chest tube
DESCRIPTION
Chest Tube. prepared by : Sana’a AL-Sulami Teacher Assistant Nursing Department. Outlines:. Definition Chest tube indication Purpose of chest insertion Sites for tube insertion types of drainage system Prepare the patient for chest tube insertion Performance chest tube procedure - PowerPoint PPT PresentationTRANSCRIPT
prepared by : Sana’a AL-SulamiTeacher AssistantNursing Department
Outlines:DefinitionChest tube indicationPurpose of chest insertionSites for tube insertiontypes of drainage systemPrepare the patient for chest tube insertionPerformance chest tube procedure Risks and complications
Learning objectives:At the end of this procedure , the students must be
able to :Define the chest tube.List of Chest tube indicationList of the Purpose of chest insertionDescribe the Sites for tube insertionDiscuss the types of drainage systemDescribe how to Prepare the patient for chest tube
insertionPerformance chest tube procedure List of the Risks and complications
Definition:
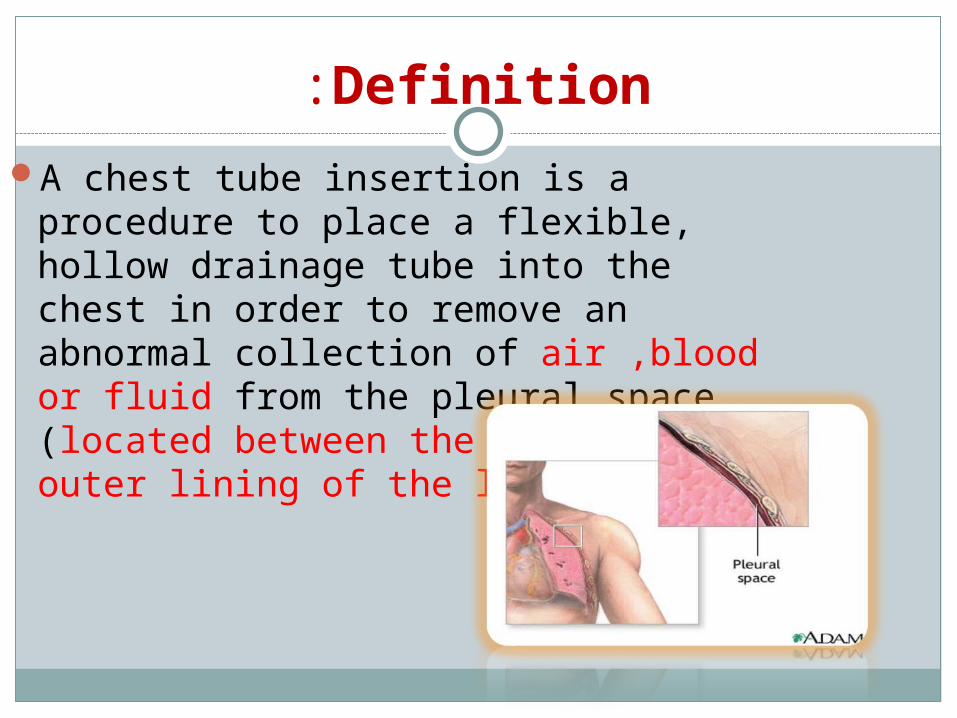
A chest tube insertion is a procedure to place a flexible, hollow drainage tube into the chest in order to remove an abnormal collection of air ,blood or fluid from the pleural space (located between the inner and outer lining of the lung).
