cihs' standard framework for levels of integrated · pdf filea review and proposed...
TRANSCRIPT

A STANDARD FRAMEWORK FOR LEvELS OF
INTEGRATED HEALTHCARE AND UPDATE
THROUGHOUT THE DOCUMENT
mARcH 2013
Acknowledgements
A Review and Proposed Standard Framework for Levels of Integrated Healthcare was developed for the SAMHSA-HRSA Center for
Integrated Health Solutions with funds under grant number 1UR1SMO60319-01 from SAMHSA-HRSA US Department of Health
and Human Services The statements findings conclusions and recommendation are those of the author(s) and do not necessarshy
ily reflect the view of SAMHSA HRSA or the US Department of Health and Human Services
Special thanks to Bern Heath Jr PhD CEO Axis Health System Kathy Reynolds MSW ACSW Vice President of Health Integration
and Wellness Promotion National Council for Community Behavioral Healthcare and Pam Wise Romero PhD Chief Clinical Officer
Axis Health Systems and for authoring this document
sAmHsA-HRsA centeR FoR IntegRAted HeAltH solUtIons
The SAMHSA-HRSA Center for Integrated Health Solutions (CIHS) promotes the development of integrated primary and behavioshy
ral health services to better address the needs of individuals with mental health and substance use conditions whether seen in
specialty behavioral health or primary care provider settings CIHS is the first ldquonational homerdquo for information experts and other
resources dedicated to bidirectional integration of behavioral health and primary care
Jointly funded by the HHSSubstance Abuse and Mental Health Services Administration and the Health Resources and Services
Administration and run by the National Council for Community Behavioral Healthcare CIHS provides training and technical assisshy
tance to community behavioral health organizations that received Primary and Behavioral Health Care Integration grants as well
as to community health centers and other primary care and behavioral health organizations
CIHSrsquos wide array of training and technical assistance helps improve the effectiveness efficiency and sustainability of integrated
services which ultimately improves the health and wellness of individuals living with behavioral health disorders
1701 K Street NW Suite 400
Washington DC 20006
2026847457
integrationtheNationalCouncilorg
wwwintegrationsamhsagov
This document is in the public domain and may be used and reprinted without permission except those copyrighted materials noted for which further reproduction is prohibited without the specific permission of copyright holders
SuggeSted Citation Heath B Wise Romero P and Reynolds K A Review and Proposed Standard Framework for Levels of Integrated Healthcare Washington DCSAMHSA-HRSA Center for Integrated Health Solutions March 2013
Ac
kn
ow
le
dg
em
en
ts
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS 2
3 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
aBStRaCt Integration of healthcare is essential to improve the individualrsquos experience of care improve the health of the general
population and reduce per capita healthcare costs The term ldquointegrationrdquo is widely and inconsistently used to describe the bringshy
ing together of healthcare components Integration has been used to reference everything from consultation to colocation to a
setting of shared health values around treating the whole person with blurred professional boundaries There have been no fully
updated taxonomies to describe the levels of integration since the 1996 Doherty McDaniel and Baird article which initially proshy
posed five levels of integration Since this seminal issue brief and preliminary framework there have been many informal and local
adaptations However without a standard classification of integrated settings discussions of integration lack clarity and precision
and research cannot confidently examine discrete aspects of integration This issue brief reviews levels of integrated healthcare
and proposes a functional standard framework for classifying sites according to these levels
KeY WoRdS integration collaborative care mental health behavioral health collaboration healthcare
BAckgRoUnd Over the last several years as healthcare reform has taken a prominent national position and mental health and substance abuse
treatments have evolved an increasing number of articles have been written on collaboration and the integration of traditional
primary care and behavioral health practices (Butler Kane amp McAlpine 2008 Collins Hewson Munger amp Wade 2010 Funk
amp Ivbijaro 2008 Lopez Coleman-Beattie amp Sanchez 2008 Mauer 2006 2009 Mauer amp Jarvis 2010 Miller Kessler amp Peek
2011 Robinson amp Reiter 2007 Russell 2010) These articles have described a wide variety of collaborative co-located and
integrated service models
Developing a standard framework to describe integrated efforts is critical for meaningful dialogue about service design as well as
for research Until there is a way to reliably categorize integration implementations meaningful comparisons of implementations
or associated health outcomes cannot occur This point is made throughout the Miller et al 2011 paper which calls for a broader
ldquolexicon for the common terms and components for collaborative care so that research questions can be framed in a consistently
understood mannerrdquo (p 2) On the clinical side integrated care developers and implementers will benefit from recognizing the
characteristics of practice change that support evolving integration models Knowing what features of integrated healthcare impleshy
mentations lead to the most favorable and stable health outcomes will be an important contribution to the health field
A standard framework also contributes to the orderly evolution of national healthcare reform and aligns with the political and
service realities defined by Berwick Nolan and Whittington (2008) Integration is essential to achieving the triple aim of improved
experience of care improved health of populations and reduced per capita healthcare cost advocated by Berwick et al The lesshy
sons learned from a reliable comparison of models and implementations provide the best foundation to inform policy decisions on
the structure of more effective healthcare as care integration moves forward
levels oF IntegRAtIon Doherty McDaniel and Baird (1995 1996) proposed the first classification by level of Until there is a way to reliably collaboration and integration They proposed the five levels of primary care-behavioral
healthcare collaboration recognizing that collaboration and integration of care were categorize integration evolving and being communicated in wide-ranging ways Doherty et alrsquos classification
implementations meaningfulinvolved both the extent of the occurrence of collaboration and the capacity for colshy
laboration in the setting but they did not focus on specific interactions An underlying comparisons of implementationspremise of the levels was that as collaboration increased the adequate handling of
complex patients would also increase The levels recognized by Doherty et al did not or associated health outcomes prescribe a particular model as best for all healthcare settings but rather served as
a foundation from which to tease apart the strengths and limitations of a variety of cannot occur
sA
mH
sA
-HR
sA
ce
nt
eR
Fo
R I
nt
eg
RA
te
d H
eA
ltH
so
lU
tIo
ns
This issue brief uses the term behavioral health to describe mental health and substance use
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
options It was proposed that use of the levels would help organizations evaluate their setting in light of their goals for collaboration
and to assist in researching outcomes and costs associated with different collaborative models with different patient populations
In the original framework Doherty et al differentiated levels by where they were practiced the cases adequately handled at each
level and the following descriptions
8 LeveL 1ndash Minimal Collaboration Mental health and other healthcare providers work in separate facilities have separate
systems and rarely communicate about cases
8 LeveL 2 ndash Basic Collaboration at a Distance Providers have separate systems at separate sites but engage in periodic
communication about shared patients mostly through telephone and letters Providers view each other as resources
8 LeveL 3 ndash Basic Collaboration Onsite Mental health and other healthcare professionals have separate systems but share
facilities Proximity supports at least occasional face-to- face meetings and communication improves and is more regular
8 LeveL 4 ndash Close Collaboration in a Partly Integrated System Mental health and other healthcare providers share the same
sites and have some systems in common such as scheduling or charting There are regular face-to-face interactions among
primary care and behavioral health providers coordinated treatment plans for difficult patients and a basic understanding
of each otherrsquos roles and cultures
8 LeveL 5 ndash Close Collaboration in a Fully Integrated System Mental health and other healthcare professionals share the
same sites vision and systems All providers are on the same team and have developed an in-depth understanding of
each otherrsquos roles and areas of expertise
The following chart summarizes these five levels of collaboration
MINIMAL COLLAbORATION
bASIC COLLAbORATION
FROM A DISTANCE
bASIC COLLAbORATION
ONSITE
CLOSE COLLAbORATION
PARTLy INTEGRATED
FULLy INTEGRATED
8 Separate systems
8 Separate facilities
8 Communication is
8 Separate systems
8 Separate facilities
8 Periodic focused
8 Separate systems
8 Same facilities
8 Regular rare
8 Little appreciation of each otherrsquos culture
ldquoNobody knows my name Who are yourdquo
communication most written
8 View each other as outside resources
8 Little understandshying of each otherrsquos culture or sharing of influence
ldquoI help your consumersrdquo
communication occasionally face-to-face
8 Some appreciation of each otherrsquos role and general sense of large picture
8Mental health usually has more influence
ldquoI am your consultantrdquo
8Some shared systems
8Same facilities
8Face-to-Face consultation coordinated treatment plans
8Basic appreciation of each otherrsquos role and cultures
8Collaborative routines difficult time and operation barriers
8Influence sharing
ldquoWe are a team in the care of consumersrdquo
8Shared systems and facilities in seamless bio-psychosocial web
8Consumers and providers have same expectations of system(s)
8In-depth appreciation of roles and culture
8Collaborative routines are regular and smooth
8Conscious influence sharing based on situation and expertise
ldquoTogether we teach others how to be a team in care of conshysumers and design a care systemrdquo
4
5 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
These five levels have formed the foundation for most subsequent level adaptations The idea that integration occurs along a
continuum of collaboration and integration is widely supported (Collins et al 2010 Miller et al 2011 Peek 2007 Reynolds
2006 Seaburn Lorenz Gunn Gawinski amp Mauksch 1996 Strohsal 1998) and adaptations have differed in the number of levels
(from three to 10) and the categories used to differentiate or describe levels
The reason for classification whether for clinical development or research
has influenced the choice of dimensions used to define each level For
example Reynolds (2006) used the same five levels but distinguishes
between levels on the basis of functional practice categories including
access services funding governance evidence-based practice and
data usage The goal of Reynoldsrsquo adaptation is to better capture the pashy
tient and staff experience at the different levels in doing so it broadens
the levelsrsquo descriptions and characteristics
Other papers and reports have classified integrated implementations
somewhat differently MaineHealth (2009) developed a site-specific ratshy
ing of integration that has four levels along a continuum of integration
with one rating in the first level and three ratings in levels two three and four There are 18 characteristics broadly categorized
as integrated services patient- and family-centeredness and practiceorganization In the first category characteristics such as
colocation patientfamily involvement and communication with patients about integrated care are rated In the second category
characteristics such as organizational leadership for integrated care providersrsquo engagement and data systemspatient are rated
More similar to Doherty et al Blount (2003) collapsed the five levels to three coordinated co-located and integrated care Reshy
cent work to develop a lexicon or common conceptual system for collaborative care between behavioral health and primary medical
clinicians (Miller et al 2011) has also adopted these three levels in describing collaborative care practice
The Milbank report Evolving Models of Behavioral Health Integration in Primary Care (Collins et al 2010) describes eight models
of integration across a variety of settings This group uses Doherty et alrsquos five level structure and the terms coordinated co-
located and integrated to differentiate these models
PRoPosed stAndARd FRAmewoRk Doherty et al established the five levels of integration recognizing differences in integrated implementations and the various forms
collaboration took in each level Based upon the initial efforts by Doherty et al and the experience accumulated over the intervenshy
ing 17 years the authors of this paper propose a new version of the levels of collaborationintegration The proposed framework
brings together valuable aspects that have evolved since the Doherty et al paper The proposed framework also includes several
enhancements that enable it to be comprehensive enough to serve as a national standard for future discussion about integrated
healthcare allow organizations implementing integration to gauge their degree of integration against acknowledged benchmarks
and serve as a foundation for comparing healthcare outcomes between integration levels
Doherty et al established the concept of levels of implementations that followed a continuum from collaboration to integration The
proposed model in this issue brief retains some of the original categorical descriptions that continue to prove useful today Blountrsquos
use of coordination colocation and integration serve as overarching categories The Milbank report which brought together
Doherty et alrsquos five levels and Blountrsquos broader categories also informs this conceptual framework
This new level of integration framework proposes six levels of collaborationintegration While the overarching framework has three
main categories mdash coordinated co-located and integrated care mdash there are two levels of degree within each category (see Table
1) It is designed to help organizations implementing integration to evaluate their degree of integration across several levels and to
determine what next steps they may want to take to enhance their integration initiatives
Coordinated Care
8 LeveL 1 mdash Minimal Collaboration
Behavioral health and primary care providers work at separate facilities and have separate systems Providers communicate
rarely about cases When communication occurs it is usually based on a particular providerrsquos need for specific information
about a mutual patient
8 LeveL 2 mdash Basic Collaboration at a Distance
Behavioral health and primary care providers maintain separate facilities and separate systems Providers view each other
as resources and communicate periodically about shared patients These communications are typically driven by specific
issues For example a primary care physician may request copy of a psychiatric evaluation to know if there is a confirmed
psychiatric diagnosis Behavioral health is most often viewed as specialty care
Co-Located Care
8 LeveL 3 mdash Basic Collaboration Onsite
Behavioral health and primary care providers co-located in the same facility but may or may not share the same practice
space Providers still use separate systems but communication becomes more regular due to close proximity especially
by phone or email with an occasional meeting to discuss shared patients Movement of patients between practices is
most often through a referral process that has a higher likelihood of success because the practices are in the same locashy
tion Providers may feel like they are part of a larger team but the team and how it operates are not clearly defined leaving
most decisions about patient care to be done independently by individual providers
8 LeveL 4 mdash Close Collaboration with Some System Integration
There is closer collaboration among primary care and behavioral healthcare providers due to colocation in the same
practice space and there is the beginning of integration in care through some shared systems A typical model may
involve a primary care setting embedding a behavioral health provider In an embedded practice the primary care front
desk schedules all appointments and the behavioral health provider has access and enters notes in the medical record
Often complex patients with multiple healthcare issues drive the need for consultation which is done through personal
communication As professionals have more opportunity to share patients they have a better basic understanding of each
otherrsquos roles
Integrated Care
8 LeveL 5 mdash Close Collaboration Approaching an Integrated Practice
There are high levels of collaboration and integration between behavioral and primary care providers The providers begin
to function as a true team with frequent personal communication The team actively seeks system solutions as they recogshy
nize barriers to care integration for a broader range of patients However some issues like the availability of an integrated
medical record may not be readily resolved Providers understand the different roles team members need to play and they
have started to change their practice and the structure of care to better achieve patient goals
8 LeveL 6 mdash Full Collaboration in a TransformedMerged Practice
The highest level of integration involves the greatest amount of practice change Fuller collaboration between providers
has allowed antecedent system cultures (whether from two separate systems or from one evolving system) to blur into a
single transformed or merged practice Providers and patients view the operation as a single health system treating the
whole person The principle of treating the whole person is applied to all patients not just targeted groups
Key elements were added to more clearly differentiate between the levels in each overarching category For coordinated care
the key element is communication The distinction between Level 1 and Level 2 is frequency and type of communication With inshy
creased communication providers have stronger relationships and greater understanding of the importance of integrated care and
sA
mH
sA
-HR
sA
ce
nt
eR
Fo
R I
nt
eg
RA
te
d H
eA
ltH
so
lU
tIo
ns
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS 6
7 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
the skills that different providers possess This communication increases
the coordination of care between separate healthcare entities
Physical proximity is the key element for the co-located care category
Although colocation does not guarantee greater collaboration or integrashy
tion it can be beneficial Taking advantage of close proximity increases
collaboration through face-to-face contact at Level 3 It can also develop
the opportunity for trust and relationship building leading to more sharing
of systems mdash the hallmark of beginning integration at Level 4 However
providers can be co-located and have no integration of their healthcare
services Each provider can still practice independently without commushy
nicating with others and with an integrated healthcare plan Colocation
reduces time spent travelling from one practitioner to another but does not guarantee integration
At Level 5 and Level 6 practice change is the key element No site can be fully integrated without changing how both behavioral
health and primary care are practiced The requisite practice change features a blending or blurring of cultures where no one disshy
cipline predominates Across many integrated implementations at several levels almost every practitioner wants integrated care
and believes it is the direction for healthcare to move towards until they realize it requires they change how they practice It is at
that point they often try to change the concepts of their integration efforts to preserve how they currently practice
A second modification proposed to the original Doherty et al structure is the use of the terms ldquocollaborationrdquo and ldquointegrationrdquo In
this framework collaboration describes how resources mdash namely the healthcare professionals mdash are brought together integration
describes how services are delivered and practices are organized and managed This idea is similar to Strosahlrsquos (1998) concept
that collaborative care involves behavioral health working with primary care while integration is behavioral health working within
and as part of primary care Recent analysis (Mauer amp Jarvis 2010) indicates that collaboration and integration can effectively
originate in either behavioral health or primary care and requires the transformation of both into a single whole In this standard
framework both collaboration and integration (beginning at Level 3) increase in degree and complexity over the continuum for
providers while similarly decreasing for clientsindividuals
An important enhancement to the levels is also found in a restructuring of the descriptive characteristics defining each level (see
Table 1) Each of the six levels begins with a general description followed by key differentiators (see Table 2A and 2B) under the
headings clinical delivery patient experience practiceorganization and business model These characteristics help differentiate
the levels They also incorporate some of the functional categories Reynolds (2006) identified in her consumerstaff experiential
perspective of the levels of integration Kodnerrsquos (2009) integrated care domains and MaineHealthrsquos (2009) Site Assessment
Finally Table 3 describes the strengths and weaknesses of each level so that these can be built upon or addressed
Although the term behavioral health has been used throughout this proposed framework integration of substance use treatment
and primary care has not been as extensive or prevalent as integration of mental health with primary care Further work is required
to more effectively support substance use integration (Butler et al 2008 Mauer 2010)
It is worth noting that even if health outcomes improve as levels of integration increase it is not reasonable to believe that all
healthcare settings would be able to easily or even with difficulty move to increasing levels of integration As primary care and
behavioral health have evolved in their own professional silos it has been the authorsrsquo experience that the bringing together of
these services and service perspectives (usually embodied in separate agencies) into a single fully integrated healthcare system
requires a large amount of administrative political and financial investments over a long-term stepwise evolutionary process It
is important to aspire to whichever level can be best achieved practically
At Level 3 colocation may be a necessary and good starting point to build trust between separate existing systems and to estabshy
lish a shared history of improved outcomes This could lead to closer collaboration and integration of vision that moves to Level
4 implementation possibly leading from there to a Level 5 partnership Such a partnership may be the highest level attainable or
may in years to come lead to a joint venture or a merger of the organizations While this has not been fully researched merging
primary and behavioral health organizations appears necessary at this point for achieving Level 6 integration
8 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
From a data standpoint this framework also posits that integrated services should be defined by location not by an algorithm of
service code combinations A single service (eg blood pressure check or depression medication check) provided in an integrated
sitesetting is considered an integrated service because it is provided in the context of that integrated sitersquos whole person care
Conversely multiple services provided in a single visit are not by definition integrated care these services could be and all too
often are provided by separate professionals without meaningful collaboration or integration By defining the level of integration
in terms of setting the authors of this framework define the context of interventions and the values (eg care team whole health
patient-centered) that form the basis of an integrated site and integrated services The key performance indicators in an integrated
care setting are population-based health status outcomes not encounter-based processservice data Individual staff productivity
must accompany and then be replaced by population-based outcomes by site
Funding structures and accountability must also change Integrated care is not supported by fee-for-service funding structures
that stumble over same day billing restrictions and do not reimburse for consultations between providers when the patient is not
physically present or electronic contacts or a large volume of care management mdash all of which are essential for improved health
outcomes in an integrated healthcare system Fee-for-service funding can emphasize the measurement of volume rather than
quality Global or blended funding structures do support integrated healthcare and will be fiscally justified by improved patient
outcomes that reduce overall healthcare cost
conclUsIon The proposed level of integration framework is a manageable practical and conceptually sound six level framework for integrated
healthcare that begins with collaboration (how resources are brought together) and moves through colocation and increasing levels
of integration (how services are framed and delivered) This standard framework is needed for clarity and precision of communicashy
tion as well as to contribute to research and practice redesign By implication the numbering of levels suggests that the higher
the level of collaborationintegration the more potential for positive impact on health outcomes and patient experience This belief
remains a hypothesis and has not been empirically tested With further research these benefits of collaborationintegration can
be more firmly stated and can identify which aspects of the collaboration integration or combination of the two contribute most
directly to health outcomes
Even if health outcomes improve as levels of integration increase it is not practical to believe that every healthcare setting will be
able at least in the near term to implement increasing levels of integration Many integrated implementations will be constrained
by community politics trust between organizational systems financing andor differing service values
Lastly this issue brief does not presume to establish a fuller lexicon for integration and healthcare as much needed as it is The
authors leave that to others better suited to the task and hope that this paper will contribute to such a lexicon The purpose is
to help those delivering services today by presenting a conceptual framework to better understand and differentiate integrated
healthcare implementations The authors believe that this framework will inform discussions about integrated healthcare and that
its use will provide opportunity for service redesign that will lead to better conceptual and practical models of care
9 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
ReFeRences
Berwick DM Nolan TW amp Whittington J (2008) The triple aim Care health and cost Health Affairs 27(3) 759-769
Blount A (2003) Integrated primary care Organizing the evidence Families Systems amp Health 21 (2) 121-33 doi 1010371091shy75272121121
Blount A (Ed) (1998) Integrated primary care The future of medical and mental health collaboration New York Norton
Butler M Kane RL McAlpine D et al Integration of Mental HealthSubstance Abuse and Primary Care No 173 (Prepared by the Minnesota Evidence-based Practice Center under Contract No 290-02-0009) AHRQ Publication No 09-E003 Rockville MD Agency for Healthcare Research and Quality October 2008
Collins C Hewson DL Munger R amp Wade T (2010) Evolving models of behavioral health Integration in primary care Report commissioned by the Milbank Memorial Fund
Doherty W (1995) The whyrsquos and levels of collaborative family health care Family Systems Medicine 13(3-4) 275-81 doi101037h0089174
Doherty WJ McDaniel SH amp Baird MA (1996) Five levels of primary carebehavioral healthcare collaboration Behavioral Healthcare Tomorrow 25-28
Funk M and G Ivbijaro eds (2008) Integrating mental health into primary care ndash A global perspective Geneva Switzerland World Health Organization and London UK World Organization of Family Doctors Available at wwwwhointmental_healthpolicyMental20health20+20primary20care-20final20low-res20140908pdf
Kodner Dennis (2009) All together now A conceptual exploration of integrated care Healthcare Quarterly 13 (Sp) 6-15
Lopez M B Coleman-Beattie L Jahnke and K Sanchez (2008) Connecting body and mind A resource guide to integrated health care in Texas and the United States Austin TX Hogg Foundation for Mental Health
Mauer B (2006) Behavioral healthprimary care integration The four quadrant model and evidence-based practices Rockville MD National Council for Community Behavioral Healthcare
Mauer B (2009) Behavioral healthprimary care integration and the person-centered healthcare home Washington DC National Council for Community Behavioral Healthcare
Mauer B (2010) Substance use disorders and the person-centered healthcare home Rockville MD National Council for Community Behavioral Healthcare
Mauer B amp Jarvis D (2010) The business case for bidirectional integrated care Mental health and substance use services in primary care settings and primary care services in specialty mental health and substance use settings Integration Policy Initiative
Maine Health Access Foundation (2009) Site Self-Assessment
Miller BF Kessler R Peek CJ (2011) A national agenda for research in collaborative care Papers from the Collaborative Care Research Network Research Development Conference AHRQ Publication No 11-0067 Rockville MD Agency for Healthcare Research and Quality
Peek CJ (2007) Integrated Care Aids to Navigation Study packet for the Pennsylvania Eastern Ohio amp West Virginia Summit Integrating Mental Health and Primary Care Pittsburgh PA
Reynolds K (2006) Mental Health Primary Care Integration Options (Unpublished document)
Robinson PJ amp Reiter JT (2007) Behavioral consultation and primary care A guide to integrating services New York Springer
Russell L (2010) Mental health care services in primary care Tackling the issues in the context of health care reform Center for American Progress Washington DC
Seaburn Lorenz Gunn Gawinksi amp Mauksch (1996) Models of collaboration A guide for mental health professionals working with health care practitioners Basic Books
Strosahl K (1998) Integrating behavioral health and primary care services The primary mental health care model In Integrated primary care The future of medical and mental health collaboration edited by A Blount pp 139-66 New York WW Norton
Strosahl K amp Robinson P (2008) The primary care behavioral health model Applications to prevention acute care and chronic condition management In R Kessler amp D Strafford (Eds) Collaborative medicine case studies Evidence in practice New York Springer
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 1
Six
Lev
els
of C
olla
bo
ratio
nIn
tegr
atio
n (C
ore
Des
crip
tions
)
CO
OR
DIN
AT
ED
KE
y E
LEM
EN
T C
OM
MU
NIC
AT
ION
CO
LO
CA
TE
D
KE
y E
LEM
EN
T P
Hy
SIC
AL
PR
Ox
IMIT
y
INT
EG
RA
TE
D
KE
y E
LEM
EN
T P
RA
CT
ICE
CH
AN
GE
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
beh
avio
ral h
ealt
h p
rim
ary
care
an
d o
ther
hea
lth
care
pro
vid
ers
wo
rk
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
Com
mun
icat
e ab
out c
ases
on
ly ra
rely
and
und
erco
mpe
lling
circ
umst
ance
s
8 8 C
omm
unic
ate
driv
en b
y pr
ovid
er n
eed
8 M
ay n
ever
mee
t in
pers
on
8 H
ave
limite
d un
ders
tand
shyin
g of
eac
h ot
herrsquos
role
s
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
8Co
mm
unic
ate
perio
dica
llyab
out s
hare
d pa
tient
s
8 C
omm
unic
ate
driv
en b
y sp
ecifi
c pa
tient
issu
es
8 M
ay m
eet a
s pa
rt of
larg
er
com
mun
ity
8Ap
prec
iate
eac
h ot
herrsquos
ro
les
as re
sour
ces
secfi t f
o oy
n eti amli s c ya il ey
e f ar h
m ss e t
a e r
n s ece hI n w 8
Hav
e se
para
te s
yste
ms
8 C
omm
unic
ate
regu
larly
ab
out s
hare
d pa
tient
s b
y ph
one
or e
-mai
l
8 C
olla
bora
te d
riven
by
need
for e
ach
othe
rrsquos
serv
ices
and
mor
e re
liabl
e re
ferra
l
8M
eet o
ccas
iona
lly to
disc
uss
case
s du
e to
clo
sepr
oxim
ity
8 F
eel p
art o
f a la
rger
yet
no
n-fo
rmal
team
e h ey
n t h
ih e t
rti ee
w hc wya tp il
e s ica
ma e f
n s maI s 8
Sha
re s
ome
syst
ems
like
sc
hedu
ling
or m
edic
alre
cord
s
8Co
mm
unic
ate
in p
erso
nas
nee
ded
8 C
olla
bora
te d
riven
by
need
for c
onsu
ltatio
n an
dco
ordi
nate
d pl
ans
for
diffi
cult
patie
nts
8 H
ave
regu
lar f
ace-
to-fa
ce
inte
ract
ions
abo
ut s
ome
patie
nts
8 H
ave
a ba
sic
unde
rsta
ndin
g of
role
san
d cu
lture
e h all
n t erih in
gt hei ar
e w h w
s ec ya t acp ili p
e s c sa e
m f icea t
am acn s eyr hI s p t
e n m e i o rh est
y ( hi
e w ti wl )c i eca cap
e f a
e s p
mm a d s
e ae
sn
s reyh ha hI t s t 8Ac
tivel
y se
ek s
yste
m
solu
tions
toge
ther
or
deve
lop
work
-a-ro
unds
8Co
mm
unic
ate
frequ
ently
in p
erso
n
8 C
olla
bora
te d
riven
by
desi
re to
be
a m
embe
r of
the
care
team
8 H
ave
regu
lar t
eam
m
eetin
gs to
dis
cuss
ove
rall
patie
nt c
are
and
spec
ific
patie
nt is
sues
8 H
ave
an in
-dep
th u
nshyde
rsta
ndin
g of
role
s an
dcu
lture
8 H
ave
reso
lved
mos
t or a
ll sy
stem
issu
es f
unct
ioni
ng
as o
ne in
tegr
ated
sys
tem
8Co
mm
unic
ate
cons
iste
ntly
at th
e sy
stem
tea
m a
nd
indi
vidu
al le
vels
8 C
olla
bora
te d
riven
by
shar
ed c
once
pt o
f tea
mca
re
8 H
ave
form
al a
nd in
form
al
mee
tings
to s
uppo
rt in
tegr
ated
mod
el o
f car
e
8 H
ave
role
s an
d cu
lture
s th
at b
lur o
r ble
nd
10
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 2
A S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Clin
ical
Del
iver
y
Scr
eeni
ng a
nd a
sses
sshym
ent d
one
acco
rdin
g to
se
para
te p
ract
ice
mod
els
Sepa
rate
trea
tmen
t pla
ns
Ev
iden
ced-
base
d pr
actic
es (E
BP)
impl
emen
ted
sepa
rate
ly
8 8 8
Scre
enin
g ba
sed
on
sepa
rate
pra
ctic
es m
al
y be
mat
ion
ma
info
rsh
ared
thro
ugh
for
requ
ests
or H
ealth
m
atio
n Ex
chan
ges
Info
r
Sepa
rate
trea
tmen
t pl
ans
shar
ed b
ased
on
esta
blis
hed
rela
tion-
een
spec
ific
ship
s be
twvi
ders
pr
o
Sepa
rate
resp
onsi
bilit
y fo
r car
eEB
Ps
8 8 8
ree
on a
spe
cific
y
ag M
a
crite
ria fo
r mor
e ef
fect
ive
sc
reen
ing
or o
ther
ral
vice
pla
ns
ms e
in-h
ouse
refe
r
Sep
arat
e se
rwi
th s
ome
shar
ed
mat
ion
that
info
r
wled
g
info
rth
em
8
Som
e sh
ared
kno
s EB
Ps
of e
ach
othe
rrsquoes
peci
ally
for h
igh
utili
zers
88
A
gree
on
spec
ific
bas
ed o
n sc
reen
ing
abili
ty to
resp
ond
to
e tre
atm
ent
resu
lts
8
Col
labo
rativ
plan
ning
for s
peci
fic
patie
nts
Som
e EB
Ps a
nd s
ome
focu
sed
train
ing
shar
ed
on in
tere
st o
r spe
cific
po
pula
tion
need
s
8 8
Con
sist
ent s
et o
f agr
eed
upon
scr
eeni
ngs
acro
ss
disc
iplin
es w
hich
gui
de
vent
ions
e tre
atm
ent
treat
men
t int
er
8
Col
labo
rativ
plan
ning
for a
ll sh
ared
patie
nts
8
EBP
s sh
ared
acr
oss
sys-
tem
with
som
e jo
int m
onishy
torin
g of
hea
lth c
ondi
tions
fo
r som
e pa
tient
s
8
8 P
opul
atio
n-ba
sed
m
edic
al a
nd b
ehav
iora
l he
alth
scr
eeni
ng is
stan
dard
pra
ctic
e wi
thre
sults
ava
ilabl
e to
all
and
resp
onse
pro
toco
lsin
pla
ce
8On
e tre
atm
ent p
lan
for a
llpa
tient
s
8EB
Ps a
re te
am s
elec
ted
train
ed a
nd im
plem
ente
dac
ross
dis
cipl
ines
as
stan
dard
pra
ctic
e
Key
Dif
fere
ntia
tor
Pat
ien
t Exp
erie
nce
ysic
al a
nd b
eshy P
atie
nt p
hha
vior
al h
ealth
nee
ds a
re
treat
ed a
s se
para
te is
sues
otia
te
Pat
ient
mus
t neg
sepa
rate
pra
ctic
es a
nd
wn w
ith
rees
of s
ucce
ss
site
s on
thei
r oyi
ng d
egarv
8 8vi
der
P
atie
nt h
ealth
nee
ds
are
treat
ed s
epar
atel
ybu
t rec
ords
are
sha
red re
d
prom
otin
g be
tter p
ro riers
y
be re
fer
y pa
tient
s
e
arie
ty o
f bar
wled
gkn
o
Pat
ient
s m
abu
t a v
vent
man
pre
from
acc
essi
ng c
are
8 8
atie
nt h
ealth
nee
ds a
re y
y b
ws
P treat
ed s
epar
atel
y at
the
sam
e lo
catio
n
8
Clo
se p
roxim
ity a
llora
ls to
be
mor
e re
fer
succ
essf
ul a
nd e
asie
r for
ho
a
lthou
gh w ar
y v
red
ma
patie
nts
gets
refe
rvi
der
pro
8
col
labo
ratio
n m
ight
Pat
ient
nee
ds a
re tr
eate
d se
para
tely
at t
he s
ame
m h
and-
offs
to
vide
rs
site
in
clud
e wa
rot
her t
reat
men
t pro na
lly
Pat
ient
s ar
e in
ter
red
with
bet
ter f
ollo
wshyre
fer
up b
ut c
olla
bora
tion
may
st
ill b
e ex
perie
nced
as
vice
s se
para
te s
er
8 8
y
e on
Pat
ient
nee
ds a
re tr
eate
d as
a te
am fo
r sha
red
patie
nts
(for t
hose
wh
o sc
reen
pos
itiv
scre
enin
g m
easu
res)
and
sepa
rate
ly fo
r oth
ers
e to
8
Car
e is
resp
onsi
vid
entifi
ed p
atie
nt n
eeds
bvi
ders
as e a
of a
team
of p
ro w
hich
feel
s lik
need
ed
one-
stop
sho
p
8
All p
atie
nt h
ealth
nee
ds ar
e tre
ated
for a
ll pa
tient
sby
a te
am w
ho fu
nctio
n et
her
ely
tog
effe
ctiv
Pat
ient
s ex
perie
nce
a se
amle
ss re
spon
se to
all h
ealth
care
nee
ds a
s in
a u
nifie
d y
pres
ent
the
prac
tice
8 8
11
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
No
coo
rdin
atio
n or
ts
em
ent o
f e
effo
r
vide
r buy
-in
en
ratio
n or
ev
up
to
vide
rs to
man
agco
llabo
rativ
Litt
le p
roto
inte
gco
llabo
ratio
nin
divi
dual
pro
initi
ate
as ti
me
and
prac
tice
limits
allo
w
8 8
Som
e pr
actic
e le
ader
shysh
ip in
mor
e sy
stem
atic
vide
r buy
-into
al
ue
ving
nee
ded
mat
ion
shar
ing
info
r
Som
e pr
oco
llabo
ratio
n an
d v
plac
ed o
n ha
mat
ion
info
r
8 8
Org
aniza
tion
lead
ers
tive
but o
ften
colo
shysu
ppor
catio
n is
vie
wed
as
a pr
ojec
t or p
rogr
am ork
and
vide
r buy
-in to
ra
ls w
Pro mak
ing
refe
rap
prec
iatio
n of
ons
ite
vaila
bilit
y a
8 8
thro
ugh
mut
ual p
robl
em-
Org
aniza
tion
lead
ers
ratio
n t i
nteg
supp
or
solv
ing
of s
ome
syst
em
riers
ba
r
Mor
e bu
y-in
to c
once
pt
vide
rs
ratio
n bu
t not
of
inte
gco
nsis
tent
acr
oss
not
all
pro
tuni
ties
for
vide
rs
pro
usin
g op
por
inte
grat
ion
or c
ompo
nent
s
8 8
ts
w
Org
aniza
tion
lead
ers if
ra
tion
ws a
nd e
ffor
t int
egsu
ppor
fund
ing
allo
plac
ed in
sol
ving
as
man
y sy
stem
issu
es a
s w
ithou
t cha
ngshy
poss
ible
in
g fu
ndam
enta
lly h
odi
scip
lines
are
pra
ctic
ed
rate
d y
not
vide
rs
e in
pra
ctic
e
ly a
ll pr
o N
ear ag
ed in
inte
g B
uy-in
ma
y fo
r ind
ivid
ual
eng
mod
el
incl
ude
chan
g
vide
rs
stra
teg
pro
8 8
y e
ervi
ded
aniza
tion
lead
ers
t ra
tion
as p
ract
ice
Org
stro
ngly
sup
por
inte
gm
odel
with
exp
ecte
dvi
ce d
eliv
e in
ser
chan
g
