chronic renal failure: what the primary … annual conference/saturday/primary care.pdfchronic...
TRANSCRIPT

CHRONIC RENAL FAILURE: WHAT THE PRIMARY CARE CAN OFFER
The annual conference of the Lebanese Society
of Family Medicine
October 2017
Dr Hiba AZAR

OUTLINE: A journey through CKD
Screening for CKD: The why, the who and the how
Slowing the progression of CKD
Management of complications of CKD: the anemia, the hyperkalemia and the CKD-MBD

Screening for CKD: The why
• CKD is a silent disease.
• CKD is a leading cause of mortality, primarily via in increase in cardiovascular mortality.
• Progression of CKD can be slowed.

Screening for CKD: The who
• Not for everybody
• Population at risk:
▪ Diabetes.
▪ Hypertension.
▪ Systemic diseases, autoimmune diseases.
▪ Family history of kidney disease.
▪ Certain ethnicities.
▪ Recurrent kidney stones and UTIs.

Screening for CKD: The who

Screening for CKD: The how
• DO NOT rely on creatinine alone. Always use calculators of eGFR, CKD-Epi or MDRD.

Screening for CKD: The how
18 years old male.
Creatnine1.2 mg/dl
CKD EPI= 88 ml/min
85 years old lady
Creatinine1.2 mg/dl
CKD EPI= 41ml/min

Screening for CKD: The how
• DO NOT ask for microalbuminuria alone in the urine spot

Screening for CKD: The how
Microalbuminuria40 mg/dl
Microalbuminuria40 mg/dl
Creatininuria1,3 g/dl
Creatininuria0.3 g/dl
UAER= 30 mg/g UAER= 133 mg/g

Screening for CKD: The how
• Creatinine for calculation of eGFR.
• UAER.
• General exam of the urine.
• Renal ultrasound.

Screening for CKD: The how

Slowing the progression of CKD

Slowing the progression of CKD
Chronic kidney disease and cardiovascular risk:epidemiology, mechanisms, and prevention. Lancet 2013
Very strong correlation between CKD , microalbuminuria and CVD mortality.
CKD doubles the risk of heart failure.
Increase in the risk of stroke, atrial fibrillation, coronary heart disease, peripheral artery disease irrespective of age and ethnicity.

Slowing the progression of CKD
• In patients with mild to moderate CKD, the risk of cardiovascular mortality is much higher than the risk of reaching end stage kidney disease.
• Only in stage 4 CKD, the risk of end stage kidney disease surpasses the risk of CV mortality.
Chronic kidney disease and cardiovascular risk:epidemiology, mechanisms, and prevention. Lancet 2013


Slowing the progression of CKD
• Lifestyle modifications
• Therapeutic interventions

Slowing the progression of CKD- lifestyle modifications
Smoking cessation Decreases CV mortality in general population. Tobacco use is associated with progression of CKD. Cessation effect not documented
Dietary counseling: Na< 2g/day Enhances effect of ACEi and ARBs on the proteinuria reduction and decrease the progression of CKD
Dietary counseling: Protein intake 0.8 g/kg/day
Protein intake more than 1.3 g/kg/day should be avoided
Reduction of BMI to 25 kg/m2
Regular physical exercise, 30 min five times weekly
Associated with reduction of cardiovascular mortality of 13%
ACP clinical practice guidelines 2013

Slowing the progression of CKD-therapeutic interventions
BP reduction to < 140/90 mm Hg for CKD patients and lower if proteinuria
Adjust according to age, comorbidities, progression of CKD, tolerance
Use of RAAS inhibitors Reduction in albuminuria, positivelyaffects renal prognosis (beware SI, high K)
No room for associating ACEi and ARB
Glycemic control Aim for an HbA1c of 7 or less unlessadvanced CKD, comorbidities and high risk of hypoglycemia
Lipid control Statins. Decrease of CV risk, no cleareffect on renal progression. Adjust dose of fibrates.
Antiplatelet therapy No specific recommandations
Uric acid lowering treatment No specific guidelines if asymptomatic
ACP clinical practice guidelines 2013

Management of complications of CKD-The anemia
The incidence of anemia increases with
the severity of kidney disease

Management of complications of CKD-The anemia
• Manifestations: fatigue, decreased tolerance to effort, cold intolerance, general malaise, irritability.
• Normocytic, normochromic anemia.
• Due to the decrease in EPO production by kidney.
• Iron deficiency is frequent: decreased oral intake, increased loss, decreased absorption, inflammation and increased demand with ESA therapy.
• Iron stores should be regularly checked and repleted in CKD patients, before starting and during treatment with EPO.

