chronic hepatitis
TRANSCRIPT

Presenter Dr Vamshi A
Guide : Dr V A Kothiwale
Co Guide : Dr Rajeev Malipatil
CHRONIC HEPATITIS

Content
INTRODUCTION AND DEFINITION
CLASSIFICATION
CAUSES

Introduction
• Chronic hepatitis represents a series of liver disorders of varying causes and severity in which hepatic inflammation and necrosis continue for at least 6 months.
• Milder forms are nonprogressive or only slowly progressive, while more severe forms may be associated with scarring and architectural reorganization, which, when advanced, lead ultimately to cirrhosis.



Classification
Cause Grade Stage

By Cause

By Grade
Histologic Activity Index(HAI)
HAI Score

By Stage

Different types of chronic hepatitis Hepatitis B Hepatitis C NAFLD ALCOHOLIC HEPATITIS AUTOIMMUNE HEPATITIS RARE CAUSES- GENETIC & DRUGS

Hepatitis B

Slide 4
1. WHO. Hepatitis B. 2002. 2. Custer B, et al. J Clin Gastroenterol. 2004;38(10 suppl):S158. 3. WHO/WPRO data.
HBsAg Prevalence (%)1
High Intermediate < Low
Country HBsAg+ (%)
China 5.3-122
South Korea 2.6-5.12
India 2.4-4.72
Taiwan 10-13.82
Vietnam 5.7-102
Japan 4.4-133
Africa 5-192
Russia 1.4-82
US/Europe 0.3-122
Geographic Distribution of Chronic HBV Infection

Hepatitis B significance of serological markers
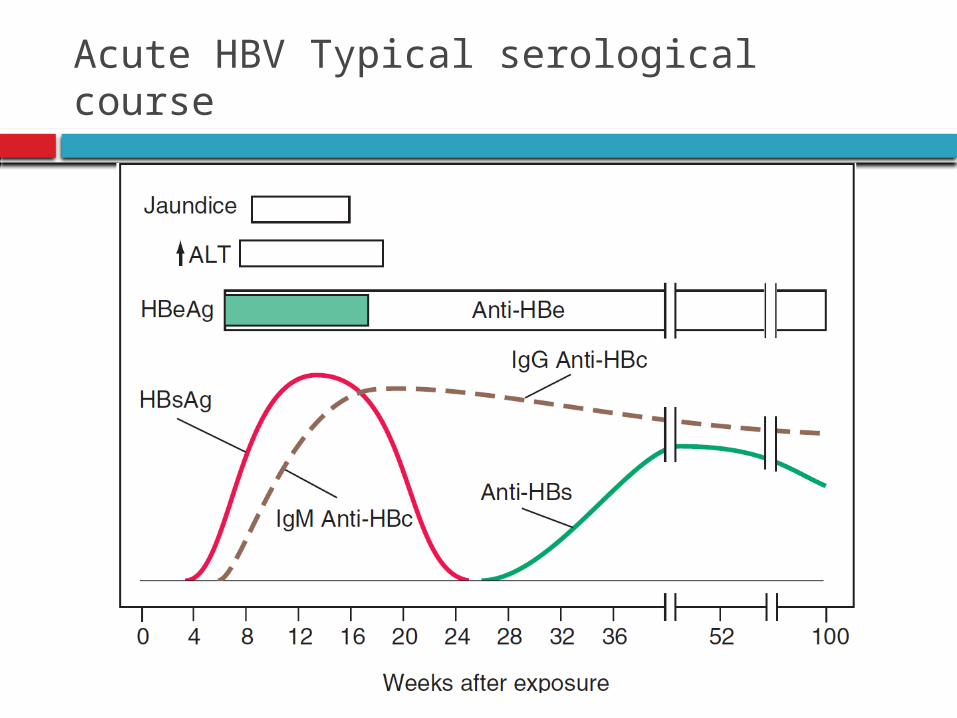
Acute HBV Typical serological course

IgM anti-HBc
Total anti-HBc
HBsAg
Acute(6 months)
HBeAg
Chronic(Years)
anti-HBe
0 4 8 12 16 20 24 28 32 36 52 Years
Weeks after Exposure
Titre
Progression to Chronic Hepatitis B Virus Infection Typical Serologic Course

Clinical course of HBVAcute hepatitis B infection
Chronic HBV infection
3-5% of adult-acquired infections
95% of infant-acquired infections
Cirrhosis
Chronic hepatitis
12-25% in 5 years
Liver failure Hepatocellular carcinoma
6-15% in 5 years 20-23% in 5 years

Phases of chronic hepatitis B

Diagnosis of Hepatitis B Virus (HBV) Infection
Chronic HBV
HBsAg
HBeAg
IgM anti-HBc
IgG anti HBc
Anti HBs
Anti Hbe
HBV DNA
Interpretation
Infection
+ + - + - - +++ HBeAG+ chronic hepatitis
+ - - + - + + Inactive carrier state
+ - - + - + ++ HBeAg- chronic hepatitis
+ + + + - + ++ Exacerbations of chronic hepatitis