Definition:
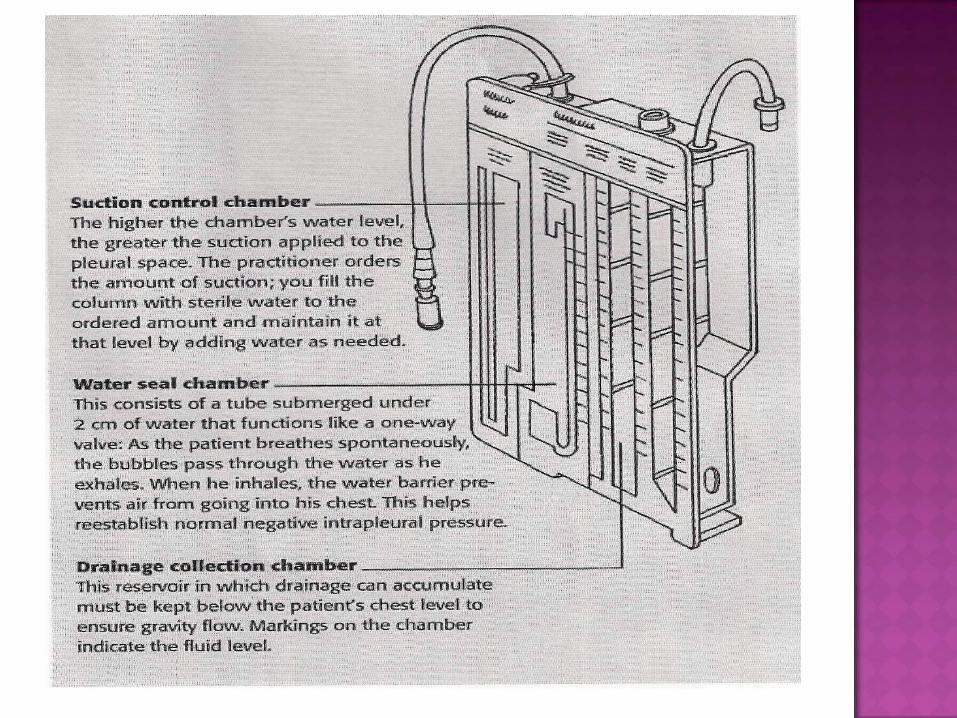
Traditional chest drainage unit consists of a collection chamber, water seal chamber, and suction control chamber.
Depending on circumstances, the practitioner may insert a chest tube at the bed side or send the patient to the operating room.
Pneumothorax. Hemothorax. Pleural effusion. Chylothorax. Empyema. Hemopnemothorax.
To return negative pressure to the intra pleural space.
To drain air from intra pleural space. To drain blood and fluid from intra
pleural space. Chest tube can administer therapy. Relieve respiratory distress.
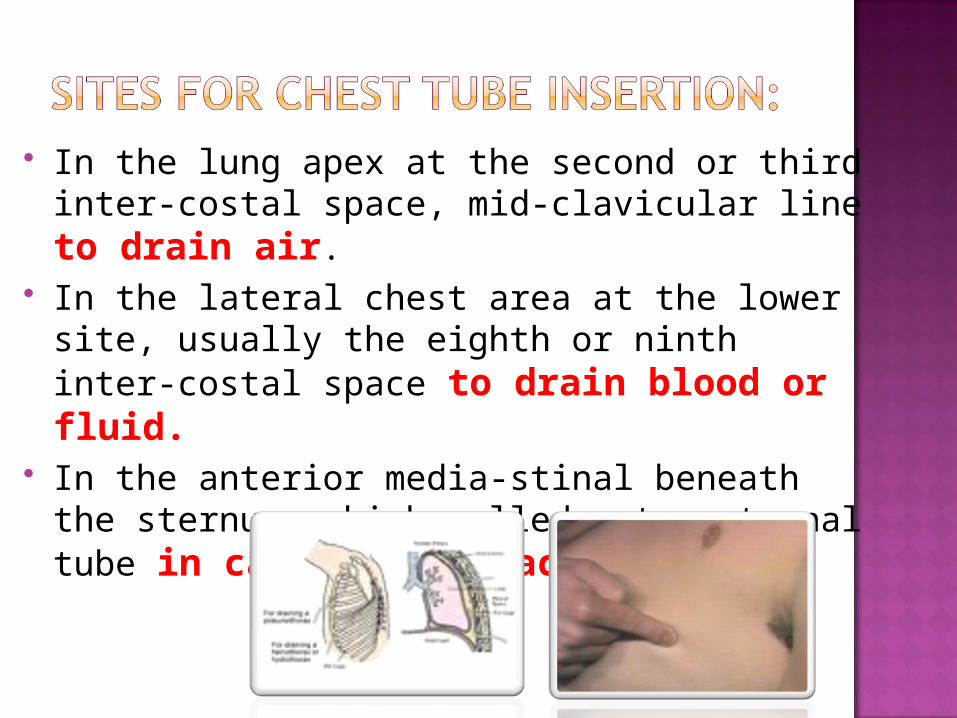
In the lung apex at the second or third inter-costal space, mid-clavicular line to drain air.
