choosing an appropriate oral contraceptive for your ... choosing an appropriate oral... · choosing...
TRANSCRIPT
1
Choosing Choosing Choosing Choosing an Appropriate an Appropriate an Appropriate an Appropriate Oral Contraceptive for Oral Contraceptive for Oral Contraceptive for Oral Contraceptive for Your Your Your Your PatientPatientPatientPatientDANIEL MA JERCZYK, PHARM.D.ASSISTANT PROFESSOR OF CLINICAL SCIENCESROOSEVELT UNIVERSITY, COLLEGE OF PHARMACY1400 N. ROOSEVELT BLVD. | SCHAUMBURG, IL 60173
Conflicts of Interest:
Dr. Majerczyk declares no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria.
Objectives: Pharmacist:
1. Describe the mechanism of action, types, benefits, and risks of oral contraceptives.
2. Identify risks and contraindications to oral contraceptives.
3. Choose the best and most effective contraceptive for a patient.
4. Discuss possible side effect/s associated with the use of oral contraceptives.
5. List patient counseling points on side effects and missed dose instructions for oral contraceptives.
Pharmacy Technician:
1. Discuss the types of drug classes found in oral contraceptives.
2. Recognize common adverse effects of oral contraceptives.
3. Identify patient characteristics that may be contraindications to the use of oral contraceptives.
Question 1
The progestin component of the contraceptive pill works by:
A. Inhibiting the release of follicle stimulating hormone (FSH) from the anterior pituitary
B. Increasing bleeding
C. Thinning the cervical mucus
D. Thickening the cervical mucus thicker, making it harder for the sperm to penetrate
2
Question 2
A contraindication to initiating a combined hormonal contraceptive is:
A. A migraine without aura and age <35 years old
B. Smoking 2 packs per day and age <35 years old
C. Current chlamydial infection
D. Blood pressure of 162/90 mmHg
Question 3
Which of the following is one of the most effective forms of contraception available:
A. The implant
B. The patch
C. The pill
D. The condom
Question 4
All of the following are considered potential unwanted side effects associated with the use of
hormonal contraceptives except:
A. Nausea
B. Dermatological Improvement
C. Weight gain
D. Hirsutism
Question 5
L.R. takes her norethindrone 0.35 mg pill every day at 3 pm. She was delayed today and realized
it it now 7 pm. What action should the patient take now:
A. She should take the pill ASAP
B. She must take 2 pills at once
C. She must use back-up contraception for the next 48 hours
D. She should start a new pack tomorrow
3
Background1,2
US has one of the highest rates of unintended pregnancy in the developed country
~ 50% of all pregnancies are unintended
~ 40% end in abortion
~ 1/3 of American women have an abortion at some point in their lives
Abortion rates has declined recently, the gap between the lower rates of unintended pregnancy in wealthy people and higher rates in disadvantaged groups has widened over the past 2 decades
This disparity suggests there is limited access to contraception for some women and adolescents, and points to the importance of addressing birth control with all patients at risk for unintended pregnancy
