circulatory adjuncts - resqpod 27 babbs - cardiol... · circulatory adjuncts ... actly the same...
TRANSCRIPT

EMERGENCY CARDIOVASCULAR CARE 0733–8651/02 $15.00 � .00
CIRCULATORY ADJUNCTS
Newer Methods ofCardiopulmonary Resuscitation
Charles F. Babbs, MD, PhD
Conventional cardiopulmonary resuscita-tion—what has come to be called standardCPR—has changed little since first introducedin the early 1960s by Kouwenhoven et al.1
Standard CPR requires chest compressions ata rate of 80 to 100 compressions/min in con-junction with mouth-to-mouth rescue breath-ing.2 Positive pressure ventilations (PPVs) aregiven at an overall rate in the range of about8 to 12 ventilations/min, depending onwhether one is doing one- or two-rescuerCPR. Refinements of standard CPR since itsintroduction in the 1960s have included in-creasing the rate of chest compression from60 compressions/min to 80 compressions/min or more, which research shows matterslittle,3 and recently decreasing the tidal vol-ume of the PPVs under certain circum-stances.2, 4 Elimination of the carotid arterypulse check in the year 2000 guidelines hasabolished unnecessary delay in starting chestcompressions by lay rescuers. Otherwise, ex-ternal CPR today is performed in approxi-
The author has no financial interest, consulting ar-rangement, or research contract with Ambu, CPRxLLC,or any other resuscitation device company that could beconstrued as a conflict of interest.
From the Department of Basic Medical Sciences, Purdue University, West Lafayette, Indiana
CARDIOLOGY CLINICS
VOLUME 20 • NUMBER 1 • FEBRUARY 2002 37
mately the same way as it was in the 1960s.In keeping with the engineering maxim that‘‘if you keep on doing what you’re doing,you’ll keep on getting what you’ve got,’’ suc-cess rates for standard CPR have changedlittle over the past 40 years.5–9 Between 15%and 40% of all victims of nontraumatic car-diac arrest are resuscitated, and approxi-mately 5% to 10% live to leave the hospital.
Despite lack of significant change on thesurface, a neglected community of researchershas made substantial progress in the labora-tory and in the clinic during this same 40-year period. Results have lead to much fun-damental understanding of the circulatoryphysiology and hemodynamics of cardiac ar-rest and resuscitation. A variety of alternativeforms of CPR have been proposed and testedin animals and in humans. All of these alter-native methods apply more kinetic energy tothe victim, either by way of an additionalrescuer or some type of mechanical device.More energetic forms of CPR include high-impulse CPR, interposed abdominal compres-sion–CPR (IAC-CPR), active compression-de-compression CPR (ACD-CPR), and vest CPR.These derivatives of standard CPR have cometo be known as circulatory adjuncts. By the

38 BABBS
year 2000, a convergence had occurred be-tween laboratory knowledge about mecha-nisms of blood flow and clinical experiencewith the various adjuncts. This long-delayedsynthesis of research findings has led to im-proved forms of practical resuscitation (ableto generate more blood flow and systemicperfusion pressure during cardiac arrestthrough the efforts of the rescuers) based onsound basic science principles. If there is onecertain truth in resuscitation science, stem-ming from the pioneering work of Redding10,Ralston et al,11 Weil and Tang,9 and Kern etal,12 it is this: Improved coronary and sys-temic perfusion pressures during cardiac ar-rest and CPR lead to improved immediateresuscitation success and improved likelihoodof longer-term, neurologically intact survival.
The improved hemodynamics, however, donot come without a price, because more phys-ical work has to be done by human or ma-chine to generate more forward flow of blood.Accordingly, adjuncts may not be appropriatefor the lone rescuer faced with a collapsedcoworker or loved one. Nevertheless, the timehas come for serious consideration of alterna-tive forms of resuscitation when adequateequipment and trained personnel are avail-able, for example, in the emergency depart-ment of a hospital. This article focuses on therelevant physiology of cardiac arrest and CPRthat makes possible the generation of sys-temic perfusion pressure substantially greaterthan that provided by standard CPR. Thereaf-ter, selected practical aspects of applying cur-rently approved circulatory adjuncts in a hos-pital setting are discussed.
MODERN PHYSIOLOGY OF BLOODFLOW DURING CARDIOPULMONARYRESUSCITATION
At least three different mechanisms can moveblood during cardiac arrest and CPR: (1) thecardiac pump, (2) the thoracic pump, and (3)the abdominal pump. The cardiac pumpmechanism was the first to be recognized bythe original discoverers of closed-chest CPR.1
This pump mechanism is operative to theextent that external chest compressionsqueezes the cardiac ventricles between the
sternum and the spine. As a result, forwardblood flow occurs through the aortic and pul-monic valves without mitral or tricuspid in-competence. In particular, when the cardiacpump mechanism is operative, the aorticvalve is open, and the mitral valve is closedduring chest compression.13 The cardiacpump mechanism is also operative duringopen-chest cardiac massage.
The thoracic pump mechanism was discov-ered in the 1980s as a result of clinical obser-vation by Criley et al14, 15 of cough CPR andextensive laboratory studies at Johns HopkinsUniversity, led by Rudikoff et al16 and Weis-feldt.17 This pump is operative to the extentthat chest compression causes a global rise inintrathoracic pressure sufficient to force bloodfrom the pulmonary vasculature, through theheart, and into the periphery. When the tho-racic pump mechanism is operative, the mi-tral and the aortic valves are open simultane-ously during chest compression.18–20 The heartacts as a conduit rather than a pumpingchamber.
The abdominal pump mechanism was dis-covered independently by workers in GreatBritain, Japan, Israel, and the United States inthe latter half of the 20th century.21–26 Thismechanism has two components: (1) arterialand (2) venous. The arterial component of theabdominal pump mechanism is operative tothe extent that abdominal compression forcesblood from the abdominal aorta into the pe-riphery against a closed aortic valve. Thus,the aortic valve is closed during abdominalcompression. The venous component of theabdominal pump mechanism is operative tothe extent that external abdominal pressureforces blood from the inferior vena cavathrough the tricuspid valve into the right ven-tricle (or through the tricuspid and pulmonicvalves into the pulmonary vasculature). Inthis case, the right heart valves are open dur-ing abdominal compression.
The operation of these three pumps—cardiac, thoracic, and abdominal—is relatedto the fundamental architecture of the cardio-vascular system. The physiology of thepumps has been demonstrated in relativelysimple mathematical models that representthe essential features of the human cardiovas-cular system.24, 27–31 Successful circulatory ad-

