chronic pain: supporting safer prescribing of analgesics · opioid analgesics, figure 1 provides a...
TRANSCRIPT

British Medical Associationbma.org.uk
Chronic pain: supporting safer
prescribing of analgesics
March 2017
1British Medical Association Chronic pain: supporting safer prescribing of analgesics
Contents
1 Background ............................................................................................................................................................2
2 Introduction ...........................................................................................................................................................32.1 Definingchronicpain ................................................................................................................................32.2 Prevalenceofchronicpain .....................................................................................................................32.3 Analgesic drugs ...........................................................................................................................................4
3 Analgesicuseforchronicpain .......................................................................................................................53.1 Analgesicprescribingforchronicpain:UKtrends...................................................................... 53.2 Analgesicuseinchronicpain–exploringtheevidence ...........................................................73.3 Potentialharmsassociatedwithlong-termanalgesicuseinchronicpain ...................11
4 Supportingthemanagementofpatientswithchronicpain ........................................................14
5 Roleoftrainingandeducationinimprovinganalgesicusefortreatingchronicpain .......205.1 A focus on undergraduate training .................................................................................................205.2 Promotingguidancetosupportimprovedanalgesicprescribingforchronicpain ...21
6 Conclusionandsummaryofrecommendations ................................................................................ 22
7 Furtherresources ............................................................................................................................................. 24
Appendix1–classificationofchronicpain .................................................................................................... 25
Appendix2–specialisttraininginpainmedicine ...................................................................................... 26
Acknowledgements ................................................................................................................................................. 27
References .................................................................................................................................................................... 28
Abbreviations
ACMD AdvisoryCouncilontheMisuseofDrugs BMA BritishMedicalAssociationBPS BritishPainSocietyCDC Centers for Disease Control and PreventionCQC CareQualityCommissionEPM EssentialPainManagement FPM FacultyofPainMedicineIASP InternationalAssociationfortheStudyofPain ICD InternationalClassificationofDiseasesNHS NationalHealthServiceNICE NationalInstituteforHealthandCareExcellenceNSAID Nonsteroidalanti-inflammatorydrugPHE PublicHealthEnglandRCGP RoyalCollegeofGeneralPractitioners RCOA RoyalCollegeofAnaesthetistsSIGN ScottishIntercollegiateGuidelinesNetworkSNRI Serotonin–norepinephrinereuptakeinhibitorSSRI SelectiveserotoninreuptakeinhibitorTCA TricyclicantidepressantWHO WorldHealthOrganization
ThispublicationwaspreparedundertheauspicesoftheBMAboardofscience.ApprovalforpublicationwasrecommendedbyBMAcouncilon24March2017.
WearegratefultotheFacultyofPainMedicineoftheRoyalCollegeofAnaesthetistsfortheirguidanceinproducingthisdocument.AfulllistofcontributorscanbefoundintheAcknowledgementssectionattheendofthisdocument.

2 British Medical Association Chronic pain: supporting safer prescribing of analgesics
1 Background
Themanagementofpatientswithchronicpaincanpresentsignificantchallenges,1 and thesubstantialpublichealthharmsinrelationtoprescriptionanalgesicsseenintheUnitedStatesandelsewherehaspromptedrenewedeffortstoassesstheroleofmedicinesinpainmanagement.TheBMA’s2016analysisreportonPrescribed drugs associated with dependence and withdrawal,notestheincreaseinanalgesicprescribingforthispatientgroup2andaddstothecurrentconversationaboutwhetherprescribinganalgesicsisalwaysinthepatient’sbestinterestsgiventhat,foropioidsinparticular,thereislimitedevidenceforefficacyintreatinglong-termpain.2,3Thisrepresentsapotentiallysignificantpublichealthissue,andourmembershavecalledfortheexplorationoffactorsthatcouldsupportthesaferprescribingofopioidanalgesics.Suchanapproachwouldensurethatpatientsareonlyprescribedmedicinesfromwhichtheyderivebenefitandwilllimitmedicationassociatedharms.Thisisimportantgiventhecostofopioidprescribing,whichinEnglandisestimatedtototalover£300million,andinScotlandtoover£32million,annually.4,5
Thisbriefingpaperhighlightssomeofthekeyissuessurroundingtheuseofanalgesicsinthemanagementofpatientswithchronicpain;settingoutarangeofrecommendationsforgovernments,policymakersandhealthcareprofessionals,withtheaimofsupportingthesaferprescribingofthesemedicines.Whilstitprovidesanintroductiontothecurrentstateoftheevidenceinthisarea,itisnotintendedtoprovideasystematicreviewoftheevidenceoractasaclinicalguide.Acomprehensiveresourcetosupporttheclinicaluseofopioids–Opioids Aware–hasrecentlybeendeveloped(seeSection 3).
IssuessurroundingtheappropriateuseofanalgesicsareofwiderelevancetoBMAmembersacrossdifferentbranchesofpractice.ThisbriefingfollowsaBMAboardofscienceseminarinSeptember2014,initiatedbyBaronessIloraFinlay(BMApresident2014-15),whichexploredproblemsfacingclinicianswhenprescribingopioidsinpalliativecareandforchronicpain.

3British Medical Association Chronic pain: supporting safer prescribing of analgesics
2 Introduction
Paincanbedefinedasanunpleasantsensoryandemotionalexperienceassociatedwithactualorpotentialtissuedamage.6Thecomplexityandprevalenceofpainmakeitamajorclinicalandsocialchallenge.Accordingtothe2015globalburdenofdiseasestudy,chronicpainconditionsareamongstthemostsignificantcausesofsufferinganddisabilityworldwide.7 Pain canoftenco-occurwithemotionalandmentalhealthdifficulties.Paincanbeassociatedwithanxietyanddepressionandmentalhealthdiagnosesandemotionaldifficultiescaninfluencetheexperienceofpainandcomplicatemanagement.Anestimated49%ofpatientsintheUKsufferingfromchronicpainalsosufferfromdepression.8Datafromthe2011HealthSurveyforEnglandindicatethat,aswellasdepression,chronicpainisassociatedwithamultitudeofnegativehealthandsocialoutcomes,includingpoorermentalwellbeing,anxiety,job/incomeloss,impairedfunctionandlimiteddailyphysicalandsocialactivities.9
2.1 Definingchronicpain
TheIASP(InternationalAssociationfortheStudyofPain)defineschronicpainaspainthathaspersistedbeyondnormaltissuehealingtime.Itcanbecontinuousorinterruptedbypain-freeintervals.10Intheabsenceofothercriteria,chronicpainisusuallytakentobepainthathaspersistedforthreemonths.Althoughthistemporaldefinitionmaybemoreusefulforresearchratherthanclinicalpurposes,theBPS(BritishPainSociety)andtheSIGN(ScottishIntercollegiateGuidelinesNetwork)usethethree-monthdefinitionasthebasisfortheirrecommendationsonthetreatmentofchronicpain.11,12
Painhasbeenhistoricallysubdividedaccordingtothepresumednatureofthetissueinjury.Theremaybeanumberofunderlyingmechanismsincludingsomatictissueinjury,damagetonervesandpainfromviscera.Thesecategoriesoftenoverlap.Thereisoftennotanidentifiablecurrentinjury,butpainmayrelatetopreviousinjuryordiseaseorabnormalsensoryprocessing.Theperceivedintensityofpaindoesnotnecessarilyrelatetothedegreeoftissueinjuryandisinfluencedbymanyfactorsincludingthepatient’sunderstandingofandconcernsaboutthepain,anxiety,distress,expectationsandpreviousexperienceofpain. 13,14,15,16 Thereisalsonowincreasingunderstandingofthelongtermhealthimpactofearlyadverseexperiences,andtheassociationbetweenemotionaltrauma,post-traumaticstressdisorderandpainhasbeenwelldescribed.17,18
Therearemultipleclassificationsofchronicpain,andAppendix 1providesanoverviewofthosethathavebeendevelopedbytheIASPforinclusioninthe11threvisionoftheWHO(WorldHealthOrganization)InternationalClassificationofDiseases.
2.2 Prevalence of chronic pain
Ithasbeenestimatedthataround20%ofadultsinEurope,andthat13%ofadultsintheUKexperiencechronicpain,thoughthisvariesdependingonthecriteriaanddefinitionsused.19,20
Ameta-analysisofpopulationstudiesestimatedthatchronicpainaffectsbetweenonethirdandonehalfoftheUKpopulation,andthatbetween10.4%and14.3%ofthepopulationoftheUKreportseverelydisablingchronicpainthatiseither‘moderately’or‘severely’limiting.21 TheNationalPainAuditestimatedthat11%ofadultsand8%ofchildrenintheUKsufferfromseverepain.20Inthe2011HealthSurveyforEngland31%ofmenand37%ofwomenoverallreportedtohavepainordiscomfortthattroubledthemallofthetimeor‘onandoff’formorethanthreemonths;22thisincreasedwithage,from14%ofmenand18%ofwomenaged16-34comparedto53%ofmenand59%ofwomenaged75andover.22
Key message – ThereisasubstantialburdenofchronicpainintheUKpopulation,thoughspecificprevalencefiguresvarydependingonthecriteriaanddefinitionsused.
4 British Medical Association Chronic pain: supporting safer prescribing of analgesics
Theincreasingprevalenceofchronicpaininapopulationwithagrowingproportionofolderpeoplemaybedirectlycontributingtotheincreasedprescribingofanalgesics,includingopioids.Numerousstudieshavesuggestedthatchronicpainismorecommonamongstolderpopulations,althoughnotnecessarilytheveryoldestagegroups.23,24Thisisparticularlythecasewhenrelatedtopaincausedbyconditionssuchasosteoarthritis,25 withtheseverityofchronicpainalsoincreasingwithage.25AsthemedianageoftheUKpopulationhasincreasedsignificantly–from33.9in1974to40.0inmid-2014–and17.6%ofthepopulationisnowover65,26 itwillbeimportanttoconsidertheimpactthismayhaveondemandforpainmanagement.
2.3 Analgesic drugs
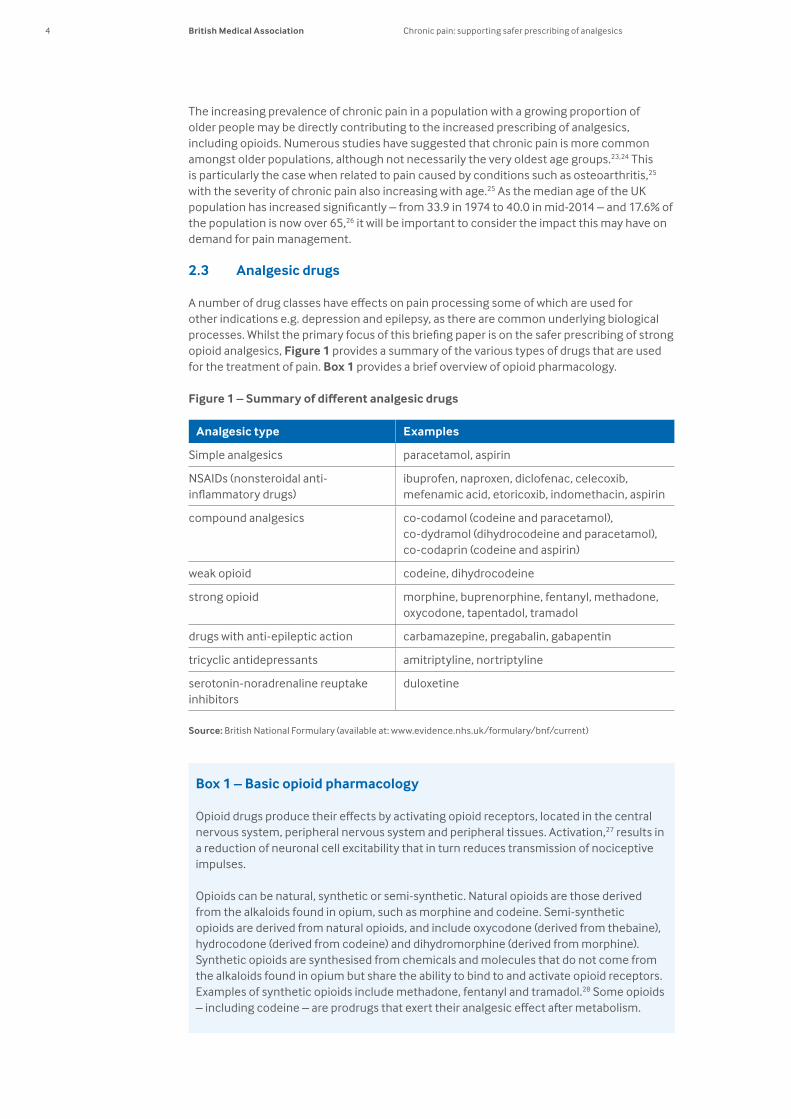
Anumberofdrugclasseshaveeffectsonpainprocessingsomeofwhichareusedforotherindicationse.g.depressionandepilepsy,astherearecommonunderlyingbiologicalprocesses.Whilsttheprimaryfocusofthisbriefingpaperisonthesaferprescribingofstrongopioidanalgesics,Figure 1providesasummaryofthevarioustypesofdrugsthatareusedforthetreatmentofpain.Box 1providesabriefoverviewofopioidpharmacology.
Figure1–Summaryofdifferentanalgesicdrugs
Analgesic type Examples
Simpleanalgesics paracetamol,aspirin
NSAIDs(nonsteroidalanti-inflammatorydrugs)
ibuprofen,naproxen,diclofenac,celecoxib,mefenamicacid,etoricoxib,indomethacin,aspirin
compoundanalgesics co-codamol(codeineandparacetamol), co-dydramol(dihydrocodeineandparacetamol),co-codaprin(codeineandaspirin)
weakopioid codeine,dihydrocodeine
strongopioid morphine,buprenorphine,fentanyl,methadone,oxycodone,tapentadol,tramadol
drugswithanti-epilepticaction carbamazepine,pregabalin,gabapentin
tricyclicantidepressants amitriptyline,nortriptyline
serotonin-noradrenalinereuptakeinhibitors
duloxetine
Source:BritishNationalFormulary(availableat:www.evidence.nhs.uk/formulary/bnf/current)
Box 1 – Basic opioid pharmacology
Opioiddrugsproducetheireffectsbyactivatingopioidreceptors,locatedinthecentralnervoussystem,peripheralnervoussystemandperipheraltissues.Activation,27 results in areductionofneuronalcellexcitabilitythatinturnreducestransmissionofnociceptiveimpulses.
Opioidscanbenatural,syntheticorsemi-synthetic.Naturalopioidsarethosederivedfromthealkaloidsfoundinopium,suchasmorphineandcodeine.Semi-syntheticopioidsarederivedfromnaturalopioids,andincludeoxycodone(derivedfromthebaine),hydrocodone(derivedfromcodeine)anddihydromorphine(derivedfrommorphine).Syntheticopioidsaresynthesisedfromchemicalsandmoleculesthatdonotcomefromthealkaloidsfoundinopiumbutsharetheabilitytobindtoandactivateopioidreceptors.Examplesofsyntheticopioidsincludemethadone,fentanylandtramadol.28Someopioids–includingcodeine–areprodrugsthatexerttheiranalgesiceffectaftermetabolism.

