choose well. live well. it’s your path · choose well. live well. it’s your path ... every...
TRANSCRIPT

Choose Well. Live Well. it’s your path
Your 2017 Guide to Benefits Enrollment
January 2017

The information in this Enrollment Guide is presented for illustrative purposes and is based on information provided by the employer. The text contained in this Guide was taken from various summary plan descriptions and benefit information. While every effort was taken to accurately report your benefits, discrepancies or errors are always possible. In case of discrepancy between the Guide and the plan documents, the actual plan documents will prevail. Information is confidential, pursuant to the Health Insurance Portability and Accountability Act of 1996. If you have any questions about the Guide, contact HR.
4 5 6 7
8 10
11 16 19 21
28
What’s Inside Changes This Year Contact Information Eligibility & Enrollment Qualifying Events Medical Coverage Prescription Coverage Dental Coverage Vision Coverage Flexible Spending Accounts Life and AD&D Coverage Disability Coverage Employee Assistance Program Notifications
31 332

Welcome to Your Benefits Open
Enrollment! We are pleased to present this
guide, which highlights the comprehensive coverage
available to you.
This guide includes only highlights of your benefits. The specific terms of coverage, exclusions & limitations are contained in the plan documents and insurance certificates. All coverage and coverage costs are subject to change at any time in the future. If you have any questions about a specific service or treatment, please contact the appropriate insurance carrier.
This booklet has been created to help you understand the benefit plans that are being offered to you. Our benefits program is designed to offer employees substantial coverage to meet both individual and family needs. Please take the time to review the information in this guide. We want you to be fully informed of the benefits available to you and your family. This guide also incorporates information on when you may change your benefit elections.
The information in this Enrollment Guide is presented for illustrativepurposes and is based on information provided by the employer. The textcontained in this Guide was taken from various summary plan descriptionsand benefit information. While every effort was taken to accurately reportyour benefits, discrepancies or errors are always possible. In case ofdiscrepancy between the Guide and the plan documents, the actual plandocuments will prevail. Information is confidential, pursuant to the HealthInsurance Portability and Accountability Act of 1996. If you have anyquestions about the Guide, contact HR.
Welcome to Benefits Open Enrollment!
We are pleased to present this guide which highlights the comprehensive coverage
available to you.
This guide includes only highlights. The specific terms of coverage, exclusions & limitations are contained in the plan documents and insurance certificates. All coverage and coverage costs are subject to change at any time in the future. If you have any questions about a specific service or treatment, please contact the appropriate insurance carrier.
This booklet has been created to help you understand the benefit plans that are being offered to you. Our benefits program is designed to offer employees substantial coverage to meet both individual and family needs. Please take the time to review the information in this guide. We want you to be fully informed of the benefits available to you and your family. This guide also incorporates information on when you may change your benefit elections.
3

MEDICAL COVERAGECHANGES THIS YEAR
Beginning Jan. 1, 2017, upon a group’s renewal, some pharmacy benefit plans will include a Preferred Pharmacy Network. This network includes at least one major chain, a grocery chain and independent pharmacies, among others. These are the participating pharmacies in the 2017 Preferred Pharmacy Network:• Walgreens• Walmart (including Sam’s Club Pharmacy)• Pharmacy Providers of Oklahoma, Inc. (PPOK) (a group of independent pharmacies)• AccessHealth (a group of independent pharmacies)
When members fill a prescription for up to a 30-day supply of a covered prescription drug from a retail pharmacy that contracts to participate in the Preferred Pharmacy Network, they may pay the lowest copay/coinsurance amount. If members fill a prescription at a non-preferred in-network pharmacy, they may pay a higher copay/coinsurance amount.For up to a 90-day supply of a covered prescription drug, members can either fill these prescriptions through the home delivery pharmacy service or at a retail pharmacy participating in the Preferred Pharmacy Network. Members will pay 3x copay of one 30-day prescription. A list of all participating pharmacies’ locations will be posted on the bcbsok.com website once available.
Letters will be sent to impacted members who are affected by one or more of these changes that will explain how the change (s) will impact them. Members will be encouraged to talk with their doctor(s) about their prescribed medications and if any changes in their drug therapy may be right for them.
All standard plans will move to the new Performance Drug List. Groups on a standard plan will also have the Preferred Pharmacy Network added to their pharmacy benefit plan. Additionally, CVS will be excluded from the Broad Pharmacy Network on Jan. 1, 2017 (regardless of renewal date).
Pharmacy Changes
4

CONTACT INFORMATIONRefer to this list when you need to contact one of your benefit vendors.
For general information contact Human Resources.
CONTACT PHONE WEBSITE / EMAIL GROUP #Human Resources: Oklahoma Baptist University· Kami Fullingim
405-585-5130 [email protected]
Medical: BlueCross Blue Shield· Member Services
(800) 942-5837 www.bcbsok.com Y04400
Dental: Delta Dental of OK· Member Services
(800) 522-0188 www.deltadentalok.org 3502-0013502-002
Vision: VSP· Member Services
(888) 600-1600 www.vsp.com 30002022
Life / AD&D and Vol. Life:Dearborn National
· Member Services
(800) 775-8805 www.dearbornnational.com F019973
Long- Term Disability (LTD):Cigna· Member Services
(800) 362-4462 www.cigna.com/customer-forms 964483
Employee Assistance Program (EAP):Cigna· Member Services
(800)538-3543 www.CignaBehavioral.com/CGI
Flexible Spending Account (FSA):Ameriflex· Member Services
(888)868-3539 https://participant.ameriflexbenefits.com
AMFOKBUOK
Broker Services:NFPKelley HarmonCortney Washington
(888) 460-8704
(405) 513-8988(405) 513-8948
www.nfp.com/CSOK
[email protected]@nfp.com
5

ELIGIBILITY& ENROLLMENT
Who is Eligible All employees who work at least 30 hours per week, and their eligible dependents, are eligible for the benefits outlined in this guide. Your coverage begins upon your hire date, provided you have completed the enrollment process within 31 days of hire date.
After your initial enrollment, you will have the opportunity to re-enroll in the Benefits Program each year during the Annual Open Enrollment period.
Eligible Dependents Your eligible dependents include: • Your spouse (unless you are legally separated)• Your dependent children who are under age 26.
How to Enroll If you are enrolling in our benefits for the first time, or wanting to make a plan/election change, just follow these simple steps:
• Request enrollment/change form(s) from yourBenefits Administrator.
• Read this guide and the instructions on your enrollmentform(s). These contain important information about yourbenefit options.
• Complete the enrollment form(s) by making your benefitelections and sign; and
• Send the enrollment form(s) to Human Resources by theenrollment deadline.
What Changes Can I Make?• Enroll if not currently on the plan• Switch to another plan option (if available)• Cancel coverage• Add/drop dependents
What is the deadline to submit changes?All Open Enrollment paperwork must be submitted to your Benefits Administrator no later than November 11, 2016.
What Happens if you Don’t Enroll For New Hires and Newly Eligible EmployeesIf you are a new hire or become eligible for benefits, and do not enroll when you are first eligible, you will receive only minimal levels of benefit coverage. In this case, you must wait until the next Annual Open Enrollment period to enroll for the coverage you want and need. If you don’t enroll, the only benefit coverage you will receive is: • Basic Life and AD&D Insurance• Long-term Disability Insurance
For Active EmployeesIf you are an active employee and don’t enrollfor benefits during the Annual Open Enrollmentperiod, your current benefit elections will automatically carry over to the next plan year – excluding your current Flexible Spending Account elections and any plans not offered in the new plan year. This feature is designed to make the enrollment process as easy as possible for employees who want to keep current coverage for another year.
When Coverage Ends If your employment ends or you lose eligibility, your coverage will end on the last day of the month following your event date. Depending upon the circumstances of your termination, you may be able to continue certain coverages under COBRA or State Continuation. For more information, refer to your continuation notice included with this guide.
6

QUALIFYING EVENTSMost individuals go through a number of life events that affect their health benefit needs and the choices they make. There are several important federal laws that affect your benefits under a job-based health plan.
While you are generally only allowed to change your benefits elections during the open enrollment period each year, certain life events provide an exception. Those life events allow you to change your benefits elections in the middle of the plan year if certain requirements are met. The following are examples of types of life events that may allow you to change your benefit elections during a plan year:
• Change in marital status (marriage, death of spouse, divorce/annulment, legal separation)
• Change in number of dependents (birth, death, adoption, eligibility status, child support order)
• Change in employment status for you or your spouse (commencement, termination, leave of absence, full-time/part-time status change)
• Change in Insurance coverage (gain or involuntary loss of coverage through another plan, including Medicaid or CHIP)
• Change of address (when you move outside the service area of your network)• Dependent child reaches limiting age
Generally, changes in your coverage elections must be made within 30 days of the qualifying event. YOU are responsible for notifying the Human Resources Department of any qualifying event and for requesting information to change your elections.
For further information on eligible qualifying events, please contact the Human Resources Department and also refer to the attached Special Enrollment Notice for qualifying events.
DON’T FORGET!Newborns will NOT be automatically
added to your coverage. You must take action within 30 days of the birth.
You are responsible
For notifying HR
Within 30 Days!
7
MEDICAL COVERAGEMEDICAL COVERAGE
Visit the link to view more information
about your benefits
QUESTIONS?
Medical CoverageHaving access to high quality, affordable health care is a great concern for most people. That’s why we are pleased to offer employees and their families comprehensive medical coverage administered by BlueCross & BlueShield of Oklahoma.
The Freedom To ChooseYou can choose between two medical Networks .Note: Plan changes can only be made during open enrollment.
• Blue Preferred – Base Plan• Lower premium option• Deeper negotiated discounts
• Blue Choice – Buy-up Plan• You have the option to buy up to this plan• Larger network of providers
These plans allow you the freedom to choose either an in-network or out-of-network provider for your health care needs. When you receive care from an in-network provider you will experience significant savings. This is because in-network providers have agreed to negotiated discounts for our employees. Should you choose to receive care from an out-of-network provider, you may have to file the claim to receive reimbursement for covered expenses and your out-of-pocket costs will be much higher.
If you are uncertain if a physician or medical facility is in your plan’s network, visit www.bcbsok.com/providers or call Customer Service at (800) 942-5837.
Blue Access for MembersSave time with self-service support tools and health and wellness resources on a convenient and secure online site.
Register for Blue Access for Members: www.bcbsok.com/member to review claims status, coverage details, download Explanation of Benefits (EOBs), request new ID cards, learn how to save money on gym memberships, hearing aids and diet-related services, and much more.
Prescription Drug CoverageWhen you enroll in our medical plan, you automatically receive prescription drug coverage.
Coverage ConsiderationsOur prescription drug benefit plan provides coverage for up to a 30-day supply of medication, with some exceptions. Our plan also provides coverage for up to a 90-day supply of maintenance medications. These medications are those drugs you may take on an ongoing basis for conditions such as high blood pressure, diabetes or high cholesterol.
Prior Authorization (PA): Our benefit plan requires prior authorization for certain drugs. This means that your doctor will need to submit a prior authorization request for coverage of these medications, and the request will need to be approved, before the medication will be covered under our plan.
Step Therapy (ST): Our benefit plan includes a step therapy program. This means you may need to try another proven, cost-effective medication before coverage may be available for the drug included in the program. Many brand drugs have less-expensive generic or brand alternatives that might be an option for you.
Dispensing Limits (DL): Drug Dispensing limits are designed to help encourage medication use as intended by the FDA. Coverage limits are placed on medications in certain drug categories. Limits may include: quantity of covered medication per prescription, quantity of covered medication in a given time period, coverage only for members within a certain age range, and coverage only for members of a specific gender. If your doctor prescribes a greater quantity of medication than what the dispensing limit allows, you can still get the medication. However, you will be responsible for the full cost of the prescription beyond what our coverage allows.
Remember, medication decisions are between you and your doctor. Discuss any questions or concerns you have about medications you are taking or are prescribed with your doctor.
8

MEDICAL COVERAGEMEDICAL COVERAGE
COVERED SERVICES Blue Preferred “Base Plan’’ BlueChoice “Buy-Up”Deductible (D)
IndividualFamily
$2,500$7,500
$2,500$7,500
Coinsurance (C) Plan 80% / You 20% Plan 80% / You 20%
Out-of-pocket Max*Includes Deductible, Coinsurance and Medical Copays
$6,600 Individual$13,200 Family
$6,600 Individual$13,200 Family
Physician Visit-Primary Care-Specialist
$30 Copay$50 Copay
$30 Copay$50 Copay
Diagnostics, Lab & X-RayComplex Imaging
Included in Office VisitDeductible + Coinsurance
Included in Office VisitDeductible + Coinsurance
Preventive Care 100% of Allowed Amount 100% of Allowed Amount
Hospitalization –-Inpatient
- Outpatient$200+ Deductible + Coinsurance
Deductible + Coinsurance$200 + Deductible + Coinsurance
Deductible + Coinsurance
Emergency Room $200 Copay (waived if admitted) then Deductible & Coinsurance
$200 Copay (waived if admitted) then Deductible & Coinsurance
Urgent Care $30 Copay $30 Copay
Medical Plans Compared The following chart compares a highlight of the in-network benefits of our plans. See the attached benefit summaries for more detail.
*The out-of-pocket limit is the most you could pay during a coverage period (usually one year) for your share of the cost of covered services.*Note: Please visit www.bcbsok.com for the most up to date hospital / provider listings.
Your Cost Per MonthOklahoma Baptist University pays 80% of the premium for employee only coverage, and 73% of dependents for eligible employees for the Blue Preferred Network. You have the option of buying up to the Blue Choice Network.
FILING STATUS OBU Cost Per Month Blue Preferred "Base Plan" BlueChoice "Buy-Up"Employee Only $308.62 $77.16 $147.24
Family $778.82 $288.04 $480.48
MEDICAL COVERAGE
9
MEDICAL COVERAGEMEDICAL COVERAGE
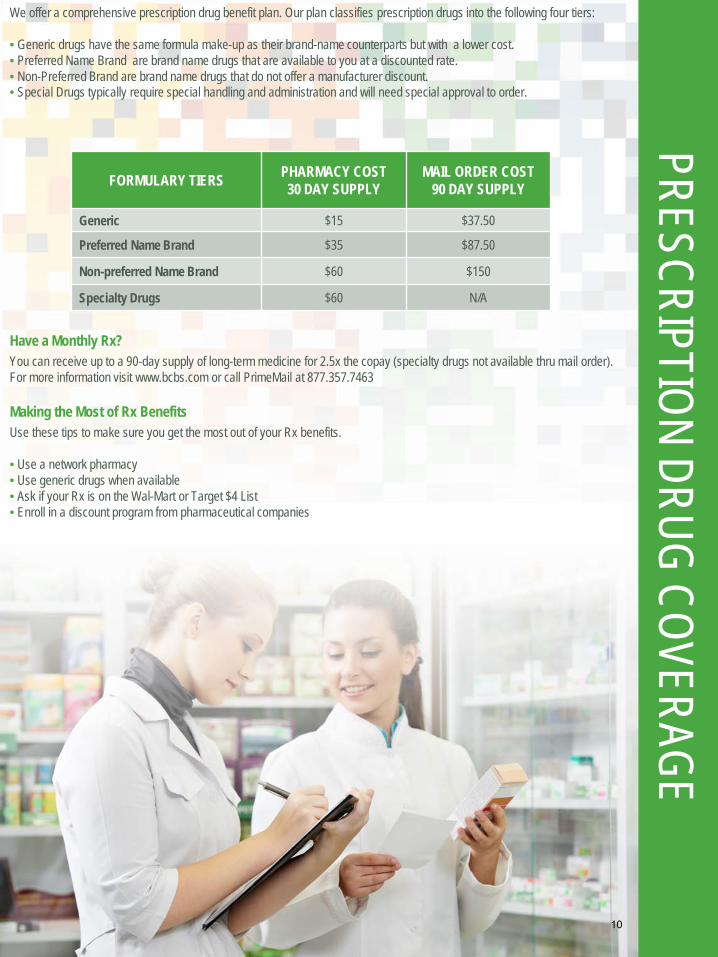
PRESCRIPTION DRUG COVERAGEWe offer a comprehensive prescription drug benefit plan. Our plan classifies prescription drugs into the following four tiers:
• Generic drugs have the same formula make-up as their brand-name counterparts but with a lower cost.• Preferred Name Brand are brand name drugs that are available to you at a discounted rate.• Non-Preferred Brand are brand name drugs that do not offer a manufacturer discount.• Special Drugs typically require special handling and administration and will need special approval to order.
FORMULARY TIERS PHARMACY COST 30 DAY SUPPLY
MAIL ORDER COST90 DAY SUPPLY
Generic $15 $37.50
Preferred Name Brand $35 $87.50
Non-preferred Name Brand $60 $150
Specialty Drugs $60 N/A
Have a Monthly Rx?You can receive up to a 90-day supply of long-term medicine for 2.5x the copay (specialty drugs not available thru mail order). For more information visit www.bcbs.com or call PrimeMail at 877.357.7463
Making the Most of Rx Benefits Use these tips to make sure you get the most out of your Rx benefits.
• Use a network pharmacy• Use generic drugs when available• Ask if your Rx is on the Wal-Mart or Target $4 List• Enroll in a discount program from pharmaceutical companies
10