CIRCULATORY ADJUNCTS 39
juncts generate greater blood flow than stan-dard CPR either by enhancing the operationof one of these pumps or by simultaneouslyinvoking the action of multiple pumps. High-impulse CPR,32–34 for example, aims to en-hance the action of the cardiac pump mecha-nism. Vest CPR35, 36 aims to enhance the actionof the thoracic pump mechanism through theaction of a pneumatic vest that is inflated anddeflated rapidly at a rate of 60 to 150 times/min. ACD-CPR37, 38 aims to improve filling ofthe either the cardiac pump or the thoracicpump by creating negative pressure in thethorax between chest compressions. IAC-CPR39–43 aims to invoke the abdominal pumptogether with either chest pump. IAC-CPRand its derivative, Lifestick (Datascope, Fair-field, NJ) CPR,44 aim to combine thoracic andabdominal pumps alternately, in such a waythat the thoracic pump primes the abdominalpump during one half of the cycle and theabdominal pump primes the thoracic pumpduring the other half of the cycle.
Regarding the question of the effectivenessof these various adjuncts, it would be difficultto compare and contrast all such methods ina single animal or clinical model; however, itis reasonable to use a mathematical model ofthe circulation that includes all three pumps.31
Such a model can be used to simulate theeffects of various circulatory adjuncts in ex-actly the same circulatory system, withoutmodel-to-model variation. It also serves todemonstrate the relevant cardiovascularphysiology of CPR.
An interesting feature of the circulatorymodel used in this article is the small numberof assumptions required to obtain realistic re-sults.31 These are limited to the existence ofcompliant vessels and resistive vascular beds,the definition of compliance (�V/�P), normalanatomy (the arrangement of connected ves-sels and cardiac chambers), and a linear rela-tion between flow and pressure (Ohm’s Law:flow � pressure/resistance).28–31 Althoughmuch more complex models of the circulationcan be created, only these basic assumptionsare needed to demonstrate the three mecha-nisms of blood flow during CPR and the rela-tive utility of various circulatory adjuncts.Circulatory systems that have these proper-ties behave similarly, including those of large
and small people and large and small experi-mental animals. The author of this article usesthe simplest realistic model of CPR physiol-ogy to illustrate the actions of the basic pumpmechanisms and to demonstrate selected cir-culatory adjuncts. The exact values of vascu-lar compliances and resistances and othertechnical details of the model, which can beimplemented in a spreadsheet, are fully de-scribed elsewhere.31
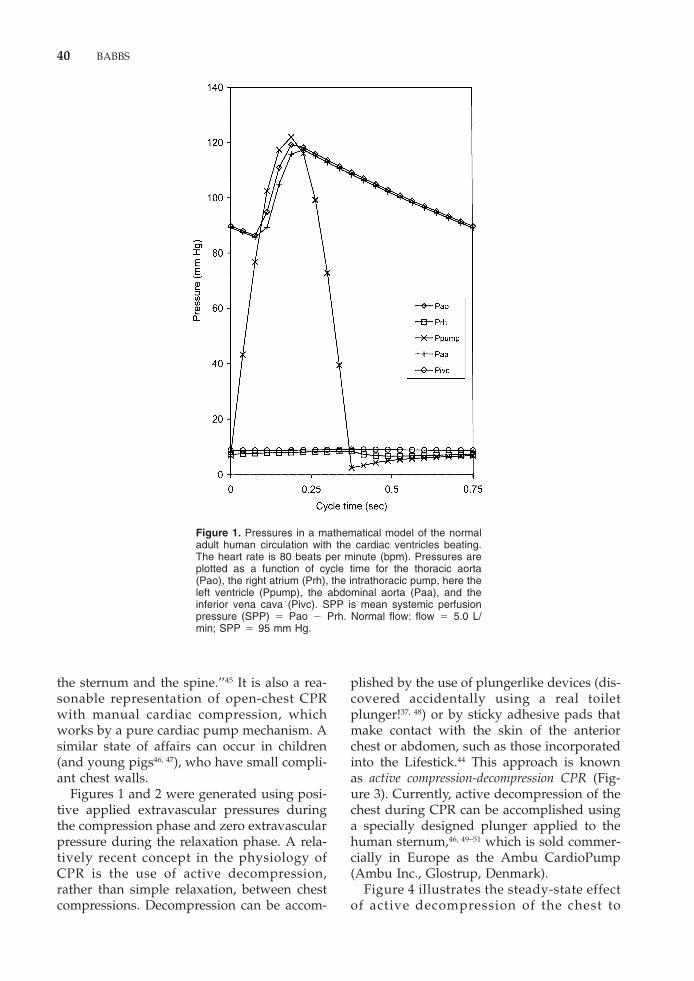
As a point of reference and calibration, Fig-ure 1 illustrates pressures throughout a sim-plified cardiovascular system for a nonar-rested circulation of a hypothetical 70-kgman. In this instance, cardiac pump generatesleft ventricular pressures (Ppump) of 122/2mm Hg at a heart rate of 80 beats/min (bpm).Systemic arterial blood pressure is 119/82 (thedata point representing the exact minimumdiastolic pressure at 82 mm Hg is not plottedon the chart), mean arterial pressure is 95 mmHg, and cardiac output is 5.0 L/min. Theseare classical textbook values for the normalhuman circulatory system.31 Note the essen-tially normal arterial pulse waveforms andlow systemic venous pressures.
Figure 2 illustrates the action of a purecardiac pump CPR in the same circulatorymodel during cardiac arrest. Steady-state con-ditions are shown after stable pressures havebeen achieved by 20 prior compressions. Inthis simulation, only the right and left ventri-cles of the heart are compressed at a rate of80 compressions/min with a half sinusoidalwaveform having a peak pressure of 60 mmHg, a typical value reported in the literatureof standard CPR29. There is no intrinsic myo-cardial contractility in this system, and thereis no pump priming effect of atrial contrac-tion (which in some circumstances could existfor a few minutes in witnessed cardiac ar-rests). The cardiac pump produces reasonableaortic pressures and very small venous pulsa-tions. Especially important to note are the lowright-sided central venous pressures through-out the compression cycle. There is substan-tial coronary perfusion pressure (aortic toright atrial gradient) throughout the cycle.Forward flow is 2.5 L/min, and systemic per-fusion pressure is 47 mm Hg. This state ofaffairs represents idealized classical externalCPR in which ‘‘the heart is squeezed between
40 BABBS
Figure 1. Pressures in a mathematical model of the normaladult human circulation with the cardiac ventricles beating.The heart rate is 80 beats per minute (bpm). Pressures areplotted as a function of cycle time for the thoracic aorta(Pao), the right atrium (Prh), the intrathoracic pump, here theleft ventricle (Ppump), the abdominal aorta (Paa), and theinferior vena cava (Pivc). SPP is mean systemic perfusionpressure (SPP) � Pao � Prh. Normal flow: flow � 5.0 L/min; SPP � 95 mm Hg.
the sternum and the spine.’’45 It is also a rea-sonable representation of open-chest CPRwith manual cardiac compression, whichworks by a pure cardiac pump mechanism. Asimilar state of affairs can occur in children(and young pigs46, 47), who have small compli-ant chest walls.
Figures 1 and 2 were generated using posi-tive applied extravascular pressures duringthe compression phase and zero extravascularpressure during the relaxation phase. A rela-tively recent concept in the physiology ofCPR is the use of active decompression,rather than simple relaxation, between chestcompressions. Decompression can be accom-
plished by the use of plungerlike devices (dis-covered accidentally using a real toiletplunger!37, 48) or by sticky adhesive pads thatmake contact with the skin of the anteriorchest or abdomen, such as those incorporatedinto the Lifestick.44 This approach is knownas active compression-decompression CPR (Fig-ure 3). Currently, active decompression of thechest during CPR can be accomplished usinga specially designed plunger applied to thehuman sternum,46, 49–51 which is sold commer-cially in Europe as the Ambu CardioPump(Ambu Inc., Glostrup, Denmark).
Figure 4 illustrates the steady-state effectof active decompression of the chest to

CIRCULATORY ADJUNCTS 41
Figure 2. Pressures in a mathematical model of the normaladult human circulation during cardiac arrest and Cardiopul-monary resuscitation (CPR) with a pure cardiac mechanism.The compression rate is 80 per minute. Cardiac compressionCPR: flow � 2.5 L/min; SPP � 47 mm Hg.
�20 mm Hg, the maximum reported in theliterature.50, 52, 53 This particular simulation isfor cardiac pump CPR. Combining positiveand negative chest pressures has a salubriouseffect upon hemodynamics. Cardiac filling isenhanced during the negative pressure phase,so that greater stroke output can be achievedon the next positive pressure phase. Note in
Figure 3. Active compression-decompression CPR (ACD-CPR) using a plungerlike de-vice.
Figure 4 the particular times near 0.55 sec-onds in the cycle when pump pressure issubstantially less than right heart pressure.At this stage, enhanced pump filling occurs.The result of enhanced pump filling is greaterforward flow and greater perfusion pressures:3.2 versus 2.5 L/min and 61 versus 47 mmHg. When more energy is applied to the ar-

