chronic disease and population health management
TRANSCRIPT

Smart Technologies inChronic Disease &
Population Health ManagementThe case for outcome-based
approaches to better healthcare
© 2016 Napier Healthcare. All Rights Reserved.
1

Smart Health Technology IntegrationBetter Chronic Disease Management and Patient Experience
© 2014 Napier Healthcare. All Rights Reserved.
2
3
© 2016 Napier Healthcare. All Rights Reserved.
Our research shows the following to be true:- Chronic Disease Management (CDM) requires holistic case management.
Remote monitoring of vital signs is achievable today.
Longer term care plans for chronic diseases will vastly improve quality of care.
With sufficient data, analytics will further drive successful health outcomes.
Mostly with elderly and increasingly with younger patients, we have to personalise the experience when they visit the facility. For instance, we should
Consider an easier Registration process or NO PROCESS at all
Use voice based GPS and WhatsApp
Chronic Disease Management and Patient ExperienceWhat is to be Done?

The 2015 report by DesignSingapore Council, Design for Ageing Gracefully–Rethinking Health & Wellness for the Elderly: Public Services, tells us that seniors:
Are very comfortable using WhatsApp, Viber and Skype, for long distance calls and to exchange photos etc. Those in the higher-income bracket (HDB 3 and above) tend to use tablets and smartphones.
Can we use WhatsApp to design a user experience for when they visit the hospital? Of course, use bigger fonts in the messaging interface, always.
Don’t like tech-enabled check-ins or SMS-based check-ins—it is too impersonal.
Prefer familiar faces in the Care team. They don’t want to meet new people at every visit.
Want “recreation” facilities in hospitals, if possible. Going to a hospital makes them feel “unsafe” and usually denotes trouble.
What can we do to make them safe? Why not have Wellness integrated instead of only sick care? Feel under represented in healthcare delivery.
Can we hire the elderly to take care of the elderly?
Watch a lot of TV.
Can that be used as a medium of interaction?
So what can we do?
Patient ExperienceA Call for Empathetic Technology
© 2014 Napier Healthcare. All Rights Reserved.
4

Enhancing Patient ExperienceEmpathetic Tech-based Options Available
© 2014 Napier Healthcare. All Rights Reserved.
5
Technologies provide for the THREE keys to better patient experience:Communication, Access to Information, Doctor/ Patient Relationship
Radio Frequency Identification (RFID) tagso Combined with location aware beaconso Tracks the location of patients moving through the systemo Alerts hospital staff of patients’ arrival/presenceo Automatically sets environmental controls based on patient preferences
Wearable technology to increase physicians’ face time with patientso Sends AV feeds from patient consultationo Scribe accesses the EHR remotely and enters patient noteso Patient notes are reviewed and signed off by the doctor
Mobile apps, kiosks, portals etc.
Analytics to find at-risk populationo Helps people manage their health conditions at home—long before they reach an acute stageo Reduces readmission rateso Uses: remote monitoring devices connected via Bluetooth, a Cloud, digital chart displays

Population HealthA Holistic Approach to Chronic Disease Management
© 2014 Napier Healthcare. All Rights Reserved.
6

Population HealthThe Health Outcomes of People in a Community
© 2016 Napier Healthcare. All Rights Reserved.
7
Population Health Management (PHM)
What is it?
Goals Why is it needed?
Benefits
Set of interventions designed to maintain/improve health of population across the full continuum of care.
Covers low-risk healthy individuals to high-risk individuals with one or more chronic conditions.
Population: Better coordinated care
Physicians: Better informed and engaged with patients
Health Care Organizations: Improved clinical outcomes and reduced costs
Health Care System: Increased preventive care and closed care gaps
Address burden of undiagnosed chronic illness that later present as acute condition
Address higher costs on the system due to chronic illness
Improve health of patient population
Redefine healthcare as a set of interdependent activities
Mitigate risk factors that exacerbate illnessSource: International Diabetes Foundation
(www.idf.org/membership/wp/ Singapore)