MEDICAL COVERAGEDENTAL COVERAGE
Dental CoverageToo often people forget about dental care. That’s unfortunate, because having healthy teeth is an important part of your overallwell-being.
Our dental plans are administered by Delta Dental of Oklahoma. Our Plans pay for preventive services without requiring a deductible for exams, x-rays and cleanings. It also includes coverage for restorative and major services including fillings, crowns and bridges.
Delta Dental PPO – Plus Premier combines the Delta Dental PPO and Delta Dental Premier networks for maximum access and savings opportunities. Members may select a dentist from either the PPO or Premier network with no balance billing (subscribers are responsible for their deductible and coinsurance amounts). Greater network savings are available when utilizing a PPO provider.
To locate a participating PPO or Premier dentist, contact Delta Dental at 1-800-522-0188 or visit their website at www.deltadentalok.org.
COVERED SERVICES IN-NETWORKPPO PLUS PREMIER
Calendar Year DeductibleWaived for Preventive Services
$100 (3 per family)
Preventive ServicesCleanings & exams Plan pays 100%
Basic ServicesFillings & extractions
Plan pays 80% after deductible
Major ServicesCrowns, caps, dentures
Plan pays 50% after deductible
Orthodontic Services(Only up to age 26) Plan pays 50% after
deductible
Annual Max BenefitOrthodontic Lifetime Max
$1,000$1,500 per child
The following is a listing of common services available through your Dental PPO Plus Premier plan.
Your Cost Per MonthOklahoma Baptist University pays 80% of the employee premium, and 73% of dependents for dental.
FILING STATUS YOUR COST PER MONTH
Employee Only $17.26
Family $79.94
FILING STATUS YOUR COST PER MONTH
Employee Only $4.46
Family $17.66
COVERED SERVICES IN-NETWORKPPO
Calendar Year DeductibleWaived for Preventive Services
$100 (3 per family)
Preventive ServicesCleanings & exams Plan pays 100%
Basic ServicesFillings & extractions
Plan pays 80% after deductible
Major ServicesCrowns, caps, dentures
Plan pays 50% after deductible
Orthodontic Services N/A
Annual Max BenefitOrthodontic Lifetime Max
$1,000N/A
Benefit HighlightsThe following is a listing of common services available through your Dental PPO Plan.
11
UW-01, Revised: Nov 2015
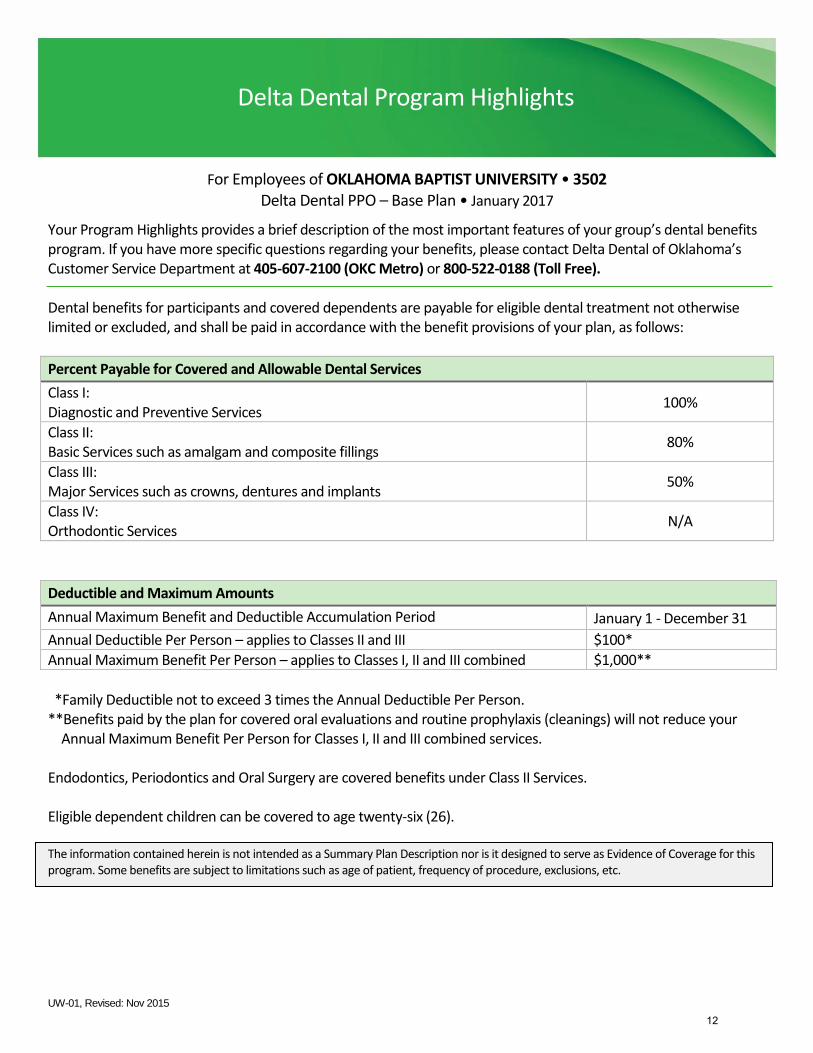
For Employees of OKLAHOMA BAPTIST UNIVERSITY • 3502 Delta Dental PPO – Base Plan • January 2017
Your Program Highlights provides a brief description of the most important features of your group’s dental benefits program. If you have more specific questions regarding your benefits, please contact Delta Dental of Oklahoma’s Customer Service Department at 405-607-2100 (OKC Metro) or 800-522-0188 (Toll Free).
Dental benefits for participants and covered dependents are payable for eligible dental treatment not otherwise limited or excluded, and shall be paid in accordance with the benefit provisions of your plan, as follows:
Percent Payable for Covered and Allowable Dental Services
Class I: Diagnostic and Preventive Services
100%
Class II: Basic Services such as amalgam and composite fillings
80%
Class III: Major Services such as crowns, dentures and implants
50%
Class IV: Orthodontic Services
N/A
Deductible and Maximum Amounts
Annual Maximum Benefit and Deductible Accumulation Period January 1 - December 31
Annual Deductible Per Person – applies to Classes II and III $100*
Annual Maximum Benefit Per Person – applies to Classes I, II and III combined $1,000**
*Family Deductible not to exceed 3 times the Annual Deductible Per Person.**Benefits paid by the plan for covered oral evaluations and routine prophylaxis (cleanings) will not reduce your
Annual Maximum Benefit Per Person for Classes I, II and III combined services.
Endodontics, Periodontics and Oral Surgery are covered benefits under Class II Services.
Eligible dependent children can be covered to age twenty-six (26).
The information contained herein is not intended as a Summary Plan Description nor is it designed to serve as Evidence of Coverage for this program. Some benefits are subject to limitations such as age of patient, frequency of procedure, exclusions, etc.
Delta Dental Program Highlights
12

UW-01, Revised: Nov 2015
Your dental benefits program allows payment for eligible services performed by any properly licensed dentist. However, maximum savings and lower out-of-pocket expenses are achieved when treatment is provided by a Delta Dental participating dentist. Below is an illustration of a typical 100/80/50/50 plan, assuming annual deductible has been satisfied.
Delta Dental PPO participating dentist Delta Dental Premier participating dentist Out-of-Network dentist
Dentist Charge $100 Dentist Charge $100 Dentist Charge $100
PPO Maximum Allowable $70 Premier Maximum Allowable $85 Prevailing Fee $75
Plan pays 80% of PPO Allowable
$56 Plan pays 80% of PPO Allowable
$56 Plan pays 80% of PPO Allowable
$56
You pay 20% of PPO Allowable
$14 You pay Difference between PPO Payment and Premier Allowable
$29 You pay Balance of the dentist charge
$44
How to use your dental program: Call the dental office of your choice and make an appointment. During your first appointment be sure to provide your dentist with the following information:
Your Group name
Your Group number
The employee’s social security or member ID number
Your dental program allows you to:
Change dentists and visit a specialist of your choice at any time without preapproval
Select a different dentist for each member of your family
Receive dental care anywhere in the world
Find a Delta Dental participating dentist: Two-thirds of the nation’s practicing dentists are Delta Dental participating dentists. To find a participating dentist, refer to our National Dentist Directory at www.DeltaDentalOK.org or call Delta Dental’s Customer Service Department at 405-607-2100 (OKC Metro) or 800-522-0188 (Toll Free).
Benefit Payment Procedure Delta Dental pays participating dentists directly. You are responsible for any co-insurance percentages, deductible amounts, charges for non-covered services and amounts in excess of your annual maximum benefit. A Delta Dental participating dentist cannot charge you for amounts payable by Delta Dental. If you obtain treatment from a nonparticipating dentist, you may have to pay the entire bill in advance. Delta Dental will directly reimburse you, or any other participant or beneficiary, if required by law, up to your plan’s maximum allowable amount.
The advantage of predetermination If you are scheduled for dental treatment that will cost more than $250, your dentist can request a predetermination of benefits by Delta Dental to determine if the proposed treatment is covered under your program, approximately how much the service will cost and your estimated share of the cost.
Filing your claim A Delta Dental participating dentist will file your claim at no charge. If necessary, a printable claim form may be obtained on our website at www.DeltaDentalOK.org. Completed claim forms should be submitted to the address below:
Delta Dental of Oklahoma - Claims Processing Center P.O. Box 548809
Oklahoma City, OK 73154-8809
13

UW-01, Revised: Nov 2015
For Employees of OKLAHOMA BAPTIST UNIVERSITY • 3502 Delta Dental PPO – Plus Premier – Buy Up Plan • January 2017
Your Program Highlights provides a brief description of the most important features of your group’s dental benefits program. If you have more specific questions regarding your benefits, please contact Delta Dental of Oklahoma’s Customer Service Department at 405-607-2100 (OKC Metro) or 800-522-0188 (Toll Free).
Dental benefits for participants and covered dependents are payable for eligible dental treatment not otherwise limited or excluded, and shall be paid in accordance with the benefit provisions of your plan, as follows:
Percent Payable for Covered and Allowable Dental Services
Class I: Diagnostic and Preventive Services
100%
Class II: Basic Services such as amalgam and composite fillings
80%
Class III: Major Services such as crowns, dentures and implants
50%
Class IV: Orthodontic Services are available to dependent children under age 26
50%
Deductible and Maximum Amounts
Annual Maximum Benefit and Deductible Accumulation Period January 1 - December 31
Annual Deductible Per Person – applies to Classes II and III $100*
Annual Maximum Benefit Per Person – applies to Classes I, II and III combined $1,000**
Lifetime Maximum Benefit Payment Per Child – applies to Class IV only $1,500
*Family Deductible not to exceed 3 times the Annual Deductible Per Person.**Benefits paid by the plan for covered oral evaluations and routine prophylaxis (cleanings) will not reduce your
Annual Maximum Benefit Per Person for Classes I, II and III combined services.
Endodontics, Periodontics and Oral Surgery are covered benefits under Class II Services.
Eligible dependent children can be covered to age twenty-six (26).
The information contained herein is not intended as a Summary Plan Description nor is it designed to serve as Evidence of Coverage for this program. Some benefits are subject to limitations such as age of patient, frequency of procedure, exclusions, etc.
Delta Dental Program Highlights
14