for d
evel
opm
ent
rate
d ca
re a
nd a
ll In
teg
com
pone
nts
embr
aced
vide
rs a
nd a
ctiv
and
reso
urce
s pr
o
by a
ll pr
ool
vem
ent i
n pr
actic
e e
vin ch
ang
8 8
Tab
le 2
b S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs c
ont
inue
d)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Pra
ctic
eO
rgan
izat
ion
Key
Dif
fere
ntia
tor
bu
sin
ess
Mo
del
Se
para
te fu
ndin
g
No s
harin
g of
reso
urce
s
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re re
sour
ces
for
sing
le p
roje
cts
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re fa
cilit
y ex
pens
es
Sepa
rate
bill
ing
prac
tices
8 8 8
but
may
S
epar
ate
fund
ing
rant
s sta
ffing
cos
ts
shar
e g
y sh
are
offic
e
uctu
re
Ma
expe
nses
or
infra
str
Sepa
rate
bill
ing
due
to
riers
sy
stem
bar
8 8 8
Bl
ende
d fu
ndin
g ba
sed
uctu
re
on c
ontra
cts
gra
nts
or
ys to
str
agre
emen
ts
Varie
ty o
f wa
8
the
shar
ing
of a
ll ex
pens
es
Billi
ng fu
nctio
n co
mbi
ned
reed
upo
n pr
oces
s or
ag
8 8
8 8Re
sour
ces
shar
ed a
nd
hole
rate
d fu
ndin
g In
teg
base
d on
mul
tiple
sour
ces
of re
venu
e
allo
cate
d ac
ross
wpr
actic
e
Billi
ng m
axim
ized
for
rate
d m
odel
and
uc
ture
in
teg
sing
le b
illin
g st
r
8
12
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 3
Ad
vant
ages
and
Wea
knes
ses
at E
ach
Leve
l of C
olla
bo
ratio
nIn
tegr
atio
n
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Ad
van
tag
es
8 E
ach
prac
tice
can
mak
e tim
ely
and
auto
nom
ous
deci
sion
s ab
out c
are
8Re
adily
und
erst
ood
asa
prac
tice
mod
el b
y pa
tient
s an
d pr
ovid
ers
8 M
aint
ains
eac
h pr
actic
ersquos
basi
c op
erat
ing
stru
ctur
eso
cha
nge
is n
ot a
di
srup
tive
fact
or
8 P
rovi
des
som
e co
ordi
natio
n an
din
form
atio
n-sh
arin
g th
at
is h
elpf
ul to
bot
h pa
tient
san
d pr
ovid
ers
8 C
oloc
atio
n al
lows
for
mor
e di
rect
inte
ract
ion
and
com
mun
icat
ion
amon
g pr
ofes
sion
als
toim
pact
pat
ient
car
e
8 R
efer
rals
mor
e su
cces
sful
du
e to
pro
ximity
8 O
ppor
tuni
ty to
dev
elop
cl
oser
pro
fess
iona
l rel
ashytio
nshi
ps
8 R
emov
al o
f som
e sy
stem
ba
rrier
s li
ke s
epar
ate
reco
rds
allo
ws c
lose
r co
llabo
ratio
n to
occ
ur
8 B
oth
beha
vior
al h
ealth
an
d m
edic
al p
rovi
ders
ca
n be
com
e m
ore
well-
info
rmed
abo
ut w
hat e
ach
can
prov
ide
8 P
atie
nts
are
view
ed a
s sh
ared
whi
ch fa
cilit
ates
m
ore
com
plet
e tre
atm
ent
plan
s
8 H
igh
leve
l of c
olla
bora
tion
lead
s to
mor
e re
spon
sive
pa
tient
car
e in
crea
sing
en
gage
men
t and
ad
here
nce
to tr
eatm
ent
plan
s
8 P
rovi
der fl
exib
ility
in
crea
ses
as s
yste
mis
sues
and
bar
riers
are
re
solve
d
8 B
oth
prov
ider
and
pat
ient
sa
tisfa
ctio
n m
ay in
crea
se
8 O
ppor
tuni
ty to
trul
y tre
at
whol
e pe
rson
8Al
l or a
lmos
t all
syst
emba
rrier
s re
solve
d a
llowi
ng
prov
ider
s to
pra
ctic
e as
hi
gh fu
nctio
ning
team
8Al
l pat
ient
nee
dsad
dres
sed
as th
ey o
ccur
8 S
hare
d kn
owle
dge
base
of
pro
vide
rs in
crea
ses
and
allo
ws e
ach
prof
essi
onal
to
resp
ond
mor
e br
oadl
yan
d ad
equa
tely
to a
ny
issu
e
Wea
knes
ses
8 S
ervi
ces
may
ove
rlap
be
dupl
icat
ed o
r eve
n wo
rk
agai
nst e
ach
othe
r
8 Im
porta
nt a
spec
ts o
f car
e m
ay n
ot b
e ad
dres
sed
or ta
ke a
long
tim
e to
be
diag
nose
d
8 S
harin
g of
info
rmat
ion
may
not
be
syst
emat
ic
enou
gh to
effe
ct o
vera
ll pa
tient
car
e
8 N
o gu
aran
tee
that
info
rshym
atio
n wi
ll ch
ange
pla
n or
st
rate
gy o
f eac
h pr
ovid
er
8 R
efer
rals
may
fail
due
to
barri
ers
lead
ing
to p
atie
nt
and
prov
ider
frus
tratio
n
8 P
roxim
ity m
ay n
ot le
ad to
gr
eate
r col
labo
ratio
nlim
iting
val
ue
8 E
ffort
is re
quire
d to
de
velo
p re
latio
nshi
ps
8 L
imite
d fle
xibili
ty if
tra
ditio
nal r
oles
are
mai
ntai
ned
8 S
yste
m is
sues
may
lim
it co
llabo
ratio
n
8 P
oten
tial f
or te
nsio
n an
d co
nflic
ting
agen
das
amon
g pr
ovid
ers
as p
ract
ice
boun
darie
s lo
osen
8 P
ract
ice
chan
ges
may
cr
eate
lack
of fi
t for
som
ees
tabl
ishe
d pr
ovid
ers
8Ti
me
is n
eede
d to
co
llabo
rate
at t
his
high
leve
l and
may
affe
ct
prac
tice
prod
uctiv
ity o
rca
denc
e of
car
e
8 S
usta
inab
ility
issu
es m
ay
stre
ss th
e pr
actic
e
8 F
ew m
odel
s at
this
leve
l wi
th e
noug
h ex
perie
nce
tosu
ppor
t val
ue
8Ou
tcom
e ex
pect
atio
ns n
otye
t est
ablis
hed
13

Acknowledgements
A Review and Proposed Standard Framework for Levels of Integrated Healthcare was developed for the SAMHSA-HRSA Center for
Integrated Health Solutions with funds under grant number 1UR1SMO60319-01 from SAMHSA-HRSA US Department of Health
and Human Services The statements findings conclusions and recommendation are those of the author(s) and do not necessarshy
ily reflect the view of SAMHSA HRSA or the US Department of Health and Human Services
Special thanks to Bern Heath Jr PhD CEO Axis Health System Kathy Reynolds MSW ACSW Vice President of Health Integration
and Wellness Promotion National Council for Community Behavioral Healthcare and Pam Wise Romero PhD Chief Clinical Officer
Axis Health Systems and for authoring this document
sAmHsA-HRsA centeR FoR IntegRAted HeAltH solUtIons
The SAMHSA-HRSA Center for Integrated Health Solutions (CIHS) promotes the development of integrated primary and behavioshy
ral health services to better address the needs of individuals with mental health and substance use conditions whether seen in
specialty behavioral health or primary care provider settings CIHS is the first ldquonational homerdquo for information experts and other
resources dedicated to bidirectional integration of behavioral health and primary care
Jointly funded by the HHSSubstance Abuse and Mental Health Services Administration and the Health Resources and Services
Administration and run by the National Council for Community Behavioral Healthcare CIHS provides training and technical assisshy
tance to community behavioral health organizations that received Primary and Behavioral Health Care Integration grants as well
as to community health centers and other primary care and behavioral health organizations
CIHSrsquos wide array of training and technical assistance helps improve the effectiveness efficiency and sustainability of integrated
services which ultimately improves the health and wellness of individuals living with behavioral health disorders
1701 K Street NW Suite 400
Washington DC 20006
2026847457
integrationtheNationalCouncilorg
wwwintegrationsamhsagov
This document is in the public domain and may be used and reprinted without permission except those copyrighted materials noted for which further reproduction is prohibited without the specific permission of copyright holders
SuggeSted Citation Heath B Wise Romero P and Reynolds K A Review and Proposed Standard Framework for Levels of Integrated Healthcare Washington DCSAMHSA-HRSA Center for Integrated Health Solutions March 2013
Ac
kn
ow
le
dg
em
en
ts
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS 2
3 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
aBStRaCt Integration of healthcare is essential to improve the individualrsquos experience of care improve the health of the general
population and reduce per capita healthcare costs The term ldquointegrationrdquo is widely and inconsistently used to describe the bringshy
ing together of healthcare components Integration has been used to reference everything from consultation to colocation to a
setting of shared health values around treating the whole person with blurred professional boundaries There have been no fully
updated taxonomies to describe the levels of integration since the 1996 Doherty McDaniel and Baird article which initially proshy
posed five levels of integration Since this seminal issue brief and preliminary framework there have been many informal and local
adaptations However without a standard classification of integrated settings discussions of integration lack clarity and precision
and research cannot confidently examine discrete aspects of integration This issue brief reviews levels of integrated healthcare
and proposes a functional standard framework for classifying sites according to these levels
KeY WoRdS integration collaborative care mental health behavioral health collaboration healthcare
BAckgRoUnd Over the last several years as healthcare reform has taken a prominent national position and mental health and substance abuse
treatments have evolved an increasing number of articles have been written on collaboration and the integration of traditional
primary care and behavioral health practices (Butler Kane amp McAlpine 2008 Collins Hewson Munger amp Wade 2010 Funk
amp Ivbijaro 2008 Lopez Coleman-Beattie amp Sanchez 2008 Mauer 2006 2009 Mauer amp Jarvis 2010 Miller Kessler amp Peek
2011 Robinson amp Reiter 2007 Russell 2010) These articles have described a wide variety of collaborative co-located and
integrated service models
Developing a standard framework to describe integrated efforts is critical for meaningful dialogue about service design as well as
for research Until there is a way to reliably categorize integration implementations meaningful comparisons of implementations
or associated health outcomes cannot occur This point is made throughout the Miller et al 2011 paper which calls for a broader
ldquolexicon for the common terms and components for collaborative care so that research questions can be framed in a consistently
understood mannerrdquo (p 2) On the clinical side integrated care developers and implementers will benefit from recognizing the
characteristics of practice change that support evolving integration models Knowing what features of integrated healthcare impleshy
mentations lead to the most favorable and stable health outcomes will be an important contribution to the health field
A standard framework also contributes to the orderly evolution of national healthcare reform and aligns with the political and
service realities defined by Berwick Nolan and Whittington (2008) Integration is essential to achieving the triple aim of improved
experience of care improved health of populations and reduced per capita healthcare cost advocated by Berwick et al The lesshy
sons learned from a reliable comparison of models and implementations provide the best foundation to inform policy decisions on
the structure of more effective healthcare as care integration moves forward
levels oF IntegRAtIon Doherty McDaniel and Baird (1995 1996) proposed the first classification by level of Until there is a way to reliably collaboration and integration They proposed the five levels of primary care-behavioral
healthcare collaboration recognizing that collaboration and integration of care were categorize integration evolving and being communicated in wide-ranging ways Doherty et alrsquos classification
implementations meaningfulinvolved both the extent of the occurrence of collaboration and the capacity for colshy
laboration in the setting but they did not focus on specific interactions An underlying comparisons of implementationspremise of the levels was that as collaboration increased the adequate handling of
complex patients would also increase The levels recognized by Doherty et al did not or associated health outcomes prescribe a particular model as best for all healthcare settings but rather served as
a foundation from which to tease apart the strengths and limitations of a variety of cannot occur
sA
mH
sA
-HR
sA
ce
nt
eR
Fo
R I
nt
eg
RA
te
d H
eA
ltH
so
lU
tIo
ns
This issue brief uses the term behavioral health to describe mental health and substance use
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
options It was proposed that use of the levels would help organizations evaluate their setting in light of their goals for collaboration
and to assist in researching outcomes and costs associated with different collaborative models with different patient populations
In the original framework Doherty et al differentiated levels by where they were practiced the cases adequately handled at each
level and the following descriptions
8 LeveL 1ndash Minimal Collaboration Mental health and other healthcare providers work in separate facilities have separate
systems and rarely communicate about cases
8 LeveL 2 ndash Basic Collaboration at a Distance Providers have separate systems at separate sites but engage in periodic
communication about shared patients mostly through telephone and letters Providers view each other as resources
8 LeveL 3 ndash Basic Collaboration Onsite Mental health and other healthcare professionals have separate systems but share
facilities Proximity supports at least occasional face-to- face meetings and communication improves and is more regular
8 LeveL 4 ndash Close Collaboration in a Partly Integrated System Mental health and other healthcare providers share the same
sites and have some systems in common such as scheduling or charting There are regular face-to-face interactions among
primary care and behavioral health providers coordinated treatment plans for difficult patients and a basic understanding
of each otherrsquos roles and cultures
8 LeveL 5 ndash Close Collaboration in a Fully Integrated System Mental health and other healthcare professionals share the
same sites vision and systems All providers are on the same team and have developed an in-depth understanding of
each otherrsquos roles and areas of expertise
The following chart summarizes these five levels of collaboration
MINIMAL COLLAbORATION
bASIC COLLAbORATION
FROM A DISTANCE
bASIC COLLAbORATION
ONSITE
CLOSE COLLAbORATION
PARTLy INTEGRATED
FULLy INTEGRATED
8 Separate systems
8 Separate facilities
8 Communication is
8 Separate systems
8 Separate facilities
8 Periodic focused
8 Separate systems
8 Same facilities
8 Regular rare
8 Little appreciation of each otherrsquos culture
ldquoNobody knows my name Who are yourdquo
communication most written
8 View each other as outside resources
8 Little understandshying of each otherrsquos culture or sharing of influence
ldquoI help your consumersrdquo
communication occasionally face-to-face
8 Some appreciation of each otherrsquos role and general sense of large picture
8Mental health usually has more influence
ldquoI am your consultantrdquo
8Some shared systems
8Same facilities
8Face-to-Face consultation coordinated treatment plans
8Basic appreciation of each otherrsquos role and cultures
8Collaborative routines difficult time and operation barriers
8Influence sharing
ldquoWe are a team in the care of consumersrdquo
8Shared systems and facilities in seamless bio-psychosocial web
8Consumers and providers have same expectations of system(s)
8In-depth appreciation of roles and culture
8Collaborative routines are regular and smooth
8Conscious influence sharing based on situation and expertise
ldquoTogether we teach others how to be a team in care of conshysumers and design a care systemrdquo
4
5 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
These five levels have formed the foundation for most subsequent level adaptations The idea that integration occurs along a
continuum of collaboration and integration is widely supported (Collins et al 2010 Miller et al 2011 Peek 2007 Reynolds
2006 Seaburn Lorenz Gunn Gawinski amp Mauksch 1996 Strohsal 1998) and adaptations have differed in the number of levels
(from three to 10) and the categories used to differentiate or describe levels
The reason for classification whether for clinical development or research
has influenced the choice of dimensions used to define each level For
example Reynolds (2006) used the same five levels but distinguishes
between levels on the basis of functional practice categories including
access services funding governance evidence-based practice and
data usage The goal of Reynoldsrsquo adaptation is to better capture the pashy
tient and staff experience at the different levels in doing so it broadens
the levelsrsquo descriptions and characteristics
Other papers and reports have classified integrated implementations
somewhat differently MaineHealth (2009) developed a site-specific ratshy
ing of integration that has four levels along a continuum of integration
with one rating in the first level and three ratings in levels two three and four There are 18 characteristics broadly categorized
as integrated services patient- and family-centeredness and practiceorganization In the first category characteristics such as
colocation patientfamily involvement and communication with patients about integrated care are rated In the second category
characteristics such as organizational leadership for integrated care providersrsquo engagement and data systemspatient are rated
More similar to Doherty et al Blount (2003) collapsed the five levels to three coordinated co-located and integrated care Reshy
cent work to develop a lexicon or common conceptual system for collaborative care between behavioral health and primary medical
clinicians (Miller et al 2011) has also adopted these three levels in describing collaborative care practice
The Milbank report Evolving Models of Behavioral Health Integration in Primary Care (Collins et al 2010) describes eight models
of integration across a variety of settings This group uses Doherty et alrsquos five level structure and the terms coordinated co-
located and integrated to differentiate these models
PRoPosed stAndARd FRAmewoRk Doherty et al established the five levels of integration recognizing differences in integrated implementations and the various forms
collaboration took in each level Based upon the initial efforts by Doherty et al and the experience accumulated over the intervenshy
ing 17 years the authors of this paper propose a new version of the levels of collaborationintegration The proposed framework
brings together valuable aspects that have evolved since the Doherty et al paper The proposed framework also includes several
enhancements that enable it to be comprehensive enough to serve as a national standard for future discussion about integrated
healthcare allow organizations implementing integration to gauge their degree of integration against acknowledged benchmarks
and serve as a foundation for comparing healthcare outcomes between integration levels
Doherty et al established the concept of levels of implementations that followed a continuum from collaboration to integration The
proposed model in this issue brief retains some of the original categorical descriptions that continue to prove useful today Blountrsquos
use of coordination colocation and integration serve as overarching categories The Milbank report which brought together
Doherty et alrsquos five levels and Blountrsquos broader categories also informs this conceptual framework
This new level of integration framework proposes six levels of collaborationintegration While the overarching framework has three
main categories mdash coordinated co-located and integrated care mdash there are two levels of degree within each category (see Table
1) It is designed to help organizations implementing integration to evaluate their degree of integration across several levels and to
determine what next steps they may want to take to enhance their integration initiatives
Coordinated Care
8 LeveL 1 mdash Minimal Collaboration
Behavioral health and primary care providers work at separate facilities and have separate systems Providers communicate
rarely about cases When communication occurs it is usually based on a particular providerrsquos need for specific information
about a mutual patient
8 LeveL 2 mdash Basic Collaboration at a Distance
Behavioral health and primary care providers maintain separate facilities and separate systems Providers view each other
as resources and communicate periodically about shared patients These communications are typically driven by specific
issues For example a primary care physician may request copy of a psychiatric evaluation to know if there is a confirmed
psychiatric diagnosis Behavioral health is most often viewed as specialty care
Co-Located Care
8 LeveL 3 mdash Basic Collaboration Onsite
Behavioral health and primary care providers co-located in the same facility but may or may not share the same practice
space Providers still use separate systems but communication becomes more regular due to close proximity especially
by phone or email with an occasional meeting to discuss shared patients Movement of patients between practices is
most often through a referral process that has a higher likelihood of success because the practices are in the same locashy
tion Providers may feel like they are part of a larger team but the team and how it operates are not clearly defined leaving
most decisions about patient care to be done independently by individual providers
8 LeveL 4 mdash Close Collaboration with Some System Integration
There is closer collaboration among primary care and behavioral healthcare providers due to colocation in the same
practice space and there is the beginning of integration in care through some shared systems A typical model may
involve a primary care setting embedding a behavioral health provider In an embedded practice the primary care front
desk schedules all appointments and the behavioral health provider has access and enters notes in the medical record
Often complex patients with multiple healthcare issues drive the need for consultation which is done through personal
communication As professionals have more opportunity to share patients they have a better basic understanding of each
otherrsquos roles
Integrated Care
8 LeveL 5 mdash Close Collaboration Approaching an Integrated Practice
There are high levels of collaboration and integration between behavioral and primary care providers The providers begin
to function as a true team with frequent personal communication The team actively seeks system solutions as they recogshy
nize barriers to care integration for a broader range of patients However some issues like the availability of an integrated
medical record may not be readily resolved Providers understand the different roles team members need to play and they
have started to change their practice and the structure of care to better achieve patient goals
8 LeveL 6 mdash Full Collaboration in a TransformedMerged Practice
The highest level of integration involves the greatest amount of practice change Fuller collaboration between providers
has allowed antecedent system cultures (whether from two separate systems or from one evolving system) to blur into a
single transformed or merged practice Providers and patients view the operation as a single health system treating the
whole person The principle of treating the whole person is applied to all patients not just targeted groups
Key elements were added to more clearly differentiate between the levels in each overarching category For coordinated care
the key element is communication The distinction between Level 1 and Level 2 is frequency and type of communication With inshy
creased communication providers have stronger relationships and greater understanding of the importance of integrated care and
sA
mH
sA
-HR
sA
ce
nt
eR
Fo
R I
nt
eg
RA
te
d H
eA
ltH
so
lU
tIo
ns
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS 6
7 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
the skills that different providers possess This communication increases
the coordination of care between separate healthcare entities
Physical proximity is the key element for the co-located care category
Although colocation does not guarantee greater collaboration or integrashy
tion it can be beneficial Taking advantage of close proximity increases
collaboration through face-to-face contact at Level 3 It can also develop
the opportunity for trust and relationship building leading to more sharing
of systems mdash the hallmark of beginning integration at Level 4 However
providers can be co-located and have no integration of their healthcare
services Each provider can still practice independently without commushy
nicating with others and with an integrated healthcare plan Colocation
reduces time spent travelling from one practitioner to another but does not guarantee integration
At Level 5 and Level 6 practice change is the key element No site can be fully integrated without changing how both behavioral
health and primary care are practiced The requisite practice change features a blending or blurring of cultures where no one disshy
cipline predominates Across many integrated implementations at several levels almost every practitioner wants integrated care
and believes it is the direction for healthcare to move towards until they realize it requires they change how they practice It is at
that point they often try to change the concepts of their integration efforts to preserve how they currently practice
A second modification proposed to the original Doherty et al structure is the use of the terms ldquocollaborationrdquo and ldquointegrationrdquo In
this framework collaboration describes how resources mdash namely the healthcare professionals mdash are brought together integration
describes how services are delivered and practices are organized and managed This idea is similar to Strosahlrsquos (1998) concept
that collaborative care involves behavioral health working with primary care while integration is behavioral health working within
and as part of primary care Recent analysis (Mauer amp Jarvis 2010) indicates that collaboration and integration can effectively
originate in either behavioral health or primary care and requires the transformation of both into a single whole In this standard
framework both collaboration and integration (beginning at Level 3) increase in degree and complexity over the continuum for
providers while similarly decreasing for clientsindividuals
An important enhancement to the levels is also found in a restructuring of the descriptive characteristics defining each level (see
Table 1) Each of the six levels begins with a general description followed by key differentiators (see Table 2A and 2B) under the
headings clinical delivery patient experience practiceorganization and business model These characteristics help differentiate
the levels They also incorporate some of the functional categories Reynolds (2006) identified in her consumerstaff experiential
perspective of the levels of integration Kodnerrsquos (2009) integrated care domains and MaineHealthrsquos (2009) Site Assessment
Finally Table 3 describes the strengths and weaknesses of each level so that these can be built upon or addressed
Although the term behavioral health has been used throughout this proposed framework integration of substance use treatment
and primary care has not been as extensive or prevalent as integration of mental health with primary care Further work is required
to more effectively support substance use integration (Butler et al 2008 Mauer 2010)
It is worth noting that even if health outcomes improve as levels of integration increase it is not reasonable to believe that all
healthcare settings would be able to easily or even with difficulty move to increasing levels of integration As primary care and
behavioral health have evolved in their own professional silos it has been the authorsrsquo experience that the bringing together of
these services and service perspectives (usually embodied in separate agencies) into a single fully integrated healthcare system
requires a large amount of administrative political and financial investments over a long-term stepwise evolutionary process It
is important to aspire to whichever level can be best achieved practically
At Level 3 colocation may be a necessary and good starting point to build trust between separate existing systems and to estabshy
lish a shared history of improved outcomes This could lead to closer collaboration and integration of vision that moves to Level
4 implementation possibly leading from there to a Level 5 partnership Such a partnership may be the highest level attainable or
may in years to come lead to a joint venture or a merger of the organizations While this has not been fully researched merging
primary and behavioral health organizations appears necessary at this point for achieving Level 6 integration
8 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
From a data standpoint this framework also posits that integrated services should be defined by location not by an algorithm of
service code combinations A single service (eg blood pressure check or depression medication check) provided in an integrated
sitesetting is considered an integrated service because it is provided in the context of that integrated sitersquos whole person care
Conversely multiple services provided in a single visit are not by definition integrated care these services could be and all too
often are provided by separate professionals without meaningful collaboration or integration By defining the level of integration
in terms of setting the authors of this framework define the context of interventions and the values (eg care team whole health
patient-centered) that form the basis of an integrated site and integrated services The key performance indicators in an integrated
care setting are population-based health status outcomes not encounter-based processservice data Individual staff productivity
must accompany and then be replaced by population-based outcomes by site
Funding structures and accountability must also change Integrated care is not supported by fee-for-service funding structures
that stumble over same day billing restrictions and do not reimburse for consultations between providers when the patient is not
physically present or electronic contacts or a large volume of care management mdash all of which are essential for improved health
outcomes in an integrated healthcare system Fee-for-service funding can emphasize the measurement of volume rather than
quality Global or blended funding structures do support integrated healthcare and will be fiscally justified by improved patient
outcomes that reduce overall healthcare cost
conclUsIon The proposed level of integration framework is a manageable practical and conceptually sound six level framework for integrated
healthcare that begins with collaboration (how resources are brought together) and moves through colocation and increasing levels
of integration (how services are framed and delivered) This standard framework is needed for clarity and precision of communicashy
tion as well as to contribute to research and practice redesign By implication the numbering of levels suggests that the higher
the level of collaborationintegration the more potential for positive impact on health outcomes and patient experience This belief
remains a hypothesis and has not been empirically tested With further research these benefits of collaborationintegration can
be more firmly stated and can identify which aspects of the collaboration integration or combination of the two contribute most
directly to health outcomes
Even if health outcomes improve as levels of integration increase it is not practical to believe that every healthcare setting will be
able at least in the near term to implement increasing levels of integration Many integrated implementations will be constrained
by community politics trust between organizational systems financing andor differing service values
Lastly this issue brief does not presume to establish a fuller lexicon for integration and healthcare as much needed as it is The
authors leave that to others better suited to the task and hope that this paper will contribute to such a lexicon The purpose is
to help those delivering services today by presenting a conceptual framework to better understand and differentiate integrated
healthcare implementations The authors believe that this framework will inform discussions about integrated healthcare and that
its use will provide opportunity for service redesign that will lead to better conceptual and practical models of care
9 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
ReFeRences
Berwick DM Nolan TW amp Whittington J (2008) The triple aim Care health and cost Health Affairs 27(3) 759-769
Blount A (2003) Integrated primary care Organizing the evidence Families Systems amp Health 21 (2) 121-33 doi 1010371091shy75272121121
Blount A (Ed) (1998) Integrated primary care The future of medical and mental health collaboration New York Norton
Butler M Kane RL McAlpine D et al Integration of Mental HealthSubstance Abuse and Primary Care No 173 (Prepared by the Minnesota Evidence-based Practice Center under Contract No 290-02-0009) AHRQ Publication No 09-E003 Rockville MD Agency for Healthcare Research and Quality October 2008
Collins C Hewson DL Munger R amp Wade T (2010) Evolving models of behavioral health Integration in primary care Report commissioned by the Milbank Memorial Fund
Doherty W (1995) The whyrsquos and levels of collaborative family health care Family Systems Medicine 13(3-4) 275-81 doi101037h0089174
Doherty WJ McDaniel SH amp Baird MA (1996) Five levels of primary carebehavioral healthcare collaboration Behavioral Healthcare Tomorrow 25-28
Funk M and G Ivbijaro eds (2008) Integrating mental health into primary care ndash A global perspective Geneva Switzerland World Health Organization and London UK World Organization of Family Doctors Available at wwwwhointmental_healthpolicyMental20health20+20primary20care-20final20low-res20140908pdf
Kodner Dennis (2009) All together now A conceptual exploration of integrated care Healthcare Quarterly 13 (Sp) 6-15
Lopez M B Coleman-Beattie L Jahnke and K Sanchez (2008) Connecting body and mind A resource guide to integrated health care in Texas and the United States Austin TX Hogg Foundation for Mental Health
Mauer B (2006) Behavioral healthprimary care integration The four quadrant model and evidence-based practices Rockville MD National Council for Community Behavioral Healthcare
Mauer B (2009) Behavioral healthprimary care integration and the person-centered healthcare home Washington DC National Council for Community Behavioral Healthcare
Mauer B (2010) Substance use disorders and the person-centered healthcare home Rockville MD National Council for Community Behavioral Healthcare
Mauer B amp Jarvis D (2010) The business case for bidirectional integrated care Mental health and substance use services in primary care settings and primary care services in specialty mental health and substance use settings Integration Policy Initiative
Maine Health Access Foundation (2009) Site Self-Assessment
Miller BF Kessler R Peek CJ (2011) A national agenda for research in collaborative care Papers from the Collaborative Care Research Network Research Development Conference AHRQ Publication No 11-0067 Rockville MD Agency for Healthcare Research and Quality
Peek CJ (2007) Integrated Care Aids to Navigation Study packet for the Pennsylvania Eastern Ohio amp West Virginia Summit Integrating Mental Health and Primary Care Pittsburgh PA
Reynolds K (2006) Mental Health Primary Care Integration Options (Unpublished document)
Robinson PJ amp Reiter JT (2007) Behavioral consultation and primary care A guide to integrating services New York Springer
Russell L (2010) Mental health care services in primary care Tackling the issues in the context of health care reform Center for American Progress Washington DC
Seaburn Lorenz Gunn Gawinksi amp Mauksch (1996) Models of collaboration A guide for mental health professionals working with health care practitioners Basic Books
Strosahl K (1998) Integrating behavioral health and primary care services The primary mental health care model In Integrated primary care The future of medical and mental health collaboration edited by A Blount pp 139-66 New York WW Norton
Strosahl K amp Robinson P (2008) The primary care behavioral health model Applications to prevention acute care and chronic condition management In R Kessler amp D Strafford (Eds) Collaborative medicine case studies Evidence in practice New York Springer
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 1
Six
Lev
els
of C
olla
bo
ratio
nIn
tegr
atio
n (C
ore
Des
crip
tions
)
CO
OR
DIN
AT
ED
KE
y E
LEM
EN
T C
OM
MU
NIC
AT
ION
CO
LO
CA
TE
D
KE
y E
LEM
EN
T P
Hy
SIC
AL
PR
Ox
IMIT
y
INT
EG
RA
TE
D
KE
y E
LEM
EN
T P
RA
CT
ICE
CH
AN
GE
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
beh
avio
ral h
ealt
h p
rim
ary
care
an
d o
ther
hea
lth
care
pro
vid
ers
wo
rk
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
Com
mun
icat
e ab
out c
ases
on
ly ra
rely
and
und
erco
mpe
lling
circ
umst
ance
s
8 8 C
omm
unic
ate
driv
en b
y pr
ovid
er n
eed
8 M
ay n
ever
mee
t in
pers
on
8 H
ave
limite
d un
ders
tand
shyin
g of
eac
h ot
herrsquos
role
s
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
8Co
mm
unic
ate
perio
dica
llyab
out s
hare
d pa
tient
s
8 C
omm
unic
ate
driv
en b
y sp
ecifi
c pa
tient
issu
es
8 M
ay m
eet a
s pa
rt of
larg
er
com
mun
ity
8Ap
prec
iate
eac
h ot
herrsquos
ro
les
as re
sour
ces
secfi t f
o oy
n eti amli s c ya il ey
e f ar h
m ss e t
a e r
n s ece hI n w 8
Hav
e se
para
te s
yste
ms
8 C
omm
unic
ate
regu
larly
ab
out s
hare
d pa
tient
s b
y ph
one
or e
-mai
l
8 C
olla
bora
te d
riven
by
need
for e
ach
othe
rrsquos
serv
ices
and
mor
e re
liabl
e re
ferra
l
8M
eet o
ccas
iona
lly to
disc
uss
case
s du
e to
clo
sepr
oxim
ity
8 F
eel p
art o
f a la
rger
yet
no
n-fo
rmal
team
e h ey
n t h
ih e t
rti ee
w hc wya tp il
e s ica
ma e f
n s maI s 8
Sha
re s
ome
syst
ems
like
sc
hedu
ling
or m
edic
alre
cord
s
8Co
mm
unic
ate
in p
erso
nas
nee
ded
8 C
olla
bora
te d
riven
by
need
for c
onsu
ltatio
n an
dco
ordi
nate
d pl
ans
for
diffi
cult
patie
nts
8 H
ave
regu
lar f
ace-
to-fa
ce
inte
ract
ions
abo
ut s
ome
patie
nts
8 H
ave
a ba
sic
unde
rsta
ndin
g of
role
san
d cu
lture
e h all
n t erih in
gt hei ar
e w h w
s ec ya t acp ili p
e s c sa e
m f icea t
am acn s eyr hI s p t
e n m e i o rh est
y ( hi
e w ti wl )c i eca cap
e f a
e s p
mm a d s
e ae
sn
s reyh ha hI t s t 8Ac
tivel
y se
ek s
yste
m
solu
tions
toge
ther
or
deve
lop
work
-a-ro
unds
8Co
mm
unic
ate
frequ
ently
in p
erso
n
8 C
olla
bora
te d
riven
by
desi
re to
be
a m
embe
r of
the
care
team
8 H
ave
regu
lar t
eam
m
eetin
gs to
dis
cuss
ove
rall
patie
nt c
are
and
spec
ific
patie
nt is
sues
8 H
ave
an in
-dep
th u
nshyde
rsta
ndin
g of
role
s an
dcu
lture
8 H
ave
reso
lved
mos
t or a
ll sy
stem
issu
es f
unct
ioni
ng
as o
ne in
tegr
ated
sys
tem
8Co
mm
unic
ate
cons
iste
ntly
at th
e sy
stem
tea
m a
nd
indi
vidu
al le
vels
8 C
olla
bora
te d
riven
by
shar
ed c
once
pt o
f tea
mca
re
8 H
ave
form
al a
nd in
form
al
mee
tings
to s
uppo
rt in
tegr
ated
mod
el o
f car
e
8 H
ave
role
s an
d cu
lture
s th
at b
lur o
r ble
nd
10
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 2
A S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Clin
ical
Del
iver
y
Scr
eeni
ng a
nd a
sses
sshym
ent d
one
acco
rdin
g to
se
para
te p
ract
ice
mod
els
Sepa
rate
trea
tmen
t pla
ns
Ev
iden
ced-
base
d pr
actic
es (E
BP)
impl
emen
ted
sepa
rate
ly
8 8 8
Scre
enin
g ba
sed
on
sepa
rate
pra
ctic
es m
al
y be
mat
ion
ma
info
rsh
ared
thro
ugh
for
requ
ests
or H
ealth
m
atio
n Ex
chan
ges
Info
r
Sepa
rate
trea
tmen
t pl
ans
shar
ed b
ased
on
esta
blis
hed
rela
tion-
een
spec
ific
ship
s be
twvi
ders
pr
o
Sepa
rate
resp
onsi
bilit
y fo
r car
eEB
Ps
8 8 8
ree
on a
spe
cific
y
ag M
a
crite
ria fo
r mor
e ef
fect
ive
sc
reen
ing
or o
ther
ral
vice
pla
ns
