children with disabilities
DESCRIPTION
Children with Disabilities. We have chosen to focus on some of the major disabilities we see with our students in our general education classrooms. Speech in Schools. - PowerPoint PPT PresentationTRANSCRIPT

CHILDREN WITH DISABILITIES
We have chosen to focus on some of the major disabilities we see with our students in our general
education classrooms.
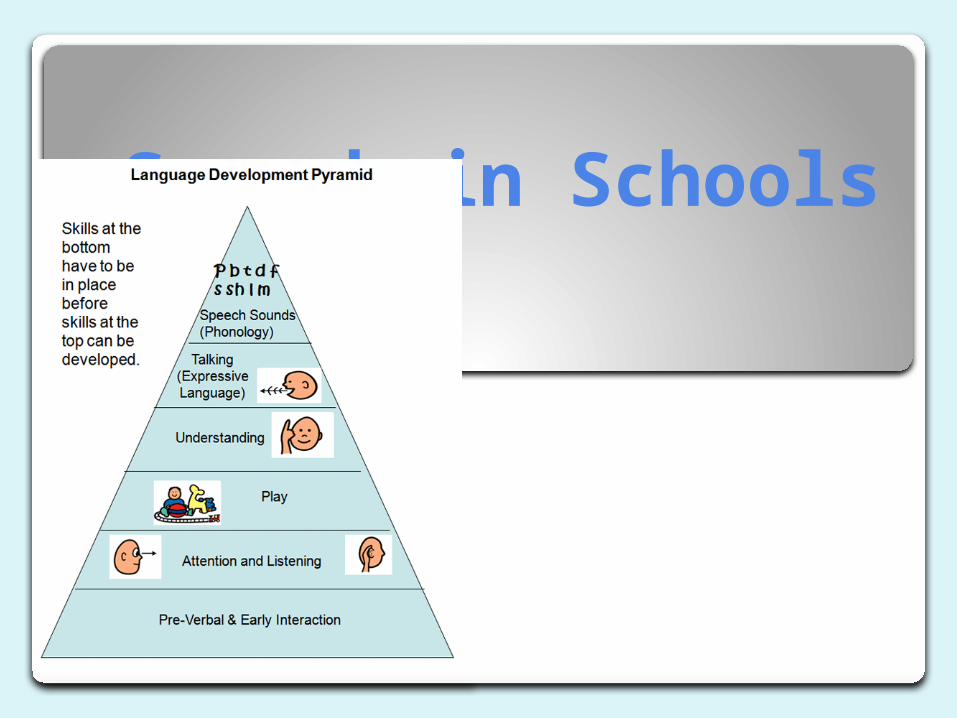

What is a “speech” problem?
an impairment of speech or sound production, voice, fluency, or language that significantly affects educational performance or social, emotional or vocational development
Who works with children in speech?
Speech and Language Pathologist- SLPs SLPs provide appropriate speech-language
services in Pre-K, elementary, middle, junior high, and high schools with no school level underserved
SLPs work with students exhibiting the full range of communication disorders, including those involving language, articulation (speech sound disorders), fluency, voice/resonance, and swallowing

Problems students may encounter that have speech problems…
below average grades inability to complete language-based activities vs. non-language based activities grades below the students ability level unable to answer/ask questions in a coherent/concise
manner peers tease student about communication problem student demonstrates embarrassment and/or
frustration regarding communication problem student demonstrates difficulty interpreting
communication intent

Speech Criterion 1
Evidence of an ongoing history of a poor performance in speech and/or language.

Speech Criterion 2
Descriptive evidence and analysis of the student’s speech and language demonstrate a significant reduction of the student’s performance in learning, communication and/or interacting socially. This includes documentation of the range of educational interventions provided and outcomes achieved.

Speech Criterion 3
Scores obtained from standardized individually administered assessment measures of expressive and/or receptive language development are at least 2 standard deviations below the mean. Where standardized assessments are inappropriate, reliance will be placed on the descriptive evidence and analysis as outlined in Criterion 2.

Speech Criterion 4
The student’s educational functioning cannot be accounted for by:
Cognitive ability, Socio-cultural factors, Hearing Impairment, Autism Spectrum Disorder, Social/emotional factors, Intellectual Impairment
Physical Impairment, Vision Impairment
Criterion 1 Impairment + Criterion 2 Activity limitations/ participation restrictions =
Disability

Misconception 2
MYTH: Group therapy is the only option in the public schools TRUTH: Speech therapy provided in the schools is based on an
educational model. In the USA, our public education is provided in a group setting (classroom). Therefore, the most common service delivery model in the schools is the small group model, where children are pulled from their class for short periods with a few other children to work on their goals with the SLP. However, there are times when the small group model is NOT appropriate for a child, and they require some 1:1 instruction. This is not as common but is IS possible, if the IEP team comes to that conclusion. Children in the schools do both in groups and 1:1 and most children do just fine in small groups, though there are always exceptions. In addition to small groups a child may also receive services in a push-in model (in the classroom) or in a consult model (indirect). Your child’s services in the schools need to be determined based on his/her individual needs and this decision should be made by the IEP team (which includes the parent).

Misconception 1
MYTH : Speech therapy in a hospital or clinic is “better” than speech therapy provided in the school setting
TRUTH: All speech-language pathologists have to have the same general levels of training, regardless of setting. This means, that the quality of your child’s therapy is not going to depend completely on the setting, but rather MANY different variables. The educational model IS different from the medical and private practice models, but one is not “better” than the other generally speaking. There are pros and cons to BOTH!