5British Medical Association Chronic pain: supporting safer prescribing of analgesics
3 Analgesic use for chronic pain
Theprescribingofopioidshasincreasedmarkedlyoverrecentyears,althoughtheevidencefortheirefficacyinthetreatmentofchronicpainconditionsremainsweak,andourincreasingknowledgeoftheirshortandlong-termsideeffects,raisesquestionsovertheiruse.2,3Thefollowingsectionshighlightrecenttrendsintheprescribingofopioidandotheranalgesics,andexploretheevidencefortheefficacy,safetyandpotentialharmsassociatedwiththeiruseinpeoplesufferingfromchronicpain.
3.1 Analgesic prescribing for chronic pain: UK trendsInrecentyearstherehasbeenasubstantialincreaseinthenumberofopioidanalgesicsprescribedforthemanagementofchronicnon-cancerpain,withincreasesoccurringinallpartsoftheUK,significantlyinexcessofanypopulationincreases(seeBox 2).Whileitisnotpossibletodetermineifitemswereprescribedforchronicpain,orwhethertheywereusedinpalliativecare,researchindicatesthatthemajorityofprescriptionsforopioidanalgesicsareforpatientswithchronicnon-cancerpain.29
Box 2 – Opioid prescribing trends in the UK
England – Therewasayearonyearincreaseinopioidprescribinginthecommunityfrom228millionitemsin1992to1.6billionin2009.30
– ThenumberofopioidanalgesicsprescribedingeneralpracticeinEnglandincreasedby1.5millionbetween2008and2013.22
– ThemostcommonlydispensedopioidanalgesicinEnglandisco-codamol,acompoundanalgesicofcodeineandparacetamol,withnumbersofprescribeditems–bychemicalname–increasingby5%from14.89millionto15.58millionbetween2010and2014.31,32 Overthesametimeperiodtheuseofmorphineroseby66%from2.44millionprescribeditemsto4.05million; buprenorphineuseroseby53%(1.19millionto1.83million);oxycodoneby44%(0.89millionto1.28million);codeineby37%(3.03millionto4.16million)andfentanylprescribingroseby22%(0.99millionto1.21million).32
Scotland – Theprescribingofanumberofopioidsincreasedbetween2010and2015.Thefastestincreaseswereseenforcodeineandmorphine.
– Over50%moremorphinewasdispensedin2014/15thanfouryearsearlier,upfrom280,351to440,472items.Codeineuseroseevenmorerapidly,witha64%increasefrom89,159to146,561items.Tramadoluserose12%from972,922to1,091,237items.Therewasalsoa33%increaseinoxycodoneuseanda23%increaseforfentanyl.33
Wales – Between2010and2014theprescribingofmorphineincreasedby105%,from168,736to345,808items,andcodeinefrom63%from85,528to120,257items.Tramadoluseroseby5%overtheperiod(563,071to592,678),buprenorphineby22%(93,843to114,559)andoxycodoneby23%(72,139to88,997).
Northern Ireland – AvailabledatafromNorthernIrelandindicatethatanalgesicuseoverallincreased by9.7%between2010and2014andby36.4%between2004and2014.34
Key message – AllpartsoftheUKhaveseensubstantialincreasesintheprescribingofopioidsoverrecentyears.

6 British Medical Association Chronic pain: supporting safer prescribing of analgesics
3.1.1 Other analgesics
Gabapentin and pregabalin TherehasbeenasteepriseinthenumberofprescriptionsofgabapentinandpregabalinforthemanagementofchronicpainingeneralpracticeinEngland.22In2012,nearlythreemillionitemsofpregabalin,andthreeandahalfmillionitemsofgabapentinwereprescribed,representinga350%and150%increaseinprescribingofthesedrugsrespectively,since2007.35,36In2013,thetotalcostforthesemedicinesinEnglandwas£237.9m,mostofwhichwasaccountedforbypregabalin,whichisstillunderpatentforuseinpain,andcostatotalof£211.2min2013.37
Scotlandhasseenasimilarlyrapidincreaseintheprescribingofgabapentinandpregabalin.Between2010/11and2014/15,thenumberofitemsdispensedforeachdrugmorethandoubled,withgabapentinrisingfrom302,736itemsto629,741,andpregabalinrisingfrom133,985to364,111items.34InWales,pregabalinitemsdispensedmorethandoubledbetween2010and2014,increasingfrom121,495to282,183,andgabapentinuserosefrom192,767to395,109items.42InNorthernIreland,pregabalinappearstobeprescribedmuchmorereadilythanintherestoftheUK,38withthecombinednumberofitemsofgabapentinandpregabalinprescribedtotalling352,000for2013,a29%riseintwoyears.39Asthesefiguresdonotbreakdowndispenseditemsbyindicationitisnotpossibletodeterminepreciselytheproportionprescribedforthetreatmentofpaincomparedto,forexample,thoseprescribedtotreatepilepsy.However,manufacturersofpregabalinhaveestimatedthatapproximately80%oftotalUKpregabalinprescriptionsareforthetreatmentofneuropathicpain.40
AntidepressantsTherehasbeenanincreaseintheuseofantidepressantsthataremostcommonlyusedorrecommendedforthetreatmentofpain.Totalprescriptionsforamitriptylineincreasedby36.1%andforduloxetineby131.3%,to11.85millionand1.36millionitemsrespectivelyinEnglandbetween2010and2014.31,32Althoughnotbrokendownbyindication,amitriptylineisnowusedmorecommonlyfortreatingpainthanitisfordepression.41InScotland,between2010/11and2014/15,amitriptylineprescriptionsincreasedby25.6%from931,799to1,169,917itemsandduloxetineby150%from60,279to150,790items.33InWales,amitriptylineincreasedby50.6%from575,196itemsto866,025items,andduloxetine108.7%from88,883to185,425items.42InNorthernIreland,prescribedamitriptylineitemsincreasedby76.2%from222,358to391,720andduloxetinefrom58,284to106,980items,or83.5%.34
NSAIDsItisnotclearwhatproportionofNSAID(nonsteroidalanti-inflammatorydrug)prescribingisforindividualswithchronicpain.TheprescribingofdiclofenacinthecommunityinEnglandhasreducedsignificantlyinrecentyears,fromover8.6millionitemstolessthan3million,nowaccountingforapproximately10%ofNSAIDprescriptions.43 ThesedatareflecttrendsthroughouttherestoftheUKwheretheprescribingofdiclofenachasdecreasedoverrecentyears.33,34,42Thishasmostlikelyresultedfromupdatedguidanceonitscardiovascularrisk(seeSection 3.3),andmayhaveimportantimplicationsfortheprescribingofopioidanalgesics.Incontrast,theprescribingofNaproxeninEnglandincreasedfrom1.1millionitemsin2005to7.6millionin2015.43 OverthesametimeperiodtheprescribingofIbuprofenincreasedfromapproximately6millionitemsto7.3million.InScotlandtheprescribingofibuprofeninthecommunityincreasedby79%between2014/15and2015/16,withNaproxenprescribingincreasingby18%.33

7British Medical Association Chronic pain: supporting safer prescribing of analgesics
3.2 Analgesic use in chronic pain – exploring the evidence
Thefollowingprovidesabriefintroductiontotheevidencesurroundingtheeffectivenessofopioidsandotheranalgesicsfortreatingchronicpain,aswellasthepotentialharmsassociatedwiththesedrugs.
3.2.1 EfficacyofopioidsforchronicpainAshighlightedbyOpioids Aware,thereisalargebodyofevidence–includingrandomisedcontrolled trialsaandsystematicreviews–thathasconcludedthatopioidsmayreducepainforsomepatientsintheshortandmediumterm(lessthan12weeks).44Theiruseinacutepainandforpainattheendoflifeiswellestablished.Thereis,however,alackofconsistentgood-qualityevidencetosupportastrongclinicalrecommendationforthelong-termuseofopioidsforpatientswithchronicpain.Meta-analysesassessingevidenceoftheeffectivenessofopioidsforpatientswithchronicpainofwhateveraetiology,havesuggestedthattheyareonlyeffectiveinaminorityofpatients.4,45,46,47,48,49,50,51,52,53
Alimitingfactoristhatmostclinicaltrialsofchronicpainmedicinesareconductedovera12-weekperiod,andthereareverylimiteddatathatprovideevidencefortheiruseforperiodsoflongerthansixmonths.Giventhelimiteddurationofmostclinicaltrialsforopioidanalgesics,andtheimpracticabilityofusingplacebocontrolsoverprolongedperiods,dataontheefficacyoflong-termusehasbeenlimitedtoassessmentincaseseriesandopen-labelextensionsofcontrolledtrials,bratherthanplacebo-controlledstudies.44Analysisofthesedatadoesnotallowfirmconclusionswithregardstofunctionalimprovementorimprovementinapatient’squalityoflife.A2015meta-analysis–assessingtheefficacy,tolerabilityandsafetyofopioidanalgesicsinopen-labelextensiontrialsoveradurationofsixmonthsormore–highlightedthatonlyaminorityofpatientsselectedforopioidtherapycompletedthestudies,yetsustainedeffectsofpainreductioncouldbeseeninthesepatients,includinginthosewithneuropathicpain.54Longtermcohortdatamayprovidefurtherinformationontheexperiencesofpatientsusingopioidslong-terminclinicalpractice.55Similarly,ithasbeensuggestedthat‘pragmatictrials’measuringawiderangeofpatientoutcomesshouldbeutilisedforassessingtheeffectivenessofpainmedications.56
Onedifficultyinassessingtheeffectivenessofopioidtreatmentarisesfromthenumberofpossibleadverseeffects,includingnausea,headache,somnolence,urinarycomplicationsandconstipation(seeSection 3.3).Manystudiessufferfromlow-compliancerates,57withpatientsdiscontinuingtreatmentduetoadverseeffectsorwithinsufficientpainrelief.
Ina2009evidencereviewbytheAmericanPainSociety,itwashighlightedthatwhilstrecommendationsfortheuseofopioidsinchronicpainhavebeenmadeonthebasisofasystematicreview,thesearerarelysupportedbyhighquality,orevenmoderatequalityevidence.Instead,theyrelyonexpertconsensustoovercomenumerousresearchgapsinareassuchasbalancingtherisksandbenefitsofopioidtherapy.58
Key messages – Thereisalackofgood-qualityevidencetosupportastrongclinicalrecommendationforthelong-termuseofopioidsforpatientswithchronicpain
– Thereareonlylimiteddatathatprovideevidencetosupporttheuseofopioidsforperiodsoflongerthansixmonths
– Manyclinicalstudiesofopioidsforchronicpainsufferfromlow-compliancerates,withpatientsdiscontinuingtreatmentduetoadverseeffectsorwithinsufficientpainrelief.
a Randomisedcontrolledtrialsarestudiesinwhichpeoplearerandomlyassignedto2(ormore)groupstotestanintervention.Onegrouphastheinterventionbeingtested,theother(controlgroup)hasanalternativeintervention,adummyintervention(placebo)ornointerventionatall.
b Open-labelextensionstudiestypicallyfollowonfromrandomisedcontrolledtrials,toallowassessmentoveralongerperiodoftime.Theyarenotplacebocontrolledandbothresearchersandparticipantsknowwhattreatmentisbeingadministered.