ms e
in-h
ouse
refe
r
Sep
arat
e se
rwi
th s
ome
shar
ed
mat
ion
that
info
r
wled
g
info
rth
em
8
Som
e sh
ared
kno
s EB
Ps
of e
ach
othe
rrsquoes
peci
ally
for h
igh
utili
zers
88
A
gree
on
spec
ific
bas
ed o
n sc
reen
ing
abili
ty to
resp
ond
to
e tre
atm
ent
resu
lts
8
Col
labo
rativ
plan
ning
for s
peci
fic
patie
nts
Som
e EB
Ps a
nd s
ome
focu
sed
train
ing
shar
ed
on in
tere
st o
r spe
cific
po
pula
tion
need
s
8 8
Con
sist
ent s
et o
f agr
eed
upon
scr
eeni
ngs
acro
ss
disc
iplin
es w
hich
gui
de
vent
ions
e tre
atm
ent
treat
men
t int
er
8
Col
labo
rativ
plan
ning
for a
ll sh
ared
patie
nts
8
EBP
s sh
ared
acr
oss
sys-
tem
with
som
e jo
int m
onishy
torin
g of
hea
lth c
ondi
tions
fo
r som
e pa
tient
s
8
8 P
opul
atio
n-ba
sed
m
edic
al a
nd b
ehav
iora
l he
alth
scr
eeni
ng is
stan
dard
pra
ctic
e wi
thre
sults
ava
ilabl
e to
all
and
resp
onse
pro
toco
lsin
pla
ce
8On
e tre
atm
ent p
lan
for a
llpa
tient
s
8EB
Ps a
re te
am s
elec
ted
train
ed a
nd im
plem
ente
dac
ross
dis
cipl
ines
as
stan
dard
pra
ctic
e
Key
Dif
fere
ntia
tor
Pat
ien
t Exp
erie
nce
ysic
al a
nd b
eshy P
atie
nt p
hha
vior
al h
ealth
nee
ds a
re
treat
ed a
s se
para
te is
sues
otia
te
Pat
ient
mus
t neg
sepa
rate
pra
ctic
es a
nd
wn w
ith
rees
of s
ucce
ss
site
s on
thei
r oyi
ng d
egarv
8 8vi
der
P
atie
nt h
ealth
nee
ds
are
treat
ed s
epar
atel
ybu
t rec
ords
are
sha
red re
d
prom
otin
g be
tter p
ro riers
y
be re
fer
y pa
tient
s
e
arie
ty o
f bar
wled
gkn
o
Pat
ient
s m
abu
t a v
vent
man
pre
from
acc
essi
ng c
are
8 8
atie
nt h
ealth
nee
ds a
re y
y b
ws
P treat
ed s
epar
atel
y at
the
sam
e lo
catio
n
8
Clo
se p
roxim
ity a
llora
ls to
be
mor
e re
fer
succ
essf
ul a
nd e
asie
r for
ho
a
lthou
gh w ar
y v
red
ma
patie
nts
gets
refe
rvi
der
pro
8
col
labo
ratio
n m
ight
Pat
ient
nee
ds a
re tr
eate
d se
para
tely
at t
he s
ame
m h
and-
offs
to
vide
rs
site
in
clud
e wa
rot
her t
reat
men
t pro na
lly
Pat
ient
s ar
e in
ter
red
with
bet
ter f
ollo
wshyre
fer
up b
ut c
olla
bora
tion
may
st
ill b
e ex
perie
nced
as
vice
s se
para
te s
er
8 8
y
e on
Pat
ient
nee
ds a
re tr
eate
d as
a te
am fo
r sha
red
patie
nts
(for t
hose
wh
o sc
reen
pos
itiv
scre
enin
g m
easu
res)
and
sepa
rate
ly fo
r oth
ers
e to
8
Car
e is
resp
onsi
vid
entifi
ed p
atie
nt n
eeds
bvi
ders
as e a
of a
team
of p
ro w
hich
feel
s lik
need
ed
one-
stop
sho
p
8
All p
atie
nt h
ealth
nee
ds ar
e tre
ated
for a
ll pa
tient
sby
a te
am w
ho fu
nctio
n et
her
ely
tog
effe
ctiv
Pat
ient
s ex
perie
nce
a se
amle
ss re
spon
se to
all h
ealth
care
nee
ds a
s in
a u
nifie
d y
pres
ent
the
prac
tice
8 8
11
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
No
coo
rdin
atio
n or
ts
em
ent o
f e
effo
r
vide
r buy
-in
en
ratio
n or
ev
up
to
vide
rs to
man
agco
llabo
rativ
Litt
le p
roto
inte
gco
llabo
ratio
nin
divi
dual
pro
initi
ate
as ti
me
and
prac
tice
limits
allo
w
8 8
Som
e pr
actic
e le
ader
shysh
ip in
mor
e sy
stem
atic
vide
r buy
-into
al
ue
ving
nee
ded
mat
ion
shar
ing
info
r
Som
e pr
oco
llabo
ratio
n an
d v
plac
ed o
n ha
mat
ion
info
r
8 8
Org
aniza
tion
lead
ers
tive
but o
ften
colo
shysu
ppor
catio
n is
vie
wed
as
a pr
ojec
t or p
rogr
am ork
and
vide
r buy
-in to
ra
ls w
Pro mak
ing
refe
rap
prec
iatio
n of
ons
ite
vaila
bilit
y a
8 8
thro
ugh
mut
ual p
robl
em-
Org
aniza
tion
lead
ers
ratio
n t i
nteg
supp
or
solv
ing
of s
ome
syst
em
riers
ba
r
Mor
e bu
y-in
to c
once
pt
vide
rs
ratio
n bu
t not
of
inte
gco
nsis
tent
acr
oss
not
all
pro
tuni
ties
for
vide
rs
pro
usin
g op
por
inte
grat
ion
or c
ompo
nent
s
8 8
ts
w
Org
aniza
tion
lead
ers if
ra
tion
ws a
nd e
ffor
t int
egsu
ppor
fund
ing
allo
plac
ed in
sol
ving
as
man
y sy
stem
issu
es a
s w
ithou
t cha
ngshy
poss
ible
in
g fu
ndam
enta
lly h
odi
scip
lines
are
pra
ctic
ed
rate
d y
not
vide
rs
e in
pra
ctic
e
ly a
ll pr
o N
ear ag
ed in
inte
g B
uy-in
ma
y fo
r ind
ivid
ual
eng
mod
el
incl
ude
chan
g
vide
rs
stra
teg
pro
8 8
y e
ervi
ded
aniza
tion
lead
ers
t ra
tion
as p
ract
ice
Org
stro
ngly
sup
por
inte
gm
odel
with
exp
ecte
dvi
ce d
eliv
e in
ser
chan
g
for d
evel
opm
ent
rate
d ca
re a
nd a
ll In
teg
com
pone
nts
embr
aced
vide
rs a
nd a
ctiv
and
reso
urce
s pr
o
by a
ll pr
ool
vem
ent i
n pr
actic
e e
vin ch
ang
8 8
Tab
le 2
b S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs c
ont
inue
d)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Pra
ctic
eO
rgan
izat
ion
Key
Dif
fere
ntia
tor
bu
sin
ess
Mo
del
Se
para
te fu
ndin
g
No s
harin
g of
reso
urce
s
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re re
sour
ces
for
sing
le p
roje
cts
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re fa
cilit
y ex
pens
es
Sepa
rate
bill
ing
prac
tices
8 8 8
but
may
S
epar
ate
fund
ing
rant
s sta
ffing
cos
ts
shar
e g
y sh
are
offic
e
uctu
re
Ma
expe
nses
or
infra
str
Sepa
rate
bill
ing
due
to
riers
sy
stem
bar
8 8 8
Bl
ende
d fu
ndin
g ba
sed
uctu
re
on c
ontra
cts
gra
nts
or
ys to
str
agre
emen
ts
Varie
ty o
f wa
8
the
shar
ing
of a
ll ex
pens
es
Billi
ng fu
nctio
n co
mbi
ned
reed
upo
n pr
oces
s or
ag
8 8
8 8Re
sour
ces
shar
ed a
nd
hole
rate
d fu
ndin
g In
teg
base
d on
mul
tiple
sour
ces
of re
venu
e
allo
cate
d ac
ross
wpr
actic
e
Billi
ng m
axim
ized
for
rate
d m
odel
and
uc
ture
in
teg
sing
le b
illin
g st
r
8
12
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 3
Ad
vant
ages
and
Wea
knes
ses
at E
ach
Leve
l of C
olla
bo
ratio
nIn
tegr
atio
n
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Ad
van
tag
es
8 E
ach
prac
tice
can
mak
e tim
ely
and
auto
nom
ous
deci
sion
s ab
out c
are
8Re
adily
und
erst
ood
asa
prac
tice
mod
el b
y pa
tient
s an
d pr
ovid
ers
8 M
aint
ains
eac
h pr
actic
ersquos
basi
c op
erat
ing
stru
ctur
eso
cha
nge
is n
ot a
di
srup
tive
fact
or
8 P
rovi
des
som
e co
ordi
natio
n an
din
form
atio
n-sh
arin
g th
at
is h
elpf
ul to
bot
h pa
tient
san
d pr
ovid
ers
8 C
oloc
atio
n al
lows
for
mor
e di
rect
inte
ract
ion
and
com
mun
icat
ion
amon
g pr
ofes
sion
als
toim
pact
pat
ient
car
e
8 R
efer
rals
mor
e su
cces
sful
du
e to
pro
ximity
8 O
ppor
tuni
ty to
dev
elop
cl
oser
pro
fess
iona
l rel
ashytio
nshi
ps
8 R
emov
al o
f som
e sy
stem
ba
rrier
s li
ke s
epar
ate
reco
rds
allo
ws c
lose
r co
llabo
ratio
n to
occ
ur
8 B
oth
beha
vior
al h
ealth
an
d m
edic
al p
rovi
ders
ca
n be
com
e m
ore
well-
info
rmed
abo
ut w
hat e
ach
can
prov
ide
8 P
atie
nts
are
view
ed a
s sh
ared
whi
ch fa
cilit
ates
m
ore
com
plet
e tre
atm
ent
plan
s
8 H
igh
leve
l of c
olla
bora
tion
lead
s to
mor
e re
spon
sive
pa
tient
car
e in
crea
sing
en
gage
men
t and
ad
here
nce
to tr
eatm
ent
plan
s
8 P
rovi
der fl
exib
ility
in
crea
ses
as s
yste
mis
sues
and
bar
riers
are
re
solve
d
8 B
oth
prov
ider
and
pat
ient
sa
tisfa
ctio
n m
ay in
crea
se
8 O
ppor
tuni
ty to
trul
y tre
at
whol
e pe
rson
8Al
l or a
lmos
t all
syst
emba
rrier
s re
solve
d a
llowi
ng
prov
ider
s to
pra
ctic
e as
hi
gh fu
nctio
ning
team
8Al
l pat
ient
nee
dsad
dres
sed
as th
ey o
ccur
8 S
hare
d kn
owle
dge
base
of
pro
vide
rs in
crea
ses
and
allo
ws e
ach
prof
essi
onal
to
resp
ond
mor
e br
oadl
yan
d ad
equa
tely
to a
ny
issu
e
Wea
knes
ses
8 S
ervi
ces
may
ove
rlap
be
dupl
icat
ed o
r eve
n wo
rk
agai
nst e
ach
othe
r
8 Im
porta
nt a
spec
ts o
f car
e m
ay n
ot b
e ad
dres
sed
or ta
ke a
long
tim
e to
be
diag
nose
d
8 S
harin
g of
info
rmat
ion
may
not
be
syst
emat
ic
enou
gh to
effe
ct o
vera
ll pa
tient
car
e
8 N
o gu
aran
tee
that
info
rshym
atio
n wi
ll ch
ange
pla
n or
st
rate
gy o
f eac
h pr
ovid
er
8 R
efer
rals
may
fail
due
to
barri
ers
lead
ing
to p
atie
nt
and
prov
ider
frus
tratio
n
8 P
roxim
ity m
ay n
ot le
ad to
gr
eate
r col
labo
ratio
nlim
iting
val
ue
8 E
ffort
is re
quire
d to
de
velo
p re
latio
nshi
ps
8 L
imite
d fle
xibili
ty if
tra
ditio
nal r
oles
are
mai
ntai
ned
8 S
yste
m is
sues
may
lim
it co
llabo
ratio
n
8 P
oten
tial f
or te
nsio
n an
d co
nflic
ting
agen
das
amon
g pr
ovid
ers
as p
ract
ice
boun
darie
s lo
osen
8 P
ract
ice
chan
ges
may
cr
eate
lack
of fi
t for
som
ees
tabl
ishe
d pr
ovid
ers
8Ti
me
is n
eede
d to
co
llabo
rate
at t
his
high
leve
l and
may
affe
ct
prac
tice
prod
uctiv
ity o
rca
denc
e of
car
e
8 S
usta
inab
ility
issu
es m
ay
stre
ss th
e pr
actic
e
8 F
ew m
odel
s at
this
leve
l wi
th e
noug
h ex
perie
nce
tosu
ppor
t val
ue
8Ou
tcom
e ex
pect
atio
ns n
otye
t est
ablis
hed
13

3 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
aBStRaCt Integration of healthcare is essential to improve the individualrsquos experience of care improve the health of the general
population and reduce per capita healthcare costs The term ldquointegrationrdquo is widely and inconsistently used to describe the bringshy
ing together of healthcare components Integration has been used to reference everything from consultation to colocation to a
setting of shared health values around treating the whole person with blurred professional boundaries There have been no fully
updated taxonomies to describe the levels of integration since the 1996 Doherty McDaniel and Baird article which initially proshy
posed five levels of integration Since this seminal issue brief and preliminary framework there have been many informal and local
adaptations However without a standard classification of integrated settings discussions of integration lack clarity and precision
and research cannot confidently examine discrete aspects of integration This issue brief reviews levels of integrated healthcare
and proposes a functional standard framework for classifying sites according to these levels
KeY WoRdS integration collaborative care mental health behavioral health collaboration healthcare
BAckgRoUnd Over the last several years as healthcare reform has taken a prominent national position and mental health and substance abuse
treatments have evolved an increasing number of articles have been written on collaboration and the integration of traditional
primary care and behavioral health practices (Butler Kane amp McAlpine 2008 Collins Hewson Munger amp Wade 2010 Funk
amp Ivbijaro 2008 Lopez Coleman-Beattie amp Sanchez 2008 Mauer 2006 2009 Mauer amp Jarvis 2010 Miller Kessler amp Peek
2011 Robinson amp Reiter 2007 Russell 2010) These articles have described a wide variety of collaborative co-located and
integrated service models
Developing a standard framework to describe integrated efforts is critical for meaningful dialogue about service design as well as
for research Until there is a way to reliably categorize integration implementations meaningful comparisons of implementations
or associated health outcomes cannot occur This point is made throughout the Miller et al 2011 paper which calls for a broader
ldquolexicon for the common terms and components for collaborative care so that research questions can be framed in a consistently
understood mannerrdquo (p 2) On the clinical side integrated care developers and implementers will benefit from recognizing the
characteristics of practice change that support evolving integration models Knowing what features of integrated healthcare impleshy
mentations lead to the most favorable and stable health outcomes will be an important contribution to the health field
A standard framework also contributes to the orderly evolution of national healthcare reform and aligns with the political and
service realities defined by Berwick Nolan and Whittington (2008) Integration is essential to achieving the triple aim of improved
experience of care improved health of populations and reduced per capita healthcare cost advocated by Berwick et al The lesshy
sons learned from a reliable comparison of models and implementations provide the best foundation to inform policy decisions on
the structure of more effective healthcare as care integration moves forward
levels oF IntegRAtIon Doherty McDaniel and Baird (1995 1996) proposed the first classification by level of Until there is a way to reliably collaboration and integration They proposed the five levels of primary care-behavioral
healthcare collaboration recognizing that collaboration and integration of care were categorize integration evolving and being communicated in wide-ranging ways Doherty et alrsquos classification
implementations meaningfulinvolved both the extent of the occurrence of collaboration and the capacity for colshy
laboration in the setting but they did not focus on specific interactions An underlying comparisons of implementationspremise of the levels was that as collaboration increased the adequate handling of
complex patients would also increase The levels recognized by Doherty et al did not or associated health outcomes prescribe a particular model as best for all healthcare settings but rather served as
a foundation from which to tease apart the strengths and limitations of a variety of cannot occur
sA
mH
sA
-HR
sA
ce
nt
eR
Fo
R I
nt
eg
RA
te
d H
eA
ltH
so
lU
tIo
ns
This issue brief uses the term behavioral health to describe mental health and substance use
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
options It was proposed that use of the levels would help organizations evaluate their setting in light of their goals for collaboration
and to assist in researching outcomes and costs associated with different collaborative models with different patient populations
In the original framework Doherty et al differentiated levels by where they were practiced the cases adequately handled at each
level and the following descriptions
8 LeveL 1ndash Minimal Collaboration Mental health and other healthcare providers work in separate facilities have separate
systems and rarely communicate about cases
8 LeveL 2 ndash Basic Collaboration at a Distance Providers have separate systems at separate sites but engage in periodic
communication about shared patients mostly through telephone and letters Providers view each other as resources
8 LeveL 3 ndash Basic Collaboration Onsite Mental health and other healthcare professionals have separate systems but share
facilities Proximity supports at least occasional face-to- face meetings and communication improves and is more regular
8 LeveL 4 ndash Close Collaboration in a Partly Integrated System Mental health and other healthcare providers share the same
sites and have some systems in common such as scheduling or charting There are regular face-to-face interactions among
primary care and behavioral health providers coordinated treatment plans for difficult patients and a basic understanding
of each otherrsquos roles and cultures
8 LeveL 5 ndash Close Collaboration in a Fully Integrated System Mental health and other healthcare professionals share the
same sites vision and systems All providers are on the same team and have developed an in-depth understanding of
each otherrsquos roles and areas of expertise
The following chart summarizes these five levels of collaboration
MINIMAL COLLAbORATION
bASIC COLLAbORATION
FROM A DISTANCE
bASIC COLLAbORATION
ONSITE
CLOSE COLLAbORATION
PARTLy INTEGRATED
FULLy INTEGRATED
8 Separate systems
8 Separate facilities
8 Communication is
8 Separate systems
8 Separate facilities
8 Periodic focused
8 Separate systems
8 Same facilities
8 Regular rare
8 Little appreciation of each otherrsquos culture
ldquoNobody knows my name Who are yourdquo
communication most written
8 View each other as outside resources
8 Little understandshying of each otherrsquos culture or sharing of influence
ldquoI help your consumersrdquo
communication occasionally face-to-face
8 Some appreciation of each otherrsquos role and general sense of large picture
8Mental health usually has more influence
ldquoI am your consultantrdquo
8Some shared systems
8Same facilities
8Face-to-Face consultation coordinated treatment plans
8Basic appreciation of each otherrsquos role and cultures
8Collaborative routines difficult time and operation barriers
8Influence sharing
ldquoWe are a team in the care of consumersrdquo
8Shared systems and facilities in seamless bio-psychosocial web
8Consumers and providers have same expectations of system(s)
8In-depth appreciation of roles and culture
8Collaborative routines are regular and smooth
8Conscious influence sharing based on situation and expertise
ldquoTogether we teach others how to be a team in care of conshysumers and design a care systemrdquo
4
5 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
These five levels have formed the foundation for most subsequent level adaptations The idea that integration occurs along a
continuum of collaboration and integration is widely supported (Collins et al 2010 Miller et al 2011 Peek 2007 Reynolds
2006 Seaburn Lorenz Gunn Gawinski amp Mauksch 1996 Strohsal 1998) and adaptations have differed in the number of levels
(from three to 10) and the categories used to differentiate or describe levels
The reason for classification whether for clinical development or research
has influenced the choice of dimensions used to define each level For
example Reynolds (2006) used the same five levels but distinguishes
between levels on the basis of functional practice categories including
access services funding governance evidence-based practice and
data usage The goal of Reynoldsrsquo adaptation is to better capture the pashy
tient and staff experience at the different levels in doing so it broadens
the levelsrsquo descriptions and characteristics
Other papers and reports have classified integrated implementations
somewhat differently MaineHealth (2009) developed a site-specific ratshy
ing of integration that has four levels along a continuum of integration
with one rating in the first level and three ratings in levels two three and four There are 18 characteristics broadly categorized
as integrated services patient- and family-centeredness and practiceorganization In the first category characteristics such as
colocation patientfamily involvement and communication with patients about integrated care are rated In the second category
characteristics such as organizational leadership for integrated care providersrsquo engagement and data systemspatient are rated
More similar to Doherty et al Blount (2003) collapsed the five levels to three coordinated co-located and integrated care Reshy
cent work to develop a lexicon or common conceptual system for collaborative care between behavioral health and primary medical
clinicians (Miller et al 2011) has also adopted these three levels in describing collaborative care practice
The Milbank report Evolving Models of Behavioral Health Integration in Primary Care (Collins et al 2010) describes eight models
of integration across a variety of settings This group uses Doherty et alrsquos five level structure and the terms coordinated co-
located and integrated to differentiate these models
PRoPosed stAndARd FRAmewoRk Doherty et al established the five levels of integration recognizing differences in integrated implementations and the various forms
collaboration took in each level Based upon the initial efforts by Doherty et al and the experience accumulated over the intervenshy
ing 17 years the authors of this paper propose a new version of the levels of collaborationintegration The proposed framework
brings together valuable aspects that have evolved since the Doherty et al paper The proposed framework also includes several
enhancements that enable it to be comprehensive enough to serve as a national standard for future discussion about integrated
healthcare allow organizations implementing integration to gauge their degree of integration against acknowledged benchmarks
and serve as a foundation for comparing healthcare outcomes between integration levels
Doherty et al established the concept of levels of implementations that followed a continuum from collaboration to integration The
proposed model in this issue brief retains some of the original categorical descriptions that continue to prove useful today Blountrsquos
use of coordination colocation and integration serve as overarching categories The Milbank report which brought together
Doherty et alrsquos five levels and Blountrsquos broader categories also informs this conceptual framework
This new level of integration framework proposes six levels of collaborationintegration While the overarching framework has three
main categories mdash coordinated co-located and integrated care mdash there are two levels of degree within each category (see Table
1) It is designed to help organizations implementing integration to evaluate their degree of integration across several levels and to
determine what next steps they may want to take to enhance their integration initiatives
Coordinated Care
8 LeveL 1 mdash Minimal Collaboration
Behavioral health and primary care providers work at separate facilities and have separate systems Providers communicate
rarely about cases When communication occurs it is usually based on a particular providerrsquos need for specific information
about a mutual patient
8 LeveL 2 mdash Basic Collaboration at a Distance
Behavioral health and primary care providers maintain separate facilities and separate systems Providers view each other
as resources and communicate periodically about shared patients These communications are typically driven by specific
issues For example a primary care physician may request copy of a psychiatric evaluation to know if there is a confirmed
psychiatric diagnosis Behavioral health is most often viewed as specialty care
Co-Located Care
8 LeveL 3 mdash Basic Collaboration Onsite
Behavioral health and primary care providers co-located in the same facility but may or may not share the same practice
space Providers still use separate systems but communication becomes more regular due to close proximity especially
by phone or email with an occasional meeting to discuss shared patients Movement of patients between practices is
most often through a referral process that has a higher likelihood of success because the practices are in the same locashy
tion Providers may feel like they are part of a larger team but the team and how it operates are not clearly defined leaving
most decisions about patient care to be done independently by individual providers
8 LeveL 4 mdash Close Collaboration with Some System Integration
There is closer collaboration among primary care and behavioral healthcare providers due to colocation in the same
practice space and there is the beginning of integration in care through some shared systems A typical model may
involve a primary care setting embedding a behavioral health provider In an embedded practice the primary care front
desk schedules all appointments and the behavioral health provider has access and enters notes in the medical record
Often complex patients with multiple healthcare issues drive the need for consultation which is done through personal
communication As professionals have more opportunity to share patients they have a better basic understanding of each
otherrsquos roles
Integrated Care
8 LeveL 5 mdash Close Collaboration Approaching an Integrated Practice
There are high levels of collaboration and integration between behavioral and primary care providers The providers begin
to function as a true team with frequent personal communication The team actively seeks system solutions as they recogshy
nize barriers to care integration for a broader range of patients However some issues like the availability of an integrated
medical record may not be readily resolved Providers understand the different roles team members need to play and they
have started to change their practice and the structure of care to better achieve patient goals
8 LeveL 6 mdash Full Collaboration in a TransformedMerged Practice
The highest level of integration involves the greatest amount of practice change Fuller collaboration between providers
has allowed antecedent system cultures (whether from two separate systems or from one evolving system) to blur into a
single transformed or merged practice Providers and patients view the operation as a single health system treating the
whole person The principle of treating the whole person is applied to all patients not just targeted groups
Key elements were added to more clearly differentiate between the levels in each overarching category For coordinated care
the key element is communication The distinction between Level 1 and Level 2 is frequency and type of communication With inshy
creased communication providers have stronger relationships and greater understanding of the importance of integrated care and
sA
mH
sA
-HR
sA
ce
nt
eR
Fo
R I
nt
eg
RA
te
d H
eA
ltH
so
lU
tIo
ns
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS 6
7 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
the skills that different providers possess This communication increases
the coordination of care between separate healthcare entities
Physical proximity is the key element for the co-located care category
Although colocation does not guarantee greater collaboration or integrashy
tion it can be beneficial Taking advantage of close proximity increases
collaboration through face-to-face contact at Level 3 It can also develop
the opportunity for trust and relationship building leading to more sharing
of systems mdash the hallmark of beginning integration at Level 4 However
providers can be co-located and have no integration of their healthcare
services Each provider can still practice independently without commushy
nicating with others and with an integrated healthcare plan Colocation
reduces time spent travelling from one practitioner to another but does not guarantee integration
At Level 5 and Level 6 practice change is the key element No site can be fully integrated without changing how both behavioral
health and primary care are practiced The requisite practice change features a blending or blurring of cultures where no one disshy
cipline predominates Across many integrated implementations at several levels almost every practitioner wants integrated care
and believes it is the direction for healthcare to move towards until they realize it requires they change how they practice It is at
that point they often try to change the concepts of their integration efforts to preserve how they currently practice
A second modification proposed to the original Doherty et al structure is the use of the terms ldquocollaborationrdquo and ldquointegrationrdquo In
this framework collaboration describes how resources mdash namely the healthcare professionals mdash are brought together integration
describes how services are delivered and practices are organized and managed This idea is similar to Strosahlrsquos (1998) concept
that collaborative care involves behavioral health working with primary care while integration is behavioral health working within
and as part of primary care Recent analysis (Mauer amp Jarvis 2010) indicates that collaboration and integration can effectively
originate in either behavioral health or primary care and requires the transformation of both into a single whole In this standard
framework both collaboration and integration (beginning at Level 3) increase in degree and complexity over the continuum for
providers while similarly decreasing for clientsindividuals
An important enhancement to the levels is also found in a restructuring of the descriptive characteristics defining each level (see
Table 1) Each of the six levels begins with a general description followed by key differentiators (see Table 2A and 2B) under the
headings clinical delivery patient experience practiceorganization and business model These characteristics help differentiate
the levels They also incorporate some of the functional categories Reynolds (2006) identified in her consumerstaff experiential
perspective of the levels of integration Kodnerrsquos (2009) integrated care domains and MaineHealthrsquos (2009) Site Assessment
Finally Table 3 describes the strengths and weaknesses of each level so that these can be built upon or addressed
Although the term behavioral health has been used throughout this proposed framework integration of substance use treatment
and primary care has not been as extensive or prevalent as integration of mental health with primary care Further work is required
to more effectively support substance use integration (Butler et al 2008 Mauer 2010)
It is worth noting that even if health outcomes improve as levels of integration increase it is not reasonable to believe that all
healthcare settings would be able to easily or even with difficulty move to increasing levels of integration As primary care and
behavioral health have evolved in their own professional silos it has been the authorsrsquo experience that the bringing together of
these services and service perspectives (usually embodied in separate agencies) into a single fully integrated healthcare system
requires a large amount of administrative political and financial investments over a long-term stepwise evolutionary process It
is important to aspire to whichever level can be best achieved practically
At Level 3 colocation may be a necessary and good starting point to build trust between separate existing systems and to estabshy
lish a shared history of improved outcomes This could lead to closer collaboration and integration of vision that moves to Level
4 implementation possibly leading from there to a Level 5 partnership Such a partnership may be the highest level attainable or
may in years to come lead to a joint venture or a merger of the organizations While this has not been fully researched merging
primary and behavioral health organizations appears necessary at this point for achieving Level 6 integration
8 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
From a data standpoint this framework also posits that integrated services should be defined by location not by an algorithm of
service code combinations A single service (eg blood pressure check or depression medication check) provided in an integrated
sitesetting is considered an integrated service because it is provided in the context of that integrated sitersquos whole person care
Conversely multiple services provided in a single visit are not by definition integrated care these services could be and all too
often are provided by separate professionals without meaningful collaboration or integration By defining the level of integration
in terms of setting the authors of this framework define the context of interventions and the values (eg care team whole health
patient-centered) that form the basis of an integrated site and integrated services The key performance indicators in an integrated
care setting are population-based health status outcomes not encounter-based processservice data Individual staff productivity
must accompany and then be replaced by population-based outcomes by site
Funding structures and accountability must also change Integrated care is not supported by fee-for-service funding structures
that stumble over same day billing restrictions and do not reimburse for consultations between providers when the patient is not
physically present or electronic contacts or a large volume of care management mdash all of which are essential for improved health
outcomes in an integrated healthcare system Fee-for-service funding can emphasize the measurement of volume rather than
quality Global or blended funding structures do support integrated healthcare and will be fiscally justified by improved patient
outcomes that reduce overall healthcare cost
conclUsIon The proposed level of integration framework is a manageable practical and conceptually sound six level framework for integrated
healthcare that begins with collaboration (how resources are brought together) and moves through colocation and increasing levels
of integration (how services are framed and delivered) This standard framework is needed for clarity and precision of communicashy
tion as well as to contribute to research and practice redesign By implication the numbering of levels suggests that the higher
the level of collaborationintegration the more potential for positive impact on health outcomes and patient experience This belief
remains a hypothesis and has not been empirically tested With further research these benefits of collaborationintegration can
be more firmly stated and can identify which aspects of the collaboration integration or combination of the two contribute most
directly to health outcomes
Even if health outcomes improve as levels of integration increase it is not practical to believe that every healthcare setting will be
able at least in the near term to implement increasing levels of integration Many integrated implementations will be constrained
by community politics trust between organizational systems financing andor differing service values
Lastly this issue brief does not presume to establish a fuller lexicon for integration and healthcare as much needed as it is The
authors leave that to others better suited to the task and hope that this paper will contribute to such a lexicon The purpose is
to help those delivering services today by presenting a conceptual framework to better understand and differentiate integrated
healthcare implementations The authors believe that this framework will inform discussions about integrated healthcare and that
its use will provide opportunity for service redesign that will lead to better conceptual and practical models of care
9 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
ReFeRences
Berwick DM Nolan TW amp Whittington J (2008) The triple aim Care health and cost Health Affairs 27(3) 759-769
Blount A (2003) Integrated primary care Organizing the evidence Families Systems amp Health 21 (2) 121-33 doi 1010371091shy75272121121
Blount A (Ed) (1998) Integrated primary care The future of medical and mental health collaboration New York Norton
Butler M Kane RL McAlpine D et al Integration of Mental HealthSubstance Abuse and Primary Care No 173 (Prepared by the Minnesota Evidence-based Practice Center under Contract No 290-02-0009) AHRQ Publication No 09-E003 Rockville MD Agency for Healthcare Research and Quality October 2008
Collins C Hewson DL Munger R amp Wade T (2010) Evolving models of behavioral health Integration in primary care Report commissioned by the Milbank Memorial Fund
Doherty W (1995) The whyrsquos and levels of collaborative family health care Family Systems Medicine 13(3-4) 275-81 doi101037h0089174
Doherty WJ McDaniel SH amp Baird MA (1996) Five levels of primary carebehavioral healthcare collaboration Behavioral Healthcare Tomorrow 25-28
Funk M and G Ivbijaro eds (2008) Integrating mental health into primary care ndash A global perspective Geneva Switzerland World Health Organization and London UK World Organization of Family Doctors Available at wwwwhointmental_healthpolicyMental20health20+20primary20care-20final20low-res20140908pdf
Kodner Dennis (2009) All together now A conceptual exploration of integrated care Healthcare Quarterly 13 (Sp) 6-15
Lopez M B Coleman-Beattie L Jahnke and K Sanchez (2008) Connecting body and mind A resource guide to integrated health care in Texas and the United States Austin TX Hogg Foundation for Mental Health
Mauer B (2006) Behavioral healthprimary care integration The four quadrant model and evidence-based practices Rockville MD National Council for Community Behavioral Healthcare
Mauer B (2009) Behavioral healthprimary care integration and the person-centered healthcare home Washington DC National Council for Community Behavioral Healthcare
Mauer B (2010) Substance use disorders and the person-centered healthcare home Rockville MD National Council for Community Behavioral Healthcare
Mauer B amp Jarvis D (2010) The business case for bidirectional integrated care Mental health and substance use services in primary care settings and primary care services in specialty mental health and substance use settings Integration Policy Initiative
Maine Health Access Foundation (2009) Site Self-Assessment
Miller BF Kessler R Peek CJ (2011) A national agenda for research in collaborative care Papers from the Collaborative Care Research Network Research Development Conference AHRQ Publication No 11-0067 Rockville MD Agency for Healthcare Research and Quality
Peek CJ (2007) Integrated Care Aids to Navigation Study packet for the Pennsylvania Eastern Ohio amp West Virginia Summit Integrating Mental Health and Primary Care Pittsburgh PA
Reynolds K (2006) Mental Health Primary Care Integration Options (Unpublished document)
Robinson PJ amp Reiter JT (2007) Behavioral consultation and primary care A guide to integrating services New York Springer
Russell L (2010) Mental health care services in primary care Tackling the issues in the context of health care reform Center for American Progress Washington DC
Seaburn Lorenz Gunn Gawinksi amp Mauksch (1996) Models of collaboration A guide for mental health professionals working with health care practitioners Basic Books
Strosahl K (1998) Integrating behavioral health and primary care services The primary mental health care model In Integrated primary care The future of medical and mental health collaboration edited by A Blount pp 139-66 New York WW Norton
Strosahl K amp Robinson P (2008) The primary care behavioral health model Applications to prevention acute care and chronic condition management In R Kessler amp D Strafford (Eds) Collaborative medicine case studies Evidence in practice New York Springer
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 1
Six
Lev
els
of C
olla
bo
ratio
nIn
tegr
atio
n (C
ore
Des
crip
tions
)
CO
OR
DIN
AT
ED
KE
y E
LEM
EN
T C
OM
MU
NIC
AT
ION
CO
LO
CA
TE
D
KE
y E
LEM
EN
T P
Hy
SIC
AL
PR
Ox
IMIT
y
INT
EG
RA
TE
D
KE
y E
LEM
EN
T P
RA
CT
ICE
CH
AN
GE
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
beh
avio
ral h
ealt
h p
rim
ary
care
an
d o
ther
hea
lth
care
pro
vid
ers
wo
rk
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
Com
mun
icat
e ab
out c
ases
on
ly ra
rely
and
und
erco
mpe
lling
circ
umst
ance
s
8 8 C
omm
unic
ate
driv
en b
y pr
ovid
er n
eed
8 M
ay n
ever
mee
t in
pers
on
8 H
ave
limite
d un
ders
tand
shyin
g of
eac
h ot
herrsquos
role
s
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
8Co
mm
unic
ate
perio
dica
llyab
out s
hare
d pa
tient
s
8 C
omm
unic
ate
driv
en b
y sp
ecifi
c pa
tient
issu
es
8 M
ay m
eet a
s pa
rt of
larg
er
com
mun
ity
8Ap
prec
iate
eac
h ot
herrsquos
ro
les
as re
sour
ces
secfi t f
o oy
n eti amli s c ya il ey
e f ar h
m ss e t
a e r
n s ece hI n w 8
Hav
e se
para
te s
yste
ms
8 C
omm
unic
ate
regu
larly
ab
out s
hare
d pa
tient
s b
y ph
one
or e
-mai
l
8 C
olla
bora
te d
riven
by
need
for e
ach
othe
rrsquos
serv
ices
and
mor
e re
liabl
e re
ferra
l
8M
eet o
ccas
iona
lly to
disc
uss
case
s du
e to
clo
sepr
oxim
ity
8 F
eel p
art o
f a la
rger
yet
no
n-fo
rmal
team
e h ey
n t h
ih e t
rti ee
w hc wya tp il
e s ica
ma e f
n s maI s 8
Sha
re s
ome
syst
ems
like
sc
hedu
ling
or m
edic
alre
cord
s
8Co
mm
unic
ate
in p
erso
nas
nee
ded
8 C
olla
bora
te d
riven
by
need
for c
onsu
ltatio
n an
dco
ordi
nate
d pl
ans
for
diffi
cult
patie
nts
8 H
ave
regu
lar f
ace-
to-fa
ce
inte
ract
ions
abo
ut s
ome
patie
nts
8 H
ave
a ba
sic
unde
rsta
ndin
g of
role
san
d cu
lture
e h all
n t erih in
gt hei ar
e w h w
s ec ya t acp ili p
e s c sa e
m f icea t
am acn s eyr hI s p t
e n m e i o rh est
y ( hi
e w ti wl )c i eca cap
e f a
e s p
mm a d s
e ae
sn
s reyh ha hI t s t 8Ac
tivel
y se
ek s
yste
m
solu
tions
