenerationcould be delayed.[13]
Reddy, 200870 III 96 40% BEV, OX/IRI 3 40 23
D'Angelica, 200771 III 64 53% BEV 0 64 NA
Adam, 200753 II 27 NA CET 3.7 50 37
LOE indicates level of evidence; BEV, bevacizumab; CAP, capecitabine; CET, cetuximab; IRI,irinotecan, OX, oxaliplatin; 5FU, 5-fluorouracil; FOL, folinic acid (= leucovorin); FOLFOX, folinicacid, 5FU and oxaliplatin; FOLFIRI, folinic acid, 5FU and irinotecan; FOLOXIRI. folinic acid, 5FUand oxaliplatin and irinotecan; NA, not available.
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
17 de 23 24/02/12 01:17
When Can We Operate Patients Subjected to Chemotherapy?
In clinical practice, many patients with hepatic metastases from CRC receive chemotherapy before the evaluation by anexperienced liver surgeon. Caution is needed regarding the number of cycles beyond a certain threshold that will fail to improvethe response, but will elevate the likelihood of postoperative complications.[67] The improved safety of liver surgery after anextended pause after chemotherapy has been demonstrated in several studies.[92] The randomized EORTC trial, in which themean time to surgery was 4 weeks after the last cycle of FOLFOX, was associated with increased complications, but notmortality.[46] In the majority of patients, liver function tests normalize after a period of about 4 weeks.[93] Administration of anoxaliplatin-based therapy combined with bevacizumab seems to be safe, if surgery follows 5 weeks after the last dose ofbevacizumab.[73,88] Similar findings were obtained regarding wound healing in a population of patients with metastatic CRC.Wound healing was impaired during the bevacizumab treatment, but normal after discontinuation for at least 4 weeks.[94]
The level of evidence concerning the latency between the last drug application and liver resection is low. A reasonablerecommendation is to avoid prolonged exposure to chemotherapy for more than 9 cycles, and to stop chemotherapy 4 weeksbefore surgery.[13,73]
Conclusion
Taken together, the data indicates that for unresectable liver metastases, downsizing chemotherapy may offer a chance forsecondary resection in about a third of patients. Although the optimal regimen for this is still unclear, it seems reasonable to startwith 2 cytotoxic drugs (5FU with either oxaliplatin or irinotecan). If this strategy fails, adding an antibody (cetuximab), or HAI maybe an alternative in the absence of extrahepatic disease. In contrast, routine neoadjuvant chemotherapy cannot berecommended due to the increased risk of complications without clear benefit on survival. In patients with multiple, borderlineresectable tumors, neoadjuvant therapy may identify good responders with favorable tumor biology and thus a better outcome.
References
Manfredi S, Lepage C, Hatem C, et al. Epidemiology and management of liver metastases from colorectal cancer. AnnSurg. 2006;244(2):254–259.
1.
Wagner JS, Adson MA, Van Heerden JA, et al. The natural history of hepatic metastases from colorectal cancer. Acomparison with resective treatment. Ann Surg. 1984;199(5):502–508.
2.
Cummings LC, Payes JD, Cooper GS. Survival after hepatic resection in metastatic colorectal cancer: a population-basedstudy. Cancer. 2007;109(4):718–726.
3.
Rees M, Tekkis PP, Welsh FK, et al. Evaluation of long-term survival after hepatic resection for metastatic colorectalcancer: a multifactorial model of 929 patients. Ann Surg. 2008;247(1):125–135.
4.
Abdalla EK, Vauthey JN, Ellis LM, et al. Recurrence and outcomes following hepatic resection, radiofrequency ablation,and combined resection/ablation for colorectal liver metastases. Ann Surg. 2004;239(6):818–825; discussion 825–827.
5.
Choti MA, Sitzmann JV, Tiburi MF, et al. Trends in long-term survival following liver resection for hepatic colorectalmetastases. Ann Surg. 2002;235(6):759–766.
6.