42 BABBS
Figure 4. Pressures in a mathematical model of the normaladult human circulation during cardiac arrest and ACD-CPRwith a pure cardiac pump mechanism. The compression rateis 80 per minute. Maximal chest compassion pressure is�60 mm Hg. Maximal decompression pressure is �20 mmHg. Cardiac compression-decompression CPR: flow � 3.2L/min; SPP � 61 mm Hg.
rested circulation in this manner, forwardflow improves. A potential advantage of theuse of negative and positive pressure phases,rather than simply greater positive pressure,is that it is less traumatic to the victim. Also,needless compression of pumping chambersthat are already empty is avoided. The use ofa decompression phase compliments the useof a compression phase for all three pumpmechanisms in CPR (see later discussion).
When it works, the cardiac pump mecha-nism is the most effective and natural of thethree pumps in CPR. Its operation in externalCPR, however, depends on good mechanicalcoupling between the sternum and the heart.In most adults, the coupling of chest compres-sion to the heart is indirect, and a thoracicpump mechanism tends to predominate.20, 35, 54
Thoracic pump CPR has a quite different setof pressure profiles. Figure 5 illustrates theaction of a pure thoracic pump. In this simu-lation, all intrathoracic blood–containingchambers are pressurized equally at a rate of80 per minute with a peak pressure of 60 mmHg, as before. This state of affairs happens in
broad-chested adults. It also happens duringvest CPR, in which a pneumatic vest encirclesthe chest to produce pulses of compressionfrom all sides simultaneously.
In thoracic pump CPR, forward flow occurseven though the heart is not being squeezedbetween the sternum and the spine. Coronaryblood flow and systemic blood flow occurwhen aortic pressure is greater than systemicvenous or right heart pressure. As shown inFigure 5, positive coronary and systemic per-fusion pressures occur mostly between com-pressions, rather than during compressions.Because of the tendency toward equalizationof aortic and venous pressures during com-pressions, forward flow with the thoracicpump mechanism tends to be less, other fac-tors being equal, than with the cardiac pumpmechanism. In a thoracic pump model of Fig-ure 5, forward flow is 0.94 L/min, and sys-temic perfusion pressure is 18 mm Hg.
If a decompression phase is added (Fig. 6),perfusion pressures are somewhat increased,but to a lesser extent than with cardiac pumpCPR. In this instance, forward flow is 1.14 L/

CIRCULATORY ADJUNCTS 43
min and systemic perfusion pressure is 22mm Hg. The difference in the responsivenessof the thoracic and cardiac pumps to negativepressure priming may be responsible forsome of the discrepancies in the reported lit-erature regarding the benefits of ACD-CPR invarious models.31 The simulated improve-ment in coronary perfusion pressures withACD-CPR (61 mm Hg for a cardiac pumpmodel and 22 mm Hg for a thoracic pumpmodel) are in keeping with the range of mea-sured coronary perfusion pressures in humanpatients during ACD-CPR. In one recentstudy,51 the generation of �20 mm Hg intra-thoracic pressure during ACD was ensuredwith the use of an inspiratory impedancevalve. These investigators found coronaryperfusion pressures of 40 to 45 mm Hg. Theseresults are consistent with those of Figures 4and 6, if one takes the modern consensusview20, 35, 54 that the operative pump mecha-nism in different animal and clinical models
Figure 5. Pressures in a mathematical model of the normaladult human circulation during cardiac arrest and CPR witha pure thoracic pump mechanism. The compression rate is80 per minute. Maximal chest compression pressure is �60mm Hg. Thoracic compression CPR: Flow � 0.93 L/min;SPP � 18 mm Hg.
is a combination of the cardiac and thoracicpumps.
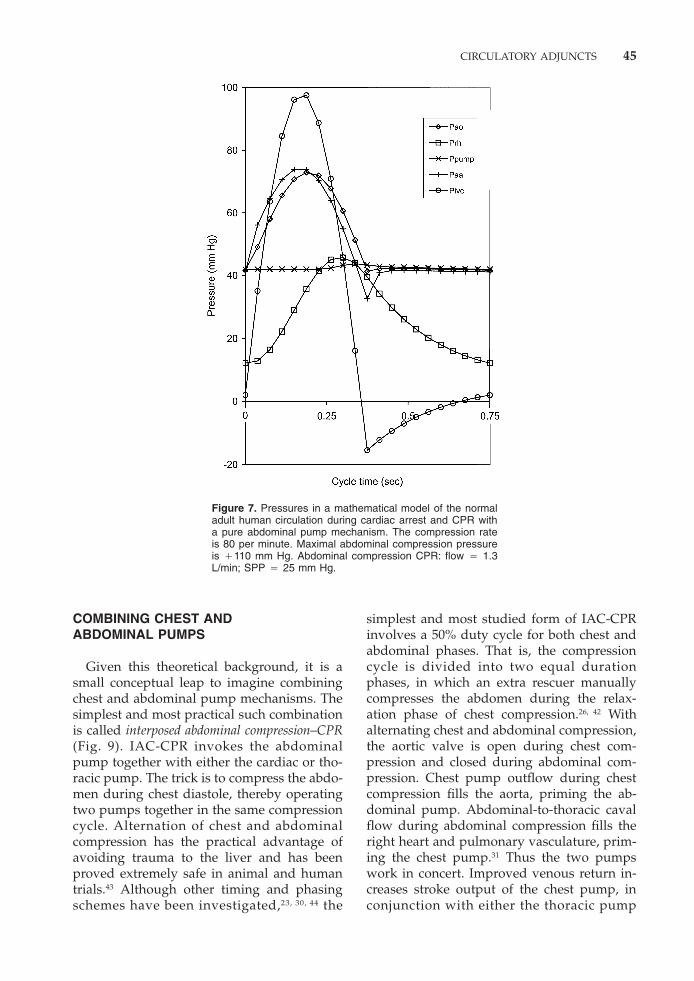
Figure 7 illustrates the steady-state actionof a pure abdominal pump. In this simula-tion, there is no chest compression. Abdomi-nal compression begins at time zero. Only theabdominal aorta and vena cava are com-pressed at a rate of 80 compressions/minwith a pressure of 110 mm Hg, values re-ported in the literature of IAC-CPR.39, 55, 56
Manual compression leading to periaorticpressures this high can be tolerated withoutpain by a conscious person.57 Artificial circu-lation can indeed be created by abdominalcompression only, as first observed experi-mentally by Rosborough et al.58 During ab-dominal compression, blood is squeezed fromthe aorta to the periphery by the positiveintra-aortic pressure acting against a closedaortic valve. During abdominal relaxation,the aortic valve opens, allowing filling of theaortic pumping chamber from the left heart