UW-01, Revised: Nov 2015
Your dental benefits program allows payment for eligible services performed by any properly licensed dentist. However, maximum savings and lower out-of-pocket expenses are achieved when treatment is provided by a Delta Dental participating dentist. Below is an illustration of a typical 100/80/50/50 plan, assuming annual deductible has been satisfied.
Delta Dental PPO participating dentist Delta Dental Premier participating dentist Out-of-Network dentist
Dentist Charge $100 Dentist Charge $100 Dentist Charge $100
PPO Maximum Allowable $70 Premier Maximum Allowable $85 Prevailing Fee $75
Plan pays 80% of PPO Allowable
$56 Plan pays 80% of Premier Allowable
$68 Plan pays 80% of Prevailing Fee
$60
You pay 20% of PPO Allowable
$14 You pay 20% of Premier Allowable
$17 You pay Balance of the dentist charge
$40
How to use your dental program: Call the dental office of your choice and make an appointment. During your first appointment be sure to provide your dentist with the following information:
Your Group name
Your Group number
The employee’s social security or member ID number
Your dental program allows you to:
Change dentists and visit a specialist of your choice at any time without preapproval
Select a different dentist for each member of your family
Receive dental care anywhere in the world
Find a Delta Dental participating dentist: Two-thirds of the nation’s practicing dentists are Delta Dental participating dentists. To find a participating dentist, refer to our National Dentist Directory at www.DeltaDentalOK.org or call Delta Dental’s Customer Service Department at 405-607-2100 (OKC Metro) or 800-522-0188 (Toll Free).
Benefit Payment Procedure Delta Dental pays participating dentists directly. You are responsible for any co-insurance percentages, deductible amounts, charges for non-covered services and amounts in excess of your annual maximum benefit. A Delta Dental participating dentist cannot charge you for amounts payable by Delta Dental. If you obtain treatment from a nonparticipating dentist, you may have to pay the entire bill in advance. Delta Dental will directly reimburse you, or any other participant or beneficiary, if required by law, up to your plan’s maximum allowable amount.
The advantage of predetermination If you are scheduled for dental treatment that will cost more than $250, your dentist can request a predetermination of benefits by Delta Dental to determine if the proposed treatment is covered under your program, approximately how much the service will cost and your estimated share of the cost.
Filing your claim A Delta Dental participating dentist will file your claim at no charge. If necessary, a printable claim form may be obtained on our website at www.DeltaDentalOK.org. Completed claim forms should be submitted to the address below:
Delta Dental of Oklahoma - Claims Processing Center P.O. Box 548809
Oklahoma City, OK 73154-8809
15
MEDICAL COVERAGEVISION COVERAGE
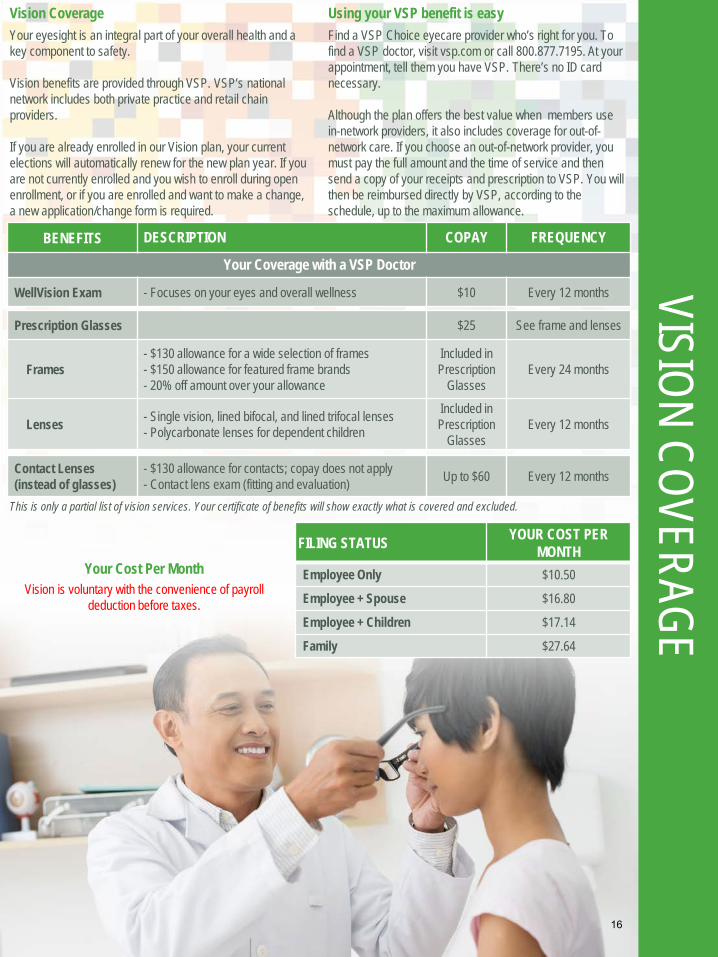
Vision CoverageYour eyesight is an integral part of your overall health and a key component to safety.
Vision benefits are provided through VSP. VSP’s national network includes both private practice and retail chain providers.
If you are already enrolled in our Vision plan, your current elections will automatically renew for the new plan year. If you are not currently enrolled and you wish to enroll during open enrollment, or if you are enrolled and want to make a change, a new application/change form is required.
BENEFITS DESCRIPTION COPAY FREQUENCY
Your Coverage with a VSP Doctor
WellVision Exam - Focuses on your eyes and overall wellness $10 Every 12 months
Prescription Glasses $25 See frame and lenses
Frames- $130 allowance for a wide selection of frames- $150 allowance for featured frame brands- 20% off amount over your allowance
Included in Prescription
GlassesEvery 24 months
Lenses - Single vision, lined bifocal, and lined trifocal lenses- Polycarbonate lenses for dependent children
Included in Prescription
GlassesEvery 12 months
Contact Lenses (instead of glasses)
- $130 allowance for contacts; copay does not apply- Contact lens exam (fitting and evaluation) Up to $60 Every 12 months
Using your VSP benefit is easyFind a VSP Choice eyecare provider who’s right for you. To find a VSP doctor, visit vsp.com or call 800.877.7195. At your appointment, tell them you have VSP. There’s no ID card necessary.
Although the plan offers the best value when members use in-network providers, it also includes coverage for out-of-network care. If you choose an out-of-network provider, you must pay the full amount and the time of service and then send a copy of your receipts and prescription to VSP. You will then be reimbursed directly by VSP, according to the schedule, up to the maximum allowance.
This is only a partial list of vision services. Your certificate of benefits will show exactly what is covered and excluded.
FILING STATUS YOUR COST PER MONTH
Employee Only $10.50
Employee + Spouse $16.80
Employee + Children $17.14
Family $27.64
Your Cost Per MonthVision is voluntary with the convenience of payroll
deduction before taxes.
16
Enroll in VSP today. You'll be glad you did.
Contact us. 800.877.7195 vsp.com
Get the best in eyecare and eyewear with OKLAHOMA BAPTIST UNIVERSITY and VSP® Vision Care. Why enroll in VSP? We invest in the things you value most—the best care at the lowest out-of-pocket costs. Because we’re the only national not-for-profit vision care company, you can trust that we’ll always put your wellness first.
You’ll like what you see with VSP.• Value and Savings. You’ll enjoy more value and the lowest out-of-
pocket costs.
• High Quality Vision Care. You’ll get the best care from a VSP provider,including a WellVision Exam®—the most comprehensive exam designedto detect eye and health conditions. Plus, when you see a VSP provider,your satisfaction is guaranteed.
• Choice of Providers. The decision is yours to make—choose a VSPprovider or any out-of-network provider.
• Great Eyewear. It’s easy to find the perfect frame at a price that fitsyour budget.
Using your VSP benefit is easy. • Register at vsp.com.
Once your plan is effective, review your benefit information.
• Find an eyecare provider who's right for you.To find a VSP provider, visit vsp.com or call 800.877.7195.
• At your appointment, tell them you have VSP. There’s no ID cardnecessary. If you’d like a card as a reference, you can print one onvsp.com.
That’s it! We’ll handle the rest—there are no claim forms to complete when you see a VSP provider.
Choice in Eyewear From classic styles to the latest designer frames, you'll find hundreds of options. Choose from featured frame brands like Anne Klein, bebe®, Calvin Klein, Flexon®, Lacoste, Nike, Nine West, and more1. Visit vsp.com to find a VSP provider who carries these brands.
17

Your VSP Vision Benefits Summary OKLAHOMA BAPTIST UNIVERSITY and VSP provide you with an affordable eyecare plan.
VSP Coverage Effective Date: 01/01/2015 VSP Provider Network: VSP Signature
Visit vsp.com for more details on your vision benefit and for exclusive savings
and promotions for VSP members.
CopayDescriptionBenefit FrequencyYour Coverage with a VSP Provider
WellVision Exam • Focuses on your eyes and overall wellness $10 Every calendar year
Prescription Glasses $25 See frame and lenses
Frame • $130 allowance for a wide selection of frames• $150 allowance for featured frame brands• 20% savings on the amount over your allowance
Included in Prescription
Glasses Every other calendar year
Lenses • Single vision, lined bifocal, and lined trifocal lenses• Polycarbonate lenses for dependent children
Included in Prescription
Glasses Every calendar year
Lens Enhancements
• Standard progressive lenses• Premium progressive lenses• Custom progressive lenses• Average savings of 35-40% on other lens enhancements
$50 $80 - $90
$120 - $160 Every calendar year
Contacts (instead of glasses)
• $130 allowance for contacts; copay does not apply• Contact lens exam (fitting and evaluation) Up to $60 Every calendar year
Extra Savings
Glasses and Sunglasses • Extra $20 to spend on featured frame brands. Go to vsp.com/specialoffers for details.• 30% savings on additional glasses and sunglasses, including lens enhancements, from the same VSP provider on
the same day as your WellVision Exam. Or get 20% from any VSP provider within 12 months of your last WellVisionExam.
Retinal Screening • No more than a $39 copay on routine retinal screening as an enhancement to a WellVision Exam
Laser Vision Correction • Average 15% off the regular price or 5% off the promotional price; discounts only available from contracted facilities• After surgery, use your frame allowance (if eligible) for sunglasses from any VSP doctor
Visit vsp.com for details, if you plan to see a provider other than a VSP network provider.
Exam ...................................................up to $50 Frame .................................................up to $70
Single Vision Lenses ..................up to $50 Lined Bifocal Lenses ..................up to $75
Lined Trifocal Lenses .................up to $100 Progressive Lenses .....................up to $75
Contacts ...........................................up to $105
Your Coverage with Out-of-Network Providers
VSP guarantees coverage from VSP network providers only. Coverage information is subject to change. In the event of a conflict between this information and your organization’s contract with VSP, the terms of the contract will prevail. Based on applicable laws, benefits may vary by location.
1 Brands/Promotion subject to change.
©2014 Vision Service Plan. All rights reserved. VSP, VSP Vision care for life, and WellVision Exam are registered
trademarks of Vision Service Plan. Flexon is a registered trademark of Marchon Eyewear, Inc. All other brands are
trademarks or registered trademarks of their respective owners.
Enroll in VSP today. You'll be glad you did. Contact us. 800.877.7195 vsp.com 18

FLEXIBLE SPENDINGMEDICAL COVERAGE
FLEXIBLE SPENDINGACCOUNTS
What is an FSA?A FSA is a Flexible Spending Account that allows participants to set aside money, before taxes, to use on eligible healthcare and dependent care expenses. Since the monies are withheld from your paycheck on a pre-tax basis, you save tax dollars and lower your taxable income.
Two Types of FSA’sHealthcare FSA: MedicalThe annual maximum amount each participant may contribute to the Health Care FSA is $2,550 per plan year.
• Deductible, Coinsurance, Office Visit Copays• Prescription• Hearing Services, Hearing Aids and Batteries• Vision Services and Eye Surgery• Dental Services and Orthodontia
Dependent Care FSA: DaycareThe annual maximum amount each participant may contribute to the Dependent Care FSA is $5,000 per plan year / per household (or $2,500 if married filingseparately).
• Before / After School Care Programs• Day Care and Nursery Schools• Preschool• Dependent Adult Day Care• Transportation Provided by Care Provider
Who is Our FSA Provider?Our Flexible Spending Accounts are administered by Ameriflex. If you have any questions regarding these benefits, please contact Ameriflex Customer Service Center at 888.868.3539 or visit https://participant.ameriflexbenefits.com.
When Can I Use My Funds?Healthcare FSA’s are fully funded at the beginning of your plan year for immediate use. Dependent Care FSA’s require that the funds be contributed before they can be used.
Use It or Lose It!Regarding the Healthcare FSA, any contributions that are not claimed for the plan year must be forfeited as required by Internal Revenue Service regulations (often referred to as the “use it or lose it” rule). You have a grace period to utilize the Prior Year’s funds until March 15, 2017. All Claims For Prior Year Funds Must Be Filed By March 31, 2017. Regarding the Dependent Care FSA, any funds left in this account at the end of the plan year will be forfeited. When you are no longer an employee, and have a balance in your FSA account, you will have 30 days to utilize those monies, or you will lose them.
How to Use Your FundsPay Me Back (Health Care or Dependent Care)Use out-of-pocket funds then request reimbursement from your FSA. File a claim online, by fax, email or mail.
19

For Non-Cardholders:
*Name - enter participants First and Last name*Employee ID - enter participant's social security number without dashes*Employer ID - this can be obtained by calling AmeriFlex’s Customer Service Dept.*New User ID - create a username specific to you*Password - create a password specific to you*Security Word - enter Mother's Maiden Name*E-Mail Address - enter your email address
Balances:Select the Accounts tab to view balances in all accounts. You can also view the Plan Year, Account Type, YTD Contributions, Annual Election, Disbursements YTD, and Disbursable Balance.
Statements:Under the Accounts tab, select Statement to prepare and print a cardholder statement. The statement will illustrate only those transactions that were successfully deducted from or deposited into the account.
History:Under the Accounts tab, select History to show a complete Transaction History. The Transaction History includes all attempted charges regardless of the success of those transactions.
Lost/Stolen Card:Under the Home tab, select Lost/Stolen Card to report your card lost or stolen. Please contact AmeriFlex to have a new cardissued.
Frequently Asked Questions:Under the Home tab, select Frequently Asked Questions to view FAQs such as definitions of terms, How Do I questions, etc.
Change Log-In Information:Select User Options from the top right corner of the screen. Within User Options you can change your password and email address.
AMERIFLEX® 302 FELLOWSHIP RD., STE. 100, MOUNT LAUREL, NEW JERSEY 08054 C ALL TOLL-FREE: 888.868.FLEX (3539) FAX: 888.631.1038
AmeriFlex Online Account InstructionsAccessing Your AmeriFlex Account via the Internet:Go to www.flex125.com. Select Employee from the left navigation menu. Next, select View Your Account Activity. You will be redirected to www.benefitspaymentsystem.com. Please note that pop-up blockers will need to be disabled in order to access this site.
To Create an Account:Click on the Participant Login button, then select Create Account from the main screen. All fields MUST be completed to create an account.
AMERIFLEX WEB-BASED FLEX ACCOUNT UTILIZATION®
www.flex125.com
20