In the lateral chest area at the lower site, usually the eighth or ninth inter-costal space to drain blood or fluid.
In the anterior media-stinal beneath the sternum, which called retro-sternal tube in case of cardiac surgery.
Types of drainage system :Thoracentesis is insertion of the needle
into the pleural space to drain air or fluid.The single bottle system is used to drain
air or small amounts of fluid from the pleural space.
Two chamber system work as a single-bottle chest drainage system, but it decrease the workload of breath.
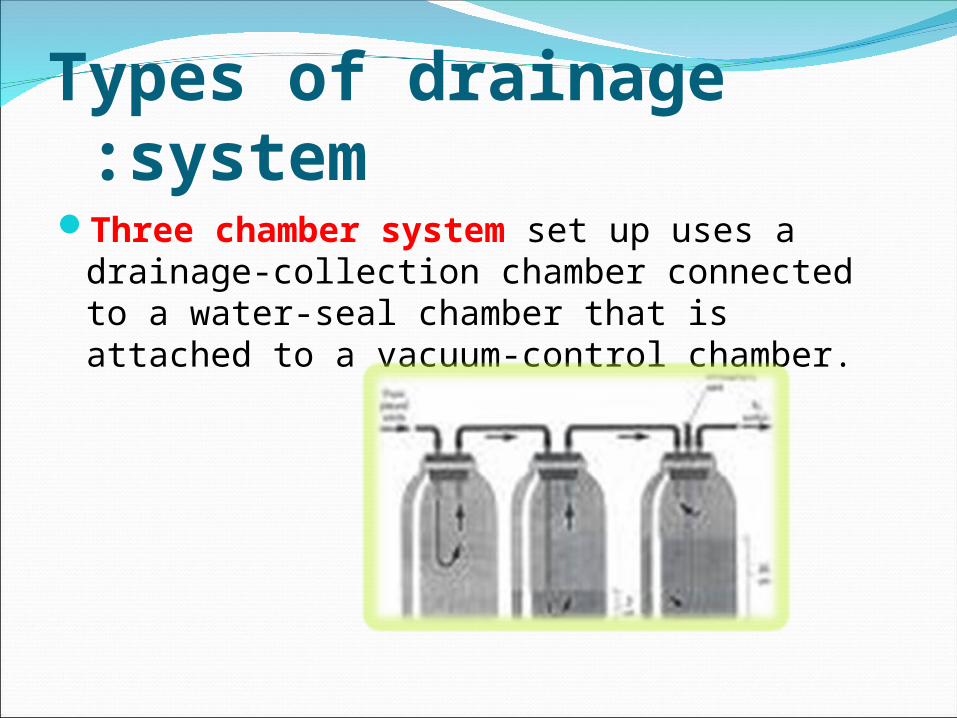
Types of drainage system :Three chamber system set up uses a
drainage-collection chamber connected to a water-seal chamber that is attached to a vacuum-control chamber.
Prepare the patient for chest tube insertion:
Make sure your patient has given informed consent.
Reinforce the practitioner’s explanation of the procedure with him and his family.
