chest wall resection and reconstruction for non small-cell lung cancer
TRANSCRIPT
CRB
CastboevTtpt
ow
G
A
1d
hest Wall Resection andeconstruction for Non-Small-Cell Lung Cancer
enjamin D. Kozower, MD
rqlcaq
atpptaMmMIospc
hest wall involvement occurs in less than 8% of patientswith newly diagnosed non-small-cell lung cancer. In the
bsence of metastatic spread, en-bloc anatomic surgical re-ection of the involved lung and chest wall is the primaryreatment for most patients. These lesions are T3 tumors and,ecause of the favorable survival following surgical resectionf T3N0 tumors, they have been reclassified as stage IIB dis-ase.1 If lymph node involvement is present, the overall sur-ival following resection of T3 tumors is reduced such that3 N1 to 2 tumors remain in the stage IIIA category. Factors
hat influence survival in this group of patients include com-leteness of resection, the extent of chest wall invasion, andhe presence of regional lymph node metastasis.2,3
Controversy exists regarding the significance of the depthf penetration and whether or not en-bloc resection of chestall (versus parietal pleura only) is required for adequate
eneral Thoracic Surgery, University of Virginia Health System, Charlottes-ville, Virginia.
ddress reprint requests to Benjamin D. Kozower, MD, Assistant Professorof Surgery, General Thoracic Surgery, University of Virginia HealthSystem, Box 800679, Charlottesville, VA 22908-0679. E-mail: bdk8g@
svirginia.edu
522-2942/07/$-see front matter © 2007 Elsevier Inc. All rights reserved.oi:10.1053/j.optechstcvs.2007.10.002
esection.4 There are no randomized data to answer thisuestion and surgeons use their personal experience and
arge published series to guide their practice. Because thehest wall resection typically adds minimal morbidity, mypproach has been to do a chest wall resection if there is anyuestion of achieving a complete resection.The need for chest wall reconstruction depends on the size
nd location of the defect. The main reasons to reconstructhe chest wall are to protect vital underlying structures and torevent paradoxical chest wall motion and respiratory com-romise. For defects greater than three ribs or 5 cm, someype of chest wall reconstruction is usually warranted. Fornterior defects with chest wall instability, a combination ofarlex (Marlex Pharmaceuticals, New Castle, DE) andethyl methacrylate works well.5 For posterior defects, a tautarlex mesh or a Gore-Tex patch (W.L. Gore & Associates,