MEDICAL COVERAGELIFE AND AD&D
COVERAGEBasic Life and AD&DLife insurance isn’t a fun thing to think about, and it may seem like an unnecessary expense. But if you have people who depend on you for financial support, then life insurance is really about protecting them in case something happens to you – your designated beneficiary would collect a financial benefit upon your death. The plans are administered by Dearborn National.
As your employer, we automatically provide a certain level of coverage for you and give you the opportunity to purchase additional coverage for you and your dependents.
Beneficiary DesignationIt is very important to designate a beneficiary for your life, supplemental life and AD&D policies - the person(s) who would receive your account balance in the event of your death. You may change/update your beneficiary information at any time. To name your beneficiary, you must complete a beneficiary designation form.
Optional Life & AD&DEmployees who wish to supplement their basic life insurance benefit may purchase additional coverage with the convenience of payroll deduction.
Guaranteed Issued Amounts (GI)Newly eligible employees are guaranteed a policy up tothe amount of $100,000 without being required toprovide any health information. For the spouse of anewly eligible employee, the GI amount is $25,000 andfor eligible dependents the GI amount is $10,000.
Evidence of Insurability (EOI)The GI amounts are only available to employees that enroll when they are first eligible. Anyone who chooses not to sign up during their initial enrollment opportunity will be required to provide evidence of good health and may be denied coverage. Evidence of insurability is also required if you elect an amount in excess of the GI amounts.
Note: No eligible person may be covered more than once under the Policy.
OPTIONAL LIFE AND AD&D
EmployeeYou must enroll to cover your dependents
- $10,000 to $500,000 Max - $10,000 Increments- $100,000 GI
Spouse
- $5,000 to $100,000 Max- Not to exceed 50% ofEmployee’s Election
- $5,000 Increments- $25,000 GI
Child(ren)Six months to 19 years (23 if FT Student)
- $10,000 Maximum- $1,000 Birth - six months
-$1,000-$10,000– six months-19 years- $1,000 Increments
AD&D Same as Optional Life
Age Reduction Schedule Same as Basic Life
Portability
If your employment ends, you may be able to convert your Group Life coverage to an Individual Life insurance policy or apply to port your group term life insurance coverage.
BASIC LIFE AND AD&D
Employee Protection1.5 times annual earnings to $200,000 Maximum.$200,000 GI
AD&D Coverage
Provides up to 100% of the Life benefit for loss of life and pays a percentage for loss of a limb due to an accident.
Age Reduction Schedule
Benefits will reduce to 35% at age 65 and to50% of original amount at age 70. Benefits terminate atretirement.
21
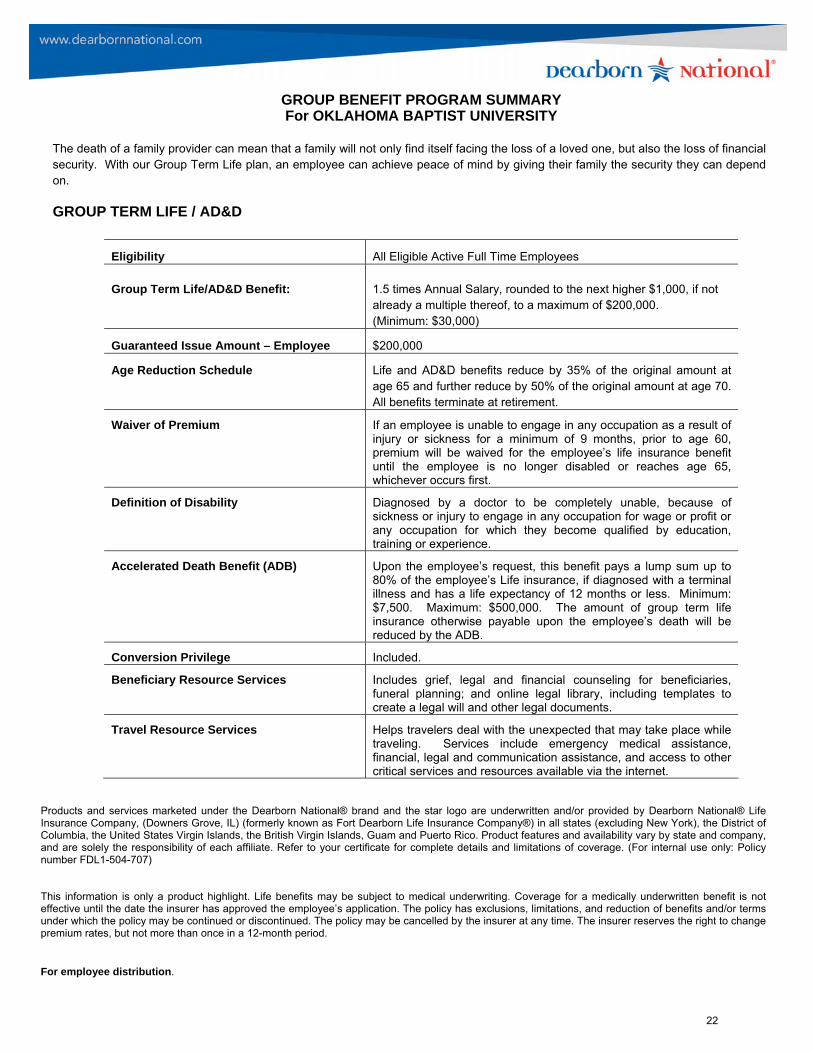
GROUP BENEFIT PROGRAM SUMMARY For OKLAHOMA BAPTIST UNIVERSITY
The death of a family provider can mean that a family will not only find itself facing the loss of a loved one, but also the loss of financial security. With our Group Term Life plan, an employee can achieve peace of mind by giving their family the security they can depend on.
GROUP TERM LIFE / AD&D
Products and services marketed under the Dearborn National® brand and the star logo are underwritten and/or provided by Dearborn National® Life Insurance Company, (Downers Grove, IL) (formerly known as Fort Dearborn Life Insurance Company®) in all states (excluding New York), the District of Columbia, the United States Virgin Islands, the British Virgin Islands, Guam and Puerto Rico. Product features and availability vary by state and company, and are solely the responsibility of each affiliate. Refer to your certificate for complete details and limitations of coverage. (For internal use only: Policy number FDL1-504-707)
This information is only a product highlight. Life benefits may be subject to medical underwriting. Coverage for a medically underwritten benefit is not effective until the date the insurer has approved the employee’s application. The policy has exclusions, limitations, and reduction of benefits and/or terms under which the policy may be continued or discontinued. The policy may be cancelled by the insurer at any time. The insurer reserves the right to change premium rates, but not more than once in a 12-month period.
For employee distribution.
Eligibility All Eligible Active Full Time Employees
Group Term Life/AD&D Benefit: 1.5 times Annual Salary, rounded to the next higher $1,000, if not already a multiple thereof, to a maximum of $200,000. (Minimum: $30,000)
Guaranteed Issue Amount – Employee $200,000
Age Reduction Schedule Life and AD&D benefits reduce by 35% of the original amount at age 65 and further reduce by 50% of the original amount at age 70. All benefits terminate at retirement.
Waiver of Premium If an employee is unable to engage in any occupation as a result of injury or sickness for a minimum of 9 months, prior to age 60, premium will be waived for the employee’s life insurance benefit until the employee is no longer disabled or reaches age 65, whichever occurs first.
Definition of Disability Diagnosed by a doctor to be completely unable, because of sickness or injury to engage in any occupation for wage or profit or any occupation for which they become qualified by education, training or experience.
Accelerated Death Benefit (ADB) Upon the employee’s request, this benefit pays a lump sum up to 80% of the employee’s Life insurance, if diagnosed with a terminal illness and has a life expectancy of 12 months or less. Minimum: $7,500. Maximum: $500,000. The amount of group term life insurance otherwise payable upon the employee’s death will be reduced by the ADB.
Conversion Privilege Included.
Beneficiary Resource Services Includes grief, legal and financial counseling for beneficiaries, funeral planning; and online legal library, including templates to create a legal will and other legal documents.
Travel Resource Services Helps travelers deal with the unexpected that may take place while traveling. Services include emergency medical assistance, financial, legal and communication assistance, and access to other critical services and resources available via the internet.
22
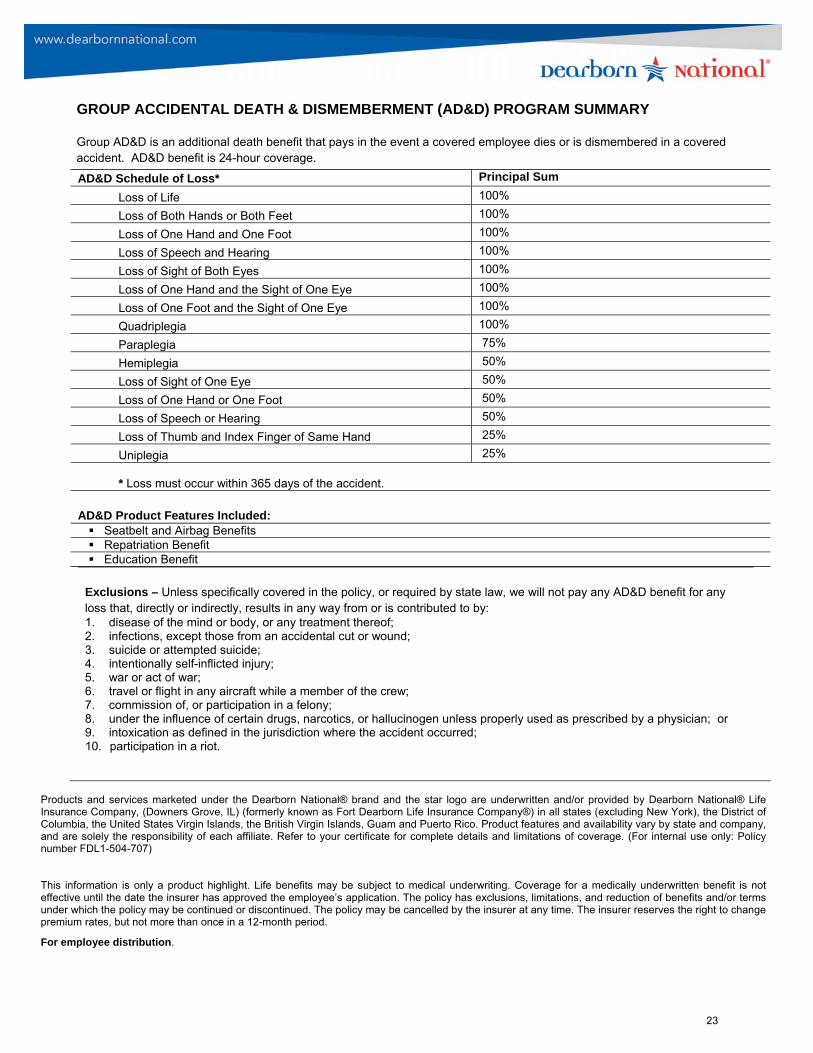
GROUP ACCIDENTAL DEATH & DISMEMBERMENT (AD&D) PROGRAM SUMMARY
Group AD&D is an additional death benefit that pays in the event a covered employee dies or is dismembered in a covered accident. AD&D benefit is 24-hour coverage.
AD&D Schedule of Loss* Principal Sum
Loss of Life 100%
Loss of Both Hands or Both Feet 100%
Loss of One Hand and One Foot 100%
Loss of Speech and Hearing 100%
Loss of Sight of Both Eyes 100%
Loss of One Hand and the Sight of One Eye 100%
Loss of One Foot and the Sight of One Eye 100%
Quadriplegia 100%
Paraplegia 75%
Hemiplegia 50%
Loss of Sight of One Eye 50%
Loss of One Hand or One Foot 50%
Loss of Speech or Hearing 50%
Loss of Thumb and Index Finger of Same Hand 25%
Uniplegia 25%
* Loss must occur within 365 days of the accident.
AD&D Product Features Included: Seatbelt and Airbag Benefits Repatriation Benefit Education Benefit
Exclusions – Unless specifically covered in the policy, or required by state law, we will not pay any AD&D benefit for any loss that, directly or indirectly, results in any way from or is contributed to by: 1. disease of the mind or body, or any treatment thereof;2. infections, except those from an accidental cut or wound;3. suicide or attempted suicide;4. intentionally self-inflicted injury;5. war or act of war;6. travel or flight in any aircraft while a member of the crew;7. commission of, or participation in a felony;8. under the influence of certain drugs, narcotics, or hallucinogen unless properly used as prescribed by a physician; or9. intoxication as defined in the jurisdiction where the accident occurred;10. participation in a riot.
Products and services marketed under the Dearborn National® brand and the star logo are underwritten and/or provided by Dearborn National® Life Insurance Company, (Downers Grove, IL) (formerly known as Fort Dearborn Life Insurance Company®) in all states (excluding New York), the District of Columbia, the United States Virgin Islands, the British Virgin Islands, Guam and Puerto Rico. Product features and availability vary by state and company, and are solely the responsibility of each affiliate. Refer to your certificate for complete details and limitations of coverage. (For internal use only: Policy number FDL1-504-707)
This information is only a product highlight. Life benefits may be subject to medical underwriting. Coverage for a medically underwritten benefit is not effective until the date the insurer has approved the employee’s application. The policy has exclusions, limitations, and reduction of benefits and/or terms under which the policy may be continued or discontinued. The policy may be cancelled by the insurer at any time. The insurer reserves the right to change premium rates, but not more than once in a 12-month period.
For employee distribution.
23

.
GROUP BENEFIT PROGRAM SUMMARY For OKLAHOMA BAPTIST UNIVERSITY - #F019973
The death of a family provider can mean that a family will not only find itself facing the loss of a loved one, but also the loss of financial security. With our Group Term Life plan, an employee can achieve peace of mind by giving their family the security they can depend on.
VOLUNTARY GROUP TERM LIFE/AD&D
Eligibility All Eligible Active Full Time Employees electing Voluntary Life
Group Term Life/AD&D Benefit: Employee $10,000 - $500,000, in increments of $10,000
Guaranteed Issue Amount* – Employee $100,000 *Guarantee issue amounts are based on a minimum participation requirement of 22% of alleligible employees. If participation requirements are not achieved, underwriting will beutilized on all employees and spouse applications.
Group Term Life/AD&D Benefit: Spouse (Includes Domestic Partners)
$5,000 - $100,000, in increments of $5,000, not to exceed 50% of the employee benefit amount.
Guaranteed Issue Amount – Spouse $25,000
Group Term Life/AD&D Benefit: Child(ren) Birth to 14 days: $1,000 Age 15 days to 6 months: $1,000 Age 6 months to 19 years (23 if full-time student): $1,000 - $10,000, in increments of $1,000
Grandfathered Benefits (Up to $500,000): If the Voluntary Life Participation Minimum stated in the Plan Design Summary above is met, all current amounts in force will be grandfathered, subject to the plan design maximums and the grandfathering limits stated. The Guarantee Issue amount shown above will only be offered to employees whose initial eligibility date (new hires) is on or after the effective date of coverage. Employees not previously covered, or those who have selected to increase their coverage, will need to provide satisfactory Evidence of Insurability. Should the Voluntary Life Participation Minimum not be met, grandfathering will not apply and satisfactory Evidence of Insurability will be required for all amounts by all applicants, including those participating in the prior carrier's plan.
Age Reduction Schedule None
Employee Contribution 100%
Waiver of Premium If an employee is unable to engage in any occupation as a result of injury or sickness for a minimum of 9 months, prior to age 60, premium will be waived for the employee’s life insurance benefit until the employee is no longer disabled or reaches age 65, whichever occurs first.
Accelerated Death Benefit (ADB) Upon the employee’s request, this benefit pays a lump sum up to 80% of the employee’s Life insurance, if diagnosed with a terminal illness and has a life expectancy of 12 months or less. Minimum: $7,500. Maximum: $500,000. The amount of group term life insurance otherwise payable upon the employee’s death will be reduced by the ADB.
Portability Feature (Life coverage) Included. (Employee & Dependent)
Conversion Privilege (Life coverage) Included.
Travel Resource Services Helps travelers deal with the unexpected that may take place while traveling. Services include emergency medical assistance, financial, legal and communication assistance, and access to other critical services and resources available via the internet.
Exclusions One-year suicide exclusion applies to Voluntary Group Term Life coverage. AD&D exclusions are the same as Basic AD&D exclusions.
This information is only a product highlight. Life benefits may be subject to medical underwriting. Coverage for a medically underwritten benefit is not effective until the date the insurer has approved the employee’s application. The policy has exclusions, limitations, and reduction of benefits and/or terms under which the policy may be continued or discontinued. The policy may be cancelled by the insurer at any time. The insurer reserves the right to change premium rates, but not more than once in a 12-month period.
Products and services marketed under the Dearborn National® brand and the star logo are underwritten and/or provided by Dearborn National® Life Insurance Company, (Downers Grove, IL) (formerly known as Fort Dearborn Life Insurance Company®) in all states (excluding New York), the District of Columbia, the United States Virgin Islands, the British Virgin Islands, Guam and Puerto Rico. Product features and availability vary by state and company, and are solely the responsibility of each affiliate. Refer to your certificate for complete details and limitations of coverage. (For internal use only: Policy number FDL1-504-707)
24