Singapore Health TodayAgeing Population and Rising Incidence of Chronic Diseases
8
© 2016 Napier Healthcare. All Rights Reserved.
Disease Prevalence (18-69 years) - 2010
Hypertension 23.5%
Diabetes 11.3%
High Total Cholesterol 17.4%
Obesity 10.8%
Daily Smoking 14.3%
Sources: Department of Statistics; Ministry of Health, Singapore; AIA Vitality Age Survey 2012, Ministry of Health Disease Burden
By 2030, the number of elderly citizens (aged 65 and above) will be 900,000.
Leading causes of death: major non-communicable diseases such as cancer, coronary heart diseases, strokes, pneumonia, diabetes and hypertension.
Common risk factors: smoking, obesity, physical inactivity and alcohol consumption.

Moving Forward with Accountable CareThe Future of Healthcare Delivery is Outcome-Focused
© 2014 Napier Healthcare. All Rights Reserved.
9

The Accountable Care ModelBased on Accountable Care*, Focused on Outcomes
10
© 2016 Napier Healthcare. All Rights Reserved.
Accountable Care/ Affiliated Care Network
Affiliated Care Network between general physicians and hospitals (enabled by a referral system between GP’s and hospitals)
Remote patient monitoring solutions aid in preventive approach to care (both for chronic diseases and ageing population)
The focus is on management of chronic diseases for people in a community.
1
2
1
1
1
1
2
* Accountable Care ties provider reimbursements to quality metrics and reductions in the total cost of care for an assigned population of patients, and is an increasingly important, Federally sponsored initiative in the USA.

Napier Healthcare is Ready to DeliverHigh-Value and Cost-Effective PHM on the National Scale
© 2014 Napier Healthcare. All Rights Reserved.
11

The Napier Advantage Enhancing healthcare delivery with an outcome-based model
12
© 2016 Napier Healthcare. All Rights Reserved.
Chronic Disease Management – Population Health Management
National Electronic Health Record (NEHR)
Care Coordination
Care Plan&
Vital Signs Monitoring
Portal
Analytics
Case Management
such as Pega or CRM currently in
use
+
To take this concept to fruition, we must work with government agencies:IDA, MOH and the Smart Nation Program Office.
Existing / Maybe
New Solutions
Transitions of Care
& Referral Management

© 2016 Napier Healthcare. All Rights Reserved.
13
APPENDIX
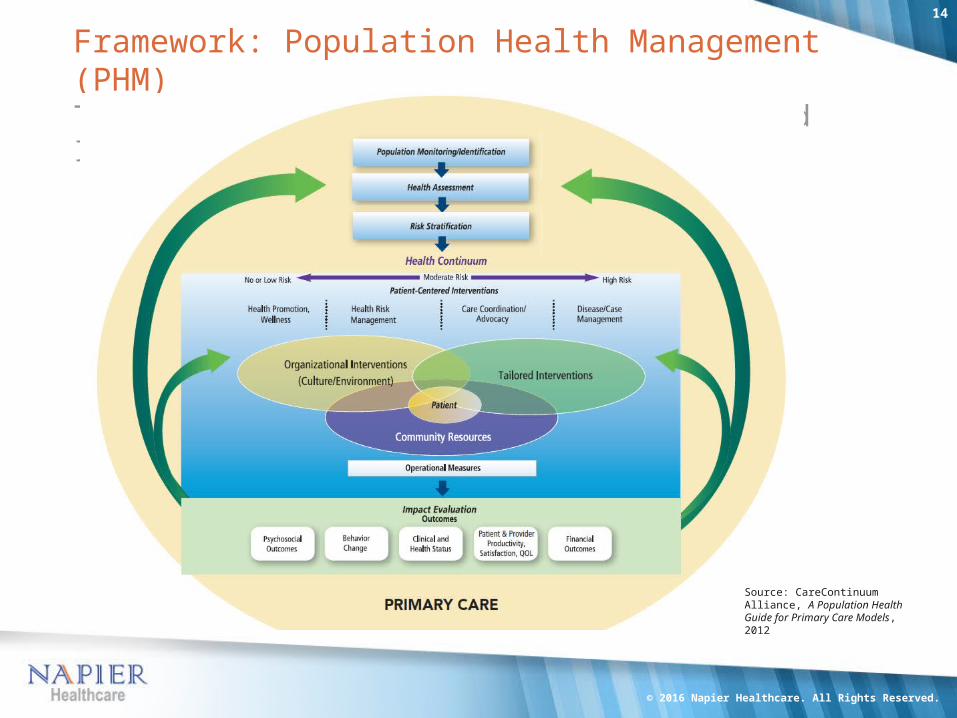
Framework: Population Health Management (PHM)The Continuum of Care and Patient-Centered Interventions
© 2016 Napier Healthcare. All Rights Reserved.
14
Source: CareContinuum Alliance, A Population Health Guide for Primary Care Models, 2012