nc, Elkton, MD) closure is adequate. Very small defects ofne to two ribs, or defects located posteriorly beneath thecapula, usually do not require reconstruction. However, if aosterior chest wall resection extends to the fifth rib or lower,hest wall reconstruction should be performed to prevent the
capula from caving into the chest.279
Fw(atIamdsptitnefichrbm
280 B.D. Kozower
Operative Technique
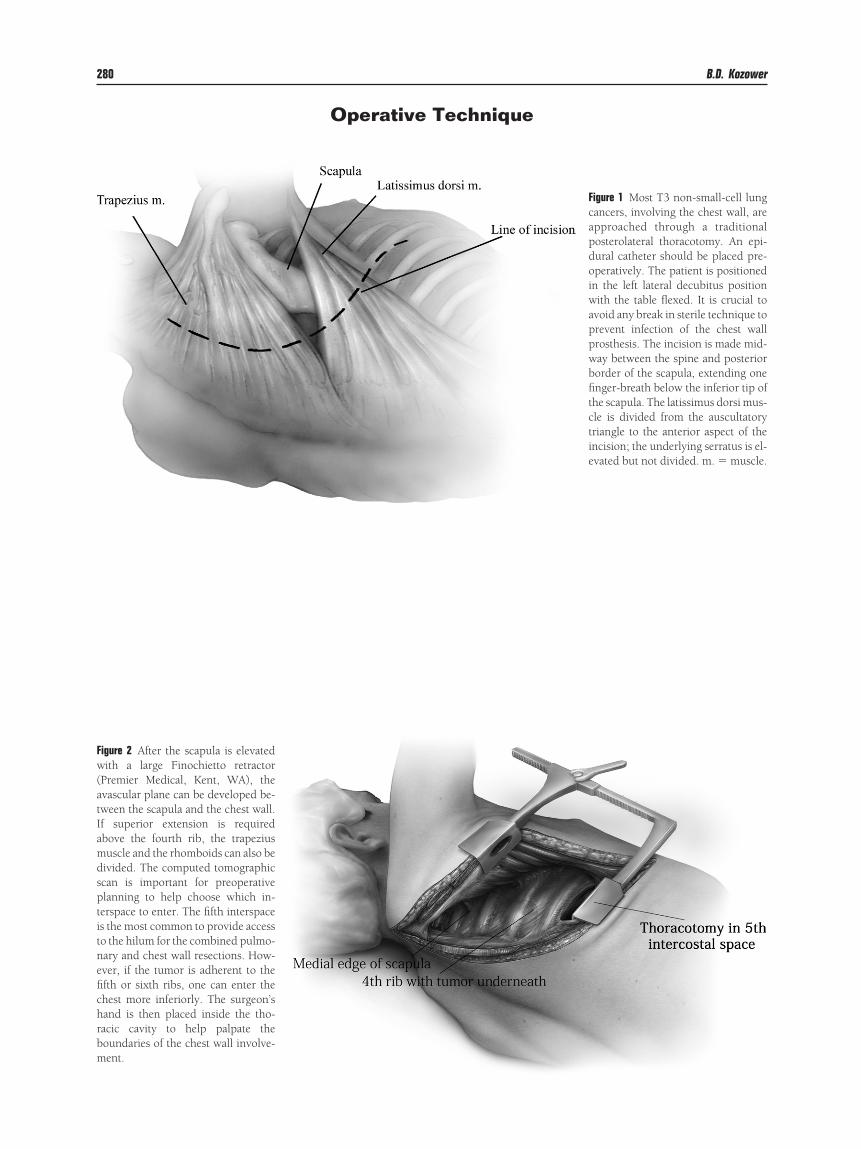
igure 2 After the scapula is elevatedith a large Finochietto retractor
Premier Medical, Kent, WA), thevascular plane can be developed be-ween the scapula and the chest wall.f superior extension is requiredbove the fourth rib, the trapeziususcle and the rhomboids can also be
ivided. The computed tomographiccan is important for preoperativelanning to help choose which in-erspace to enter. The fifth interspaces the most common to provide accesso the hilum for the combined pulmo-ary and chest wall resections. How-ver, if the tumor is adherent to thefth or sixth ribs, one can enter thehest more inferiorly. The surgeon’sand is then placed inside the tho-acic cavity to help palpate theoundaries of the chest wall involve-ent.
Figure 1 Most T3 non-small-cell lungcancers, involving the chest wall, areapproached through a traditionalposterolateral thoracotomy. An epi-dural catheter should be placed pre-operatively. The patient is positionedin the left lateral decubitus positionwith the table flexed. It is crucial toavoid any break in sterile technique toprevent infection of the chest wallprosthesis. The incision is made mid-way between the spine and posteriorborder of the scapula, extending onefinger-breath below the inferior tip ofthe scapula. The latissimus dorsi mus-cle is divided from the auscultatorytriangle to the anterior aspect of theincision; the underlying serratus is el-evated but not divided. m. � muscle.

Ftcdhttfmetwa
Chest wall resection and reconstruction for NSCLC 281
igure 3 One can palpate the ex-ent of the tumor adherent to thehest wall. Much of this can beone under direct vision. It iselpful to mark the boundary ofhe chest wall resection with cau-ery. This should be at least 2 cmrom the tumor to insure negative
argins. Oftentimes the superiorxtent is difficult to determine andhis can be done after the chestall has been partially resected
nd reflected.
Figure 4 The thoracotomy shown hasbeen performed in the fifth intercostalspace. The chest wall resection is usu-ally begun anteriorly. Occasionally, it ishelpful to take a piece of the anteriorribs out to improve mobilization of thechest wall segment. The intercostalbundles are ligated individually. Afterthe inferior and anterior sections havebeen mobilized, one can begin mobiliz-ing the posterior segment of the chestwall resection.