For employee distribution
GROUP ACCIDENTAL DEATH & DISMEMBERMENT (AD&D) PROGRAM SUMMARY
Group AD&D is an additional death benefit that pays in the event a covered employee dies or is dismembered in a covered accident. AD&D benefit is 24-hour coverage.
AD&D Schedule of Loss* Principal Sum
Loss of Life 100%
Loss of Both Hands or Both Feet 100%
Loss of One Hand and One Foot 100%
Loss of Speech and Hearing 100%
Loss of Sight of Both Eyes 100%
Loss of One Hand and the Sight of One Eye 100%
Loss of One Foot and the Sight of One Eye 100%
Quadriplegia 100%
Paraplegia 75%
Hemiplegia 50%
Loss of Sight of One Eye 50%
Loss of One Hand or One Foot 50%
Loss of Speech or Hearing 50%
Loss of Thumb and Index Finger of Same Hand 25%
Uniplegia 25%
* Loss must occur within 365 days of the accident.
AD&D Product Features Included: Seatbelt and Airbag Benefits Repatriation Benefit Education Benefit
Exclusions – Unless specifically covered in the policy, or required by state law, we will not pay any AD&D benefit for any loss that, directly or indirectly, results in any way from or is contributed to by: 1. disease of the mind or body, or any treatment thereof;2. infections, except those from an accidental cut or wound;3. suicide or attempted suicide;4. intentionally self-inflicted injury;5. war or act of war;6. travel or flight in any aircraft while a member of the crew;7. commission of, or participation in a felony;8. under the influence of certain drugs, narcotics, or hallucinogen unless properly used as prescribed by a physician; or9. intoxication as defined in the jurisdiction where the accident occurred;10. participation in a riot.
This information is only a product highlight. Life benefits may be subject to medical underwriting. Coverage for a medically underwritten benefit is not effective until the date the insurer has approved the employee’s application. The policy has exclusions, limitations, and reduction of benefits and/or terms under which the policy may be continued or discontinued. The policy may be cancelled by the insurer at any time. The insurer reserves the right to change premium rates, but not more than once in a 12-month period.
Products and services marketed under the Dearborn National® brand and the star logo are underwritten and/or provided by Dearborn National® Life Insurance Company, (Downers Grove, IL) (formerly known as Fort Dearborn Life Insurance Company®) in all states (excluding New York), the District of Columbia, the United States Virgin Islands, the British Virgin Islands, Guam and Puerto Rico. Product features and availability vary by state and company, and are solely the responsibility of each affiliate. Refer to your certificate for complete details and limitations of coverage. (For internal use only: Policy number FDL1-504-707)
For employee distribution
25

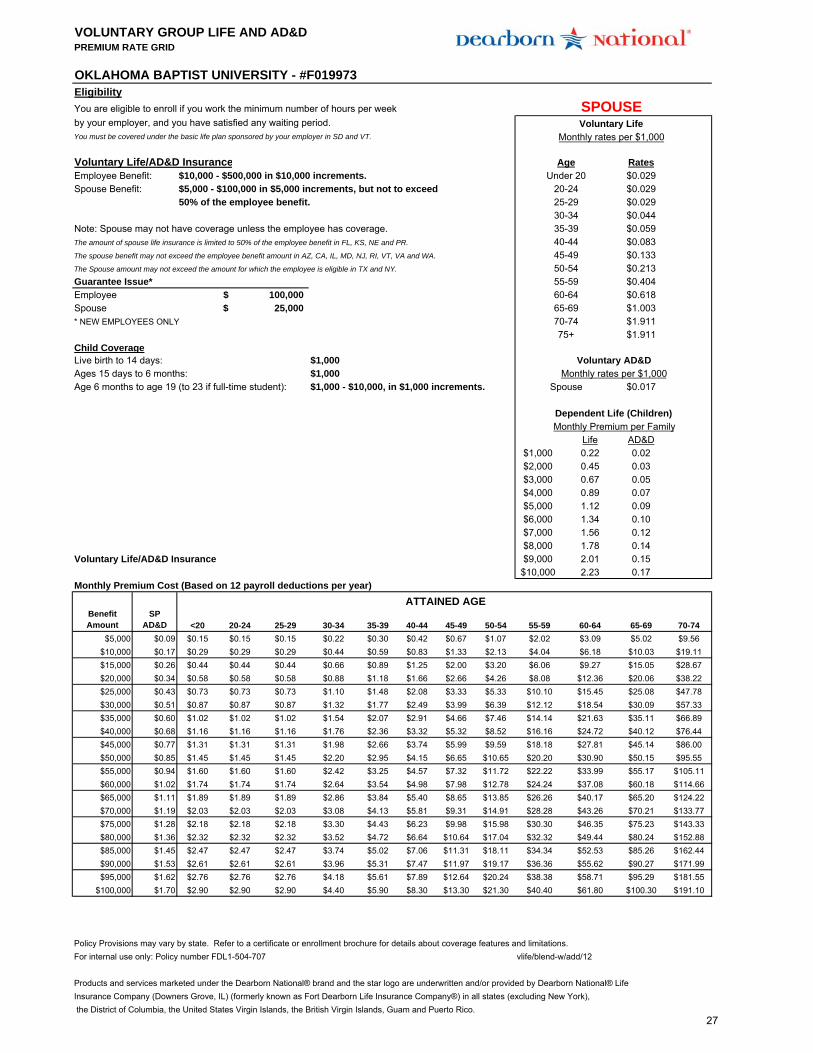
VOLUNTARY GROUP LIFE AND AD&DPREMIUM RATE GRID
Eligibility
You are eligible to enroll if you work the minimum number of hours per week by your employer, and you have satisfied any waiting period.You must be covered under the basic life plan sponsored by your employer in SD and VT.
Voluntary Life/AD&D Insurance RatesEmployee Benefit: $10,000 - $500,000 in $10,000 increments. $0.029Spouse Benefit: $5,000 - $100,000 in $5,000 increments, but not to exceed $0.029
50% of the employee benefit. $0.029$0.044
Note: Spouse may not have coverage unless the employee has coverage. $0.059The amount of spouse life insurance is limited to 50% of the employee benefit in FL, KS, NE and PR. $0.083The spouse benefit may not exceed the employee benefit amount in AZ, CA, IL, MD, NJ, RI, VT, VA and WA. $0.133The Spouse amount may not exceed the amount for which the employee is eligible in TX and NY. $0.213Guarantee Issue* $0.404Employee $0.618Spouse $1.003* NEW EMPLOYEES ONLY $1.911
$1.911Child CoverageLive birth to 14 days: $1,000Ages 15 days to 6 months: $1,000Age 6 months to age 19 (to 23 if full-time student): $1,000 - $10,000, in $1,000 increments. $0.017
Life AD&D$1,000 0.22 0.02$2,000 0.45 0.03$3,000 0.67 0.05$4,000 0.89 0.07$5,000 1.12 0.09$6,000 1.34 0.10$7,000 1.56 0.12$8,000 1.78 0.14
Voluntary Life/AD&D Insurance $9,000 2.01 0.15$10,000 2.23 0.17
Monthly Premium Cost (Based on 12 payroll deductions per year)
Benefit Amount
EE AD&D <20 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74
$10,000 $0.17 $0.29 $0.29 $0.29 $0.44 $0.59 $0.83 $1.33 $2.13 $4.04 $6.18 $10.03 $19.11$20,000 $0.34 $0.58 $0.58 $0.58 $0.88 $1.18 $1.66 $2.66 $4.26 $8.08 $12.36 $20.06 $38.22$30,000 $0.51 $0.87 $0.87 $0.87 $1.32 $1.77 $2.49 $3.99 $6.39 $12.12 $18.54 $30.09 $57.33$40,000 $0.68 $1.16 $1.16 $1.16 $1.76 $2.36 $3.32 $5.32 $8.52 $16.16 $24.72 $40.12 $76.44$50,000 $0.85 $1.45 $1.45 $1.45 $2.20 $2.95 $4.15 $6.65 $10.65 $20.20 $30.90 $50.15 $95.55$60,000 $1.02 $1.74 $1.74 $1.74 $2.64 $3.54 $4.98 $7.98 $12.78 $24.24 $37.08 $60.18 $114.66$70,000 $1.19 $2.03 $2.03 $2.03 $3.08 $4.13 $5.81 $9.31 $14.91 $28.28 $43.26 $70.21 $133.77$80,000 $1.36 $2.32 $2.32 $2.32 $3.52 $4.72 $6.64 $10.64 $17.04 $32.32 $49.44 $80.24 $152.88$90,000 $1.53 $2.61 $2.61 $2.61 $3.96 $5.31 $7.47 $11.97 $19.17 $36.36 $55.62 $90.27 $171.99
$100,000 $1.70 $2.90 $2.90 $2.90 $4.40 $5.90 $8.30 $13.30 $21.30 $40.40 $61.80 $100.30 $191.10$110,000 $1.87 $3.19 $3.19 $3.19 $4.84 $6.49 $9.13 $14.63 $23.43 $44.44 $67.98 $110.33 $210.21$120,000 $2.04 $3.48 $3.48 $3.48 $5.28 $7.08 $9.96 $15.96 $25.56 $48.48 $74.16 $120.36 $229.32$130,000 $2.21 $3.77 $3.77 $3.77 $5.72 $7.67 $10.79 $17.29 $27.69 $52.52 $80.34 $130.39 $248.43$140,000 $2.38 $4.06 $4.06 $4.06 $6.16 $8.26 $11.62 $18.62 $29.82 $56.56 $86.52 $140.42 $267.54$150,000 $2.55 $4.35 $4.35 $4.35 $6.60 $8.85 $12.45 $19.95 $31.95 $60.60 $92.70 $150.45 $286.65$200,000 $3.40 $5.80 $5.80 $5.80 $8.80 $11.80 $16.60 $26.60 $42.60 $80.80 $123.60 $200.60 $382.20$250,000 $4.25 $7.25 $7.25 $7.25 $11.00 $14.75 $20.75 $33.25 $53.25 $101.00 $154.50 $250.75 $477.75$300,000 $5.10 $8.70 $8.70 $8.70 $13.20 $17.70 $24.90 $39.90 $63.90 $121.20 $185.40 $300.90 $573.30$350,000 $5.95 $10.15 $10.15 $10.15 $15.40 $20.65 $29.05 $46.55 $74.55 $141.40 $216.30 $351.05 $668.85$400,000 $6.80 $11.60 $11.60 $11.60 $17.60 $23.60 $33.20 $53.20 $85.20 $161.60 $247.20 $401.20 $764.40$450,000 $7.65 $13.05 $13.05 $13.05 $19.80 $26.55 $37.35 $59.85 $95.85 $181.80 $278.10 $451.35 $859.95$500,000 $8.50 $14.50 $14.50 $14.50 $22.00 $29.50 $41.50 $66.50 $106.50 $202.00 $309.00 $501.50 $955.50
Policy Provisions may vary by state. Refer to a certificate or enrollment brochure for details about coverage features and limitations.For internal use only: Policy number FDL1-504-707 vlife/blend-w/add/12
Products and services marketed under the Dearborn National® brand and the star logo are underwritten and/or provided by Dearborn National® LifeInsurance Company (Downers Grove, IL) (formerly known as Fort Dearborn Life Insurance Company®) in all states (excluding New York), the District of Columbia, the United States Virgin Islands, the British Virgin Islands, Guam and Puerto Rico.
OKLAHOMA BAPTIST UNIVERSITY - #F019973
100,000$
45-49
Age
ATTAINED AGE
35-3940-44
60-6455-5950-54
30-34
20-24
Monthly Premium per Family
25,000$
25-29
EMPLOYEE Voluntary Life Monthly
rates per $1,000
Dependent Life (Children)
65-69
EmployeeMonthly rates per $1,000
70-7475+
Voluntary AD&D
Under 20
26
VOLUNTARY GROUP LIFE AND AD&DPREMIUM RATE GRID
Eligibility
You are eligible to enroll if you work the minimum number of hours per week by your employer, and you have satisfied any waiting period.You must be covered under the basic life plan sponsored by your employer in SD and VT.
Voluntary Life/AD&D Insurance RatesEmployee Benefit: $10,000 - $500,000 in $10,000 increments. $0.029Spouse Benefit: $5,000 - $100,000 in $5,000 increments, but not to exceed $0.029
50% of the employee benefit. $0.029$0.044
Note: Spouse may not have coverage unless the employee has coverage. $0.059The amount of spouse life insurance is limited to 50% of the employee benefit in FL, KS, NE and PR. $0.083The spouse benefit may not exceed the employee benefit amount in AZ, CA, IL, MD, NJ, RI, VT, VA and WA. $0.133The Spouse amount may not exceed the amount for which the employee is eligible in TX and NY. $0.213Guarantee Issue* $0.404Employee $0.618Spouse $1.003* NEW EMPLOYEES ONLY $1.911
$1.911Child CoverageLive birth to 14 days: $1,000Ages 15 days to 6 months: $1,000Age 6 months to age 19 (to 23 if full-time student): $1,000 - $10,000, in $1,000 increments. $0.017
Life AD&D$1,000 0.22 0.02$2,000 0.45 0.03$3,000 0.67 0.05$4,000 0.89 0.07$5,000 1.12 0.09$6,000 1.34 0.10$7,000 1.56 0.12$8,000 1.78 0.14
Voluntary Life/AD&D Insurance $9,000 2.01 0.15$10,000 2.23 0.17
Monthly Premium Cost (Based on 12 payroll deductions per year)
Benefit Amount
SP AD&D <20 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74
$5,000 $0.09 $0.15 $0.15 $0.15 $0.22 $0.30 $0.42 $0.67 $1.07 $2.02 $3.09 $5.02 $9.56$10,000 $0.17 $0.29 $0.29 $0.29 $0.44 $0.59 $0.83 $1.33 $2.13 $4.04 $6.18 $10.03 $19.11$15,000 $0.26 $0.44 $0.44 $0.44 $0.66 $0.89 $1.25 $2.00 $3.20 $6.06 $9.27 $15.05 $28.67$20,000 $0.34 $0.58 $0.58 $0.58 $0.88 $1.18 $1.66 $2.66 $4.26 $8.08 $12.36 $20.06 $38.22$25,000 $0.43 $0.73 $0.73 $0.73 $1.10 $1.48 $2.08 $3.33 $5.33 $10.10 $15.45 $25.08 $47.78$30,000 $0.51 $0.87 $0.87 $0.87 $1.32 $1.77 $2.49 $3.99 $6.39 $12.12 $18.54 $30.09 $57.33$35,000 $0.60 $1.02 $1.02 $1.02 $1.54 $2.07 $2.91 $4.66 $7.46 $14.14 $21.63 $35.11 $66.89$40,000 $0.68 $1.16 $1.16 $1.16 $1.76 $2.36 $3.32 $5.32 $8.52 $16.16 $24.72 $40.12 $76.44$45,000 $0.77 $1.31 $1.31 $1.31 $1.98 $2.66 $3.74 $5.99 $9.59 $18.18 $27.81 $45.14 $86.00$50,000 $0.85 $1.45 $1.45 $1.45 $2.20 $2.95 $4.15 $6.65 $10.65 $20.20 $30.90 $50.15 $95.55$55,000 $0.94 $1.60 $1.60 $1.60 $2.42 $3.25 $4.57 $7.32 $11.72 $22.22 $33.99 $55.17 $105.11$60,000 $1.02 $1.74 $1.74 $1.74 $2.64 $3.54 $4.98 $7.98 $12.78 $24.24 $37.08 $60.18 $114.66$65,000 $1.11 $1.89 $1.89 $1.89 $2.86 $3.84 $5.40 $8.65 $13.85 $26.26 $40.17 $65.20 $124.22$70,000 $1.19 $2.03 $2.03 $2.03 $3.08 $4.13 $5.81 $9.31 $14.91 $28.28 $43.26 $70.21 $133.77$75,000 $1.28 $2.18 $2.18 $2.18 $3.30 $4.43 $6.23 $9.98 $15.98 $30.30 $46.35 $75.23 $143.33$80,000 $1.36 $2.32 $2.32 $2.32 $3.52 $4.72 $6.64 $10.64 $17.04 $32.32 $49.44 $80.24 $152.88$85,000 $1.45 $2.47 $2.47 $2.47 $3.74 $5.02 $7.06 $11.31 $18.11 $34.34 $52.53 $85.26 $162.44$90,000 $1.53 $2.61 $2.61 $2.61 $3.96 $5.31 $7.47 $11.97 $19.17 $36.36 $55.62 $90.27 $171.99$95,000 $1.62 $2.76 $2.76 $2.76 $4.18 $5.61 $7.89 $12.64 $20.24 $38.38 $58.71 $95.29 $181.55
$100,000 $1.70 $2.90 $2.90 $2.90 $4.40 $5.90 $8.30 $13.30 $21.30 $40.40 $61.80 $100.30 $191.10
Policy Provisions may vary by state. Refer to a certificate or enrollment brochure for details about coverage features and limitations.For internal use only: Policy number FDL1-504-707 vlife/blend-w/add/12
Products and services marketed under the Dearborn National® brand and the star logo are underwritten and/or provided by Dearborn National® LifeInsurance Company (Downers Grove, IL) (formerly known as Fort Dearborn Life Insurance Company®) in all states (excluding New York), the District of Columbia, the United States Virgin Islands, the British Virgin Islands, Guam and Puerto Rico.
Voluntary AD&DMonthly rates per $1,000
Spouse
Dependent Life (Children)Monthly Premium per Family
ATTAINED AGE
25,000$ 65-6970-7475+
50-5455-59
100,000$ 60-64
20-2425-2930-3435-3940-4445-49
OKLAHOMA BAPTIST UNIVERSITY - #F019973
SPOUSEVoluntary Life
Monthly rates per $1,000
AgeUnder 20
27