8 British Medical Association Chronic pain: supporting safer prescribing of analgesics
Current guidance on opioid prescribing for chronic pain Despitelimitationsintheevidence,guidanceisavailableforprescribersintheUKontheuseofopioidsfortreatingpain.ClinicalguidancefromNICE(NationalInstituteofHealthandCareExcellence)ondrugtreatmentforneuropathicpainrecommendstheuseofmorphineortramadoltotreatneuropathicpainonlywhenadvisedbyaspecialist.59Ithasgradedmostoftheavailableevidenceasloworverylowduetoinsufficientfollow-upperiods.59Separately,guidancefromtheIASPNeuropathicPainSpecialInterestGroup(NeuPSIG)–basedonsystematicreviewandmeta-analysis–madeonlyweakrecommendationsfortheuseoftramadolandotherstrongopioidsassecondandthird-linetreatments,respectively,forneuropathicpaininadults.46Originallydevelopedtoassistthetreatmentofcancer-relatedpain,theWHO’sanalgesicladderisoftenusedasaguidetothetreatmentofchronicpainbutithasneverbeenvalidatedinthissetting.Theanalgesicladdersuggeststhatwithincreasingreportedpainintensity,increasinglystronganalgesicsshouldbeprovidedanddosesofstrongopioidsincreaseduntilpainiscontrolled.Chronicpainisacomplexentityreflectingfactorsbeyondtheoriginal,orongoing,stimuli.Furthermore,theevidencethatescalationofopioiddosesinthissettingconfersanimprovementinpainorfunctionisweakandthereisstrongevidencethatharmfromopioidsisdoserelated. IthasbeensuggestedthatuseoftheWHOladderinpatientswithlongtermpainfailstorecognisethecomplexityofthechronicpainexperience,andmaycontributetoinappropriateprescribing.60
In2010,theBPSproducedgoodpracticeguidelinesonopioiduseinpersistentpain,statingthat,whileopioidscanbeeffective,otherevidence-basedinterventionsshouldbeusedifavailable.11 Opioids Awarereplacesandsupersedesthe2010guidanceandplacesemphasisongeneralprinciplesofgoodprescribingpracticeunderpinnedbyanunderstandingoftheconditionbeingtreated,appropriatepainassessmentandmonitoringofprescribingtoensurethatmedicinesthatareineffectivearestopped(seeBox 3).61
Box 3 – ‘Opioids Aware’ prescribing resource
Opioids AwareisaprescribingresourcefundedbyPHE(PublicHealthEngland)andproducedbytheFPM(FacultyofPainMedicine)inconjunctionwithNHSEngland,othermedicalRoyalColleges,NICE,theCQC(CareQualityCommission),NHSBSA (NHSBusinessServicesAuthority),theRoyalPharmaceuticalSocietyandtheBritishPainSociety.Theresourceaimstosupportallhealthcareprofessionals,patients,andcarersinunderstandingthepotentialbenefitsandharmsofopioidtreatment.
Recognisingthatexistingguidancehasbeenrelativelyunsuccessfulininfluencingtheuseofanalgesics,ithastakenadifferentapproach.Itinsteadbreaksdowntheavailableevidenceintosmallersections,makingitmoreaccessibleandplacingopioidsinthewidercontextofpainmanagement.Itprovidesguidanceinthefollowingareas:
– Bestprofessionalpractice; – Thecondition,thepatient,thecontext – Clinicaluseofopioids – Astructuredapproachtoopioidprescribing – Informationforpatients
Theresourcecoversissuessuchasopioidsandthelaw;writingprescriptions;reportingharms;theroleofpharmacistsinsafeprescribing;assessingandmanaginglong-termpain;theroleofmedicines;effectivenessofopioids;sideeffectsandharms;prescribingtrends;problemdruguseandspecialcircumstances.

9British Medical Association Chronic pain: supporting safer prescribing of analgesics
Adetailedexplanationoftherisksandbenefitsmustbeundertakenwiththepatientbeforeopioidsarestarted.Asmallproportionofpeoplemayobtaingoodpainreliefwithopioidsinthelongtermifthedoseiskeptlowandespeciallyiftheiruseisintermittent.Thesepatientscanbemanagedwithregularmonitoring.Toomanypeoplewithchronicpainareprescribedopioidsathighdoses.Theriskofharmincreasessubstantiallyathighdose.Aboveanoralmorphineequivalentdailydoseof120mg,furtherbenefitisunlikely.Ifbenefitinpainreductionandimprovedfunctionisnotachievedatlowdose,opioidsshouldbediscontinued,evenifnoothertreatmentisreadilyavailable.
Chronicpainisverycomplexandifpatientshavedisablingsymptomsthatdonotrespondtotreatment,adetailedassessmentofthemanyemotionalinfluencesontheirpainexperienceisnecessary.ThismaybedonebyaGPorinapainmanagementservice.Patientswithchronicpaininhighdoseopioidsshouldbereferredtospecialistpainmanagementservices,andifpossiblejointpainandaddictionservices.Theidealpracticeisthentoreducetheopioiddose.FurtherguidanceisavailablefromOpioids Aware
Recommendation:Tobetterinformclinicalpracticemoreresearchisrequiredintotheeffectsoflong-termprescribingofopioidsforpainrelief,includingtheirefficacy &safetyforperiodslongerthansixmonths.
3.2.2 Efficacyofotheranalgesicsforchronicpain
Gabapentin and pregabalinGabapentinandpregabalinarelicensedintheUKforthetreatmentofneuropathicpainandrefractoryepilepsy.Pregabalinisalsolicensedforthetreatmentofgeneralisedanxietydisorder.Theevidencefortheuseofgabapentinandpregabalinforthetreatmentofneuropathicpainismorecomprehensivethanthatofopioids,asreflectedintheirindicationsandtheirrecommendeduseinguidelines.NICEclinicalguidanceforprimarycareprofessionalsondrugtreatmentforneuropathicpainrecommendstheuseofgabapentinorpregabalin(aswellastheanti-depressantsduloxetineoramitriptyline)asinitialtreatment,withdueconsiderationofapatient’sco-morbiditiesandcontext.59,62 Thisrecommendationisbasedonevidencefromrandomisedcontroltrialsshowingthatbothreducepainincomparisontoaplacebo.59Separately,asystematic-reviewandmeta-analysisfromtheNeuPSIGoftheIASPrecommendedgabapentinandpregabalinforfirst-lineuseinadultswithneuropathicpain.46Despitetheserecommendations,a2014systematicreviewconcludedthatoverhalfofpatientstreatedwithgabapentinforchronicneuropathicpainorfibromyalgiacwillnothavesubstantialpainrelief,determinedasareductioninpainintensityofatleast50%.63Sixineverytenpatientscanexpecttohavesomeadverseeffects,suchasdizziness,somnolence(drowsiness),peripheraloedema(swelling)orgaitdisturbance.63
Aseparate2009systematicreviewconsideringtheuseofpregabalinsimilarlyfoundnousefulbenefittoasignificantproportionofpatients.64However,inbothcases,asmallnumberofpatientswerefoundtobenefitsubstantially,includingwithmarkedimprovementsintheirqualityoflife,whilemorebenefittedmoderately. Thereisnogoodevidenceforeffectivenessofgabapentinandpregabalinforacutepainorforlong-termpainthatisnotofneuropathicorigin.Moreresearchisrequiredtoensuregabapentinandpregabalinareusedinthebestpossibleway,tomaximisethepotentialbenefittopatientswithchronicpain,whilstminimisingtheriskofharm.50
c Fibromyalgiaisalong-termconditionthatcancausewidespreadpainandsymptomsinmanyotherbodilysystems.

10 British Medical Association Chronic pain: supporting safer prescribing of analgesics
AntidepressantsThereisevidencethatsomeantidepressantsmaybehelpfulforsomepatientswithchronicpain.A2007systematicreviewsuggestedthatanumberofantidepressants–in-particulartricyclicantidepressants–canbeeffectiveinthetreatmentofchronicpain.65However,a2015systematicreviewassessingtheuseofthetricyclicantidepressantamitriptylineforthetreatmentofneuropathicpainconcludedthat,despiteitswidespreaduseandsuccessfultreatmentinmanypeoplewithneuropathicpain,thereisalackofsupportiveunbiasedevidenceforitsbeneficialeffect,withfewstudiesmeetingthemostrecentresearchstandards.66
Inareviewof19studiesconsideringtheanalgesiceffectofSNRIs(serotonin-noradrenalinereuptakeinhibitors),12foundthattheyprovideclinicallyimportantpainreliefandareassociatedwithfewerside-effectsthantricyclicantidepressants.67Thereismoderatelystrongevidence–basedontheGradeProsystemofassessingevidenced–thattheSNRIsduloxetinereducespainindiabeticneuropathyandfibromyalgia.Asystematicreview,consideringsixrandomisedcontrolledtrials,concludedthatduloxetineisusefulforrelievingpainfromfibromyalgiaanddiabeticneuropathy,andaboutaseffectiveasotheravailabledrugs.68Althoughonesystematicreviewsuggeststhatamitriptylinedemonstratessuperiorefficacytoduloxetine.69Asystematic-reviewandmeta-analysisfromtheNeuPSIGoftheIASPrecommendedSNRIsortricyclicantidepressantsasfirst-linetherapyforneuropathicpain.46
NICEguidanceforthetreatmentofneuropathicpainrecommendstheuseofamitriptylineandduloxetineasfirstlinetreatmentsforneuropathicpain,alongsidegabapentinandpregabalin.Switchingbetweenthesefourisrecommendedifthefirstisnotsuccessful.62 SIGNguidanceforthetreatmentofchronicpainrecommendstheuseofamitriptylineforneuropathicpainandfibromyalgia,andtotryalternativetricyclicantidepressantsifthere isaneedtoreducesideeffects.
NSAIDsA2015systematicreviewconcludedthatthereisnoevidencetosupportorrefutetheuseofNSAIDsinneuropathicpainconditions,70whichisreflectedintheguidanceavailableforthetreatmentofneuropathicpain.A2015reviewofNSAIDsforchroniclowbackpainconcludedthattherewaslowqualityevidencethattheyareslightlymoreeffectivethanplacebo.71 AseparatereviewoftopicalNSAIDsforchronicmusculoskeletalpainindicatedthattheyprovidedsignificantlymoretrialparticipantswhohadosteoarthritisofthekneeorhandwithgoodlevelsofpainreliefthanplacebo,butthattherewasnoevidencefortheeffectivenessoftopicalNSAIDsinotherchronicpainfulconditions.72
d GradeProistheofficialsoftwareoftheGradingofRecommendationsAssessment,DevelopmentandEvaluation(GRADE)WorkingGroup,withthegoalofcreatingacommonapproachtogradingqualityofevidence.IthasbeenupdatedforusebyCochranereviewauthorstocreatesummaryoffindingstables. http://tech.cochrane.org/revman/other-resources/gradepro/about-gradepro

11British Medical Association Chronic pain: supporting safer prescribing of analgesics
3.3 Potential harms associated with long-term analgesic use in chronic pain
Therearesignificantpublichealthconcernsabouttheharmfuleffectsofanalgesics,particularlyregardingtheirlong-termuse.Thefollowingbrieflyexploresthepotentialharmsassociatedwiththeuseofopioids,andotheranalgesics,forthetreatmentofchronicpain.
Box 4 – Opioid prescribing in the USA
ConcernsabouttheharmscausedbyextensiveprescribingofopioidshavebecomeparticularlypertinentasaresultoftheirextensivemisuseintheUSA.
AccordingtotheCDC(CentersforDiseaseControl),theannualnumberofopioidprescriptionsintheUSAquadrupledbetween1999and2014.73Thisincreasehasbeenmatchedbyasteepincreaseinopioid-relatedmortality.74Mortalitytrendsindicatearapidincreaseinthenumberofdeathsfromunintentionaldrugpoisoningwithopioidanalgesics,withdeathsinvolvingopioidsrisingfrom4,041in1999to14,459in2007.44Seventy-fivepercentofallpharmaceuticaloverdosedeathsintheUSAin2010involvedopioids.75In2014,morethan14,000peoplediedfromoverdosesinvolvingprescriptionopioids.74AccordingtodatafromtheCDC,prescriptiondrugoverdosesintheUSAoccurdisproportionatelyamongstpatientswhoareseeingmultipledoctors,orseeingonedoctorandreceivingahighdosage.76
IntheUK,therehasbeenafocusonunderstandingthelessonsthatcanbelearnedfromthesignificantprescriptionopioidmisuseintheUSA.Thishasincludedexplorationoftheextenttowhichthesituationiscomparablebetweenthetwocountries,andidentifyingwhichcontributoryfactorsmaybeuniquetotheUSA.77,78 Ithas,forexample,beensuggestedthatpharmaceuticalcompanymarketingpracticesintheUSAhaveservedtoinflatethebenefitsandobscuretheharmsofprescriptionopioids.78IthasalsobeenhighlightedthatspecificdifferencesinthehealthcaresystemsofthetwocountriesmayinfluencetherelativeharmsassociatedwithopioidmisuseintheUSAandUK,77,78asmayeachcountry’swiderpolicyonillicitdrugs.77
3.3.1 Harms associated with opioids
Mortality AshighlightedinSection 3.1,prescribingdataindicatesthattheuseofopioidshasincreasedsubstantiallyintheUK.TodatethishasnotresultedinthesamesignificantincreaseinopioidrelateddeathsthathasbeenseenintheUSA(seeBox 4).77TheUKhas,however,seenanincreaseindeathsinvolvingopioidswithheroin,methadoneandmorphine(thislatternotedatpostmortemasametaboliteofheroin)beingthebiggestcontributors.AlthoughthetotalnumbersaresubstantiallylowerthanintheUSA,theoveralltrendsaresimilar.ThoughitshouldbenotedthatintheUSAprescriptionopioiddeathssignificantlypredominateoverheroin.79EnglandandWalesexperiencedadoublingofannualdeathsinvolvingcodeinebetween2005and2009,80andtherewereatotalof128deathsinvolvingcodeinein2015.81 Therehasalsobeenasignificantincreaseinthenumberofdeathsrelatedtotramadol,risingfromonerecordedinEnglandandWalesin1996,to208in2014althoughmostrecent(2015)datashowafallinthelast12months.81Thesemortalitydatapromptedschedulingofthedruge in 2014.82Mosttramadoldeathswereinconjunctionwithotherdrugsanditisnotknownwhetherthetramadolwasorwasnotprescribedforthosepatientsinwhomthedrugwasmentionedonthedeathcertificate.InScotland,tramadol-relateddeathsincreasedfromeightin2001to34in2011.55 StatisticsfromNorthernIrelandalsoshowanincreaseindeathsfromarangeofopioids.Between2003and2013,thenumberofdeathsinwhichtramadolwasmentionedonthedeathcertificaterosefrom0to20,althoughthisisdownfromahighof31in2012.Deathsinvolvingcodeinerosefrom2to22overthesameperiod.83
e FurtherinformationfromNICEaboutcontrolleddrugsisavailablehere.