Management of complications of CKD-The anemia
CKD w/o anemia
eGFR>45 ml/min
Once yearly
eGFR< 45 ml/min
Twice yearly
CKD/anemia w/o ESA
eGFR>45 ml/min
Twice yearly
eGFR< 45 ml/min
Every 3 Months
CKD/anemia with ESA
Every 2 to four weeks at initiation
Then every 3 months
Suggested scheme for monitoring for anemia by KDIGO
KDIGO guidelines Kidney International 2012

Management of complications of CKD-The anemia
Guidelines for iron therapy in CKD patients

Management of complications of CKD-The anemia
• KDIGO guidelines for the management of anemia
✓ESA should be started after repletion of iron stores if Hb level is lower than 10g/dl.
✓Aim for a Hb level between 11 and 12g/dl.
✓Hb should not increase by more than 1-1.5 g/dl every month.
✓Hb above 12 g/dl under ESA therapy is associated with increased risk of stroke and worsening hypertension
KDIGO guidelines Kidney International 2012

Management of complications of CKD-The hyperkalemia
• Hyperkalemia is a common clinical problem in CKD patients.
• Particularly in diabetics and with the use of RAAS inhibitors.
Kovesdy CP, Am J Med 128:1281–1287, 2015

Management of complications of CKD-The hyperkalemia
Murray et al KI 2016

Management of complications of CKD-The hyperkalemia
• Diet.
• Use of diuretics. Correct metabolic acidosis.
• Avoid use of other drugs affect K levels.
• Sodium polystyrene sulfonate: a lot of controversies about efficacy and safety. Mostly used in the acute setting. Contraindicated if ileus, postoperative setting, opioids... Risk of colonic necrosis

Management of complications of CKD-The hyperkalemia
• Patiromer: recently approved by FDA for use in acute and chronic hyperkalemia. Nonabsorbal polymer that exchanges potassium for calcium. Decreases safely K by 0.5-1 Meq/l. GI side effects. Interaction with other medications... Effect of calcium load in CKD patients?
• Zirconium cyclosilicate: ZS 9. Exchanges K for Na and hydrogen. Decreases K by 0.5-1 mEg/l. SI: edema. Not yet approved by FDA.

Management of complications of CKD-The hyperkalemia

Management of complications of CKD-The CKD-MBD
www.kdigo.org
CalciumPhosphorusPTHVitamin DFGF23
Renal osteodystrphyAdynamicbone diseaseosteomalacia

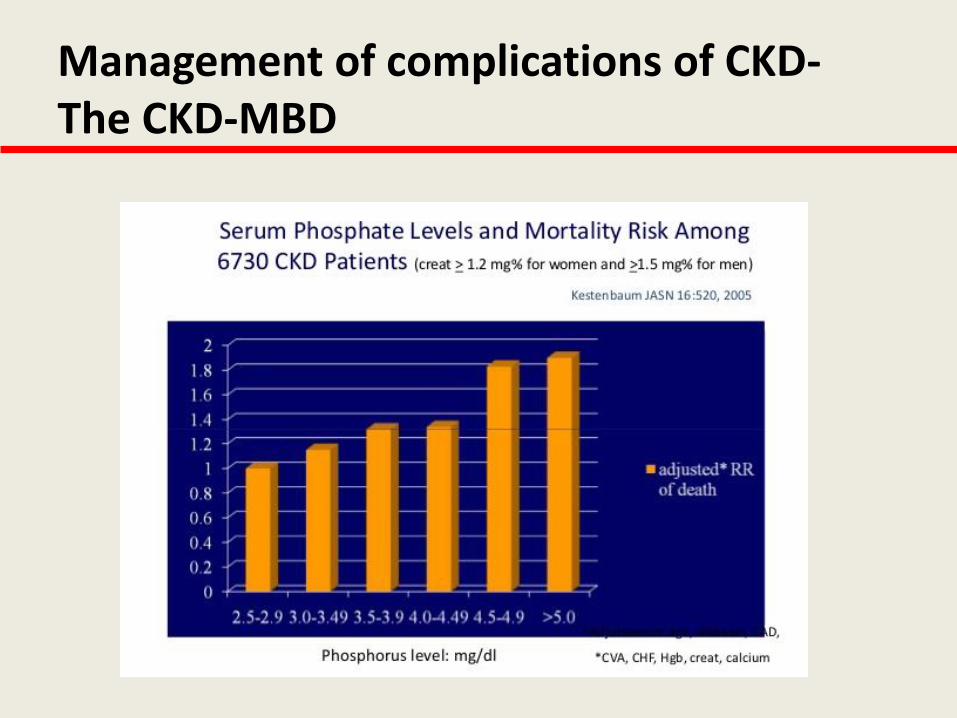
Management of complications of CKD-The CKD-MBD
Prevalence of abnormal mineral metabolism in CKD
Levin et al KI 2007; 71:31-38
Management of complications of CKD-The CKD-MBD
Management of complications of CKD-The CKD-MBD