282 B.D. Kozower
Figure 5 The posterior portion of the chest wall resec-tion may be challenging if the tumor approaches thevertebral bodies. To improve exposure, I elevate theerector spinae muscles to identify the junctionof the ribs with the transverse processes. If there isadequate distance between the rib and the transverseprocess, the head of the rib is disarticulated at thecostovertebral joint using a periosteal elevator (A). Ifthe costovertebral joint is involved, the transverseprocess should be transected flush with the laminausing a curved osteotome (B). The osteotome shouldbe held at a right angle to the vertebral body to avoidentering the spinal canal. The intercostal bundlesshould be securely ligated with heavy silk ties or he-moclips to prevent bleeding and cerebrospinal fluidleaks. If more extensive vertebral body involvement ispresent, I have performed more extensive resectionsworking with a neurosurgeon or an orthopedic spinesurgeon.
When possible, I prefer to perform the chest wallresection first followed by the pulmonary resection.The resected chest wall is left en bloc with the at-tached lung. The pulmonary resection is thenperformed in standard fashion. Occasionally, it is ad-vantageous to perform the pulmonary resection first.If the lung is fixed posteriorly, an anterior, fissureless,approach is quite useful. In addition, the lobectomymay improve exposure to the medial, anterior chestwall and avoid tension on the pulmonary vessels.

Chest wall resection and reconstruction for NSCLC 283
Figure 6 After the pulmonary and chest wall resection have been performed, a decision needs to be made about chestwall reconstruction. For defects greater than three ribs or 5 cm, some type of chest wall reconstruction is usuallywarranted. My first choice for lateral and posterior defects is 2-mm-thick Gore-Tex. This can also be quite useful whenthe fifth or sixth ribs have been resected posteriorly to prevent the scapula tip from caving into the chest. The Gore-Texis measured after being placed over the chest wall defect. The patch is cut to size and sewn around the inferior andsuperior ribs with interrupted 0-0 Prolene suture. Anteriorly and posteriorly, it is helpful to drill a hole in the ribs. I haveused the Midas Rex Gold Touch drill (Medtronic, Inc, Minneapolis, MN). The suture can then be passed through theholes and subsequently through the Gore-Tex. It is important to make sure that it is quite taut to prevent a flail segment.
The chest tubes need to be inserted and the lung reinflated before finishing the chest wall reconstruction.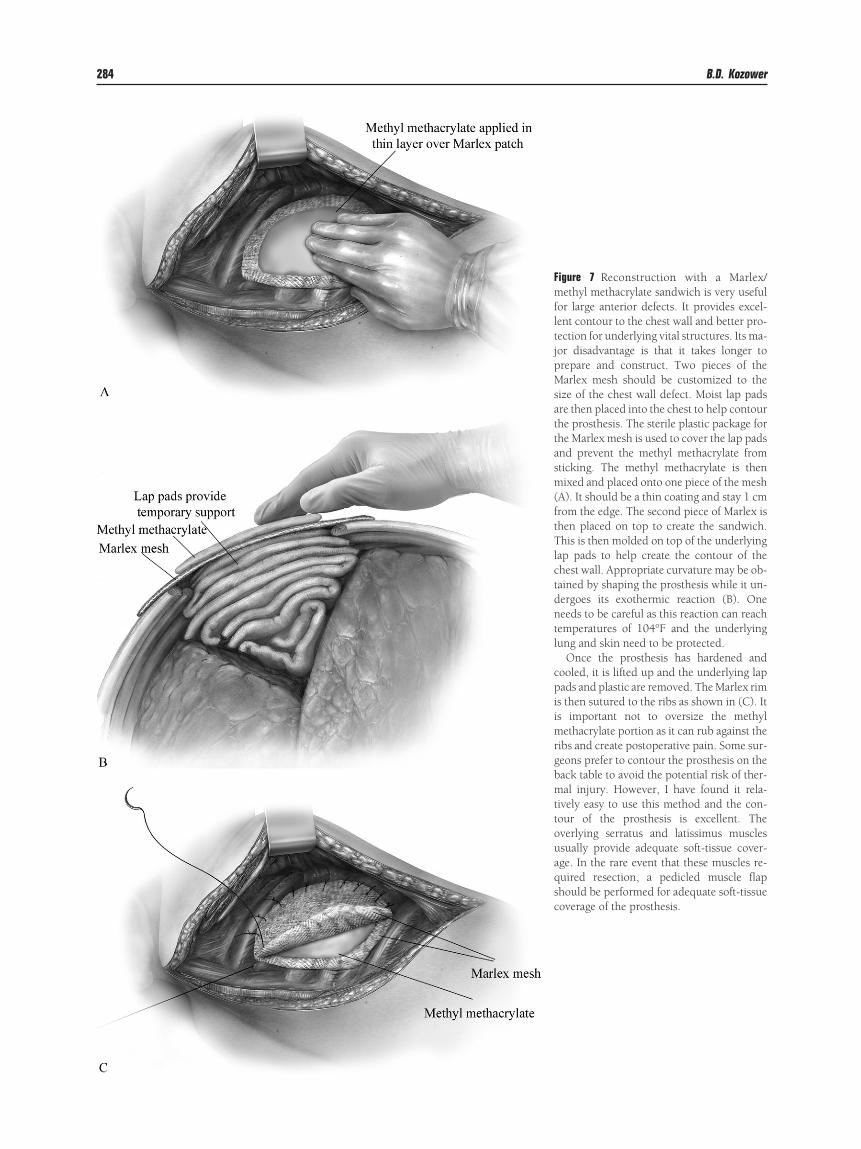
284 B.D. Kozower