toge
ther
or
deve
lop
work
-a-ro
unds
8Co
mm
unic
ate
frequ
ently
in p
erso
n
8 C
olla
bora
te d
riven
by
desi
re to
be
a m
embe
r of
the
care
team
8 H
ave
regu
lar t
eam
m
eetin
gs to
dis
cuss
ove
rall
patie
nt c
are
and
spec
ific
patie
nt is
sues
8 H
ave
an in
-dep
th u
nshyde
rsta
ndin
g of
role
s an
dcu
lture
8 H
ave
reso
lved
mos
t or a
ll sy
stem
issu
es f
unct
ioni
ng
as o
ne in
tegr
ated
sys
tem
8Co
mm
unic
ate
cons
iste
ntly
at th
e sy
stem
tea
m a
nd
indi
vidu
al le
vels
8 C
olla
bora
te d
riven
by
shar
ed c
once
pt o
f tea
mca
re
8 H
ave
form
al a
nd in
form
al
mee
tings
to s
uppo
rt in
tegr
ated
mod
el o
f car
e
8 H
ave
role
s an
d cu
lture
s th
at b
lur o
r ble
nd
10
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 2
A S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Clin
ical
Del
iver
y
Scr
eeni
ng a
nd a
sses
sshym
ent d
one
acco
rdin
g to
se
para
te p
ract
ice
mod
els
Sepa
rate
trea
tmen
t pla
ns
Ev
iden
ced-
base
d pr
actic
es (E
BP)
impl
emen
ted
sepa
rate
ly
8 8 8
Scre
enin
g ba
sed
on
sepa
rate
pra
ctic
es m
al
y be
mat
ion
ma
info
rsh
ared
thro
ugh
for
requ
ests
or H
ealth
m
atio
n Ex
chan
ges
Info
r
Sepa
rate
trea
tmen
t pl
ans
shar
ed b
ased
on
esta
blis
hed
rela
tion-
een
spec
ific
ship
s be
twvi
ders
pr
o
Sepa
rate
resp
onsi
bilit
y fo
r car
eEB
Ps
8 8 8
ree
on a
spe
cific
y
ag M
a
crite
ria fo
r mor
e ef
fect
ive
sc
reen
ing
or o
ther
ral
vice
pla
ns
ms e
in-h
ouse
refe
r
Sep
arat
e se
rwi
th s
ome
shar
ed
mat
ion
that
info
r
wled
g
info
rth
em
8
Som
e sh
ared
kno
s EB
Ps
of e
ach
othe
rrsquoes
peci
ally
for h
igh
utili
zers
88
A
gree
on
spec
ific
bas
ed o
n sc
reen
ing
abili
ty to
resp
ond
to
e tre
atm
ent
resu
lts
8
Col
labo
rativ
plan
ning
for s
peci
fic
patie
nts
Som
e EB
Ps a
nd s
ome
focu
sed
train
ing
shar
ed
on in
tere
st o
r spe
cific
po
pula
tion
need
s
8 8
Con
sist
ent s
et o
f agr
eed
upon
scr
eeni
ngs
acro
ss
disc
iplin
es w
hich
gui
de
vent
ions
e tre
atm
ent
treat
men
t int
er
8
Col
labo
rativ
plan
ning
for a
ll sh
ared
patie
nts
8
EBP
s sh
ared
acr
oss
sys-
tem
with
som
e jo
int m
onishy
torin
g of
hea
lth c
ondi
tions
fo
r som
e pa
tient
s
8
8 P
opul
atio
n-ba
sed
m
edic
al a
nd b
ehav
iora
l he
alth
scr
eeni
ng is
stan
dard
pra
ctic
e wi
thre
sults
ava
ilabl
e to
all
and
resp
onse
pro
toco
lsin
pla
ce
8On
e tre
atm
ent p
lan
for a
llpa
tient
s
8EB
Ps a
re te
am s
elec
ted
train
ed a
nd im
plem
ente
dac
ross
dis
cipl
ines
as
stan
dard
pra
ctic
e
Key
Dif
fere
ntia
tor
Pat
ien
t Exp
erie
nce
ysic
al a
nd b
eshy P
atie
nt p
hha
vior
al h
ealth
nee
ds a
re
treat
ed a
s se
para
te is
sues
otia
te
Pat
ient
mus
t neg
sepa
rate
pra
ctic
es a
nd
wn w
ith
rees
of s
ucce
ss
site
s on
thei
r oyi
ng d
egarv
8 8vi
der
P
atie
nt h
ealth
nee
ds
are
treat
ed s
epar
atel
ybu
t rec
ords
are
sha
red re
d
prom
otin
g be
tter p
ro riers
y
be re
fer
y pa
tient
s
e
arie
ty o
f bar
wled
gkn
o
Pat
ient
s m
abu
t a v
vent
man
pre
from
acc
essi
ng c
are
8 8
atie
nt h
ealth
nee
ds a
re y
y b
ws
P treat
ed s
epar
atel
y at
the
sam
e lo
catio
n
8
Clo
se p
roxim
ity a
llora
ls to
be
mor
e re
fer
succ
essf
ul a
nd e
asie
r for
ho
a
lthou
gh w ar
y v
red
ma
patie
nts
gets
refe
rvi
der
pro
8
col
labo
ratio
n m
ight
Pat
ient
nee
ds a
re tr
eate
d se
para
tely
at t
he s
ame
m h
and-
offs
to
vide
rs
site
in
clud
e wa
rot
her t
reat
men
t pro na
lly
Pat
ient
s ar
e in
ter
red
with
bet
ter f
ollo
wshyre
fer
up b
ut c
olla
bora
tion
may
st
ill b
e ex
perie
nced
as
vice
s se
para
te s
er
8 8
y
e on
Pat
ient
nee
ds a
re tr
eate
d as
a te
am fo
r sha
red
patie
nts
(for t
hose
wh
o sc
reen
pos
itiv
scre
enin
g m
easu
res)
and
sepa
rate
ly fo
r oth
ers
e to
8
Car
e is
resp
onsi
vid
entifi
ed p
atie
nt n
eeds
bvi
ders
as e a
of a
team
of p
ro w
hich
feel
s lik
need
ed
one-
stop
sho
p
8
All p
atie
nt h
ealth
nee
ds ar
e tre
ated
for a
ll pa
tient
sby
a te
am w
ho fu
nctio
n et
her
ely
tog
effe
ctiv
Pat
ient
s ex
perie
nce
a se
amle
ss re
spon
se to
all h
ealth
care
nee
ds a
s in
a u
nifie
d y
pres
ent
the
prac
tice
8 8
11
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
No
coo
rdin
atio
n or
ts
em
ent o
f e
effo
r
vide
r buy
-in
en
ratio
n or
ev
up
to
vide
rs to
man
agco
llabo
rativ
Litt
le p
roto
inte
gco
llabo
ratio
nin
divi
dual
pro
initi
ate
as ti
me
and
prac
tice
limits
allo
w
8 8
Som
e pr
actic
e le
ader
shysh
ip in
mor
e sy
stem
atic
vide
r buy
-into
al
ue
ving
nee
ded
mat
ion
shar
ing
info
r
Som
e pr
oco
llabo
ratio
n an
d v
plac
ed o
n ha
mat
ion
info
r
8 8
Org
aniza
tion
lead
ers
tive
but o
ften
colo
shysu
ppor
catio
n is
vie
wed
as
a pr
ojec
t or p
rogr
am ork
and
vide
r buy
-in to
ra
ls w
Pro mak
ing
refe
rap
prec
iatio
n of
ons
ite
vaila
bilit
y a
8 8
thro
ugh
mut
ual p
robl
em-
Org
aniza
tion
lead
ers
ratio
n t i
nteg
supp
or
solv
ing
of s
ome
syst
em
riers
ba
r
Mor
e bu
y-in
to c
once
pt
vide
rs
ratio
n bu
t not
of
inte
gco
nsis
tent
acr
oss
not
all
pro
tuni
ties
for
vide
rs
pro
usin
g op
por
inte
grat
ion
or c
ompo
nent
s
8 8
ts
w
Org
aniza
tion
lead
ers if
ra
tion
ws a
nd e
ffor
t int
egsu
ppor
fund
ing
allo
plac
ed in
sol
ving
as
man
y sy
stem
issu
es a
s w
ithou
t cha
ngshy
poss
ible
in
g fu
ndam
enta
lly h
odi
scip
lines
are
pra
ctic
ed
rate
d y
not
vide
rs
e in
pra
ctic
e
ly a
ll pr
o N
ear ag
ed in
inte
g B
uy-in
ma
y fo
r ind
ivid
ual
eng
mod
el
incl
ude
chan
g
vide
rs
stra
teg
pro
8 8
y e
ervi
ded
aniza
tion
lead
ers
t ra
tion
as p
ract
ice
Org
stro
ngly
sup
por
inte
gm
odel
with
exp
ecte
dvi
ce d
eliv
e in
ser
chan
g
for d
evel
opm
ent
rate
d ca
re a
nd a
ll In
teg
com
pone
nts
embr
aced
vide
rs a
nd a
ctiv
and
reso
urce
s pr
o
by a
ll pr
ool
vem
ent i
n pr
actic
e e
vin ch
ang
8 8
Tab
le 2
b S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs c
ont
inue
d)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Pra
ctic
eO
rgan
izat
ion
Key
Dif
fere
ntia
tor
bu
sin
ess
Mo
del
Se
para
te fu
ndin
g
No s
harin
g of
reso
urce
s
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re re
sour
ces
for
sing
le p
roje
cts
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re fa
cilit
y ex
pens
es
Sepa
rate
bill
ing
prac
tices
8 8 8
but
may
S
epar
ate
fund
ing
rant
s sta
ffing
cos
ts
shar
e g
y sh
are
offic
e
uctu
re
Ma
expe
nses
or
infra
str
Sepa
rate
bill
ing
due
to
riers
sy
stem
bar
8 8 8
Bl
ende
d fu
ndin
g ba
sed
uctu
re
on c
ontra
cts
gra
nts
or
ys to
str
agre
emen
ts
Varie
ty o
f wa
8
the
shar
ing
of a
ll ex
pens
es
Billi
ng fu
nctio
n co
mbi
ned
reed
upo
n pr
oces
s or
ag
8 8
8 8Re
sour
ces
shar
ed a
nd
hole
rate
d fu
ndin
g In
teg
base
d on
mul
tiple
sour
ces
of re
venu
e
allo
cate
d ac
ross
wpr
actic
e
Billi
ng m
axim
ized
for
rate
d m
odel
and
uc
ture
in
teg
sing
le b
illin
g st
r
8
12
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 3
Ad
vant
ages
and
Wea
knes
ses
at E
ach
Leve
l of C
olla
bo
ratio
nIn
tegr
atio
n
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Ad
van
tag
es
8 E
ach
prac
tice
can
mak
e tim
ely
and
auto
nom
ous
deci
sion
s ab
out c
are
8Re
adily
und
erst
ood
asa
prac
tice
mod
el b
y pa
tient
s an
d pr
ovid
ers
8 M
aint
ains
eac
h pr
actic
ersquos
basi
c op
erat
ing
stru
ctur
eso
cha
nge
is n
ot a
di
srup
tive
fact
or
8 P
rovi
des
som
e co
ordi
natio
n an
din
form
atio
n-sh
arin
g th
at
is h
elpf
ul to
bot
h pa
tient
san
d pr
ovid
ers
8 C
oloc
atio
n al
lows
for
mor
e di
rect
inte
ract
ion
and
com
mun
icat
ion
amon
g pr
ofes
sion
als
toim
pact
pat
ient
car
e
8 R
efer
rals
mor
e su
cces
sful
du
e to
pro
ximity
8 O
ppor
tuni
ty to
dev
elop
cl
oser
pro
fess
iona
l rel
ashytio
nshi
ps
8 R
emov
al o
f som
e sy
stem
ba
rrier
s li
ke s
epar
ate
reco
rds
allo
ws c
lose
r co
llabo
ratio
n to
occ
ur
8 B
oth
beha
vior
al h
ealth
an
d m
edic
al p
rovi
ders
ca
n be
com
e m
ore
well-
info
rmed
abo
ut w
hat e
ach
can
prov
ide
8 P
atie
nts
are
view
ed a
s sh
ared
whi
ch fa
cilit
ates
m
ore
com
plet
e tre
atm
ent
plan
s
8 H
igh
leve
l of c
olla
bora
tion
lead
s to
mor
e re
spon
sive
pa
tient
car
e in
crea
sing
en
gage
men
t and
ad
here
nce
to tr
eatm
ent
plan
s
8 P
rovi
der fl
exib
ility
in
crea
ses
as s
yste
mis
sues
and
bar
riers
are
re
solve
d
8 B
oth
prov
ider
and
pat
ient
sa
tisfa
ctio
n m
ay in
crea
se
8 O
ppor
tuni
ty to
trul
y tre
at
whol
e pe
rson
8Al
l or a
lmos
t all
syst
emba
rrier
s re
solve
d a
llowi
ng
prov
ider
s to
pra
ctic
e as
hi
gh fu
nctio
ning
team
8Al
l pat
ient
nee
dsad
dres
sed
as th
ey o
ccur
8 S
hare
d kn
owle
dge
base
of
pro
vide
rs in
crea
ses
and
allo
ws e
ach
prof
essi
onal
to
resp
ond
mor
e br
oadl
yan
d ad
equa
tely
to a
ny
issu
e
Wea
knes
ses
8 S
ervi
ces
may
ove
rlap
be
dupl
icat
ed o
r eve
n wo
rk
agai
nst e
ach
othe
r
8 Im
porta
nt a
spec
ts o
f car
e m
ay n
ot b
e ad
dres
sed
or ta
ke a
long
tim
e to
be
diag
nose
d
8 S
harin
g of
info
rmat
ion
may
not
be
syst
emat
ic
enou
gh to
effe
ct o
vera
ll pa
tient
car
e
8 N
o gu
aran
tee
that
info
rshym
atio
n wi
ll ch
ange
pla
n or
st
rate
gy o
f eac
h pr
ovid
er
8 R
efer
rals
may
fail
due
to
barri
ers
lead
ing
to p
atie
nt
and
prov
ider
frus
tratio
n
8 P
roxim
ity m
ay n
ot le
ad to
gr
eate
r col
labo
ratio
nlim
iting
val
ue
8 E
ffort
is re
quire
d to
de
velo
p re
latio
nshi
ps
8 L
imite
d fle
xibili
ty if
tra
ditio
nal r
oles
are
mai
ntai
ned
8 S
yste
m is
sues
may
lim
it co
llabo
ratio
n
8 P
oten
tial f
or te
nsio
n an
d co
nflic
ting
agen
das
amon
g pr
ovid
ers
as p
ract
ice
boun
darie
s lo
osen
8 P
ract
ice
chan
ges
may
cr
eate
lack
of fi
t for
som
ees
tabl
ishe
d pr
ovid
ers
8Ti
me
is n
eede
d to
co
llabo
rate
at t
his
high
leve
l and
may
affe
ct
prac
tice
prod
uctiv
ity o
rca
denc
e of
car
e
8 S
usta
inab
ility
issu
es m
ay
stre
ss th
e pr
actic
e
8 F
ew m
odel
s at
this
leve
l wi
th e
noug
h ex
perie
nce
tosu
ppor
t val
ue
8Ou
tcom
e ex
pect
atio
ns n
otye
t est
ablis
hed
13
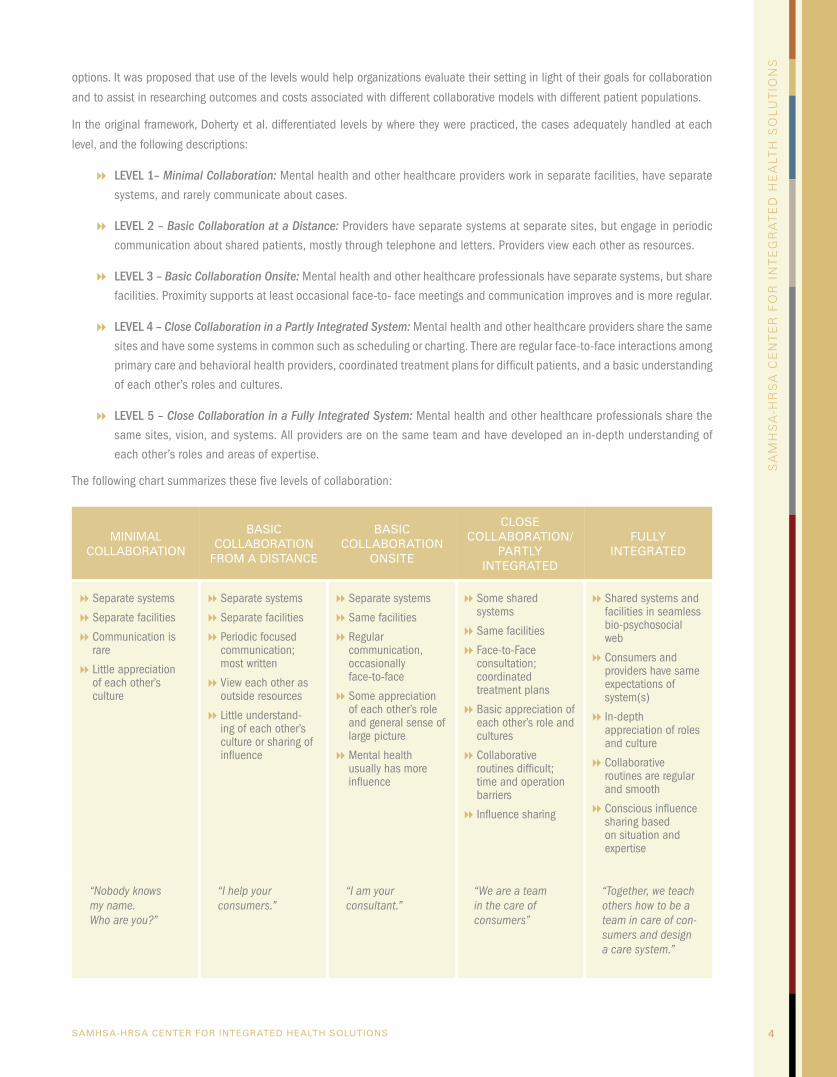
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
options It was proposed that use of the levels would help organizations evaluate their setting in light of their goals for collaboration
and to assist in researching outcomes and costs associated with different collaborative models with different patient populations
In the original framework Doherty et al differentiated levels by where they were practiced the cases adequately handled at each
level and the following descriptions
8 LeveL 1ndash Minimal Collaboration Mental health and other healthcare providers work in separate facilities have separate
systems and rarely communicate about cases
8 LeveL 2 ndash Basic Collaboration at a Distance Providers have separate systems at separate sites but engage in periodic
communication about shared patients mostly through telephone and letters Providers view each other as resources
8 LeveL 3 ndash Basic Collaboration Onsite Mental health and other healthcare professionals have separate systems but share
facilities Proximity supports at least occasional face-to- face meetings and communication improves and is more regular
8 LeveL 4 ndash Close Collaboration in a Partly Integrated System Mental health and other healthcare providers share the same
sites and have some systems in common such as scheduling or charting There are regular face-to-face interactions among
primary care and behavioral health providers coordinated treatment plans for difficult patients and a basic understanding
of each otherrsquos roles and cultures
8 LeveL 5 ndash Close Collaboration in a Fully Integrated System Mental health and other healthcare professionals share the
same sites vision and systems All providers are on the same team and have developed an in-depth understanding of
each otherrsquos roles and areas of expertise
The following chart summarizes these five levels of collaboration
MINIMAL COLLAbORATION
bASIC COLLAbORATION
FROM A DISTANCE
bASIC COLLAbORATION
ONSITE
CLOSE COLLAbORATION
PARTLy INTEGRATED
FULLy INTEGRATED
8 Separate systems
8 Separate facilities
8 Communication is
8 Separate systems
8 Separate facilities
8 Periodic focused
8 Separate systems
8 Same facilities
8 Regular rare
8 Little appreciation of each otherrsquos culture
ldquoNobody knows my name Who are yourdquo
communication most written
8 View each other as outside resources
8 Little understandshying of each otherrsquos culture or sharing of influence
ldquoI help your consumersrdquo
communication occasionally face-to-face
8 Some appreciation of each otherrsquos role and general sense of large picture
8Mental health usually has more influence
ldquoI am your consultantrdquo
8Some shared systems
8Same facilities
8Face-to-Face consultation coordinated treatment plans
8Basic appreciation of each otherrsquos role and cultures
8Collaborative routines difficult time and operation barriers
8Influence sharing
ldquoWe are a team in the care of consumersrdquo
8Shared systems and facilities in seamless bio-psychosocial web
8Consumers and providers have same expectations of system(s)
8In-depth appreciation of roles and culture
8Collaborative routines are regular and smooth
8Conscious influence sharing based on situation and expertise
ldquoTogether we teach others how to be a team in care of conshysumers and design a care systemrdquo
4
5 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
These five levels have formed the foundation for most subsequent level adaptations The idea that integration occurs along a
continuum of collaboration and integration is widely supported (Collins et al 2010 Miller et al 2011 Peek 2007 Reynolds
2006 Seaburn Lorenz Gunn Gawinski amp Mauksch 1996 Strohsal 1998) and adaptations have differed in the number of levels
(from three to 10) and the categories used to differentiate or describe levels
The reason for classification whether for clinical development or research
has influenced the choice of dimensions used to define each level For
example Reynolds (2006) used the same five levels but distinguishes
between levels on the basis of functional practice categories including
access services funding governance evidence-based practice and
data usage The goal of Reynoldsrsquo adaptation is to better capture the pashy
tient and staff experience at the different levels in doing so it broadens
the levelsrsquo descriptions and characteristics
Other papers and reports have classified integrated implementations
somewhat differently MaineHealth (2009) developed a site-specific ratshy
ing of integration that has four levels along a continuum of integration
with one rating in the first level and three ratings in levels two three and four There are 18 characteristics broadly categorized
as integrated services patient- and family-centeredness and practiceorganization In the first category characteristics such as
colocation patientfamily involvement and communication with patients about integrated care are rated In the second category
characteristics such as organizational leadership for integrated care providersrsquo engagement and data systemspatient are rated
More similar to Doherty et al Blount (2003) collapsed the five levels to three coordinated co-located and integrated care Reshy
cent work to develop a lexicon or common conceptual system for collaborative care between behavioral health and primary medical
clinicians (Miller et al 2011) has also adopted these three levels in describing collaborative care practice
The Milbank report Evolving Models of Behavioral Health Integration in Primary Care (Collins et al 2010) describes eight models
of integration across a variety of settings This group uses Doherty et alrsquos five level structure and the terms coordinated co-
located and integrated to differentiate these models
PRoPosed stAndARd FRAmewoRk Doherty et al established the five levels of integration recognizing differences in integrated implementations and the various forms
collaboration took in each level Based upon the initial efforts by Doherty et al and the experience accumulated over the intervenshy
ing 17 years the authors of this paper propose a new version of the levels of collaborationintegration The proposed framework
brings together valuable aspects that have evolved since the Doherty et al paper The proposed framework also includes several
enhancements that enable it to be comprehensive enough to serve as a national standard for future discussion about integrated
healthcare allow organizations implementing integration to gauge their degree of integration against acknowledged benchmarks
and serve as a foundation for comparing healthcare outcomes between integration levels
Doherty et al established the concept of levels of implementations that followed a continuum from collaboration to integration The
proposed model in this issue brief retains some of the original categorical descriptions that continue to prove useful today Blountrsquos
use of coordination colocation and integration serve as overarching categories The Milbank report which brought together
Doherty et alrsquos five levels and Blountrsquos broader categories also informs this conceptual framework
This new level of integration framework proposes six levels of collaborationintegration While the overarching framework has three
main categories mdash coordinated co-located and integrated care mdash there are two levels of degree within each category (see Table
1) It is designed to help organizations implementing integration to evaluate their degree of integration across several levels and to
determine what next steps they may want to take to enhance their integration initiatives
Coordinated Care
8 LeveL 1 mdash Minimal Collaboration
Behavioral health and primary care providers work at separate facilities and have separate systems Providers communicate
rarely about cases When communication occurs it is usually based on a particular providerrsquos need for specific information
about a mutual patient
8 LeveL 2 mdash Basic Collaboration at a Distance
Behavioral health and primary care providers maintain separate facilities and separate systems Providers view each other
as resources and communicate periodically about shared patients These communications are typically driven by specific
issues For example a primary care physician may request copy of a psychiatric evaluation to know if there is a confirmed
psychiatric diagnosis Behavioral health is most often viewed as specialty care
Co-Located Care
8 LeveL 3 mdash Basic Collaboration Onsite
Behavioral health and primary care providers co-located in the same facility but may or may not share the same practice
space Providers still use separate systems but communication becomes more regular due to close proximity especially
by phone or email with an occasional meeting to discuss shared patients Movement of patients between practices is
most often through a referral process that has a higher likelihood of success because the practices are in the same locashy
tion Providers may feel like they are part of a larger team but the team and how it operates are not clearly defined leaving
most decisions about patient care to be done independently by individual providers
8 LeveL 4 mdash Close Collaboration with Some System Integration
There is closer collaboration among primary care and behavioral healthcare providers due to colocation in the same
practice space and there is the beginning of integration in care through some shared systems A typical model may
involve a primary care setting embedding a behavioral health provider In an embedded practice the primary care front
desk schedules all appointments and the behavioral health provider has access and enters notes in the medical record
Often complex patients with multiple healthcare issues drive the need for consultation which is done through personal
communication As professionals have more opportunity to share patients they have a better basic understanding of each
otherrsquos roles
Integrated Care
8 LeveL 5 mdash Close Collaboration Approaching an Integrated Practice
There are high levels of collaboration and integration between behavioral and primary care providers The providers begin
to function as a true team with frequent personal communication The team actively seeks system solutions as they recogshy
nize barriers to care integration for a broader range of patients However some issues like the availability of an integrated
medical record may not be readily resolved Providers understand the different roles team members need to play and they
have started to change their practice and the structure of care to better achieve patient goals
8 LeveL 6 mdash Full Collaboration in a TransformedMerged Practice
The highest level of integration involves the greatest amount of practice change Fuller collaboration between providers
has allowed antecedent system cultures (whether from two separate systems or from one evolving system) to blur into a
single transformed or merged practice Providers and patients view the operation as a single health system treating the
whole person The principle of treating the whole person is applied to all patients not just targeted groups
Key elements were added to more clearly differentiate between the levels in each overarching category For coordinated care
the key element is communication The distinction between Level 1 and Level 2 is frequency and type of communication With inshy
creased communication providers have stronger relationships and greater understanding of the importance of integrated care and
sA
mH
sA
-HR
sA
ce
nt
eR
Fo
R I
nt
eg
RA
te
d H
eA
ltH
so
lU
tIo
ns
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS 6
7 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
the skills that different providers possess This communication increases
the coordination of care between separate healthcare entities
Physical proximity is the key element for the co-located care category
Although colocation does not guarantee greater collaboration or integrashy
tion it can be beneficial Taking advantage of close proximity increases
collaboration through face-to-face contact at Level 3 It can also develop
the opportunity for trust and relationship building leading to more sharing
of systems mdash the hallmark of beginning integration at Level 4 However
providers can be co-located and have no integration of their healthcare
services Each provider can still practice independently without commushy
nicating with others and with an integrated healthcare plan Colocation
reduces time spent travelling from one practitioner to another but does not guarantee integration
At Level 5 and Level 6 practice change is the key element No site can be fully integrated without changing how both behavioral
health and primary care are practiced The requisite practice change features a blending or blurring of cultures where no one disshy
cipline predominates Across many integrated implementations at several levels almost every practitioner wants integrated care
and believes it is the direction for healthcare to move towards until they realize it requires they change how they practice It is at
that point they often try to change the concepts of their integration efforts to preserve how they currently practice
A second modification proposed to the original Doherty et al structure is the use of the terms ldquocollaborationrdquo and ldquointegrationrdquo In
this framework collaboration describes how resources mdash namely the healthcare professionals mdash are brought together integration
describes how services are delivered and practices are organized and managed This idea is similar to Strosahlrsquos (1998) concept
that collaborative care involves behavioral health working with primary care while integration is behavioral health working within
and as part of primary care Recent analysis (Mauer amp Jarvis 2010) indicates that collaboration and integration can effectively
originate in either behavioral health or primary care and requires the transformation of both into a single whole In this standard
framework both collaboration and integration (beginning at Level 3) increase in degree and complexity over the continuum for
providers while similarly decreasing for clientsindividuals
An important enhancement to the levels is also found in a restructuring of the descriptive characteristics defining each level (see
Table 1) Each of the six levels begins with a general description followed by key differentiators (see Table 2A and 2B) under the
headings clinical delivery patient experience practiceorganization and business model These characteristics help differentiate
the levels They also incorporate some of the functional categories Reynolds (2006) identified in her consumerstaff experiential
perspective of the levels of integration Kodnerrsquos (2009) integrated care domains and MaineHealthrsquos (2009) Site Assessment
Finally Table 3 describes the strengths and weaknesses of each level so that these can be built upon or addressed
Although the term behavioral health has been used throughout this proposed framework integration of substance use treatment
and primary care has not been as extensive or prevalent as integration of mental health with primary care Further work is required
to more effectively support substance use integration (Butler et al 2008 Mauer 2010)
It is worth noting that even if health outcomes improve as levels of integration increase it is not reasonable to believe that all
healthcare settings would be able to easily or even with difficulty move to increasing levels of integration As primary care and
behavioral health have evolved in their own professional silos it has been the authorsrsquo experience that the bringing together of
these services and service perspectives (usually embodied in separate agencies) into a single fully integrated healthcare system
requires a large amount of administrative political and financial investments over a long-term stepwise evolutionary process It
is important to aspire to whichever level can be best achieved practically
At Level 3 colocation may be a necessary and good starting point to build trust between separate existing systems and to estabshy
lish a shared history of improved outcomes This could lead to closer collaboration and integration of vision that moves to Level
4 implementation possibly leading from there to a Level 5 partnership Such a partnership may be the highest level attainable or
may in years to come lead to a joint venture or a merger of the organizations While this has not been fully researched merging
primary and behavioral health organizations appears necessary at this point for achieving Level 6 integration
8 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
From a data standpoint this framework also posits that integrated services should be defined by location not by an algorithm of
service code combinations A single service (eg blood pressure check or depression medication check) provided in an integrated
sitesetting is considered an integrated service because it is provided in the context of that integrated sitersquos whole person care
Conversely multiple services provided in a single visit are not by definition integrated care these services could be and all too
often are provided by separate professionals without meaningful collaboration or integration By defining the level of integration
in terms of setting the authors of this framework define the context of interventions and the values (eg care team whole health
patient-centered) that form the basis of an integrated site and integrated services The key performance indicators in an integrated
care setting are population-based health status outcomes not encounter-based processservice data Individual staff productivity
must accompany and then be replaced by population-based outcomes by site
Funding structures and accountability must also change Integrated care is not supported by fee-for-service funding structures
that stumble over same day billing restrictions and do not reimburse for consultations between providers when the patient is not
physically present or electronic contacts or a large volume of care management mdash all of which are essential for improved health
outcomes in an integrated healthcare system Fee-for-service funding can emphasize the measurement of volume rather than
quality Global or blended funding structures do support integrated healthcare and will be fiscally justified by improved patient
outcomes that reduce overall healthcare cost
conclUsIon The proposed level of integration framework is a manageable practical and conceptually sound six level framework for integrated
healthcare that begins with collaboration (how resources are brought together) and moves through colocation and increasing levels
of integration (how services are framed and delivered) This standard framework is needed for clarity and precision of communicashy
tion as well as to contribute to research and practice redesign By implication the numbering of levels suggests that the higher
the level of collaborationintegration the more potential for positive impact on health outcomes and patient experience This belief
remains a hypothesis and has not been empirically tested With further research these benefits of collaborationintegration can
be more firmly stated and can identify which aspects of the collaboration integration or combination of the two contribute most
directly to health outcomes
Even if health outcomes improve as levels of integration increase it is not practical to believe that every healthcare setting will be
able at least in the near term to implement increasing levels of integration Many integrated implementations will be constrained
by community politics trust between organizational systems financing andor differing service values
Lastly this issue brief does not presume to establish a fuller lexicon for integration and healthcare as much needed as it is The
authors leave that to others better suited to the task and hope that this paper will contribute to such a lexicon The purpose is
to help those delivering services today by presenting a conceptual framework to better understand and differentiate integrated
healthcare implementations The authors believe that this framework will inform discussions about integrated healthcare and that
its use will provide opportunity for service redesign that will lead to better conceptual and practical models of care
9 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
ReFeRences
Berwick DM Nolan TW amp Whittington J (2008) The triple aim Care health and cost Health Affairs 27(3) 759-769
Blount A (2003) Integrated primary care Organizing the evidence Families Systems amp Health 21 (2) 121-33 doi 1010371091shy75272121121
Blount A (Ed) (1998) Integrated primary care The future of medical and mental health collaboration New York Norton
Butler M Kane RL McAlpine D et al Integration of Mental HealthSubstance Abuse and Primary Care No 173 (Prepared by the Minnesota Evidence-based Practice Center under Contract No 290-02-0009) AHRQ Publication No 09-E003 Rockville MD Agency for Healthcare Research and Quality October 2008
Collins C Hewson DL Munger R amp Wade T (2010) Evolving models of behavioral health Integration in primary care Report commissioned by the Milbank Memorial Fund
Doherty W (1995) The whyrsquos and levels of collaborative family health care Family Systems Medicine 13(3-4) 275-81 doi101037h0089174
Doherty WJ McDaniel SH amp Baird MA (1996) Five levels of primary carebehavioral healthcare collaboration Behavioral Healthcare Tomorrow 25-28
Funk M and G Ivbijaro eds (2008) Integrating mental health into primary care ndash A global perspective Geneva Switzerland World Health Organization and London UK World Organization of Family Doctors Available at wwwwhointmental_healthpolicyMental20health20+20primary20care-20final20low-res20140908pdf
Kodner Dennis (2009) All together now A conceptual exploration of integrated care Healthcare Quarterly 13 (Sp) 6-15
Lopez M B Coleman-Beattie L Jahnke and K Sanchez (2008) Connecting body and mind A resource guide to integrated health care in Texas and the United States Austin TX Hogg Foundation for Mental Health
Mauer B (2006) Behavioral healthprimary care integration The four quadrant model and evidence-based practices Rockville MD National Council for Community Behavioral Healthcare
Mauer B (2009) Behavioral healthprimary care integration and the person-centered healthcare home Washington DC National Council for Community Behavioral Healthcare
Mauer B (2010) Substance use disorders and the person-centered healthcare home Rockville MD National Council for Community Behavioral Healthcare
Mauer B amp Jarvis D (2010) The business case for bidirectional integrated care Mental health and substance use services in primary care settings and primary care services in specialty mental health and substance use settings Integration Policy Initiative
Maine Health Access Foundation (2009) Site Self-Assessment
Miller BF Kessler R Peek CJ (2011) A national agenda for research in collaborative care Papers from the Collaborative Care Research Network Research Development Conference AHRQ Publication No 11-0067 Rockville MD Agency for Healthcare Research and Quality
Peek CJ (2007) Integrated Care Aids to Navigation Study packet for the Pennsylvania Eastern Ohio amp West Virginia Summit Integrating Mental Health and Primary Care Pittsburgh PA
Reynolds K (2006) Mental Health Primary Care Integration Options (Unpublished document)
Robinson PJ amp Reiter JT (2007) Behavioral consultation and primary care A guide to integrating services New York Springer
Russell L (2010) Mental health care services in primary care Tackling the issues in the context of health care reform Center for American Progress Washington DC
Seaburn Lorenz Gunn Gawinksi amp Mauksch (1996) Models of collaboration A guide for mental health professionals working with health care practitioners Basic Books
Strosahl K (1998) Integrating behavioral health and primary care services The primary mental health care model In Integrated primary care The future of medical and mental health collaboration edited by A Blount pp 139-66 New York WW Norton
Strosahl K amp Robinson P (2008) The primary care behavioral health model Applications to prevention acute care and chronic condition management In R Kessler amp D Strafford (Eds) Collaborative medicine case studies Evidence in practice New York Springer
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 1
Six
Lev
els
of C
olla
bo
ratio
nIn
tegr
atio
n (C
ore
Des
crip
tions
)
CO
OR
DIN
AT
ED
KE
y E
LEM
EN
T C
OM
MU
NIC
AT
ION
CO
LO
CA
TE
D
KE
y E
LEM
EN
T P
Hy
SIC
AL
PR
Ox
IMIT
y
INT
EG
RA
TE
D
KE
y E
LEM
EN
T P
RA
CT
ICE
CH
AN
GE
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
beh
avio
ral h
ealt
h p
rim
ary
care
an
d o
ther
hea
lth
care
pro
vid
ers
wo
rk
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
Com
mun
icat
e ab
out c
ases
on
ly ra
rely
and
und
erco
mpe
lling
circ
umst
ance
s
8 8 C
omm
unic
ate
driv
en b
y pr
ovid
er n
eed
8 M
ay n
ever
mee
t in
pers
on
8 H
ave
limite
d un
ders
tand
shyin
g of
eac
h ot
herrsquos
role
s
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
8Co
mm
unic
ate
perio
dica
llyab
out s
hare
d pa
tient
s
8 C
omm
unic
ate
driv
en b
y sp
ecifi
c pa
tient
issu
es
8 M
ay m
eet a
s pa
rt of
larg
er
com
mun
ity
8Ap
prec
iate
eac
h ot
herrsquos
ro
les
as re
sour
ces
secfi t f
o oy
n eti amli s c ya il ey
e f ar h
m ss e t
a e r
n s ece hI n w 8
Hav
e se
para
te s
yste
ms
8 C
omm
unic
ate
regu
larly
ab
out s
hare
d pa
tient
s b
y ph
one
or e
-mai
l
8 C
olla
bora
te d
riven
by
need
for e
ach
othe
rrsquos
serv
ices
and
mor
e re
liabl
e re
ferra
l
8M
eet o
ccas
iona
lly to
disc
uss
case
s du
e to
clo
sepr
oxim
ity
8 F
eel p
art o
f a la
rger
yet
no
n-fo
rmal
team
e h ey
n t h
ih e t
rti ee
w hc wya tp il
e s ica
ma e f
n s maI s 8
Sha
re s
ome
syst
ems
like
sc
hedu
ling
or m
edic
alre
cord
s
8Co
mm
unic
ate
in p
erso
nas
nee
ded
8 C
olla
bora
te d
riven
by
need
for c
onsu
ltatio
n an
dco
ordi
nate
d pl
ans
for
diffi
cult
patie
nts
8 H
ave
regu
lar f
ace-
to-fa
ce
inte
ract
ions
abo
ut s
ome
patie
nts
8 H
ave
a ba
sic
unde
rsta
ndin
g of
role
san
d cu
lture
e h all
n t erih in
gt hei ar
e w h w
s ec ya t acp ili p
e s c sa e
m f icea t
am acn s eyr hI s p t
e n m e i o rh est
y ( hi
e w ti wl )c i eca cap
e f a
e s p
mm a d s
e ae
sn
s reyh ha hI t s t 8Ac
tivel
y se
ek s
yste
m
solu
tions
toge
ther
or
deve
lop
work
-a-ro
unds
8Co
mm
unic
ate
frequ
ently
in p
erso
n
8 C
olla
bora
te d
riven
by
desi
re to
be
a m
embe
r of
the
care
team
8 H
ave
regu
lar t
eam
m
eetin
gs to
dis
cuss
ove
rall
patie
nt c
are
and
spec
ific
patie
nt is
sues
8 H
ave
an in
-dep
th u
nshyde
rsta
ndin
g of
role
s an
dcu
lture
8 H
ave
reso
lved
mos
t or a
ll sy
stem
issu
es f
unct
ioni
ng
as o
ne in
tegr
ated
sys
tem
8Co
mm
unic
ate
cons
iste
ntly
at th
e sy
stem
tea
m a
nd
indi
vidu
al le
vels
8 C
olla
bora
te d
riven
by
shar
ed c
once
pt o
f tea
mca
re
8 H
ave
form
al a
nd in
form
al
mee
tings
to s
uppo
rt in
tegr
ated
mod
el o
f car
e
8 H
ave
role
s an
d cu
lture
s th
at b
lur o
r ble
nd
10
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 2
A S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Clin
ical
Del
iver
y
Scr
eeni
ng a
nd a
sses
sshym
ent d
one
acco
rdin
g to
se
para
te p
ract
ice
mod
els
Sepa
rate
trea
tmen
t pla
ns
Ev
iden
ced-
base
d pr
actic
es (E
BP)
impl
emen
ted
sepa
rate
ly
8 8 8
Scre
enin
g ba
sed
on
sepa
rate
pra
ctic
es m
al
y be
mat
ion
ma
info
rsh
ared
thro
ugh
for
requ
ests
or H
ealth
m
atio
n Ex
chan
ges
Info
r
Sepa
rate
trea
tmen
t pl
ans
shar
ed b
ased
on
esta
blis
hed
rela
tion-
een
spec
ific
ship
s be
twvi
ders
pr
o
Sepa
rate
resp
onsi
bilit
y fo
r car
eEB
Ps
8 8 8
ree
on a
spe
cific
y
ag M
a
crite
ria fo
r mor
e ef
fect
ive
sc
reen
ing
or o
ther
ral
vice
pla
ns
ms e
in-h
ouse
refe
r
Sep
arat
e se
rwi
th s
ome
shar
ed
mat
ion
that
info
r
wled
g
info
rth
em
8
Som
e sh
ared
kno
s EB
Ps
of e
ach
othe
rrsquoes
peci
ally
for h
igh
utili
zers
88
A
gree
on
spec
ific
bas
ed o
n sc
reen
ing
abili
ty to
resp
ond
to
e tre
atm
ent
resu
lts
8
Col
labo
rativ
plan
ning
for s
peci
fic
patie
nts
Som
e EB
Ps a
nd s
ome
focu
sed
train
ing
shar
ed
on in
tere
st o
r spe
cific
po
pula
tion
need
s
8 8
Con
sist
ent s
et o
f agr
eed
upon
scr
eeni
ngs
acro
ss
disc
iplin
es w
hich
gui
de
vent
ions
e tre
atm
ent
treat
men
t int
er
8
Col
labo
rativ
plan
ning
for a
ll sh
ared
patie
nts
8
EBP
s sh
ared
acr
oss
sys-
tem
with
som
e jo
int m
onishy
torin
g of
hea
lth c
ondi
tions
fo
r som
e pa
tient
s
8
8 P
opul
atio
n-ba
sed
m
edic
al a
nd b
ehav
iora
l he
alth
scr
eeni
ng is
stan
dard
pra
ctic
e wi
thre
sults
ava
ilabl
e to
all
and
resp
onse
pro
toco
lsin
pla
ce
8On
e tre
atm
ent p
lan
for a
llpa
tient
s
8EB
Ps a
re te
am s
elec
ted
train
ed a
nd im
plem
ente
dac
ross
dis
cipl
ines
as
stan
dard
pra
ctic
e
Key
Dif
fere
ntia
tor
Pat
ien
t Exp
erie
nce
ysic
al a
nd b
eshy P
atie
nt p
hha
vior
al h
ealth
nee
ds a
re
treat
ed a
s se
para
te is
sues
otia
te
Pat
ient
mus
t neg
sepa
rate
pra
ctic
es a
nd
wn w
ith
rees
of s
ucce
ss
site
s on
thei
r oyi
ng d
egarv
8 8vi
der
P
atie
nt h
ealth
nee
ds
are
treat
ed s
epar
atel
ybu
t rec
ords
are
sha
red re
d
prom
otin
g be
tter p
ro riers
y
be re
fer
y pa
tient
s
e
arie
ty o
f bar
wled
gkn
o
Pat
ient
s m
abu
t a v
vent
man
pre
from
acc
essi
ng c
are
8 8
atie
nt h
ealth
nee
ds a
re y
y b
ws
P treat
ed s
epar
atel
y at
the
sam
e lo
catio
n
8
Clo
se p
roxim
ity a
llora
ls to
be
mor
e re
fer
succ
essf
ul a
nd e
asie
r for
ho
a
lthou
gh w ar
y v
red
ma
patie
nts
gets
refe
rvi
der
pro
8
col