Meet K.L. & Y.D.
K.L.
◦ 27 year old female
◦ Current smoker
◦ Has seasonal allergies and thyroid disease
Y.D.
◦ 30 year old female
◦ Has a very busy life
◦ Afraid of needles
◦ Takes Rx and OTC medications
Questions to consider:
1. What more would you like to know/ask?
2. What contraceptive would you choose and why?
Initial Counseling3
Contraceptive counseling should aim to maximize:
◦ Efficacy
◦ Patient satisfaction
◦ Long-term adherence
Selecting an appropriate contraceptive method requires:
◦ Complete medical history, with special focus on ruling out the most common contraindications
◦ The World Health Organization (WHO) has produced a chart recording the absolute and relative contraindications to the different contraceptive methods
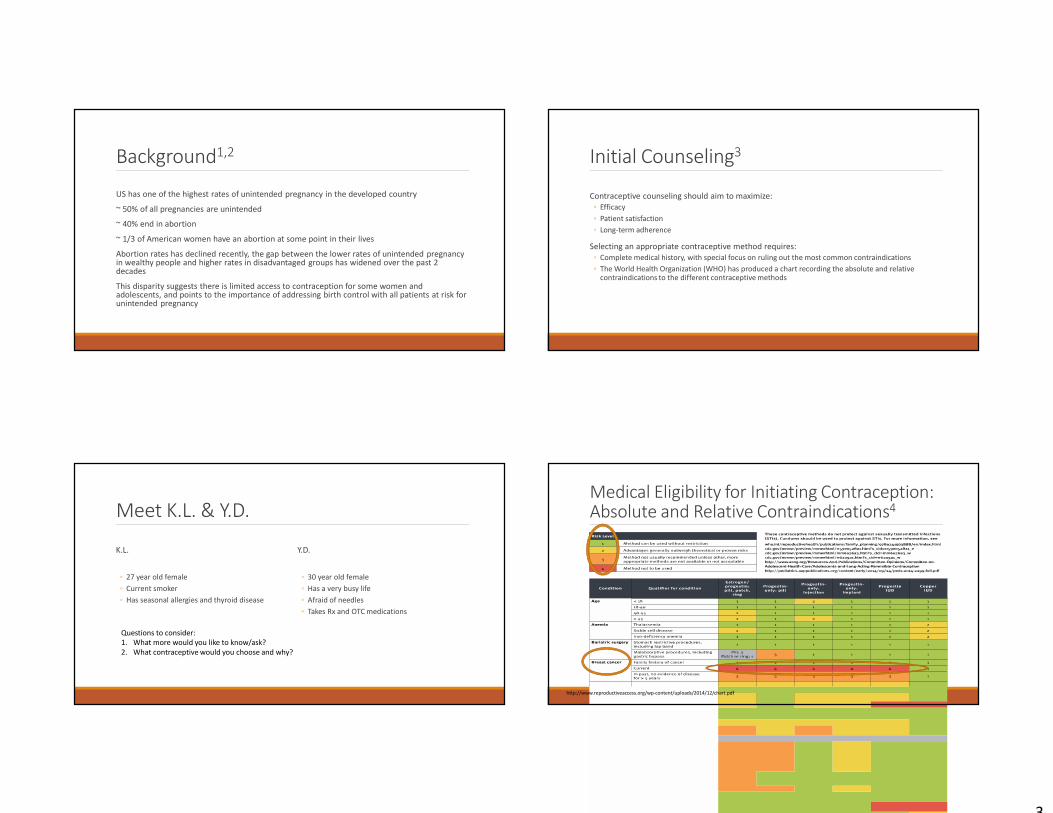
Medical Eligibility for Initiating Contraception: Absolute and Relative Contraindications4
http://www.reproductiveaccess.org/wp-content/uploads/2014/12/chart.pdf
4
Medical Eligibility for Initiating Contraception: Absolute and Relative Contraindications4
http://www.reproductiveaccess.org/wp-content/uploads/2014/12/chart.pdf
Hormonal Contraceptive Products
Pharmacology
◦ Mechanism of Action (MOA)
◦ Description of how hormonal contraceptive products affect phases of the menstrual cycle
Key features of agents
◦ Progestin content and effect
◦ Estrogen content and effect
◦ Combined (progestin and estrogen)
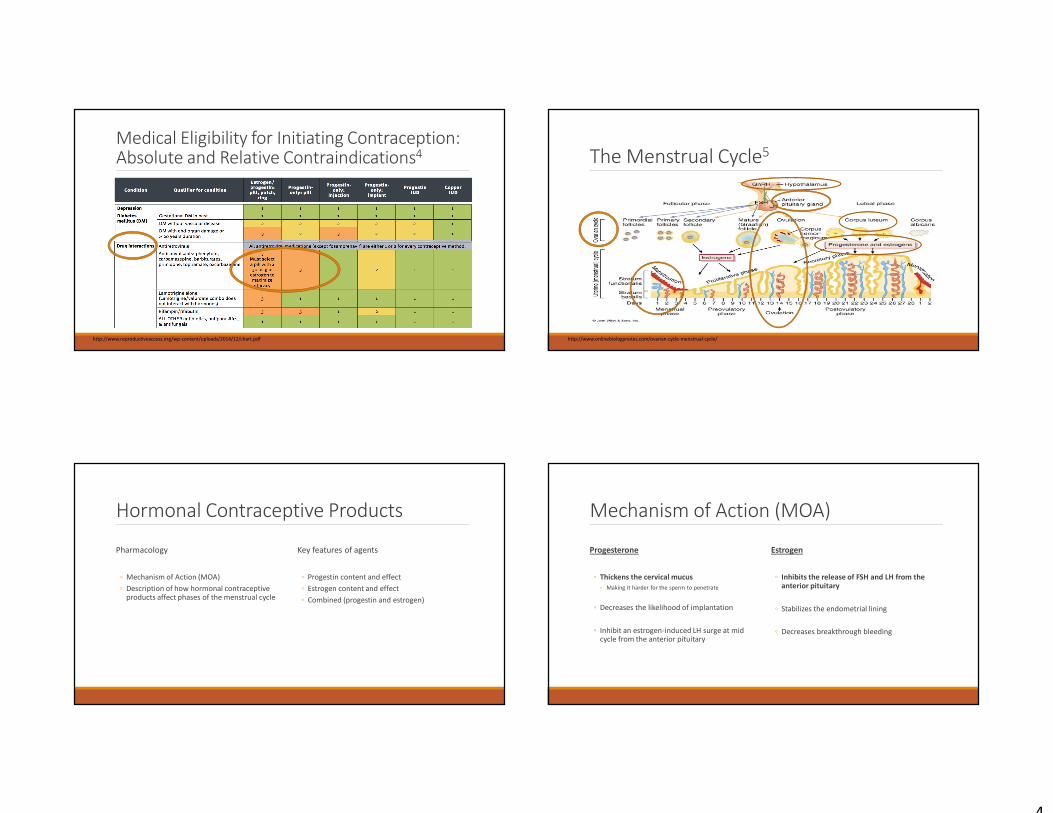
The Menstrual Cycle5
http://www.onlinebiologynotes.com/ovarian-cycle-menstrual-cycle/
Mechanism of Action (MOA)
Progesterone
◦ Thickens the cervical mucus
◦ Making it harder for the sperm to penetrate
◦ Decreases the likelihood of implantation
◦ Inhibit an estrogen-induced LH surge at mid cycle from the anterior pituitary
Estrogen
◦ Inhibits the release of FSH and LH from the anterior pituitary
◦ Stabilizes the endometrial lining
◦ Decreases breakthrough bleeding
5
Contraception Forms and their Efficacy5
https://www.cdc.gov/reproductivehealth/contraception/unintendedpregnancy/pdf/Contraceptive_methods_508.pdf
Hormonal Contraceptives
More Effective Methods Include:
Pills:
◦ Progestin only
◦ Combination (estrogen and progestin)
Least Effective Methods Include:
◦ Spermicides
◦ Condoms
◦ Withdrawal Method
Progestin Only Contraceptives
Prevent ovulation by inhibiting the release of LH and the LH surge from the pituitary
Also act on the female reproductive system in additional ways:
◦ Thicken cervical mucus
◦ Inhibit sperm penetration past the cervix, into the uterus, and fallopian tubes
◦ Inhibit implantation
◦ By promoting atrophy (thinning) of the endometrial lining
http://e.hormone.tulane.edu/lear
ning/progestins.html
Classification of Progestins6
https://www.medscape.org/viewarticle/559116_6
6
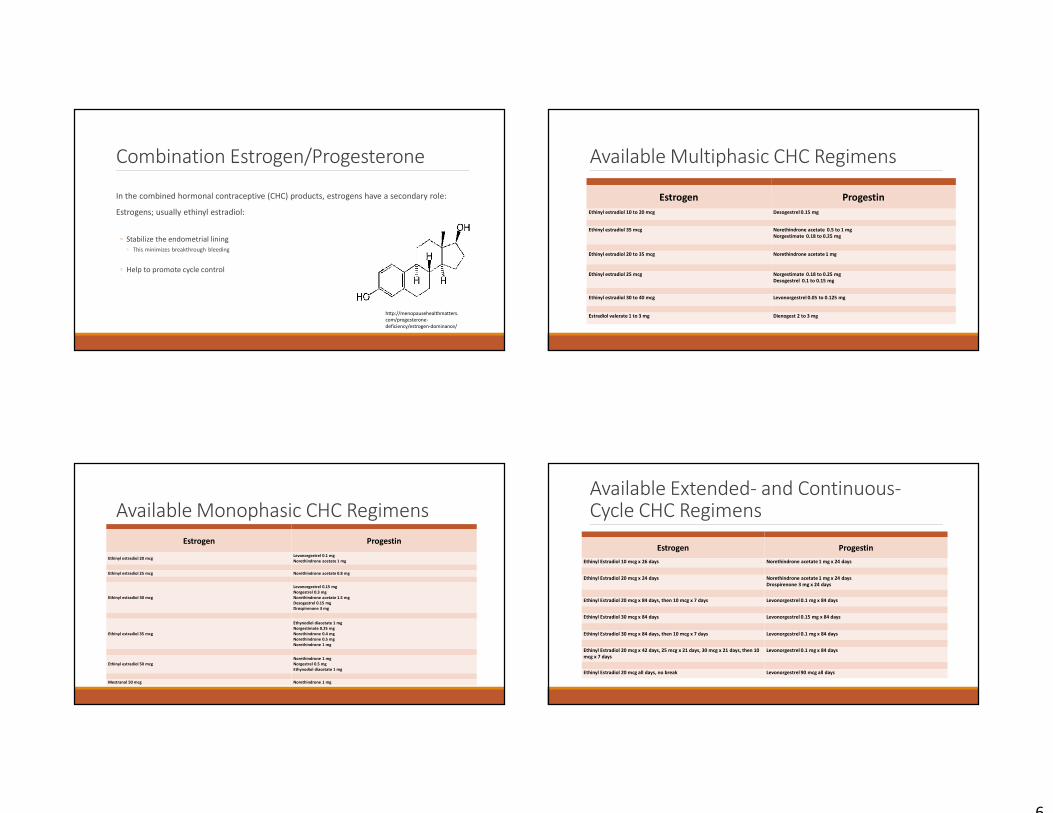
Combination Estrogen/Progesterone
In the combined hormonal contraceptive (CHC) products, estrogens have a secondary role:
Estrogens; usually ethinyl estradiol:
◦ Stabilize the endometrial lining
◦ This minimizes breakthrough bleeding
◦ Help to promote cycle control
http://menopausehealthmatters.