Fernandez FG, Drebin JA, Linehan DC, et al. Five-year survival after resection of hepatic metastases from colorectalcancer in patients screened by positron emission tomography with F-18 fluorodeoxyglucose (FDG-PET). Ann Surg.2004;240(3):438–447; discussion 447–450.
7.
Pawlik TM, Scoggins CR, Zorzi D, et al. Effect of surgical margin status on survival and site of recurrence after hepaticresection for colorectal metastases. Ann Surg. 2005;241(5):715–722, discussion 722–724.
8.
Figueras J, Torras J, Valls C, et al. Surgical resection of colorectal liver metastases in patients with expanded indications:a single-center experience with 501 patients. Dis Colon Rectum. 2007;50(4):478–488.
9.
Belghiti J, Hiramatsu K, Benoist S, et al. Seven hundred forty-seven hepatectomies in the 1990s: an update to evaluatethe actual risk of liver resection. J Am Coll Surg. 2000;191(1):38–46.
10.
Breitenstein S, DeOliveira ML, Raptis DA, et al. Novel and simple preoperative score predicting complications followingliver resection in non-cirrhotic patients. Ann Surg. 2010 Nov;252(5):726–34.
11.
Adam R, Wicherts DA, de Haas RJ, et al. Patients with initially unresectable colorectal liver metastases: is there apossibility of cure? J Clin Oncol. 2009;27(11):1829–1835.
12.
Clavien PA, Petrowsky H, DeOliveira ML, et al. Strategies for safer liver surgery and partial liver transplantation. N Engl JMed. 2007;356(15):1545–1559.
13.
Chen ML, Fang CH, Liang LS, et al. A meta-analysis of chemotherapy regimen fluorouracil/leucovorin/oxaliplatin14.
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
18 de 23 24/02/12 01:17
compared with fluorouracil/leucovorin in treating advanced colorectal cancer. Surg Oncol. 2010;19(1):38–45.Saltz LB, Cox JV, Blanke C, et al. Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. IrinotecanStudy Group. N Engl J Med. 2000;343(13):905–914.
15.
Douillard JY, Cunningham D, Roth AD, et al. Irinotecan combined with fluorouracil compared with fluorouracil alone asfirst-line treatment for metastatic colorectal cancer: a multicentre randomised trial. Lancet. 2000;355(9209):1041–1047.
16.
de Gramont A, Figer A, Seymour M, et al. Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment inadvanced colorectal cancer. JClin Oncol. 2000;18(16):2938–2947.
17.
Giacchetti S, Perpoint B, Zidani R, et al. Phase III multicenter randomized trial of oxaliplatin added to chronomodulatedfluorouracil-leucovorin as first-line treatment of metastatic colorectal cancer. J Clin Oncol. 2000;18(1):136–147.
18.
Tabernero J, Van Cutsem E, Diaz-Rubio E, et al. Phase II trial of cetuximab in combination with fluorouracil, leucovorin,and oxaliplatin in the first-line treatment of metastatic colorectal cancer. J Clin Oncol. 2007;25(33):5225–5232.
19.
Saltz LB, Clarke S, Diaz-Rubio E, et al. Bevacizumab in combination with oxaliplatin-based chemotherapy as first-linetherapy in metastatic colorectal cancer: a randomized phase III study. J Clin Oncol. 2008;26(12):2013–2019.
20.
Portier G, Elias D, Bouche O, et al. Multicenter randomized trial of adjuvant fluorouracil and folinic acid compared withsurgery alone after resection of colorectal liver metastases: FFCD ACHBTH AURC 9002 trial. J Clin Oncol.2006;24(31):4976–4982.
21.
Adam R, Laurent A, Azoulay D, et al. Two-stage hepatectomy: a planned strategy to treat irresectable liver tumors. AnnSurg. 2000;232(6):777–785.
22.
Phillips B, Ball C, Sackett D, et al. Oxford Centre for Evidence-basedMedicine - Levels of Evidence (March 2009)[http://www.cebm.net/website]. 1998, 2009.
23.