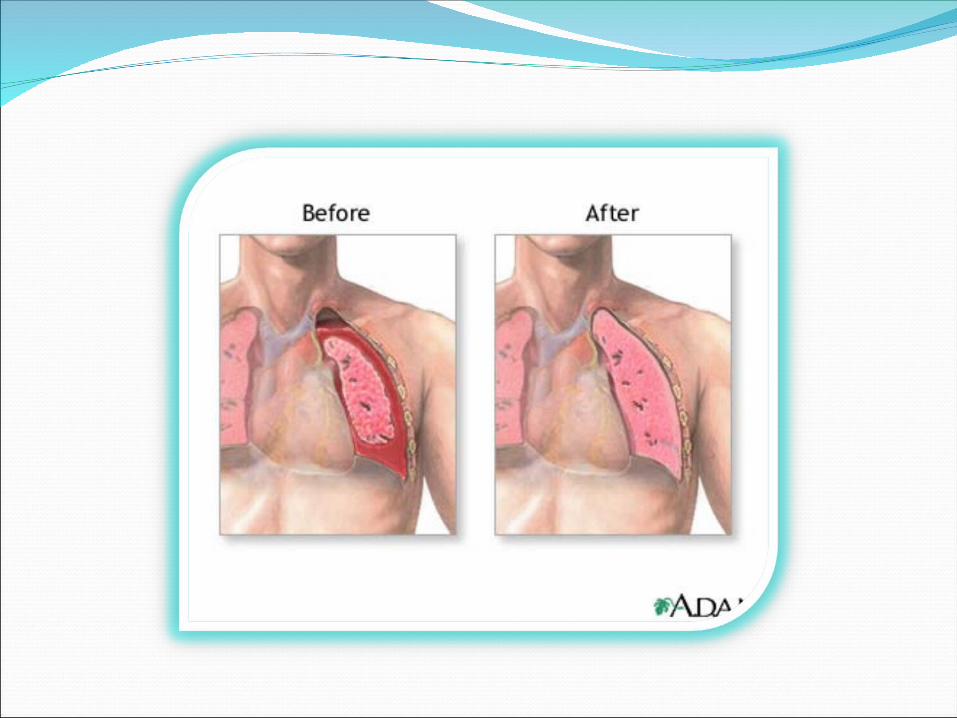
Explain that his breathing will be easier once the tube is inserted and his lung starts to re-expand.
Tell him he will receive a local anesthetic to reduce discomfort.
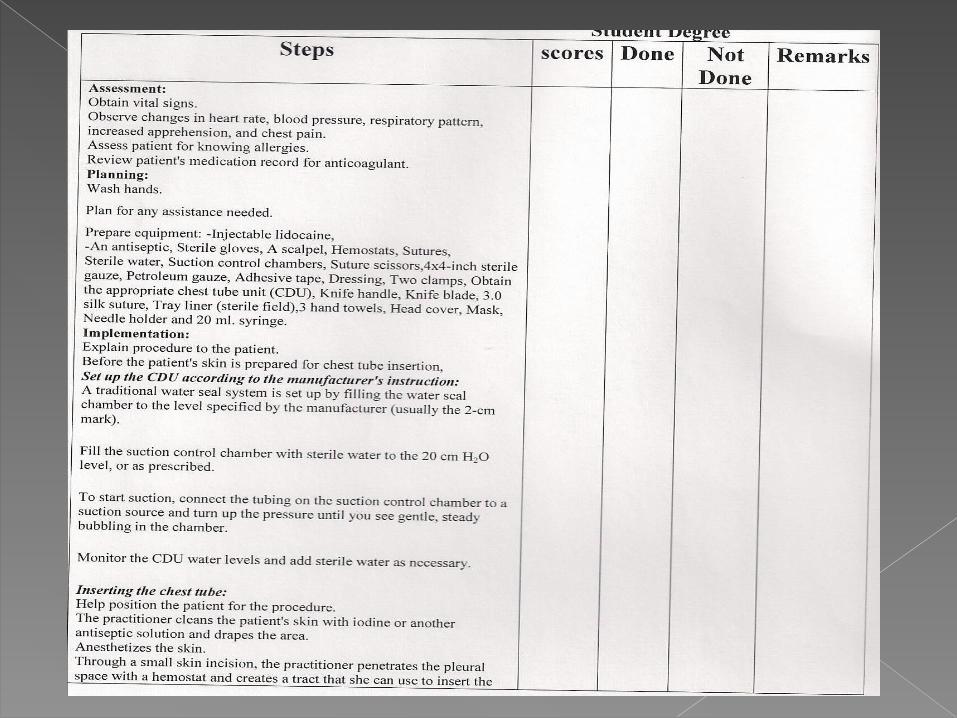
Performance chest tube procedure:
Assessment: Obtain vital signs Observe any changes in heart
rate, blood pressure, respiratory pattern, increased apprehension, and chest pain.
Assess patient for knowing allergies.
Review patient’s medication record for anticoagulant.