com/progesterone-
deficiency/estrogen-dominance/
Available Monophasic CHC Regimens
Estrogen Progestin
Ethinyl estradiol 20 mcgLevonorgestrel 0.1 mg
Norethindrone acetate 1 mg
Ethinyl estradiol 25 mcg Norethindrone acetate 0.8 mg
Ethinyl estradiol 30 mcg
Levonorgestrel 0.15 mg
Norgestrel 0.3 mg
Norethindrone acetate 1.5 mg
Desogestrel 0.15 mg
Drospirenone 3 mg
Ethinyl estradiol 35 mcg
Ethynodiol diacetate 1 mg
Norgestimate 0.25 mg
Norethindrone 0.4 mg
Norethindrone 0.5 mg
Norethindrone 1 mg
Ethinyl estradiol 50 mcg
Norethindrone 1 mg
Norgestrel 0.5 mg
Ethynodiol diacetate 1 mg
Mestranol 50 mcg Norethindrone 1 mg
Available Multiphasic CHC Regimens
Estrogen Progestin
Ethinyl estradiol 10 to 20 mcg Desogestrel 0.15 mg
Ethinyl estradiol 35 mcg Norethindrone acetate 0.5 to 1 mg
Norgestimate 0.18 to 0.25 mg
Ethinyl estradiol 20 to 35 mcg Norethindrone acetate 1 mg
Ethinyl estradiol 25 mcg Norgestimate 0.18 to 0.25 mg
Desogestrel 0.1 to 0.15 mg
Ethinyl estradiol 30 to 40 mcg Levonorgestrel 0.05 to 0.125 mg
Estradiol valerate 1 to 3 mg Dienogest 2 to 3 mg
Available Extended- and Continuous-Cycle CHC Regimens
Estrogen Progestin
Ethinyl Estradiol 10 mcg x 26 days Norethindrone acetate 1 mg x 24 days
Ethinyl Estradiol 20 mcg x 24 days Norethindrone acetate 1 mg x 24 days
Drospirenone 3 mg x 24 days
Ethinyl Estradiol 20 mcg x 84 days, then 10 mcg x 7 days Levonorgestrel 0.1 mg x 84 days
Ethinyl Estradiol 30 mcg x 84 days Levonorgestrel 0.15 mg x 84 days
Ethinyl Estradiol 30 mcg x 84 days, then 10 mcg x 7 days Levonorgestrel 0.1 mg x 84 days
Ethinyl Estradiol 20 mcg x 42 days, 25 mcg x 21 days, 30 mcg x 21 days, then 10
mcg x 7 days
Levonorgestrel 0.1 mg x 84 days
Ethinyl Estradiol 20 mcg all days, no break Levonorgestrel 90 mcg all days
7
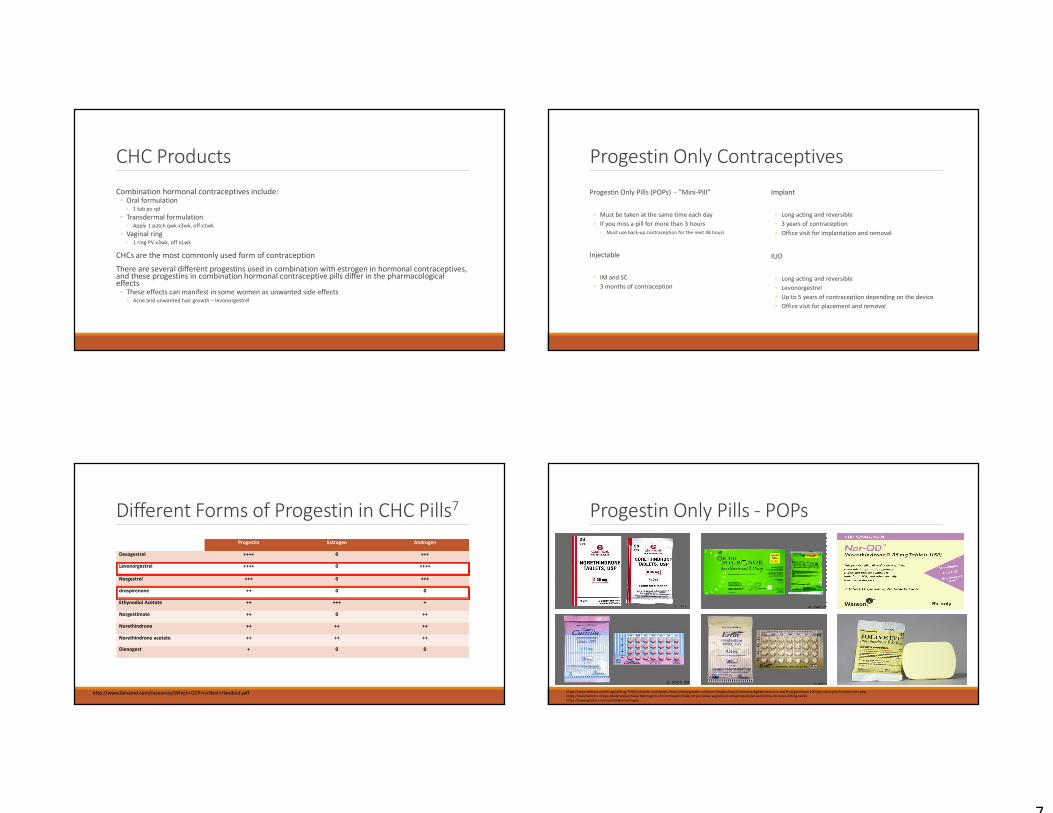
CHC Products
Combination hormonal contraceptives include:◦ Oral formulation
◦ 1 tab po qd
◦ Transdermal formulation ◦ Apply 1 patch qwk x3wk, off x1wk
◦ Vaginal ring◦ 1 ring PV x3wk, off x1wk
CHCs are the most commonly used form of contraception