44 BABBS
Figure 6. Pressures in a mathematical model of the normaladult human circulation during cardiac arrest and ACD-CPRwith a pure thoracic pump mechanism. The compression rateis 80 per minute. Maximal chest compression pressure is�60 mm Hg. Maximal chest decompression pressure is �20mm Hg. Thoracic compression-decompression CPR: flow �1.1 L/min; SPP � 22 mm Hg.
and lungs. Only one valve is needed toachieve forward flow, as can be demonstratedby deliberately rendering the other threeheart valves incompetent.29 It is important tonote that the abdominal aortic pressure wave-form at 0 to 0.2 seconds in the cycle leads thethoracic aortic pressure waveform in time,indicating retrograde flow in the aorta. Pumppressures change very little, because the chestpump is acting as a passive conduit. There isa positive coronary perfusion pressure duringmost of the compression cycle. Forward flowis 1.3 L/min and coronary perfusion pressureis 25 mm Hg.
Figure 8 shows the potential benefit of add-ing active abdominal decompression (�20mm Hg pulses) to abdominal compression.Such a manipulation is possible using a stickyadhesive abdominal pad, and has been imple-mented practically in the experimental Lifes-tick device. In this simulation, there is still nochest compression. The abdominal pump is
filling when chest pump pressure is greaterthan thoracic aortic pressure near 0.4 secondsin the cycle. At this time, the low resistanceaortic valve is open. With active abdominaldecompression, the filling pressure differ-ences are more obvious than when abdominaldecompression is absent. During subsequentabdominal compression positive pressure inthe aorta, which is greater than that in thechest pump, closes the aortic valve. Theslower rise of right heart pressures comparedwith inferior vena cava pressures is associ-ated with differences in the capacitances ofthese structures. Near 0.3 seconds of the cycle,the chest pump, including the heart andlungs, fills when right heart pressure exceedschest pump pressure. Thus forward flow oc-curs around the entire circuit with abdominalcompression–decompression alone. As in thecase of the cardiac and thoracic pumps, theaddition of active decompression enhancesabdominal pump performance (see Fig. 8).
CIRCULATORY ADJUNCTS 45
Figure 7. Pressures in a mathematical model of the normaladult human circulation during cardiac arrest and CPR witha pure abdominal pump mechanism. The compression rateis 80 per minute. Maximal abdominal compression pressureis �110 mm Hg. Abdominal compression CPR: flow � 1.3L/min; SPP � 25 mm Hg.
COMBINING CHEST ANDABDOMINAL PUMPS
Given this theoretical background, it is asmall conceptual leap to imagine combiningchest and abdominal pump mechanisms. Thesimplest and most practical such combinationis called interposed abdominal compression–CPR(Fig. 9). IAC-CPR invokes the abdominalpump together with either the cardiac or tho-racic pump. The trick is to compress the abdo-men during chest diastole, thereby operatingtwo pumps together in the same compressioncycle. Alternation of chest and abdominalcompression has the practical advantage ofavoiding trauma to the liver and has beenproved extremely safe in animal and humantrials.43 Although other timing and phasingschemes have been investigated,23, 30, 44 the
simplest and most studied form of IAC-CPRinvolves a 50% duty cycle for both chest andabdominal phases. That is, the compressioncycle is divided into two equal durationphases, in which an extra rescuer manuallycompresses the abdomen during the relax-ation phase of chest compression.26, 42 Withalternating chest and abdominal compression,the aortic valve is open during chest com-pression and closed during abdominal com-pression. Chest pump outflow during chestcompression fills the aorta, priming the ab-dominal pump. Abdominal-to-thoracic cavalflow during abdominal compression fills theright heart and pulmonary vasculature, prim-ing the chest pump.31 Thus the two pumpswork in concert. Improved venous return in-creases stroke output of the chest pump, inconjunction with either the thoracic pump

46 BABBS
Figure 8. Pressures in a mathematical model of the normaladult human circulation during cardiac arrest and ACD-CPRwith a pure abdominal pump mechanism. The compressionrate is 80 per minute. Maximal abdominal compression pres-sure is �110 mm Hg. Maximal abdominal decompression is�30 mm Hg. Abdominal compression-decompression CPR:flow � 1.6 L/min; SPP � 30 mm Hg.
mechanism or direct cardiac compression.Abdominal compression also produces count-erpressure on the abdominal aorta, inducingretrograde flow toward the heart and brainbetween chest compressions.59 This abdomi-nal pump action on the arterial side increasesflow in a manner analogous to an intra-aorticballoon pump.29, 43
The effectiveness of such combined chestand abdominal compression was discoveredempirically22, 26 long before the theoreticalphysiology had been worked out.27–31 Indeedthe positive hemodynamic effects of IAC dur-
ing CPR have been confirmed in 20 of 21animal studies using canine and porcinemodels.43, 60 After encouraging laboratorystudies, clinical trials of IAC-CPR were per-formed. Three randomized clinical trials ofIAC-CPR for in-hospital cardiac arrest haveshown statistically significant improvementof outcome measures.42, 61–62 One randomizedtrial of prehospital IAC-CPR, combined,when possible, with standard CPR in thefield, showed no difference in outcome.63
These studies are summarized in Table 1.Pooled analysis of all available data for pre-

CIRCULATORY ADJUNCTS 47
Figure 9. Interposed abdominal compression (IAC) CPR (IAC-CPR).
hospital and in-hospital resuscitations showsstatistically significant improvement in the re-turn of spontaneous circulation with IAC-CPR. When only in-hospital studies are exam-ined, the effect of IAC becomes much greaterand is highly statistically significant. Pooleddata from two studies that examined long-term, neurologically intact survival followingin-hospital resuscitations show a positive ben-efit of IAC-CPR compared with standardCPR. Thus strong preclinical and clinical evi-dence supports the use of IAC-CPR for in-hospital resuscitations.
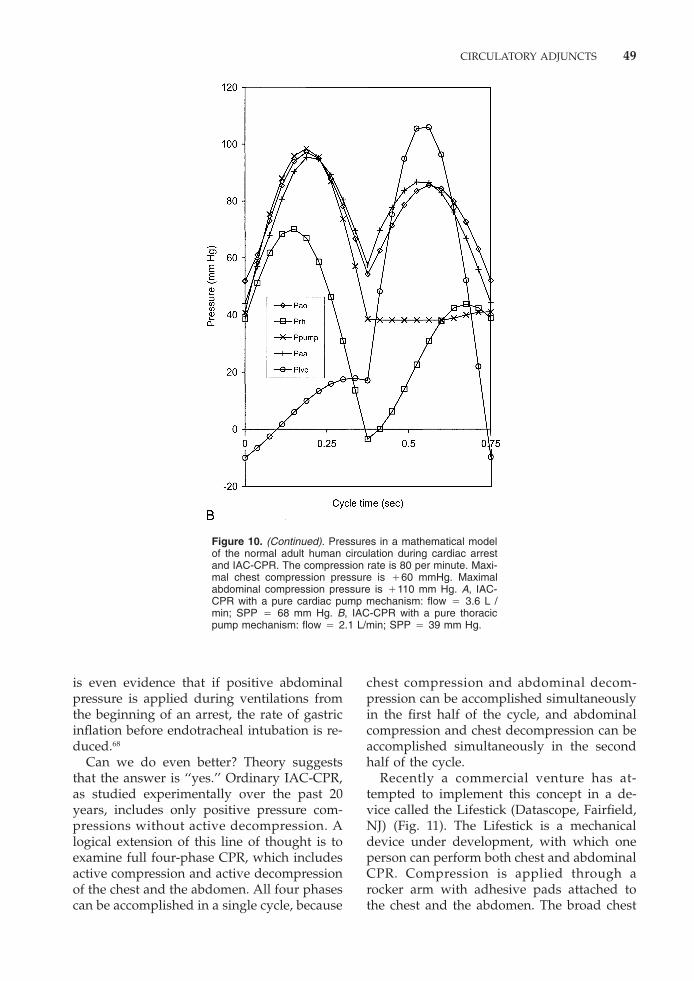
For the purpose of the present discussion,the hemodynamic benefits of IAC-CPR canbe demonstrated in the same mathematicalmodel with which basic physiology is investi-gated. Figure 10A illustrates the addition of110 mm Hg IACs to 60 mm Hg peak thoraciccompressions in a cardiac pump model. In
Table 1. RESULTS OF CLINICAL STUDIES OF INTERPOSED ABDOMINAL COMPRESSION–CARDIOPULMONARYRESUSCITATION VERSUS STANDARD CARDIOPULMONARY RESUSCITATION
IAC-CPR Standard POutcome Measure Studies (%) CPR (%) Value
Return of spontaneous circulation in- or out-of-hospital Mateer63 40/145 (28) 45/146 (31) .54Ward61 6/16 (38) 3/17 (18) .19Sack42 29/48 (60) 14/55 (25) .00014Sack62 33/67 (49) 21/76 (28) .0067All 4 studies 108/276 (39) 83/294 (28) .0056
Return of spontaneous circulation after in-hospital Ward61 6/16 (38) 3/17 (18) .19resuscitation Sack42 29/48 (60) 14/55 (25) .00014
Sack62 33/67 (49) 21/76 (28) .0067All 3 studies 68/131 (52) 38/148 (26) .000003
Survival to discharge, neurologically intact after in- Ward61 1/16 (6) 0/17 (0) .3017hospital resuscitation Sack42 8/48 (17) 3/55 (5) .0700
Both studies 9/64 (14) 3/72 (4) .0453
this instance, the cardiac and abdominalpump mechanisms are combined. (Eventhough more external force is applied to thechest than to the abdomen in practice, typicalintrathoracic pressure pulses are less than in-tra-abdominal pressure pulses because of thestiffness of the chest wall.) The double arterialpressure peaks in Figure 10A attest to theeffects of the double pump approach. Sys-temic perfusion pressure is sustainedthroughout both phases of the compressioncycle. Enhanced filling of the chest pump isevident at cycle times near 0.7 seconds. Fillingof the abdominal pump chamber (ie, theaorta) can be seen at cycle times near 0.125seconds. The increased forward flow in thismodel 3.6 L/min with IAC versus 2.5 L/minfor cardiac pump CPR. Systemic perfusionpressure is 68 mm Hg versus 47 mm Hg forcardiac pump CPR. Thus the ratio of perfu-