MEDICAL COVERAGEDISABILITY COVERAGE
Disability CoverageYou receive Long Term Disability coverage to replace a portion or your income if you become disabled due to a non-work related injury or illness.
An illness or injury that keeps you out of work for a long period of time can be financially devastating for you and your family. These plans are designed to help protect your financial security by providing replacement income if you are disabled due to anon-work related injury or illness.
Your disability benefits coordinate with other sources of disability income you receive, such as Social Security, Workers Compensation and State Disability, to provide you with a steady source of income.
LONG-TERM DISABILITY (LTD)
Benefits Begin After 90 Days of Disability
Benefit Duration Normal Retirement Age
Income Replaced 60% of Earnings
Maximum Benefit $8,000 Per Month
28

How do I report a long-term disability (LTD) claim? Simply do one of the following:
Call toll-free 1.800.36.Cigna (24462) or 1.866.562.8421(Español). A representative will walk you through the process.
Fill out a claim form online at myCigna.com.
When do I report a claim? At least 30 days before the start of your LTD.
What information do I need? Before you call or go online, please have this information handy:
Your name, address, phone number, birth date, Social Securitynumber and email address.
Employment information, such as date hired and job title.
The reason for your claim – illness, injury or pregnancy.
A description of your illness, symptoms, and/or diagnosis.Include the date your symptoms started and if you’ve had thesesymptoms before.
Workers’ compensation claims you’ve filed or plan to file.
Details about doctor, hospital or clinic visits, including datesand contact information.
What happens next? During the call, we’ll ask for your permission to get your medical
information. Here’s how it works:
After you give us your claim information, you’ll be transferred toa recorded message.
Listen to the recording and answer “Yes” or “No” to the questions.
At the end of the recording, say “Yes” if you give permission or“No” if you do not.
You can cancel your permission at any time by calling yourCigna claim manager.
After the call, Cigna will send you a letter. It’ll include a copy of the recorded message for your records. It’ll also include a form that gives us permission to get other information we may need to finish
processing your claim. Please sign and return that form. Check with your doctor to see if there are any other forms you need to sign.
A Cigna claim manager will call you and your employer for a list of
your job requirements. The claim manager will also call your doctor for your medical records. This information will help us figure out how long you may be out of work, and the benefits you may be able
to receive.
What happens if my claim is approved? Cigna will send you an approval letter that gives you an
explanation of your benefits.
Cigna will tell your employer that we approved your claim, andthe date you plan to return to work.
What happens if my claim is denied? Cigna will send you a letter that explains why. The letter will also
tell you how you can appeal the decision.
Cigna will let your employer know the claim is denied.
You should call your employer when you get the letter to discussyour return-to-work date.
How to report a LONG-TERM DISABILITY CLAIM Under your company’s group disability insurance plan
How to Report a Disability 1.800.36.Cigna (24462) or 1.866.562.8421 (Español)
Visit: myCigna.com
Please have this information handy:
Your name, address, phone number, birth date, date of hire,Social Security number and your employer’s name, address andphone number.
Date of your claim and when you plan to return to work. If you’repregnant, give your expected delivery date.
Name, address and phone number of each doctor you areseeing for this absence.
Cut and carry for easy reference
If you need immediate medical attention, please call 911
29

What can I expect while I’m out? Your Cigna claim manager will stay in touch to help you return to work quickly and safely. We may work with you, your doctor and your employer to talk about different work options. This may include
an adjustment to your job or work schedule. Your employer may also call you to check on your progress and offer support.
What if I plan to return to work when my long-term disability benefits end? Your Cigna claim manager may work with your employer on any
return-to-work plans. Your benefit payments will be calculated by the exact date you return to work, and whether or not you return to work part-time or full-time. This will also help determine if you qualify
for continued payments.
Question? Call 1.800.36.Cigna (24462). A Cigna representative is available to help you between 7:00 am and 7:00 pm CST.
If you have a question regarding an existing claim or you need plan
information, please contact your (inset claim office name claim
office) claim office at (insert claim office phone number).
“Cigna” is a registered service mark, and the “Tree of Life” logo and GO YOU are service marks, of Cigna Intellectual Property, Inc., licensed for use by Cigna Corporation and its operating subsidiaries. All products and services are provided exclusively by such operating subsidiaries and not by Cigna Corporation. Such operating subsidiaries include Life Insurance Company of North America, Cigna Life Insurance Company of New York, and Connecticut General Life Insurance Company. All models are used for illustrative purposes only. ©2012 Cigna. Some content provided under license. 617496l LTD 859634
30

MEDICAL COVERAGEEm
ployee Assistance (EAP) / Life Assistance Program (LAP)
Employee Assistance ProgramPersonal issues, planning for life events or simply managing daily life can affect your work, health and family.Cigna provides support, resources and information for personal and work-life issues. Cigna is company-sponsored, confidential and provided at no charge to you and your dependents.
Confidential CounselingThis no-cost counseling service helps you address stress, relationship and other personal issues you and your family may face. Cigna Advocates, who are available to you 24/7, will listen to your concerns and quickly refer you to in-person counseling and other local resources for:
• Stress, anxiety and depression • Job pressures• Relationship/marital conflicts • Grief and loss• Problems with children • Substance abuse
Other Information and ResourcesIn addition to Confidential Counseling services, Cigna provides many services and resources to assist you with:
• Financial Information and Resources• Legal Consultation• Parenting• Online Skill Builders• Self- Service Support• Help for New Parents
Call to get the assistance you need:Toll Free – 800-538-3543or visit www.cignabehavior.com/CGI.com
31

Whatever life throws at you - THROW IT OUR WAY.
“Cigna,” the “Tree of Life” logo and “GO YOU” are registered service marks of Cigna Intellectual Property, Inc., licensed for use by Cigna Corporation and its operating subsidiaries. All products and services are provided by or through such operating subsidiaries and not by Cigna Corporation. Such operating subsidiaries include Connecticut General Life Insurance Company, Cigna Health and Life Insurance Company, Life Insurance Company of North America, Cigna Life Insurance Company of New York, Cigna Behavioral Health, Inc., and HMO or service company subsidiaries of Cigna Health Corporation.
877376 06/14 © 2014 Cigna. Some content provided under license.
1. Some Healthy Rewards programs are not available in all states. If your Cigna plan includes coverage for any of these services, this program is in addition to, not instead of, your plan benefits. A discount program is NOT insurance, and you must pay the entire discounted charge.
2. Legal consultations and discounts are excluded for employment-related issues.
Life. Just when you think you have it figured out, along comes a challenge. But whether those challenges are big or small, your Life Assistance Program is available to help you and your family find a solution and restore your peace of mind.
Call us anytime, any day.
We’re just a phone call away whenever you need us – at no cost to you. An advocate is ready to help assess your needs and develop a solution to help resolve your concerns. He or she can also direct you to an array of resources in your community and online tools, including an article library.
Visit a specialist.
For face-to-face assistance, you have three sessions available to you and your household members. Call us to request a referral.
Reward yourself.
Access your Healthy Rewards®1 discount program for discounts on a range of health and wellness services and products from participating providers.
Achieve work/life balance.
It’s a constant challenge. If you’d like help handling life’s demands, call us for extra support. We can provide guidance or a referral to a service in your community on topics such as:
Legal consultation.2 Receive a 30-minute free consultation and up to a 25% discount on select fees.
Parenting. Receive guidance on child development, sibling rivalry, separation anxiety and much more.
Senior care. Learn about challenges and solutions associated with caring for an aging loved one.
Child care. Whether you need care all day or just after school, find a place that’s right for your family.
Pet Care. From grooming to boarding to veterinary services, find what you need to care for your pet.
Temporary back-up care. Don’t let an unplanned event get the best of you – find back-up child care.
Life Assistance Program 24/7
These are just a few examples of the support available to you. Call to get the assistance you need to help resolve life’s challenges.
800.538.3543 | Visit us at: www.CignaBehavioral.com/CGI
Self-service support – at your fingertips. Educational materials on work/life topics such as caregiving, daily living and working smarter are available online, as well as personal assessments and interactive tools, including a savings center and relocation center.
Additional features. Try using the online skill builders or attend a webinar to help you learn new skills and adopt positive work/life balance habits – for good.
Call us anytime, any day or go online for information or resources to help resolve life’s challenges.
32

NOTIFICATIONS
CHIP Notice COBRA General Notice
HIPAA Basics – Your Right to Privacy Lifetime and Annual Limits
Medicare Part D Women’s Health & Cancer Rights Act
Mental Health Parity & Addiction Equity Dependent Coverage
Special Enrollment Notice Patient Protection
33

Premium Assistance under Medicaid and the Children’s Health Insurance Program (CHIP)
If you or your children are eligible for Medicaid or CHIP and you’re eligible for health coverage from your employer, your state may have a premium assistance program that can help pay for coverage, using funds from their Medicaid or CHIP programs. If you or your children aren’t eligible for Medicaid or CHIP, you won’t be eligible for these premium assistance programs but you may be able to buy individual insurance coverage through the Health Insurance Marketplace. For more information, visit www.healthcare.gov.
If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, contact your State Medicaid or CHIP office to find out if premium assistance is available.
If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, ask your state if it has aprogram that might help you pay the premiums for an employer-sponsored plan.
If you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must allow you to enroll in your employer plan if you aren’t already enrolled. This is called a “special enrollment” opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, contact the Department of Labor at www.askebsa.dol.gov or call 1-866-444-EBSA (3272).
If you live in one of the following states, you may be eligible for assistance paying your employer health plan premiums. The following list of states is current as of January 31, 2016. Contact your State for more information on eligibility –
ALABAMA – Medicaid GEORGIA – Medicaid
Website: www.myalhipp.com
Phone: 1-855-692-5447
Website: http://dch.georgia.gov
- Click on Health Insurance Premium Payment (HIPP)
Phone: 404-656-4507
ALASKA – Medicaid INDIANA – Medicaid
Website: http://health.hss.state.ak.us/dpa/programs/medicaid/
Phone (Outside of Anchorage): 1-888-318-8890
Phone (Anchorage): 907-269-6529
Healthy Indiana Plan for low-income adults 19-64
Website: http://www.hip.in.gov Phone: 1-877-438-4479
All other Medicaid
Website: http://www.indianamedicaid.com
Phone 1-800-403-0964
COLORADO – Medicaid IOWA – Medicaid
Medicaid Website: http://www.colorado.gov/hcpf
Medicaid Customer Contact Center: 1-800-221-3943
Website: www.dhs.state.ia.us/hipp/
Phone: 1-888-346-9562 FLORIDA – Medicaid KANSAS – Medicaid
Website: https://www.flmedicaidtplrecovery.com/
Phone: 1-877-357-3268
Website: http://www.kdheks.gov/hcf/
Phone: 1-785-296-3512
34

KENTUCKY – Medicaid NEW HAMPSHIRE – Medicaid
Website: http://chfs.ky.gov/dms/default.htm
Phone: 1-800-635-2570
Website: http://www.dhhs.nh.gov/oii/documents/hippapp.pdf
Phone: 603-271-5218
LOUISIANA – Medicaid NEW JERSEY – Medicaid and CHIP
Website: http://dhh.louisiana.gov/index.cfm/subhome/1/n/331
Phone: 1-888-695-2447
Medicaid Website: http://www.state.nj.us/humanservices/dmahs/clients/medicaid/
Medicaid Phone: 609-631-2392
CHIP Website: http://www.njfamilycare.org/index.html
CHIP Phone: 1-800-701-0710
MAINE – Medicaid NEW YORK – Medicaid
Website: http://www.maine.gov/dhhs/ofi/public-assistance/index.html
Phone: 1-800-977-6003
TTY: Maine relay 711
Website: http://www.nyhealth.gov/health_care/medicaid/
Phone: 1-800-541-2831
MASSACHUSETTS – Medicaid and CHIP NORTH CAROLINA – Medicaid
Website: http://www.mass.gov/MassHealth
Phone: 1-800-462-1120
Website: http://www.ncdhhs.gov/dma
Phone: 919-855-4100
MINNESOTA – Medicaid NORTH DAKOTA – Medicaid
Website: http://mn.gov/dhs/ma/
Phone: 1-800-657-3739
Website: http://www.nd.gov/dhs/services/medicalserv/medicaid/
Phone: 1-844-854-4825
MISSOURI – Medicaid OKLAHOMA – Medicaid and CHIP
Website: http://www.dss.mo.gov/mhd/participants/pages/hipp.htm
Phone: 573-751-2005
Website: http://www.insureoklahoma.org
Phone: 1-888-365-3742
MONTANA – Medicaid OREGON – Medicaid
Website: http://dphhs.mt.gov/MontanaHealthcarePrograms/HIPP
Phone: 1-800-694-3084
Website: http://www.oregonhealthykids.gov http://www.hijossaludablesoregon.gov Phone: 1-800-699-9075
NEBRASKA – Medicaid PENNSYLVANIA – Medicaid
Website: http://dhhs.ne.gov/Children_Family_Services/AccessNebraska/Pages/accessnebraska_index.aspx
Phone: 1-855-632-7633
Website: http://www.dpw.state.pa.us/hipp
Phone: 1-800-692-7462
NEVADA – Medicaid RHODE ISLAND – Medicaid
Medicaid Website: http://dwss.nv.gov/
Medicaid Phone: 1-800-992-0900
Website: www.ohhs.ri.gov
Phone: 401-462-5300
35

SOUTH CAROLINA – Medicaid VIRGINIA – Medicaid and CHIP
Website: http://www.scdhhs.gov
Phone: 1-888-549-0820
Medicaid Website: http://www.coverva.org/programs_premium_assistance.cfm
Medicaid Phone: 1-800-432-5924
CHIP Website: http://www.coverva.org/programs_premium_assistance.cfm
CHIP Phone: 1-855-242-8282
SOUTH DAKOTA - Medicaid WASHINGTON – Medicaid
Website: http://dss.sd.gov
Phone: 1-888-828-0059
Website: http://www.hca.wa.gov/medicaid/premiumpymt/pages/ index.aspx
Phone: 1-800-562-3022 ext. 15473
TEXAS – Medicaid WEST VIRGINIA – Medicaid
Website: https://www.gethipptexas.com/
Phone: 1-800-440-0493
Website: http://www.dhhr.wv.gov/bms/Medicaid%20Expansion/Pages/default.aspx.
Phone: 1-877-598-5820, HMS Third Party Liability
UTAH – Medicaid and CHIP WISCONSIN – Medicaid and CHIP
Website:
Medicaid: http://health.utah.gov/medicaid
CHIP: http://health.utah.gov/chip
Phone: 1-877-543-7669
Website:
https://www.dhs.wisconsin.gov/publications/p1/p10095.pdf
Phone: 1-800-362-3002
VERMONT– Medicaid WYOMING – Medicaid
Website: http://www.greenmountaincare.org/
Phone: 1-800-250-8427
Website: https://wyequalitycare.acs-inc.com/
Phone: 307-777-7531
To see if any other states have added a premium assistance program since January 31, 2016, or for more information on special enrollment rights, contact either: U.S. Department of Labor U.S. Department of Health and Human Services Employee Benefits Security Administration Centers for Medicare & Medicaid Services www.dol.gov/ebsa www.cms.hhs.gov 1-866-444-EBSA (3272) 1-877-267-2323, Menu Option 4, Ext. 61565 OMB Control Number 1210-0137 (expires 10/31/2016)
36