There are several different progestins used in combination with estrogen in hormonal contraceptives, and these progestins in combination hormonal contraceptive pills differ in the pharmacological effects
◦ These effects can manifest in some women as unwanted side effects◦ Acne and unwanted hair growth – levonorgestrel
Different Forms of Progestin in CHC Pills7
http://www.fainamd.com/resources/Which+OCP+is+Best+Handout.pdf
Progestin Estrogen Androgen
Desogestrel ++++ 0 +++
Levonorgestrel ++++ 0 ++++
Norgestrel +++ 0 +++
drospirenone ++ 0 0
Ethynodiol Acetate ++ +++ +
Norgestimate ++ 0 ++
Norethindrone ++ ++ ++
Norethindrone acetate ++ ++ ++
Dienogest + 0 0
Progestin Only Contraceptives
Progestin Only Pills (POPs) - ”Mini-Pill”
◦ Must be taken at the same time each day
◦ If you miss a pill for more than 3 hours
◦ Must use back-up contraception for the next 48 hours
Injectable
◦ IM and SC
◦ 3 months of contraception
Implant
◦ Long acting and reversible
◦ 3 years of contraception
◦ Office visit for implantation and removal
IUD
◦ Long acting and reversible
◦ Levonorgestrel
◦ Up to 5 years of contraception depending on the device
◦ Office visit for placement and removal
Progestin Only Pills - POPs
https://www.webmd.com/drugs/2/drug-75915/jolivette-oral/details, https://www.goodrx.com/errin/images, http://contracts.digitaltreasure.co.bw/fr-ca/generique-100-mg-avana-prix-le-moins-cher.php,
https://dailymed.nlm.nih.gov/dailymed/archives/fdaDrugInfo.cfm?archiveid=15386, https://www.aegisshield.com/products/janssen/ortho-micronor-035mg-tablet
https://www.goodrx.com/norethindrone/images
8
Non-Contraceptive Benefits of Hormonal Contraceptives
Medicating the symptoms of dysmenorrhea
◦ Painful/difficult menses
Reducing the frequency and length of the menstrual cycle
Reducing menorrhagia
◦ Heavy menstrual bleeding
Reducing the rates of some cancers
◦ Ovarian
◦ Endometrial
Improving certain skin conditions
◦ Acne
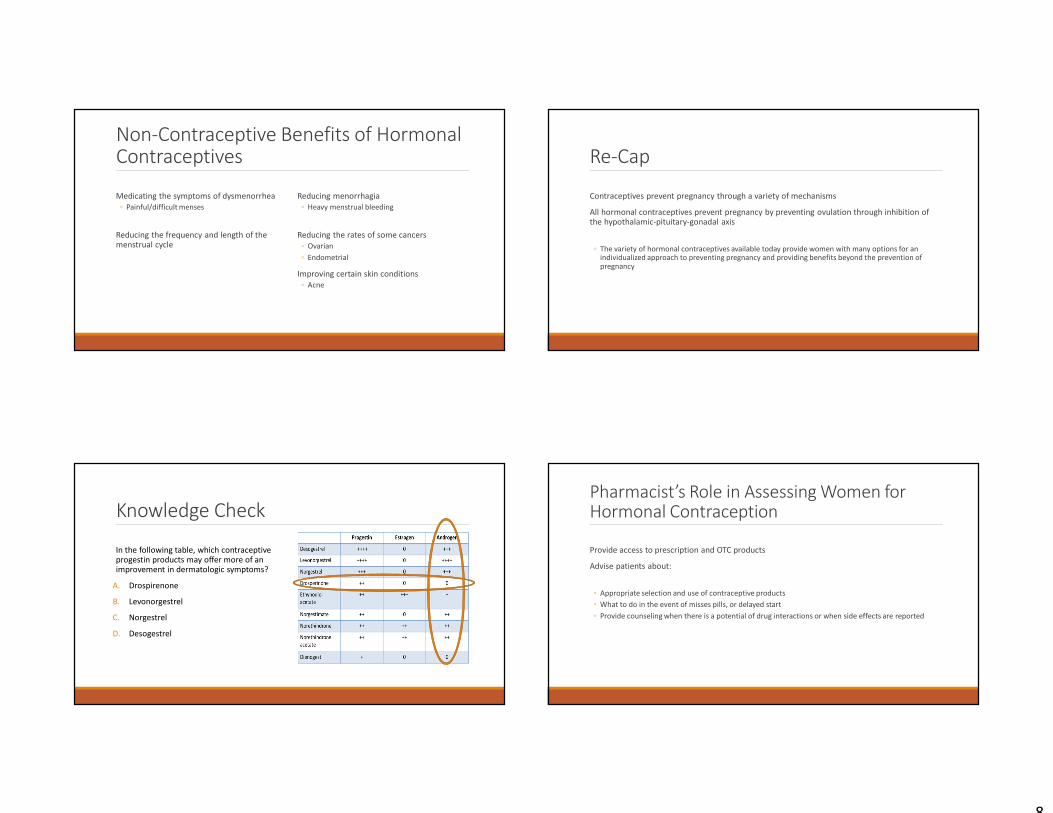
Knowledge Check
In the following table, which contraceptive progestin products may offer more of an improvement in dermatologic symptoms?