labo
ratio
n m
ight
Pat
ient
nee
ds a
re tr
eate
d se
para
tely
at t
he s
ame
m h
and-
offs
to
vide
rs
site
in
clud
e wa
rot
her t
reat
men
t pro na
lly
Pat
ient
s ar
e in
ter
red
with
bet
ter f
ollo
wshyre
fer
up b
ut c
olla
bora
tion
may
st
ill b
e ex
perie
nced
as
vice
s se
para
te s
er
8 8
y
e on
Pat
ient
nee
ds a
re tr
eate
d as
a te
am fo
r sha
red
patie
nts
(for t
hose
wh
o sc
reen
pos
itiv
scre
enin
g m
easu
res)
and
sepa
rate
ly fo
r oth
ers
e to
8
Car
e is
resp
onsi
vid
entifi
ed p
atie
nt n
eeds
bvi
ders
as e a
of a
team
of p
ro w
hich
feel
s lik
need
ed
one-
stop
sho
p
8
All p
atie
nt h
ealth
nee
ds ar
e tre
ated
for a
ll pa
tient
sby
a te
am w
ho fu
nctio
n et
her
ely
tog
effe
ctiv
Pat
ient
s ex
perie
nce
a se
amle
ss re
spon
se to
all h
ealth
care
nee
ds a
s in
a u
nifie
d y
pres
ent
the
prac
tice
8 8
11
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
No
coo
rdin
atio
n or
ts
em
ent o
f e
effo
r
vide
r buy
-in
en
ratio
n or
ev
up
to
vide
rs to
man
agco
llabo
rativ
Litt
le p
roto
inte
gco
llabo
ratio
nin
divi
dual
pro
initi
ate
as ti
me
and
prac
tice
limits
allo
w
8 8
Som
e pr
actic
e le
ader
shysh
ip in
mor
e sy
stem
atic
vide
r buy
-into
al
ue
ving
nee
ded
mat
ion
shar
ing
info
r
Som
e pr
oco
llabo
ratio
n an
d v
plac
ed o
n ha
mat
ion
info
r
8 8
Org
aniza
tion
lead
ers
tive
but o
ften
colo
shysu
ppor
catio
n is
vie
wed
as
a pr
ojec
t or p
rogr
am ork
and
vide
r buy
-in to
ra
ls w
Pro mak
ing
refe
rap
prec
iatio
n of
ons
ite
vaila
bilit
y a
8 8
thro
ugh
mut
ual p
robl
em-
Org
aniza
tion
lead
ers
ratio
n t i
nteg
supp
or
solv
ing
of s
ome
syst
em
riers
ba
r
Mor
e bu
y-in
to c
once
pt
vide
rs
ratio
n bu
t not
of
inte
gco
nsis
tent
acr
oss
not
all
pro
tuni
ties
for
vide
rs
pro
usin
g op
por
inte
grat
ion
or c
ompo
nent
s
8 8
ts
w
Org
aniza
tion
lead
ers if
ra
tion
ws a
nd e
ffor
t int
egsu
ppor
fund
ing
allo
plac
ed in
sol
ving
as
man
y sy
stem
issu
es a
s w
ithou
t cha
ngshy
poss
ible
in
g fu
ndam
enta
lly h
odi
scip
lines
are
pra
ctic
ed
rate
d y
not
vide
rs
e in
pra
ctic
e
ly a
ll pr
o N
ear ag
ed in
inte
g B
uy-in
ma
y fo
r ind
ivid
ual
eng
mod
el
incl
ude
chan
g
vide
rs
stra
teg
pro
8 8
y e
ervi
ded
aniza
tion
lead
ers
t ra
tion
as p
ract
ice
Org
stro
ngly
sup
por
inte
gm
odel
with
exp
ecte
dvi
ce d
eliv
e in
ser
chan
g
for d
evel
opm
ent
rate
d ca
re a
nd a
ll In
teg
com
pone
nts
embr
aced
vide
rs a
nd a
ctiv
and
reso
urce
s pr
o
by a
ll pr
ool
vem
ent i
n pr
actic
e e
vin ch
ang
8 8
Tab
le 2
b S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs c
ont
inue
d)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Pra
ctic
eO
rgan
izat
ion
Key
Dif
fere
ntia
tor
bu
sin
ess
Mo
del
Se
para
te fu
ndin
g
No s
harin
g of
reso
urce
s
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re re
sour
ces
for
sing
le p
roje
cts
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re fa
cilit
y ex
pens
es
Sepa
rate
bill
ing
prac
tices
8 8 8
but
may
S
epar
ate
fund
ing
rant
s sta
ffing
cos
ts
shar
e g
y sh
are
offic
e
uctu
re
Ma
expe
nses
or
infra
str
Sepa
rate
bill
ing
due
to
riers
sy
stem
bar
8 8 8
Bl
ende
d fu
ndin
g ba
sed
uctu
re
on c
ontra
cts
gra
nts
or
ys to
str
agre
emen
ts
Varie
ty o
f wa
8
the
shar
ing
of a
ll ex
pens
es
Billi
ng fu
nctio
n co
mbi
ned
reed
upo
n pr
oces
s or
ag
8 8
8 8Re
sour
ces
shar
ed a
nd
hole
rate
d fu
ndin
g In
teg
base
d on
mul
tiple
sour
ces
of re
venu
e
allo
cate
d ac
ross
wpr
actic
e
Billi
ng m
axim
ized
for
rate
d m
odel
and
uc
ture
in
teg
sing
le b
illin
g st
r
8
12
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 3
Ad
vant
ages
and
Wea
knes
ses
at E
ach
Leve
l of C
olla
bo
ratio
nIn
tegr
atio
n
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Ad
van
tag
es
8 E
ach
prac
tice
can
mak
e tim
ely
and
auto
nom
ous
deci
sion
s ab
out c
are
8Re
adily
und
erst
ood
asa
prac
tice
mod
el b
y pa
tient
s an
d pr
ovid
ers
8 M
aint
ains
eac
h pr
actic
ersquos
basi
c op
erat
ing
stru
ctur
eso
cha
nge
is n
ot a
di
srup
tive
fact
or
8 P
rovi
des
som
e co
ordi
natio
n an
din
form
atio
n-sh
arin
g th
at
is h
elpf
ul to
bot
h pa
tient
san
d pr
ovid
ers
8 C
oloc
atio
n al
lows
for
mor
e di
rect
inte
ract
ion
and
com
mun
icat
ion
amon
g pr
ofes
sion
als
toim
pact
pat
ient
car
e
8 R
efer
rals
mor
e su
cces
sful
du
e to
pro
ximity
8 O
ppor
tuni
ty to
dev
elop
cl
oser
pro
fess
iona
l rel
ashytio
nshi
ps
8 R
emov
al o
f som
e sy
stem
ba
rrier
s li
ke s
epar
ate
reco
rds
allo
ws c
lose
r co
llabo
ratio
n to
occ
ur
8 B
oth
beha
vior
al h
ealth
an
d m
edic
al p
rovi
ders
ca
n be
com
e m
ore
well-
info
rmed
abo
ut w
hat e
ach
can
prov
ide
8 P
atie
nts
are
view
ed a
s sh
ared
whi
ch fa
cilit
ates
m
ore
com
plet
e tre
atm
ent
plan
s
8 H
igh
leve
l of c
olla
bora
tion
lead
s to
mor
e re
spon
sive
pa
tient
car
e in
crea
sing
en
gage
men
t and
ad
here
nce
to tr
eatm
ent
plan
s
8 P
rovi
der fl
exib
ility
in
crea
ses
as s
yste
mis
sues
and
bar
riers
are
re
solve
d
8 B
oth
prov
ider
and
pat
ient
sa
tisfa
ctio
n m
ay in
crea
se
8 O
ppor
tuni
ty to
trul
y tre
at
whol
e pe
rson
8Al
l or a
lmos
t all
syst
emba
rrier
s re
solve
d a
llowi
ng
prov
ider
s to
pra
ctic
e as
hi
gh fu
nctio
ning
team
8Al
l pat
ient
nee
dsad
dres
sed
as th
ey o
ccur
8 S
hare
d kn
owle
dge
base
of
pro
vide
rs in
crea
ses
and
allo
ws e
ach
prof
essi
onal
to
resp
ond
mor
e br
oadl
yan
d ad
equa
tely
to a
ny
issu
e
Wea
knes
ses
8 S
ervi
ces
may
ove
rlap
be
dupl
icat
ed o
r eve
n wo
rk
agai
nst e
ach
othe
r
8 Im
porta
nt a
spec
ts o
f car
e m
ay n
ot b
e ad
dres
sed
or ta
ke a
long
tim
e to
be
diag
nose
d
8 S
harin
g of
info
rmat
ion
may
not
be
syst
emat
ic
enou
gh to
effe
ct o
vera
ll pa
tient
car
e
8 N
o gu
aran
tee
that
info
rshym
atio
n wi
ll ch
ange
pla
n or
st
rate
gy o
f eac
h pr
ovid
er
8 R
efer
rals
may
fail
due
to
barri
ers
lead
ing
to p
atie
nt
and
prov
ider
frus
tratio
n
8 P
roxim
ity m
ay n
ot le
ad to
gr
eate
r col
labo
ratio
nlim
iting
val
ue
8 E
ffort
is re
quire
d to
de
velo
p re
latio
nshi
ps
8 L
imite
d fle
xibili
ty if
tra
ditio
nal r
oles
are
mai
ntai
ned
8 S
yste
m is
sues
may
lim
it co
llabo
ratio
n
8 P
oten
tial f
or te
nsio
n an
d co
nflic
ting
agen
das
amon
g pr
ovid
ers
as p
ract
ice
boun
darie
s lo
osen
8 P
ract
ice
chan
ges
may
cr
eate
lack
of fi
t for
som
ees
tabl
ishe
d pr
ovid
ers
8Ti
me
is n
eede
d to
co
llabo
rate
at t
his
high
leve
l and
may
affe
ct
prac
tice
prod
uctiv
ity o
rca
denc
e of
car
e
8 S
usta
inab
ility
issu
es m
ay
stre
ss th
e pr
actic
e
8 F
ew m
odel
s at
this
leve
l wi
th e
noug
h ex
perie
nce
tosu
ppor
t val
ue
8Ou
tcom
e ex
pect
atio
ns n
otye
t est
ablis
hed
13

5 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
These five levels have formed the foundation for most subsequent level adaptations The idea that integration occurs along a
continuum of collaboration and integration is widely supported (Collins et al 2010 Miller et al 2011 Peek 2007 Reynolds
2006 Seaburn Lorenz Gunn Gawinski amp Mauksch 1996 Strohsal 1998) and adaptations have differed in the number of levels
(from three to 10) and the categories used to differentiate or describe levels
The reason for classification whether for clinical development or research
has influenced the choice of dimensions used to define each level For
example Reynolds (2006) used the same five levels but distinguishes
between levels on the basis of functional practice categories including
access services funding governance evidence-based practice and
data usage The goal of Reynoldsrsquo adaptation is to better capture the pashy
tient and staff experience at the different levels in doing so it broadens
the levelsrsquo descriptions and characteristics
Other papers and reports have classified integrated implementations
somewhat differently MaineHealth (2009) developed a site-specific ratshy
ing of integration that has four levels along a continuum of integration
with one rating in the first level and three ratings in levels two three and four There are 18 characteristics broadly categorized
as integrated services patient- and family-centeredness and practiceorganization In the first category characteristics such as
colocation patientfamily involvement and communication with patients about integrated care are rated In the second category
characteristics such as organizational leadership for integrated care providersrsquo engagement and data systemspatient are rated
More similar to Doherty et al Blount (2003) collapsed the five levels to three coordinated co-located and integrated care Reshy
cent work to develop a lexicon or common conceptual system for collaborative care between behavioral health and primary medical
clinicians (Miller et al 2011) has also adopted these three levels in describing collaborative care practice
The Milbank report Evolving Models of Behavioral Health Integration in Primary Care (Collins et al 2010) describes eight models
of integration across a variety of settings This group uses Doherty et alrsquos five level structure and the terms coordinated co-
located and integrated to differentiate these models
PRoPosed stAndARd FRAmewoRk Doherty et al established the five levels of integration recognizing differences in integrated implementations and the various forms
collaboration took in each level Based upon the initial efforts by Doherty et al and the experience accumulated over the intervenshy
ing 17 years the authors of this paper propose a new version of the levels of collaborationintegration The proposed framework
brings together valuable aspects that have evolved since the Doherty et al paper The proposed framework also includes several
enhancements that enable it to be comprehensive enough to serve as a national standard for future discussion about integrated
healthcare allow organizations implementing integration to gauge their degree of integration against acknowledged benchmarks
and serve as a foundation for comparing healthcare outcomes between integration levels
Doherty et al established the concept of levels of implementations that followed a continuum from collaboration to integration The
proposed model in this issue brief retains some of the original categorical descriptions that continue to prove useful today Blountrsquos
use of coordination colocation and integration serve as overarching categories The Milbank report which brought together
Doherty et alrsquos five levels and Blountrsquos broader categories also informs this conceptual framework
This new level of integration framework proposes six levels of collaborationintegration While the overarching framework has three
main categories mdash coordinated co-located and integrated care mdash there are two levels of degree within each category (see Table
1) It is designed to help organizations implementing integration to evaluate their degree of integration across several levels and to
determine what next steps they may want to take to enhance their integration initiatives
Coordinated Care
8 LeveL 1 mdash Minimal Collaboration
Behavioral health and primary care providers work at separate facilities and have separate systems Providers communicate
rarely about cases When communication occurs it is usually based on a particular providerrsquos need for specific information
about a mutual patient
8 LeveL 2 mdash Basic Collaboration at a Distance
Behavioral health and primary care providers maintain separate facilities and separate systems Providers view each other
as resources and communicate periodically about shared patients These communications are typically driven by specific
issues For example a primary care physician may request copy of a psychiatric evaluation to know if there is a confirmed
psychiatric diagnosis Behavioral health is most often viewed as specialty care
Co-Located Care
8 LeveL 3 mdash Basic Collaboration Onsite
Behavioral health and primary care providers co-located in the same facility but may or may not share the same practice
space Providers still use separate systems but communication becomes more regular due to close proximity especially
by phone or email with an occasional meeting to discuss shared patients Movement of patients between practices is
most often through a referral process that has a higher likelihood of success because the practices are in the same locashy
tion Providers may feel like they are part of a larger team but the team and how it operates are not clearly defined leaving
most decisions about patient care to be done independently by individual providers
8 LeveL 4 mdash Close Collaboration with Some System Integration
There is closer collaboration among primary care and behavioral healthcare providers due to colocation in the same
practice space and there is the beginning of integration in care through some shared systems A typical model may
involve a primary care setting embedding a behavioral health provider In an embedded practice the primary care front
desk schedules all appointments and the behavioral health provider has access and enters notes in the medical record
Often complex patients with multiple healthcare issues drive the need for consultation which is done through personal
communication As professionals have more opportunity to share patients they have a better basic understanding of each
otherrsquos roles
Integrated Care
8 LeveL 5 mdash Close Collaboration Approaching an Integrated Practice
There are high levels of collaboration and integration between behavioral and primary care providers The providers begin
to function as a true team with frequent personal communication The team actively seeks system solutions as they recogshy
nize barriers to care integration for a broader range of patients However some issues like the availability of an integrated
medical record may not be readily resolved Providers understand the different roles team members need to play and they
have started to change their practice and the structure of care to better achieve patient goals
8 LeveL 6 mdash Full Collaboration in a TransformedMerged Practice
The highest level of integration involves the greatest amount of practice change Fuller collaboration between providers
has allowed antecedent system cultures (whether from two separate systems or from one evolving system) to blur into a
single transformed or merged practice Providers and patients view the operation as a single health system treating the
whole person The principle of treating the whole person is applied to all patients not just targeted groups
Key elements were added to more clearly differentiate between the levels in each overarching category For coordinated care
the key element is communication The distinction between Level 1 and Level 2 is frequency and type of communication With inshy
creased communication providers have stronger relationships and greater understanding of the importance of integrated care and
sA
mH
sA
-HR
sA
ce
nt
eR
Fo
R I
nt
eg
RA
te
d H
eA
ltH
so
lU
tIo
ns
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS 6
7 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
the skills that different providers possess This communication increases
the coordination of care between separate healthcare entities
Physical proximity is the key element for the co-located care category
Although colocation does not guarantee greater collaboration or integrashy
tion it can be beneficial Taking advantage of close proximity increases
collaboration through face-to-face contact at Level 3 It can also develop
the opportunity for trust and relationship building leading to more sharing
of systems mdash the hallmark of beginning integration at Level 4 However
providers can be co-located and have no integration of their healthcare
services Each provider can still practice independently without commushy
nicating with others and with an integrated healthcare plan Colocation
reduces time spent travelling from one practitioner to another but does not guarantee integration
At Level 5 and Level 6 practice change is the key element No site can be fully integrated without changing how both behavioral
health and primary care are practiced The requisite practice change features a blending or blurring of cultures where no one disshy
cipline predominates Across many integrated implementations at several levels almost every practitioner wants integrated care
and believes it is the direction for healthcare to move towards until they realize it requires they change how they practice It is at
that point they often try to change the concepts of their integration efforts to preserve how they currently practice
A second modification proposed to the original Doherty et al structure is the use of the terms ldquocollaborationrdquo and ldquointegrationrdquo In
this framework collaboration describes how resources mdash namely the healthcare professionals mdash are brought together integration
describes how services are delivered and practices are organized and managed This idea is similar to Strosahlrsquos (1998) concept
that collaborative care involves behavioral health working with primary care while integration is behavioral health working within
and as part of primary care Recent analysis (Mauer amp Jarvis 2010) indicates that collaboration and integration can effectively
originate in either behavioral health or primary care and requires the transformation of both into a single whole In this standard
framework both collaboration and integration (beginning at Level 3) increase in degree and complexity over the continuum for
providers while similarly decreasing for clientsindividuals
An important enhancement to the levels is also found in a restructuring of the descriptive characteristics defining each level (see
Table 1) Each of the six levels begins with a general description followed by key differentiators (see Table 2A and 2B) under the
headings clinical delivery patient experience practiceorganization and business model These characteristics help differentiate
the levels They also incorporate some of the functional categories Reynolds (2006) identified in her consumerstaff experiential
perspective of the levels of integration Kodnerrsquos (2009) integrated care domains and MaineHealthrsquos (2009) Site Assessment
Finally Table 3 describes the strengths and weaknesses of each level so that these can be built upon or addressed
Although the term behavioral health has been used throughout this proposed framework integration of substance use treatment
and primary care has not been as extensive or prevalent as integration of mental health with primary care Further work is required
to more effectively support substance use integration (Butler et al 2008 Mauer 2010)
It is worth noting that even if health outcomes improve as levels of integration increase it is not reasonable to believe that all
healthcare settings would be able to easily or even with difficulty move to increasing levels of integration As primary care and
behavioral health have evolved in their own professional silos it has been the authorsrsquo experience that the bringing together of
these services and service perspectives (usually embodied in separate agencies) into a single fully integrated healthcare system
requires a large amount of administrative political and financial investments over a long-term stepwise evolutionary process It
is important to aspire to whichever level can be best achieved practically
At Level 3 colocation may be a necessary and good starting point to build trust between separate existing systems and to estabshy
lish a shared history of improved outcomes This could lead to closer collaboration and integration of vision that moves to Level
4 implementation possibly leading from there to a Level 5 partnership Such a partnership may be the highest level attainable or
may in years to come lead to a joint venture or a merger of the organizations While this has not been fully researched merging
primary and behavioral health organizations appears necessary at this point for achieving Level 6 integration
8 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
From a data standpoint this framework also posits that integrated services should be defined by location not by an algorithm of
service code combinations A single service (eg blood pressure check or depression medication check) provided in an integrated
sitesetting is considered an integrated service because it is provided in the context of that integrated sitersquos whole person care
Conversely multiple services provided in a single visit are not by definition integrated care these services could be and all too
often are provided by separate professionals without meaningful collaboration or integration By defining the level of integration
in terms of setting the authors of this framework define the context of interventions and the values (eg care team whole health
patient-centered) that form the basis of an integrated site and integrated services The key performance indicators in an integrated
care setting are population-based health status outcomes not encounter-based processservice data Individual staff productivity
must accompany and then be replaced by population-based outcomes by site
Funding structures and accountability must also change Integrated care is not supported by fee-for-service funding structures
that stumble over same day billing restrictions and do not reimburse for consultations between providers when the patient is not
physically present or electronic contacts or a large volume of care management mdash all of which are essential for improved health
outcomes in an integrated healthcare system Fee-for-service funding can emphasize the measurement of volume rather than
quality Global or blended funding structures do support integrated healthcare and will be fiscally justified by improved patient
outcomes that reduce overall healthcare cost
conclUsIon The proposed level of integration framework is a manageable practical and conceptually sound six level framework for integrated
healthcare that begins with collaboration (how resources are brought together) and moves through colocation and increasing levels
of integration (how services are framed and delivered) This standard framework is needed for clarity and precision of communicashy
tion as well as to contribute to research and practice redesign By implication the numbering of levels suggests that the higher
the level of collaborationintegration the more potential for positive impact on health outcomes and patient experience This belief
remains a hypothesis and has not been empirically tested With further research these benefits of collaborationintegration can
be more firmly stated and can identify which aspects of the collaboration integration or combination of the two contribute most
directly to health outcomes
Even if health outcomes improve as levels of integration increase it is not practical to believe that every healthcare setting will be
able at least in the near term to implement increasing levels of integration Many integrated implementations will be constrained
by community politics trust between organizational systems financing andor differing service values
Lastly this issue brief does not presume to establish a fuller lexicon for integration and healthcare as much needed as it is The
authors leave that to others better suited to the task and hope that this paper will contribute to such a lexicon The purpose is
to help those delivering services today by presenting a conceptual framework to better understand and differentiate integrated
healthcare implementations The authors believe that this framework will inform discussions about integrated healthcare and that
its use will provide opportunity for service redesign that will lead to better conceptual and practical models of care
9 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
ReFeRences
Berwick DM Nolan TW amp Whittington J (2008) The triple aim Care health and cost Health Affairs 27(3) 759-769
Blount A (2003) Integrated primary care Organizing the evidence Families Systems amp Health 21 (2) 121-33 doi 1010371091shy75272121121
Blount A (Ed) (1998) Integrated primary care The future of medical and mental health collaboration New York Norton
Butler M Kane RL McAlpine D et al Integration of Mental HealthSubstance Abuse and Primary Care No 173 (Prepared by the Minnesota Evidence-based Practice Center under Contract No 290-02-0009) AHRQ Publication No 09-E003 Rockville MD Agency for Healthcare Research and Quality October 2008
Collins C Hewson DL Munger R amp Wade T (2010) Evolving models of behavioral health Integration in primary care Report commissioned by the Milbank Memorial Fund
Doherty W (1995) The whyrsquos and levels of collaborative family health care Family Systems Medicine 13(3-4) 275-81 doi101037h0089174
Doherty WJ McDaniel SH amp Baird MA (1996) Five levels of primary carebehavioral healthcare collaboration Behavioral Healthcare Tomorrow 25-28
Funk M and G Ivbijaro eds (2008) Integrating mental health into primary care ndash A global perspective Geneva Switzerland World Health Organization and London UK World Organization of Family Doctors Available at wwwwhointmental_healthpolicyMental20health20+20primary20care-20final20low-res20140908pdf
Kodner Dennis (2009) All together now A conceptual exploration of integrated care Healthcare Quarterly 13 (Sp) 6-15
Lopez M B Coleman-Beattie L Jahnke and K Sanchez (2008) Connecting body and mind A resource guide to integrated health care in Texas and the United States Austin TX Hogg Foundation for Mental Health
Mauer B (2006) Behavioral healthprimary care integration The four quadrant model and evidence-based practices Rockville MD National Council for Community Behavioral Healthcare
Mauer B (2009) Behavioral healthprimary care integration and the person-centered healthcare home Washington DC National Council for Community Behavioral Healthcare
Mauer B (2010) Substance use disorders and the person-centered healthcare home Rockville MD National Council for Community Behavioral Healthcare
Mauer B amp Jarvis D (2010) The business case for bidirectional integrated care Mental health and substance use services in primary care settings and primary care services in specialty mental health and substance use settings Integration Policy Initiative
Maine Health Access Foundation (2009) Site Self-Assessment
Miller BF Kessler R Peek CJ (2011) A national agenda for research in collaborative care Papers from the Collaborative Care Research Network Research Development Conference AHRQ Publication No 11-0067 Rockville MD Agency for Healthcare Research and Quality
Peek CJ (2007) Integrated Care Aids to Navigation Study packet for the Pennsylvania Eastern Ohio amp West Virginia Summit Integrating Mental Health and Primary Care Pittsburgh PA
Reynolds K (2006) Mental Health Primary Care Integration Options (Unpublished document)
Robinson PJ amp Reiter JT (2007) Behavioral consultation and primary care A guide to integrating services New York Springer
Russell L (2010) Mental health care services in primary care Tackling the issues in the context of health care reform Center for American Progress Washington DC
Seaburn Lorenz Gunn Gawinksi amp Mauksch (1996) Models of collaboration A guide for mental health professionals working with health care practitioners Basic Books
Strosahl K (1998) Integrating behavioral health and primary care services The primary mental health care model In Integrated primary care The future of medical and mental health collaboration edited by A Blount pp 139-66 New York WW Norton
Strosahl K amp Robinson P (2008) The primary care behavioral health model Applications to prevention acute care and chronic condition management In R Kessler amp D Strafford (Eds) Collaborative medicine case studies Evidence in practice New York Springer
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 1
Six
Lev
els
of C
olla
bo
ratio
nIn
tegr
atio
n (C
ore
Des
crip
tions
)
CO
OR
DIN
AT
ED
KE
y E
LEM
EN
T C
OM
MU
NIC
AT
ION
CO
LO
CA
TE
D
KE
y E
LEM
EN
T P
Hy
SIC
AL
PR
Ox
IMIT
y
INT
EG
RA
TE
D
KE
y E
LEM
EN
T P
RA
CT
ICE
CH
AN
GE
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
beh
avio
ral h
ealt
h p
rim
ary
care
an
d o
ther
hea
lth
care
pro
vid
ers
wo
rk
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
Com
mun
icat
e ab
out c
ases
on
ly ra
rely
and
und
erco
mpe
lling
circ
umst
ance
s
8 8 C
omm
unic
ate
driv
en b
y pr
ovid
er n
eed
8 M
ay n
ever
mee
t in
pers
on
8 H
ave
limite
d un
ders
tand
shyin
g of
eac
h ot
herrsquos
role
s
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
8Co
mm
unic
ate
perio
dica
llyab
out s
hare
d pa
tient
s
8 C
omm
unic
ate
driv
en b
y sp
ecifi
c pa
tient
issu
es
8 M
ay m
eet a
s pa
rt of
larg
er
com
mun
ity
8Ap
prec
iate
eac
h ot
herrsquos
ro
les
as re
sour
ces
secfi t f
o oy
n eti amli s c ya il ey
e f ar h
m ss e t
a e r
n s ece hI n w 8
Hav
e se
para
te s
yste
ms
8 C
omm
unic
ate
regu
larly
ab
out s
hare
d pa
tient
s b
y ph
one
or e
-mai
l
8 C
olla
bora
te d
riven
by
need
for e
ach
othe
rrsquos
serv
ices
and
mor
e re
liabl
e re
ferra
l
8M
eet o
ccas
iona
lly to
disc
uss
case
s du
e to
clo
sepr
oxim
ity
8 F
eel p
art o
f a la
rger
yet
no
n-fo
rmal
team
e h ey
n t h
ih e t
rti ee
w hc wya tp il
e s ica
ma e f
n s maI s 8
Sha
re s
ome
syst
ems
like
sc
hedu
ling
or m
edic
alre
cord
s
8Co
mm
unic
ate
in p
erso
nas
nee
ded
8 C
olla
bora
te d
riven
by
need
for c
onsu
ltatio
n an
dco
ordi
nate
d pl
ans
for
diffi
cult
patie
nts
8 H
ave
regu
lar f
ace-
to-fa
ce
inte
ract
ions
abo
ut s
ome
patie
nts
8 H
ave
a ba
sic
unde
rsta
ndin
g of
role
san
d cu
lture
e h all
n t erih in
gt hei ar
e w h w
s ec ya t acp ili p
e s c sa e
m f icea t
am acn s eyr hI s p t
e n m e i o rh est
y ( hi
e w ti wl )c i eca cap
e f a
e s p
mm a d s
e ae
sn
s reyh ha hI t s t 8Ac
tivel
y se
ek s
yste
m
solu
tions
toge
ther
or
deve
lop
work
-a-ro
unds
8Co
mm
unic
ate
frequ
ently
in p
erso
n
8 C
olla
bora
te d
riven
by
desi
re to
be
a m
embe
r of
the
care
team
8 H
ave
regu
lar t
eam
m
eetin
gs to
dis
cuss
ove
rall
patie
nt c
are
and
spec
ific
patie
nt is
sues
8 H
ave
an in
-dep
th u
nshyde
rsta
ndin
g of
role
s an
dcu
lture
8 H
ave
reso
lved
mos
t or a
ll sy
stem
issu
es f
unct
ioni
ng
as o
ne in
tegr
ated
sys
tem
8Co
mm
unic
ate
cons
iste
ntly
at th
e sy
stem
tea
m a
nd
indi
vidu
al le
vels
8 C
olla
bora
te d
riven
by
shar
ed c
once
pt o
f tea
mca
re
8 H
ave
form
al a
nd in
form
al
mee
tings
to s
uppo
rt in
tegr
ated
mod
el o
f car
e
8 H
ave
role
s an
d cu
lture
s th
at b
lur o
r ble
nd
10
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 2
A S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Clin
ical
Del
iver
y
Scr
eeni
ng a
nd a
sses
sshym
ent d
one
acco
rdin
g to
se
para
te p
ract
ice
mod
els
Sepa
rate
trea
tmen
t pla
ns
Ev
iden
ced-
base
d pr
actic
es (E
BP)
impl
emen
ted
sepa
rate
ly
8 8 8
Scre
enin
g ba
sed
on
sepa
rate
pra
ctic
es m
al
y be
mat
ion
ma
info
rsh
ared
thro
ugh
for
requ
ests
or H
ealth
m
atio
n Ex
chan
ges
Info
r
Sepa
rate
trea
tmen
t pl
ans
shar
ed b
ased
on
esta
blis
hed
rela
tion-
een
spec
ific
ship
s be
twvi
ders
pr
o
Sepa
rate
resp
onsi
bilit
y fo
r car
eEB
Ps
8 8 8
ree
on a
spe
cific
y
ag M
a
crite
ria fo
r mor
e ef
fect
ive
sc
reen
ing
or o
ther
ral
vice
pla
ns
ms e
in-h
ouse
refe
r
Sep
arat
e se
rwi
th s
ome
shar
ed
mat
ion
that
info
r
wled
g
info
rth
em
8
Som
e sh
ared
kno
s EB
Ps
of e
ach
othe
rrsquoes
peci
ally
for h
igh
utili
zers
88
A
gree
on
spec
ific
bas
ed o
n sc
reen
ing
abili
ty to
resp
ond
to
e tre
atm
ent
resu
lts
8
Col
labo
rativ
plan
ning
for s
peci
fic
patie
nts
Som
e EB
Ps a
nd s
ome
focu
sed
train
ing
shar
ed
on in
tere
st o
r spe
cific
po
pula
tion
need
s
8 8
Con
sist
ent s
et o
f agr
eed
upon
scr
eeni
ngs
acro
ss
disc
iplin
es w
hich
gui
de
vent
ions
e tre
atm
ent
treat
men
t int
er
8
Col
labo
rativ
plan
ning
for a
ll sh
ared
patie
nts
8
EBP
s sh
ared
acr
oss
sys-
tem
with
som
e jo
int m
onishy
torin
g of
hea
lth c
ondi
tions
fo
r som
e pa
tient
s
8
8 P
opul
atio
n-ba
sed
m
edic
al a
nd b
ehav
iora
l he
alth
scr
eeni
ng is
stan
dard
pra
ctic
e wi
thre
sults
ava
ilabl
e to
all
and
resp
onse
pro
toco
lsin
pla
ce
8On
e tre
atm
ent p
lan
for a
llpa
tient
s
8EB
Ps a
re te
am s
elec
ted
train
ed a
nd im
plem
ente
dac
ross
dis
cipl
ines
as
stan
dard
pra
ctic
e
Key
Dif
fere
ntia
tor
Pat
ien
t Exp
erie
nce
ysic
al a
nd b
eshy P
atie
nt p
hha
vior
al h
ealth
nee
ds a
re
treat
ed a
s se
para
te is
sues
otia
te
Pat
ient
mus
t neg
sepa
rate
pra
ctic
es a
nd
wn w
ith
rees
of s
ucce
ss
site
s on
thei
r oyi
ng d
egarv
8 8vi
der
P
atie
nt h
ealth
nee
ds
are
treat
ed s
epar
atel
ybu
t rec
ords
are
sha
red re
d
prom
otin
g be
tter p
ro riers
y
be re
fer
y pa
tient
s
e
arie
ty o
f bar
wled
gkn
o
Pat
ient
s m
abu
t a v
vent
man
pre
from
acc
essi
ng c
are
8 8
atie
nt h
ealth
nee
ds a
re y
y b
ws
P treat
ed s
epar
atel
y at
the
sam
e lo
catio
n
8
Clo
se p
roxim
ity a
llora
ls to
be
mor
e re
fer
succ
essf
ul a
nd e
asie
r for
ho
a
lthou
gh w ar
y v
red
ma
patie
nts
gets
refe
rvi
der
pro
8
col
labo
ratio
n m
ight
Pat
ient
nee
ds a
re tr
eate
d se
para
tely
at t
he s
ame
m h
and-
offs
to
vide
rs
site
in
clud
e wa
rot
her t
reat
men
t pro na
lly
Pat
ient
s ar
e in
ter
red
with
bet
ter f
ollo
wshyre
fer
up b
ut c
olla
bora
tion
may
st
ill b
e ex
perie
nced
as
vice
s se
para
te s
er
8 8
y
e on
Pat
ient
nee
ds a
re tr
eate
d as
a te
am fo
r sha
red
patie
nts
(for t
hose
wh
o sc
reen
pos
itiv
scre
enin
g m
easu
res)
and
sepa
rate
ly fo
r oth
ers
e to
8
Car
e is
resp
onsi
vid
entifi
ed p
atie
nt n
eeds
bvi
ders
as e a
of a
team
of p
ro w
hich
feel
s lik
need
ed
one-
stop
sho
p
8
All p
atie
nt h
ealth
nee
ds ar
e tre
ated
for a
ll pa
tient
sby
a te
am w
ho fu
nctio
n et
her
ely
tog
effe
ctiv
Pat
ient
s ex
perie
nce
a se
amle
ss re
spon
se to
all h
ealth
care
nee
ds a
s in
a u
nifie
d y
pres
ent
the
prac
tice
8 8
11
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
No
coo
rdin
atio
n or
ts
em
ent o
f e
effo
r
vide
r buy
-in
en
ratio
n or
ev
up
to
vide
rs to
man
agco
llabo
rativ
Litt
le p
roto
inte
gco
llabo
ratio
nin
divi
dual
pro
initi
ate
as ti
me
and
prac
tice
limits
allo
w
8 8
Som
e pr
actic
e le
ader
shysh
ip in
mor
e sy
stem
atic
vide
r buy
-into
al
ue
ving
nee
ded
mat
ion
shar
ing
info
r
Som
e pr
oco
llabo
ratio
n an
d v
plac
ed o
n ha
mat
ion
info
r
8 8
Org
aniza
tion
lead
ers
tive
but o
ften
colo
shysu
ppor
catio
n is
vie
wed
as
a pr
ojec
t or p
rogr
am ork
and
vide
r buy
-in to
ra
ls w
Pro mak
ing
refe
rap
prec
iatio
n of
ons
ite
vaila
bilit
y a
8 8
thro
ugh
mut
ual p
robl
em-
Org
aniza
tion
lead
ers
ratio
n t i
nteg
supp
or
solv
ing
of s
ome
syst
em
riers
ba
r
Mor
e bu
y-in
to c
once
pt
vide
rs
ratio
n bu
t not
of
inte
gco
nsis
tent
acr
oss
not
all
pro
tuni
ties
for
vide
rs
pro
usin
g op
por
inte
grat
ion
or c
ompo
nent
s
8 8
ts
w
Org
aniza
tion
lead
ers if
ra
tion
ws a
nd e
ffor
t int
egsu
ppor
fund
ing
allo
plac
ed in
sol
ving
as
man
y sy
stem
issu
es a
s w
ithou
t cha
ngshy
poss
ible
in
g fu
ndam
enta
lly h
odi
scip
lines
are
pra
ctic
ed
rate
d y
not
vide
rs
e in
pra
ctic
e
ly a
ll pr
o N
ear ag
ed in
inte
g B
uy-in
ma
y fo
r ind
ivid
ual
eng
mod
el
incl
ude
chan
g
vide
rs
stra
teg
pro
8 8
y e
ervi
ded
aniza
tion
lead
ers
t ra
tion
as p
ract
ice
Org
stro
ngly
sup
por
inte
gm
odel
with
exp
ecte
dvi
ce d
eliv
e in
ser
chan
g
for d
evel
opm
ent
rate
d ca
re a
nd a
ll In
teg
com
pone
nts
embr
aced
vide
rs a
nd a
ctiv
and
reso
urce
s pr
o
by a
ll pr
ool
vem
ent i
n pr
actic
e e
vin ch
ang
8 8
Tab
le 2
b S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs c
ont
inue
d)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Pra
ctic
eO
rgan
izat
ion
Key
Dif
fere
ntia
tor
bu
sin
ess
Mo
del
Se
para
te fu
ndin
g
No s
harin
g of
reso
urce
s
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re re
sour
ces
for
sing
le p
roje
cts
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re fa
cilit
y ex
pens
es
Sepa
rate
bill
ing
prac
tices
8 8 8
but
may
S
epar
ate
fund
ing
rant
s sta
ffing
cos
ts
shar
e g
y sh
are
offic
e
uctu
re
Ma
expe
nses
or
infra
str
Sepa
rate
bill
ing
due
to
riers
sy
stem
bar
8 8 8
Bl
ende
d fu
ndin
g ba
sed
uctu
re
on c
ontra
cts
gra
nts
or
ys to
str
agre
emen
ts
Varie
ty o
f wa
8
the
shar
ing
of a
ll ex
pens
es
Billi
ng fu
nctio
n co
mbi
ned
reed
upo
n pr
oces
s or
ag
8 8
8 8Re
sour
ces
shar
ed a
nd
hole
rate
d fu
ndin
g In
teg
base
d on
mul
tiple
sour
ces
of re
venu
e
allo
cate
d ac
ross
wpr
actic
e
Billi
ng m
axim
ized
for
rate
d m
odel
and
uc
ture
in
teg
sing
le b
illin
g st
r
8
12
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 3
Ad
vant
ages
and
Wea
knes
ses
at E
ach
Leve
l of C
olla
bo
ratio
nIn
tegr
atio
n
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Ad
van
tag
es
8 E
ach
prac
tice
can
mak
e tim
ely
and
auto
nom
ous
deci
sion
s ab
out c
are
8Re
adily
und
erst
ood
asa
prac
tice
mod
el b
y pa
tient
s an
d pr
ovid
ers
8 M
aint
ains
eac
h pr
actic
ersquos
basi
c op
erat
ing
stru
ctur
eso
cha
nge
is n
ot a
di
srup
tive
fact
or
8 P
rovi
des
som
e co
ordi
natio
n an
din
form
atio
n-sh
arin
g th
at
is h
elpf
ul to
bot
h pa
tient
san
d pr
ovid
ers
8 C
oloc
atio
n al
lows
for
mor
e di
rect
inte
ract
ion
and
com
mun
icat
ion
amon
g pr
ofes
sion
als
toim
pact
pat
ient
car
e
8 R
efer
rals
mor
e su
cces
sful
du
e to
pro
ximity
8 O
ppor
tuni
ty to
dev
elop
cl
oser
pro
fess
iona
l rel
ashytio
nshi
ps
8 R
emov
al o
f som
e sy
stem
ba
rrier
s li
ke s
epar
ate
reco
rds
allo
ws c
lose
r co
llabo
ratio
n to
occ
ur
8 B
oth
beha
vior
al h
ealth
an
d m
edic
al p
rovi
ders
ca
n be
com
e m
ore
well-
info
rmed
abo
ut w
hat e
ach
can
prov
ide
8 P
atie
nts
are
view
ed a
s sh
ared
whi
ch fa
cilit
ates
m
ore
com
plet
e tre
atm
ent
plan
s
8 H
igh
leve
l of c
olla
bora
tion
lead
s to
mor
e re
spon
sive
pa
tient
car
e in
crea
sing
en
gage
men
t and
ad
here
nce
to tr
eatm
ent
plan
s
8 P
rovi
der fl
exib
ility
in
crea
ses
as s
yste
mis
sues
and
bar
riers
are
re
solve
d
8 B
oth
prov
ider
and
pat
ient
sa
tisfa
ctio
n m
ay in
crea
se
8 O
ppor
tuni
ty to
trul
y tre
at
whol
e pe
rson
8Al
l or a
lmos
t all
syst
emba
rrier
s re
solve
d a
llowi
ng
prov
ider
s to
pra
ctic
e as
hi
gh fu
nctio
ning
team
8Al
l pat
ient
nee
dsad
dres
sed
as th
ey o
ccur
8 S
hare
d kn
owle
dge
base
of
pro
vide
rs in
crea
ses
and
allo
ws e
ach
prof
essi
onal
to
resp
ond
mor
e br
oadl
yan
d ad
equa
tely
to a
ny
issu
e
Wea
knes
ses
8 S
ervi
ces
may
ove
rlap
be
dupl
icat
ed o
r eve
n wo
rk
agai
nst e
ach
othe
r
8 Im
porta
nt a
spec
ts o
f car
e m
ay n
ot b
e ad
dres
sed
or ta
ke a
long
tim
e to
be
diag
nose
d
8 S
harin
g of
info
rmat
ion
may
not
be
syst
emat
ic
enou
gh to
effe
ct o
vera
ll pa
tient
car
e
8 N
o gu
aran
tee
that
info
rshym
atio
n wi
ll ch
ange
pla
n or
st
rate
gy o
f eac
h pr
ovid
er
8 R
efer
rals
may
fail
due
to
barri
ers
lead
ing
to p
atie
nt
and
prov
ider
frus
tratio
n
8 P
roxim
ity m
ay n
ot le
ad to
gr
eate
r col
labo
ratio
nlim
iting
val
ue
8 E
ffort
is re
quire
d to
de
velo
p re
latio
nshi
ps
8 L
imite
d fle
xibili
ty if
tra
ditio
nal r
oles
are
mai
ntai
ned
8 S
yste
m is
sues
may
lim
it co
llabo
ratio
n
8 P
oten
tial f
or te
nsio
n an
d co
nflic
ting
agen
das
amon
g pr
ovid
ers
as p
ract
ice
boun
darie
s lo
osen
8 P
ract
ice
chan
ges
may
cr
eate
lack
of fi
t for
som
ees
tabl
ishe
d pr
ovid
ers
8Ti
me
is n
eede
d to
co
llabo
rate
at t
his
high
leve
l and
may
affe
ct
prac
tice
prod
uctiv
ity o
rca
denc
e of
car
e
8 S
usta
inab
ility
issu
es m
ay
stre
ss th
e pr
actic
e
8 F
ew m
odel
s at
this
leve
l wi
th e
noug
h ex
perie
nce
tosu
ppor
t val
ue
8Ou
tcom
e ex
pect
atio
ns n
otye
t est
ablis
hed
13

Coordinated Care