Bokemeyer C, Bondarenko I,Makhson A, et al. Fluorouracil, leucovorin, and oxaliplatin with andwithout cetuximab in thefirst-line treatment of metastatic colorectal cancer. J Clin Oncol. 2009;27(5):663–671.
24.
Falcone A, Ricci S, Brunetti I, et al. Phase III trial of infusional fluorouracil, leucovorin, oxaliplatin, and irinotecan(FOLFOXIRI) compared with infusional fluorouracil, leucovorin, and irinotecan (FOLFIRI) as first-line treatment formetastatic colorectal cancer: the Gruppo Oncologico Nord Ovest. JClin Oncol. 2007;25(13):1670–1676.
25.
Delaunoit T,Alberts SR, Sargent DJ, et al. Chemotherapy permits resection of metastatic colorectal cancer: experiencefrom Intergroup N9741. Ann Oncol. 2005;16(3):425–429.
26.
Van Cutsem E, Kohne CH, Hitre E, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectalcancer. N Engl J Med. 2009;360(14):1408–1417.
27.
Piessevaux H. Early tumor shrinkage for the prediction of efficacy of cetuximab in metastatic colorectal cancer (MCRC):Analysis from the CRYSTAL study. ESMO abstract 596P 2010.
28.
Maughan TS, Adams R, Smith CG, et al. Identification of potentially responsive subsets when cetuximab is added tooxaliplatin-fluoropyrimidine chemotherapy (CT) in first-line advanced colorectal cancer (aCRC): Mature results of the MRCCOIN trial. J Clin Oncol (Meeting Abstracts). 2010;28(15_suppl):3502.
29.
De Roock W, Jonker DJ, Di Nicolantonio F, et al. Association of KRAS p. G13D mutation with outcome in patients withchemotherapy-refractory metastatic colorectal cancer treated with cetuximab. JAMA. 2010;304(16):1812–1820.
30.
De RoockW, Claes B, Bernasconi D, et al. Effects of KRAS, BRAF, NRAS, and PIK3CA mutations on the efficacy ofcetuximab plus chemotherapy in chemotherapy-refractory metastatic colorectal cancer: a retrospective consortiumanalysis. Lancet Oncol. 2010;11(8):753–762.
31.
Folprecht G, Gruenberger T, Bechstein WO, et al. Tumour response and secondary resectability of colorectal livermetastases following neoadjuvant chemotherapy with cetuximab: the CELIM randomised phase 2 trial. LancetOncol.2010;11(1):38–47.
32.
Douillard JY, Siena S, Cassidy J, et al. Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin,and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastaticcolorectal cancer: the PRIME study. J ClinOncol. 2010;28(31):4697–4705.
33.
Hecht JR, Mitchell E, Chidiac T, et al. A randomized phase IIIB trial of chemotherapy, bevacizumab, and panitumumabcompared with chemotherapy and bevacizumab alone for metastatic colorectal cancer. J Clin Oncol. 2009;27(5):672–680.
34.
Tol J, Koopman M, Cats A, et al. Chemotherapy, bevacizumab, and cetuximab in metastatic colorectal cancer. N Engl JMed. 2009;360(6):563–572.
35.
Kemeny N, Daly J, Reichman B, et al. Intrahepatic or systemic infusion of fluorodeoxyuridine in patients with livermetastases from colorectal carcinoma. A randomized trial. Ann Intern Med. 1987;107(4):459–465.
36.
Selzner N, Pestalozzi BC, Kadry Z, et al. Downstaging colorectal liver metastases by concomitant unilateral portal veinligation and selective intra-arterial chemotherapy. Br J Surg. 2006;93(5):587–592.
37.
Clavien PA, Selzner N, Morse M, et al. Downstaging of hepatocellular carcinoma and liver metastases from colorectal38.