48 BABBS
Figure 10. See legend on opposite page
sion during IAC-CPR to perfusion duringstandard CPR is 1.44 in a pure cardiac pumpmodel.
Figure 10B illustrates the addition of 110mm Hg IACs to 60 mm Hg peak thoraciccompressions in a pure thoracic pump model,illustrating similar effects of the double pumpapproach when the thoracic and abdominalpump mechanisms are combined. The in-creased forward flow in this model is 2.1 L/min with IAC versus 0.93 L/min for thoracicpump CPR. Systemic perfusion pressure is 39mm Hg versus 18 mm Hg for thoracic pumpCPR. Thus, there is a roughly 2-fold ratioof perfusion during IAC-CPR to perfusionduring standard CPR in a thoracic pumpmodel versus a roughly 1.5-fold ratio of per-fusion during IAC-CPR to perfusion duringstandard CPR in a cardiac pump model. Ifone takes the modern consensus view20, 35, 54
that the operative pump mechanism in differ-
ent animal and clinical models is a combina-tion of the cardiac and thoracic pumps, thesesimulation results agree perfectly with the ag-gregate results of laboratory and clinical re-search on IAC-CPR, in which systemic perfu-sion pressure or carbon dioxide excretionserved as measures of overall forwardflow.26, 43, 59, 61 These research studies found a1.5- to 2-fold improvement in perfusion withthe addition of IAC.
The safety of IACs, as reviewed pre-viously,43 has been well documented in 426humans, 151 dogs, and 14 pigs. Only oneisolated case report of traumatic pancreatitisin a child describes local trauma from abdom-inal compression during CPR.64 These datacompare favorably with the well-known andfrequent incidence of rib fracture and pulmo-nary contusion from chest compression dur-ing CPR.65–67 Increased emesis and aspirationfrom IAC have not been reported, and there
CIRCULATORY ADJUNCTS 49
Figure 10. (Continued). Pressures in a mathematical modelof the normal adult human circulation during cardiac arrestand IAC-CPR. The compression rate is 80 per minute. Maxi-mal chest compression pressure is �60 mmHg. Maximalabdominal compression pressure is �110 mm Hg. A, IAC-CPR with a pure cardiac pump mechanism: flow � 3.6 L /min; SPP � 68 mm Hg. B, IAC-CPR with a pure thoracicpump mechanism: flow � 2.1 L/min; SPP � 39 mm Hg.
is even evidence that if positive abdominalpressure is applied during ventilations fromthe beginning of an arrest, the rate of gastricinflation before endotracheal intubation is re-duced.68
Can we do even better? Theory suggeststhat the answer is ‘‘yes.’’ Ordinary IAC-CPR,as studied experimentally over the past 20years, includes only positive pressure com-pressions without active decompression. Alogical extension of this line of thought is toexamine full four-phase CPR, which includesactive compression and active decompressionof the chest and the abdomen. All four phasescan be accomplished in a single cycle, because
chest compression and abdominal decom-pression can be accomplished simultaneouslyin the first half of the cycle, and abdominalcompression and chest decompression can beaccomplished simultaneously in the secondhalf of the cycle.
Recently a commercial venture has at-tempted to implement this concept in a de-vice called the Lifestick (Datascope, Fairfield,NJ) (Fig. 11). The Lifestick is a mechanicaldevice under development, with which oneperson can perform both chest and abdominalCPR. Compression is applied through arocker arm with adhesive pads attached tothe chest and the abdomen. The broad chest