8 LeveL 1 mdash Minimal Collaboration
Behavioral health and primary care providers work at separate facilities and have separate systems Providers communicate
rarely about cases When communication occurs it is usually based on a particular providerrsquos need for specific information
about a mutual patient
8 LeveL 2 mdash Basic Collaboration at a Distance
Behavioral health and primary care providers maintain separate facilities and separate systems Providers view each other
as resources and communicate periodically about shared patients These communications are typically driven by specific
issues For example a primary care physician may request copy of a psychiatric evaluation to know if there is a confirmed
psychiatric diagnosis Behavioral health is most often viewed as specialty care
Co-Located Care
8 LeveL 3 mdash Basic Collaboration Onsite
Behavioral health and primary care providers co-located in the same facility but may or may not share the same practice
space Providers still use separate systems but communication becomes more regular due to close proximity especially
by phone or email with an occasional meeting to discuss shared patients Movement of patients between practices is
most often through a referral process that has a higher likelihood of success because the practices are in the same locashy
tion Providers may feel like they are part of a larger team but the team and how it operates are not clearly defined leaving
most decisions about patient care to be done independently by individual providers
8 LeveL 4 mdash Close Collaboration with Some System Integration
There is closer collaboration among primary care and behavioral healthcare providers due to colocation in the same
practice space and there is the beginning of integration in care through some shared systems A typical model may
involve a primary care setting embedding a behavioral health provider In an embedded practice the primary care front
desk schedules all appointments and the behavioral health provider has access and enters notes in the medical record
Often complex patients with multiple healthcare issues drive the need for consultation which is done through personal
communication As professionals have more opportunity to share patients they have a better basic understanding of each
otherrsquos roles
Integrated Care
8 LeveL 5 mdash Close Collaboration Approaching an Integrated Practice
There are high levels of collaboration and integration between behavioral and primary care providers The providers begin
to function as a true team with frequent personal communication The team actively seeks system solutions as they recogshy
nize barriers to care integration for a broader range of patients However some issues like the availability of an integrated
medical record may not be readily resolved Providers understand the different roles team members need to play and they
have started to change their practice and the structure of care to better achieve patient goals
8 LeveL 6 mdash Full Collaboration in a TransformedMerged Practice
The highest level of integration involves the greatest amount of practice change Fuller collaboration between providers
has allowed antecedent system cultures (whether from two separate systems or from one evolving system) to blur into a
single transformed or merged practice Providers and patients view the operation as a single health system treating the
whole person The principle of treating the whole person is applied to all patients not just targeted groups
Key elements were added to more clearly differentiate between the levels in each overarching category For coordinated care
the key element is communication The distinction between Level 1 and Level 2 is frequency and type of communication With inshy
creased communication providers have stronger relationships and greater understanding of the importance of integrated care and
sA
mH
sA
-HR
sA
ce
nt
eR
Fo
R I
nt
eg
RA
te
d H
eA
ltH
so
lU
tIo
ns
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS 6
7 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
the skills that different providers possess This communication increases
the coordination of care between separate healthcare entities
Physical proximity is the key element for the co-located care category
Although colocation does not guarantee greater collaboration or integrashy
tion it can be beneficial Taking advantage of close proximity increases
collaboration through face-to-face contact at Level 3 It can also develop
the opportunity for trust and relationship building leading to more sharing
of systems mdash the hallmark of beginning integration at Level 4 However
providers can be co-located and have no integration of their healthcare
services Each provider can still practice independently without commushy
nicating with others and with an integrated healthcare plan Colocation
reduces time spent travelling from one practitioner to another but does not guarantee integration
At Level 5 and Level 6 practice change is the key element No site can be fully integrated without changing how both behavioral
health and primary care are practiced The requisite practice change features a blending or blurring of cultures where no one disshy
cipline predominates Across many integrated implementations at several levels almost every practitioner wants integrated care
and believes it is the direction for healthcare to move towards until they realize it requires they change how they practice It is at
that point they often try to change the concepts of their integration efforts to preserve how they currently practice
A second modification proposed to the original Doherty et al structure is the use of the terms ldquocollaborationrdquo and ldquointegrationrdquo In
this framework collaboration describes how resources mdash namely the healthcare professionals mdash are brought together integration
describes how services are delivered and practices are organized and managed This idea is similar to Strosahlrsquos (1998) concept
that collaborative care involves behavioral health working with primary care while integration is behavioral health working within
and as part of primary care Recent analysis (Mauer amp Jarvis 2010) indicates that collaboration and integration can effectively
originate in either behavioral health or primary care and requires the transformation of both into a single whole In this standard
framework both collaboration and integration (beginning at Level 3) increase in degree and complexity over the continuum for
providers while similarly decreasing for clientsindividuals
An important enhancement to the levels is also found in a restructuring of the descriptive characteristics defining each level (see
Table 1) Each of the six levels begins with a general description followed by key differentiators (see Table 2A and 2B) under the
headings clinical delivery patient experience practiceorganization and business model These characteristics help differentiate
the levels They also incorporate some of the functional categories Reynolds (2006) identified in her consumerstaff experiential
perspective of the levels of integration Kodnerrsquos (2009) integrated care domains and MaineHealthrsquos (2009) Site Assessment
Finally Table 3 describes the strengths and weaknesses of each level so that these can be built upon or addressed
Although the term behavioral health has been used throughout this proposed framework integration of substance use treatment
and primary care has not been as extensive or prevalent as integration of mental health with primary care Further work is required
to more effectively support substance use integration (Butler et al 2008 Mauer 2010)
It is worth noting that even if health outcomes improve as levels of integration increase it is not reasonable to believe that all
healthcare settings would be able to easily or even with difficulty move to increasing levels of integration As primary care and
behavioral health have evolved in their own professional silos it has been the authorsrsquo experience that the bringing together of
these services and service perspectives (usually embodied in separate agencies) into a single fully integrated healthcare system
requires a large amount of administrative political and financial investments over a long-term stepwise evolutionary process It
is important to aspire to whichever level can be best achieved practically
At Level 3 colocation may be a necessary and good starting point to build trust between separate existing systems and to estabshy
lish a shared history of improved outcomes This could lead to closer collaboration and integration of vision that moves to Level
4 implementation possibly leading from there to a Level 5 partnership Such a partnership may be the highest level attainable or
may in years to come lead to a joint venture or a merger of the organizations While this has not been fully researched merging
primary and behavioral health organizations appears necessary at this point for achieving Level 6 integration
8 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
From a data standpoint this framework also posits that integrated services should be defined by location not by an algorithm of
service code combinations A single service (eg blood pressure check or depression medication check) provided in an integrated
sitesetting is considered an integrated service because it is provided in the context of that integrated sitersquos whole person care
Conversely multiple services provided in a single visit are not by definition integrated care these services could be and all too
often are provided by separate professionals without meaningful collaboration or integration By defining the level of integration
in terms of setting the authors of this framework define the context of interventions and the values (eg care team whole health
patient-centered) that form the basis of an integrated site and integrated services The key performance indicators in an integrated
care setting are population-based health status outcomes not encounter-based processservice data Individual staff productivity
must accompany and then be replaced by population-based outcomes by site
Funding structures and accountability must also change Integrated care is not supported by fee-for-service funding structures
that stumble over same day billing restrictions and do not reimburse for consultations between providers when the patient is not
physically present or electronic contacts or a large volume of care management mdash all of which are essential for improved health
outcomes in an integrated healthcare system Fee-for-service funding can emphasize the measurement of volume rather than
quality Global or blended funding structures do support integrated healthcare and will be fiscally justified by improved patient
outcomes that reduce overall healthcare cost
conclUsIon The proposed level of integration framework is a manageable practical and conceptually sound six level framework for integrated
healthcare that begins with collaboration (how resources are brought together) and moves through colocation and increasing levels
of integration (how services are framed and delivered) This standard framework is needed for clarity and precision of communicashy
tion as well as to contribute to research and practice redesign By implication the numbering of levels suggests that the higher
the level of collaborationintegration the more potential for positive impact on health outcomes and patient experience This belief
remains a hypothesis and has not been empirically tested With further research these benefits of collaborationintegration can
be more firmly stated and can identify which aspects of the collaboration integration or combination of the two contribute most
directly to health outcomes
Even if health outcomes improve as levels of integration increase it is not practical to believe that every healthcare setting will be
able at least in the near term to implement increasing levels of integration Many integrated implementations will be constrained
by community politics trust between organizational systems financing andor differing service values
Lastly this issue brief does not presume to establish a fuller lexicon for integration and healthcare as much needed as it is The
authors leave that to others better suited to the task and hope that this paper will contribute to such a lexicon The purpose is
to help those delivering services today by presenting a conceptual framework to better understand and differentiate integrated
healthcare implementations The authors believe that this framework will inform discussions about integrated healthcare and that
its use will provide opportunity for service redesign that will lead to better conceptual and practical models of care
9 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
ReFeRences
Berwick DM Nolan TW amp Whittington J (2008) The triple aim Care health and cost Health Affairs 27(3) 759-769
Blount A (2003) Integrated primary care Organizing the evidence Families Systems amp Health 21 (2) 121-33 doi 1010371091shy75272121121
Blount A (Ed) (1998) Integrated primary care The future of medical and mental health collaboration New York Norton
Butler M Kane RL McAlpine D et al Integration of Mental HealthSubstance Abuse and Primary Care No 173 (Prepared by the Minnesota Evidence-based Practice Center under Contract No 290-02-0009) AHRQ Publication No 09-E003 Rockville MD Agency for Healthcare Research and Quality October 2008
Collins C Hewson DL Munger R amp Wade T (2010) Evolving models of behavioral health Integration in primary care Report commissioned by the Milbank Memorial Fund
Doherty W (1995) The whyrsquos and levels of collaborative family health care Family Systems Medicine 13(3-4) 275-81 doi101037h0089174
Doherty WJ McDaniel SH amp Baird MA (1996) Five levels of primary carebehavioral healthcare collaboration Behavioral Healthcare Tomorrow 25-28
Funk M and G Ivbijaro eds (2008) Integrating mental health into primary care ndash A global perspective Geneva Switzerland World Health Organization and London UK World Organization of Family Doctors Available at wwwwhointmental_healthpolicyMental20health20+20primary20care-20final20low-res20140908pdf
Kodner Dennis (2009) All together now A conceptual exploration of integrated care Healthcare Quarterly 13 (Sp) 6-15
Lopez M B Coleman-Beattie L Jahnke and K Sanchez (2008) Connecting body and mind A resource guide to integrated health care in Texas and the United States Austin TX Hogg Foundation for Mental Health
Mauer B (2006) Behavioral healthprimary care integration The four quadrant model and evidence-based practices Rockville MD National Council for Community Behavioral Healthcare
Mauer B (2009) Behavioral healthprimary care integration and the person-centered healthcare home Washington DC National Council for Community Behavioral Healthcare
Mauer B (2010) Substance use disorders and the person-centered healthcare home Rockville MD National Council for Community Behavioral Healthcare
Mauer B amp Jarvis D (2010) The business case for bidirectional integrated care Mental health and substance use services in primary care settings and primary care services in specialty mental health and substance use settings Integration Policy Initiative
Maine Health Access Foundation (2009) Site Self-Assessment
Miller BF Kessler R Peek CJ (2011) A national agenda for research in collaborative care Papers from the Collaborative Care Research Network Research Development Conference AHRQ Publication No 11-0067 Rockville MD Agency for Healthcare Research and Quality
Peek CJ (2007) Integrated Care Aids to Navigation Study packet for the Pennsylvania Eastern Ohio amp West Virginia Summit Integrating Mental Health and Primary Care Pittsburgh PA
Reynolds K (2006) Mental Health Primary Care Integration Options (Unpublished document)
Robinson PJ amp Reiter JT (2007) Behavioral consultation and primary care A guide to integrating services New York Springer
Russell L (2010) Mental health care services in primary care Tackling the issues in the context of health care reform Center for American Progress Washington DC
Seaburn Lorenz Gunn Gawinksi amp Mauksch (1996) Models of collaboration A guide for mental health professionals working with health care practitioners Basic Books
Strosahl K (1998) Integrating behavioral health and primary care services The primary mental health care model In Integrated primary care The future of medical and mental health collaboration edited by A Blount pp 139-66 New York WW Norton
Strosahl K amp Robinson P (2008) The primary care behavioral health model Applications to prevention acute care and chronic condition management In R Kessler amp D Strafford (Eds) Collaborative medicine case studies Evidence in practice New York Springer
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 1
Six
Lev
els
of C
olla
bo
ratio
nIn
tegr
atio
n (C
ore
Des
crip
tions
)
CO
OR
DIN
AT
ED
KE
y E
LEM
EN
T C
OM
MU
NIC
AT
ION
CO
LO
CA
TE
D
KE
y E
LEM
EN
T P
Hy
SIC
AL
PR
Ox
IMIT
y
INT
EG
RA
TE
D
KE
y E
LEM
EN
T P
RA
CT
ICE
CH
AN
GE
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
beh
avio
ral h
ealt
h p
rim
ary
care
an
d o
ther
hea
lth
care
pro
vid
ers
wo
rk
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
Com
mun
icat
e ab
out c
ases
on
ly ra
rely
and
und
erco
mpe
lling
circ
umst
ance
s
8 8 C
omm
unic
ate
driv
en b
y pr
ovid
er n
eed
8 M
ay n
ever
mee
t in
pers
on
8 H
ave
limite
d un
ders
tand
shyin
g of
eac
h ot
herrsquos
role
s
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
8Co
mm
unic
ate
perio
dica
llyab
out s
hare
d pa
tient
s
8 C
omm
unic
ate
driv
en b
y sp
ecifi
c pa
tient
issu
es
8 M
ay m
eet a
s pa
rt of
larg
er
com
mun
ity
8Ap
prec
iate
eac
h ot
herrsquos
ro
les
as re
sour
ces
secfi t f
o oy
n eti amli s c ya il ey
e f ar h
m ss e t
a e r
n s ece hI n w 8
Hav
e se
para
te s
yste
ms
8 C
omm
unic
ate
regu
larly
ab
out s
hare
d pa
tient
s b
y ph
one
or e
-mai
l
8 C
olla
bora
te d
riven
by
need
for e
ach
othe
rrsquos
serv
ices
and
mor
e re
liabl
e re
ferra
l
8M
eet o
ccas
iona
lly to
disc
uss
case
s du
e to
clo
sepr
oxim
ity
8 F
eel p
art o
f a la
rger
yet
no
n-fo
rmal
team
e h ey
n t h
ih e t
rti ee
w hc wya tp il
e s ica
ma e f
n s maI s 8
Sha
re s
ome
syst
ems
like
sc
hedu
ling
or m
edic
alre
cord
s
8Co
mm
unic
ate
in p
erso
nas
nee
ded
8 C
olla
bora
te d
riven
by
need
for c
onsu
ltatio
n an
dco
ordi
nate
d pl
ans
for
diffi
cult
patie
nts
8 H
ave
regu
lar f
ace-
to-fa
ce
inte
ract
ions
abo
ut s
ome
patie
nts
8 H
ave
a ba
sic
unde
rsta
ndin
g of
role
san
d cu
lture
e h all
n t erih in
gt hei ar
e w h w
s ec ya t acp ili p
e s c sa e
m f icea t
am acn s eyr hI s p t
e n m e i o rh est
y ( hi
e w ti wl )c i eca cap
e f a
e s p
mm a d s
e ae
sn
s reyh ha hI t s t 8Ac
tivel
y se
ek s
yste
m
solu
tions
toge
ther
or
deve
lop
work
-a-ro
unds
8Co
mm
unic
ate
frequ
ently
in p
erso
n
8 C
olla
bora
te d
riven
by
desi
re to
be
a m
embe
r of
the
care
team
8 H
ave
regu
lar t
eam
m
eetin
gs to
dis
cuss
ove
rall
patie
nt c
are
and
spec
ific
patie
nt is
sues
8 H
ave
an in
-dep
th u
nshyde
rsta
ndin
g of
role
s an
dcu
lture
8 H
ave
reso
lved
mos
t or a
ll sy
stem
issu
es f
unct
ioni
ng
as o
ne in
tegr
ated
sys
tem
8Co
mm
unic
ate
cons
iste
ntly
at th
e sy
stem
tea
m a
nd
indi
vidu
al le
vels
8 C
olla
bora
te d
riven
by
shar
ed c
once
pt o
f tea
mca
re
8 H
ave
form
al a
nd in
form
al
mee
tings
to s
uppo
rt in
tegr
ated
mod
el o
f car
e
8 H
ave
role
s an
d cu
lture
s th
at b
lur o
r ble
nd
10
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 2
A S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Clin
ical
Del
iver
y
Scr
eeni
ng a
nd a
sses
sshym
ent d
one
acco
rdin
g to
se
para
te p
ract
ice
mod
els
Sepa
rate
trea
tmen
t pla
ns
Ev
iden
ced-
base
d pr
actic
es (E
BP)
impl
emen
ted
sepa
rate
ly
8 8 8
Scre
enin
g ba
sed
on
sepa
rate
pra
ctic
es m
al
y be
mat
ion
ma
info
rsh
ared
thro
ugh
for
requ
ests
or H
ealth
m
atio
n Ex
chan
ges
Info
r
Sepa
rate
trea
tmen
t pl
ans
shar
ed b
ased
on
esta
blis
hed
rela
tion-
een
spec
ific
ship
s be
twvi
ders
pr
o
Sepa
rate
resp
onsi
bilit
y fo
r car
eEB
Ps
8 8 8
ree
on a
spe
cific
y
ag M
a
crite
ria fo
r mor
e ef
fect
ive
sc
reen
ing
or o
ther
ral
vice
pla
ns
ms e
in-h
ouse
refe
r
Sep
arat
e se
rwi
th s
ome
shar
ed
mat
ion
that
info
r
wled
g
info
rth
em
8
Som
e sh
ared
kno
s EB
Ps
of e
ach
othe
rrsquoes
peci
ally
for h
igh
utili
zers
88
A
gree
on
spec
ific
bas
ed o
n sc
reen
ing
abili
ty to
resp
ond
to
e tre
atm
ent
resu
lts
8
Col
labo
rativ
plan
ning
for s
peci
fic
patie
nts
Som
e EB
Ps a
nd s
ome
focu
sed
train
ing
shar
ed
on in
tere
st o
r spe
cific
po
pula
tion
need
s
8 8
Con
sist
ent s
et o
f agr
eed
upon
scr
eeni
ngs
acro
ss
disc
iplin
es w
hich
gui
de
vent
ions
e tre
atm
ent
treat
men
t int
er
8
Col
labo
rativ
plan
ning
for a
ll sh
ared
patie
nts
8
EBP
s sh
ared
acr
oss
sys-
tem
with
som
e jo
int m
onishy
torin
g of
hea
lth c
ondi
tions
fo
r som
e pa
tient
s
8
8 P
opul
atio
n-ba
sed
m
edic
al a
nd b
ehav
iora
l he
alth
scr
eeni
ng is
stan
dard
pra
ctic
e wi
thre
sults
ava
ilabl
e to
all
and
resp
onse
pro
toco
lsin
pla
ce
8On
e tre
atm
ent p
lan
for a
llpa
tient
s
8EB
Ps a
re te
am s
elec
ted
train
ed a
nd im
plem
ente
dac
ross
dis
cipl
ines
as
stan
dard
pra
ctic
e
Key
Dif
fere
ntia
tor
Pat
ien
t Exp
erie
nce
ysic
al a
nd b
eshy P
atie
nt p
hha
vior
al h
ealth
nee
ds a
re
treat
ed a
s se
para
te is
sues
otia
te
Pat
ient
mus
t neg
sepa
rate
pra
ctic
es a
nd
wn w
ith
rees
of s
ucce
ss
site
s on
thei
r oyi
ng d
egarv
8 8vi
der
P
atie
nt h
ealth
nee
ds
are
treat
ed s
epar
atel
ybu
t rec
ords
are
sha
red re
d
prom
otin
g be
tter p
ro riers
y
be re
fer
y pa
tient
s
e
arie
ty o
f bar
wled
gkn
o
Pat
ient
s m
abu
t a v
vent
man
pre
from
acc
essi
ng c
are
8 8
atie
nt h
ealth
nee
ds a
re y
y b
ws
P treat
ed s
epar
atel
y at
the
sam
e lo
catio
n
8
Clo
se p
roxim
ity a
llora
ls to
be
mor
e re
fer
succ
essf
ul a
nd e
asie
r for
ho
a
lthou
gh w ar
y v
red
ma
patie
nts
gets
refe
rvi
der
pro
8
col
labo
ratio
n m
ight
Pat
ient
nee
ds a
re tr
eate
d se
para
tely
at t
he s
ame
m h
and-
offs
to
vide
rs
site
in
clud
e wa
rot
her t
reat
men
t pro na
lly
Pat
ient
s ar
e in
ter
red
with
bet
ter f
ollo
wshyre
fer
up b
ut c
olla
bora
tion
may
st
ill b
e ex
perie
nced
as
vice
s se
para
te s
er
8 8
y
e on
Pat
ient
nee
ds a
re tr
eate
d as
a te
am fo
r sha
red
patie
nts
(for t
hose
wh
o sc
reen
pos
itiv
scre
enin
g m
easu
res)
and
sepa
rate
ly fo
r oth
ers
e to
8
Car
e is
resp
onsi
vid
entifi
ed p
atie
nt n
eeds
bvi
ders
as e a
of a
team
of p
ro w
hich
feel
s lik
need
ed
one-
stop
sho
p
8
All p
atie
nt h
ealth
nee
ds ar
e tre
ated
for a
ll pa
tient
sby
a te
am w
ho fu
nctio
n et
her
ely
tog
effe
ctiv
Pat
ient
s ex
perie
nce
a se
amle
ss re
spon
se to
all h
ealth
care
nee
ds a
s in
a u
nifie
d y
pres
ent
the
prac
tice
8 8
11
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
No
coo
rdin
atio
n or
ts
em
ent o
f e
effo
r
vide
r buy
-in
en
ratio
n or
ev
up
to
vide
rs to
man
agco
llabo
rativ
Litt
le p
roto
inte
gco
llabo
ratio
nin
divi
dual
pro
initi
ate
as ti
me
and
prac
tice
limits
allo
w
8 8
Som
e pr
actic
e le
ader
shysh
ip in
mor
e sy
stem
atic
vide
r buy
-into
al
ue
ving
nee
ded
mat
ion
shar
ing
info
r
Som
e pr
oco
llabo
ratio
n an
d v
plac
ed o
n ha
mat
ion
info
r
8 8
Org
aniza
tion
lead
ers
tive
but o
ften
colo
shysu
ppor
catio
n is
vie
wed
as
a pr
ojec
t or p
rogr
am ork
and
vide
r buy
-in to
ra
ls w
Pro mak
ing
refe
rap
prec
iatio
n of
ons
ite
vaila
bilit
y a
8 8
thro
ugh
mut
ual p
robl
em-
Org
aniza
tion
lead
ers
ratio
n t i
nteg
supp
or
solv
ing
of s
ome
syst
em
riers
ba
r
Mor
e bu
y-in
to c
once
pt
vide
rs
ratio
n bu
t not
of
inte
gco
nsis
tent
acr
oss
not
all
pro
tuni
ties
for
vide
rs
pro
usin
g op
por
inte
grat
ion
or c
ompo
nent
s
8 8
ts
w
Org
aniza
tion
lead
ers if
ra
tion
ws a
nd e
ffor
t int
egsu
ppor
fund
ing
allo
plac
ed in
sol
ving
as
man
y sy
stem
issu
es a
s w
ithou
t cha
ngshy
poss
ible
in
g fu
ndam
enta
lly h
odi
scip
lines
are
pra
ctic
ed
rate
d y
not
vide
rs
e in
pra
ctic
e
ly a
ll pr
o N
ear ag
ed in
inte
g B
uy-in
ma
y fo
r ind
ivid
ual
eng
mod
el
incl
ude
chan
g
vide
rs
stra
teg
pro
8 8
y e
ervi
ded
aniza
tion
lead
ers
t ra
tion
as p
ract
ice
Org
stro
ngly
sup
por
inte
gm
odel
with
exp
ecte
dvi
ce d
eliv
e in
ser
chan
g
for d
evel
opm
ent
rate
d ca
re a
nd a
ll In
teg
com
pone
nts
embr
aced
vide
rs a
nd a
ctiv
and
reso
urce
s pr
o
by a
ll pr
ool
vem
ent i
n pr
actic
e e
vin ch
ang
8 8
Tab
le 2
b S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs c
ont
inue
d)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Pra
ctic
eO
rgan
izat
ion
Key
Dif
fere
ntia
tor
bu
sin
ess
Mo
del
Se
para
te fu
ndin
g
No s
harin
g of
reso
urce
s
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re re
sour
ces
for
sing
le p
roje
cts
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re fa
cilit
y ex
pens
es
Sepa
rate
bill
ing
prac
tices
8 8 8
but
may
S
epar
ate
fund
ing
rant
s sta
ffing
cos
ts
shar
e g
y sh
are
offic
e
uctu
re
Ma
expe
nses
or
infra
str
Sepa
rate
bill
ing
due
to
riers
sy
stem
bar
8 8 8
Bl
ende
d fu
ndin
g ba
sed
uctu
re
on c
ontra
cts
gra
nts
or
ys to
str
agre
emen
ts
Varie
ty o
f wa
8
the
shar
ing
of a
ll ex
pens
es
Billi
ng fu
nctio
n co
mbi
ned
reed
upo
n pr
oces
s or
ag
8 8
8 8Re
sour
ces
shar
ed a
nd
hole
rate
d fu
ndin
g In
teg
base
d on
mul
tiple
sour
ces
of re
venu
e
allo
cate
d ac
ross
wpr
actic
e
Billi
ng m
axim
ized
for
rate
d m
odel
and
uc
ture
in
teg
sing
le b
illin
g st
r
8
12
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 3
Ad
vant
ages
and
Wea
knes
ses
at E
ach
Leve
l of C
olla
bo
ratio
nIn
tegr
atio
n
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Ad
van
tag
es
8 E
ach
prac
tice
can
mak
e tim
ely
and
auto
nom
ous
deci
sion
s ab
out c
are
8Re
adily
und
erst
ood
asa
prac
tice
mod
el b
y pa
tient
s an
d pr
ovid
ers
8 M
aint
ains
eac
h pr
actic
ersquos
basi
c op
erat
ing
stru
ctur
eso
cha
nge
is n
ot a
di
srup
tive
fact
or
8 P
rovi
des
som
e co
ordi
natio
n an
din
form
atio
n-sh
arin
g th
at
is h
elpf
ul to
bot
h pa
tient
san
d pr
ovid
ers
8 C
oloc
atio
n al
lows
for
mor
e di
rect
inte
ract
ion
and
com
mun
icat
ion
amon
g pr
ofes
sion
als
toim
pact
pat
ient
car
e
8 R
efer
rals
mor
e su
cces
sful
du
e to
pro
ximity
8 O
ppor
tuni
ty to
dev
elop
cl
oser
pro
fess
iona
l rel
ashytio
nshi
ps
8 R
emov
al o
f som
e sy
stem
ba
rrier
s li
ke s
epar
ate
reco
rds
allo
ws c
lose
r co
llabo
ratio
n to
occ
ur
8 B
oth
beha
vior
al h
ealth
an
d m
edic
al p
rovi
ders
ca
n be
com
e m
ore
well-
info
rmed
abo
ut w
hat e
ach
can
prov
ide
8 P
atie
nts
are
view
ed a
s sh
ared
whi
ch fa
cilit
ates
m
ore
com
plet
e tre
atm
ent
plan
s
8 H
igh
leve
l of c
olla
bora
tion
lead
s to
mor
e re
spon
sive
pa
tient
car
e in
crea
sing
en
gage
men
t and
ad
here
nce
to tr
eatm
ent
plan
s
8 P
rovi
der fl
exib
ility
in
crea
ses
as s
yste
mis
sues
and
bar
riers
are
re
solve
d
8 B
oth
prov
ider
and
pat
ient
sa
tisfa
ctio
n m
ay in
crea
se
8 O
ppor
tuni
ty to
trul
y tre
at
whol
e pe
rson
8Al
l or a
lmos
t all
syst
emba
rrier
s re
solve
d a
llowi
ng
prov
ider
s to
pra
ctic
e as
hi
gh fu
nctio
ning
team
8Al
l pat
ient
nee
dsad
dres
sed
as th
ey o
ccur
8 S
hare
d kn
owle
dge
base
of
pro
vide
rs in
crea
ses
and
allo
ws e
ach
prof
essi
onal
to
resp
ond
mor
e br
oadl
yan
d ad
equa
tely
to a
ny
issu
e
Wea
knes
ses
8 S
ervi
ces
may
ove
rlap
be
dupl
icat
ed o
r eve
n wo
rk
agai
nst e
ach
othe
r
8 Im
porta
nt a
spec
ts o
f car
e m
ay n
ot b
e ad
dres
sed
or ta
ke a
long
tim
e to
be
diag
nose
d
8 S
harin
g of
info
rmat
ion
may
not
be
syst
emat
ic
enou
gh to
effe
ct o
vera
ll pa
tient
car
e
8 N
o gu
aran
tee
that
info
rshym
atio
n wi
ll ch
ange
pla
n or
st
rate
gy o
f eac
h pr
ovid
er
8 R
efer
rals
may
fail
due
to
barri
ers
lead
ing
to p
atie
nt
and
prov
ider
frus
tratio
n
8 P
roxim
ity m
ay n
ot le
ad to
gr
eate
r col
labo
ratio
nlim
iting
val
ue
8 E
ffort
is re
quire
d to
de
velo
p re
latio
nshi
ps
8 L
imite
d fle
xibili
ty if
tra
ditio
nal r
oles
are
mai
ntai
ned
8 S
yste
m is
sues
may
lim
it co
llabo
ratio
n
8 P
oten
tial f
or te
nsio
n an
d co
nflic
ting
agen
das
amon
g pr
ovid
ers
as p
ract
ice
boun
darie
s lo
osen
8 P
ract
ice
chan
ges
may
cr
eate
lack
of fi
t for
som
ees
tabl
ishe
d pr
ovid
ers
8Ti
me
is n
eede
d to
co
llabo
rate
at t
his
high
leve
l and
may
affe
ct
prac
tice
prod
uctiv
ity o
rca
denc
e of
car
e
8 S
usta
inab
ility
issu
es m
ay
stre
ss th
e pr
actic
e
8 F
ew m
odel
s at
this
leve
l wi
th e
noug
h ex
perie
nce
tosu
ppor
t val
ue
8Ou
tcom
e ex
pect
atio
ns n
otye
t est
ablis
hed
13

7 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
the skills that different providers possess This communication increases
the coordination of care between separate healthcare entities
Physical proximity is the key element for the co-located care category
Although colocation does not guarantee greater collaboration or integrashy
tion it can be beneficial Taking advantage of close proximity increases
collaboration through face-to-face contact at Level 3 It can also develop
the opportunity for trust and relationship building leading to more sharing
of systems mdash the hallmark of beginning integration at Level 4 However
providers can be co-located and have no integration of their healthcare
services Each provider can still practice independently without commushy
nicating with others and with an integrated healthcare plan Colocation
reduces time spent travelling from one practitioner to another but does not guarantee integration
At Level 5 and Level 6 practice change is the key element No site can be fully integrated without changing how both behavioral
health and primary care are practiced The requisite practice change features a blending or blurring of cultures where no one disshy
cipline predominates Across many integrated implementations at several levels almost every practitioner wants integrated care
and believes it is the direction for healthcare to move towards until they realize it requires they change how they practice It is at
that point they often try to change the concepts of their integration efforts to preserve how they currently practice
A second modification proposed to the original Doherty et al structure is the use of the terms ldquocollaborationrdquo and ldquointegrationrdquo In
this framework collaboration describes how resources mdash namely the healthcare professionals mdash are brought together integration
describes how services are delivered and practices are organized and managed This idea is similar to Strosahlrsquos (1998) concept
that collaborative care involves behavioral health working with primary care while integration is behavioral health working within
and as part of primary care Recent analysis (Mauer amp Jarvis 2010) indicates that collaboration and integration can effectively
originate in either behavioral health or primary care and requires the transformation of both into a single whole In this standard
framework both collaboration and integration (beginning at Level 3) increase in degree and complexity over the continuum for
providers while similarly decreasing for clientsindividuals
An important enhancement to the levels is also found in a restructuring of the descriptive characteristics defining each level (see
Table 1) Each of the six levels begins with a general description followed by key differentiators (see Table 2A and 2B) under the
headings clinical delivery patient experience practiceorganization and business model These characteristics help differentiate
the levels They also incorporate some of the functional categories Reynolds (2006) identified in her consumerstaff experiential
perspective of the levels of integration Kodnerrsquos (2009) integrated care domains and MaineHealthrsquos (2009) Site Assessment
Finally Table 3 describes the strengths and weaknesses of each level so that these can be built upon or addressed
Although the term behavioral health has been used throughout this proposed framework integration of substance use treatment
and primary care has not been as extensive or prevalent as integration of mental health with primary care Further work is required
to more effectively support substance use integration (Butler et al 2008 Mauer 2010)
It is worth noting that even if health outcomes improve as levels of integration increase it is not reasonable to believe that all
healthcare settings would be able to easily or even with difficulty move to increasing levels of integration As primary care and
behavioral health have evolved in their own professional silos it has been the authorsrsquo experience that the bringing together of
these services and service perspectives (usually embodied in separate agencies) into a single fully integrated healthcare system
requires a large amount of administrative political and financial investments over a long-term stepwise evolutionary process It
is important to aspire to whichever level can be best achieved practically
At Level 3 colocation may be a necessary and good starting point to build trust between separate existing systems and to estabshy
lish a shared history of improved outcomes This could lead to closer collaboration and integration of vision that moves to Level
4 implementation possibly leading from there to a Level 5 partnership Such a partnership may be the highest level attainable or
may in years to come lead to a joint venture or a merger of the organizations While this has not been fully researched merging
primary and behavioral health organizations appears necessary at this point for achieving Level 6 integration
8 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
From a data standpoint this framework also posits that integrated services should be defined by location not by an algorithm of
service code combinations A single service (eg blood pressure check or depression medication check) provided in an integrated
sitesetting is considered an integrated service because it is provided in the context of that integrated sitersquos whole person care
Conversely multiple services provided in a single visit are not by definition integrated care these services could be and all too
often are provided by separate professionals without meaningful collaboration or integration By defining the level of integration
in terms of setting the authors of this framework define the context of interventions and the values (eg care team whole health
patient-centered) that form the basis of an integrated site and integrated services The key performance indicators in an integrated
care setting are population-based health status outcomes not encounter-based processservice data Individual staff productivity
must accompany and then be replaced by population-based outcomes by site
Funding structures and accountability must also change Integrated care is not supported by fee-for-service funding structures
that stumble over same day billing restrictions and do not reimburse for consultations between providers when the patient is not
physically present or electronic contacts or a large volume of care management mdash all of which are essential for improved health
outcomes in an integrated healthcare system Fee-for-service funding can emphasize the measurement of volume rather than
quality Global or blended funding structures do support integrated healthcare and will be fiscally justified by improved patient
outcomes that reduce overall healthcare cost
conclUsIon The proposed level of integration framework is a manageable practical and conceptually sound six level framework for integrated
healthcare that begins with collaboration (how resources are brought together) and moves through colocation and increasing levels
of integration (how services are framed and delivered) This standard framework is needed for clarity and precision of communicashy
tion as well as to contribute to research and practice redesign By implication the numbering of levels suggests that the higher
the level of collaborationintegration the more potential for positive impact on health outcomes and patient experience This belief
remains a hypothesis and has not been empirically tested With further research these benefits of collaborationintegration can
be more firmly stated and can identify which aspects of the collaboration integration or combination of the two contribute most
directly to health outcomes
Even if health outcomes improve as levels of integration increase it is not practical to believe that every healthcare setting will be
able at least in the near term to implement increasing levels of integration Many integrated implementations will be constrained
by community politics trust between organizational systems financing andor differing service values
Lastly this issue brief does not presume to establish a fuller lexicon for integration and healthcare as much needed as it is The
authors leave that to others better suited to the task and hope that this paper will contribute to such a lexicon The purpose is
to help those delivering services today by presenting a conceptual framework to better understand and differentiate integrated
healthcare implementations The authors believe that this framework will inform discussions about integrated healthcare and that
its use will provide opportunity for service redesign that will lead to better conceptual and practical models of care
9 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
ReFeRences
Berwick DM Nolan TW amp Whittington J (2008) The triple aim Care health and cost Health Affairs 27(3) 759-769
Blount A (2003) Integrated primary care Organizing the evidence Families Systems amp Health 21 (2) 121-33 doi 1010371091shy75272121121
Blount A (Ed) (1998) Integrated primary care The future of medical and mental health collaboration New York Norton
Butler M Kane RL McAlpine D et al Integration of Mental HealthSubstance Abuse and Primary Care No 173 (Prepared by the Minnesota Evidence-based Practice Center under Contract No 290-02-0009) AHRQ Publication No 09-E003 Rockville MD Agency for Healthcare Research and Quality October 2008
Collins C Hewson DL Munger R amp Wade T (2010) Evolving models of behavioral health Integration in primary care Report commissioned by the Milbank Memorial Fund
Doherty W (1995) The whyrsquos and levels of collaborative family health care Family Systems Medicine 13(3-4) 275-81 doi101037h0089174
Doherty WJ McDaniel SH amp Baird MA (1996) Five levels of primary carebehavioral healthcare collaboration Behavioral Healthcare Tomorrow 25-28
Funk M and G Ivbijaro eds (2008) Integrating mental health into primary care ndash A global perspective Geneva Switzerland World Health Organization and London UK World Organization of Family Doctors Available at wwwwhointmental_healthpolicyMental20health20+20primary20care-20final20low-res20140908pdf
Kodner Dennis (2009) All together now A conceptual exploration of integrated care Healthcare Quarterly 13 (Sp) 6-15
Lopez M B Coleman-Beattie L Jahnke and K Sanchez (2008) Connecting body and mind A resource guide to integrated health care in Texas and the United States Austin TX Hogg Foundation for Mental Health
Mauer B (2006) Behavioral healthprimary care integration The four quadrant model and evidence-based practices Rockville MD National Council for Community Behavioral Healthcare
Mauer B (2009) Behavioral healthprimary care integration and the person-centered healthcare home Washington DC National Council for Community Behavioral Healthcare