The PHM WorkflowSteps in the Provision Model
© 2016 Napier Healthcare. All Rights Reserved.
15
Stratify, Design & Monitor Population
Identify Gaps in Care
Stratify Risks
Engage Patients
Managed Care
Measure Outcomes
PHM Workflow Chronic Disease Management
Identify the disease profile (e.g., Diabetes) along with the target population based on demographics and risk factors
Health assessment: Map the risk factors and the gaps in care at all levels—preventive, primary and above
Identify and stratify the population based on the level of risk involved (gaps in care, demographic, social etc.)
Community outreach and patient engagement programs
Technology enabled chronic disease management program to reduce the gaps—referral program, health promotion, risk management etc.
Remote patient monitoring to measure the outcomes of the program

PHM: Key ComponentsFoundation for Comprehensive Care and Management of Costs
© 2016 Napier Healthcare. All Rights Reserved.
16
1. PhysiciansProvide care consistent with PHM goals
2. Primary Care Physicians/General PractitionersThis group enables scalability for larger populations
3. Data AnalysisData is aggregated from EMRs, ePrescriptions, Practice Managers, Payers, HIEs and Labs to be analyzed for actionable outcomes
4. Benefit Program CoordinationFinancial incentives to be offered for participation in PHM
5. TechnologyEnables information to be pushed to patients
6. Referral MechanismEases the path along the continuum of care between primary and tertiary levels
7. Physician IncentivesEnsures involvement at PCP level
8. Replication AbilityApplied to community at large

Analytics in PHMLaying the Path to Actionable Insights
© 2016 Napier Healthcare. All Rights Reserved.
17
Source of Data Action Items
Electronic Medical Records
Electronic Prescriptions
Practice Manager Data
Payers Information
Hospital Information Exchanges
Laboratories
Data Analysis
Deliver Preventive Care
Treat Chronic Diseases
Perform Patient Outreach
Assess risk and Analyze cost
Report Outcomes and close care gaps
Clinical data (Biometric, Lab & HRA data)
Utilization data (How do people access/ use healthcare?)
Adherence data (Care plans, Medication plans & Preventive care)
Operational data (Participation, productivity, disability data and other metrics)
Financial data (How does healthcare activity translate into dollars (savings)?)
Satisfaction data (How participants/ stakeholders view your efforts?)
Top Areas for Data Analysis
Source: Health Intelligence Network, Napier Analysis

Technology Adoption in HealthcareThe Factors Influencing IT Investments
© 2016 Napier Healthcare. All Rights Reserved.
18
Source: Technology in the NHS—Transforming the Patient’s Experience of Care
THANK YOU
w w w . n a p i e r h e a l t h c a r e . c o mi n f o @ n a p i e r h e a l t h c a r e . c o m
19
© 2016 Napier Healthcare. All Rights Reserved.