Diagnostic criteria for chronic HBV1. HBsAg+ >6 m
2. Serum HBV DNA >10 IU/mL (may be lower for HBeAg negative patients)
3. Persistent or intermittent elevation in ALT/AST levels
4. Liver biopsy showing chronic hepatitis (necroinflammatory score ≥4)
5

Slide 12
When to treat HBV?
HBeAg Positive
Treat
Monitor ALT Q3mos for 1y
HBeAg Negative
HBV DNA >20,000 IU/mL HBV DNA >2,000 IU/mL
Normal ALT
Consider Liver Biopsy If >40yrs
Significant fibrosis or inflammation
Elevated ALT
ALT Level

Treatment
Main goal of treatment of chronic Hep B is to prevent cirrohosis , hepatic failure and HCC.

Treatment Options
7 drugs have been approved to date Injectable Interferon (INF) α, Pegylated Interferon(PEG), Lamivudine, Adefovir, Entecavir, Telbivudine, Tenofovir.

INTERFERONS
Antiviral, antiproliferative and immunomodulatory effects.
IFN-α and -β bind to the same receptor and have predominantly antiviral effects.
IFN-γ binds to a separate receptor and has more marked immunoregulatory action but less potent antiviral effects.
Pegylation reduces rate of absorption,renal clearance, decreases immunogenecity and increases half life.

The recommended dose is 180 μg weekly for 48 weeks.
pegIFN-α2a monotherapy was superior to lamivudine monotherapy in inducing HBeAg seroconversion.
a/e include initial flu like illness, fever, chills, headache, malaise, myalgia, emotional liability.
The strongest predictor of response in HBeAg+ patients is pretreatment ALT level. other being histologic activity, low HBV DNA level.

LAMIVUDINE
Nucleoside analogue. Effective in suppressing HBV replication. Recommended dose for adults with normal renal
function (creatinine clearance >50 mL/min) and no HIV infection is 100 mg daily PO

Adefovir Dipivoxil
• Inhibit reverse transcriptase• Effective in lamivudine-resistant HBV• 10 mg daily PO

Entecavir: orally administered cyclopentyl guanosine analog.
Emtricitabine
Tenofovir
Telbivudine (sebivo)

Definition of Response to Antiviral Therapy of Chronic Hepatitis B

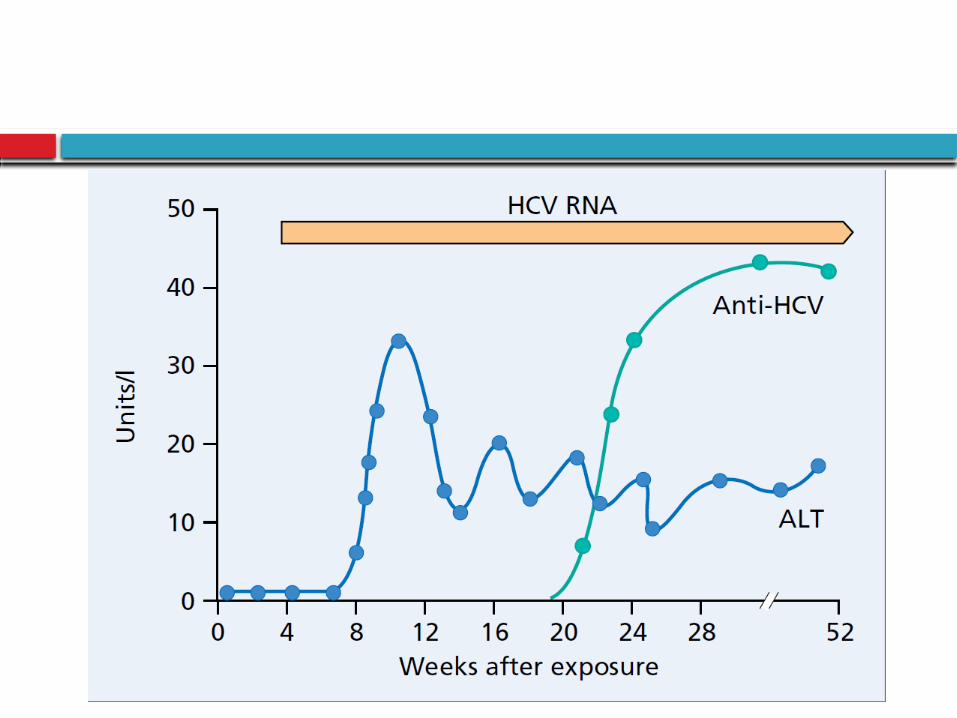
Chronic Hepatitis C
Overview: Prevalence: 170 million worldwide New cases/yr: ~3-4 million worldwide Progression to cirrhosis occurs in about 20−25%
followed for 20yrs Leading cause of chronic liver disease,
cirrhosis, HCC.