A. Drospirenone
B. Levonorgestrel
C. Norgestrel
D. Desogestrel
Re-Cap
Contraceptives prevent pregnancy through a variety of mechanisms
All hormonal contraceptives prevent pregnancy by preventing ovulation through inhibition of the hypothalamic-pituitary-gonadal axis
◦ The variety of hormonal contraceptives available today provide women with many options for an individualized approach to preventing pregnancy and providing benefits beyond the prevention of pregnancy
Pharmacist’s Role in Assessing Women for Hormonal Contraception
Provide access to prescription and OTC products
Advise patients about:
◦ Appropriate selection and use of contraceptive products
◦ What to do in the event of misses pills, or delayed start
◦ Provide counseling when there is a potential of drug interactions or when side effects are reported
9
Hormonal Contraception Self-Screening Tool Questions8
http://www.pharmacy.ca.gov/laws_regs/1746_1_pt.pdf
Pharmacy Practitioners Patient Care Process9
https://jcpp.net/patient-care-process/
Hormonal Contraceptive Indications
All Contraceptives All Contraceptives
Prevent pregnancy
Additional Benefits of Some Contraceptives Additional Benefits of Some Contraceptives
Dermatological Improvement
Treat symptoms of premenstrual dysphoric disorder (PMDD)
Menstrual Suppression
Off-label Uses Off-label Uses
Regulation of menstrual cycle
Risk reduction for certain cancers
PCOS management
Reduction of menstrual bleeding
Contraceptive Method Selection
SafetySafety EfficacyEfficacyPast
experiencePast
experienceEase of accessEase of access
ReversibilityReversibility ConvenienceConvenience AdherenceAdherencePersonal
preference Personal
preference
Cost Cost Privacy Privacy
10
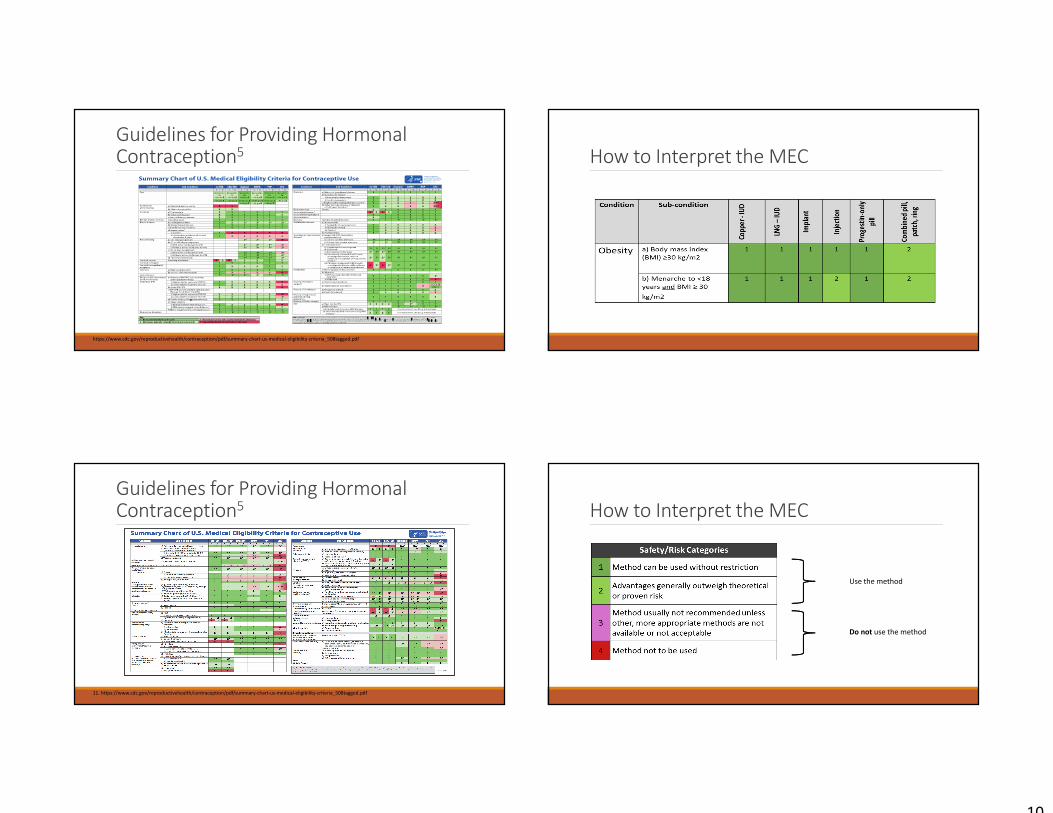
Guidelines for Providing Hormonal Contraception5
https://www.cdc.gov/reproductivehealth/contraception/pdf/summary-chart-us-medical-eligibility-criteria_508tagged.pdf
Guidelines for Providing Hormonal Contraception5
11. https://www.cdc.gov/reproductivehealth/contraception/pdf/summary-chart-us-medical-eligibility-criteria_508tagged.pdf
How to Interpret the MEC
How to Interpret the MEC
Use the method
Do not use the method
11
Guidelines for Providing Hormonal Contraception5
http://apps.who.int/iris/bitstream/10665/252267/1/9789241565400-eng.pdf
Contraception App By Centers For Disease Control and Prevention
https://itunes.apple.com/us/app/contraception/id595752188?mt=8
Assessment Procedure for Prescribing Hormonal Contraceptives
Selected Practice Recommendations for Examination and Tests Needed5
http://apps.who.int/iris/bitstream/10665/252267/1/9789241565400-eng.pdf
12
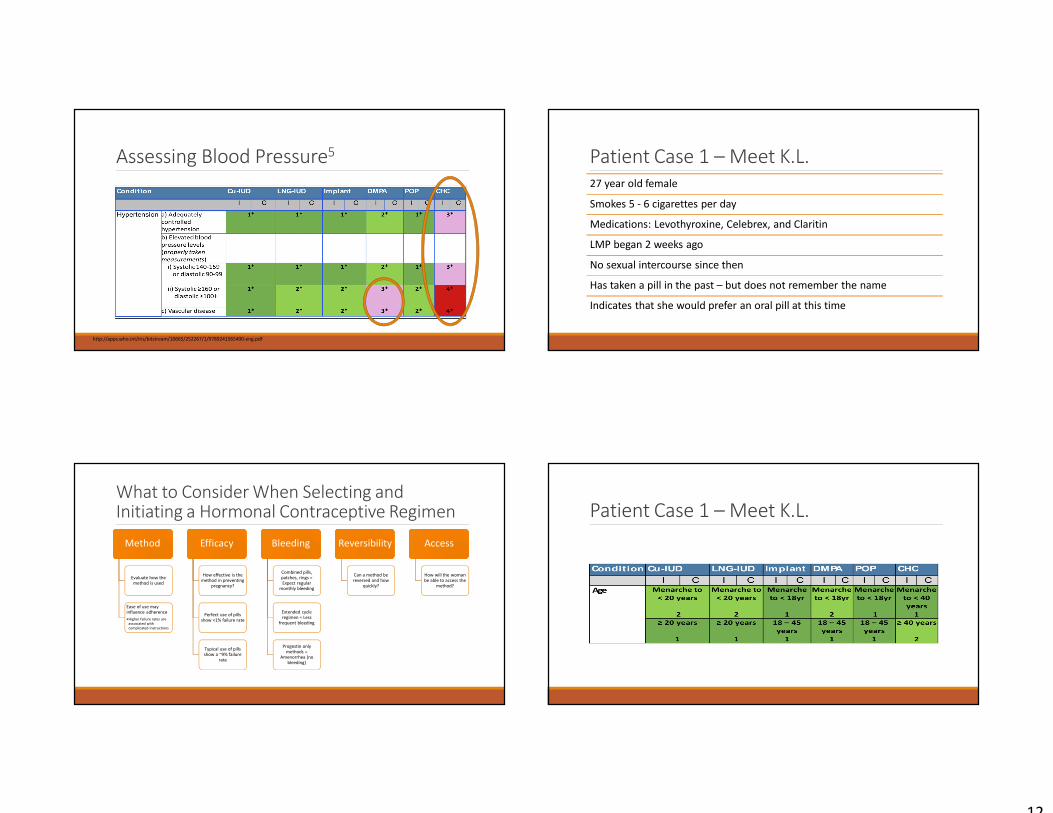
Assessing Blood Pressure5
http://apps.who.int/iris/bitstream/10665/252267/1/9789241565400-eng.pdf
What to Consider When Selecting and Initiating a Hormonal Contraceptive Regimen
MethodMethod
Evaluate how the method is used
Ease of use may influence adherence
•Higher failure rates are
associated with
complicated instructions
EfficacyEfficacy
How effective is the method in preventing
pregnancy?