Management of complications of CKD-The CKD-MBD
Dg of biochemical abnormalities

Management of complications of CKD-The CKD-MBD
Dg of biochemical abnormalities

Management of complications of CKD-The CKD-MBD
Dg bone disease

Management of complications of CKD-The CKD-MBD
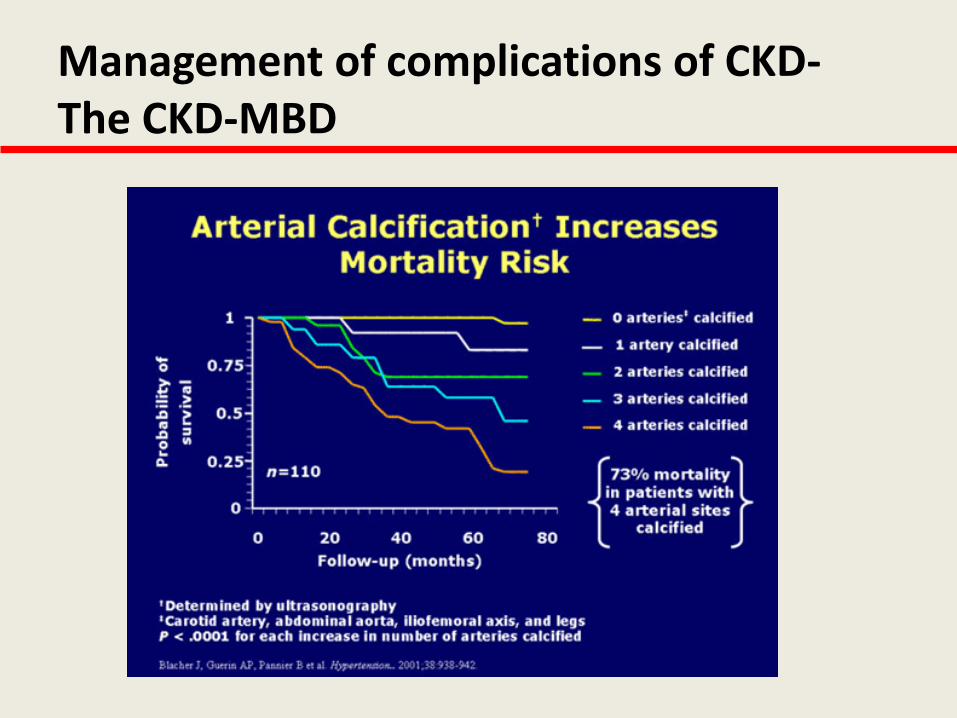
Dg of vascular calcifications

Management of complications of CKD-The CKD-MBD
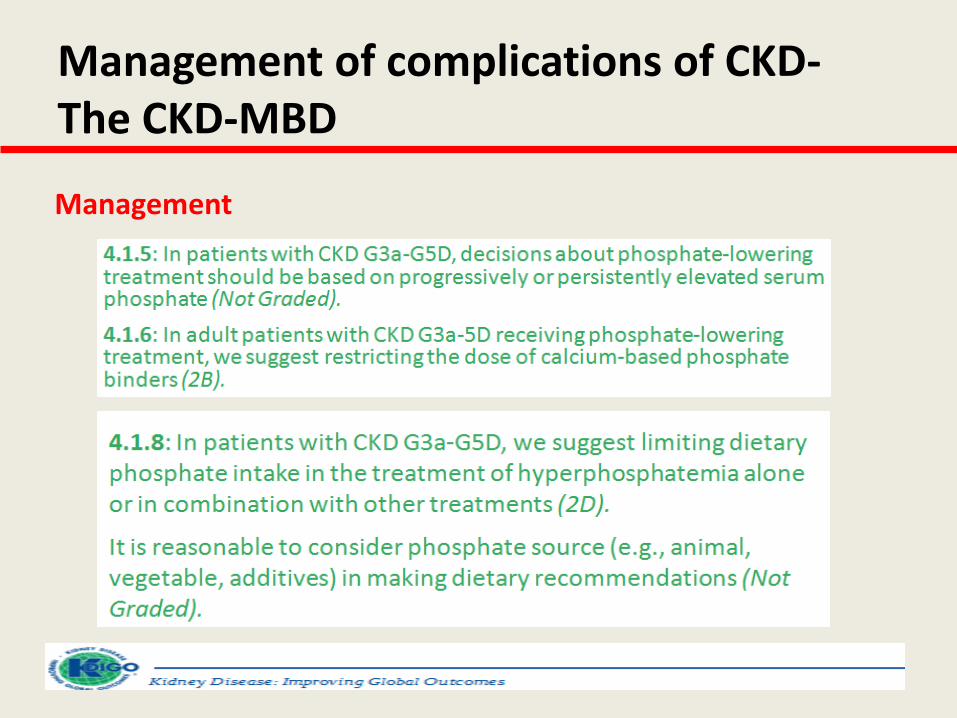
Management
Management of complications of CKD-The CKD-MBD
Management

Management of complications of CKD-The CKD-MBD

Thank you for your attention