General Notice Of COBRA Continuation Coverage Rights ** Continuation Coverage Rights Under COBRA **
Introduction You’re getting this notice because you recently gained coverage under a group health plan (the Plan). This notice has important information about your right to COBRA continuation coverage, which is a temporary extension of coverage under the Plan. This notice explains COBRA continuation coverage, when it may become available to you and your family, and what you need to do to protect your right to get it. When you become eligible for COBRA, you may also become eligible for other coverage options that may cost less than COBRA continuation coverage.
The right to COBRA continuation coverage was created by a federal law, the Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA). COBRA continuation coverage can become available to you and other members of your family when group health coverage would otherwise end. For more information about your rights and obligations under the Plan and under federal law, you should review the Plan’s Summary Plan Description or contact the Plan Administrator.
You may have other options available to you when you lose group health coverage. For example, you may be eligible to buy an individual plan through the Health Insurance Marketplace. By enrolling in coverage through the Marketplace, you may qualify for lower costs on your monthly premiums and lower out-of-pocket costs. Additionally, you may qualify for a 30- day special enrollment period for another group health plan for which you are eligible (such as a spouse’s plan), even if that plan generally doesn’t accept late enrollees.
What is COBRA continuation coverage? COBRA continuation coverage is a continuation of Plan coverage when it would otherwise end because of a life event. This is also called a “qualifying event.” Specific qualifying events are listed later in this notice. After a qualifying event, COBRA continuation coverage must be offered to each person who is a “qualified beneficiary.” You, your spouse, and your dependent children could become qualified beneficiaries if coverage under the Plan is lost because of the qualifying event. Under the Plan, qualified beneficiaries who elect COBRA continuation coverage must pay for COBRA continuation coverage.
If you’re an employee, you’ll become a qualified beneficiary if you lose your coverage under the Plan because of the following qualifying events:
• Your hours of employment are reduced, or• Your employment ends for any reason other than your gross misconduct.
If you’re the spouse of an employee, you’ll become a qualified beneficiary if you lose your coverage under the Plan because of the following qualifying events:
• Your spouse dies;• Your spouse’s hours of employment are reduced;• Your spouse’s employment ends for any reason other than his or her gross misconduct;• Your spouse becomes entitled to Medicare benefits (under Part A, Part B, or both); or• You become divorced or legally separated from your spouse.
Your dependent children will become qualified beneficiaries if they lose coverage under the Plan because of the following qualifying events:
• The parent-employee dies;• The parent-employee’s hours of employment are reduced;• The parent-employee’s employment ends for any reason other than his or her gross misconduct;• The parent-employee becomes entitled to Medicare benefits (Part A, Part B, or both);• The parents become divorced or legally separated; or• The child stops being eligible for coverage under the Plan as a “dependent child.”
37

When is COBRA continuation coverage available? The Plan will offer COBRA continuation coverage to qualified beneficiaries only after the Plan Administrator has been notified that a qualifying event has occurred. The employer must notify the Plan Administrator of the following qualifying events:
• The end of employment or reduction of hours of employment; • Death of the employee; or • The employee’s becoming entitled to Medicare benefits (under Part A, Part B, or both).
For all other qualifying events (divorce or legal separation of the employee and spouse or a dependent child’s losing eligibility for coverage as a dependent child), you must notify the Plan Administrator within 60 days after the qualifying event occurs. You must provide this notice to your Benefits Administrator listed in your Benefits Enrollment Guide. How is COBRA continuation coverage provided? Once the Plan Administrator receives notice that a qualifying event has occurred, COBRA continuation coverage will be offered to each of the qualified beneficiaries. Each qualified beneficiary will have an independent right to elect COBRA continuation coverage. Covered employees may elect COBRA continuation coverage on behalf of their spouses, and parents may elect COBRA continuation coverage on behalf of their children. COBRA continuation coverage is a temporary continuation of coverage that generally lasts for 18 months due to employment termination or reduction of hours of work. Certain qualifying events, or a second qualifying event during the initial period of coverage, may permit a beneficiary to receive a maximum of 36 months of coverage. There are also ways in which this 18-month period of COBRA continuation coverage can be extended: Disability extension of 18-month period of COBRA continuation coverage If you or anyone in your family covered under the Plan is determined by Social Security to be disabled and you notify the Plan Administrator in a timely fashion, you and your entire family may be entitled to get up to an additional 11 months of COBRA continuation coverage, for a maximum of 29 months. The disability would have to have started at some time before the 60th day of COBRA continuation coverage and must last at least until the end of the 18-month period of COBRA continuation coverage. Second qualifying event extension of 18-month period of continuation coverage If your family experiences another qualifying event during the 18 months of COBRA continuation coverage, the spouse and dependent children in your family can get up to 18 additional months of COBRA continuation coverage, for a maximum of 36 months, if the Plan is properly notified about the second qualifying event. This extension may be available to the spouse and any dependent children getting COBRA continuation coverage if the employee or former employee dies; becomes entitled to Medicare benefits (under Part A, Part B, or both); gets divorced or legally separated; or if the dependent child stops being eligible under the Plan as a dependent child. This extension is only available if the second qualifying event would have caused the spouse or dependent child to lose coverage under the Plan had the first qualifying event not occurred. Are there other coverage options besides COBRA Continuation Coverage? Yes. Instead of enrolling in COBRA continuation coverage, there may be other coverage options for you and your family through the Health Insurance Marketplace, Medicaid, or other group health plan coverage options (such as a spouse’s plan) through what is called a “special enrollment period.” Some of these options may cost less than COBRA continuation coverage. You can learn more about many of these options at www.healthcare.gov. If you have questions Questions concerning your Plan or your COBRA continuation coverage rights should be addressed to the contact or contacts identified below. For more information about your rights under the Employee Retirement Income Security Act (ERISA), including COBRA, the Patient Protection and Affordable Care Act, and other laws affecting group health plans, contact the nearest Regional or District Office of the U.S. Department of Labor’s Employee Benefits Security Administration (EBSA) in your area or visit www.dol.gov/ebsa. (Addresses and phone numbers of Regional and District EBSA Offices are available through EBSA’s website.) For more information about the Marketplace, visit www.HealthCare.gov.
38

Keep your Plan informed of address changes To protect your family’s rights, let the Plan Administrator know about any changes in the addresses of family members. You should also keep a copy, for your records, of any notices you send to the Plan Administrator.
Plan contact information Contact your Benefits Administrator listed in your Benefits Enrollment Guide for additional information about the plan and COBRA continuation coverage.
Please refer to the Plan’s most recent summary plan description for any updated Plan contact information.
HIPAA Basics Your Right to Privacy
In April 2003, the final regulations that place restrictions on how personally identifiable health information may be used and disclosed by certain organizations became effective.
These regulations (the Privacy Rules) implement the privacy requirements contained within the Administrative Simplification subtitle of the Health Insurance Portability and Accountability Act of 1996 (HIPAA).
While some states have laws that protect health information, the HIPAA Privacy Rules establish a uniform, minimum level of privacy protections for all health information. In summary, the HIPAA Privacy Rules:
• Set limits on how health information may be used and disclosed;
• Require that individuals be told how their health information will be used and disclosed;
• Provide individuals with a right to access, amend or copy their medical records;
• Give individuals a right to receive an accounting of disclosures, to request special restrictions, and toreceive confidential communications; and
• Impose fines where the requirements contained within the regulations are not met.
Restrictions on Use & Disclosure The rules allow health care providers, health plans, and health care clearinghouses (Covered Entities) to use and disclose your personally identifiable health information for purposes of treatment, payment, or health care operations.
For example, your health care provider may submit your health information to a health insurance company in order to seek payment for the treatment provided to you. Your primary care physician can share your health information with a specialist that he or she recommends you consult. In these cases, your written permission to disclose your health information is not required.
In general, any use or disclosure not considered treatment, payment, or a health care operation requires your written authorization, unless an exception applies. For example, your physician may not share your health information with your employer or a life insurance carrier without your written permission.
However, disclosure of health information is permitted for certain purposes specifically listed in the HIPAA Privacy Rules, such as national security, law enforcement and public health issues. If you authorize release of your health information to a third party, the information released may no longer be protected by HIPAA.
Notice of Privacy Practices You are entitled to receive an explanation of how your personally identifiable health information will be used and disclosed.
For example, a physician or hospital is required to provide you with a Notice of Privacy Practices at your first visit. You will be required to sign an acknowledgement indicating that you received the Notice of Privacy Practices.
If you have health insurance coverage, the insurance company or health plan will also provide you with a Notice of Privacy Practices immediately after you are enrolled in the plan. It is important that you read the Notice of Privacy Practices in order to understand your rights and know who to contact if you feel your privacy rights have been violated.
39

Right to Access, Amend, or Copy You have a right to view and copy your medical records. You may be charged a fee for the cost of reproduction. If you believe that information within your medical records is incorrect or if important information is missing, you have a right to request that your medical records be amended. Right to an Accounting of Disclosure You also have a right to a list of uses and disclosures made of your medical records where the use or disclosure was not for purposes of treatment, payment, health care operations, or pursuant to your written authorization. Right to Request Restrictions You may request in writing that a health care provider or health plan not use or disclose information for treatment, payment, or other administrative purposes unless specifically authorized by you, when required by law, or in emergency circumstances. Health care providers and health plans must consider your request, but are not legally obligated to agree to those restrictions. Confidential Communications You have a right to receive confidential communications containing your health information. Health care providers and health plans are required to accommodate your reasonable requests. For example, you may ask that a physician contact you at your place of employment or send communications regarding treatment to an alternate address. Violations of Privacy Rights If you believe that your privacy rights have been violated, you may contact the Privacy Officer for the organization that you feel has violated your right to privacy. The name of the Privacy Officer should be included in the Notice of Privacy Practices provided to you by that organization. If the Privacy Officer does not adequately resolve your concerns, you may contact the Department of Health and Human Services — Office of Civil Rights (OCR). OCR is responsible for enforcing the HIPAA Privacy Rules. Its Web site contains instructions on how to file a complaint www.hhs.gov/ocr/privacy/hipaa/complaints and a complaint form www.hhs.gov/ocr/privacy/hipaa/complaints/hipcomplaintpackage.pdf Penalties for Noncompliance The HIPAA Privacy Rules do not provide individuals with a private right to sue, although methodologies for allowing a portion of civil penalties to be paid to affected individuals must be established by February 17, 2012. Currently, health care providers, health plans, and health care clearinghouses that do not comply with the HIPAA Privacy Rules may be subject to civil money penalties ranging from $100 to $50,000 per violation, with maximum penalties ranging from $25,000 per year to $1.5 million per year. Criminal violations of the HIPAA Privacy Rules may also be referred to the Department of Justice for enforcement. Criminal penalties for such violations include:
• $50,000 and/or up to one year in prison for knowingly obtaining or disclosing protected health information not permitted by law;
• $100,000 and/or up to five years in prison for obtaining or disclosing protected health information under
false pretenses; and
• $250,000 and/or up to ten years in prison for obtaining protected health information with an intent to sell, transfer, or use it for commercial advantage, personal gain, or malicious harm.
State Attorneys General (AG) may also bring suit against Covered Entities to enjoin further violations and obtain damages on behalf of residents of their states, if HHS has not already taken action. The AG may seek damages of up to $100 per violation, with a maximum of $25,000 per year for identical violations. HIPAA Privacy Resources
• Office of Civil Rights (HHS) www.hhs.gov/ocr/ • Health Privacy Project www.healthprivacy.org
40