Perfect use of pills show <1% failure rate
Typical use of pills show a ~9% failure
rate
BleedingBleeding
Combined pills, patches, rings = Expect regular
monthly bleeding
Extended cycle regimen = Less
frequent bleeding
Progestin only methods =
Amenorrhea (no bleeding)
ReversibilityReversibility
Can a method be reversed and how
quickly?
AccessAccess
How will the woman be able to access the
method?
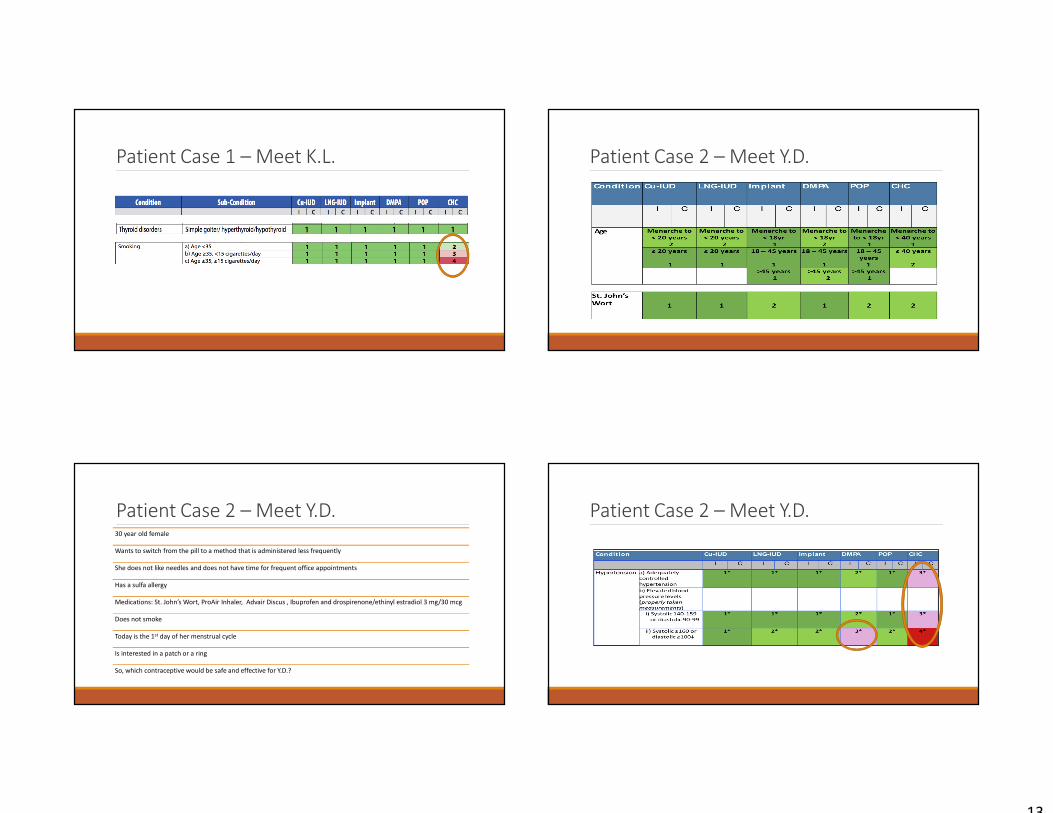
Patient Case 1 – Meet K.L.
27 year old female
Smokes 5 - 6 cigarettes per day
Medications: Levothyroxine, Celebrex, and Claritin
LMP began 2 weeks ago
No sexual intercourse since then
Has taken a pill in the past – but does not remember the name
Indicates that she would prefer an oral pill at this time
Patient Case 1 – Meet K.L.
13
Patient Case 1 – Meet K.L.
Patient Case 2 – Meet Y.D. 30 year old female
Wants to switch from the pill to a method that is administered less frequently
She does not like needles and does not have time for frequent office appointments
Has a sulfa allergy
Medications: St. John’s Wort, ProAir Inhaler, Advair Discus , Ibuprofen and drospirenone/ethinyl estradiol 3 mg/30 mcg
Does not smoke
Today is the 1st day of her menstrual cycle
Is interested in a patch or a ring
So, which contraceptive would be safe and effective for Y.D.?
Patient Case 2 – Meet Y.D.
Patient Case 2 – Meet Y.D.
