choosing the right medical treatment and recent advances
DESCRIPTION
CHOOSING THE RIGHT MEDICAL TREATMENT AND RECENT ADVANCES. NEELIMA THAKUR, MD. Epilepsy Burden. The lifetime likelihood of Experiencing at least 1 seizure is ~ 9%. Receiving a diagnosis of epilepsy is ~ 3%. Approximately 200,000 new cases of seizures and epilepsy occur each year. - PowerPoint PPT PresentationTRANSCRIPT

CHOOSING THE RIGHT MEDICAL TREATMENT AND
RECENT ADVANCES
NEELIMA THAKUR, MD.

Epilepsy Burden
• The lifetime likelihood of – Experiencing at least 1 seizure is ~ 9%. – Receiving a diagnosis of epilepsy is ~3%.
• Approximately 200,000 new cases of seizures and epilepsy occur each year.
• Epilepsy and seizures affect nearly 3 million Americans of all ages, at an estimated annual cost of $17.6 billion in direct and indirect costs.

Seizures are defined as abnormal discharge of electrical activity from brain neurons resulting in transient loss of motor, sensory or mental function.

• Provoked seizures• Acute symptomatic.
• Often a reversible cause.
•By definition, these are not epilepsy.
• Unprovoked seizures• 2 unprovoked seizures 24hrs apart is considered
epilepsy.
Seizure types

First unprovoked seizure – risk of seizure recurrence.
• 24-74 % in first 5 years.– Normal EEG and imaging studies – 24%– Abnormal EEG and imaging studies- 74%
• After 2nd unprovoked seizure – 80%
First unprovoked seizure
• Risk factors for seizure recurrence – Family history- Abnormal EEG - Abnormal neuroimaging.- Seizure in sleep.
First unprovoked seizure
• 50 % seizures recur in the first year• 80% with in two years.
First unprovoked seizure
• Current Guidelines
– No antiepileptic drugs (AEDs) if • There are no other risk factors • Normal EEG.

Anti epileptic Drugs
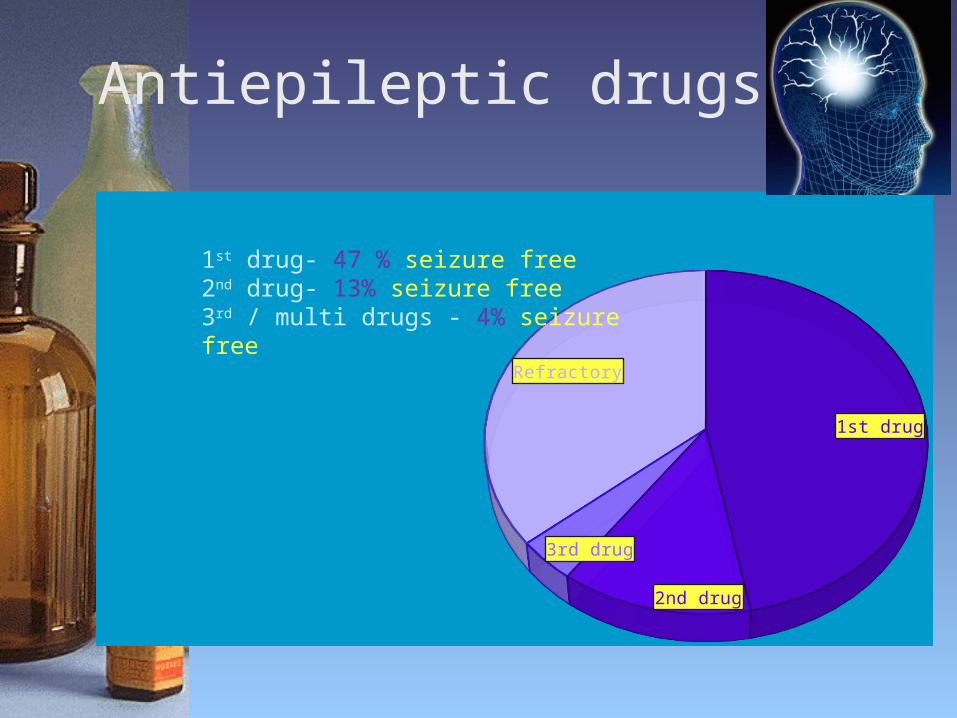
Antiepileptic drugs
1st drug
2nd drug
3rd drug
Refractory
1st drug- 47 % seizure free2nd drug- 13% seizure free3rd / multi drugs - 4% seizure free
Epilepsy outcome at >7 years.
• Seizure free >7years - 59 %• Seizure free >1 year and relapses- 16 %
Which AED to choose?
Anti epileptic Drugs
• 1850 : Bromides• 1910: Phenobarbital• 1940: Phenytoin• 1950: Ethosuximide• 1958: ACTH• 1954: Primidone• 1968: Carbamazepine• 1975: Clonazepam• 1978: Depakote