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
19 de 23 24/02/12 01:17

cancer by selective intra-arterial chemotherapy. Surgery. 2002;131(4):433–442.Jaeck D, Oussoultzoglou E, Rosso E, et al. A two-stage hepatectomy procedure combined with portal vein embolization toachieve curative resection for initially unresectable multiple and bilobar colorectal liver metastases. AnnSurg.2004;240(6):1037–1049; discussion 1049–1051.
39.
Mocellin S, Pilati P, Lise M, et al. Meta-analysis of hepatic arterial infusion for unresectable liver metastases fromcolorectal cancer: the end of an era? JClin Oncol. 2007;25(35):5649–5654.
40.
Ducreux M, Ychou M, Laplanche A, et al. Hepatic arterial oxaliplatin infusion plus intravenous chemotherapy in colorectalcancer with inoperable hepatic metastases: a trial of the gastrointestinal group of the Federation Nationale des Centres deLutte Contre le Cancer. J Clin Oncol. 2005;23(22):4881–4887.
41.
Boige V, Malka D, Elias D, et al. Hepatic arterial infusion of oxaliplatin and intravenous LV5FU2 in unresectable livermetastases from colorectal cancer after systemic chemotherapy failure. Ann Surg Oncol. 2008;15(1):219–226.
42.
Goere D, Deshaies I, de Baere T, et al. Prolonged survival of initially unresectable hepatic colorectal cancer patientstreated with hepatic arterial infusion of oxaliplatin followed by radical surgery of metastases. Ann Surg.2010;251(4):686–691.
43.
Elias D, Goere D, Boige V, et al. Outcome of posthepatectomy-missing colorectal liver metastases after completeresponse to chemotherapy: impact of adjuvant intra-arterial hepatic oxaliplatin. Ann Surg Oncol. 2007;14(11):3188–3194.
44.
Auer RC, White RR,Kemeny NE, et al. Predictors of a true complete response among disappearing liver metastases fromcolorectal cancer after chemotherapy. Cancer. 2010;116(6):1502–1509.
45.
Nordlinger B, Sorbye H, Glimelius B, et al. Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alonefor resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): a randomised controlled trial.Lancet. 2008;371(9617):1007–1016.
46.
Adam R, Bhangui P, Poston G, et al. Is perioperative chemotherapy useful for solitary, metachronous, colorectal livermetastases? Ann Surg. 2010;252(5):774–787.
47.
Reddy SK, Zorzi D, Lum YW, et al. Timing of multimodality therapy for resectable synchronous colorectal livermetastases: a retrospective multi-institutional analysis. Ann Surg Oncol. 2009;16(7):1809–1819.
48.
Allen PJ,Kemeny N, Jarnagin W, et al. Importance of response to neoadjuvant chemotherapy in patients undergoingresection of synchronous colorectal liver metastases. J Gastrointest Surg. 2003;7(1):109–115; discussion 116–117.
49.
Adam R, Pascal G, Castaing D, et al. Tumor progression while on chemotherapy: a contraindication to liver resection formultiple colorectal metastases? Ann Surg. 2004;240(6):1052–1061; discussion 1061–1064.
50.
Blazer DG, 3rd, Kishi Y,Maru DM, et al. Pathologic response to preoperative chemotherapy: a new outcome end pointafter resection of hepatic colorectal metastases. J Clin Oncol. 2008;26(33):5344–5351.
51.
Mentha G, Terraz S, Morel P, et al. Dangerous halo after neoadjuvant chemotherapy and two-step hepatectomy forcolorectal liver metastases. Br JSurg. 2009;96(1):95–103.
52.
Benoist S, Brouquet A, Penna C, et al. Complete response of colorectal liver metastases after chemotherapy: does itmean cure? J Clin Oncol. 2006;24(24):3939–3945.
53.
Adam R, Aloia T, Levi F, et al. Hepatic resection after rescue cetuximab treatment for colorectal liver metastasespreviously refractory to conventional systemic therapy. J Clin Oncol. 2007;25(29):4593–4602.
54.
Zorzi D, Laurent A, Pawlik TM, et al. Chemotherapy-associated hepatotoxicity and surgery for colorectal liver metastases.Br J Surg. 2007;94(3):274–286.