12 British Medical Association Chronic pain: supporting safer prescribing of analgesics
Respiratory depressionOpioidscanhaveaneffectonrespirationviaanumberofmechanisms,84andrespiratorydepressionhasbeenhighlightedasaparticularprobleminacutepainmanagement–wherepatientshavenotdevelopedtolerance.44 Inpatientswithchronicpain,therearespecificconcernsoverdisturbanceofnocturnalrespiratorycontrol.85Forexample,therehavebeenreportedfatalitiesinpatientswithsleepapnoeawhoareprescribedopioids,andparticularrisksarisewhenopioidsareprescribedwithothersedativedrugs,particularlybenzodiazepines.44
Endocrine and immune effects Thereisevidencethatopioidusecanadverselyimpactuponarangeofendocrinefunctions.86AshighlightedinOpioids Aware,opioiduseisassociatedwithhypogonadismandadrenalinsufficiencyinbothsexes.61 Ithasalsobeendemonstratedinanimalandhumanstudiesthatopioidscanhaveasuppressiveeffectonimmunefunction,butthatthismaydifferfordifferentopioidanalgesics.61,87
Hypersensitivity to pain (hyperalgesia)Anumberofstudieshaveindicatedthat,paradoxically,prolongeduseofopioidscanresultinhypersensitivitytopain(hyperalgesia).A2006systematicreviewofopioid-inducedhyperalgesiahighlightedthatopioidanalgesicscanrenderpatientsmoresensitivetopainandpotentiallymayaggravatepre-existingpain.88 Opioids Awarestatesthathyperalgesiahasbeendemonstratedinpreclinicalstudies,inpatientsreceivinghighdosepotentopioidsasacomponentofgeneralanaesthesiaandinexperimentalstudiesofpatientsmaintainedonmethadoneforthetreatmentofopioidaddiction.Theclinicalsignificanceofthesefindingsinroutineprescribingisnotknown.61
Dependence and withdrawal The2016BMAanalysisreportonPrescribed drugs associated with dependence and withdrawalhighlightedthepotentialthatopioids,prescribedtotreatchronicpain,willleadtotoleranceandphysicaldependence,especiallywithprolongedtreatmentandathigherdoses.2Thereportalsonotedthatwithdrawalsymptomscanbesevereanddisabling.2It shouldbenotedthattoleranceandtheexperienceofwithdrawalsymptomsonopioidcessationarenormalpharmacologicaleffectsofopioidtreatmentandshouldnotbeconfusedwithaddictionoropioidmisuseorabuse.Therearecertainriskfactors–includingco-morbidmentalhealthdisordersandsubstancemisusedisorders–thatlong-termepidemiologicaldataindicateareassociatedwithindividualsbeingmorelikelytoreceiveopioidprescriptionsforpain.Patientswiththeseriskfactorsaremorelikelytobeprescribedhigherdosesofopioidsandmorelikelytobeco-prescribedothercentrallyactingdrugsincludingbenzodiazepines–aphenomenondescribedas‘adverseselection’.44
3.3.2 Harms associated with other analgesics
Gabapentin and pregabalin Aswithopioids,gabapentinandpregabalinhavebeenassociatedwithincreasingmortalityintheUK.Instancesofgabapentinbeingmentionedondeathcertificatesincreasedsignificantly,from4in2010to49in2015.81Pregabalinhasshownanincreasingtrendintermsofprescriptionlevels,positivepost-mortemtoxicologyfindings,andinthemisuseofthedrugbeingimplicatedindeath.59Instancesofgabapentinbeingmentionedondeathcertificatesincreasedfrom4in2010to90in2015.81
ThedependencepotentialassociatedwithgabapentinandpregabalinhasalsoledtoconcernsthatthenumberofpeoplemisusingtheseprescriptionmedicinesmayberisingintheUK. PHEandNHSEnglandhaveproducedadviceforprescribersonthepotentialformisuseofgabapentinandpregabalin,warningofthedangersofdependenceandthediversionofprescribeddrugs –wherebydrugsareunlawfullytransferredfromtheirintendedrecipienttoanotheruserordistributor.37Highlevelsofmisuse,particularlyofpregabalin,havebeenreportedinprisonpopulations,and, inJanuary2016,theACMD(AdvisoryCouncilfortheMisuseofDrugs)recommendedthat–duetotheharmsassociatedwiththesedrugs–gabapentinandpregabalinshouldbecontrolledundertheMisuseofDrugsAct1971.89

13British Medical Association Chronic pain: supporting safer prescribing of analgesics
AntidepressantsDatafromtheOfficeforNationalStatisticsindicatethat,in2013,therewere466deathsinEnglandandWalesassociatedwithantidepressants,withthenumberofdeathsassociatedwithamitriptylinerisingby12%since2012.90Thoughavailabledatadoesnotallowforadistinctionbetweenpatientswhoweretakingantidepressantsfordepressionandthosetakingthemforthereliefofpain.
TCAs(tricyclicantidepressants)areassociatedwithanumberofadverseeffects,includingdrymouth,constipation,tachycardia,cardiacarrhythmia,andblurredvision.Overdosewiththesedrugsisassociatedwithahighrateoffatality.91IncomparisontoTCAs,SSRIs(selectiveserotoninreuptakeinhibitors)havemoretolerablesideeffectsandgreaterrelativesafetyinoverdose,92,93butareassociatedwithgreaterwithdrawalsymptomsinpeoplediscontinuinguse.94A2009systematicreviewoftheuseoftheSNRIduloxetineindicatedthatmostpeopletakingitwillhaveatleastonesideeffect,butthesearemostlyminor.Neverthelessaboutoneinsixpeoplediscontinueduloxetineasaresultofsideeffects.68
NSAIDs TherearespecificissuesaroundtheuseofNSAIDs,includinglong-standingandwell-recognisedgastrointestinal,cardiovascularandrenalsafetyconcerns,whichhavebeensummarisedinNICEprescribingguidance.95ThishighlightsthatadecisiontoprescribeNSAIDsshouldbebasedonanassessmentofaperson’sindividualriskfactors,includinganyhistoryofcardiovascularandgastrointestinalillness.95ConcernsoverthecardiovascularandgastrointestinalsafetyofNSAIDsmayhavecontributedtoincreasedprescribingofotheranalgesic classes.

14 British Medical Association Chronic pain: supporting safer prescribing of analgesics
4 Supporting the management of patients with chronic pain
Overthelastfewdecades,opioidshavebeenincreasinglyusedintheUKtomanagechronicpain.Potentialreasonsforthisincludetheavailabilityofnewpreparationsandformulationsofopioids,changesinpatientexpectation,prescribingpractice,andsocietalattitudes.12Otherstudieshaveidentifiedalackofconsensusregardingappropriateuseofmedicines,alackofsuitablealternatives,thedifficultystoppingorreducingapatient’sopioidprescription,andpatientdemandforopioidtreatments(includingfromthosewhomaybeaddictedoraredivertingprescriptionmedicines).96Afurthercontributoryfactoristhehistoricunder-treatmentofpain,whichmayhavemotivatedwell-intentionedeffortstoenhancetheavailabilityofprescriptionanalgesics,includingopioids.96Giventheweakevidencebaseandpotentialharmsassociatedwithlongtermanalgesicusediscussedintheprecedingsection,thereisaneedtoexploretherangeofsupportrequiredforpatientssufferingfromchronicpain.
Thefollowingsectionsfocusonthestepsrequiredtoensurethatallpatientswithchronicpainhaveaccesstothemostappropriatetreatment,andtoensuredoctorsareadequatelysupportedinthemanagementofthesepatients.
4.1.1 Attitudes towards the use of opioidsfor chronic painAnalysisoftheattitudestoopioidprescribingintheUSAhassuggestedthat,historically,concernsaboutaddiction,thepotentialforincreaseddisabilityandlackofefficacyoverlongertime-periodslimitedtheiruseinthetreatmentofchronicpain.97Inthe1980s,reportsandarticlesbegantoemergethatsuggestedopioidscould,orshould,beusedtotreatchronicpain,basedonearlierexperiencestreatingcancerpatients. Twopapershavebeenidentifiedasbeingparticularlyinfluentialinthisregard.97In1986,PortenoyandFoleypublishedapaperdescribingtheirexperiencesoftreatingpatientswithnon-malignantpainthatstronglyadvocatedtheuseofopioidsoverlongerperiodsoftime.98In1990,Melzackwrote‘TheTragedyofNeedlessPain’,97,99whichcalledformoreresearchintotheuseofopioidsfornon-cancerchronicpain,arguingthatpeoplewereunnecessarilysufferingfrompainbecauseoffearsofaddiction.
Prescribingbehaviourinrelationtoopioidsmaybesubjecttoarangeofinfluences.A2007surveyofGPs’attitudesfoundthat53%ofthosewithoutspecialisttrainingfeltthatboththeirmedicalschoolandprimarycaretrainingwereinadequatewithregardtopainmanagement.100Evensoitsuggestedthatthepresenceofguidelinesandthelevelofspecialisttraininghadlittleimpactontheprescribingofopioids.InthestudyGPswhodidnotcommonlyprescribeopioidswerefoundtobeolder,andtohavebeenpracticingforlonger,thanthosewhodid.100 Aseparate2008surveyofGPsintheUKindicatedthatthelikelihoodofprescribingopioidsmaybeinfluencedbyapractitioner’sage,genderanddegreeofspecialisttraining.101AfurthersmallqualitativestudyoftheattitudesofGPstoprescribingsuggestedthattheyhadamorecautiousapproachtoprescribingopioidsforchronicnon-cancerpainthanforcancer-relatedpain.102
A2015qualitativestudyofopioidprescribinginprimarycarehighlightedarangeoffactorsidentifiedbypatientsanddoctorsthatinfluencedprescribinginthissetting.Theseincludedthedifficultiesofshort-term,oftenemotionallychargedconsultations;highlightingtheimportanceofcontinuityinthedoctor-patientrelationship.103

15British Medical Association Chronic pain: supporting safer prescribing of analgesics
4.1.2 Challenges when stopping opioid treatment Doctorscanfacesignificantchallengesinstoppingopioidtreatmentforpatientsinwhomthesemedicationshavenotprovidedeffectivepainrelief.Thismayresultinpatientsbeingprescribedopioidsdespitethefactthattheyarereceivingnobenefitfromthem.Assetout in Opioids Aware (seeSection 3.2), ifitisthoughtopioidtherapymayplayaroleinapatient’spainmanagement,atrialshouldbeinitiatedtoestablishwhetherapatientachievesareductioninpainwiththeuseofopioids–ifnottheyshouldbestopped.44Thedifficultiesinceasingopioidtreatmentifnoteffectivehavebeenacknowledged.3Itcan,forexample,beverydifficulttotellapatientthattheirtreatmentisnotworkingwhentheyareclearlyinpain,andthereareoftenfewalternativestousingopioidsinattemptingtoreducechronicpain.3
Guidanceontheuseofopioidsforchronicpaindoesrecommendstrategiestomanagethis.Forexample,theSIGNpathwayforusingstrongopioidsinpatientswithchronicpainrecommendsatrialofopioidswithstoppingrulesagreedwiththepatient,suchasiftreatmentgoalsarenotmet,orifthereisnoclearevidenceofdoseresponse.104Ithasbeenhighlightedthatwhileopioids,aswellasotheranalgesicsincludinggabapentinandpregabalin,canworkeffectivelytorelievepain,thisisonlyachievedinasmallpercentageofpatients,andprescribersmustexpectanalgesicstofailforthemajorityofpatients.105Itisunusualforanyanalgesic,includingopioids,tocompletelyeliminatepain,andthatthefocusoftreatmentshouldbeonreducingapatient’spainwithaviewtoimprovingtheirqualityoflife.
Recommendation:Considerationshouldbegiventotherangeofsupportthatisrequiredfordoctorsandpatientsduringtheprocessofassessment,trialandreviewofopioidtreatmentforchronicpain.Thisshouldincludesupportforstoppingopioidtreatmentthatisnotworking.
4.1.3 SupportingtheeffectivemanagementofchronicpaininprimarycareMostpatientswithchronicpainfirstcontacthealthservicesthroughprimarycare,andaresubsequentlymanagedinthissetting.AccordingtotheRCGP(RoyalCollegeofGeneralPractitioners),peoplewithchronicpainconsulttheirGParoundfivetimesmorefrequentlythanthosewithout,andchronicpainisapresentingconditioninaround22%of consultations.106Itisgenerallyacceptedthatmorestraightforwardpainproblemscanbeassessedandmanagedbynon-specialistsinaprimarycaresetting,withspecialistcarerequiredforcomplexpain,andevenwhenpatientsarereferredtospecialisttreatment,theirongoingcareislikelytoreturntotheirGP.107Ina2015parliamentaryreport,theChronicPainPolicyCoalitioncalledforaminimumstandardofyearlyassessmentofpatientsbeingtreatedwithopioidsfortheirchronicpain.108
Supportingactioninthisareaisdependentuponadequateresourcingofgeneralpractice.AshighlightedintheBMA’s2015visionforgeneralpractice–Responsive, safe and sustainable: towards a new future for general practice–havingsufficienttimetospendwithpatientsisoneoftheleadingfactorsidentifiedbyGPsthatcouldhelpthemtobetterdelivertheessentialsofgeneralpractice.109Thevalueofadequateconsultationtimesisparticularlyimportantforpatientsthathavecomplexconditionswhichmayrequiregreaterexploration,asisoftenthecaseforpeoplesufferingfromchronicpain.Sufficientresourcesarealsonecessarytosupportregularreviewsofmedicationuse.Furtherconsiderationshouldbegiventotheroleofpharmacistsinpainmanagementinprimarycaresettings.110,111
Recommendation:Sufficientinvestmentandresourcesforprimarycare,includinglongerconsultationtimes,arerequiredtosupportimprovementsinanalgesicprescribingforpatientswithchronicpain.