Mauer B (2010) Substance use disorders and the person-centered healthcare home Rockville MD National Council for Community Behavioral Healthcare
Mauer B amp Jarvis D (2010) The business case for bidirectional integrated care Mental health and substance use services in primary care settings and primary care services in specialty mental health and substance use settings Integration Policy Initiative
Maine Health Access Foundation (2009) Site Self-Assessment
Miller BF Kessler R Peek CJ (2011) A national agenda for research in collaborative care Papers from the Collaborative Care Research Network Research Development Conference AHRQ Publication No 11-0067 Rockville MD Agency for Healthcare Research and Quality
Peek CJ (2007) Integrated Care Aids to Navigation Study packet for the Pennsylvania Eastern Ohio amp West Virginia Summit Integrating Mental Health and Primary Care Pittsburgh PA
Reynolds K (2006) Mental Health Primary Care Integration Options (Unpublished document)
Robinson PJ amp Reiter JT (2007) Behavioral consultation and primary care A guide to integrating services New York Springer
Russell L (2010) Mental health care services in primary care Tackling the issues in the context of health care reform Center for American Progress Washington DC
Seaburn Lorenz Gunn Gawinksi amp Mauksch (1996) Models of collaboration A guide for mental health professionals working with health care practitioners Basic Books
Strosahl K (1998) Integrating behavioral health and primary care services The primary mental health care model In Integrated primary care The future of medical and mental health collaboration edited by A Blount pp 139-66 New York WW Norton
Strosahl K amp Robinson P (2008) The primary care behavioral health model Applications to prevention acute care and chronic condition management In R Kessler amp D Strafford (Eds) Collaborative medicine case studies Evidence in practice New York Springer
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 1
Six
Lev
els
of C
olla
bo
ratio
nIn
tegr
atio
n (C
ore
Des
crip
tions
)
CO
OR
DIN
AT
ED
KE
y E
LEM
EN
T C
OM
MU
NIC
AT
ION
CO
LO
CA
TE
D
KE
y E
LEM
EN
T P
Hy
SIC
AL
PR
Ox
IMIT
y
INT
EG
RA
TE
D
KE
y E
LEM
EN
T P
RA
CT
ICE
CH
AN
GE
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
beh
avio
ral h
ealt
h p
rim
ary
care
an
d o
ther
hea
lth
care
pro
vid
ers
wo
rk
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
Com
mun
icat
e ab
out c
ases
on
ly ra
rely
and
und
erco
mpe
lling
circ
umst
ance
s
8 8 C
omm
unic
ate
driv
en b
y pr
ovid
er n
eed
8 M
ay n
ever
mee
t in
pers
on
8 H
ave
limite
d un
ders
tand
shyin
g of
eac
h ot
herrsquos
role
s
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
8Co
mm
unic
ate
perio
dica
llyab
out s
hare
d pa
tient
s
8 C
omm
unic
ate
driv
en b
y sp
ecifi
c pa
tient
issu
es
8 M
ay m
eet a
s pa
rt of
larg
er
com
mun
ity
8Ap
prec
iate
eac
h ot
herrsquos
ro
les
as re
sour
ces
secfi t f
o oy
n eti amli s c ya il ey
e f ar h
m ss e t
a e r
n s ece hI n w 8
Hav
e se
para
te s
yste
ms
8 C
omm
unic
ate
regu
larly
ab
out s
hare
d pa
tient
s b
y ph
one
or e
-mai
l
8 C
olla
bora
te d
riven
by
need
for e
ach
othe
rrsquos
serv
ices
and
mor
e re
liabl
e re
ferra
l
8M
eet o
ccas
iona
lly to
disc
uss
case
s du
e to
clo
sepr
oxim
ity
8 F
eel p
art o
f a la
rger
yet
no
n-fo
rmal
team
e h ey
n t h
ih e t
rti ee
w hc wya tp il
e s ica
ma e f
n s maI s 8
Sha
re s
ome
syst
ems
like
sc
hedu
ling
or m
edic
alre
cord
s
8Co
mm
unic
ate
in p
erso
nas
nee
ded
8 C
olla
bora
te d
riven
by
need
for c
onsu
ltatio
n an
dco
ordi
nate
d pl
ans
for
diffi
cult
patie
nts
8 H
ave
regu
lar f
ace-
to-fa
ce
inte
ract
ions
abo
ut s
ome
patie
nts
8 H
ave
a ba
sic
unde
rsta
ndin
g of
role
san
d cu
lture
e h all
n t erih in
gt hei ar
e w h w
s ec ya t acp ili p
e s c sa e
m f icea t
am acn s eyr hI s p t
e n m e i o rh est
y ( hi
e w ti wl )c i eca cap
e f a
e s p
mm a d s
e ae
sn
s reyh ha hI t s t 8Ac
tivel
y se
ek s
yste
m
solu
tions
toge
ther
or
deve
lop
work
-a-ro
unds
8Co
mm
unic
ate
frequ
ently
in p
erso
n
8 C
olla
bora
te d
riven
by
desi
re to
be
a m
embe
r of
the
care
team
8 H
ave
regu
lar t
eam
m
eetin
gs to
dis
cuss
ove
rall
patie
nt c
are
and
spec
ific
patie
nt is
sues
8 H
ave
an in
-dep
th u
nshyde
rsta
ndin
g of
role
s an
dcu
lture
8 H
ave
reso
lved
mos
t or a
ll sy
stem
issu
es f
unct
ioni
ng
as o
ne in
tegr
ated
sys
tem
8Co
mm
unic
ate
cons
iste
ntly
at th
e sy
stem
tea
m a
nd
indi
vidu
al le
vels
8 C
olla
bora
te d
riven
by
shar
ed c
once
pt o
f tea
mca
re
8 H
ave
form
al a
nd in
form
al
mee
tings
to s
uppo
rt in
tegr
ated
mod
el o
f car
e
8 H
ave
role
s an
d cu
lture
s th
at b
lur o
r ble
nd
10
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 2
A S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Clin
ical
Del
iver
y
Scr
eeni
ng a
nd a
sses
sshym
ent d
one
acco
rdin
g to
se
para
te p
ract
ice
mod
els
Sepa
rate
trea
tmen
t pla
ns
Ev
iden
ced-
base
d pr
actic
es (E
BP)
impl
emen
ted
sepa
rate
ly
8 8 8
Scre
enin
g ba
sed
on
sepa
rate
pra
ctic
es m
al
y be
mat
ion
ma
info
rsh
ared
thro
ugh
for
requ
ests
or H
ealth
m
atio
n Ex
chan
ges
Info
r
Sepa
rate
trea
tmen
t pl
ans
shar
ed b
ased
on
esta
blis
hed
rela
tion-
een
spec
ific
ship
s be
twvi
ders
pr
o
Sepa
rate
resp
onsi
bilit
y fo
r car
eEB
Ps
8 8 8
ree
on a
spe
cific
y
ag M
a
crite
ria fo
r mor
e ef
fect
ive
sc
reen
ing
or o
ther
ral
vice
pla
ns
ms e
in-h
ouse
refe
r
Sep
arat
e se
rwi
th s
ome
shar
ed
mat
ion
that
info
r
wled
g
info
rth
em
8
Som
e sh
ared
kno
s EB
Ps
of e
ach
othe
rrsquoes
peci
ally
for h
igh
utili
zers
88
A
gree
on
spec
ific
bas
ed o
n sc
reen
ing
abili
ty to
resp
ond
to
e tre
atm
ent
resu
lts
8
Col
labo
rativ
plan
ning
for s
peci
fic
patie
nts
Som
e EB
Ps a
nd s
ome
focu
sed
train
ing
shar
ed
on in
tere
st o
r spe
cific
po
pula
tion
need
s
8 8
Con
sist
ent s
et o
f agr
eed
upon
scr
eeni
ngs
acro
ss
disc
iplin
es w
hich
gui
de
vent
ions
e tre
atm
ent
treat
men
t int
er
8
Col
labo
rativ
plan
ning
for a
ll sh
ared
patie
nts
8
EBP
s sh
ared
acr
oss
sys-
tem
with
som
e jo
int m
onishy
torin
g of
hea
lth c
ondi
tions
fo
r som
e pa
tient
s
8
8 P
opul
atio
n-ba
sed
m
edic
al a
nd b
ehav
iora
l he
alth
scr
eeni
ng is
stan
dard
pra
ctic
e wi
thre
sults
ava
ilabl
e to
all
and
resp
onse
pro
toco
lsin
pla
ce
8On
e tre
atm
ent p
lan
for a
llpa
tient
s
8EB
Ps a
re te
am s
elec
ted
train
ed a
nd im
plem
ente
dac
ross
dis
cipl
ines
as
stan
dard
pra
ctic
e
Key
Dif
fere
ntia
tor
Pat
ien
t Exp
erie
nce
ysic
al a
nd b
eshy P
atie
nt p
hha
vior
al h
ealth
nee
ds a
re
treat
ed a
s se
para
te is
sues
otia
te
Pat
ient
mus
t neg
sepa
rate
pra
ctic
es a
nd
wn w
ith
rees
of s
ucce
ss
site
s on
thei
r oyi
ng d
egarv
8 8vi
der
P
atie
nt h
ealth
nee
ds
are
treat
ed s
epar
atel
ybu
t rec
ords
are
sha
red re
d
prom
otin
g be
tter p
ro riers
y
be re
fer
y pa
tient
s
e
arie
ty o
f bar
wled
gkn
o
Pat
ient
s m
abu
t a v
vent
man
pre
from
acc
essi
ng c
are
8 8
atie
nt h
ealth
nee
ds a
re y
y b
ws
P treat
ed s
epar
atel
y at
the
sam
e lo
catio
n
8
Clo
se p
roxim
ity a
llora
ls to
be
mor
e re
fer
succ
essf
ul a
nd e
asie
r for
ho
a
lthou
gh w ar
y v
red
ma
patie
nts
gets
refe
rvi
der
pro
8
col
labo
ratio
n m
ight
Pat
ient
nee
ds a
re tr
eate
d se
para
tely
at t
he s
ame
m h
and-
offs
to
vide
rs
site
in
clud
e wa
rot
her t
reat
men
t pro na
lly
Pat
ient
s ar
e in
ter
red
with
bet
ter f
ollo
wshyre
fer
up b
ut c
olla
bora
tion
may
st
ill b
e ex
perie
nced
as
vice
s se
para
te s
er
8 8
y
e on
Pat
ient
nee
ds a
re tr
eate
d as
a te
am fo
r sha
red
patie
nts
(for t
hose
wh
o sc
reen
pos
itiv
scre
enin
g m
easu
res)
and
sepa
rate
ly fo
r oth
ers
e to
8
Car
e is
resp
onsi
vid
entifi
ed p
atie
nt n
eeds
bvi
ders
as e a
of a
team
of p
ro w
hich
feel
s lik
need
ed
one-
stop
sho
p
8
All p
atie
nt h
ealth
nee
ds ar
e tre
ated
for a
ll pa
tient
sby
a te
am w
ho fu
nctio
n et
her
ely
tog
effe
ctiv
Pat
ient
s ex
perie
nce
a se
amle
ss re
spon
se to
all h
ealth
care
nee
ds a
s in
a u
nifie
d y
pres
ent
the
prac
tice
8 8
11
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
No
coo
rdin
atio
n or
ts
em
ent o
f e
effo
r
vide
r buy
-in
en
ratio
n or
ev
up
to
vide
rs to
man
agco
llabo
rativ
Litt
le p
roto
inte
gco
llabo
ratio
nin
divi
dual
pro
initi
ate
as ti
me
and
prac
tice
limits
allo
w
8 8
Som
e pr
actic
e le
ader
shysh
ip in
mor
e sy
stem
atic
vide
r buy
-into
al
ue
ving
nee
ded
mat
ion
shar
ing
info
r
Som
e pr
oco
llabo
ratio
n an
d v
plac
ed o
n ha
mat
ion
info
r
8 8
Org
aniza
tion
lead
ers
tive
but o
ften
colo
shysu
ppor
catio
n is
vie
wed
as
a pr
ojec
t or p
rogr
am ork
and
vide
r buy
-in to
ra
ls w
Pro mak
ing
refe
rap
prec
iatio
n of
ons
ite
vaila
bilit
y a
8 8
thro
ugh
mut
ual p
robl
em-
Org
aniza
tion
lead
ers
ratio
n t i
nteg
supp
or
solv
ing
of s
ome
syst
em
riers
ba
r
Mor
e bu
y-in
to c
once
pt
vide
rs
ratio
n bu
t not
of
inte
gco
nsis
tent
acr
oss
not
all
pro
tuni
ties
for
vide
rs
pro
usin
g op
por
inte
grat
ion
or c
ompo
nent
s
8 8
ts
w
Org
aniza
tion
lead
ers if
ra
tion
ws a
nd e
ffor
t int
egsu
ppor
fund
ing
allo
plac
ed in
sol
ving
as
man
y sy
stem
issu
es a
s w
ithou
t cha
ngshy
poss
ible
in
g fu
ndam
enta
lly h
odi
scip
lines
are
pra
ctic
ed
rate
d y
not
vide
rs
e in
pra
ctic
e
ly a
ll pr
o N
ear ag
ed in
inte
g B
uy-in
ma
y fo
r ind
ivid
ual
eng
mod
el
incl
ude
chan
g
vide
rs
stra
teg
pro
8 8
y e
ervi
ded
aniza
tion
lead
ers
t ra
tion
as p
ract
ice
Org
stro
ngly
sup
por
inte
gm
odel
with
exp
ecte
dvi
ce d
eliv
e in
ser
chan
g
for d
evel
opm
ent
rate
d ca
re a
nd a
ll In
teg
com
pone
nts
embr
aced
vide
rs a
nd a
ctiv
and
reso
urce
s pr
o
by a
ll pr
ool
vem
ent i
n pr
actic
e e
vin ch
ang
8 8
Tab
le 2
b S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs c
ont
inue
d)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Pra
ctic
eO
rgan
izat
ion
Key
Dif
fere
ntia
tor
bu
sin
ess
Mo
del
Se
para
te fu
ndin
g
No s
harin
g of
reso
urce
s
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re re
sour
ces
for
sing
le p
roje
cts
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re fa
cilit
y ex
pens
es
Sepa
rate
bill
ing
prac
tices
8 8 8
but
may
S
epar
ate
fund
ing
rant
s sta
ffing
cos
ts
shar
e g
y sh
are
offic
e
uctu
re
Ma
expe
nses
or
infra
str
Sepa
rate
bill
ing
due
to
riers
sy
stem
bar
8 8 8
Bl
ende
d fu
ndin
g ba
sed
uctu
re
on c
ontra
cts
gra
nts
or
ys to
str
agre
emen
ts
Varie
ty o
f wa
8
the
shar
ing
of a
ll ex
pens
es
Billi
ng fu
nctio
n co
mbi
ned
reed
upo
n pr
oces
s or
ag
8 8
8 8Re
sour
ces
shar
ed a
nd
hole
rate
d fu
ndin
g In
teg
base
d on
mul
tiple
sour
ces
of re
venu
e
allo
cate
d ac
ross
wpr
actic
e
Billi
ng m
axim
ized
for
rate
d m
odel
and
uc
ture
in
teg
sing
le b
illin
g st
r
8
12
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 3
Ad
vant
ages
and
Wea
knes
ses
at E
ach
Leve
l of C
olla
bo
ratio
nIn
tegr
atio
n
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Ad
van
tag
es
8 E
ach
prac
tice
can
mak
e tim
ely
and
auto
nom
ous
deci
sion
s ab
out c
are
8Re
adily
und
erst
ood
asa
prac
tice
mod
el b
y pa
tient
s an
d pr
ovid
ers
8 M
aint
ains
eac
h pr
actic
ersquos
basi
c op
erat
ing
stru
ctur
eso
cha
nge
is n
ot a
di
srup
tive
fact
or
8 P
rovi
des
som
e co
ordi
natio
n an
din
form
atio
n-sh
arin
g th
at
is h
elpf
ul to
bot
h pa
tient
san
d pr
ovid
ers
8 C
oloc
atio
n al
lows
for
mor
e di
rect
inte
ract
ion
and
com
mun
icat
ion
amon
g pr
ofes
sion
als
toim
pact
pat
ient
car
e
8 R
efer
rals
mor
e su
cces
sful
du
e to
pro
ximity
8 O
ppor
tuni
ty to
dev
elop
cl
oser
pro
fess
iona
l rel
ashytio
nshi
ps
8 R
emov
al o
f som
e sy
stem
ba
rrier
s li
ke s
epar
ate
reco
rds
allo
ws c
lose
r co
llabo
ratio
n to
occ
ur
8 B
oth
beha
vior
al h
ealth
an
d m
edic
al p
rovi
ders
ca
n be
com
e m
ore
well-
info
rmed
abo
ut w
hat e
ach
can
prov
ide
8 P
atie
nts
are
view
ed a
s sh
ared
whi
ch fa
cilit
ates
m
ore
com
plet
e tre
atm
ent
plan
s
8 H
igh
leve
l of c
olla
bora
tion
lead
s to
mor
e re
spon
sive
pa
tient
car
e in
crea
sing
en
gage
men
t and
ad
here
nce
to tr
eatm
ent
plan
s
8 P
rovi
der fl
exib
ility
in
crea
ses
as s
yste
mis
sues
and
bar
riers
are
re
solve
d
8 B
oth
prov
ider
and
pat
ient
sa
tisfa
ctio
n m
ay in
crea
se
8 O
ppor
tuni
ty to
trul
y tre
at
whol
e pe
rson
8Al
l or a
lmos
t all
syst
emba
rrier
s re
solve
d a
llowi
ng
prov
ider
s to
pra
ctic
e as
hi
gh fu
nctio
ning
team
8Al
l pat
ient
nee
dsad
dres
sed
as th
ey o
ccur
8 S
hare
d kn
owle
dge
base
of
pro
vide
rs in
crea
ses
and
allo
ws e
ach
prof
essi
onal
to
resp
ond
mor
e br
oadl
yan
d ad
equa
tely
to a
ny
issu
e
Wea
knes
ses
8 S
ervi
ces
may
ove
rlap
be
dupl
icat
ed o
r eve
n wo
rk
agai
nst e
ach
othe
r
8 Im
porta
nt a
spec
ts o
f car
e m
ay n
ot b
e ad
dres
sed
or ta
ke a
long
tim
e to
be
diag
nose
d
8 S
harin
g of
info
rmat
ion
may
not
be
syst
emat
ic
enou
gh to
effe
ct o
vera
ll pa
tient
car
e
8 N
o gu
aran
tee
that
info
rshym
atio
n wi
ll ch
ange
pla
n or
st
rate
gy o
f eac
h pr
ovid
er
8 R
efer
rals
may
fail
due
to
barri
ers
lead
ing
to p
atie
nt
and
prov
ider
frus
tratio
n
8 P
roxim
ity m
ay n
ot le
ad to
gr
eate
r col
labo
ratio
nlim
iting
val
ue
8 E
ffort
is re
quire
d to
de
velo
p re
latio
nshi
ps
8 L
imite
d fle
xibili
ty if
tra
ditio
nal r
oles
are
mai
ntai
ned
8 S
yste
m is
sues
may
lim
it co
llabo
ratio
n
8 P
oten
tial f
or te
nsio
n an
d co
nflic
ting
agen
das
amon
g pr
ovid
ers
as p
ract
ice
boun
darie
s lo
osen
8 P
ract
ice
chan
ges
may
cr
eate
lack
of fi
t for
som
ees
tabl
ishe
d pr
ovid
ers
8Ti
me
is n
eede
d to
co
llabo
rate
at t
his
high
leve
l and
may
affe
ct
prac
tice
prod
uctiv
ity o
rca
denc
e of
car
e
8 S
usta
inab
ility
issu
es m
ay
stre
ss th
e pr
actic
e
8 F
ew m
odel
s at
this
leve
l wi
th e
noug
h ex
perie
nce
tosu
ppor
t val
ue
8Ou
tcom
e ex
pect
atio
ns n
otye
t est
ablis
hed
13

8 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
From a data standpoint this framework also posits that integrated services should be defined by location not by an algorithm of
service code combinations A single service (eg blood pressure check or depression medication check) provided in an integrated
sitesetting is considered an integrated service because it is provided in the context of that integrated sitersquos whole person care
Conversely multiple services provided in a single visit are not by definition integrated care these services could be and all too
often are provided by separate professionals without meaningful collaboration or integration By defining the level of integration
in terms of setting the authors of this framework define the context of interventions and the values (eg care team whole health
patient-centered) that form the basis of an integrated site and integrated services The key performance indicators in an integrated
care setting are population-based health status outcomes not encounter-based processservice data Individual staff productivity
must accompany and then be replaced by population-based outcomes by site
Funding structures and accountability must also change Integrated care is not supported by fee-for-service funding structures
that stumble over same day billing restrictions and do not reimburse for consultations between providers when the patient is not
physically present or electronic contacts or a large volume of care management mdash all of which are essential for improved health
outcomes in an integrated healthcare system Fee-for-service funding can emphasize the measurement of volume rather than
quality Global or blended funding structures do support integrated healthcare and will be fiscally justified by improved patient
outcomes that reduce overall healthcare cost
conclUsIon The proposed level of integration framework is a manageable practical and conceptually sound six level framework for integrated
healthcare that begins with collaboration (how resources are brought together) and moves through colocation and increasing levels
of integration (how services are framed and delivered) This standard framework is needed for clarity and precision of communicashy
tion as well as to contribute to research and practice redesign By implication the numbering of levels suggests that the higher
the level of collaborationintegration the more potential for positive impact on health outcomes and patient experience This belief
remains a hypothesis and has not been empirically tested With further research these benefits of collaborationintegration can
be more firmly stated and can identify which aspects of the collaboration integration or combination of the two contribute most
directly to health outcomes
Even if health outcomes improve as levels of integration increase it is not practical to believe that every healthcare setting will be
able at least in the near term to implement increasing levels of integration Many integrated implementations will be constrained
by community politics trust between organizational systems financing andor differing service values
Lastly this issue brief does not presume to establish a fuller lexicon for integration and healthcare as much needed as it is The
authors leave that to others better suited to the task and hope that this paper will contribute to such a lexicon The purpose is
to help those delivering services today by presenting a conceptual framework to better understand and differentiate integrated
healthcare implementations The authors believe that this framework will inform discussions about integrated healthcare and that
its use will provide opportunity for service redesign that will lead to better conceptual and practical models of care
9 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
ReFeRences
Berwick DM Nolan TW amp Whittington J (2008) The triple aim Care health and cost Health Affairs 27(3) 759-769
Blount A (2003) Integrated primary care Organizing the evidence Families Systems amp Health 21 (2) 121-33 doi 1010371091shy75272121121
Blount A (Ed) (1998) Integrated primary care The future of medical and mental health collaboration New York Norton
Butler M Kane RL McAlpine D et al Integration of Mental HealthSubstance Abuse and Primary Care No 173 (Prepared by the Minnesota Evidence-based Practice Center under Contract No 290-02-0009) AHRQ Publication No 09-E003 Rockville MD Agency for Healthcare Research and Quality October 2008
Collins C Hewson DL Munger R amp Wade T (2010) Evolving models of behavioral health Integration in primary care Report commissioned by the Milbank Memorial Fund
Doherty W (1995) The whyrsquos and levels of collaborative family health care Family Systems Medicine 13(3-4) 275-81 doi101037h0089174
Doherty WJ McDaniel SH amp Baird MA (1996) Five levels of primary carebehavioral healthcare collaboration Behavioral Healthcare Tomorrow 25-28
Funk M and G Ivbijaro eds (2008) Integrating mental health into primary care ndash A global perspective Geneva Switzerland World Health Organization and London UK World Organization of Family Doctors Available at wwwwhointmental_healthpolicyMental20health20+20primary20care-20final20low-res20140908pdf
Kodner Dennis (2009) All together now A conceptual exploration of integrated care Healthcare Quarterly 13 (Sp) 6-15
Lopez M B Coleman-Beattie L Jahnke and K Sanchez (2008) Connecting body and mind A resource guide to integrated health care in Texas and the United States Austin TX Hogg Foundation for Mental Health
Mauer B (2006) Behavioral healthprimary care integration The four quadrant model and evidence-based practices Rockville MD National Council for Community Behavioral Healthcare
Mauer B (2009) Behavioral healthprimary care integration and the person-centered healthcare home Washington DC National Council for Community Behavioral Healthcare
Mauer B (2010) Substance use disorders and the person-centered healthcare home Rockville MD National Council for Community Behavioral Healthcare
Mauer B amp Jarvis D (2010) The business case for bidirectional integrated care Mental health and substance use services in primary care settings and primary care services in specialty mental health and substance use settings Integration Policy Initiative
Maine Health Access Foundation (2009) Site Self-Assessment
Miller BF Kessler R Peek CJ (2011) A national agenda for research in collaborative care Papers from the Collaborative Care Research Network Research Development Conference AHRQ Publication No 11-0067 Rockville MD Agency for Healthcare Research and Quality
Peek CJ (2007) Integrated Care Aids to Navigation Study packet for the Pennsylvania Eastern Ohio amp West Virginia Summit Integrating Mental Health and Primary Care Pittsburgh PA
Reynolds K (2006) Mental Health Primary Care Integration Options (Unpublished document)
Robinson PJ amp Reiter JT (2007) Behavioral consultation and primary care A guide to integrating services New York Springer
Russell L (2010) Mental health care services in primary care Tackling the issues in the context of health care reform Center for American Progress Washington DC
Seaburn Lorenz Gunn Gawinksi amp Mauksch (1996) Models of collaboration A guide for mental health professionals working with health care practitioners Basic Books
Strosahl K (1998) Integrating behavioral health and primary care services The primary mental health care model In Integrated primary care The future of medical and mental health collaboration edited by A Blount pp 139-66 New York WW Norton
Strosahl K amp Robinson P (2008) The primary care behavioral health model Applications to prevention acute care and chronic condition management In R Kessler amp D Strafford (Eds) Collaborative medicine case studies Evidence in practice New York Springer
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 1
Six
Lev
els
of C
olla
bo
ratio
nIn
tegr
atio
n (C
ore
Des
crip
tions
)
CO
OR
DIN
AT
ED
KE
y E
LEM
EN
T C
OM
MU
NIC
AT
ION
CO
LO
CA
TE
D
KE
y E
LEM
EN
T P
Hy
SIC
AL
PR
Ox
IMIT
y
INT
EG
RA
TE
D
KE
y E
LEM
EN
T P
RA
CT
ICE
CH
AN
GE
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
beh
avio
ral h
ealt
h p
rim
ary
care
an
d o
ther
hea
lth
care
pro
vid
ers
wo
rk
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
Com
mun
icat
e ab
out c
ases
on
ly ra
rely
and
und
erco
mpe
lling
circ
umst
ance
s
8 8 C
omm
unic
ate
driv
en b
y pr
ovid
er n
eed
8 M
ay n
ever
mee
t in
pers
on
8 H
ave
limite
d un
ders
tand
shyin
g of
eac
h ot
herrsquos
role
s
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
8Co
mm
unic
ate
perio
dica
llyab
out s
hare
d pa
tient
s
8 C
omm
unic
ate
driv
en b
y sp
ecifi
c pa
tient
issu
es
8 M
ay m
eet a
s pa
rt of
larg
er
com
mun
ity
8Ap
prec
iate
eac
h ot
herrsquos
ro
les
as re
sour
ces
secfi t f
o oy
n eti amli s c ya il ey
e f ar h
m ss e t
a e r
n s ece hI n w 8
Hav
e se
para
te s
yste
ms
8 C
omm
unic
ate
regu
larly
ab
out s
hare
d pa
tient
s b
y ph
one
or e
-mai
l
8 C
olla
bora
te d
riven
by
need
for e
ach
othe
rrsquos
serv
ices
and
mor
e re
liabl
e re
ferra
l
8M
eet o
ccas
iona
lly to
disc
uss
case
s du
e to
clo
sepr
oxim
ity
8 F
eel p
art o
f a la
rger
yet
no
n-fo
rmal
team
e h ey
n t h
ih e t
rti ee
w hc wya tp il
e s ica
ma e f
n s maI s 8
Sha
re s
ome
syst
ems
like
sc
hedu
ling
or m
edic
alre
cord
s
8Co
mm
unic
ate
in p
erso
nas
nee
ded
8 C
olla
bora
te d
riven
by
need
for c
onsu
ltatio
n an
dco
ordi
nate
d pl
ans
for
diffi
cult
patie
nts
8 H
ave
regu
lar f
ace-
to-fa
ce
inte
ract
ions
abo
ut s
ome
patie
nts
8 H
ave
a ba
sic
unde
rsta
ndin
g of
role
san
d cu
lture
e h all
n t erih in
gt hei ar
e w h w
s ec ya t acp ili p
e s c sa e
m f icea t
am acn s eyr hI s p t
e n m e i o rh est
y ( hi
e w ti wl )c i eca cap
e f a
e s p
mm a d s
e ae
sn
s reyh ha hI t s t 8Ac
tivel
y se
ek s
yste
m
solu
tions
toge
ther
or
deve
lop
work
-a-ro
unds
8Co
mm
unic
ate
frequ
ently
in p
erso
n
8 C
olla
bora
te d
riven
by
desi
re to
be
a m
embe
r of
the
care
team
8 H
ave
regu
lar t
eam
m
eetin
gs to
dis
cuss
ove
rall
patie
nt c
are
and
spec
ific
patie
nt is
sues
8 H
ave
an in
-dep
th u
nshyde
rsta
ndin
g of
role
s an
dcu
lture
8 H
ave
reso
lved
mos
t or a
ll sy
stem
issu
es f
unct
ioni
ng
as o
ne in
tegr
ated
sys
tem
8Co
mm
unic
ate
cons
iste
ntly
at th
e sy
stem
tea
m a
nd
indi
vidu
al le
vels
8 C
olla
bora
te d
riven
by
shar
ed c
once
pt o
f tea
mca
re
8 H
ave
form
al a
nd in
form
al
mee
tings
to s
uppo
rt in
tegr
ated
mod
el o
f car
e
8 H
ave
role
s an
d cu
lture
s th
at b
lur o
r ble
nd
10
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 2
A S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Clin
ical
Del
iver
y
Scr
eeni
ng a
nd a
sses
sshym
ent d
one
acco
rdin
g to
se
para
te p
ract
ice
mod
els
Sepa
rate
trea
tmen
t pla
ns
Ev
iden
ced-
base
d pr
actic
es (E
BP)
impl
emen
ted
sepa
rate
ly
8 8 8
Scre
enin
g ba
sed
on
sepa
rate
pra
ctic
es m
al
y be
mat
ion
ma
info
rsh
ared
thro
ugh
for
requ
ests
or H
ealth
m
atio
n Ex
chan
ges
Info
r
Sepa
rate
trea
tmen
t pl
ans
shar
ed b
ased
on
esta
blis
hed
rela
tion-
een
spec
ific
ship
s be
twvi
ders
pr
o
Sepa
rate
resp
onsi
bilit
y fo
r car
eEB
Ps
8 8 8
ree
on a
spe
cific
y
ag M
a
crite
ria fo
r mor
e ef
fect
ive
sc
reen
ing
or o
ther
ral
vice
pla
ns
ms e
in-h
ouse
refe
r
Sep
arat
e se
rwi
th s
ome
shar
ed
mat
ion
that
info
r
wled
g
info
rth
em
8
Som
e sh
ared
kno
s EB
Ps
of e
ach
othe
rrsquoes
peci
ally
for h
igh
utili
zers
88
A
gree
on
spec
ific
bas
ed o
n sc
reen
ing
abili
ty to
resp
ond
to
e tre
atm
ent
resu
lts
8
Col
labo
rativ
plan
ning
for s
peci
fic
patie
nts
Som
e EB
Ps a
nd s
ome
focu
sed
train
ing
shar
ed
on in
tere
st o
r spe
cific
po
pula
tion
need
s
8 8
Con
sist
ent s
et o
f agr
eed
upon
scr
eeni
ngs
acro
ss
disc
iplin
es w
hich
gui
de
vent
ions
e tre
atm
ent
treat
men
t int
er
8
Col
labo
rativ
plan
ning
for a
ll sh
ared
patie
nts
8
EBP
s sh
ared
acr
oss
sys-
tem
with
som
e jo
int m
onishy
torin
g of
hea
lth c
ondi
tions
fo
r som
e pa
tient
s
8
8 P
opul
atio
n-ba
sed
m
edic
al a
nd b
ehav
iora
l he
alth
scr
eeni
ng is
stan
dard
pra
ctic
e wi
thre
sults
ava
ilabl
e to
all
and
resp
onse
pro
toco
lsin
pla
ce
8On
e tre
atm
ent p
lan
for a
llpa
tient
s
8EB
Ps a
re te
am s
elec
ted
train
ed a
nd im
plem
ente
dac
ross
dis
cipl
ines
as
stan
dard
pra
ctic
e
Key
Dif
fere
ntia
tor
Pat
ien
t Exp
erie
nce
ysic
al a
nd b
eshy P
atie
nt p
hha
vior
al h
ealth
nee
ds a
re
treat
ed a
s se
para
te is
sues
otia
te
Pat
ient
mus
t neg
sepa
rate
pra
ctic
es a
nd
wn w
ith
rees
of s
ucce
ss
site
s on
thei
r oyi
ng d
egarv
8 8vi
der
P
atie
nt h
ealth
nee
ds
are
treat
ed s
epar
atel
ybu
t rec
ords
are
sha
red re
d
prom
otin
g be
tter p
ro riers
y
be re
fer
y pa
tient
s
e
arie
ty o
f bar
wled
gkn
o
Pat
ient
s m
abu
t a v
vent
man
pre
from
acc
essi
ng c
are
8 8
atie
nt h
ealth
nee
ds a
re y
y b
ws
P treat
ed s
epar
atel
y at
the
sam
e lo
catio
n
8
Clo
se p
roxim
ity a
llora
ls to
be
mor
e re
fer
succ
essf
ul a
nd e
asie
r for
ho
a
lthou
gh w ar
y v
red
ma
patie
nts
gets
refe
rvi
der
pro
8
col
labo
ratio
n m
ight
Pat
ient
nee
ds a
re tr
eate
d se
para
tely
at t
he s
ame
m h
and-
offs
to
vide
rs
site
in
clud
e wa
rot
her t
reat
men
t pro na
lly
Pat
ient
s ar
e in
ter
red
with
bet
ter f
ollo
wshyre
fer
up b
ut c
olla
bora
tion
may
st
ill b
e ex
perie
nced
as
vice
s se
para
te s
er
8 8
y
e on
Pat
ient
nee
ds a
re tr
eate
d as
a te
am fo
r sha
red
patie
nts
(for t
hose
wh
o sc
reen
pos
itiv
scre
enin
g m
easu
res)
and
sepa
rate
ly fo
r oth
ers
e to
8
Car
e is
resp
onsi
vid
entifi
ed p
atie
nt n
eeds
bvi
ders
as e a
of a
team
of p
ro w
hich
feel
s lik
need
ed
one-
stop
sho
p
8
All p
atie
nt h
ealth
nee
ds ar
e tre
ated
for a
ll pa
tient
sby
a te
am w
ho fu
nctio
n et
her
ely
tog
effe
ctiv
Pat
ient
s ex
perie
nce
a se
amle
ss re
spon
se to
all h
ealth
care
nee
ds a
s in
a u
nifie
d y
pres
ent
the
prac
tice
8 8
11
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
No
coo
rdin
atio
n or
ts
em
ent o
f e
effo
r
vide
r buy
-in
en
ratio
n or
ev
up
to
vide
rs to
man
agco
llabo
rativ
Litt
le p
roto
inte
gco
llabo
ratio
nin
divi
dual
pro
initi
ate
as ti
me
and
prac
tice
limits
allo
w
8 8
Som
e pr
actic
e le
ader
shysh
ip in
mor
e sy
stem
atic
vide
r buy
-into
al
ue
ving
nee
ded
mat
ion
shar
ing
info
r
Som
e pr
oco
llabo
ratio
n an
d v
plac
ed o
n ha
mat
ion
info
r
8 8
Org
aniza
tion
lead
ers
tive
but o
ften
colo
shysu
ppor
catio
n is
vie
wed
as
a pr
ojec
t or p
rogr
am ork
and
vide
r buy
-in to
ra
ls w
Pro mak
ing
refe
rap
prec
iatio
n of
ons
ite
vaila
bilit
y a
8 8
thro
ugh
mut
ual p
robl
em-
Org
aniza
tion
lead
ers
ratio
n t i
nteg
supp
or
solv
ing
of s
ome
syst
em
riers
ba
r
Mor
e bu
y-in
to c
once
pt
vide
rs
ratio
n bu
t not
of
inte
gco
nsis
tent
acr
oss
not
all
pro
tuni
ties
for
vide
rs
pro
usin
g op
por
inte
grat
ion
or c
ompo
nent
s
8 8
ts
w
Org
aniza
tion
lead
ers if
ra
tion
ws a
nd e
ffor
t int
egsu
ppor
fund
ing
allo
plac
ed in
sol
ving
as
man
y sy
stem
issu
es a
s w
ithou
t cha
ngshy
poss
ible
in
g fu
ndam
enta
lly h
odi
scip
lines
are
pra
ctic
ed
rate
d y
not
vide
rs
e in
pra
ctic
e
ly a
ll pr
o N
ear ag
ed in
inte
g B
uy-in
ma
y fo
r ind
ivid
ual
eng
mod
el
incl
ude
chan
g
vide
rs
stra
teg
pro
8 8
y e
ervi
ded
aniza
tion
lead
ers
t ra
tion
as p
ract
ice
Org
stro
ngly
sup
por
inte
gm
odel
with
exp
ecte
dvi
ce d
eliv
e in
ser
chan
g
for d
evel
opm
ent
rate
d ca
re a
nd a
ll In
teg
com
pone
nts
embr
aced
vide
rs a
nd a
ctiv
and
reso
urce
s pr
o
by a
ll pr
ool
vem
ent i
n pr
actic
e e
vin ch
ang
8 8
Tab
le 2
b S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs c
ont
inue
d)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Pra
ctic
eO
rgan
izat
ion
Key
Dif
fere
ntia
tor
bu
sin
ess
Mo
del
Se
para
te fu
ndin
g
No s
harin
g of
reso
urce
s
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re re
sour
ces
for
sing
le p
roje
cts
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re fa
cilit
y ex
pens
es
Sepa
rate
bill
ing
prac
tices
8 8 8
but
may
S
epar
ate
fund
ing
rant
s sta
ffing
cos
ts
shar
e g
y sh
are
offic
e
uctu
re
Ma
expe
nses
or
infra
str
Sepa
rate
bill
ing
due
to
riers
sy
stem
bar
8 8 8
Bl
ende
d fu
ndin
g ba
sed
uctu
re
on c
ontra
cts
gra
nts
or
ys to
str
agre
emen
ts
Varie
ty o
f wa
8
the
shar
ing
of a
ll ex
pens
es
Billi
ng fu
nctio
n co
mbi
ned
reed
upo
n pr
oces
s or
ag
8 8
8 8Re
sour
ces
shar
ed a
nd
hole
rate
d fu
ndin
g In
teg
base
d on
mul
tiple
sour
ces
of re
venu
e
allo
cate
d ac
ross
wpr
actic
e
Billi
ng m
axim
ized
for
rate
d m
odel
and
uc
ture
in
teg
sing
le b
illin
g st
r
8
12
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 3
Ad
vant
ages
and
Wea
knes
ses
at E
ach
Leve
l of C
olla
bo
ratio
nIn
tegr
atio
n
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Ad
van
tag
es
8 E
ach
prac
tice
can
mak
e tim
ely
and
auto
nom
ous
deci
sion
s ab
out c
are
8Re
adily
und
erst
ood
asa
prac
tice
mod
el b
y pa
tient
s an
d pr
ovid
ers
8 M
aint
ains
eac
h pr
actic
ersquos
basi
c op
erat
ing
stru
ctur
eso
cha
nge
is n
ot a
di
srup
tive
fact
or
8 P
rovi
des
som
e co
ordi
natio
n an
din
form
atio
n-sh
arin
g th
at
is h
elpf
ul to
bot
h pa
tient
san
d pr
ovid
ers
8 C
oloc
atio
n al
lows
for
mor
e di
rect
inte
ract
ion
and
com
mun
icat
ion
amon
g pr
ofes
sion
als
toim
pact
pat
ient
car
e
8 R
efer
rals
mor
e su
cces
sful
du
e to
pro
ximity
8 O
ppor
tuni
ty to
dev
elop
cl
oser
pro
fess
iona
l rel
ashytio
nshi
ps
8 R
emov
al o
f som
e sy
stem
ba
rrier
s li
ke s
epar
ate
reco
rds
allo
ws c
lose
r co
llabo
ratio
n to
occ
ur
8 B
oth
beha
vior
al h
ealth
an
d m
edic
al p
rovi
ders
ca
n be
com
e m
ore
well-
info
rmed
abo
ut w
hat e
ach
can
prov
ide
8 P
atie
nts
are
view
ed a
s sh
ared
whi
ch fa
cilit
ates
m
ore
com
plet
e tre
atm
ent
plan
s
8 H
igh
leve
l of c
olla
bora
tion
lead
s to
mor
e re
spon
sive
pa
tient
car
e in
crea
sing
en
gage
men
t and
ad
here
nce
to tr
eatm
ent
plan
s
8 P
rovi
der fl
exib
ility
in
crea
ses
as s
yste
mis
sues
and
bar
riers
are
re
solve
d
8 B
oth
prov
ider
and
pat
ient
sa
tisfa
ctio
n m
ay in
crea
se
8 O
ppor
tuni
ty to
trul
y tre
at
whol
e pe
rson
8Al
l or a
lmos
t all
syst
emba
rrier
s re
solve
d a
llowi
ng
prov
ider
s to
pra
ctic
e as
hi
gh fu
nctio
ning
team
8Al
l pat
ient
nee
dsad
dres
sed
as th
ey o
ccur
8 S
hare
d kn
owle
dge
base
of
pro
vide
rs in
crea
ses
and
allo
ws e
ach
prof
essi
onal
to
resp
ond
mor
e br
oadl
yan
d ad
equa
tely
to a
ny
issu
e
Wea
knes
ses
8 S
ervi
ces
may
ove
rlap
be
dupl
icat
ed o
r eve
n wo
rk
agai
nst e
ach
othe
r
8 Im
porta
nt a
spec
ts o
f car
e m
ay n
ot b
e ad
dres
sed
or ta
ke a
long
tim
e to
be
diag
nose
d
8 S
harin
g of
info
rmat
ion
may
not
be
syst
emat
ic
enou
gh to
effe
ct o
vera
ll pa
tient
car
e
8 N
o gu
aran
tee
that
info
rshym
atio
n wi
ll ch
ange
pla
n or
st
rate
gy o
f eac
h pr
ovid
er
8 R
efer
rals
may
fail
due
to
barri
ers
lead
ing
to p
atie
nt
and
prov
ider
frus
tratio
n
8 P
roxim
ity m
ay n
ot le
ad to
gr
eate
r col
labo
ratio
nlim
iting
val
ue
8 E
ffort
is re
quire
d to
de
velo
p re
latio
nshi
ps
8 L
imite
d fle
xibili
ty if
tra
ditio
nal r
oles
are
mai
ntai
ned
8 S
yste
m is
sues
may
lim
it co
llabo
ratio
n
8 P
oten
tial f
or te
nsio
n an
d co
nflic
ting
agen
das
amon
g pr
ovid
ers
as p
ract
ice
boun
darie
s lo
osen
8 P
ract
ice
chan
ges
may
cr
eate
lack
of fi
t for
som
ees
tabl
ishe
d pr
ovid
ers
8Ti
me
is n
eede
d to
co
llabo
rate
at t
his
high
leve
l and
may
affe
ct
prac
tice
prod
uctiv
ity o
rca
denc
e of
car
e
8 S
usta
inab
ility
issu
es m
ay
stre
ss th
e pr
actic
e
8 F
ew m
odel
s at
this
leve
l wi
th e
noug
h ex
perie
nce
tosu
ppor
t val
ue
8Ou
tcom
e ex
pect
atio
ns n
otye
t est
ablis
hed
13

9 SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
ReFeRences
Berwick DM Nolan TW amp Whittington J (2008) The triple aim Care health and cost Health Affairs 27(3) 759-769
Blount A (2003) Integrated primary care Organizing the evidence Families Systems amp Health 21 (2) 121-33 doi 1010371091shy75272121121
Blount A (Ed) (1998) Integrated primary care The future of medical and mental health collaboration New York Norton
Butler M Kane RL McAlpine D et al Integration of Mental HealthSubstance Abuse and Primary Care No 173 (Prepared by the Minnesota Evidence-based Practice Center under Contract No 290-02-0009) AHRQ Publication No 09-E003 Rockville MD Agency for Healthcare Research and Quality October 2008
Collins C Hewson DL Munger R amp Wade T (2010) Evolving models of behavioral health Integration in primary care Report commissioned by the Milbank Memorial Fund
Doherty W (1995) The whyrsquos and levels of collaborative family health care Family Systems Medicine 13(3-4) 275-81 doi101037h0089174
Doherty WJ McDaniel SH amp Baird MA (1996) Five levels of primary carebehavioral healthcare collaboration Behavioral Healthcare Tomorrow 25-28
Funk M and G Ivbijaro eds (2008) Integrating mental health into primary care ndash A global perspective Geneva Switzerland World Health Organization and London UK World Organization of Family Doctors Available at wwwwhointmental_healthpolicyMental20health20+20primary20care-20final20low-res20140908pdf
Kodner Dennis (2009) All together now A conceptual exploration of integrated care Healthcare Quarterly 13 (Sp) 6-15
Lopez M B Coleman-Beattie L Jahnke and K Sanchez (2008) Connecting body and mind A resource guide to integrated health care in Texas and the United States Austin TX Hogg Foundation for Mental Health
Mauer B (2006) Behavioral healthprimary care integration The four quadrant model and evidence-based practices Rockville MD National Council for Community Behavioral Healthcare
Mauer B (2009) Behavioral healthprimary care integration and the person-centered healthcare home Washington DC National Council for Community Behavioral Healthcare
Mauer B (2010) Substance use disorders and the person-centered healthcare home Rockville MD National Council for Community Behavioral Healthcare
Mauer B amp Jarvis D (2010) The business case for bidirectional integrated care Mental health and substance use services in primary care settings and primary care services in specialty mental health and substance use settings Integration Policy Initiative
Maine Health Access Foundation (2009) Site Self-Assessment
Miller BF Kessler R Peek CJ (2011) A national agenda for research in collaborative care Papers from the Collaborative Care Research Network Research Development Conference AHRQ Publication No 11-0067 Rockville MD Agency for Healthcare Research and Quality
Peek CJ (2007) Integrated Care Aids to Navigation Study packet for the Pennsylvania Eastern Ohio amp West Virginia Summit Integrating Mental Health and Primary Care Pittsburgh PA
Reynolds K (2006) Mental Health Primary Care Integration Options (Unpublished document)
Robinson PJ amp Reiter JT (2007) Behavioral consultation and primary care A guide to integrating services New York Springer
Russell L (2010) Mental health care services in primary care Tackling the issues in the context of health care reform Center for American Progress Washington DC
Seaburn Lorenz Gunn Gawinksi amp Mauksch (1996) Models of collaboration A guide for mental health professionals working with health care practitioners Basic Books
Strosahl K (1998) Integrating behavioral health and primary care services The primary mental health care model In Integrated primary care The future of medical and mental health collaboration edited by A Blount pp 139-66 New York WW Norton
Strosahl K amp Robinson P (2008) The primary care behavioral health model Applications to prevention acute care and chronic condition management In R Kessler amp D Strafford (Eds) Collaborative medicine case studies Evidence in practice New York Springer
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 1
Six
Lev
els
of C
olla
bo
ratio
nIn
tegr
atio
n (C
ore
Des
crip
tions
)
CO
OR
DIN
AT
ED
KE
y E
LEM
EN
T C
OM
MU
NIC
AT
ION
CO
LO
CA
TE
D
KE
y E
LEM
EN
T P
Hy
SIC
AL
PR
Ox
IMIT
y
INT
EG
RA
TE
D
KE
y E
LEM
EN
T P
RA
CT
ICE
CH
AN
GE
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
beh
avio
ral h
ealt
h p
rim
ary
care
an
d o
ther
hea
lth
care
pro
vid
ers
wo
rk
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
Com
mun
icat
e ab
out c
ases
on
ly ra
rely
and
und
erco
mpe
lling
circ
umst
ance
s
8 8 C
omm
unic
ate
driv
en b
y pr
ovid
er n
eed
8 M
ay n
ever
mee
t in
pers
on
8 H
ave
limite
d un
ders
tand
shyin
g of
eac
h ot
herrsquos
role
s
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
8Co
mm
unic
ate
perio
dica
llyab
out s
hare
d pa
tient
s
8 C
omm
unic
ate
driv
en b
y sp
ecifi
c pa
tient
issu
es
8 M
ay m
eet a
s pa
rt of
larg
er
com
mun
ity
8Ap
prec
iate
eac
h ot
herrsquos
ro
les
as re
sour
ces
secfi t f
o oy
n eti amli s c ya il ey
e f ar h
m ss e t
a e r
n s ece hI n w 8
Hav
e se
para
te s
yste
ms
8 C
omm
unic
ate
regu
larly
ab
out s
hare
d pa
tient
s b
y ph
one
or e
-mai
l
8 C
olla
bora
te d
riven
by
need
for e
ach
othe
rrsquos
serv
ices
and
mor
e re
liabl
e re
ferra
l
8M
eet o
ccas
iona
lly to
disc
uss
case
s du
e to
clo
sepr
oxim
ity
8 F
eel p
art o
f a la
rger
yet
no
n-fo
rmal
team
e h ey
n t h
ih e t
rti ee
w hc wya tp il
e s ica
ma e f
n s maI s 8
Sha
re s
ome
syst
ems
like
sc
hedu
ling
or m
edic
alre
cord
s
8Co
mm
unic
ate
in p
erso
nas
nee
ded
8 C
olla
bora
te d
riven
by
need
for c
onsu
ltatio
n an
dco
ordi
nate
d pl
ans
for
diffi
cult
patie
nts
8 H
ave
regu
lar f
ace-
to-fa
ce
inte
ract
ions
abo
ut s
ome
patie
nts
8 H
ave
a ba
sic
unde
rsta
ndin
g of
role
san
d cu
lture
e h all
n t erih in
gt hei ar
e w h w
s ec ya t acp ili p
e s c sa e
m f icea t
am acn s eyr hI s p t
e n m e i o rh est
y ( hi
e w ti wl )c i eca cap
e f a
e s p
mm a d s
e ae
sn
s reyh ha hI t s t 8Ac
tivel
y se
ek s
yste
m
solu
tions
toge
ther
or
deve
lop
work
-a-ro
unds
8Co
mm
unic
ate
frequ
ently
in p
erso
n
8 C
olla
bora
te d
riven
by
desi
re to
be
a m
embe
r of
the
care
team
8 H
ave
regu
lar t
eam
m
eetin
gs to
dis
cuss