50 BABBS
Figure 11. Four-phase CPR with a Lifestick (Datascope, Fairfield, NJ).
compression pad of early models precludescardiac pump mechanism but also obviatesrib fracture. Because the chest and abdominalpads are adhesive, it is possible to obtain ameasure of upward retraction of the chestduring the abdominal compression phase andvice versa by a rocking motion of the device.Such a device in principle has the advantageof permitting active compression and decom-pression of both chest and abdomen.31
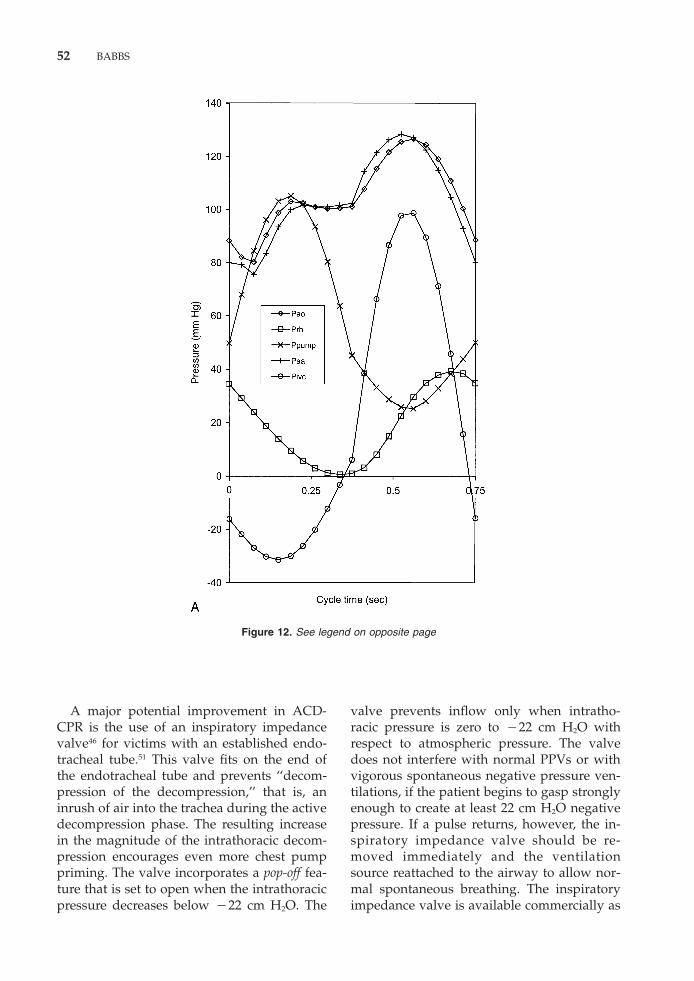
The hemodynamic potential of such four-phase CPR is illustrated in Figure 12. Figure12A shows cardiovascular pressures duringcardiac pump and abdominal pump CPRwith active compression and decompression.The four-phase method produces dramati-cally large pressure fluctuations in the chestand abdominal vascular compartments, al-though the external compression forces areno different than those used for standard CPRor conventional IAC-CPR, and the appliedexternal decompression forces are substan-tially less than the compression forces. Nearlynormal systemic perfusion pressures are ob-tained throughout the cycle. There is no re-striction of positive coronary and systemicperfusion pressure to the diastolic phase. For-ward blood flow is 4.6 L/min, approachingthe textbook value of 5.0 L/min for the nor-mal circulation in a 70-kg man. These levelsare a far cry from the 20% of normal forwardflow that has come to be expected from stan-
dard CPR.69-70 Routine practical implementa-tion of full four-phase CPR has yet to beachieved, partly as a result of legal and com-mercial wrangling unrelated to science andengineering; however, animal studies with aprototype Lifestick device are encouraging.44
The forgoing survey of resuscitation physi-ology suggests a significant potential for im-provement of current CPR through the appli-cation of combinations of positive andnegative pressure to the chest and the abdo-men. The most recent American Heart Associ-ation guidelines2 for CPR and emergency car-diovascular care permit the judicious use oftwo advanced forms of CPR at the discretionof a physician under conditions in which ade-quate equipment and trained personnel areavailable. These approved adjuncts includeIAC-CPR and ACD-CPR. As so-called ‘‘classIIb’’ interventions, IAC- and ACD-CPR areconsidered within the standard of care, whichreasonably prudent physicians can choose touse.71 IAC-CPR and ACD-CPR are consideredoptional or alternative interventions by mostexperts. Technically these adjuncts could beperformed together under the guidelines inselected clinical settings to achieve at leasta three-phase CPR, which has hemodynamicbenefits nearly as great as four-phase CPR.31
This new state of affairs, in which emergencydepartment physicians have considerableprofessional discretion, brings us to consider

CIRCULATORY ADJUNCTS 51
practical aspects of implementing the newCPR adjuncts.
PRACTICAL ASPECTS OF ACTIVECOMPRESSION-DECOMPRESSIONCARDIOPULMONARYRESUSCITATION
Active compression-decompression CPRrequires use of a plungerlike device, sold asthe CardioPump or ResQ-Pump (CPRx LLC,Minneapolis, MN). With a two-handed gripon the handles of the device, a rescuer canapply active compression and decompression.Teams in Europe, especially in Paris, havebeen trained to use the CardioPump withgood results, including improved survival at1 year after resuscitation compared with stan-dard CPR.72 Some studies have reportedmixed results with the CardioPump,73–77 per-haps as a result of less intensive training.78–79
Those considering use of ACD-CPR are ad-vised to train well in the use of the deviceand repeat training often.78 Training manne-quins and other educational materials areavailable from Ambu Inc. (Glostrup, Den-mark).
At the time of this writing, the AmbuCardioPumps are not approved for use inthe United States by the US Food and DrugAdministration. They are commercially avail-able outside the United States and are manu-factured by Ambu, Inc. and marketed in theWestern Hemisphere by CPRx LLC (Minne-apolis, MN). The CardioPump weighs 0.58 kgand costs about $300. The vacuum cup is 135mm in diameter and is made of soft siliconerubber. The cup can be removed for cleaningand for autoclave sterilization after use. Thevacuum cup is not electrically conducting anddoes not interfere with transchest electricaldefibrillation; it has been designed to adhereto a variety of chest anatomies, including wethairy skin, without losing contact with thechest wall during decompression. Earliermodels did not work well on women withlarger breasts, 80–81 and the cup may still sealpoorly in about 10% of women.
Rescuer fatigue is a known problem withACD-CPR, because more energy is needed toperform ACD than to do active compressionalone.79, 82 Back fatigue is definitely reduced ifthe rescuer either kneels beside the thorax of
the victim or works astride the victim on hisor her knees. A blanket or pillow under theknees of the rescuer may allow the rescuer’sarms and back to be straighter when usingthe CardioPump device.72 Because the handleis offset from the chest by about 15 cm, therescuer’s shoulders need to be higher overthe victim than in conventional CPR. If thepatient is on a table or raised surface, a stoolmay be needed by the rescuer to provide thenecessary elevation.
While using a CardioPump, the armsshould be straight and the back of the rescueras close to vertical as possible. The elbowsshould be locked. Wrists should be firm, suchas in gripping a tennis racquet. In this posi-tion, the rescuer can work effectively by rai-sing and lowering the hips against gravity. Asthe rescuer’s hips are lowered in the kneelingposition, the weight of the rescuer’s bodycan be used to apply compression. As therescuer’s hips are raised, the quadriceps mus-cles of the anterior thigh can work to applydecompression while the rescuer’s arms re-main straight.*
As fatigue sets in, rescuers tend to revert toformer habitual methods of chest compres-sion without decompression, and the benefitsof ACD-CPR are lost. Remembering to liftup during each cycle is the most challengingaspect of using a CardioPump device. A forcegauge on the handle indicates the targetranges of compression and decompressionforce for chests of soft, normal, or stiff charac-teristics. The gauge provides useful biofeed-back. The duty cycle for ACD-CPR is 50%compression time, 50% decompression time.Further details of ACD-CPR methodologyand training are described by Wik et al.78
*The reader is encouraged to try this motion in thekneeling position while palpating the quadriceps, gluteusmaximus, and hamstring muscles. Note that when thehips are raised when kneeling, the leg is extended andthe knee joint by the quadriceps and the thigh is ex-tended at the hip joint by the hamstrings. Posterior com-partment (hamstring) muscles and the gluteus maximusmuscles are also active in the kneeling position. Relianceon the large anterior and posterior thigh muscles andgluteus muscles minimizes fatigue and keeps the exerciseaerobic for either male or female rescuers. These samemuscles also should be used as much as possible inthe standing position to minimize fatigue. Upper-bodystrength is not required, once rescuers learn to use legmuscles and not back muscles. Nevertheless, adequatepersonnel need to be available so that frequent changescan occur every 3 to 5 minutes to avoid fatigue.
52 BABBS
Figure 12. See legend on opposite page
A major potential improvement in ACD-CPR is the use of an inspiratory impedancevalve46 for victims with an established endo-tracheal tube.51 This valve fits on the end ofthe endotracheal tube and prevents ‘‘decom-pression of the decompression,’’ that is, aninrush of air into the trachea during the activedecompression phase. The resulting increasein the magnitude of the intrathoracic decom-pression encourages even more chest pumppriming. The valve incorporates a pop-off fea-ture that is set to open when the intrathoracicpressure decreases below �22 cm H2O. The
valve prevents inflow only when intratho-racic pressure is zero to �22 cm H2O withrespect to atmospheric pressure. The valvedoes not interfere with normal PPVs or withvigorous spontaneous negative pressure ven-tilations, if the patient begins to gasp stronglyenough to create at least 22 cm H2O negativepressure. If a pulse returns, however, the in-spiratory impedance valve should be re-moved immediately and the ventilationsource reattached to the airway to allow nor-mal spontaneous breathing. The inspiratoryimpedance valve is available commercially as

CIRCULATORY ADJUNCTS 53
Figure 12. Pressures in a mathematical model of the normaladult human circulation during cardiac arrest and four-phaseCPR. The compression rate is 80 per minute. Maximal chestcompression pressure is �60 mm Hg. Maximal abdominalcompression pressure is �110 mm Hg. Maximal chest de-compression pressure is �20 mm Hg. Maximal abdominaldecompression pressure is �30 mm Hg. A, Four-phase CPRwith cardiac pump: flow � 4.6 L /min, SPP � 86 mm Hg. B,Four-phase Lifestick CPR with thoracic pump: flow 2.7 L/min; SPP � 51 mm Hg.