1990s: Newer AEDs were developed.
• lamotrigine (Lamictal) • felbamate (Felbatol) • levetiracetam (Keppra)• topiramate (Topamax)• oxcarbazepine (Trileptal)• zonisamide (Zonegran)• pregabalin (Lyrica)• lacosamide (Vimpat)• rufinamide (Banzel)• vigabatrin (Sabril)• clobazam (Onfi)• ezogabine (Potiga)• perampanel (Fycompa)• eslicarbazepine (Aptiom)
• Good efficacy,• Fewer toxic effects, • Better tolerability

Following criteria may be helpful
– Type of epilepsy– Comorbidities– Side effect profile– Pharmacokinetics– Drug-drug interactions– Single dose-Compliance– Women– Elderly

Type of epilepsy• Primarily generalized epilepsies.
– ethosuximide ( Absence seizures)– valproate– topiramate– zonisamide– lamotrigine– levetiracetam– rufinamaide– clobazam– vigabatrin.

Primarily generalized epilepsies
• Avoid carbamazepine, gabapentin, Phenytoin.

Efficacy Primarily generalized epilepsy
• Absence seizures – ethosuximide, valproate are effective than
lamotrigine.
• Atonic seizures : clobazam.• Primarily generalized epilepsies:
valproate>topamax and leviteracetam.

Type of epilepsy
• Partial EpilepsiesAll AEDs except ethosuximide.
Efficacy-Partial seizures
• Not possible to compare efficacy as there are no major head to head trials.
• The study population, inclusion and exclusion criteria are different. ‘
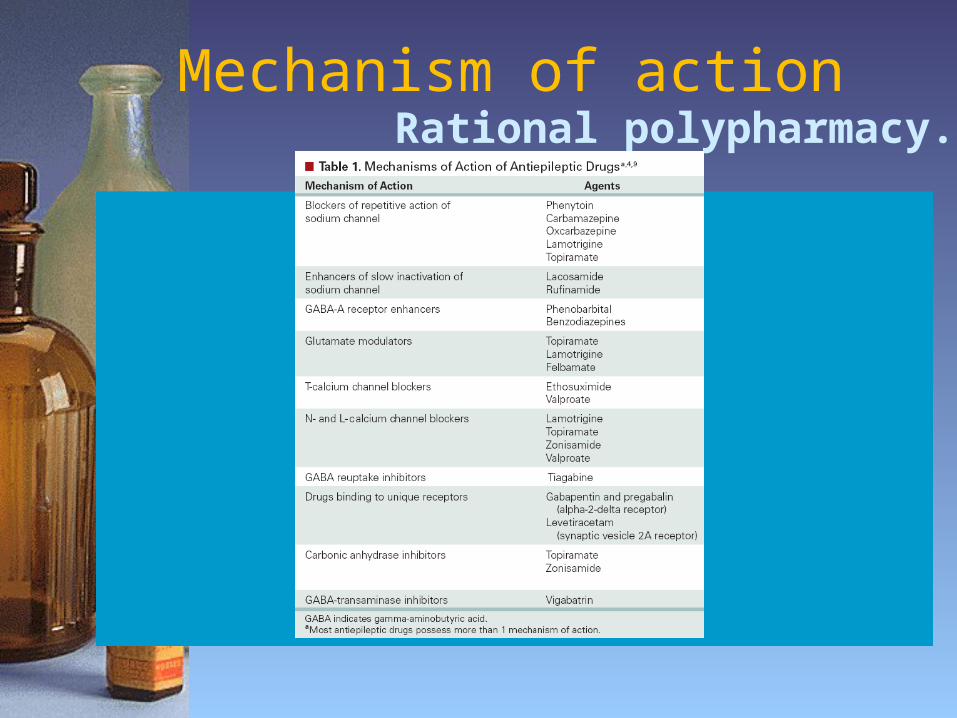
Mechanism of action Rational polypharmacy.

Comorbidities
• Bipolar disorder/depression/anxiety: valproate, lamotrigine, carbamazepine, oxcarbazepine.
• Migraines: valproate, topiramate, zonisamide.
• Obesity: topiramate, zonisamide
• Neuropathy:
gabapentin, lyrica, carbamazepine, oxcarbazepine.
ComorbiditiesAEDs to avoid
• Psychiatric/behavorial problems: levetiracetam.
• Osteoporosis: phenobarbital, phenytoin, valproate, carbamazepine.
• Renal stones : topamax, zonegran.
• Obesity: valproate, pregabalin, gabapentin.
• Diabetes: valproate.

Liver dysfunction
Drugs of choice• leviteracetam• lacosamide• pregabalin• gabapentin
Renal dysfunction
Decrease drug doses that are cleared primarily by kidneys
– levetiracetam– lacosamide– pregabalin– gabapentin
Hemodialysis
Risk of drug removal is high for non protein bound drugs
Doses need to be adjusted accordingly.
• High risk levetiracetam
lacosamide
phenobarbital
topiramate.
• Low risk phenytoin
valproate
lamotrigine.
carbamazepine

Drug interactions
Liver enzyme(CYP 450 & UGT) inducersphenytoin, phenobarbital, carbamazepine, oxcarbazepine,
topiramate, felbamate, rufinamide.• Liver enzyme inhibitors
– valproate, felbamate.