55.
Morris-Stiff G, Tan YM, Vauthey JN. Hepatic complications following preoperative chemotherapy with oxaliplatin oririnotecan for hepatic colorectal metastases. Eur J Surg Oncol. 2008;34(6):609–614.
56.
Fong Y, Bentrem DJ. CASH (Chemotherapy-Associated Steatohepatitis) costs. Ann Surg. 2006;243(1):8–9.57.Vauthey JN, Pawlik TM, Ribero D, et al. Chemotherapy regimen predicts steatohepatitis and an increase in 90-daymortality after surgery for hepatic colorectal metastases. J Clin Oncol. 2006;24(13):2065–2072.
58.
Rubbia-Brandt L, Audard V, Sartoretti P, et al. Severe hepatic sinusoidal obstruction associated with oxaliplatin-basedchemotherapy in patients with metastatic colorectal cancer. Ann Oncol. 2004;15(3):460–466.
59.
Rubbia-Brandt L, Lauwers GY, Wang H, et al. Sinusoidal obstruction syndrome and nodular regenerative hyperplasia arefrequent oxaliplatin-associated liver lesions and partially prevented by bevacizumab in patients with hepatic colorectalmetastasis. Histopathology. 2010;56(4):430–439.
60.
Vetelainen R, van Vliet AK, van Gulik TM. Severe steatosis increases hepatocellular injury and impairs liver regenerationin a rat model of partial hepatectomy. Ann Surg. 2007;245(1):44–50.
61.
DeAngelis RA, Markiewski MM, Taub R, et al. A high-fat diet impairs liver regeneration in C57BL/6 mice throughoverexpression of the NF-kappaB inhibitor, IkappaBalpha. Hepatology. 2005;42(5):1148–1157.
62.
Ryan P, Nanji S, Pollett A, et al. Chemotherapy-induced liver injury in metastatic colorectal cancer: semiquantitative63.
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
20 de 23 24/02/12 01:17
histologic analysis of 334 resected liver specimens shows that vascular injury but not steatohepatitis is associated withpreoperative chemotherapy. Am J Surg Pathol. 2010;34(6):784–791.El-Badry AM, Breitenstein S, Jochum W, et al. Assessment of hepatic steatosis by expert pathologists: the end of a goldstandard. Ann Surg. 2009;250(5):691–697.
64.
Nakano H, Oussoultzoglou E, Rosso E, et al. Sinusoidal injury increases morbidity after major hepatectomy in patientswith colorectal liver metastases receiving preoperative chemotherapy. Ann Surg. 2008;247(1):118–124.
65.
AloiaT, SebaghM, Plasse M, et al.Liver histology and surgical outcomes after preoperative chemotherapy with fluorouracilplus oxaliplatin in colorectal cancer liver metastases. J Clin Oncol. 2006;24(31):4983–4990.
66.
Kishi Y, Zorzi D, Contreras CM, et al. Extended preoperative chemotherapy does not improve pathologic response andincreases postoperative liver insufficiency after hepatic resection for colorectal liver metastases. Ann SurgOncol. 2010Nov;17(11):2870–6.
67.
Adam R, Bhangui P, Poston G, et al. Is perioperative chemotherapy useful for metachronous solitary colorectal livermetastases? Ann Surg. 2010 Nov;252(5):774–87.
68.
Tanaka K, Shimada H, Ueda M, et al. Perioperative complications after hepatectomy with or without intra-arterialchemotherapy for bilobar colorectal cancer liver metastases. Surgery. 2006;139(5):599–607.
69.
Barnett KT, Malafa MP. Complications of hepatic artery infusion: a review of 4580 reported cases. Int J GastrointestCancer. 2001;30(3):147–160.
70.
Reddy SK, Morse MA, Hurwitz HI, et al. Addition of bevacizumab to irinotecan- and oxaliplatin-based preoperativechemotherapy regimens does not increase morbidity after resection of colorectal liver metastases. J AmColl Surg.2008;206(1):96–106.