16 British Medical Association Chronic pain: supporting safer prescribing of analgesics
4.1.4 Supporting the development of specialist chronic pain servicesSomepatientswithchronicpain,includingthosewithcomplexco-morbidities,willrequirethesupportofspecialistservices.115Specialistsinpainmedicineplayacentralroleinpainmanagementascompetentphysicianswiththetrainingandexpertisetounderstandandmanagepainfulmedicalconditions,diagnosetreatableunderlyingcausesofpainandhighlightunmetphysicalandmentalhealthneeds.Referraltospecialistpainservicesisindicatedwherepainisassociatedwitheitherorbothhighlevelsofdistressand disabilityorwhenseverepainremainsrefractorytotreatment.Improvingaccesstospecialistserviceswouldbettersupportpatientstocopewithpain,andmayreduceinappropriateprescribingofstronganalgesics.Amultidisciplinary/multiprofessionalapproachisrecognisedasthemainrequirementforthisandthereshouldbereadyaccesstopainmanagementprogrammesforpatientswhoarelikelytobenefit(seeBox 5).112Multidisciplinarychronicpainservicesaremoreeffectivethannotreatment,ortreatmentasusual,forarangeofpatientoutcomes,includingpainexperience,moodandactivitylevels.115Therearearangeoffactorsthatimpactuponaccesstospecialistservices,including:thegeographicaldistributionofclinics;whetherservicesmeettheminimumstandardsforamultidisciplinaryservice;andreferraltopainmanagementservicesandthewaitingtimestoaccessthem.113 Thedevelopmentofspecialistservicesnecessitatessufficientavailabilityofappropriatelytrainedhealthcareprofessionals.Ithas,forexample,beenhighlightedthatthereisalackofpainmedicinespecialistsinsomepartsofEnglandandWales,andasawholeEngland&Walescurrentlyhavefewerchronicpainconsultantsper100,000populationthanScotlandandNorthernIreland–equatingtoatotalshortfallof118chronicpainspecialists.114
Box 5 – Pain management programmes
TheBPShaveproducedguidelinesforpainmanagementprogrammesforadults.Thesehighlightthattheprincipleofpainmanagementprogrammesisto“enablepeoplewithchronicpaintoachieveasnormalalifeaspossiblebyreducingphysicaldisabilityandemotionaldistress,andimprovingtheindividual’sabilitytoself-managepain-associateddisabilityandreducerelianceonhealthcareresources”.115
Thoughtheyshouldnotnecessarilybeexpectedtoachieveareductioninapatient’spain,thereisgoodevidencefortheefficacyofpainmanagementprogrammesinimprovingpainexperienceandphysicalfunctioningandfortheirpotentialtoreducemedicationuse.115
Psychologicalinterventionsmayhaveanimportantroleinthetreatmentofsomepatientswithchronicpain.Thereismoderateevidencethatpsychologicaltherapiescanhelppeoplewithchronicpainreducenegativemood(depressionandanxiety),anddisability.116 Thoughforsometypesofpain–forexampleneuropathicpain–thereisalackofstudiesassessingtheeffectivenessofthesetherapies.117Researchalsosuggeststhatpatient’sattitudestowardstheirpaincanhaveaninfluenceontheirqualityoflife.Forexample,fearofmovementasaresultofthepain,andotherpain-relatedfearscanbemoredisablingthanthepainitself,sotacklingsuchissuesisavitalconsiderationofanytreatment.118
Itisveryimportantthatco-morbidmentalhealthdisordersareidentifiedandmanagedappropriately.Oneapopulation-basedcase-controlstudyfconductedinManchesterfoundthatpatientswithchronicpainwerethreetimesmorelikelytosufferfromamentaldisorder,withmostpatientssufferingfrommoodandanxietydisorders.119
f Case-controlstudiesareobservationalstudiesthatcomparegroupsofpeoplewithandwithoutaparticulardisease or condition.
17British Medical Association Chronic pain: supporting safer prescribing of analgesics
Patientswithcomplexmultiplemedicalsymptoms,particularlyiftheyarefindingitdifficulttoreducehighharmfuldosesofopioids,needtobemanagedinteamswithmentalhealthexpertiseindiagnosingandmanagingcommonmentalhealthdisordersincludingsignificantdepression,personalityvulnerabilities,post-traumaticstressdisorder,somatisationdisorder,addiction,andinmanagingtheemotionaleffectsofprevioustraumaticexperiences.
Access to servicesThereishighvariationinaccesstomultidisciplinarycare,withmanypainclinicsnothavingadequateaccesstoapsychologist,physiotherapistandphysician.20The2012NationalPainAuditfoundthatonly40%ofpainclinicsinEngland,and60%inWales,mettheminimummultidisciplinarystandard–thepresenceofapsychologist,physiotherapistandphysician–comparedto64%and80%respectivelythatself-identifiedasmultidisciplinary.Thereportrecommendedbetteraccesstophysiotherapyandpsychologygiventhehighrateofanxietyanddepression,andthelinkwithpoorphysicalfunctioning.20Italsohighlightedthatpainclinicsshouldbeabletotreatawidevarietyofconditions;theaudit,forexample,indicatedthatsomeclinicsappeartofocusmainlyonspinalpainorothermusculoskeletalcomplaints,despitetheneedfortreatmentforconditionssuchaspelvicpainornon-musculoskeletalneuropathicpain.20FreedomofinformationrequestsfromtheChronicPainPolicyCoalitioninJune2013indicatedthat,ofall211CCGsinEngland,28%hadnonamedclinicalleadforpainservices,27%couldnotprovideanamedmanageriallead,and29%ofdidnotcommissionmultidisciplinarypainservices.120
Closerworkingbetweendifferentpartsofthehealthcaresystemisessential.Integratedworkingbetweenprimarycareandthespecialisttreatmentprovidedbysecondarycare,orspecialistcommunity-basedservices,isincreasinglyseenasthemoreappropriatemodelofcareforachievingthebestpatientoutcomes.112,121Patientsshouldbeabletomoveseamlesslybetweendifferentpartsofthesystemandbetweendifferentproviders,toensurethattheyreceivetimelyaccesstotheservicesrequired.112
WaitingtimesforspecialistservicesarenotconsistentacrosstheUK,withsomepatientshavingtowaitconsiderablylongerforspecialisttreatment.A2014reportbyHealthcareImprovementScotlandhighlightedsignificantvariationinwaitingtimesforspecialistservices,in-particularinaccesstopainpsychologyservices.122TheNationalPainAudit’sfinalreport–whichfocusedonEnglandandWales–suggestedthattheRCoA(RoyalCollegeofAnaesthetists)shouldadopttheIASPswaitingtimeguidanceforitsgoodpracticeguideforpainservices.Thisrecommendsthatpatientsshouldbeseenwithineightweeksforroutineorregulartreatment,onemonthforurgentorsemi-urgentcases,andoneweekforthemosturgent cases.20
Service provisionThereisavarietyofguidanceavailableontheprovisionofservices.SpecificguidanceonthecommissioningofchronicpainserviceshasbeenpublishedbytheRCGP,andendorsedbytheBPS,ChronicPainPolicyCoalitionandFPM.112Itexploreshowthecommissioningprocesscanbettersupportchronicpainpatientsandhowdoctorscanengagewithcommissionersmoreeffectively.Itskeypointsincludethat:
– painmanagementisbestdeliveredbymultidisciplinaryandmultiprofessionalteams; – thereshouldbeequityofprovisionacrosssocioeconomicscales,withservicesmeetingtheneedsoflocalpopulations;
– clinicalprofessionaladvicetocommissionersiskeytodeliveringthebestvalueservices – peopleshouldbeatthecentreofamulti-morbiditiesapproach,andinvolvedinservicedesignanddelivery.

18 British Medical Association Chronic pain: supporting safer prescribing of analgesics
TheFPMhavepublishedcorestandardsforpainmanagementservicesintheUK,whichareintendedtoprovideaclinicalguidelineandaframeworkforthoseplanningservices.113
Thesesetoutcorestandardsforpainmanagementservicesincommunity,secondarycare,andspecialistsettings.Theyhighlightthatspecialistpainmanagementservicesinthecommunityorsecondarycareshouldalwaysinvolveamultidisciplinaryteam,andthatamultidisciplinaryteammustinclude:
– medicalconsultants – nurses – physiotherapists – psychologists – pharmacists
Oftenthiswillalsoincludeoccupationaltherapists,andwhereavailable,suitablytrainedGPsaswellasSAS(specialtyandassociatespecialist)doctors.113 Thereneedtobecloseworkingrelationshipsinrelatedmedicaldisciplinesincludingorthopaedicsurgery,neurosurgery,neurologyandpsychiatry.
Somepainmanagementservicesholdcombinedpainandsubstancemisuseclinicswherepatientswhohavepainandwhoareusinghighdosesofprescribedopioidsorrecreationaldrugsandalcoholcanbeassessedandmanaged.
TheBPSguidelinesonpainmanagementprogrammesoutlinetheevidenceformultidisciplinaryservices,howpatientsshouldbereferredandtheresourcesthataserviceshouldhaveaccessto.Theyhighlighttheimportanceofpainmanagementprogrammesbeingproperlyresourcedwithadequatetime,personnelandfacilities,andrecognisetheneedtoimproveaccesstotheseprogrammestosupportearlyinterventionaswellascomprehensiverehabilitation.115TheBPShasalsodevelopeda‘commissioninghub’,whichisintendedtoprovideasourceofinformationondifferentservicemodels,commissioningissuesandoutcomesfromacrossthecountry.
Key messages – Painmanagementisbestdeliveredbymultidisciplinaryandmultiprofessionalteams. – ThereishighvariationinaccesstomultidisciplinarycareandwaitingtimesforspecialistpainservicesarenotconsistentacrosstheUK
4.1.5 Non-pharmacological interventions for chronic pain Non-pharmacologicaltreatmentmaybeeffectiveinreducinglong-termpainanddisabilityinsomepatientswithchronicpain.123Thesetreatmentoptionscanalsoaugmentandcomplementanalgesicuse.123Itisthereforeimportantthatpatientshaveaccessto,andopportunitytobenefitfrom,arangeofeffectivenon-pharmacologicaltreatmentoptionswhereappropriate.Non-pharmacologicalinterventionsforchronicpainincludepsychologicallybasedinterventions,suchasbehaviouraltherapies,aswellasphysicaltherapies.12 Thecorestandardsforpainmanagementservices,publishedbytheFPM,recommendthatpainmanagementprogrammesshouldutilisepharmacologicalandnon-pharmacologicaltreatmentoptions,andthatpatientswithchronicpainshouldhaveaccesstoclinicalpsychologyandspecialistphysiotherapyearlyintheirtreatmentpathway.115 As highlightedintheBPSguidelinesforpainmanagementprogrammes,thereisevidencefortheefficacyofcognitivebehaviouraltherapypainmanagementprogrammesinimprovingpainexperience,mood,coping,negativeoutlookonpain,andactivitylevels.115 Thoughthereremainsalackofstudiesassessingtheefficacyofpsychologicalapproachesforsometypesofpain.117 Furtherworkisalsorequiredtodeveloptheevidencebaseforinvasiveinterventionsinthetreatmentofchronicpain.124

19British Medical Association Chronic pain: supporting safer prescribing of analgesics
Recommendations: – Allrelevantcommissioningandproviderorganisations–includingCCGsinEngland,healthboardsinScotlandandWales,andtheHealthandSocialCareBoardinNorthernIreland–shouldensurethatmultidisciplinarypainmanagementservicesareavailableforpatientsintheirareaandthatthesearecommissionedaccordingtoavailableguidance.Theseorganisationsshouldalsoworktoensuretimelyaccesstopainmanagementprogrammes,tosupportearlyinterventionandcomprehensiverehabilitationforpatientswithchronicpain.
– Allhealthcareprovidersthatareresponsibleforthemanagementofpatientswithchronicpainshouldbefamiliarwiththerangeofnon-pharmacologicalinterventionsthatmaybeeffectiveforthemanagementofchronicpain–includingphysicalandpsychologicaltherapies.Healthcareprofessionalsshouldalsobeawareofthelocalavailabilityoftheseservices.