Single daily dose
Improves Patient compliance.
XR formulations may have lesser side effects.
• Q day AEDs Phenytoin, Phenobarbital and zonegran.
• XR formulation
Depakote ER, Lamictal XR, Keppra XR, Oxtellar XR and Trokendi XR.

Epilepsy in Elderly
• The prevalence and incidence of epilepsy are highest in later life!!
• Approximately 7% of seniors have epilepsy.
• 25% of new cases occur in elderly

AEDs : Elderly
• Older people with a first unprovoked seizure are more likely to develop recurring seizures than are younger adults.
• Starting AEDs after a single unprovoked seizure may be appropriate in some cases.

AEDs: Elderly

AEDs - Elderly
TREAT CAUTIOUSLY!
– Elderly are more susceptible to the adverse effects of drugs than their younger patients.
– Pharmacokinetics and pharmacodynamics of AEDs differ in old age .
– Drug-drug interactions

AEDs- Elderly Treatment Challenges• Comorbidities complicate the treatment options.
• Polypharmacy make them susceptible to drug interactions.
• Adherence may not be as good in elderly patients with epilepsy.
AEDs - Elderly
• Pharmacokinetic– Albumin results in free fraction phenytoin,
carbamazepine and valproate.– Drug metabolism is affected by decreased liver
enzymes.– Drug excretion is affected by decreased renal
clearance.
AEDs - Elderly
• In general the preferred drugs are– levetiracetam– lamotrigine– gabapentin

AEDs-Pregnancy
Concerns– Effect of AEDs on Fetus and infant during
• Pregnancy• Breast feeding.
– AED pharmacokinetics affecting levels during• Pregnancy• Postpartum

AEDs - Pregnancy
Teratogenic risks mono vs polytherapy.
• Single AED 3.1 %• Two AEDs 5.8 %• Three AEDs 8.3%
AEDs - Pregnancy
• Major malformations with monotherapy– valproate 9.3%– phenobarbital 5.5 %– topiramate 4.2 %– carbamazepine 3%– phenytoin 2.9%– levetiracetam 2.4%– lamotrigine 2.0%

AEDs - Pregnancy
• Pharmacokineticslamotrigine & levetiracetam
clearance during pregnancy
level up to 50% of baseline.• Postpartum-
clearance returns to baseline and drug levels.
• Check monthly levels and adjust dose.
AEDs - Pregnancy
In general, levetiracetam, lamotrigine, oxcarbazepine and carbamazepine are considered relatively safe.
Newer AEDs
• Ezogabine (Potiga)• Perampanel (Fycompa)• Eslicarbazepine (Aptiom)

Ezogabine (Potiga)2011
• Mechanism of action: Potassium Channel
• Approved for add on treatment for Partial epilepsy.
• It is the first neuronal potassium channel opener developed for the treatment of epilepsy .
Ezogabine (Potiga)
• Mechanism of action: Potassium Channel
• Approved as add on treatment for Partial epilepsy
.• First neuronal potassium channel opener
developed for the treatment of epilepsy .

Ezogabine (Potiga)
Absorption and Metabolism:– Well absorbed. Food has no influence.– Not known whether excreted in human milk. – Metabolized in liver.
– Dosage adjustment is required in patients with moderate and greater renal or hepatic impairment .
– *urine bilirubin can show falsely elevated readings
Ezogabine (Potiga)
• Drug interactions– Carbamazepine, phenytoin may Potiga levels. – Potiga has no effect on other AED levels. – POTIGA may digoxin serum concentrations. – Alcohol systemic exposure to POTIGA

Ezogabine (Potiga)
Adverse reactionsFDA warning blue skin discoloration and eye abnormalities characterized by pigment changes in the retina
Initial and periodic eye exams are recommended.
– Urinary retention– Neuropsychiatric symptoms- confusion, psychosis– QT interval prolongation

Perampanel (Fycompa)2012
• Mechanism of action: AMPA glutamate receptor noncompetitive antagonist.
• Approved as add on treatment for Partial epilepsy.

Perampanel (Fycompa)
• Absorption and Metabolism:– Well absorbed. Food has no influence.– Not known whether excreted in human milk. – Metabolized in liver. Dosage adjustment is required in patients
with moderate and greater renal or hepatic impairment .

Perampanel(Fycompa)
Drug interactions– Does not effect other AEDs.– Enzyme inducers perampanel levels.

Perampanel (Fycompa)
• Adverse reactions– Neuro-psychiatric symptoms ( black box
warning for aggression and hostility).– Dizziness , Somnolence fatigue, blurred vision.– Pregnancy category C
Eslicarbazepine (Aptiom)2013
• Mechanism of action: Na channel blocker. the prodrug metabolizes to eslicarbazepine..
• Approved as add on treatment for Partial epilepsy.
Eslicarbazepine (Aptiom)
• Absorption and Metabolism:– Well absorbed. Food has no influence.– Metabolized in liver and kidneys.
• Drug interactions and Side effectsSimilar but more tolerable than oxcarbazepine