Figure 7 Reconstruction with a Marlex/methyl methacrylate sandwich is very usefulfor large anterior defects. It provides excel-lent contour to the chest wall and better pro-tection for underlying vital structures. Its ma-jor disadvantage is that it takes longer toprepare and construct. Two pieces of theMarlex mesh should be customized to thesize of the chest wall defect. Moist lap padsare then placed into the chest to help contourthe prosthesis. The sterile plastic package forthe Marlex mesh is used to cover the lap padsand prevent the methyl methacrylate fromsticking. The methyl methacrylate is thenmixed and placed onto one piece of the mesh(A). It should be a thin coating and stay 1 cmfrom the edge. The second piece of Marlex isthen placed on top to create the sandwich.This is then molded on top of the underlyinglap pads to help create the contour of thechest wall. Appropriate curvature may be ob-tained by shaping the prosthesis while it un-dergoes its exothermic reaction (B). Oneneeds to be careful as this reaction can reachtemperatures of 104°F and the underlyinglung and skin need to be protected.
Once the prosthesis has hardened andcooled, it is lifted up and the underlying lappads and plastic are removed. The Marlex rimis then sutured to the ribs as shown in (C). Itis important not to oversize the methylmethacrylate portion as it can rub against theribs and create postoperative pain. Some sur-geons prefer to contour the prosthesis on theback table to avoid the potential risk of ther-mal injury. However, I have found it rela-tively easy to use this method and the con-tour of the prosthesis is excellent. Theoverlying serratus and latissimus musclesusually provide adequate soft-tissue cover-age. In the rare event that these muscles re-quired resection, a pedicled muscle flapshould be performed for adequate soft-tissuecoverage of the prosthesis.

R1
2
3
4
5
Chest wall resection and reconstruction for NSCLC 285
eferences. Burkhart HM, Allen MS, Nichols FC 3rd, et al: Results of en bloc resec-
tion for bronchogenic carcinoma with chest wall invasion. J ThoracCardiovasc Surg 123:670-675, 2002
. Matsuoka H, Nishio W, Okada M, et al: Resection of chest wall invasionin patients with non-small cell lung cancer. See comment. Eur J Cardio-
thorac Surg 26:1200-1204, 2004. Doddoli C, D’Journo B, Le Pimpec-Barthes F, et al: Lung cancer invad-ing the chest wall: a plea for en-bloc resection but the need for newtreatment strategies. See comment. Ann Thorac Surg 80:2032-2040,2005
. Karmy-Jones R, Vallieres E: Non-small cell lung cancer with chest wallinvolvement. Chest 123:1323-1325, 2003
. McCormack PM: Use of prosthetic materials in chest-wall reconstruc-
tion. Assets and liabilities. Surg Clin North Am 69:965-976, 1989