71.
D'Angelica M, Kornprat P, Gonen M, et al. Lack of evidence for increased operative morbidity after hepatectomy withperioperative use of bevacizumab: a matched case-control study. Ann Surg Oncol. 2007;14(2):759–765.
72.
Kesmodel SB, Ellis LM, Lin E, et al. Preoperative bevacizumab does not significantly increase postoperative complicationrates in patients undergoing hepatic surgery for colorectal cancer liver metastases. J Clin Oncol. 2008;26(32):5254–5260.
73.
Mahfud M, Breitenstein S, El-Badry AM, et al. Impact of preoperative bevacizumab on complications after resection ofcolorectal liver metastases: case-matched control study. World J Surg. 2010;34(1):92–100.
74.
Tamandl D, Gruenberger B, Klinger M, et al. Liver resection remains a safe procedure after neoadjuvant chemotherapyincluding bevacizumab: a case-controlled study. Ann Surg. 2010;252(1):124–130.
75.
Folprecht G, Gruenberger T, Bechstein WO, et al. Tumour response and secondary resectability of colorectal livermetastases following neoadjuvant chemotherapy with cetuximab: the CELIM randomised phase 2 trial. LancetOncol.2010 Jan;11(1):38–47.
76.
Masi G, Loupakis F, Pollina L, et al. Long-term outcome of initially unresectable metastatic colorectal cancer patientstreated with 5-fluorouracil/leucovorin, oxaliplatin, and irinotecan (FOLFOXIRI) followed by radical surgery of metastases.Ann Surg. 2009;249(3):420–425.
77.
Clavien PA, Oberkofler CE, Raptis DA, et al. What is critical for liver surgery and partial liver transplantation: size orquality? Hepatology. 2010;52(2):715–729.
78.
BrouquetA,Benoist S, Julie C, et al. Risk factors for chemotherapy-associated liver injuries: amultivariate analysis of agroup of 146 patients with colorectal metastases. Surgery. 2009;145(4):362–371.
79.
Soubrane O, Brouquet A, Zalinski S, et al. Predicting high grade lesions of sinusoidal obstruction syndrome related tooxaliplatin-based chemotherapy for colorectal liver metastases: correlation with post-hepatectomy outcome. Ann Surg.2010;251(3):454–460.
80.
Overman MJ, Maru DM, Charnsangavej C, et al. Oxaliplatin-mediated increase in spleen size as a biomarker for thedevelopment of hepatic sinusoidal injury. J Clin Oncol. 2010;28(15):2549–2555.
81.
Ribero D, Wang H, Donadon M, et al. Bevacizumab improves pathologic response and protects against hepatic injury inpatients treated with oxaliplatin-based chemotherapy for colorectal liver metastases. Cancer. 2007;110(12):2761–2767.
82.
Deleve LD, Wang X, Tsai J, et al. Sinusoidal obstruction syndrome (venoocclusive disease) in the rat is prevented bymatrix metalloproteinase inhibition. Gastroenterology. 2003;125(3):882–890.
83.
Covey AM, Brown KT, Jarnagin WR, et al. Combined portal vein embolization and neoadjuvant chemotherapy as atreatment strategy for resectable hepatic colorectal metastases. Ann Surg. 2008;247(3):451–455.
84.
Goere D, Farges O, Leporrier J, et al. Chemotherapy does not impair hypertrophy of the left liver after right portal veinobstruction. J Gastrointest Surg. 2006;10(3):365–370.
85.
Giraudo G, Greget M, Oussoultzoglou E, et al. Preoperative contralateral portal vein embolization before major hepaticresection is a safe and efficient procedure: a large single institution experience. Surgery. 2008;143(4):476–482.
86.
Zorzi D, Chun YS, Madoff DC, et al. Chemotherapy with bevacizumab does not affect liver regeneration after portal vein87.