ove
rall
patie
nt c
are
and
spec
ific
patie
nt is
sues
8 H
ave
an in
-dep
th u
nshyde
rsta
ndin
g of
role
s an
dcu
lture
8 H
ave
reso
lved
mos
t or a
ll sy
stem
issu
es f
unct
ioni
ng
as o
ne in
tegr
ated
sys
tem
8Co
mm
unic
ate
cons
iste
ntly
at th
e sy
stem
tea
m a
nd
indi
vidu
al le
vels
8 C
olla
bora
te d
riven
by
shar
ed c
once
pt o
f tea
mca
re
8 H
ave
form
al a
nd in
form
al
mee
tings
to s
uppo
rt in
tegr
ated
mod
el o
f car
e
8 H
ave
role
s an
d cu
lture
s th
at b
lur o
r ble
nd
10
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 2
A S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Clin
ical
Del
iver
y
Scr
eeni
ng a
nd a
sses
sshym
ent d
one
acco
rdin
g to
se
para
te p
ract
ice
mod
els
Sepa
rate
trea
tmen
t pla
ns
Ev
iden
ced-
base
d pr
actic
es (E
BP)
impl
emen
ted
sepa
rate
ly
8 8 8
Scre
enin
g ba
sed
on
sepa
rate
pra
ctic
es m
al
y be
mat
ion
ma
info
rsh
ared
thro
ugh
for
requ
ests
or H
ealth
m
atio
n Ex
chan
ges
Info
r
Sepa
rate
trea
tmen
t pl
ans
shar
ed b
ased
on
esta
blis
hed
rela
tion-
een
spec
ific
ship
s be
twvi
ders
pr
o
Sepa
rate
resp
onsi
bilit
y fo
r car
eEB
Ps
8 8 8
ree
on a
spe
cific
y
ag M
a
crite
ria fo
r mor
e ef
fect
ive
sc
reen
ing
or o
ther
ral
vice
pla
ns
ms e
in-h
ouse
refe
r
Sep
arat
e se
rwi
th s
ome
shar
ed
mat
ion
that
info
r
wled
g
info
rth
em
8
Som
e sh
ared
kno
s EB
Ps
of e
ach
othe
rrsquoes
peci
ally
for h
igh
utili
zers
88
A
gree
on
spec
ific
bas
ed o
n sc
reen
ing
abili
ty to
resp
ond
to
e tre
atm
ent
resu
lts
8
Col
labo
rativ
plan
ning
for s
peci
fic
patie
nts
Som
e EB
Ps a
nd s
ome
focu
sed
train
ing
shar
ed
on in
tere
st o
r spe
cific
po
pula
tion
need
s
8 8
Con
sist
ent s
et o
f agr
eed
upon
scr
eeni
ngs
acro
ss
disc
iplin
es w
hich
gui
de
vent
ions
e tre
atm
ent
treat
men
t int
er
8
Col
labo
rativ
plan
ning
for a
ll sh
ared
patie
nts
8
EBP
s sh
ared
acr
oss
sys-
tem
with
som
e jo
int m
onishy
torin
g of
hea
lth c
ondi
tions
fo
r som
e pa
tient
s
8
8 P
opul
atio
n-ba
sed
m
edic
al a
nd b
ehav
iora
l he
alth
scr
eeni
ng is
stan
dard
pra
ctic
e wi
thre
sults
ava
ilabl
e to
all
and
resp
onse
pro
toco
lsin
pla
ce
8On
e tre
atm
ent p
lan
for a
llpa
tient
s
8EB
Ps a
re te
am s
elec
ted
train
ed a
nd im
plem
ente
dac
ross
dis
cipl
ines
as
stan
dard
pra
ctic
e
Key
Dif
fere
ntia
tor
Pat
ien
t Exp
erie
nce
ysic
al a
nd b
eshy P
atie
nt p
hha
vior
al h
ealth
nee
ds a
re
treat
ed a
s se
para
te is
sues
otia
te
Pat
ient
mus
t neg
sepa
rate
pra
ctic
es a
nd
wn w
ith
rees
of s
ucce
ss
site
s on
thei
r oyi
ng d
egarv
8 8vi
der
P
atie
nt h
ealth
nee
ds
are
treat
ed s
epar
atel
ybu
t rec
ords
are
sha
red re
d
prom
otin
g be
tter p
ro riers
y
be re
fer
y pa
tient
s
e
arie
ty o
f bar
wled
gkn
o
Pat
ient
s m
abu
t a v
vent
man
pre
from
acc
essi
ng c
are
8 8
atie
nt h
ealth
nee
ds a
re y
y b
ws
P treat
ed s
epar
atel
y at
the
sam
e lo
catio
n
8
Clo
se p
roxim
ity a
llora
ls to
be
mor
e re
fer
succ
essf
ul a
nd e
asie
r for
ho
a
lthou
gh w ar
y v
red
ma
patie
nts
gets
refe
rvi
der
pro
8
col
labo
ratio
n m
ight
Pat
ient
nee
ds a
re tr
eate
d se
para
tely
at t
he s
ame
m h
and-
offs
to
vide
rs
site
in
clud
e wa
rot
her t
reat
men
t pro na
lly
Pat
ient
s ar
e in
ter
red
with
bet
ter f
ollo
wshyre
fer
up b
ut c
olla
bora
tion
may
st
ill b
e ex
perie
nced
as
vice
s se
para
te s
er
8 8
y
e on
Pat
ient
nee
ds a
re tr
eate
d as
a te
am fo
r sha
red
patie
nts
(for t
hose
wh
o sc
reen
pos
itiv
scre
enin
g m
easu
res)
and
sepa
rate
ly fo
r oth
ers
e to
8
Car
e is
resp
onsi
vid
entifi
ed p
atie
nt n
eeds
bvi
ders
as e a
of a
team
of p
ro w
hich
feel
s lik
need
ed
one-
stop
sho
p
8
All p
atie
nt h
ealth
nee
ds ar
e tre
ated
for a
ll pa
tient
sby
a te
am w
ho fu
nctio
n et
her
ely
tog
effe
ctiv
Pat
ient
s ex
perie
nce
a se
amle
ss re
spon
se to
all h
ealth
care
nee
ds a
s in
a u
nifie
d y
pres
ent
the
prac
tice
8 8
11
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
No
coo
rdin
atio
n or
ts
em
ent o
f e
effo
r
vide
r buy
-in
en
ratio
n or
ev
up
to
vide
rs to
man
agco
llabo
rativ
Litt
le p
roto
inte
gco
llabo
ratio
nin
divi
dual
pro
initi
ate
as ti
me
and
prac
tice
limits
allo
w
8 8
Som
e pr
actic
e le
ader
shysh
ip in
mor
e sy
stem
atic
vide
r buy
-into
al
ue
ving
nee
ded
mat
ion
shar
ing
info
r
Som
e pr
oco
llabo
ratio
n an
d v
plac
ed o
n ha
mat
ion
info
r
8 8
Org
aniza
tion
lead
ers
tive
but o
ften
colo
shysu
ppor
catio
n is
vie
wed
as
a pr
ojec
t or p
rogr
am ork
and
vide
r buy
-in to
ra
ls w
Pro mak
ing
refe
rap
prec
iatio
n of
ons
ite
vaila
bilit
y a
8 8
thro
ugh
mut
ual p
robl
em-
Org
aniza
tion
lead
ers
ratio
n t i
nteg
supp
or
solv
ing
of s
ome
syst
em
riers
ba
r
Mor
e bu
y-in
to c
once
pt
vide
rs
ratio
n bu
t not
of
inte
gco
nsis
tent
acr
oss
not
all
pro
tuni
ties
for
vide
rs
pro
usin
g op
por
inte
grat
ion
or c
ompo
nent
s
8 8
ts
w
Org
aniza
tion
lead
ers if
ra
tion
ws a
nd e
ffor
t int
egsu
ppor
fund
ing
allo
plac
ed in
sol
ving
as
man
y sy
stem
issu
es a
s w
ithou
t cha
ngshy
poss
ible
in
g fu
ndam
enta
lly h
odi
scip
lines
are
pra
ctic
ed
rate
d y
not
vide
rs
e in
pra
ctic
e
ly a
ll pr
o N
ear ag
ed in
inte
g B
uy-in
ma
y fo
r ind
ivid
ual
eng
mod
el
incl
ude
chan
g
vide
rs
stra
teg
pro
8 8
y e
ervi
ded
aniza
tion
lead
ers
t ra
tion
as p
ract
ice
Org
stro
ngly
sup
por
inte
gm
odel
with
exp
ecte
dvi
ce d
eliv
e in
ser
chan
g
for d
evel
opm
ent
rate
d ca
re a
nd a
ll In
teg
com
pone
nts
embr
aced
vide
rs a
nd a
ctiv
and
reso
urce
s pr
o
by a
ll pr
ool
vem
ent i
n pr
actic
e e
vin ch
ang
8 8
Tab
le 2
b S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs c
ont
inue
d)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Pra
ctic
eO
rgan
izat
ion
Key
Dif
fere
ntia
tor
bu
sin
ess
Mo
del
Se
para
te fu
ndin
g
No s
harin
g of
reso
urce
s
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re re
sour
ces
for
sing
le p
roje
cts
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re fa
cilit
y ex
pens
es
Sepa
rate
bill
ing
prac
tices
8 8 8
but
may
S
epar
ate
fund
ing
rant
s sta
ffing
cos
ts
shar
e g
y sh
are
offic
e
uctu
re
Ma
expe
nses
or
infra
str
Sepa
rate
bill
ing
due
to
riers
sy
stem
bar
8 8 8
Bl
ende
d fu
ndin
g ba
sed
uctu
re
on c
ontra
cts
gra
nts
or
ys to
str
agre
emen
ts
Varie
ty o
f wa
8
the
shar
ing
of a
ll ex
pens
es
Billi
ng fu
nctio
n co
mbi
ned
reed
upo
n pr
oces
s or
ag
8 8
8 8Re
sour
ces
shar
ed a
nd
hole
rate
d fu
ndin
g In
teg
base
d on
mul
tiple
sour
ces
of re
venu
e
allo
cate
d ac
ross
wpr
actic
e
Billi
ng m
axim
ized
for
rate
d m
odel
and
uc
ture
in
teg
sing
le b
illin
g st
r
8
12
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 3
Ad
vant
ages
and
Wea
knes
ses
at E
ach
Leve
l of C
olla
bo
ratio
nIn
tegr
atio
n
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Ad
van
tag
es
8 E
ach
prac
tice
can
mak
e tim
ely
and
auto
nom
ous
deci
sion
s ab
out c
are
8Re
adily
und
erst
ood
asa
prac
tice
mod
el b
y pa
tient
s an
d pr
ovid
ers
8 M
aint
ains
eac
h pr
actic
ersquos
basi
c op
erat
ing
stru
ctur
eso
cha
nge
is n
ot a
di
srup
tive
fact
or
8 P
rovi
des
som
e co
ordi
natio
n an
din
form
atio
n-sh
arin
g th
at
is h
elpf
ul to
bot
h pa
tient
san
d pr
ovid
ers
8 C
oloc
atio
n al
lows
for
mor
e di
rect
inte
ract
ion
and
com
mun
icat
ion
amon
g pr
ofes
sion
als
toim
pact
pat
ient
car
e
8 R
efer
rals
mor
e su
cces
sful
du
e to
pro
ximity
8 O
ppor
tuni
ty to
dev
elop
cl
oser
pro
fess
iona
l rel
ashytio
nshi
ps
8 R
emov
al o
f som
e sy
stem
ba
rrier
s li
ke s
epar
ate
reco
rds
allo
ws c
lose
r co
llabo
ratio
n to
occ
ur
8 B
oth
beha
vior
al h
ealth
an
d m
edic
al p
rovi
ders
ca
n be
com
e m
ore
well-
info
rmed
abo
ut w
hat e
ach
can
prov
ide
8 P
atie
nts
are
view
ed a
s sh
ared
whi
ch fa
cilit
ates
m
ore
com
plet
e tre
atm
ent
plan
s
8 H
igh
leve
l of c
olla
bora
tion
lead
s to
mor
e re
spon
sive
pa
tient
car
e in
crea
sing
en
gage
men
t and
ad
here
nce
to tr
eatm
ent
plan
s
8 P
rovi
der fl
exib
ility
in
crea
ses
as s
yste
mis
sues
and
bar
riers
are
re
solve
d
8 B
oth
prov
ider
and
pat
ient
sa
tisfa
ctio
n m
ay in
crea
se
8 O
ppor
tuni
ty to
trul
y tre
at
whol
e pe
rson
8Al
l or a
lmos
t all
syst
emba
rrier
s re
solve
d a
llowi
ng
prov
ider
s to
pra
ctic
e as
hi
gh fu
nctio
ning
team
8Al
l pat
ient
nee
dsad
dres
sed
as th
ey o
ccur
8 S
hare
d kn
owle
dge
base
of
pro
vide
rs in
crea
ses
and
allo
ws e
ach
prof
essi
onal
to
resp
ond
mor
e br
oadl
yan
d ad
equa
tely
to a
ny
issu
e
Wea
knes
ses
8 S
ervi
ces
may
ove
rlap
be
dupl
icat
ed o
r eve
n wo
rk
agai
nst e
ach
othe
r
8 Im
porta
nt a
spec
ts o
f car
e m
ay n
ot b
e ad
dres
sed
or ta
ke a
long
tim
e to
be
diag
nose
d
8 S
harin
g of
info
rmat
ion
may
not
be
syst
emat
ic
enou
gh to
effe
ct o
vera
ll pa
tient
car
e
8 N
o gu
aran
tee
that
info
rshym
atio
n wi
ll ch
ange
pla
n or
st
rate
gy o
f eac
h pr
ovid
er
8 R
efer
rals
may
fail
due
to
barri
ers
lead
ing
to p
atie
nt
and
prov
ider
frus
tratio
n
8 P
roxim
ity m
ay n
ot le
ad to
gr
eate
r col
labo
ratio
nlim
iting
val
ue
8 E
ffort
is re
quire
d to
de
velo
p re
latio
nshi
ps
8 L
imite
d fle
xibili
ty if
tra
ditio
nal r
oles
are
mai
ntai
ned
8 S
yste
m is
sues
may
lim
it co
llabo
ratio
n
8 P
oten
tial f
or te
nsio
n an
d co
nflic
ting
agen
das
amon
g pr
ovid
ers
as p
ract
ice
boun
darie
s lo
osen
8 P
ract
ice
chan
ges
may
cr
eate
lack
of fi
t for
som
ees
tabl
ishe
d pr
ovid
ers
8Ti
me
is n
eede
d to
co
llabo
rate
at t
his
high
leve
l and
may
affe
ct
prac
tice
prod
uctiv
ity o
rca
denc
e of
car
e
8 S
usta
inab
ility
issu
es m
ay
stre
ss th
e pr
actic
e
8 F
ew m
odel
s at
this
leve
l wi
th e
noug
h ex
perie
nce
tosu
ppor
t val
ue
8Ou
tcom
e ex
pect
atio
ns n
otye
t est
ablis
hed
13

SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 1
Six
Lev
els
of C
olla
bo
ratio
nIn
tegr
atio
n (C
ore
Des
crip
tions
)
CO
OR
DIN
AT
ED
KE
y E
LEM
EN
T C
OM
MU
NIC
AT
ION
CO
LO
CA
TE
D
KE
y E
LEM
EN
T P
Hy
SIC
AL
PR
Ox
IMIT
y
INT
EG
RA
TE
D
KE
y E
LEM
EN
T P
RA
CT
ICE
CH
AN
GE
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
beh
avio
ral h
ealt
h p
rim
ary
care
an
d o
ther
hea
lth
care
pro
vid
ers
wo
rk
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
Com
mun
icat
e ab
out c
ases
on
ly ra
rely
and
und
erco
mpe
lling
circ
umst
ance
s
8 8 C
omm
unic
ate
driv
en b
y pr
ovid
er n
eed
8 M
ay n
ever
mee
t in
pers
on
8 H
ave
limite
d un
ders
tand
shyin
g of
eac
h ot
herrsquos
role
s
In s
epar
ate
faci
litie
swh
ere
they
8 H
ave
sepa
rate
sys
tem
s
8Co
mm
unic
ate
perio
dica
llyab
out s
hare
d pa
tient
s
8 C
omm
unic
ate
driv
en b
y sp
ecifi
c pa
tient
issu
es
8 M
ay m
eet a
s pa
rt of
larg
er
com
mun
ity
8Ap
prec
iate
eac
h ot
herrsquos
ro
les
as re
sour
ces
secfi t f
o oy
n eti amli s c ya il ey
e f ar h
m ss e t
a e r
n s ece hI n w 8
Hav
e se
para
te s
yste
ms
8 C
omm
unic
ate
regu
larly
ab
out s
hare
d pa
tient
s b
y ph
one
or e
-mai
l
8 C
olla
bora
te d
riven
by
need
for e
ach
othe
rrsquos
serv
ices
and
mor
e re
liabl
e re
ferra
l
8M
eet o
ccas
iona
lly to
disc
uss
case
s du
e to
clo
sepr
oxim
ity
8 F
eel p
art o
f a la
rger
yet
no
n-fo
rmal
team
e h ey
n t h
ih e t
rti ee
w hc wya tp il
e s ica
ma e f
n s maI s 8
Sha
re s
ome
syst
ems
like
sc
hedu
ling
or m
edic
alre
cord
s
8Co
mm
unic
ate
in p
erso
nas
nee
ded
8 C
olla
bora
te d
riven
by
need
for c
onsu
ltatio
n an
dco
ordi
nate
d pl
ans
for
diffi
cult
patie
nts
8 H
ave
regu
lar f
ace-
to-fa
ce
inte
ract
ions
abo
ut s
ome
patie
nts
8 H
ave
a ba
sic
unde
rsta
ndin
g of
role
san
d cu
lture
e h all
n t erih in
gt hei ar
e w h w
s ec ya t acp ili p
e s c sa e
m f icea t
am acn s eyr hI s p t
e n m e i o rh est
y ( hi
e w ti wl )c i eca cap
e f a
e s p
mm a d s
e ae
sn
s reyh ha hI t s t 8Ac
tivel
y se
ek s
yste
m
solu
tions
toge
ther
or
deve
lop
work
-a-ro
unds
8Co
mm
unic
ate
frequ
ently
in p
erso
n
8 C
olla
bora
te d
riven
by
desi
re to
be
a m
embe
r of
the
care
team
8 H
ave
regu
lar t
eam
m
eetin
gs to
dis
cuss
ove
rall
patie
nt c
are
and
spec
ific
patie
nt is
sues
8 H
ave
an in
-dep
th u
nshyde
rsta
ndin
g of
role
s an
dcu
lture
8 H
ave
reso
lved
mos
t or a
ll sy
stem
issu
es f
unct
ioni
ng
as o
ne in
tegr
ated
sys
tem
8Co
mm
unic
ate
cons
iste
ntly
at th
e sy
stem
tea
m a
nd
indi
vidu
al le
vels
8 C
olla
bora
te d
riven
by
shar
ed c
once
pt o
f tea
mca
re
8 H
ave
form
al a
nd in
form
al
mee
tings
to s
uppo
rt in
tegr
ated
mod
el o
f car
e
8 H
ave
role
s an
d cu
lture
s th
at b
lur o
r ble
nd
10
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 2
A S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Clin
ical
Del
iver
y
Scr
eeni
ng a
nd a
sses
sshym
ent d
one
acco
rdin
g to
se
para
te p
ract
ice
mod
els
Sepa
rate
trea
tmen
t pla
ns
Ev
iden
ced-
base
d pr
actic
es (E
BP)
impl
emen
ted
sepa
rate
ly
8 8 8
Scre
enin
g ba
sed
on
sepa
rate
pra
ctic
es m
al
y be
mat
ion
ma
info
rsh
ared
thro
ugh
for
requ
ests
or H
ealth
m
atio
n Ex
chan
ges
Info
r
Sepa
rate
trea
tmen
t pl
ans
shar
ed b
ased
on
esta
blis
hed
rela
tion-
een
spec
ific
ship
s be
twvi
ders
pr
o
Sepa
rate
resp
onsi
bilit
y fo
r car
eEB
Ps
8 8 8
ree
on a
spe
cific
y
ag M
a
crite
ria fo
r mor
e ef
fect
ive
sc
reen
ing
or o
ther
ral
vice
pla
ns
ms e
in-h
ouse
refe
r
Sep
arat
e se
rwi
th s
ome
shar
ed
mat
ion
that
info
r
wled
g
info
rth
em
8
Som
e sh
ared
kno
s EB
Ps
of e
ach
othe
rrsquoes
peci
ally
for h
igh
utili
zers
88
A
gree
on
spec
ific
bas
ed o
n sc
reen
ing
abili
ty to
resp
ond
to
e tre
atm
ent
resu
lts
8
Col
labo
rativ
plan
ning
for s
peci
fic
patie
nts
Som
e EB
Ps a
nd s
ome
focu
sed
train
ing
shar
ed
on in
tere
st o
r spe
cific
po
pula
tion
need
s
8 8
Con
sist
ent s
et o
f agr
eed
upon
scr
eeni
ngs
acro
ss
disc
iplin
es w
hich
gui
de
vent
ions
e tre
atm
ent
treat
men
t int
er
8
Col
labo
rativ
plan
ning
for a
ll sh
ared
patie
nts
8
EBP
s sh
ared
acr
oss
sys-
tem
with
som
e jo
int m
onishy
torin
g of
hea
lth c
ondi
tions
fo
r som
e pa
tient
s
8
8 P
opul
atio
n-ba
sed
m
edic
al a
nd b
ehav
iora
l he
alth
scr
eeni
ng is
stan
dard
pra
ctic
e wi
thre
sults
ava
ilabl
e to
all
and
resp
onse
pro
toco
lsin
pla
ce
8On
e tre
atm
ent p
lan
for a
llpa
tient
s
8EB
Ps a
re te
am s
elec
ted
train
ed a
nd im
plem
ente
dac
ross
dis
cipl
ines
as
stan
dard
pra
ctic
e
Key
Dif
fere
ntia
tor
Pat
ien
t Exp
erie
nce
ysic
al a
nd b
eshy P
atie
nt p
hha
vior
al h
ealth
nee
ds a
re
treat
ed a
s se
para
te is
sues
otia
te
Pat
ient
mus
t neg
sepa
rate
pra
ctic
es a
nd
wn w
ith
rees
of s
ucce
ss
site
s on
thei
r oyi
ng d
egarv
8 8vi
der
P
atie
nt h
ealth
nee
ds
are
treat
ed s
epar
atel
ybu
t rec
ords
are
sha
red re
d
prom
otin
g be
tter p
ro riers
y
be re
fer
y pa
tient
s
e
arie
ty o
f bar
wled
gkn
o
Pat
ient
s m
abu
t a v
vent
man
pre
from
acc
essi
ng c
are
8 8
atie
nt h
ealth
nee
ds a
re y
y b
ws
P treat
ed s
epar
atel
y at
the
sam
e lo
catio
n
8
Clo
se p
roxim
ity a
llora
ls to
be
mor
e re
fer
succ
essf
ul a
nd e
asie
r for
ho
a
lthou
gh w ar
y v
red
ma
patie
nts
gets
refe
rvi
der
pro
8
col
labo
ratio
n m
ight
Pat
ient
nee
ds a
re tr
eate
d se
para
tely
at t
he s
ame
m h
and-
offs
to
vide
rs
site
in
clud
e wa
rot
her t
reat
men
t pro na
lly
Pat
ient
s ar
e in
ter
red
with
bet
ter f
ollo
wshyre
fer
up b
ut c
olla
bora
tion
may
st
ill b
e ex
perie
nced
as
vice
s se
para
te s
er
8 8
y
e on
Pat
ient
nee
ds a
re tr
eate
d as
a te
am fo
r sha
red
patie
nts
(for t
hose
wh
o sc
reen
pos
itiv
scre
enin
g m
easu
res)
and
sepa
rate
ly fo
r oth
ers
e to
8
Car
e is
resp
onsi
vid
entifi
ed p
atie
nt n
eeds
bvi
ders
as e a
of a
team
of p
ro w
hich
feel
s lik
need
ed
one-
stop
sho
p
8
All p
atie
nt h
ealth
nee
ds ar
e tre
ated
for a
ll pa
tient
sby
a te
am w
ho fu
nctio
n et
her
ely
tog
effe
ctiv
Pat
ient
s ex
perie
nce
a se
amle
ss re
spon
se to
all h
ealth
care
nee
ds a
s in
a u
nifie
d y
pres
ent
the
prac
tice
8 8
11
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
No
coo
rdin
atio
n or
ts
em
ent o
f e
effo
r
vide
r buy
-in
en
ratio
n or
ev
up
to
vide
rs to
man
agco
llabo
rativ
Litt
le p
roto
inte
gco
llabo
ratio
nin
divi
dual
pro
initi
ate
as ti
me
and
prac
tice
limits
allo
w
8 8
Som
e pr
actic
e le
ader
shysh
ip in
mor
e sy
stem
atic
vide
r buy
-into
al
ue
ving
nee
ded
mat
ion
shar
ing
info
r
Som
e pr
oco
llabo
ratio
n an
d v
plac
ed o
n ha
mat
ion
info
r
8 8
Org
aniza
tion
lead
ers
tive
but o
ften
colo
shysu
ppor
catio
n is
vie
wed
as
a pr
ojec
t or p
rogr
am ork
and
vide
r buy
-in to
ra
ls w
Pro mak
ing
refe
rap
prec
iatio
n of
ons
ite
vaila
bilit
y a
8 8
thro
ugh
mut
ual p
robl
em-
Org
aniza
tion
lead
ers
ratio
n t i
nteg
supp
or
solv
ing
of s
ome
syst
em
riers
ba
r
Mor
e bu
y-in
to c
once
pt
vide
rs
ratio
n bu
t not
of
inte
gco
nsis
tent
acr
oss
not
all
pro
tuni
ties
for
vide
rs
pro
usin
g op
por
inte
grat
ion
or c
ompo
nent
s
8 8
ts
w
Org
aniza
tion
lead
ers if
ra
tion
ws a
nd e
ffor
t int
egsu
ppor
fund
ing
allo
plac
ed in
sol
ving
as
man
y sy
stem
issu
es a
s w
ithou
t cha
ngshy
poss
ible
in
g fu
ndam
enta
lly h
odi
scip
lines
are
pra
ctic
ed
rate
d y
not
vide
rs
e in
pra
ctic
e
ly a
ll pr
o N
ear ag
ed in
inte
g B
uy-in
ma
y fo
r ind
ivid
ual
eng
mod
el
incl
ude
chan
g
vide
rs
stra
teg
pro
8 8
y e
ervi
ded
aniza
tion
lead
ers
t ra
tion
as p
ract
ice
Org
stro
ngly
sup
por
inte
gm
odel
with
exp
ecte
dvi
ce d
eliv
e in
ser
chan
g
for d
evel
opm
ent
rate
d ca
re a
nd a
ll In
teg
com
pone
nts
embr
aced
vide
rs a
nd a
ctiv
and
reso
urce
s pr
o
by a
ll pr
ool
vem
ent i
n pr
actic
e e
vin ch
ang
8 8
Tab
le 2
b S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs c
ont
inue
d)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Pra
ctic
eO
rgan
izat
ion
Key
Dif
fere
ntia
tor
bu
sin
ess
Mo
del
Se
para
te fu
ndin
g
No s
harin
g of
reso
urce
s
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re re
sour
ces
for
sing
le p
roje
cts
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re fa
cilit
y ex
pens
es
Sepa
rate
bill
ing
prac
tices
8 8 8
but
may
S
epar
ate
fund
ing
rant
s sta
ffing
cos
ts
shar
e g
y sh
are
offic
e
uctu
re
Ma
expe
nses
or
infra
str
Sepa
rate
bill
ing
due
to
riers
sy
stem
bar
8 8 8
Bl
ende
d fu
ndin
g ba
sed
uctu
re
on c
ontra
cts
gra
nts
or
ys to
str
agre
emen
ts
Varie
ty o
f wa
8
the
shar
ing
of a
ll ex
pens
es
Billi
ng fu
nctio
n co
mbi
ned
reed
upo
n pr
oces
s or
ag
8 8
8 8Re
sour
ces
shar
ed a
nd
hole
rate
d fu
ndin
g In
teg
base
d on
mul
tiple
sour
ces
of re
venu
e
allo
cate
d ac
ross
wpr
actic
e
Billi
ng m
axim
ized
for
rate
d m
odel
and
uc
ture
in
teg
sing
le b
illin
g st
r
8
12
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 3
Ad
vant
ages
and
Wea
knes
ses
at E
ach
Leve
l of C
olla
bo
ratio
nIn
tegr
atio
n
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Ad
van
tag
es
8 E
ach
prac
tice
can
mak
e tim
ely
and
auto
nom
ous
deci
sion
s ab
out c
are
8Re
adily
und
erst
ood
asa
prac
tice
mod
el b
y pa
tient
s an
d pr
ovid
ers
8 M
aint
ains
eac
h pr
actic
ersquos
basi
c op
erat
ing
stru
ctur
eso
cha
nge
is n
ot a
di
srup
tive
fact
or
8 P
rovi
des
som
e co
ordi
natio
n an
din
form
atio
n-sh
arin
g th
at
is h
elpf
ul to
bot
h pa
tient
san
d pr
ovid
ers
8 C
oloc
atio
n al
lows
for
mor
e di
rect
inte
ract
ion
and
com
mun
icat
ion
amon
g pr
ofes
sion
als
toim
pact
pat
ient
car
e
8 R
efer
rals
mor
e su
cces
sful
du
e to
pro
ximity
8 O
ppor
tuni
ty to
dev
elop
cl
oser
pro
fess
iona
l rel
ashytio
nshi
ps
8 R
emov
al o
f som
e sy
stem
ba
rrier
s li
ke s
epar
ate
reco
rds
allo
ws c
lose
r co
llabo
ratio
n to
occ
ur
8 B
oth
beha
vior
al h
ealth
an
d m
edic
al p
rovi
ders
ca
n be
com
e m
ore
well-
info
rmed
abo
ut w
hat e
ach
can
prov
ide
8 P
atie
nts
are
view
ed a
s sh
ared
whi
ch fa
cilit
ates
m
ore
com
plet
e tre
atm
ent
plan
s
8 H
igh
leve
l of c
olla
bora
tion
lead
s to
mor
e re
spon
sive
pa
tient
car
e in
crea
sing
en
gage
men
t and
ad
here
nce
to tr
eatm
ent
plan
s
8 P
rovi
der fl
exib
ility
in
crea
ses
as s
yste
mis
sues
and
bar
riers
are
re
solve
d
8 B
oth
prov
ider
and
pat
ient
sa
tisfa
ctio
n m
ay in
crea
se
8 O
ppor
tuni
ty to
trul
y tre
at
whol
e pe
rson
8Al
l or a
lmos
t all
syst
emba
rrier
s re
solve
d a
llowi
ng
prov
ider
s to
pra
ctic
e as
hi
gh fu
nctio
ning
team
8Al
l pat
ient
nee
dsad
dres
sed
as th
ey o
ccur
8 S
hare
d kn
owle
dge
base
of
pro
vide
rs in
crea
ses
and
allo
ws e
ach
prof
essi
onal
to
resp
ond
mor
e br
oadl
yan
d ad
equa
tely
to a
ny
issu
e
Wea
knes
ses
8 S
ervi
ces
may
ove
rlap
be
dupl
icat
ed o
r eve
n wo
rk
agai
nst e
ach
othe
r
8 Im
porta
nt a
spec
ts o
f car
e m
ay n
ot b
e ad
dres
sed
or ta
ke a
long
tim
e to
be
diag
nose
d
8 S
harin
g of
info
rmat
ion
may
not
be
syst
emat
ic
enou
gh to
effe
ct o
vera
ll pa
tient
car
e
8 N
o gu
aran
tee
that
info
rshym
atio
n wi
ll ch
ange
pla
n or
st
rate
gy o
f eac
h pr
ovid
er
8 R
efer
rals
may
fail
due
to
barri
ers
lead
ing
to p
atie
nt
and
prov
ider
frus
tratio
n
8 P
roxim
ity m
ay n
ot le
ad to
gr
eate
r col
labo
ratio
nlim
iting
val
ue
8 E
ffort
is re
quire
d to
de
velo
p re
latio
nshi
ps
8 L
imite
d fle
xibili
ty if
tra
ditio
nal r
oles
are
mai
ntai
ned
8 S
yste
m is
sues
may
lim
it co
llabo
ratio
n
8 P
oten
tial f
or te
nsio
n an
d co
nflic
ting
agen
das
amon
g pr
ovid
ers
as p
ract
ice
boun
darie
s lo
osen
8 P
ract
ice
chan
ges
may
cr
eate
lack
of fi
t for
som
ees
tabl
ishe
d pr
ovid
ers
8Ti
me
is n
eede
d to
co
llabo
rate
at t
his
high
leve
l and
may
affe
ct
prac
tice
prod
uctiv
ity o
rca
denc
e of
car
e
8 S
usta
inab
ility
issu
es m
ay
stre
ss th
e pr
actic
e
8 F
ew m
odel
s at
this
leve
l wi
th e
noug
h ex
perie
nce
tosu
ppor
t val
ue
8Ou
tcom
e ex
pect
atio
ns n
otye
t est
ablis
hed
13

SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 2
A S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Clin
ical
Del
iver
y
Scr
eeni
ng a
nd a
sses
sshym
ent d
one
acco
rdin
g to
se
para
te p
ract
ice
mod
els
Sepa
rate
trea
tmen
t pla
ns
Ev
iden
ced-
base
d pr
actic
es (E
BP)
impl
emen
ted
sepa
rate
ly
8 8 8
Scre
enin
g ba
sed
on
sepa
rate
pra
ctic
es m
al
y be
mat
ion
ma
info
rsh
ared
thro
ugh
for
requ
ests
or H
ealth
m
atio
n Ex
chan
ges
Info
r
Sepa
rate
trea
tmen
t pl
ans
shar
ed b
ased
on
esta
blis
hed
rela
tion-
een
spec
ific
ship
s be
twvi
ders
pr
o
Sepa
rate
resp
onsi
bilit
y fo
r car
eEB
Ps
8 8 8
ree
on a
spe
cific
y
ag M
a
crite
ria fo
r mor
e ef
fect
ive
sc
reen
ing
or o
ther
ral
vice
pla
ns
ms e
in-h
ouse
refe
r
Sep
arat
e se
rwi
th s
ome
shar
ed
mat
ion
that
info
r
wled
g
info
rth
em
8
Som
e sh
ared
kno
s EB
Ps
of e
ach
othe
rrsquoes
peci
ally
for h
igh
utili
zers
88
A
gree
on
spec
ific
bas
ed o
n sc
reen
ing
abili
ty to
resp
ond
to
e tre
atm
ent
resu
lts
8
Col
labo
rativ
plan
ning
for s
peci
fic
patie
nts
Som
e EB
Ps a
nd s
ome
focu
sed
train
ing
shar
ed
on in
tere
st o
r spe
cific
po
pula
tion
need
s
8 8
Con
sist
ent s
et o
f agr
eed
upon
scr
eeni
ngs
acro
ss
disc
iplin
es w
hich
gui
de
vent
ions
e tre
atm
ent
treat
men
t int
er
8
Col
labo
rativ
plan
ning
for a
ll sh
ared
patie
nts
8
EBP
s sh
ared
acr
oss
sys-
tem
with
som
e jo
int m
onishy
torin
g of
hea
lth c
ondi
tions
fo
r som
e pa
tient
s
8
8 P
opul
atio
n-ba
sed
m
edic
al a
nd b
ehav
iora
l he
alth
scr
eeni
ng is
stan
dard
pra
ctic
e wi
thre
sults
ava
ilabl
e to
all
and
resp
onse
pro
toco
lsin
pla
ce
8On
e tre
atm
ent p
lan
for a
llpa
tient
s
8EB
Ps a
re te
am s
elec
ted
train
ed a
nd im
plem
ente
dac
ross
dis
cipl
ines
as
stan
dard
pra
ctic
e
Key
Dif
fere
ntia
tor
Pat
ien
t Exp
erie
nce
ysic
al a
nd b
eshy P
atie
nt p
hha
vior
al h
ealth
nee
ds a
re
treat
ed a
s se
para
te is
sues
otia
te
Pat
ient
mus
t neg
sepa
rate
pra
ctic
es a
nd
wn w
ith
rees
of s
ucce
ss
site
s on
thei
r oyi
ng d
egarv
8 8vi
der
P
atie
nt h
ealth
nee
ds
are
treat
ed s
epar
atel
ybu
t rec
ords
are
sha
red re
d
prom
otin
g be
tter p
ro riers
y
be re
fer
y pa
tient
s
e
arie
ty o
f bar
wled
gkn
o
Pat
ient
s m
abu
t a v
vent
man
pre
from
acc
essi
ng c
are
8 8
atie
nt h
ealth
nee
ds a
re y
y b
ws
P treat
ed s
epar
atel
y at
the
sam
e lo
catio
n
8
Clo
se p
roxim
ity a
llora
ls to
be
mor
e re
fer
succ
essf
ul a
nd e
asie
r for
ho
a
lthou
gh w ar
y v
red
ma
patie
nts
gets
refe
rvi
der
pro
8
col
labo
ratio
n m
ight
Pat
ient
nee
ds a
re tr
eate
d se
para
tely
at t
he s
ame
m h
and-
offs
to
vide
rs
site
in
clud
e wa
rot
her t
reat
men
t pro na
lly
Pat
ient
s ar
e in
ter
red
with
bet
ter f
ollo
wshyre
fer
up b
ut c
olla
bora
tion
may
st
ill b
e ex
perie
nced
as
vice
s se
para
te s
er
8 8
y
e on
Pat
ient
nee
ds a
re tr
eate
d as
a te
am fo
r sha
red
patie
nts
(for t
hose
wh
o sc
reen
pos
itiv
scre
enin
g m
easu
res)
and
sepa
rate
ly fo
r oth
ers
e to
8
Car
e is
resp
onsi
vid
entifi
ed p
atie
nt n
eeds
bvi
ders
as e a
of a
team
of p
ro w
hich
feel
s lik
need
ed
one-
stop
sho
p
8
All p
atie
nt h
ealth
nee
ds ar
e tre
ated
for a
ll pa
tient
sby
a te
am w
ho fu
nctio
n et
her
ely
tog
effe
ctiv
Pat
ient
s ex
perie
nce
a se
amle
ss re
spon
se to
all h
ealth
care
nee
ds a
s in
a u
nifie
d y
pres
ent
the
prac
tice
8 8
11
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
No
coo
rdin
atio
n or
ts
em
ent o
f e
effo
r
vide
r buy
-in
en
ratio
n or
ev
up
to
vide
rs to
man
agco
llabo
rativ
Litt
le p
roto
inte
gco
llabo
ratio
nin
divi
dual
pro
initi
ate
as ti
me
and
prac
tice
limits
allo
w
8 8
Som
e pr
actic
e le
ader
shysh
ip in
mor
e sy
stem
atic
vide
r buy
-into
al
ue
ving
nee
ded
mat
ion
shar
ing
info
r
Som
e pr
oco
llabo
ratio
n an
d v
plac
ed o
n ha
mat
ion
info
r
8 8
Org
aniza
tion
lead
ers
tive
but o
ften
colo
shysu
ppor
catio
n is
vie
wed
as
a pr
ojec
t or p
rogr
am ork
and
vide
r buy
-in to
ra
ls w
Pro mak
ing
refe
rap
prec
iatio
n of
ons
ite
vaila
bilit
y a
8 8
thro
ugh
mut
ual p
robl
em-
Org
aniza
tion
lead
ers
ratio
n t i
nteg
supp
or
solv
ing
of s
ome
syst
em
riers
ba
r
Mor
e bu
y-in
to c
once
pt
vide
rs
ratio
n bu
t not
of
inte
gco
nsis
tent
acr
oss
not
all
pro
tuni
ties
for
vide
rs
pro
usin
g op
por
inte
grat
ion
or c
ompo
nent
s
8 8
ts
w
Org
aniza
tion
lead
ers if
ra
tion
ws a
nd e
ffor
t int
egsu
ppor
fund
ing
allo
plac
ed in
sol
ving
as
man
y sy
stem
issu
es a
s w
ithou
t cha
ngshy
poss
ible
in
g fu
ndam
enta
lly h
odi
scip
lines
are
pra
ctic
ed
rate
d y
not
vide
rs
e in
pra
ctic
e
ly a
ll pr
o N
ear ag
ed in
inte
g B
uy-in
ma
y fo
r ind
ivid
ual
eng
mod
el
incl
ude
chan
g
vide
rs
stra
teg
pro
8 8
y e
ervi
ded
aniza
tion
lead
ers
t ra
tion
as p
ract
ice
Org
stro
ngly
sup
por
inte
gm
odel
with
exp
ecte
dvi
ce d
eliv
e in
ser
chan
g
for d
evel
opm
ent
rate
d ca
re a
nd a
ll In
teg
com
pone
nts
embr
aced
vide
rs a
nd a
ctiv
and
reso
urce
s pr
o
by a
ll pr
ool
vem
ent i
n pr
actic
e e
vin ch
ang
8 8
Tab
le 2
b S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs c
ont
inue
d)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Pra
ctic
eO
rgan
izat
ion
Key
Dif
fere
ntia
tor
bu
sin
ess
Mo
del
Se
para
te fu
ndin
g
No s
harin
g of
reso
urce
s
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re re
sour
ces
for
sing
le p
roje
cts
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re fa
cilit
y ex
pens
es
Sepa
rate
bill
ing
prac
tices
8 8 8
but
may
S
epar
ate
fund
ing
rant
s sta
ffing
cos
ts
shar
e g
y sh
are
offic
e
uctu
re
Ma
expe
nses
or
infra
str
Sepa
rate
bill
ing
due
to
riers
sy
stem
bar
8 8 8
Bl
ende
d fu
ndin
g ba
sed
uctu
re
on c
ontra
cts
gra
nts
or
ys to
str
agre
emen
ts
Varie
ty o
f wa
8
the
shar
ing
of a
ll ex
pens
es
Billi
ng fu
nctio
n co
mbi
ned
reed
upo
n pr
oces
s or
ag
8 8
8 8Re
sour
ces
shar
ed a
nd
hole
rate
d fu
ndin
g In
teg
base
d on
mul
tiple
sour
ces
of re
venu
e
allo
cate
d ac
ross
wpr
actic
e
Billi
ng m
axim
ized
for
rate
d m
odel
and
uc
ture
in
teg
sing
le b
illin
g st
r
8
12
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 3
Ad
vant
ages
and
Wea
knes
ses
at E
ach
Leve
l of C
olla
bo
ratio
nIn
tegr
atio
n
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Ad
van
tag
es
8 E
ach
prac
tice
can
mak
e tim
ely
and
auto
nom
ous
deci
sion
s ab
out c
are
8Re
adily
und
erst
ood
asa
prac
tice
mod
el b
y pa
tient
s an
d pr
ovid
ers
8 M
aint
ains
eac
h pr
actic
ersquos
basi
c op
erat
ing
stru
ctur
eso
cha
nge
is n
ot a
di
srup
tive
fact
or
8 P
rovi
des
som
e co
ordi
natio
n an
din
form
atio
n-sh
arin
g th
at
is h
elpf
ul to
bot
h pa
tient
san
d pr
ovid
ers
8 C
oloc
atio
n al
lows
for
mor
e di
rect
inte
ract
ion
and
com
mun
icat
ion
amon
g pr
ofes
sion
als
toim
pact
pat
ient
car
e
8 R
efer
rals
mor
e su
cces
sful
du
e to
pro
ximity
8 O
ppor
tuni
ty to
dev
elop
cl
oser
pro
fess
iona
l rel
ashytio
nshi
ps
8 R
emov
al o
f som
e sy
stem
ba
rrier
s li
ke s
epar
ate
reco
rds
allo
ws c
lose
r co
llabo
ratio
n to
occ
ur
8 B
oth
beha
vior
al h
ealth
an
d m
edic
al p
rovi
ders
ca
n be
com
e m
ore
well-
info
rmed
abo
ut w
hat e
ach
can
prov
ide
8 P
atie
nts
are
view
ed a
s sh
ared
whi
ch fa
cilit
ates
m
ore
com
plet
e tre
atm
ent
plan
s
8 H
igh
leve
l of c
olla
bora
tion
lead
s to
mor
e re
spon
sive
pa
tient
car
e in
crea
sing
en
gage
men
t and
ad
here
nce
to tr
eatm
ent
plan
s
8 P
rovi
der fl
exib
ility
in
crea
ses
as s
yste
mis
sues
and
bar
riers
are
re
solve
d
8 B
oth
prov
ider
and
pat
ient
sa
tisfa
ctio
n m
ay in
crea
se
8 O
ppor
tuni
ty to
trul
y tre
at
whol
e pe
rson
8Al
l or a
lmos
t all
syst
emba
rrier
s re
solve
d a
llowi
ng
prov
ider
s to
pra
ctic
e as
hi
gh fu
nctio
ning
team
8Al
l pat
ient
nee
dsad
dres
sed
as th
ey o
ccur
8 S
hare
d kn
owle
dge
base
of
pro
vide
rs in
crea
ses
and
allo
ws e
ach
prof
essi
onal
to
resp
ond
mor
e br
oadl
yan
d ad
equa
tely
to a
ny
issu
e
Wea
knes
ses
8 S
ervi
ces
may
ove
rlap
be
dupl
icat
ed o
r eve
n wo
rk
agai
nst e
ach
othe
r
8 Im
porta
nt a
spec
ts o
f car
e m
ay n
ot b
e ad
dres
sed
or ta
ke a
long
tim
e to
be
diag
nose
d
8 S
harin
g of
info
rmat
ion
may
not
be
syst
emat
ic
enou
gh to
effe
ct o
vera
ll pa
tient
car
e
8 N
o gu
aran
tee
that
info
rshym
atio
n wi
ll ch
ange
pla
n or
st
rate
gy o
f eac
h pr
ovid
er
8 R
efer
rals
may
fail
due
to
barri
ers
lead
ing
to p
atie
nt
and
prov
ider
frus
tratio
n
8 P
roxim
ity m
ay n
ot le
ad to
gr
eate
r col
labo
ratio
nlim
iting
val
ue
8 E
ffort
is re
quire
d to
de
velo
p re
latio
nshi
ps
8 L
imite
d fle
xibili
ty if
tra
ditio
nal r
oles
are
mai
ntai
ned
8 S
yste
m is
sues
may
lim
it co
llabo
ratio
n
8 P
oten
tial f
or te
nsio
n an
d co
nflic
ting
agen
das
amon
g pr
ovid
ers
as p
ract
ice
boun
darie
s lo
osen
8 P
ract
ice
chan
ges
may
cr
eate
lack
of fi
t for
som
ees
tabl
ishe
d pr
ovid
ers
8Ti
me
is n
eede
d to
co
llabo
rate
at t
his
high
leve
l and
may
affe
ct
prac
tice
prod
uctiv
ity o
rca
denc
e of
car
e
8 S
usta
inab
ility
issu
es m
ay
stre
ss th
e pr
actic
e
8 F
ew m
odel
s at
this
leve
l wi
th e
noug
h ex
perie
nce
tosu
ppor
t val
ue
8Ou
tcom
e ex
pect
atio
ns n
otye
t est
ablis
hed
13

SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
No
coo
rdin
atio
n or
ts
em
ent o
f e
effo
r
vide
r buy
-in
en
ratio
n or
ev
up
to
vide
rs to
man
agco
llabo
rativ
Litt
le p
roto
inte
gco
llabo
ratio
nin
divi
dual
pro
initi
ate
as ti
me
and
prac
tice
limits
allo
w
8 8
Som
e pr
actic
e le
ader
shysh
ip in
mor
e sy
stem
atic
vide
r buy
-into
al
ue
ving
nee
ded
mat
ion
shar
ing
info
r
Som
e pr
oco
llabo
ratio
n an
d v
plac
ed o
n ha
mat
ion
info
r
8 8
Org
aniza
tion
lead
ers
tive
but o
ften
colo
shysu
ppor
catio
n is
vie
wed
as
a pr
ojec
t or p
rogr
am ork
and
vide
r buy
-in to
ra
ls w
Pro mak
ing
refe
rap
prec
iatio
n of
ons
ite
vaila
bilit
y a
8 8
thro
ugh
mut
ual p
robl
em-
Org
aniza
tion
lead
ers
ratio
n t i
nteg
supp
or
solv
ing
of s
ome
syst
em
riers
ba
r
Mor
e bu
y-in
to c
once
pt
vide
rs
ratio
n bu
t not
of
inte
gco
nsis
tent
acr
oss
not
all
pro
tuni
ties
for
vide
rs
pro
usin
g op
por
inte
grat
ion
or c
ompo
nent
s
8 8
ts
w
Org
aniza
tion
lead
ers if
ra
tion
ws a
nd e
ffor
t int
egsu
ppor
fund
ing
allo
plac
ed in
sol
ving
as
man
y sy
stem
issu
es a
s w
ithou
t cha
ngshy
poss
ible
in
g fu
ndam
enta
lly h
odi
scip
lines
are
pra
ctic
ed
rate
d y
not
vide
rs
e in
pra
ctic
e
ly a
ll pr
o N
ear ag
ed in
inte
g B
uy-in
ma
y fo
r ind
ivid
ual
eng
mod
el
incl
ude
chan
g
vide
rs
stra
teg
pro
8 8
y e
ervi
ded
aniza
tion
lead
ers
t ra
tion
as p
ract
ice
Org
stro
ngly
sup
por
inte
gm
odel
with
exp
ecte
dvi
ce d
eliv
e in
ser
chan
g
for d
evel
opm
ent
rate
d ca
re a
nd a
ll In
teg
com
pone
nts
embr
aced
vide
rs a
nd a
ctiv
and
reso
urce
s pr
o
by a
ll pr
ool
vem
ent i
n pr
actic
e e
vin ch
ang
8 8
Tab
le 2
b S
ix L
evel
s o
f Co
llab
ora
tion
Inte
grat
ion
(Key
Diff
eren
tiato
rs c
ont
inue
d)
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Key
Dif
fere
ntia
tor
Pra
ctic
eO
rgan
izat
ion
Key
Dif
fere
ntia
tor
bu
sin
ess
Mo
del
Se
para
te fu
ndin
g
No s
harin
g of
reso
urce
s
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re re
sour
ces
for
sing
le p
roje
cts
Sepa
rate
bill
ing
prac
tices
8 8 8
Sepa
rate
fund
ing
May
sha
re fa
cilit
y ex
pens
es
Sepa
rate
bill
ing
prac
tices
8 8 8
but
may
S
epar
ate
fund
ing
rant
s sta
ffing
cos
ts
shar
e g
y sh
are
offic
e
uctu
re
Ma
expe
nses
or
infra
str
Sepa
rate
bill
ing
due
to
riers
sy
stem
bar
8 8 8
Bl
ende
d fu
ndin
g ba
sed
uctu
re
on c
ontra
cts
gra
nts
or
ys to
str
agre
emen
ts
Varie
ty o
f wa
8
the
shar
ing
of a
ll ex
pens
es
Billi
ng fu
nctio
n co
mbi
ned
reed
upo
n pr
oces
s or
ag
8 8
8 8Re
sour
ces
shar
ed a
nd
hole
rate
d fu
ndin
g In
teg
base
d on
mul
tiple
sour
ces
of re
venu
e
allo
cate
d ac
ross
wpr
actic
e
Billi
ng m
axim
ized
for
rate
d m
odel
and
uc
ture
in
teg
sing
le b
illin
g st
r
8
12
SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 3
Ad
vant
ages
and
Wea
knes
ses
at E
ach
Leve
l of C
olla
bo
ratio
nIn
tegr
atio
n
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Ad
van
tag
es
8 E
ach
prac
tice
can
mak
e tim
ely
and
auto
nom
ous
deci
sion
s ab
out c
are
8Re
adily
und
erst
ood
asa
prac
tice
mod
el b
y pa
tient
s an
d pr
ovid
ers
8 M
aint
ains
eac
h pr
actic
ersquos
basi
c op
erat
ing
stru
ctur
eso
cha
nge
is n
ot a
di
srup
tive
fact
or
8 P
rovi
des
som
e co
ordi
natio
n an
din
form
atio
n-sh
arin
g th
at
is h
elpf
ul to
bot
h pa
tient
san
d pr
ovid
ers
8 C
oloc
atio
n al
lows
for
mor
e di
rect
inte
ract
ion
and
com
mun
icat
ion
amon
g pr
ofes
sion
als
toim
pact
pat
ient
car
e
8 R
efer
rals
mor
e su
cces
sful
du
e to
pro
ximity
8 O
ppor
tuni
ty to
dev
elop
cl
oser
pro
fess
iona
l rel
ashytio
nshi
ps
8 R
emov
al o
f som
e sy
stem
ba
rrier
s li
ke s
epar
ate
reco
rds
allo
ws c
lose
r co
llabo
ratio
n to
occ
ur
8 B
oth
beha
vior
al h
ealth
an
d m
edic
al p
rovi
ders
ca
n be
com
e m
ore
well-
info
rmed
abo
ut w
hat e
ach
can
prov
ide
8 P
atie
nts
are
view
ed a
s sh
ared
whi
ch fa
cilit
ates
m
ore
com
plet
e tre
atm
ent
plan
s
8 H
igh
leve
l of c
olla
bora
tion
lead
s to
mor
e re
spon
sive
pa
tient
car
e in
crea
sing
en
gage
men
t and
ad
here
nce
to tr
eatm
ent
plan
s
8 P
rovi
der fl
exib
ility
in
crea
ses
as s
yste
mis
sues
and
bar
riers
are
re
solve
d
8 B
oth
prov
ider
and
pat
ient
sa
tisfa
ctio
n m
ay in
crea
se
8 O
ppor
tuni
ty to
trul
y tre
at
whol
e pe
rson
8Al
l or a
lmos
t all
syst
emba
rrier
s re
solve
d a
llowi
ng
prov
ider
s to
pra
ctic
e as
hi
gh fu
nctio
ning
team
8Al
l pat
ient
nee
dsad
dres
sed
as th
ey o
ccur
8 S
hare
d kn
owle
dge
base
of
pro
vide
rs in
crea
ses
and
allo
ws e
ach
prof
essi
onal
to
resp
ond
mor
e br
oadl
yan
d ad
equa
tely
to a
ny
issu
e
Wea
knes
ses
8 S
ervi
ces
may
ove
rlap
be
dupl
icat
ed o
r eve
n wo
rk
agai
nst e
ach
othe
r
8 Im
porta
nt a
spec
ts o
f car
e m
ay n
ot b
e ad
dres
sed
or ta
ke a
long
tim
e to
be
diag
nose
d
8 S
harin
g of
info
rmat
ion
may
not
be
syst
emat
ic
enou
gh to
effe
ct o
vera
ll pa
tient
car
e
8 N
o gu
aran
tee
that
info
rshym
atio
n wi
ll ch
ange
pla
n or
st
rate
gy o
f eac
h pr
ovid
er
8 R
efer
rals
may
fail
due
to
barri
ers
lead
ing
to p
atie
nt
and
prov
ider
frus
tratio
n
8 P
roxim
ity m
ay n
ot le
ad to
gr
eate
r col
labo
ratio
nlim
iting
val
ue
8 E
ffort
is re
quire
d to
de
velo
p re
latio
nshi
ps
8 L
imite
d fle
xibili
ty if
tra
ditio
nal r
oles
are
mai
ntai
ned
8 S
yste
m is
sues
may
lim
it co
llabo
ratio
n
8 P
oten
tial f
or te
nsio
n an
d co
nflic
ting
agen
das
amon
g pr
ovid
ers
as p
ract
ice
boun
darie
s lo
osen
8 P
ract
ice
chan
ges
may
cr
eate
lack
of fi
t for
som
ees
tabl
ishe
d pr
ovid
ers
8Ti
me
is n
eede
d to
co
llabo
rate
at t
his
high
leve
l and
may
affe
ct
prac
tice
prod
uctiv
ity o
rca
denc
e of
car
e
8 S
usta
inab
ility
issu
es m
ay
stre
ss th
e pr
actic
e
8 F
ew m
odel
s at
this
leve
l wi
th e
noug
h ex
perie
nce
tosu
ppor
t val
ue
8Ou
tcom
e ex
pect
atio
ns n
otye
t est
ablis
hed
13

SAMHSA-HRSA CENTER FOR INTEGRATED HEALTH SOLUTIONS
SA
MH
SA
-HR
SA
Ce
nt
eR
fo
R I
nt
eg
RA
te
d H
eA
ltH
So
lu
tIo
nS
-
Tab
le 3
Ad
vant
ages
and
Wea
knes
ses
at E
ach
Leve
l of C
olla
bo
ratio
nIn
tegr
atio
n
CO
OR
DIN
AT
ED
C
O L
OC
AT
ED
IN
TE
GR
AT
ED
LEv
EL
1M
inim
al C
olla
bo
ratio
n
LEv
EL
2b
asic
Co
llab
ora
tion
at a
Dis
tan
ce
LEv
EL
3b
asic
Co
llab
ora
tion
On
site
LEv
EL
4C
lose
Co
llab
ora
tion
On
site
wit
h S
om
e S
yste
m In
teg
ratio
n
LEv
EL
5C
lose
Co
llab
ora
tion
Ap
pro
achi
ng
an In
teg
rate
d P
ract
ice
LEv
EL
6Fu
ll C
olla
bo
ratio
n in
a Tr
ansf
orm
ed M
erg
ed
Inte
gra
ted
Pra
ctic
e
Ad
van
tag
es
8 E
ach
prac
tice
can
mak
e tim
ely
and
auto
nom
ous
deci
sion
s ab
out c
are
8Re
adily
und
erst
ood
asa
prac
tice
mod
el b
y pa
tient
s an
d pr
ovid
ers
8 M
aint
ains
eac
h pr
actic
ersquos
basi
c op
erat
ing
stru
ctur
eso
cha
nge
is n
ot a
di
srup
tive
fact
or
8 P
rovi
des
som
e co
ordi
natio
n an
din
form
atio
n-sh
arin
g th
at
is h
elpf
ul to
bot
h pa
tient
san
d pr
ovid
ers
8 C
oloc
atio
n al
lows
for
mor
e di
rect
inte
ract
ion
and
com
mun
icat
ion
amon
g pr
ofes
sion
als
toim
pact
pat
ient
car
e
8 R
efer
rals
mor
e su
cces
sful
du
e to
pro
ximity
8 O
ppor
tuni
ty to
dev
elop
cl
oser
pro
fess
iona
l rel
ashytio
nshi
ps
8 R
emov
al o
f som
e sy
stem
ba
rrier
s li
ke s
epar
ate
reco
rds
allo
ws c
lose
r co
llabo
ratio
n to
occ
ur
8 B
oth
beha
vior
al h
ealth
an
d m
edic
al p
rovi
ders
ca
n be
com
e m
ore
well-
info
rmed
abo
ut w
hat e
ach
can
prov
ide
8 P
atie
nts
are
view
ed a
s sh
ared
whi
ch fa
cilit
ates
m
ore
com
plet
e tre
atm
ent
plan
s
8 H
igh
leve
l of c
olla
bora
tion
lead
s to
mor
e re
spon
sive
pa
tient
car
e in
crea
sing
en
gage
men
t and
ad
here
nce
to tr
eatm
ent
plan
s
8 P
rovi
der fl
exib
ility
in
crea
ses
as s
yste
mis
sues
and
bar
riers
are
re
solve
d
8 B
oth
prov
ider
and
pat
ient
sa
tisfa
ctio
n m
ay in
crea
se
8 O
ppor
tuni
ty to
trul
y tre
at
whol
e pe
rson
8Al
l or a
lmos
t all
syst
emba
rrier
s re
solve
d a
llowi
ng
prov
ider
s to
pra
ctic
e as
hi
gh fu
nctio
ning
team
8Al
l pat
ient
nee
dsad
dres
sed
as th
ey o
ccur
8 S
hare
d kn
owle
dge
base
of
pro
vide
rs in
crea
ses
and
allo
ws e
ach
prof
essi
onal
to
resp
ond
mor
e br
oadl
yan
d ad
equa
tely
to a
ny
issu
e
Wea
knes
ses
8 S
ervi
ces
may
ove
rlap
be
dupl
icat
ed o
r eve
n wo
rk
agai
nst e
ach
othe
r
8 Im
porta
nt a
spec
ts o
f car
e m
ay n
ot b
e ad
dres
sed
or ta
ke a
long
tim
e to
be
diag
nose
d
8 S
harin
g of
info
rmat
ion
may
not
be
syst
emat
ic
enou
gh to
effe
ct o
vera
ll pa
tient
car
e
8 N
o gu
aran
tee
that
info
rshym
atio
n wi
ll ch
ange
pla
n or
st
rate
gy o
f eac
h pr
ovid
er
8 R
efer
rals
may
fail
due
to
barri
ers
lead
ing
to p
atie
nt
and
prov
ider
frus
tratio
n
8 P
roxim
ity m
ay n
ot le
ad to
gr
eate
r col
labo
ratio
nlim
iting
val
ue
8 E
ffort
is re
quire
d to
de
velo
p re
latio
nshi
ps
8 L
imite
d fle
xibili
ty if
tra
ditio
nal r
oles
are
mai
ntai
ned
8 S
yste
m is
sues
may
lim
it co
llabo
ratio
n
8 P
oten
tial f
or te
nsio
n an
d co
nflic
ting
agen
das
amon
g pr
ovid
ers
as p
ract
ice
boun
darie
s lo
osen
8 P
ract
ice
chan
ges
may
cr
eate
lack
of fi
t for
som
ees
tabl
ishe
d pr
ovid
ers
8Ti
me
is n
eede
d to
co
llabo
rate
at t
his
high
leve
l and
may
affe
ct
prac
tice
prod
uctiv
ity o
rca
denc
e of
car
e
8 S
usta
inab
ility
issu
es m
ay
stre
ss th
e pr
actic
e
8 F
ew m
odel
s at
this
leve
l wi
th e
noug
h ex
perie
nce
tosu
ppor
t val
ue
8Ou
tcom
e ex
pect
atio
ns n
otye
t est
ablis
hed
13