20 British Medical Association Chronic pain: supporting safer prescribing of analgesics
5 Role of training and education in improving analgesic use for treating chronic pain
Thefollowingsectionexplorestheroleoftrainingandeducationinsupportingimprovementsinanalgesicprescribing.Itparticularlyfocusesonthestepsrequiredtoensureallnon-specialistshavethebasicknowledgeandskillstosupporttheappropriatemanagementofpatientswithchronicpain.ForinformationAppendix 2 providesanoverviewofthetrainingpathwayforpainmedicinespecialistsintheUK.Thereisaneedtoensurethattraininginmedicalschools,aswellaspostgraduatetraining–bothingeneralpracticeandforsecondarycaredoctorswhoarenotspecialistsinpainmedicine–equipsclinicianswiththeknowledgeandskillstosupporttheappropriatemanagementofpatientswithchronicpain.Trainingontheprinciplesofpainmanagementshouldensureallclinicianswhoarenon-specialistsinpainmedicineare:
– awarethatitisoftenunlikelythatanalgesics,includingopioids,willcompletelyeliminatepainandthattheyarelikelytobeeffectiveinonlyaminorityofpatients;
– awarethataswellasbeingacomponentofotherconditions,chronicpainisalong termconditioninitsownright,andlikemanyotherlongtermconditionsitusually cannotbecured;
– abletoeffectivelymanagetheexpectationsthatpatientsmayhaveabouttheirtreatment,forinstance,withregardtothelikelihoodthattreatmentwillsuccessfullyreducetheirchronicpainandthedegreeofpainreductionitcanberealisticallyexpectedtoachieve;
– comfortablehighlightingthatthefocusoftreatmentislikelytobeonreducingratherthaneliminatingpain,andmaintainingfunction,withaviewtoimprovingqualityoflife;
– abletoaccessspecialistinputandadvicetosupporttheseconversationswithpatients.
Aswellasthesebasicprinciples,theroleofdoctorsinassistingthosewithchronicpaintomanagetheimpactoftheirconditionandliveindependentlyhasbeenspecificallyhighlightedasanareathatwouldbenefitfromimprovedtraining.TheChronicPainPolicyCoalitionhavesuggestedthathealthcareprofessionalsshouldbe‘trainedtoencouragepeoplelivingwithchronicpaintoparticipateineducationandpeersupportprogrammestoaidindependentliving’.108Healthcareprofessionalsshouldalsobecomfortableinprovidinginformationregardingsupportedself-managementofchronicpain.113
5.1 A focus on undergraduate training
In2008,theChiefMedicalOfficer’s150thannualreportrecommendedthattraininginchronicpainbeincludedinthecurriculaofallhealthcareprofessionals.8Itnotedatthetimethatteachingatundergraduatelevelwaspatchyandinconsistent.ResearchintotheprovisionofpaineducationinmedicalschoolsacrossEurope–basedoninformationonthecontentofcurriculain2013–foundthattherewerecompulsorydedicatedmodulesinpaininonly4%ofUKmedicalschools,andonly11%offeredcompulsoryorelectivemodules.125 FiftypercentofmedicalschoolsintheUKdocumentedpain-specifictopicswithintheircurricula,eitheraspartofcompulsorydedicatedpainmodules,orpainwithinothercompulsorymodules–thelowestlevelof15Europeancountries,althoughtheresearchersdidindicatethatthelevelofdetailavailablewastoovariabletoallowcomprehensiveanalysis.125AdvancingtheProvisionofPainEducationandLearning(APPEAL)–aEuropewidereviewofundergraduatepaineducation–calledonmedicalschools,painspecialists,medicalstudentsandpolicymakerstoensurethatundergraduatestudentsreceivepaineducationtoallowthemtoadequatelytreatpain,inlightoftherelativelylittlecoverageitreceivesatpresent.126
TheGMC’s(GeneralMedicalCouncil)Outcomes for graduatesincludestherequirementtobeabletoprescribedrugssafelyandeffectively,andtoplandrugtherapyforcommonindications,includingpain.127Itisimportantthatthereisclearguidanceontheknowledgeandskillsinpainmanagementthatstudentsshouldbeexpectedtoacquireoverthecourseoftheirundergraduatequalifications.Medicalschoolsshouldconsiderhowtoincorporate

21British Medical Association Chronic pain: supporting safer prescribing of analgesics
existingresourcesintotheirindividualcurricula.DespitetheproductionofpaincurriculabyIASP,128evidenceoftranslationintomoreeffectiveundergraduateeducationinpainislimited.
Arecentinternationalconsensushassetoutthecorecompetenciesinpainassessmentandmanagementthatshouldbeincludedinthecurriculaofallmedicalschoolsworldwide.129Thesecompetenciesareintendedtodriveimprovementsindeliveryofpaineducationandhelpshiftemphasistowardspainasadisease.Itisrecommendedthatthesecompetenciesareassessedwithintheexaminationprocessforgraduation.Inanotherinitiative,theFPMiscurrentlysupportingtheintroductionofapainmanagementcourse‘EssentialPainManagement-lite’tomedicalschools(seeBox 6)withemphasisondeliveryofpre-determinedpaincontent.TheFPMhasalsoproducedguidanceonthecompetenciesrequiredforarangeofpaininterventions,aswellasguidancespecifictothemanagementofpaediatricpain.130
Box 6 – Essential Pain Management (EPM-lite)
EPM-liteisascaleddownessentialpainmanagementcoursedesignedtobedeliveredtomedicalundergraduatesinhalfaday,withtheaimofexpandingthelevelofpainmanagementknowledgetaughtatundergraduatelevel.In2014,theFPMbeganaprojectofintroducingEPM-lite,andithasnowbeendeliveredinseveralUKmedicalschools.131
Recommendations: – Paincompetenciesshouldbeincludedinthecurriculaofallmedicalschoolsandbeassessedingraduationexaminations
– Medicalschoolsshouldensurethatexistingresources–suchastheIASP’scurriculumoutlineonpainandtheFPM’sEPM-liteprogramme–areusedeffectivelytoensuresufficienthighqualityundergraduateteachingonthebasicsofpainmanagement.
5.2 Promoting guidance to support improved analgesic prescribing for chronic pain
Topromotetheappropriatemanagementofchronicpain,renewedemphasisisrequiredontheutilisationofexistingguidance,andthedevelopmentoftoolstoassisthealthcareprofessionalswhenprescribinganalgesics.Aconsiderableamountofguidancehasalreadybeenproducedsettingouttherecommendedwaysofmanagingpainforpatientssufferingfromchronicpain(seeSection 3.2).Althoughawiderangeguidanceisavailabletosupportprescribing,thecontinuedincreaseinthelong-termuseofopioidstotreatchronicpain–despitethelackofevidenceoftheirlong-termeffectivenessinmostpatients–indicatesanongoingneedtopromotebestpractice,andtomonitorcloselycurrentprescribingtrends.
Recommendation: Existingguidanceonthemanagementofchronicpainandtheappropriateprescribingofanalgesicsneedstobepromoted,andconsiderationgivenhowitcanbemaximisedtosupportmoreappropriateuseofanalgesics,includingamongstclinicianswhoarenotspecialistsinpainmedicine.

22 British Medical Association Chronic pain: supporting safer prescribing of analgesics
6 Conclusion and summary of recommendations
Overrecentyearstherehasbeenasubstantialincreaseintheprescribingofopioids,leadingtosignificantpublichealthconcernsthattheharmsassociatedwiththesemedicationsareincreasing.Muchofthisincreasedprescribingislikelyassociatedwiththeiruseforthetreatmentofchronicpainbut,thereislimitedevidencetosupporttheirlong-termuseformostpatients.
Chronicpainisacomplexcondition,whichhasasubstantialimpactonthelivesofthoseaffected.Thereliefofpainshouldbeseenasaclinicalpriority,yettheprescribingofopioidsisoftennotthemostappropriateoreffectivetreatmentoptionformanypatientswithchronicpain,andcanriskexposingpatientstounnecessaryharm.Ifitisthoughtopioidtherapymayplayaroleinapatient’spainmanagement,atrialshouldbeinitiatedtoestablishwhetherapatientachievesareductioninpainwiththeuseofopioids–ifnottheyshouldbestopped.Patientsshouldbefullyinformedofpotentialbenefitsandharmsfromthistrial.Doseescalationshouldbelimitedasriskofharmrisesasdoseincreases,especiallyifthereisinadequatereliefofpain.Analgesicusebypatientswithchronicpainshouldbereviewedregularly.Bettersupportisrequiredforbothdoctorsandpatientsinstoppingopioidtreatmentwherethishasnotprovidedeffectivepainrelief.Adequateresourcesarerequiredtomoveawayfromprescribingasa‘default’option,towardsacomprehensive,multidisciplinaryapproachtothemanagementofchronicpain,whichisnowrecognisedasalong-termconditioninitsownright.Theneedtoavoidtreatmentsorproceduresthatareunlikelytobeofbenefithasbeenrecognisedacrossdifferentbranchesofmedicine,includingthroughthe‘choosingwisely’initiativefromtheAcademyofMedicalRoyalColleges.132
Supportingimprovementsinthetreatmentofchronicpain,andtheuseofanalgesics,necessitatesactionacrossarangeofareas,includingtheprovisionofservices;research;training;continuededucationandprofessionaldevelopment,andthedevelopmentandpromotionofguidance.Thisreportsetsoutarangeofrecommendationsforactionintheseareasthatneedtobetakenforwardbygovernments,policymakersandprofessionalsacrosstheUK.

23British Medical Association Chronic pain: supporting safer prescribing of analgesics
Summary of recommendations
Developing the evidence base – Tobetterinformclinicalpracticemoreresearchisrequiredintotheeffectsoflong-termprescribingofopioidsforpainrelief,includingtheirefficacy&safetyforperiodslongerthansixmonths.
Pain management – Considerationshouldbegiventotherangeofsupportthatisrequiredfordoctorsandpatientsduringtheprocessofassessment,trialandreviewofopioidtreatmentforchronicpain.Thisshouldincludesupportforstoppingopioidtreatmentthatisnotworking.
– Sufficientinvestmentandresourcesforprimarycare,includinglongerconsultationtimes,arerequiredtosupportimprovementsinanalgesicprescribingforpatientswithchronicpain.
– Allrelevantcommissioningandproviderorganisations–includingCCGsinEngland,healthboardsinScotlandandWales,andtheHealthandSocialCareBoardinNorthernIreland–shouldensurethatmultidisciplinarypainmanagementservicesareavailableforpatientsintheirareaandthatthesearecommissionedaccordingtoavailableguidance.Theseorganisationsshouldalsoworktoensuretimelyaccesstopainmanagementprogrammes,tosupportearlyinterventionandcomprehensiverehabilitationforpatientswithchronicpain.
– Allhealthcareprovidersthatareresponsibleforthemanagementofpatientswithchronicpainshouldbefamiliarwiththerangeofnon-pharmacologicalinterventionsthatmaybeeffectiveforthemanagementofchronicpain-includingphysicalandpsychologicaltherapies.Healthcareprofessionalsshouldalsobeawareofthelocalavailabilityoftheseservices.
Training and education – Paincompetenciesshouldbeincludedinthecurriculaofallmedicalschoolsandbeassessedingraduationexaminations.
– Medicalschoolsshouldensurethatexistingresources–suchastheIASP’scurriculumoutlineonpainandtheFPM’sEPM-liteprogramme–areusedeffectivelytoensuresufficienthighqualityundergraduateteachingonthebasicsofpainmanagement.
– Existingguidanceonthemanagementofchronicpainandtheappropriateprescribingofanalgesicsneedstobepromoted,andconsiderationgivenhowitcanbemaximisedtosupportmoreappropriateuseofanalgesics,includingamongstclinicianswhoarenotspecialistsinpainmedicine.

24 British Medical Association Chronic pain: supporting safer prescribing of analgesics
7 Further resources
Please note: this listing of publications is intended for further information only. The BMA is not responsible for the content or accuracy of external websites, nor does it endorse or otherwise guarantee the veracity of statements made in non-BMA publications.
Supporting individuals affected by prescribed drugs associated with dependence and withdrawal – BritishMedicalAssociationAvailableat: https://www.bma.org.uk/collective-voice/policy-and-research/public-and-population-health/prescribed-drugs-dependence-and-withdrawal
Opioids Aware: A resource for patients and healthcare professionals to support prescribing of opioid medicines for pain–HostedbytheFacultyofPainMedicineAvailableat:https://www.fpm.ac.uk/faculty-of-pain-medicine/opioids-aware
Core Standards for Pain Management Services in the UK–FacultyofPainMedicineAvailableat:http://www.rcoa.ac.uk/system/files/FPM-CSPMS-UK2015.pdf
The hidden suffering of chronic pain–TheChronicPainPolicyCoalitionAvailableat:http://www.policyconnect.org.uk/cppc/research/hidden-suffering-chronic-pain-booklet-parliamentarians
Pain Management Services: Planning for the future: Guiding clinicians in their engagement with commissioners – RoyalCollegeofGeneralPractitioners Available at: http://www.rcoa.ac.uk/system/files/FPM-Pain-Management-Services.pdf
National Pain Audit Final Report 2010-2012(EnglandandWales)Availableat:http://www.nationalpainaudit.org/media/files/NationalPainAudit-2012.pdf
Guidance on the management of pain in older people (2013) – BritishGeriatricsSocietyAvailableat:http://www.bgs.org.uk/pdfs/pain/age_ageing_pain_supplement.pdf

25British Medical Association Chronic pain: supporting safer prescribing of analgesics
Appendix1–classificationofchronicpain
ThebelowtablehighlightstheclassificationsofchronicpainthathavebeendevelopedbytheIASPforinclusioninthe11threvisionoftheWHOInternationalClassificationofDiseases.
ClassificationofchronicpainforICD-11
ThecurrentversionoftheWHO’sInternational Classification of Diseases(ICD-10) includesdiagnosticcategoriesforchronicpainconditions.Forthe11threvisionoftheICDataskforceledbytheIASPhasdevelopedanewclassificationofchronicpain,dividedintothefollowingsevengroups.
1. Chronic primary pain –Chronicprimarypainispainin1ormoreanatomicregionsthatpersistsorrecursforlongerthan3monthsandisassociatedwithsignificantemotionaldistressorsignificantfunctionaldisability(interferencewithactivitiesofdailylifeandparticipationinsocialroles)andthatcannotbebetterexplained byanotherchronicpaincondition.
2. Chronic cancer pain – Chroniccancerpainincludespaincausedbythecanceritself(theprimarytumorormetastases)andpainthatiscausedbythecancertreatment(surgical,chemotherapy,radiotherapy,andothers).
3. Chronic post-surgical and post-traumatic pain – Painthatdevelopsafterasurgicalprocedureoratissueinjury(involvinganytrauma,includingburns)andpersistsatleast3monthsaftersurgeryortissuetrauma.
4. Chronic neuropathic pain –Chronicneuropathicpainiscausedbyalesionordiseaseofthesomatosensorynervoussystem.
5. Chronic headache and orofacial pain – Chronicheadacheandchronicorofacialpainisdefinedasheadachesororofacialpainsthatoccuronatleast50%ofthedaysduringatleast3months.
6. Chronic visceral pain – Chronicvisceralpainispersistentorrecurrentpainthatoriginatesfromtheinternalorgansoftheheadandneckregionandthethoracic,abdominal,andpelviccavities
7. Chronic musculoskeletal pain – Chronicmusculoskeletalpainisdefinedaspersistentorrecurrentpainthatarisesaspartofadiseaseprocessdirectlyaffectingbone(s),joint(s),muscle(s),orrelatedsofttissue(s).
Source:TreedeRD,RiefW,BarkeA(2015)AclassificationofchronicpainforICD-11.Pain 156(6):1003–1007