14
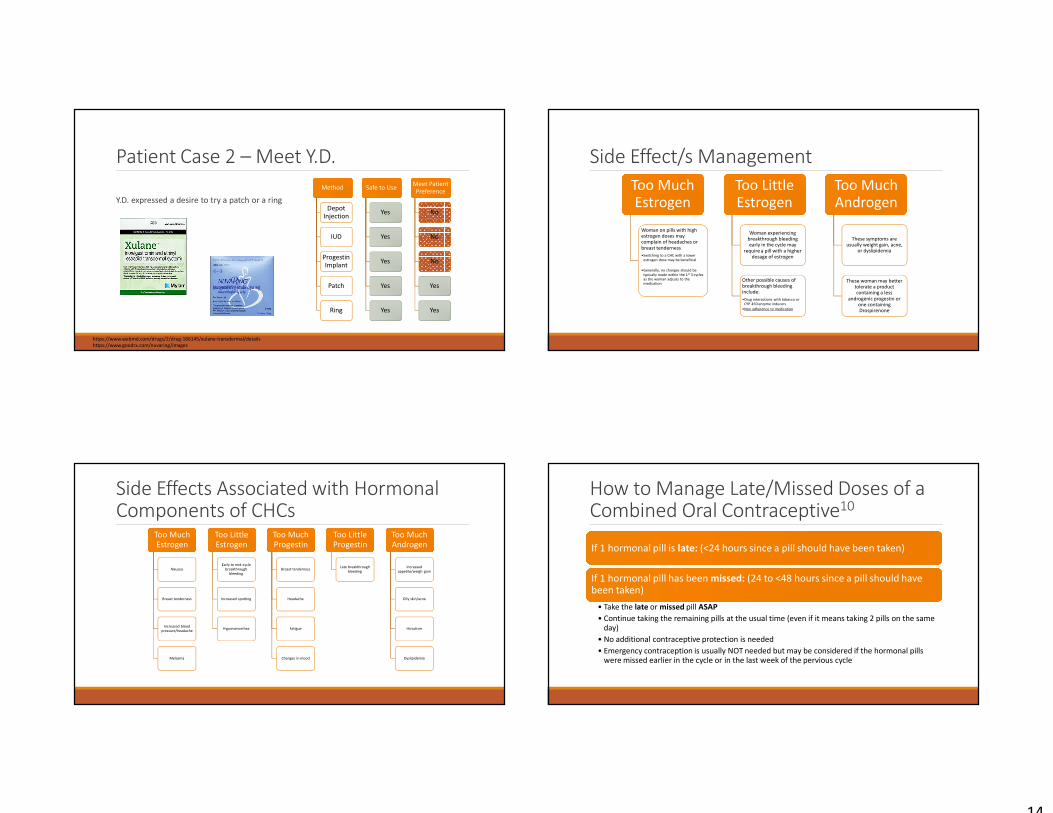
Patient Case 2 – Meet Y.D.
MethodMethod
Depot Injection
IUD
Progestin Implant
Patch
Ring
Safe to UseSafe to Use
Yes
Yes
Yes
Yes
Yes
Meet Patient
Preference
Meet Patient
Preference
No
No
No
Yes
Yes
Y.D. expressed a desire to try a patch or a ring
https://www.webmd.com/drugs/2/drug-166145/xulane-transdermal/details
https://www.goodrx.com/nuvaring/images
Side Effects Associated with Hormonal Components of CHCs
Too Much Estrogen
Too Much Estrogen
Nausea
Breast tenderness
Increased blood
pressure/headache
Melasma
Too Little EstrogenToo Little Estrogen
Early to mid-cycle
breakthrough
bleeding
Increased spotting
Hypomenorrhea
Too Much Progestin Too Much Progestin
Breast tenderness
Headache
Fatigue
Changes in mood
Too Little ProgestinToo Little Progestin
Late breakthrough
bleeding
Too Much AndrogenToo Much Androgen
Increased
appetite/weigh gain
Oily skin/acne
Hirsutism
Dyslipidemia
Side Effect/s Management
Too Much Estrogen
Too Much Estrogen
Woman on pills with high estrogen doses may complain of headaches or breast tenderness
•Switching to a CHC with a lower
estrogen dose may be beneficial
•Generally, no changes should be
typically made within the 1st 3 cycles
as the woman adjusts to the medication
Too Little EstrogenToo Little Estrogen
Woman experiencing breakthrough bleeding early in the cycle may
require a pill with a higher dosage of estrogen
Other possible causes of breakthrough bleeding include:
•Drug interactions with tobacco or
CYP 450 enzyme inducers
•Non adherence to medication
Too Much AndrogenToo Much Androgen
These symptoms are usually weight gain, acne,
or dyslipidemia
These woman may better tolerate a product containing a less
androgenic progestin or one containing Drospirenone
How to Manage Late/Missed Doses of a Combined Oral Contraceptive10
If 1 hormonal pill is late: (<24 hours since a pill should have been taken)If 1 hormonal pill is late: (<24 hours since a pill should have been taken)
If 1 hormonal pill has been missed: (24 to <48 hours since a pill should have been taken)If 1 hormonal pill has been missed: (24 to <48 hours since a pill should have been taken)
• Take the late or missed pill ASAP
• Continue taking the remaining pills at the usual time (even if it means taking 2 pills on the same day)
• No additional contraceptive protection is needed
• Emergency contraception is usually NOT needed but may be considered if the hormonal pills were missed earlier in the cycle or in the last week of the pervious cycle
15
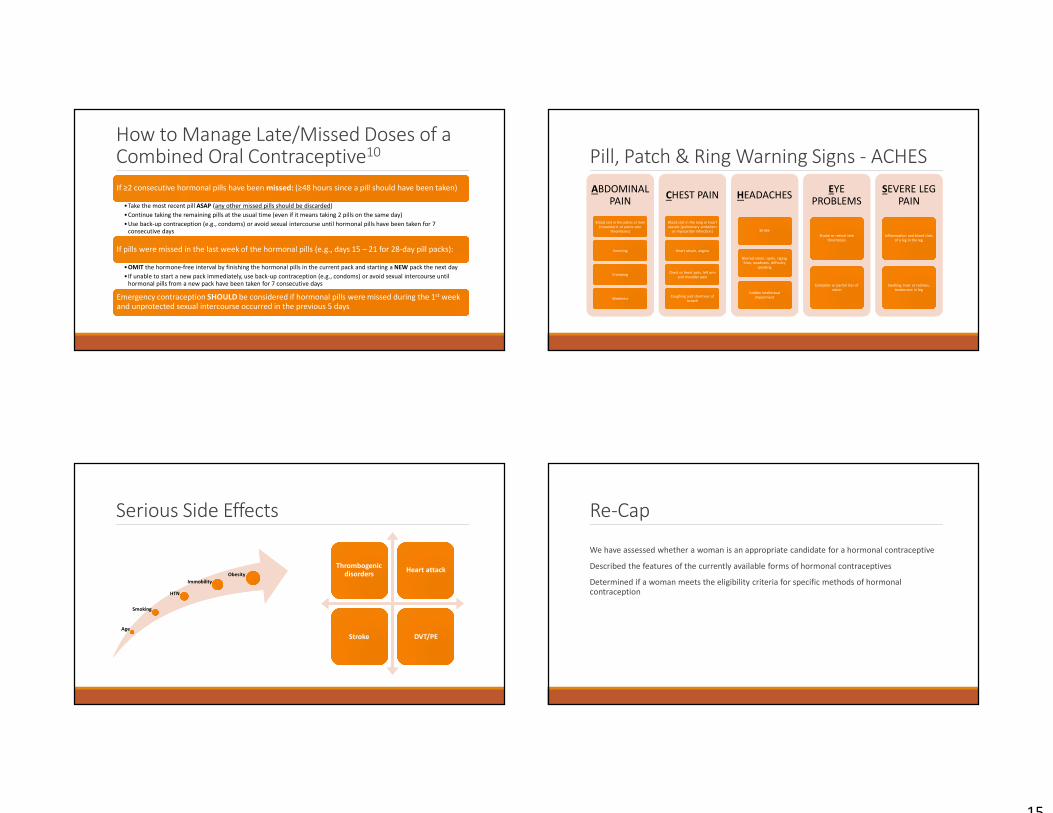
How to Manage Late/Missed Doses of a Combined Oral Contraceptive10
If ≥2 consecutive hormonal pills have been missed: (≥48 hours since a pill should have been taken)If ≥2 consecutive hormonal pills have been missed: (≥48 hours since a pill should have been taken)
•Take the most recent pill ASAP (any other missed pills should be discarded)
•Continue taking the remaining pills at the usual time (even if it means taking 2 pills on the same day)
•Use back-up contraception (e.g., condoms) or avoid sexual intercourse until hormonal pills have been taken for 7 consecutive days
If pills were missed in the last week of the hormonal pills (e.g., days 15 – 21 for 28-day pill packs):If pills were missed in the last week of the hormonal pills (e.g., days 15 – 21 for 28-day pill packs):
•OMIT the hormone-free interval by finishing the hormonal pills in the current pack and starting a NEW pack the next day
•If unable to start a new pack immediately, use back-up contraception (e.g., condoms) or avoid sexual intercourse until hormonal pills from a new pack have been taken for 7 consecutive days