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
21 de 23 24/02/12 01:17
embolization in the treatment of colorectal liver metastases. Ann Surg Oncol. 2008;15(10):2765–2772.Gruenberger B, Tamandl D, Schueller J, et al. Bevacizumab, capecitabine, and oxaliplatin as neoadjuvant therapy forpatients with potentially curable metastatic colorectal cancer. J Clin Oncol. 2008;26(11):1830–1835.
88.
Aussilhou B, Dokmak S, Faivre S, et al. Preoperative liver hypertrophy induced by portal flow occlusion before majorhepatic resection for colorectal metastases can be impaired by bevacizumab. Ann Surg Oncol. 2009;16(6):1553–1559.
89.
Taniguchi E, Sakisaka S, Matsuo K, et al. Expression and role of vascular endothelial growth factor in liver regenerationafter partial hepatectomy in rats. J Histochem Cytochem. 2001;49(1):121–130.
90.
Drixler TA, Vogten MJ, Ritchie ED, et al. Liver regeneration is an angiogenesis- associated phenomenon. Ann Surg.2002;236(6):703–711; discussion 711–712.
91.
Welsh FK, Tilney HS, Tekkis PP, et al. Safe liver resection following chemotherapy for colorectal metastases is a matter oftiming. Br J Cancer. 2007;96(7):1037–1042.
92.
Takamoto T, Hashimoto T, Sano K, et al. Recovery of liver function after the cessation of preoperative chemotherapy forcolorectal liver metastasis. AnnSurg Oncol. 2010;17(10):2747–2755.
93.
Scappaticci FA, Fehrenbacher L, Cartwright T, et al. Surgical wound healing complications in metastatic colorectal cancerpatients treated with bevacizumab. J Surg Oncol. 2005;91(3):173–180.
94.
Wein A, Riedel C, Kockerling F, et al. Impact of surgery on survival in palliative patients with metastatic colorectal cancerafter first line treatment with weekly 24-hour infusion of high-dose 5-fluorouracil and folinic acid. Ann Oncol.2001;12(12):1721–7.
95.
Chun YS, Vauthey JN, Ribero D, et al. Systemic chemotherapy and two-stage hepatectomy for extensive bilateralcolorectal liver metastases: perioperative safety and survival. J Gastrointest Surg. 2007;11(11):1498–504; discussion1504–5.
96.
Adam R, Delvart V, Pascal G, et al. Rescue surgery for unresectable colorectal liver metastases downstaged bychemotherapy: a model to predict long-term survival. Ann Surg. 2004;240(4):644–57; discussion 657–8.
97.
Teufel A, Steinmann S, Siebler J, et al. Irinotecan plus folinic acid/continuous 5-fluorouracil as simplified bimonthlyFOLFIRI regimen for first-line therapy of metastatic colorectal cancer. BMC Cancer. 2004;4:38.
98.
Tanaka K, Adam R, Shimada H, et al. Role of neoadjuvant chemotherapy in the treatment of multiple colorectalmetastases to the liver. Br J Surg. 2003;90(8):963–9.
99.
Bismuth H, Adam R, Levi F, et al. Resection of nonresectable liver metastases from colorectal cancer after neoadjuvantchemotherapy. Ann Surg. 1996;224(4):509–20.
100.
Masi G, Cupini S, Marcucci L, et al. Treatment with 5-fluorouracil/folinic acid, oxaliplatin, and irinotecan enables surgicalresection of metastases in patients with initially unresectable metastatic colorectal cancer. Ann SurgOncol.2006;13(1):58–65.
101.
Bathe OF, Ernst S, Sutherland FR, et al. A phase II experience with neoadjuvant irinotecan (CPT-11), 5-fluorouracil (5-FU)and leucovorin (LV) for colorectal liver metastases. BMC Cancer. 2009;9:156.
102.
Tamandl D, Gruenberger B, Herberger B, et al. Surgery after neoadjuvant chemotherapy for colorectal liver metastases issafe and feasible in elderly patients. J Surg Oncol. 2009;100(5):364–71.
103.