26 British Medical Association Chronic pain: supporting safer prescribing of analgesics
Appendix 2 – specialist training in pain medicine
TheFPMistheprofessionalbodyresponsibleforthetraining,assessment,practiceandcontinuingprofessionaldevelopmentofpainmedicinespecialistsintheUK. Itdescribestheroleofpainmedicinephysiciansasundertaking“[…] the comprehensive assessment and management of patients with acute, chronic and cancer pain using pharmacological, interventional, physical and psychological techniques in a multidisciplinary setting.”
Traineeanaesthetiststhatwishtospecialiseinpainmedicinemustundertake 12monthsormoreofadvancedpaintrainingindesignatedspecialistcentres.Successfulcompletionofthistraining,alongsidecontinuousassessmentandpassingoftheFPMexaminationleadstotheawardofFFPMRCA(FellowshipoftheFacultyofPainMedicineoftheRoyalCollegeofAnaesthetists)ortheDiploma(DFPMRCA)forthosetraineeswhohaveaqualificationthatisequivalenttoFRCA.133,134

27British Medical Association Chronic pain: supporting safer prescribing of analgesics
Acknowledgements
Editorial boardBoard of science chair ProfessorParveenKumarPolicy director RajJethwaHead of public health and healthcare LenaLevyHead of science and public health GeorgeRoycroftResearch and writing RobertWilson ThomasAndrews
Board of science ThisreportwaspreparedundertheauspicesoftheBMAboardofscience,whosemembershipfor2016-17wasasfollows:Professor Pali Hungin PresidentDrMarkPorter CouncilchairDrDavidWrigley CouncildeputychairDrAndrewDearden TreasurerDrAntheaMowat Representativebodychair
ProfessorParveenKumar BoardofsciencechairDrPaulDarragh BoardofsciencedeputychairDrJSBamrahProfessorPeterDangerfieldDrShreelataDattaDrKittyMohanMrRamMoorthyDrMelodyRedmanProfessorMichaelRees(deputymember)DrPenelopeToffDr Ian Wilson
JacquelineAdams(BMAPatientliaisongrouprepresentative)DrIainThomasRobertKennedy(BMApublichealthmedicinecommitteerepresentative)
TheAssociationisgratefulforthehelpprovidedbytheBMAcommitteesandoutsideexperts.Wewouldparticularlyliketothank:
– DrBeverlyCollettOBE(FacultyofPainMedicine) – DrCathyStannard(FacultyofPainMedicine) – DrPaulWilkinson(FacultyofPainMedicine) – ProfessorAndrewRice(ImperialCollegeLondon) – ProfessorRogerKnaggs(UniversityofNottingham) – DrMartinJohnson

28 British Medical Association Chronic pain: supporting safer prescribing of analgesics
References
1 KristianssonMH,BrorssonA,WachtlerCetal(2011)Pain,powerandpatience– Anarrativestudyofgeneralpractitioners’relationswithchronicpainpatients. BMC Family Practice 12:31
2 BritishMedicalAssociation(2015)Prescribed drugs associated with dependence and withrawl – building a consensus for action: Analysis report.London:BritishMedicalAssociation
3 StannardC(2013)OpioidsintheUK:What’stheproblem?BMJ 347:f5108
4 www.rcpsych.ac.uk/pdf/FPM-Opioids-Aware-Press-Release.pdf
5 www.isdscotland.org/Health-Topics/Prescribing-and-medicines/Community-Dispensing/Prescription-Cost-Analysis
6 http://www.iasp-pain.org/Taxonomy
7 VOS,Tetal.2015.Global,regional,andnationalincidence,prevalence,andyearslivedwithdisabilityfor301acuteandchronicdiseasesandinjuriesin188countries,1990–2013:asystematicanalysisfortheGlobalBurdenofDiseaseStudy2013.TheLancet,386,743-800.
8 DepartmentofHealth(2009)On the State of Public Health: Annual Report of the Chief Medical Officer 2008.DepartmentofHealth:London.
9 www.hscic.gov.uk
10 WorldHealthOrganization(2015)International Statistical Classification of Diseases and Related Health Problems 10th Revision.Availableatwww.who.int/classifications/icd/en/
11 BritishPainSociety(2010)Opioids for persistent pain. London:BritishPainSociety.Availableonlineat:www.britishpainsociety.org/static/uploads/resources/files/book_opioid_patient.pdf
12 SIGN(2013)Sign 136 – Management of Chronic Pain. Availableatwww.sign.ac.uk/pdf/SIGN136.pdf
13 TreedeRD,RiefW,BArkeA(2015)AclassificationofchronicpainforICD-11.Pain 156(6):1003–1007
14 https://www.rcoa.ac.uk/faculty-of-pain-medicine/opioids-aware/condition-patient-context/about-pain
15 HauserW,KossevaM,UceylerNetal(2011)Emotional,PhysicalandSexualAbuseinFibromyalgiaSyndrome:Asystematicreviewwithmeta-analysis.ArthritisCareandResearch63(6):808-820
16 HoweC,RobinsonJ,SullivanM(2015)Psychiatricandpsychologicalperspectivesonchronicpain. Phys Med Rehabil Clin N Am26(2):283-300
17 HauserW,KossevaM,UceylerNetal(2011)Emotional,PhysicalandSexualAbuseinFibromyalgiaSyndrome:Asystematicreviewwithmeta-analysis.ArthritisCareandResearch63(6):808-820
18 HoweC,RobinsonJ,SullivanM(2015)Psychiatricandpsychologicalperspectivesonchronicpain. Phys Med Rehabil Clin N Am26(2):283-300
19 BreivikH,CollettB,VentafriddaV(2006)SurveyofchronicpaininEurope:prevalence,impactondailylife,andtreatment.European Journal of Pain 10(4):287-333
20 NationalPainAudit(2012)Final report of the National Pain Audit 2010-2012.Availableat:www.nationalpainaudit.org/
21 FayazA,CroftP,LangfordRMetal(2016)PrevalenceofchronicpainintheUK:asystematicreviewandmeta-analysisofpopulationstudies.BMJ Open 6 e010364

29British Medical Association Chronic pain: supporting safer prescribing of analgesics
22 www.hscic.gov.uk
23 SaastamoinenP,Leino-ArjasP,LaaksonenMetal(2005)Socio-economicdifferencesintheprevalenceofacute,chronicanddisablingchronicpainamongageingemployees.Pain 114(3):364-371.
24 SmithM,DavisM,StanoMetal(2013)AgingBabyBoomersandtheRisingCostofChronicBackPain:SecularTrendAnalysisofLongitudinalMedicalExpendituresPanelSurveyDataforYears2000to2007. Journal of Manipulative and Physiological Therapeutics 36(1):2-11.
25 BreivikH,CollettB&VentafriddaV(2006)SurveyofchronicpaininEurope:prevalence,impactondailylife,andtreatment.European Journal of Pain 10(4):287-333.
26 OfficeforNationalStatistics(2015)Ageing of the UK population.Availableat:http://www.ons.gov.uk/ons/rel/pop-estimate/population-estimates-for-uk--england-and-wales--scotland-and-northern-ireland/mid-2014/sty-ageing-of-the-uk-population.html
27 VacantiC,SegalS,SikkaPetal(2011)Essential Clinical Anesthesia. Cambridge:CambridgeUniversityPress
28 SinatraRS,JahrJS&Watkins-PitchfordJ(2010)The Essence of Analgesia and Analgesics. Cambridge:CambridgeUniversityPress.
29 ZinCS,ChenL-C,KnaggsRD(2014)Changesintrendsandpatternofstrongopioidprescribinginprimarycare.EuropeanJournalofPain18(9):1343–1351
30 NationalTreatmentAgencyforSubstanceMisuse(2006)Addiction to medicine. Availabeat:www.nta.nhs.uk/uploads/addictiontomedicinesmay2011a.pdf
31 HealthandSocialCareInformationCentre(2010)Prescription cost analysis.Leeds:HealthandSocialCareInformationCentre.Availableat:http://www.hscic.gov.uk/catalogue/PUB02274/pres-cost-anal-eng-2010-rep.pdf
32 HealthandSocialCareInformationCentre(2014)Prescription cost analysis.Leeds:HealthandSocialCareInformationCentreAvailableonlineat:http://www.hscic.gov.uk/catalogue/PUB17274/pres-cost-anal-eng-2014-rep.pdf
33 ISDScotland,Prescriptioncostanalysis,Datatables–PrescribingandMedicines,Availableat:www.isdscotland.org/Health-Topics/Prescribing-and-medicines/Publications/data-tables.asp?id=939
34 HSCBusinessServicesOrganisation,PharmaceuticalStatisticsAvailableat:www.hscbusiness.hscni.net/services/1806.htm
35 LoftusH(2014)Potentialmisuseofpregabalinandgabapentin.British Medical Journal 348:g1290.
36 SpenceD(2013)Badmedicine:gabapentinandpregabalin.British Medical Journal 347:f6747.
37 PublicHealthEnglandandNHSEngland(2014)Advice for prescribers on the risk of the misuse of pregabalin and gabapentin.Availableat:www.gov.uk/government/publications/pregabalin-and-gabapentin-advice-for-prescribers-on-the-risk-of-misuse
38 NorthernIrelandAuditOffice(2014)Primary care prescribing: Report to the Northern Ireland Assembly by the Comptroller and Auditor GeneralAvailableat:www.niauditoffice.gov.uk/prescribing_-_media_release_12_november.pdf
39 HealthandSocialCareBoard(2015)Advice for prescribers on the risk of misuse of pregabalin and gabapentin.Availableat:niformulary.hscni.net/Formulary/Adult/PDF/PregabalinAndGabapentinRiskOfMisuseAdviceHSCBWebVersion.pdf
40 JackA(2015)Pfizerstepsupbattletodefendcontrolofpregabalin.British Medical Journal 350:h3119.

30 British Medical Association Chronic pain: supporting safer prescribing of analgesics
41 SpenceR,RobertsA,AritiCetal(2014)Focus on: Antidepressant prescribing.TheHealthFoundationandtheNuffieldTrust.Availableonlineat:www.health.org.uk/sites/default/files/QualityWatch_FocusOnAndidepressantPrescribing.pdf
42 WelshGovernment,Prescriptionsdispensedinthecommunity.Availableat:gov.wales/statistics-and-research/prescriptions-dispensed-community/?lang=en
43 http://digital.nhs.uk/article/2021/
44 https://www.rcoa.ac.uk/faculty-of-pain-medicine/opioids-aware
45 FinnerupNB,SindrupSH&JensenTS(2010)Theevidenceforpharmacologicaltreatmentofneuropathicpain.Pain 150:573-81.
46 FinnerupNB,AttalN,HaroutounianSetal(2015)Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis.TheLancetNeurology14(2):162-73
47 HollingsheadJ,DühmkeRM&CornblathDR(2006)Tramadolforneuropathicpain. Cochrane Database of Systematic Reviews 3: CD003726.
48 FreynhagenR&BennettMI(2009)Diagnosisandmanagementofneuropathicpain. British Medical Journal 339:b3002.
49 EisenbergE,McNicolE&CarrDB(2006)Opioidsforneuropathicpain. Cochrane Database of Systematic Reviews.8: CD006146.
50 NüeschE,RutjesAW,HusniEetal(2009)Oralortransdermalopioidsforosteoarthritisofthekneeorhip. Cochrane Database of Systematic Reviews 4:CD003115.
51 GaskellH,DerryS,StannardCetal(2016)Oxycodoneforneuropathicpaininadults.Cochrane database of systematic reviews 7:CD010692
52 DerryS,StannardC,ColePetal(2016)Fentanylforneuropathicpaininadults.Cochrane database of systematic reviews 10:CD011605
53 ChouR,TurnerJA,DevineEBetal(2015) Theeffectivenessandrisksoflong-term
opioidtherapyforchronicpain:Asystematicreviewforanationalinstitutesof
healthpathwaystopreventionworkshop.Annals of Internal Medicine 162:276
54 HaueserW,BernardyK,Maier(2015)Long-termopioidtherapyinchronicnoncancerpain.Der Schmerz 29(1):96-108
55 CampbellG,NielsenS,BrunoRetal(2015)ThePainandOpioidsINTreatmentstudy:characteristicsofacohortusingopioidstomanagechronicnon-cancerpain.Pain 156(2):231-42
56 RowbothamMC,GilronI,GlazerCetal(2013)Canpragmatictrialshelpusbetterunderstandchronicpainandimprovetreatment?Pain 154(5):643-6
57 MooreRA,DerryS&WiffenPJ(2013)Challengesindesignandinterpretationofchronicpaintrials.British Journal of Anaesthesia 111(1):38-45.
58 ChouR,FanciulloGJ,FinePGetal(2009)ClinicalGuidelinesfortheUseofChronicOpioidTherapyinChronicNoncancerPain.Journal of Pain 10(2):113-130.
59 NationalInstituteforHealthandCareExcellence(2015)Neuropathic pain – drug treatment. Availableatcks.nice.org.uk/neuropathic-pain-drug-treatment#!supportingevidence1
60 BalantyneJC,KalsoE,StannardC(2016)WHOanalgesicladder:Agoodconceptgoneastray.BMJ352:i20
61 www.rcoa.ac.uk/faculty-of-pain-medicine/opioids-aware
62 NationalInstituteforHealthandCareExcellence(2013)Neuropathic pain – pharmacological management. Availableonlineatguidance.nice.org.uk/cg173