Emergency contraception SHOULD be considered if hormonal pills were missed during the 1st week and unprotected sexual intercourse occurred in the previous 5 daysEmergency contraception SHOULD be considered if hormonal pills were missed during the 1st week and unprotected sexual intercourse occurred in the previous 5 days
Serious Side Effects
Thrombogenicdisorders
Thrombogenicdisorders
Heart attackHeart attack
StrokeStroke DVT/PEDVT/PEAge
Smoking
HTN
Immobility
Obesity
Pill, Patch & Ring Warning Signs - ACHES
ABDOMINAL PAIN
ABDOMINAL PAIN
Blood clot in the pelvis or liver
[mesenteric or pelvic vein
thrombosis]
Blood clot in the pelvis or liver
[mesenteric or pelvic vein
thrombosis]
VomitingVomiting
CrampingCramping
WeaknessWeakness
CHEST PAINCHEST PAIN
Blood clot in the lung or heart
vessels [pulmonary embolism
or myocardial infarction]
Blood clot in the lung or heart
vessels [pulmonary embolism
or myocardial infarction]
Heart attack, anginaHeart attack, angina
Chest or heart pain, left arm
and shoulder pain
Chest or heart pain, left arm
and shoulder pain
Coughing and shortness of
breath
Coughing and shortness of
breath
HEADACHESHEADACHES
StrokeStroke
Blurred vision, spots, zigzag
lines, weakness, difficulty
speaking
Blurred vision, spots, zigzag
lines, weakness, difficulty
speaking
Sudden intellectual
impairment
Sudden intellectual
impairment
EYE PROBLEMS
EYE PROBLEMS
Stroke or retinal vein
thrombosis
Stroke or retinal vein
thrombosis
Complete or partial loss of
vision
Complete or partial loss of
vision
SEVERE LEG PAIN
SEVERE LEG PAIN
Inflammation and blood clots
of a leg in the leg
Inflammation and blood clots
of a leg in the leg
Swelling, heat or redness,
tenderness in leg
Swelling, heat or redness,
tenderness in leg
Re-Cap
We have assessed whether a woman is an appropriate candidate for a hormonal contraceptive
Described the features of the currently available forms of hormonal contraceptives
Determined if a woman meets the eligibility criteria for specific methods of hormonal contraception
16
Questions/Contact Info:
Daniel Majerczyk, Pharm.D.Assistant Professor of Clinical SciencesRoosevelt University, College of Pharmacy1400 N. Roosevelt Blvd. | Schaumburg, IL 60173
Email: [email protected]
References: 1. Hatcher R. Contraceptive technology. 20th ed. New York: Ardent Media; 2011.
2. Finer LB, Henshaw SK. Disparities in rates of unintended pregnancy in the United States, 1994 and 2001; Perspect Sex Reprod Health. 2006,38:90-96.
3. World Health Organization. Medical eligibility criteria for contraceptive use. 5th ed. 2015. http://www.who.int (last accessed 12 November 2017).
4. Reproductiveaccess. Reproductiveaccess Online Web Site. Available at: https://www.reproductiveaccess.org/resource/medical-eligibility-initiating-contraception/. Accessed November 12, 2017.
5. World Health Organization. Medical eligibility criteria for contraceptive use. 5th ed. 2015. http://www.who.int (last accessed 12 November 2017).
6. Stewart FH, Harper CC, Ellertson CE, et al. Clinical breast and pelvic examination requirements for hormonal contraception: Current practice vs evidence. JAMA. 2001;285:2232-2239.
7. Centers for Disease Control and Prevention (CDC). Update to CDC's US medical eligibility criteria for contraceptive use, 2010: revised recommendations for the use of hormonal contraception among women at high risk for HIV infection or infected with HIV. MMWR Morb Mortal Wkly Rep. 2012;61:449-452.
8. Landry DJ, Wei J, Frost JJ. Public and private providers' involvement in improving their patients' contraceptive use. Contraception. 2008;78:42-51.
9. Cipolle RJ, Strand LM, Morley PC. Pharmaceutical Care Practice: The Patient Centered Approach to Medication Management, 3rd ed. New York: McGraw-Hill; 2012.
10. White KO, Westhoff C. The effect of pack supply on oral contraceptive pill continuation: a randomized controlled trial. Obstet Gynecol. 2011;118:615-622.