54 BABBS
a resuscitation device called the Resusci-Valveor ResQ-Valve (CPRx LLC, Minneapolis,MN). The valve is a disposable device thatcosts between $30 and $50.
PRACTICAL ASPECTS OFINTERPOSED ABDOMINALCOMPRESSION—CARDIOPULMONARYRESUSCITATION
From a practical standpoint, the simplest,least expensive, and longest studied CPR ad-junct is IAC-CPR. This method is essentiallydeviceless. There is no equipment cost, andthere is no requirement for FDA approval.IAC-CPR can be performed by two hands ofa third rescuer, as shown in Figure 9. IAC-CPR is especially appropriate for in-hospitalresuscitations, where the dictum ‘‘When extrahands are free, do IAC’’ may well apply. IAC-CPR is performed most easily when the rescu-ers compressing the chest and abdomen areon opposite sides of the patient. Because themost favorable clinical results have been ob-tained when IAC-CPR is applied from thebeginning of resuscitation, early applicationof the technique is to be encouraged. Use ofIAC-CPR as a last-ditch effort after pro-longed, failed advanced cardiac life support(ACLS) is not recommended and has not beenshown to be effective.61 Obviously, IAC is notrecommended for pregnant women, personssuspected of having an abdominal aortic an-eurysm, or persons known to have had recentabdominal surgery.
The abdominal compression technique inIAC-CPR involves rhythmic, manual com-pression of the mid-abdomen. The abdominalcompression point is located in the midline,halfway between the xiphoid process and theumbilicus. The recommended force of abdom-inal compression is that sufficient to generateapproximately 110 mm Hg external pressureon the abdominal aorta and vena cava and isequivalent to that required to optimally pal-pate the aortic pulse in a patient or volunteerwhen the heart is beating normally.83 Thetechnique for compression of the abdomen issimilar in most respects to the technique forcompression of the chest.
Hand Position andCompression Technique
The umbilicus should be visible and notcovered by the compressing hands. Just aschest compression is applied making contactwith the heel of one hand, which is coveredby the heel of the other hand, abdominalcompression is applied in the same manner.The heel of the rescuer’s bottom hand shouldlie along the midline of the abdomen. Thismidline position keeps the main force of com-pression over the abdominal vena cava andaorta. The fingers may be either extended orinterlaced but should be kept off the abdo-men.
A straight-armed abdominal compressiontechnique, similar to that used for chest com-pression, is ergonomically effective. Becausethe abdomen is composed of soft tissues with-out the bony resistance of the rib cage, ade-quate compressions do not require strongmuscular effort. In practical training, studentslearn the force required to produce safe andeffective 110 mm Hg pressure pulses withinthe abdomen using a folded blood pressurecuff and gauge (see later discussion). Thedepth of abdominal compression is not unlikethat of chest compression, 1.5 to 2 inches, ina normal sized, nonobese adult. For obesepatients, greater compression depth may benecessary. Compressions can be delivered tothe abdominal compression point straightdown in the vertical plane, or to maximizeaortic counterpulsation, from the left side ofthe victim at 11� left of vertical.83 In principle,when IAC-CPR is performed properly, thecarotid or femoral pulse demonstrates doublepeaks, denoting both chest and abdominalcompressions.31, 55 The clinical utility of as-sessing a double pulse in this setting, how-ever, has not been investigated.
Coordination of Chest andAbdominal Compressions
The rhythm of abdominal compression isnatural and easy to learn. If the chest com-pressor counts ‘‘one-and-two-and-three . . . ,’’the abdominal rescuer applies pressure dur-ing ‘‘and,’’ and releases pressure during eachcounted number. The release of abdominal

CIRCULATORY ADJUNCTS 55
pressure between chest compressions isneeded for chest and abdominal pump mech-anisms to work together31 and also to avoidentrapment of the right lobe of the liver underthe sternum when the chest is compressed.Thus, abdominal pressure should be appliedwhenever chest compressions are relaxed,and abdominal pressure should be relaxedwhenever chest compressions are applied.Abdominal pressure can maintained duringventilations to minimize gastric inflation ifno endotracheal tube is in place.68 The mostwidely used and tested duty cycle is 50%chest/50% abdominal compression time.There is some theoretical advantage to 30%chest/70% abdominal compression time30, butthis variation has not yet been tested in hu-mans.
If two-rescuer CPR has been establishedand a third rescuer becomes available, thisperson should take a position on the oppositeside of the patient from the second rescuerwho is performing chest compressions, locateproper hand position, sense the rhythm ofchest compressions, and begin then IACs. Ifrescuers doing chest and abdominal compres-sions wish to switch positions (abdominalcompressions are less tiring, because there isno ribcage resistance), it is natural for themto slide headward and footward, respectively,during a ventilation, because they are on op-posite sides of the patient.
Training Individuals To DoInterposed AbdominalCompression–CardiopulmonaryResuscitation
A detailed analysis of the ergonomic com-plexity of IAC (available from the author onrequest) suggests that it is no more compli-cated to learn and perform than is opening anairway. The following modifications of wholebody mannequins for teaching three-rescuerIAC-CPR are performed easily and are inex-pensive:
1. Add extra foam rubber to the lower tho-racic compartment of the mannequinand to the abdominal compartment tosimulate subcostal soft tissues.
2. Wrap a standard blood pressure cuffaround a towel and place it in the ab-dominal compartment beneath the ab-dominal compression point (5 cm head-ward of the umbilicus) in the midline.Bring the tubing, aneroid manometergauge, and squeeze bulb out at beltlineof the mannequin so that the gauge isvisible to the trainees. Tape target pres-sure markers on the manometer dial at120 mm Hg. Inflate cuff to a resting pres-sure of 10 mm Hg.
3. During practice sessions coach traineesto hit the target pressure during IAC.The issue of how hard to press has beenaddressed in detail elsewhere.83
If a mannequin is not available, a rolledblood pressure cuff placed inside a rolledtowel is a useful training model. Successfulpractice sessions can be conducted in as littleas 5 minutes. The following sequence maybe used:
1. The abdominal rescuer takes position onopposite side of victim from chest com-pressor.
2. Chest compressor says, ‘‘You press here(pointing to the abdominal compressionpoint) whenever I release.’’
3. Chest compressor counts ‘‘one-and-two-and-three. . . .’’ Abdominal rescuer ap-plies pressure during ‘‘and.’’
4. Start with slow-motion practice, andthen gradually increase to a normal com-pression rate. With this kind of practicesession, health care professionals can betaught to perform IAC with little timeor trouble.
Combining InterposedAbdominal Compressionwith Active Compression-Decompression–CardiopulmonaryResuscitation
In selected research settings, there is goodreason to investigate combining the methodsof ACD and IAC-CPR to create three-phaseCPR. Such a method is practically achievablewith current technology, omitting only thefourth phase, active abdominal decompres-