Performance chest tube procedure:
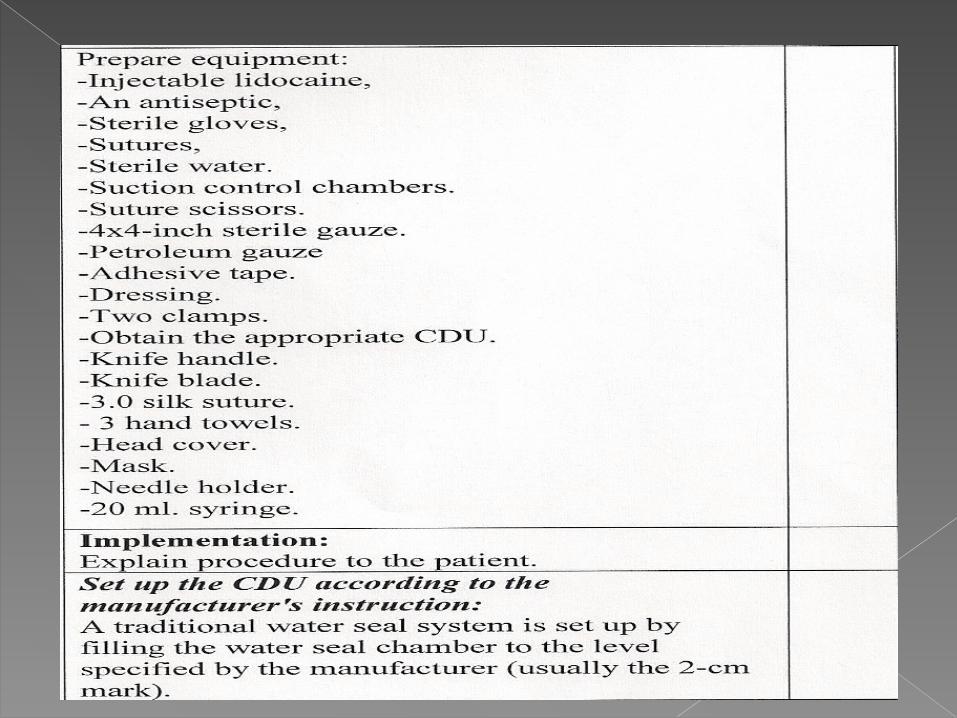
Planning: Wash hands. Prepare the equipment:
Injectable lidocaine An antiseptic Sterile gloves Sutures Sterile water Suction control
chambers Suture scissors 4*4 inch sterile gauze Petroleum gauze Adhesive tapeH
Dressing Two clamps Obtain the appropriate
CDU Knife handle Knife blade 3.0 silk suture 3 hand towels Head cover Mask Needle holder 20 ml syringe
Implementation:Explain procedure to the patient.Set up the CDU to the manufacturer’s structure.Fill the suction control chamber with sterile
water to the 20 cm H2O level, or as prescribed.To start suction, connect the tubing on the
suction control chamber to a suction source and turn up the pressure until you see gentle, steady bubbling in the chamber.
Monitor the CDU water levels and add sterile water as necessary.
Help position the patient for the procedure. The practitioner cleans the patient’s skin
with iodine or other antiseptic solution and drapes the area.
The practitioners anesthetizes the skin. Through a small skin incision, the
practitioner penetrate the pleural space with a hemostat and creates a tract that she can use to insert the catheter.