Scoggins CR, Campbell ML, Landry CS, et al. Preoperative chemotherapy does not increase morbidity or mortality ofhepatic resection for colorectal cancer metastases. Ann Surg Oncol. 2009;16(1):35–41.
104.
Lubezky N, Ben-Haim M, Nakache R, et al. Clinical presentation can predict disease course in patients with intraductalpapillary mucinous neoplasm of the pancreas. World J Surg. 2010;34(1):126–32.
105.
Gallagher DJ, Zheng J, CapanuM, et al. Response to neoadjuvant chemotherapy does not predict overall survival forpatients with synchronous colorectal hepatic metastases. Ann Surg Oncol. 2009;16(7):1844–51.
106.
Gruenberger B, ScheithauerW, Punzengruber R, et al. Importance of response to neoadjuvant chemotherapy inpotentially curable colorectal cancer liver metastases. BMC Cancer. 2008;8:120.
107.
Wein A, Riedel C, Bruckl W, et al. Neoadjuvant treatment with weekly highdose 5-Fluorouracil as 24-hour infusion, folinicacid and oxaliplatin in patients with primary resectable livermetastases of colorectal cancer. Oncology. 2003;64(2):131–8.
108.
Small RM, Lubezky N, Shmueli E, et al. Response to chemotherapy predicts survival following resection of hepaticcolo-rectal metastases in patients treated with neoadjuvant therapy. J Surg Oncol. 2009;99(2):93–8.
109.
Sahajpal A, Vollmer CM, Jr., Dixon E, et al. Chemotherapy for colorectal cancer prior to liver resection for colorectalcancer hepatic metastases does not adversely affect peri-operative outcomes. J Surg Oncol. 2007;95(1):22–7.
110.
Hubert C, Fervaille C, Sempoux C, et al. Prevalence and clinical relevance of pathological hepatic changes occurring afterneoadjuvant chemotherapy for colorectal liver metastases. Surgery. 2010;147(2):185–94.
111.
Pawlik TM, Olino K, Gleisner AL, et al. Preoperative chemotherapy for colorectal liver metastases: impact on hepatichistology and postoperative outcome. J Gastrointest Surg. 2007;11(7):860–8.
112.
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
22 de 23 24/02/12 01:17

K.L. and A.R. contributed equally to this manuscript.
AcknowledgmentsWe would like to thank Dr. Bostjan Humar for his excellent input.
Annals of Surgery. 2012;255(2):237-247. © 2012 Lippincott Williams & Wilkins
Hewes JC, Dighe S, Morris RW, et al. Preoperative chemotherapy and the outcome of liver resection for colorectalmetastases. World J Surg. 2007;31(2):353–64; discussion 365–6.
113.
Karoui M, Penna C, Amin-Hashem M, et al. Influence of preoperative chemotherapy on the risk of major hepatectomy forcolorectal liver metastases. Ann Surg. 2006;243(1):1–7.
114.
Yedibela S, Elad L, Wein A, et al. Neoadjuvant chemotherapy does not increase postoperative complication rate afterresection of colorectal liver metastases. Eur J Surg Oncol. 2005;31(2):141–6.
115.
Parikh AA, Gentner B, Wu TT, et al. Perioperative complications in patients undergoing major liver resection with orwithout neoadjuvant chemotherapy. J Gastrointest Surg. 2003;7(8):1082–8.
116.
Konopke R, Kersting S, Bunk A, et al. Colorectal liver metastasis surgery: analysis of risk factors predicting postoperativecomplications in relation to the extent of resection. Int J Colorectal Dis. 2009;24(6):687–97.
117.
Malik HZ, Farid S, Al-Mukthar A, et al. A critical appraisal of the role of neoadjuvant chemotheraphy for colorectal livermetastases: a case-controlled study. Ann Surg Oncol 2007;14(2):3519–26.
118.
Chemotherapy Before Liver Resection of Colorectal Metastases... http://www.medscape.com/viewarticle/757907_print
23 de 23 24/02/12 01:17