Lifetime and Annual Limits PPACA generally prohibits group health plans, and group and individual health insurance issuers, from imposing lifetime or annual limits on the dollar value of health benefits, effective for plan years beginning on or after Sept. 23, 2010. Although annual limits are generally prohibited, “restricted annual limits” are permitted for essential health benefits for plan years beginning before Jan. 1, 2014. Restricted Annual Limits The interim final rules establish a three-year phased approach for restricted annual limits. Annual limits may not be less than the following amounts for plan years beginning before Jan. 1, 2014:
• $750,000 for plan years beginning on or after Sept. 23, 2010, but before Sept. 23, 2011; • $1.25 million for plan years beginning on or after Sept. 23, 2011, but before Sept. 23, 2012; and • $2 million for plan years beginning on or after Sept. 23, 2012, but before Jan. 1, 2014.
These are minimums for plan years; plans may use higher annual limits or impose no limits. The limits apply on an individual-by-individual basis, so that any annual limit on benefits applied to families cannot cause an individual to be denied the minimum annual benefit for the plan year. The restricted annual limits are designed to ensure that individuals would have access to needed services with a minimal impact on premiums. However, they could affect limited benefit plans or “mini-med” plans that generally have limits significantly below the permitted limits. The regulations provide that the restricted annual limits could be waived by the Department of Health and Human Services (HHS) if compliance with the restrictions would result in a significant decrease in access to benefits or a significant increase in premiums. HHS granted a number of waivers and then closed the waiver program to new applications effective Sept. 22, 2011. Waivers and/or extensions received before that date could be effective until plan years beginning on or after Jan. 1, 2014, when all annual limits for essential health benefits will be prohibited. As a condition to receiving a waiver, a group health plan or health insurance issuer must provide a notice informing each participant that the plan or policy does not meet the restricted annual limits for essential benefits because it has received a waiver of that requirement. Waiver recipients must also provide annual updates to HHS regarding plan information and benefits. Covered Plans The prohibition on lifetime and annual limits applies to both new and grandfathered group health plans. However, it does not apply to grandfathered individual policies. The restrictions on annual limits do not apply to account-based plans like health flexible spending arrangements (health FSAs), medical savings accounts (MSAs) and health savings accounts (HSAs). Essential Health Benefits PPACA specifically provides that plans may impose annual or lifetime per-individual limits on specific covered benefits that are not “essential health benefits.” Each state will set its own definition of essential health benefits, but it will include at least the following general categories of items and services:
• Ambulatory patient services; • Emergency services; • Hospitalization; • Maternity and newborn care; • Mental health and substance use disorder services, including behavioral health treatment; • Prescription drugs; • Rehabilitative and habilitative services and devices; • Laboratory services; • Preventive and wellness services, including chronic disease management; and • Pediatric services, including oral and vision care.
Until standards are issued, plans can use a good faith effort to comply with a reasonable interpretation of essential health benefits and must apply it consistently. The interim final rules clarify that a plan can still exclude all benefits for a condition. Such exclusion will not be considered an annual or lifetime limit as long as no benefits are provided for the condition. Enrollment Opportunities Under the interim final rules, individuals who reached a lifetime limit prior to the date the regulations were effective and are otherwise eligible for plan coverage must have been given a notice that the lifetime limit no longer applies. They must have been permitted to re- enroll in the plan if they were no longer enrolled. The notices and enrollment opportunity must have been provided no later than the first day of the first plan year beginning on or after Sept. 23, 2010. Anyone who was eligible for the enrollment opportunity must have been treated as a special enrollee eligible to enroll in all of the benefit packages available to similarly situated individuals upon initial enrollment.
41
Important Notice About Your Prescription Drug Coverage and Medicare
Please read this notice carefully and keep it where you can find it. This notice has information about your current prescription drug coverage and about your options under Medicare’s prescription drug coverage. This information can help you decide whether or not you want to join a Medicare drug plan. If you are considering joining, you should compare your current coverage, including which drugs are covered at what cost, with the coverage and costs of the plans offering Medicare prescription drug coverage in your area. Information about where you can get help to make decisions about your prescription drug coverage is at the end of this notice.
There are two important things you need to know about your current coverage and Medicare’s prescription drug coverage:
1. Medicare prescription drug coverage became available in 2006 to everyone with Medicare. You can get this coverage if youjoin a Medicare Prescription Drug Plan or join a Medicare Advantage Plan (like an HMO or PPO) that offers prescription drugcoverage. All Medicare drug plans provide at least a standard level of coverage set by Medicare. Some plans may also offermore coverage for a higher monthly premium.
2. It has determined that our prescription drug coverage is, on average for all plan participants, expected to pay out as much asstandard Medicare prescription drug coverage pays and is therefore considered Creditable Coverage. Because your existingcoverage is Creditable Coverage, you can keep this coverage and not pay a higher premium (a penalty) if you later decide tojoin a Medicare drug plan.
When Can You Join A Medicare Drug Plan? You can join a Medicare drug plan when you first become eligible for Medicare and each year from October 15 to December 7. However, if you lose your current creditable prescription drug coverage, through no fault of your own, you will also be eligible for a two (2) month Special Enrollment Period (SEP) to join a Medicare drug plan.
What Happens To Your Current Coverage If You Decide to Join A Medicare Drug Plan? If you decide to join a Medicare drug plan, your current coverage will not be affected. Your current coverage pays for other health expenses in addition to prescription drugs. You and your dependents can keep this coverage if you elect Part D prescription drug coverage but this plan will not coordinate with your Part D coverage. If you do decide to join a Medicare drug plan and drop your current coverage, be aware that you and your dependents will not be able to get this coverage back until our next open enrollment period or if you experience a qualifying event.
When Will You Pay A Higher Premium (Penalty) To Join A Medicare Drug Plan? You should also know that if you drop or lose your current coverage and don’t join a Medicare drug plan within 63 continuous days after your current coverage ends, you may pay a higher premium (a penalty) to join a Medicare drug plan later. If you go 63 continuous days or longer without creditable prescription drug coverage, your monthly premium may go up by at least 1% of the Medicare base beneficiary premium per month for every month that you did not have that coverage. For example, if you go nineteen months without creditable coverage, your premium may consistently be at least 19% higher than the Medicare base beneficiary premium. You may have to pay this higher premium (a penalty) as long as you have Medicare prescription drug coverage. In addition, you may have to wait until the following October to join.
For More Information About This Notice Or Your Current Prescription Drug Coverage… Contact the person listed below for further information. NOTE: You’ll get this notice each year. You will also get it before the next period you can join a Medicare drug plan, and if this coverage changes. You also may request a copy of this notice at any time.
For More Information About Your Options Under Medicare Prescription Drug Coverage… More detailed information about Medicare plans that offer prescription drug coverage is in the “Medicare & You” handbook. You’ll get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly by Medicare drug plans. For more information about Medicare prescription drug coverage:
• Visit www.medicare.gov• Call your State Health Insurance Assistance Program (see the inside back cover of your copy of the “Medicare & You”
handbook for their telephone number) for personalized help• Call 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048.
If you have limited income and resources, extra help paying for Medicare prescription drug coverage is available. For information about this extra help, visit Social Security on the web at www.socialsecurity.gov, or call them at 1-800-772-1213 (TTY 1-800-325-0778).
Remember: Keep this Creditable Coverage notice. If you decide to join one of the Medicare drug plans, you may be required to provide a copy of this notice when you join to show whether or not you havemaintained creditable coverage and, therefore,
whether or not you are required to pay a higher premium (a penalty).
CMS Form 10182-CC Updated April 1, 2011 According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is 0938-0990. The time required to complete this information collection is estimated to average 8 hours per response initially, including the time to review instructions, search existing data resources, gather the data needed, and complete and review the information collection. If you have comments concerning the accuracy of the time estimate(s) or suggestions for improving this form, please write to: CMS, 7500 Security Boulevard, Attn: PRA Reports Clearance Officer, Mail Stop C4-26-05, Baltimore, Maryland 21244-1850.
42

Women’s Health and Cancer Rights Act (WHCRA) of 1998 Common questions and answers The benefits related to mastectomies changed quite a bit with the Women’s Health and Cancer Rights Act (WHCRA) of 1998. This article will answer some of the common questions patients have about the WHCRA.
What does WHCRA cover? If you are enrolled in a health plan that covers the medical and surgical costs of a mastectomy, the WHCRA states that your plan must also cover the costs of certain reconstructive surgery and other post-mastectomy benefits, including:
• All stages of reconstruction of the breast on which the mastectomy was performed• Surgery and reconstruction of the other breast to produce a symmetrical appearance• External breast forms that fit into your bra for before or during reconstruction• Treatment of any physical complications of the mastectomy, including lymphedema
I had a mastectomy due to non-cancer related health issues. Am I covered under WHCRA?
Yes. These rights are not limited to cancer patients. If your plan covers mastectomies, WHCRA rights apply.
My job does not offer a group health plan. Does WHCRA apply to my individual health insurance policy? Yes. WHCRA applies to group health plans that are provided by an employer or union as well as to individual health insurance policies that are not based on employment.
I receive health benefits through my church. Am I still covered under WHCRA? There are certain “church” and “governmental” plans that are not subject to this law. Generally, though, any plan that provides coverage for mastectomies must also comply with WHCRA. Check with your provider for information specific to your plan.
Will my co-pay for reconstructive surgery be more expensive than my co-pay for other health conditions? No. If your health plan requires a co-payment for other health conditions, the co-pay for your mastectomy benefits must be the same. For example, it is a violation of WHCRA for your plan to cover 90 percent of hip replacement surgery but to only cover 70 percent of breast reconstruction.
Is my health plan required to inform me of my rights under WHCRA? Yes. Your health plan must provide you with a notice of your rights under WHCRA when you first enroll in the health plan, and then annually after that.
43

The Mental Health Parity and Addiction Equity Act of 2008
Under the Mental Health Parity and Addiction Equity Act of 2008 (MHPAEA), the financial requirements and treatment limits that group health plans and health insurance issuers apply to mental health or substance use disorder benefits generally cannot be more restrictive than those applicable to medical and surgical benefits. The MHPAEA supplemented the Mental Health Parity Act of 1996 (MHPA), which required parity with respect to aggregate lifetime and annual dollar limits for mental health benefits. The MHPAEA also extended the parity requirements to substance use disorder benefits.
The MHPAEA generally applies to plans sponsored by employers with more than 50 employees, including self-insured plans and fully insured arrangements. The MHPAEA generally became effective for plan years beginning on or after Oct. 3, 2009 (Jan. 1, 2010 for calendar year plans).
The MHPAEA does not require a plan to provide mental health or substance use disorder benefits. However, if a plan provides medical and surgical benefits and mental health and substance use disorder benefits, it must comply with the federal parity requirements.
The MHPAEA contains the following parity requirements:
• The financial requirements (such as deductibles, copayments, coinsurance and out-of-pocket limits) applicableto mental health and substance use disorder benefits cannot be more restrictive than the predominant financialrequirements applied to substantially all medical and surgical benefits.
• Treatment limitations (such as frequency of treatment, number of visits, days of coverage or other similar limitson the scope or duration of coverage) must also comply with the MHPAEA’s parity requirements. Non-quantitative treatment limitations (such as medical management standards, formulary design anddeterminations of usual, customary or reasonable amounts) are subject to a separate parity requirement.
• If medical and surgical benefits are offered on an out-of-network basis, a plan or issuer must also offer mentalhealth and substance use disorder benefits on an out-of-network basis.
In addition, the MHPAEA requires plans to make certain information available with respect to mental health and substance use disorder benefits, such as the criteria for medical necessity determinations and the reason for any denial of reimbursement or payment for mental health or substance use disorder services.
The Departments of Health and Human Services, Labor and Treasury (Departments) issued interim final rules to implement the MHPAEA and to demonstrate how the MHPAEA applies to group health plans and health insurance issuers. The rules became applicable for plan years beginning on or after July 1, 2010.
A plan’s coverage or mental health and substance use disorder benefits may be affected by the health care reform law. The health care reform law is very broad and its specific effect on mental health and substance use disorder benefits is still somewhat unclear. Additional regulatory guidance would be helpful.
44

Dependent Coverage Up to Age 26 The Affordable Care Act (ACA) provides that health plans and issuers that offer dependent coverage to children on their parents’ plans must make the coverage available until the adult child reaches the age of 26. The extension of coverage to young adult children took effect on the first day of the first plan year that began on or after Sept. 23, 2010.
What Does the Law Require? Group health plans and health insurance issuers offering group or individual health insurance policies that provide dependent coverage of children must make coverage available for adult children up to age 26, regardless of the child’s marital status.
The mandate applies to plans that have “grandfathered” status under ACA and to non-grandfathered plans. However, for plan years beginning before Jan. 1, 2014, grandfathered plans are not required to cover adult children under age 26 if they are eligible for other employer-sponsored group health coverage.
Parents can decide whether to add adult children to their plan. ACA’s extension of dependent coverage did not create independent enrollment rights for dependents. In addition, there is no requirement to cover the child of a dependent child (that is, a grandchild).
Restrictions on Definition of “Dependent” ACA restricts the definition of “dependent” that health plans and issuers may use for children under the age of 26. A plan or issuer may not define dependent for purposes of eligibility for this coverage other than in terms of the child’s age and the relationship between the child and the participant.
For example, a plan or issuer may not deny or restrict coverage for a child who is under age 26 based on one or more of the following factors:
• Financial dependence on the participant or any other person;• Residency with the participant or with any other person;• Student status;• Marital status;• Employment status; or• Eligibility for other coverage (unless the plan or coverage has grandfathered status and the child is eligible for
other employer-sponsored group health coverage for plan years beginning before Jan. 1, 2014).
Although the term “child” is not specifically defined in ACA, guidance indicates that it means an individual who is a son, daughter, stepson, stepdaughter or adopted child of the participant. There is some suggestion that a foster child would be included as well, although this is not entirely clear.
Uniformity in Plan Terms The terms of the plan or health insurance coverage providing dependent coverage of children, including the premiums charged, cannot vary based on age (except for children who are age 26 or older). This means that adult children must be offered all of the benefit packages available to other plan participants, and these dependents cannot be required to pay more for coverage.
The following examples illustrate the uniformity requirement.
Example: A group health plan offers a choice of self-only or family health coverage. Dependent coverage is provided under family health coverage for children of participants who have not reached age 26. The plan imposes an additional premium surcharge for children who are older than age 18. This plan violates the uniformity requirement because the plan varies the terms for dependent coverage of children based on age.
Example: A group health plan offers a choice among the following tiers of health coverage: self-only, self-plus-one, self- plus-two and self-plus-three-or-more. The cost of coverage increases based on the number of covered individuals. The plan provides dependent coverage of children who have not reached age 26. In this example, the plan does not violate the uniformity requirement. Although the cost of coverage increases for tiers with more covered individuals, the increase applies without regard to the age of any child.
Example: A group health plan offers two benefit packages -- an HMO option and an indemnity option. Dependent coverage is provided for children of participants who have not reached age 26. The plan limits children who are older than age 18 to the HMO option. This plan violates the uniformity requirement because the plan, by limiting children who are older than age 18 to the HMO option, varies the terms for dependent coverage of children based on age.
45

When did the Law Become Effective? The extension of dependent coverage provision took effect for plan years beginning on or after Sept. 23, 2010, though some plans and issuers extended coverage to adult children before this date. All plans and issuers should now be in compliance with the age 26 dependent coverage requirement.
What if State Laws Differ from Federal Law? More than two-thirds of states have passed laws that require insured group health plans to cover dependents after they turn 18 years old, often into their mid to late 20s and in some cases later. For example, in New Jersey, unmarried children can stay on a parent's plan until they are 31 years old. These state mandates, to the extent they require coverage past age 26, will continue to apply to insured health coverage.
What are the Tax Effects of the extended dependent coverage? Under federal tax law, employers can offer tax-free health coverage to employees’ adult children through the end of the year in which the children turn age 26. It does not matter whether the children are tax dependents for federal income tax purposes. All states have passed tax laws conforming to the federal tax law.
Often, adult children that obtain coverage pursuant to state law are not tax dependents for federal income tax purposes. In the event state laws mandate coverage past age 26, federal tax law generally requires employers to impute the fair market value of the dependent coverage as income to employees for tax years after the children turn age 26, unless employees pay for the coverage on an after-tax basis.
More Information Additional information on ACA’s young adult coverage requirement is available at: www.healthcare.gov/law/features/choices/young-adult-coverage/index.html.
The interim final regulations on the young adult coverage requirement, as published in the Federal Register on May 13, 2010, are available at: www.gpo.gov/fdsys/pkg/FR-2010-05-13/pdf/2010-11391.pdf.
46

Special Enrollment Notice This notice is being provided to insure that you understand your right to apply for group health insurance coverage. You should read this notice even if you plan to waive coverage at this time.
Loss of Other Coverage If you are declining coverage for yourself or your dependents (including your spouse) because of other health insurance or group health plan coverage, you may be able to enroll yourself and your dependents in this plan if you or your dependents lose eligibility for that other coverage (or if the employer stops contributing toward your or your dependents’ other coverage). However, you must request enrollment within 30 days after your or your dependents’ other coverage ends (or after the employer stops contributing toward the other coverage).
Example: You waived coverage because you were covered under a plan offered by your spouse's employer. Your spouse terminates his employment. If you notify your employer within 30 days of the date coverage ends, you and your eligible dependents may apply for coverage under our health plan.
Marriage, Birth, or Adoption If you have a new dependent as a result of a marriage, birth, adoption, or placement for adoption, you may be able to enroll yourself and your dependents. However, you must request enrollment within 30 days after the marriage, birth, or placement for adoption.
Example: When you were hired by us, you were single and chose not to elect health insurance benefits. One year later, you marry. You and your eligible dependents are entitled to enroll in this group health plan. However, you must apply within 30 days from the date of your marriage.
Medicaid or CHIP If you or your dependents lose eligibility for coverage under Medicaid or the Children’s Health Insurance Program (CHIP) or become eligible for a premium assistance subsidy under Medicaid or CHIP, you may be able to enroll yourself and your dependents. You must request enrollment within 60 days of the loss of Medicaid or CHIP coverage or the determination of eligibility for a premium assistance subsidy.
Example: When you were hired by us, your children received health coverage under CHIP and you did not enroll them in our health plan. Because of changes in your income, your children are no longer eligible for CHIP coverage. You may enroll them in this group health plan if you apply within 60 days of the date of their loss of CHIP coverage.
For More Information or Assistance To request special enrollment or obtain more information, please contact your Benefits Administrator.
Note: If you and your eligible dependents enroll during a special enrollment period, as described above, you are not considered a late enrollee. Therefore, your group health plan may not require you to serve a pre-existing condition waiting period of more than 12 months. Any preexisting condition waiting period will be reduced by time served in a qualified plan.
47