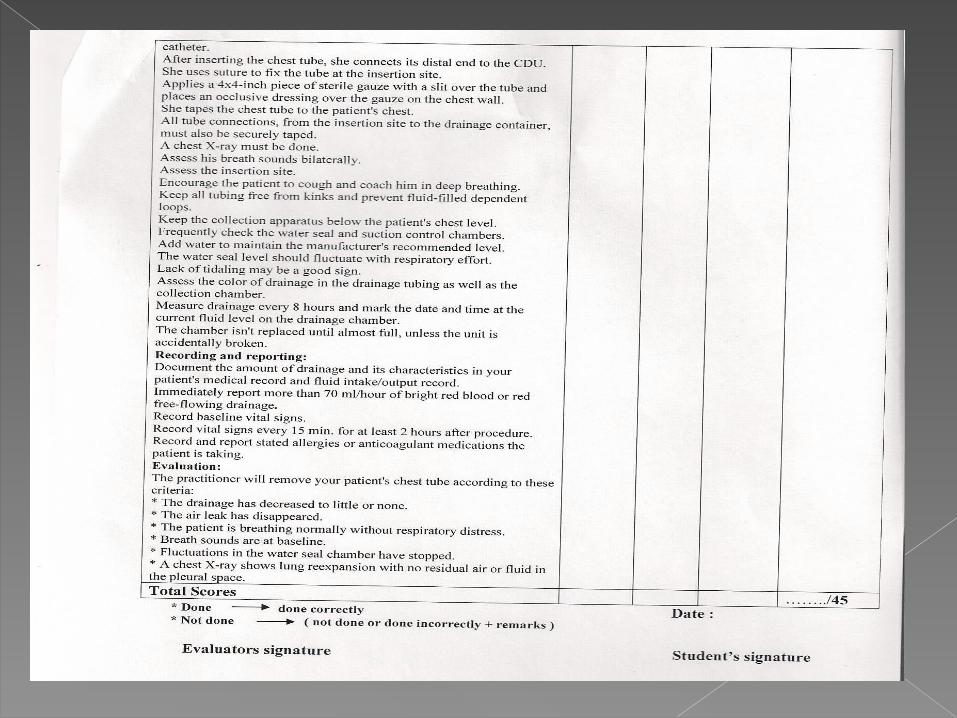
Connects its distal end to the CDU. Uses suture to fix the tube at the
insertion site. Applies 4*4 inch piece of sterile gauze
with a slit over the tube and places an occlusive dressing over the gauze on the chest wall.
Chest x-ray must be done. Assess his breath sounds bilaterally. Encourage the patient to cough and coach him in deep breathing.
Keeps all tubes free from kinks. Keep the collection apparatus below the
patient’s chest level Add water to maintain the manufacturer's
recommended level. The water seal level should fluctuate with
respiratory effort. Assess the color of drainage in the drainage
tubing as well as the collection chamber. Measure the drainage level every 8 hours.
Recording and Reporting:Document the amount of drainage and its
characteristics in your patient’s medical record.Immediately report more than 70 ml/hour of
bright red blood or red free – flowing drainage.Record baseline vital signs.(record vital signs
every 15 min. for at least 2 hours after procedure).
Record and report stated allergies or anticoagulant medications the patient is taking.
Ensure the tubing is not kinked.Gently milk the tubing in the direction of the
drainage system.Maintain drainage system below the level of
the chest.Turn the client frequently. Report drainage on the dressing
immediately .Observe for fluctuation of the fluid in tube .Palpate the area around the chest tube
insertion site.
situate the drainage system to avoid breakage.
Place tow clamps at the bedside .Encourage the client to coughing and
deep breathing every 2 hours.Instruct the client to exhale or strain as
the tube withdrawn by the physician.Encourage movement of the arm on the
affected side.Evaluation the client.
Evaluation:Practitioner will remove patient’s chest tube
according to:The drainage has decreased to little amount or
none.The patient is breathing normally without
respiratory distress.Breath sounds are at baseline.Fluctuations in the water seal have stopped.Chest x-ray shows lung re-expansion with no
residual air or fluid in the pleural space.
Place the patient in semi-fowler’s position or on his unaffected side.
Place a linen saver pad under the affected side .
Put on clean gloves and remove the chest tube dressings. discard the soiled linen.
The physician puts on sterile gloves holds the chest tube in place with sterile forceps , and cuts suture anchoring the tube.
Make sure the chest tube is securely clamped, and instruct the patient to perform Valsalv’s maneuver
The physician holds airtight dressing, usually petroleum gauze , he can cover the insertion site immediately after removing the tube.
Dispose the chest tube, soiled gloves, and equipment according to your facility’s policy.
Take the vital signs as ordered and assess the depth and quality of the patient’s respiration.

Risks and Complications:Bleeding.Infection.Subcutaneous emphysema.Other rare potential include lung trauma,
broncho-pleural fistula.