Clinical Presentation
Most patients with chronic hepatitis have asymptomatic elevations of serum aminotransferase levels and do not have physical signs of liver disease.
6% have symptomatic liver disease. Fatigue is the most common symptom. Dull right upper quadrant pain. Less common-
anorexia,nausea,pruritis,arthralgia,myalgia

Risk factors

Natural history

Treatment
Viral eradication
Prevention of disease progression
Sustained loss of HCV RNA in serum (3-6 mos post-Tx)
Normalization of liver enzymes
Improved liver histology Improved quality of life
Goals Endpoints

Treatment options


Non Alcoholic Fatty Liver Disease(NAFLD)
NAFLD was first described in the 1950s when fatty liver was characterized in a group of obese patients.
In 1980, Ludwig and colleagues at the Mayo Clinic described 20 obese, diabetic, nonalcoholic patients who had similar findings on liver biopsy to patients with alcoholic liver disease, and the term nonalcoholic steatohepatitis was introduced


Signs and symptoms
Asymptomatic in majority of cases
Fatigue
Right upper quardant pain or discomfort
Hepatomegaly (50%)
Obesity
Hypertension

Diagnosis NAFLD is a diagnosis of exclusion
-Alcoholic Hepatitis
-Drug induced Hepatitis (tamoxifen, amiodarone)
-Viral Hepatitis
-Autoimmune Hepatitis
-Metabolic (Wilson and Hemochromatosis)

The most challenging DDX is alcoholic hepatitis
The histologic picture of both conditions is similar
Consumption of alcohol less than 10 g/d in women and 20 g/d in men

Imaging
Ultrasonography- helps in detecting the fatty infiltration of the liver
and helps in determining the size of the liver.

Liver biospy
Gold standard for both diagnosis and prognosis Shows characteristic macrovascular steostosis with
occasional vesicular fat.

Algorithm for Management of NASH

Alcoholic hepatitis
The threshold for developing alcoholic liver disease in men is an intake of >60–80 g/d of alcohol for 10 years, while women are at increased risk for developing similar degrees of liver injury by consuming 20–40 g/d.
Ingestion of 160 g/d is associated with a 25-fold increased risk of developing alcoholic cirrhosis.
Only 10 – 15 % of alcoholics develop cirrohosis.

How is Alcoholic hepatitis diagnosed?
History of recent excessive alcohol ingestion Serum bilirubin more than 80mmol/l ALT <300 IU (or AST<500 IU) Exclusion of autoimmune, chronic viral or
malignant liver disease

Characteristic features of alcoholic hepatitis (but not necessary for diagnosis)
Pyrexia, Hepatomegaly, A hepatic bruit, Ascites, Encephalopathy, AST: ALT ratio greater than 1.5, Peripheral leucocytosis.

Prognosis
Discriminant score:
4.6 x(PTtest – Ptcontrol)+S.bilirubin(mg/dl)
American College of Gastroenterology defines severity as a modified Discriminant Function (mDF)> 32


Autoimmune Hepatitis(AIH)
AIH represents a chronic, mainly periportal hepatitis with lymphocytic infiltrates, plasma cells, and piecemeal necrosis.
Etiology is unclear. Female predominance, hypergammaglobulinemia,
circulating autoantibodies, and a good response to immunosuppressive treatment.

Exclusion of other chronic diseases Viral hepatitis (HBV and HCV) Alcoholic liver disease and NAFLD Drug-induced hepatotoxicity Wilson disease Hereditary hemochromatosis Alpha-1-antitrypsin deficiency Primary biliary cirrhosis Primary sclerosing cholangitis

Severe disease (untreated) 40% die within 6 months of diagnosis 40% of survivors develop cirrhosis 54% of cirrhotics develop varices within 2 years of
diagnosis of cirrhosis 20% of patients with varices will bleed

Clinical features Type 1 Type 2 Type 3
Diagnostic autoantibodies
ASMA
ANA
Antiactin
Anti LKM
PD 450,IID6
Synthetic core motif peptides 254-271
SLP
Cytokeratins 8 & 18
Age 10 y-elderly Pediatric (2-14 y)Rare in adults
Adults (30-50 y)
Women (%) 78 89 90
Concurrent immune disease (%)
41 34 58
Gamma globulin elevation
+++ + ++
Low IgA No occasional No
HLA association
Steroid response
Progression of response
B8, DR3, DR4
+++
48
B14, Dr3, C4AQO
++
82
Uncertain
+++
75

Goals of Treatment
Induce remission
Prevent disease progression
Minimize relapse of disease
Improve survival
Minimize medication side effects

Indications for treatment
Absolute Relative
Serum AST 10-fold or more greater than the upper limit of normal
Symptoms (eg, fatigue, arthralgia, jaundice)
Serum AST 5-fold or more greater than the upper limit of normal and gamma-globulin level 2-fold or more greater than normal
Serum AST and/or gamma-globulin less than absolute criteria
Bridging necrosis or multiacinar necrosis on
histologic examination
Interface hepatitis

Treatment Options

THANK YOU

Slide 7
Natural history of HBV