31British Medical Association Chronic pain: supporting safer prescribing of analgesics
63 MooreRA,WiffenPJ,DerrySetal(2014)Gabapentinforchronicneuropathicpainandfibromyalgiainadults.The Cochrane Database of Systematic Reviews 4:CD007938.
64 MooreRA.StraubeS,WiffenPJetal(2009)Pregabalinforacuteandchronicpaininadults. Cochrane Database of Systematic Reviews 3:CD007076.
65 SaartoT,WiffenPJ(2007)Antidepressantsforneuropathicpain.Cochrane Database of Systematic Reviews CD005454
66 MooreRA,DerryS,AldingtonDetal(2015)Amitriptylineforneuropathicpaininadults. Cochrane Database of Systematic Reviews 7: CD008242
67 EbertMH&KernsRD(2011)Behavioral and Psychopharmacologic Pain Management. Cambridge: CambridgeUniversityPress
68 LunnMPT,HughesRAC&WiffenPJ(2009)Duloxetinefortreatingpainfulneuropathyorchronicpain.Cochrane Database of Systematic Reviews 4: CD007115
69 HauserW,WolfeF,TolleTetal(2012)Theroleofantidepressantsinthemanagementoffibromyalgiasyndrome:asystematicreviewandmeta-analysis.CNS Drugs 6(4):297-307
70 MooreR,ChiC,WiffenPJetal(2015)Oralnonsteroidalanti-inflammatorydrugs(NSAIDs)forneuropathicpaininadults.Cochrane Database of Systematic Reviews 10:CD010902
71 EnthovenWT,RoelofsPD,DeyoRA(2016)Non-steroidalanti-inflammatorydrugsforchroniclowbackpain.Cochrane Database of Systematic Reviews CD012087
72 DerryS,MooreAR,RabbieR(2012)TopicalNSAIDsforchronicmusculoskeletalpainin adults. Cochrane Database of Systematic Reviews CD007400
73 http://www.cdc.gov/drugoverdose/data/prescribing.html
74 http://www.cdc.gov/drugoverdose/data/overdose.html
75 KingNB,FraserV,BoikosCetal(2014)Determinantsofincreasedopioid-relatedmortalityintheUnitedStatesandCanada,1990–2013:asystematicreview.American Journal of Public Health 104(8):e32-e42.
76 ManchikantiL,HelmS,FellowsBetal(2012)OpioidEpidemicintheUnitedStates.Pain Physician 15 (Suppl3):ES9-ES38
77 WeisbergD,StannardCFLostintranslation?LearningfromtheopioidepidemicintheUSA(invitededitorial)Anaesthesia2013;68:1207-1219
78 WeisbergD,BeckerW,FiellinDandStannardCPrescriptionopioidmisuseintheUSAandUK:CautionarylessonsInternational Journal ofJ Drug Policy2014;25:1124-1130
79 GiraudonI,LowitzK,DarganPetal(2013)PrescriptionopioidabuseintheUK.British Journal of Clinical Pharmacology 76(5):823-824.
80 OfficeforNatibonalStatistics(2010) Statistical bulletin: Deaths related to drug poisoning in England and Wales.Cardiff:OfficeforNationalStatistics
81 OfficeforNationalStatistics(2016)Statistical bulletin: Deaths Related to Drug Poisoning in England and Wales: 2015 registrations. Cardiff:OfficeforNationalStatistics
82 TheMisuseofDrugsandMisuseofDrugs(SafeCustody)(Amendment)(England,WalesandScotland)Regulations2014.Availableat:http://www.legislation.gov.uk/uksi/2014/
83 NorthernIrelandStatisticsandResearchAgency,Alcohol and Drug Deaths.Availableat:www.nisra.gov.uk/demography/default.asp30.htm
84 PattinsonK.T(2008)Opioidsandthecontrolofrespiration. British Journal of Anaesthesia 6:747-758.

32 British Medical Association Chronic pain: supporting safer prescribing of analgesics
85 RoseAR,CatchesidePG, McEvoyRD(2014)SleepDisorderedBreathingandChronicRespiratoryFailureinPatientswithChronicPainonLongTermOpioidTherapy.Journal of Clinical Sleep Medicine. 10(8):847–852
86 SeyfriedO,HesterJ(2012)Opioidsandendocrinedysfunction. British Journal of Pain 6(1):17–24
87 Al-HashimiM,ScottSWM,ThompsonJP(2013)Opioidsandimmunemodulation:morequestionsthananswers.British Journal of Anaesthesia 111(1):80-88.
88 AngstMS,ClarkJD(2006)Opioid-inducedHyperalgesia:AQualitativeSystematicReview.Anesthesiology 104(3):570-87
89 https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/491854/ACMD_Advice_-_Pregabalin_and_gabapentin.pdf
90 OfficeforNationalStatistics(2014)DeathsRelatedtoDrugPoisoninginEnglandandWales,2013.Availableonlineat:www.ons.gov.uk/ons/dcp171778_375498.pdf
91 https://www.evidence.nhs.uk/formulary/bnf
92 LeoRJ,BarkinRL(2003)AntidepressantUseinChronicPainManagement:IsThereEvidenceofaRoleforDuloxetine?Primary Care Companion to The Journal of Clinical Psychiatry 5(3)118-123.
93 https://www.evidence.nhs.uk/formulary/bnf/current/4-central-nervous-system/43-antidepressant-drugs/433-selective-serotonin-re-uptake-inhibitors
94 FavaGA,GattiA,BelaiseCetal(2015)WithdrawalSymptomsafterSelectiveSerotoninReuptakeInhibitorDiscontinuation:ASystematicReview.Psychotherapy and psychosomatics 84(2):72-81
95 NationalInstituteforHealthandCareExcellence(2015)Clinical Knowledge Summary: NSAIDs – prescribing issues.Availableat:https://cks.nice.org.uk/nsaids-prescribing-issues#!scenario
96 LyapustinaT&AlexanderG(2015)Theprescriptionopioidaddictionandabuseepidemic:howithappenedandwhatwecandoaboutit.The Pharmaceutical Journal 294 (7866).
97 RosenblumA,MarschL,JosephHetal(2008)OpioidsandtheTreatmentofChronicPain:Controversies,CurrentStatusandFutureDirections.Experimental and Clinical Psychopharmacology 16(5):405-416.
98 PortenoyRK,FoleyKM(1986)Chronicuseofopioidanalgesicsinnon-malignantpain:Reportof38cases.Pain 25:171–186.
99 MelzackR(1990)Thetragedyofneedlesspain.Scientific American 262:27–33
100 HutchinsonK,MorelandAME,WilliamsCdCAetal(2007)Exploringbeliefsandpracticeofopioidprescribingforpersistentnon-cancerpainbygeneralpractitioners.European Journal of Pain 11:93-98.
101 McCrackenL,VellemanS,EcclestonC(2008)Patternsofprescriptionandconcernaboutopioidanalgesicsforchronicnon-malignantpainingeneralpractice.Primary Health Care Research & Development 9:146–156
102 SeamarkD,SeamarkC,GreavesCetal(2013)GPsprescribingofstrongopioiddrugsforpatientswithchronicnon-cancerpain:aqualitativestudy.British Journal of General Practice 63(617): e821-e828.
103 McCrorieC,ClossSJ,HouseAetal(2015)Understandinglong-termopioidprescribingfornon-cancerpaininprimarycare:aqualitativestudyBMC Family Practice. 16:121
104 SIGN(2013)Managementofchronicpain:Pathwayforusingstrongopioidsinpatientswithchronicpain.Availableonlineat:www.ckp.scot.nhs.uk/Published/PathwayViewer.aspx?id=608

33British Medical Association Chronic pain: supporting safer prescribing of analgesics
105 MooreA,DerryS,EcclestonC&KalsoE(2013)Expectanalgesicfailure:pursueanalgesic success. BMJ 346:f2690.
106 http://www.rcgp.org.uk/clinical-and-research/clinical-resources/chronic-pain.aspx
107 SmithB(2002)Chronicpain:AprimarycareconditioninAdebajoA&DicksonD(eds)(2005)Collected Reports on the Rheumatic Diseases 2005.Availableonlineat:www.arthritisresearchuk.org/~/media/Files/Education/Hands-On/IP09-Sep-2002.ashx
108 ChronicPainPolicyCoalition(2015)The hidden suffering of chronic pain.London:ChronicPainPolicyCoalition.
109 BritishMedicalAssociation(2015)Responsive, safe and sustainable: towards a new future for general practice.London:BritishMedicalAssociation
110 BruhnH,BondCM,ElliottAMetal(2013)Pharmacist-ledmanagementofchronicpaininprimarycare:resultsfromarandomisedcontrolledexploratorytrial.BMJ Open 3(4)e002361
111 NeilsonAR,BruhnH,BondCMetal(2015)Pharmacist-ledmanagementofchronicpaininprimarycare:costsandbenefitsinapilotrandomisedcontrolledtrial.BMJ Open 5(4)e006874
112 RoyalCollegeofGeneralPractitioners(2014)Pain Management Services: Planning for the Future.London:RoyalCollegeofGeneralPractitioners
113 RoyalCollegeofAnaesthetists(2015)Core standards for pain management services in the UK.London:RoyalCollegeofAnaesthetists
114 FacultyofPainMedicine(2014)HealthEducationEnglandCallforEvidence: FacultyofPainMedicineSubmission.London:FacultyofPainMedicine.Availableat: http://www.fpm.ac.uk/system/files/FPM-HEE-Call-for-Evidence-submission.pdf
115 BritishPainSociety(2013)Guidelines for Pain Management Programmes for adults. London:BritishPainSociety.
116 WilliamsACdeC,EcclestonC&MorleyS(2012)Psychologicaltherapiesforthemanagementofchronicpain(excludingheadache)inadults.Cochrane Database of Systematic Reviews CD007407.
117 EcclestonC,HearnL&WilliamsACdeC(2015)Psychologicaltherapiesforthemanagementofchronicneuropathicpaininadults.Cochrane Database of Systematic Reviews CD011259
118 LewisS,BellD&GillandersD(2007)Managingchronicpaininpeoplewithlearningdisabilities:acasestudy.British Journal of Learning Disabilities 35(2):93-98.
119 BenjaminS,MorrisS,McBethJetal(2000)Theassociationbetweenchronicwidespreadpainandmentaldisorder:Apopulation-basedstudy.Arthritis and Rheumatology 43(3):561-567.
120 CPPCpressrelease(9.12.14)CPPC Releases Freedom of Information data on commissioning.Availableonlineat:www.policyconnect.org.uk/cppc/news/cppc-releases-freedom-information-data-commissioning
121 RowbothamDJ&CollettBJ(2014)Guidelines for the provision of anaesthetic services: Anaesthesia services for chronic pain management 2014.London:RoyalCollegeofAnaesthetists
122 HealthcareImprovementScotland(2014)Chronic pain services in Scotland: where are we now? Edinburgh:HealthcareImprovementScotland
123 ChangKL,FillingimR,HurleyRW(2015)Chronicpainmanagement:nonpharmacologicaltherapiesforchronicpain.FP Essentials 432:21-6.
124 DworkinRH,O’ConnorAB,KentJetal(2013)Interventionalmanagementofneuropathicpain:NeuPSIGrecommendations.Pain 154(11):2249-61

34 British Medical Association Chronic pain: supporting safer prescribing of analgesics
125 BriggsEV,BattelliD,GordonDetal(2015)CurrentpaineducationwithinundergraduatemedicalstudiesacrossEurope:AdvancingtheProvisionofPainEducationandLearning(APPEAL)study.BMJ Open 5:e006984.
126 APPEAL–AdvancingtheProvisionofPainEducationandLearning.Availableonlineat:www.efic.org/index.asp?sub=lWaAG1sc58KESH
127 GMC(2015)Outcomes for graduates.London:GMC.Availableonlineat:www.gmc-uk.org/static/documents/content/Outcomes_for_graduates_Jul_15.pdf
128 IASP(2012)IASP Curricula. Availableonlineat:www.iasp-pain.org/Education/CurriculaList.aspx?navItemNumber=647
129 FishmanSM,YoungHM,ArwoodELetal(2013)Corecompetenciesforpainmanagement:Resultsofaninterprofessionalconsensussummit.Pain Medicine 14(7):971–981
130 FacultyofPainMedicine:Guidance on competencies for Paediatric Pain Medicine. Availableat:https://www.rcoa.ac.uk/system/files/FPM-GuidancePPM.pdf
131 http://www.rcoa.ac.uk/faculty-of-pain-medicine/essential-pain-management/epm-lite
132 http://www.aomrc.org.uk/quality-policy-delivery/healthcare-policy/choosing-wisely/
133 https://www.rcoa.ac.uk/faculty-of-pain-medicine/
134 FacultyofPainMedicineoftheRoyalCollegeofAnesthetists.What is a pain medicine doctor?London:FacultyofPainMedicine.Availableat:https://www.rcoa.ac.uk/system/files/FPM-What-is-Pain-Doctor.pdf

British Medical AssociationBMAHouse,TavistockSquare,LondonWC1H9JPbma.org.uk
©BritishMedicalAssociation,2017BMA20170191