Effective Practices
Using data to guide clinical decision making and determine the effectiveness of service
Determining appropriate context(s) for service delivery (e.g., home, school, tele-practice, community
providing intervention and support services for children diagnosed with speech and language disorders
Counseling individuals, families, coworkers, educators, and other persons in the community regarding acceptance, adaptation, and decision making about communication

EXAMPLE OF STUTTERING VIDEO
• http://www.youtube.com/watch?v=da6xnm5feV4
EXAMPLE OF “S” DISTORTION LISP
• http://www.youtube.com/watch?v=nB3D-wi-FSQ

ADHD
A resource for teachers, parents, and friends

Definition of ADHD
Attention Deficit Hyperactivity Disorder (ADHD) is defined as a neurobiological disorder which is usually diagnosed during the primary school years. Symptoms are usually manifest before the age of seven, but sometimes continue into adolescence. Children with ADHD have developmentally inappropriate behavior, including poor attention skills, impulsivity, and hyperactivity. They may also struggle with low self-esteem, troubled relationships, and poor performance in school.

Characteristics
The American Speech-Language-Hearing Association is in agreement that there are two distinct characteristics of High Incidence Disability:
- hyperactivity-impulsivity
- inattention

Behaviors Associated with ADHD
1. Poorly sustained attention in almost all situations
2. Diminished persistence on tasks not having immediate consequences
3. Impulsivity, poor delay of gratification
4. Impaired adherence to commands to regulate or inhibit behavior in social contexts
5. More active, restless than normal children
6. Difficulty adhering to rules and regulations

DSM-III-R Diagnostic Criteria for Attention Deficit Hyperactivity Disorder
1. Often fidgets with hands or feet or squirms in seat (in adolescents may be limited to subjective feelings of restlessness).
2. Has difficulty remaining seated when required to.3. Is easily distracted by extraneous stimuli.4. Has difficulty awaiting turns in games or group situations.5. Often blurts out answers to questions before they have been completed.6. Has difficulty following through on instructions from others (not due to oppositional
behavior or failure of comprehension).7. Has difficulty sustaining attention in tasks or play activities.8. Often shifts from one uncompleted activity to another.9. Has difficulty playing quietly.10. Often talks excessively.11. Often interrupts or intrudes on others, e.g., butts into other people's games.12. Often does not seem to listen to what is being said to him or her.13. Often loses things necessary for tasks or activities at school or at home (e.g., toys,
pencils, books).14. Often engages in physically dangerous activities.

Three Components of Successful Programs for Children with ADHD
Academic Instruction: provide an advance organizer, set learning expectations, state needed material, and simplify instructions, choices, and scheduling
Behavioral Interventions: define appropriate behavior while giving praise, give praise immediately, selectively ignore inappropriate behavior, remove nuisance items, allow for "escape valve" outlets, behavioral prompts like visual clues and hand gestures, tangible rewards, self-management systems, and positive behavioral interventions and supports
Classroom Accommodations: seat the child near the teacher or a student role model, provide low-distraction work areas, pointers, egg timers, classroom lights, music, proper use of classroom furniture

What Can Teachers & Parents Do?
Teachers should be looking for signs of ADHD. Since teachers cannot diagnose children themselves, they should reach out to the parents. Teachers should keep detailed logs of observations and specific events that will help the parents and doctor make their decisions. Parents then need to seek out a doctor to thoroughly examine the child. Teachers can do several activities and strategies to make the environment more suitable for a child with ADHD.

Psychomotor Strategies
Sensual Strategies
Intellectual Strategies
Imaginational Strategies
Emotional Strategies
• Allow time for physical or verbal activity, before, during, and after school activities.• Be sure the physical or verbal activities are acceptable and not distracting to those around them.• Provide time for spontaneity and open-ended, freewheeling activities.
• Whenever possible, create an environment which limits offensive stimuli and provides comfort.• Provide appropriate opportunities for being in the limelight by giving unexpected attention, or facilitating creative and dramatic productions that have an audience.
• Show how to find the answers to questions. This respects and encourages a person’s passion to analyze, synthesize, and seek understanding.• Provide or suggest ways for those interested in moral and ethical issues to act upon their concerns.• If individuals seem critical or too outspoken to others, help them to see how their intent may be perceived as cruel or disrespectful.
• Imaginational people may confuse reality and fiction because their memories and new ideas become blended in their mind.• Help individuals to differentiate between their imagination and the real world.• Help people use their imagination to function in the real world and promote learning and productivity.
• Accept all feelings, regardless of intensity.• Teach individuals to anticipate physical and emotional responses and prepare for them

Appropriate Intervention & Support
Research shows that we should not assume that interventions recommended for children with ADHD would also work for gifted children with the disorder. Finding the right treatment is key! Interventions should result from knowing the unique strengths and needs of the specific child. This can be scary for the child. During intervention, it is important to keep the focus on talent development and not on the child’s deficits. This will promote a more positive outcome and minimize problems of social and emotional adjustment.

Great Links
http://www.pbs.org/wgbh/misunderstoodminds/attention.html
http://www.asha.org/public/speech/disorders/adhd.htm

References
http://www.ncld.org/types-learning-disabilities/dyslexia/what-is-dyslexia
http://www.mayoclinic.com/health/dyslexia/DS00224/DSECTION=treatments%2Dand%2Ddrugs
American Psychiatric Association (1994). Diagnostic and statistical manual of mental disorders. Washington, DC: Author.
Barkley, R.A. (1998). Attention deficit hyperactivity disorder: A handbook for diagnosis and treatment. NewYork, NY: Guilford Press.
Baum, S, Owen, S.V., & Dixon, J. (1991). To be gifted and learning disabled: From definition to practical intervention strategies. Mansfield Center, CT: Creative Learning Press.
Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised, Washington, DC, American Psychiatric Association, 1987.