56 BABBS
sion, from full four-phase CPR. Advance ex-perience with the two techniques separately,is prudent before attempting to combinethem. Moreover, full consideration of the fol-lowing warnings and caveats is in order.
WARNINGS ABOUT THE GENERALUSE OF CIRCULATORY ADJUNCTS
Because of the requirement for specialtraining and sometimes special equipment,advanced forms of CPR are best performedin a hospital by trained health care providers.
Endotracheal intubation is prudent beforeinstituting CPR adjuncts. Most studies ofIAC-CPR have required that an endotrachealtube be in place for fear of regurgitation inresponse to IAC (a fear not substantiated bydata43). Similarly, an endotracheal tube is de-sirable if ACD-CPR is performed with an in-spiratory impedance valve. The valve can beused with a tightly sealed facemask, but extracare must be taken to avoid leaks.
It is extremely important in one’s enthusi-asm for CPR adjuncts not to delay electricalventricular defibrillation when ventricularfibrillation (VF) is present. New data confirmthe old84, 85: that if VF has been present for lessthan 4 to 5 minutes, electrical defibrillation isclearly the treatment of choice. For longerdown-times however, there is evidence that avasopressor drug plus effective CPR, whichproduces good coronary perfusion pressure,can improve resuscitation success. As long asdefibrillation is not delayed, enhanced CPRmethods, such as IAC-CPR, can potentiallybenefit patients in the hands of trained healthcare providers.
If initial shocks are not successful for VF,the rescuer should institute adjuncts early—not as a last resort after failed ACLS. Adjunctsdo not work on dead people. Their use afterfailed ACLS will only lead to unjustified cyni-cism.
With more powerful and effective CPR mo-dalities, one can expect an increased numberof discharge survivals72, 86; however, one alsomust expect an increased number of individu-als who survive only briefly. It is probably anunavoidable result of multiplied probabili-ties that, in addition to greater numbers of
lives saved, there also could be greater num-bers of people who are resuscitated and sub-sequently die a day or so later. It is evenpossible, although not yet shown by pub-lished data, that more effective techniques ofresuscitation might produce increased num-bers of individuals resuscitated to a lingeringvegetative state. Clinical experience with thenew modalities will be needed to determinewhich individuals are at greatest risk for thismost undesirable outcome. IAC- or ACD-CPRcannot change underlying pathology or con-trol the quality of care after resuscitation.There is however, theoretical, experimental,and clinical evidence that these improved,more energetic, and more aggressive resusci-tation methods can improve blood flow dur-ing CPR, and in turn the probability of neuro-logically intact short- and long-term survival.
SUMMARY
Principles of cardiovascular physiology tellus that during cardiac arrest and CPR, for-ward flow of blood can be generated by exter-nal compression or decompression of eitherthe chest or the abdomen. Standard CPRutilizes only one of these modes—chestcompression—and generates roughly 1 L/min forward flow in an adult human,45 whichis 20% of normal cardiac output. IAC-CPRuses two of these modes—chest compressionand abdominal compression—and generatesroughly twice the forward flow, or 2 L/minin an adult human.61 ACD-CPR uses two ofthese modes—chest compression and chestdecompression—and also generates roughlytwice the forward flow as standard CPR,51
although the results are somewhat model de-pendent. The studies by Sack et al86 with IAC-CPR and by Plaisance et al72 with ACD-CPRsuggest that when methods that double per-fusion are employed methodically, resuscita-tion outcome in terms of short- and long-termsurvival are also roughly doubled.72, 86 Thisstate of affairs is fortunate, because it is possi-ble that factors, such as severe underlyingdisease or the quality of postresuscitationcare, could blunt or cancel positive effects ofimproved blood flow during the brief resusci-

CIRCULATORY ADJUNCTS 57
tation period. Theoretically, full four-phaseCPR, including active compression and de-compression of both chest and abdomen, iscapable of generating 4 L/min forward flowor greater, which is 80% of normal, and thereis a reasonable prospect of achieving 100% ofnormal flow under conditions in which allfour phases are optimized.87 Standard CPR isclearly not the ultimate form of external CPR.There is real, credible evidence that substan-tial improvements in resuscitation methodsand results will be possible in the next de-cade.
References
1. Kouwenhoven WB, Jude JR, Knickerbocker GG:Closed-chest cardiac massage. JAMA 173:1064–1067,1960
2. Cummins RO: Guidelines 2000 for cardiopulmonaryresuscitation and emergency cardiovascular care: In-ternational consensus on science. Circulation102(suppl I):I-1–I-384, 2000
3. Fitzgerald KR, Babbs CF, Frissora HA, et al: Cardiacoutput during cardiopulmonary resuscitation at vari-ous compression rates and durations. American Jour-nal of Physiology 241:H442–H448, 1981
4. Idris AH: Reassessing the need for ventilation duringCPR. Ann Emerg Med 27:569–575, 1996
5. Jude JR, Kouwenhoven WB, Knickerbocker GG: Car-diac arrest: Report of application of external cardiacmassage on 118 patients. JAMA 178:1063–1070, 1961
6. Kuisma M, Alaspaa A: Out-of-hospital cardiac arrestsof non-cardiac origin: Epidemiology and outcome.Eur Heart J 18:1122–1128, 1997
7. Cobb LA, Werner JA, Trobaugh GB: Sudden cardiacdeath II: Outcome of resuscitation, management, andfuture directions. Modern Concepts of Cardiovascu-lar Disease 49:37–42, 1980
8. Eisenberg MS, Hallstrom A: Long-term survival afterout-of-hospital cardiac arrest. N Engl J Med 306:1340–1343, 1982
9. Weil MH, Tang W: Cardiopulmonary resuscitation:A promise as yet largely unfulfilled. Disease-a-month43:429–501, 1997
10. Redding JS: Abdominal compression in cardiopulmo-nary resuscitation. Anesthesia and Analgesia 50:668–675, 1971
11. Ralston SH, Voorhees WD, Babbs CF: Intrapulmonaryepinephrine during cardiopulmonary resuscitation:Improved regional blood flow and resuscitation indogs. Ann Emerg Med 13:79–86, 1984
12. Kern KB, Ewy GA, Voorhees WD, et al: Myocardialperfusion pressure: A predictor of 24-hour survivalduring prolonged cardiac arrest in dogs. Resuscita-tion 16:241–250, 1988
13. Mair P, Furtwaengler W, Baubin M: Aortic-valvefunction during cardiopulmonary resuscitation. NEngl J Med 329:1965–1966, 1993
14. Criley JM, Blaufuss AH, Kissel GL: Cough-inducedcardiac compression: A self-administered form of car-
diopulmonary resuscitation. JAMA 236:1246–1250,1976
15. Criley JM, Niemann JT, Rosborough JP, et al: Theheart is a conduit in CPR. Crit Care Med 9:373–374,1981
16. Rudikoff MT, Maughan WL, Effron M, et al: Mecha-nisms of blood flow during cardiopulmonary resusci-tation. Circulation 61:345–352, 1980
17. Weisfeldt ML: Physiology of cardiopulmonary resus-citation. Ann Rev Med 32:435–442, 1981
18. Feneley MP, Maier GW, Gaynor JW, et al: Sequenceof mitral valve motion and transmitral blood flowduring manual cardiopulmonary resuscitation indogs. Circulation 76:363–375, 1987
19. Gall F: Incompetence of the atrioventricular valvesduring cardiac massage. J Cardiovasc Surg 6:356–360, 1965
20. Paradis NA, Martin GB, Goetting MG, et al: Simulta-neous aortic, jugular bulb, and right atrial pressuresduring cardiopulmonary resuscitation in humans: In-sights into mechanisms. Circulation 80:361–368, 1989
21. Rainer EH, Bullough J: Respiratory and cardiac arrestduring anaesthesia in children. BMJ 1024–1028, 1957
22. Ohomoto T, Miura I, Konno S: A new method ofexternal cardiac massage to improve diastolic aug-mentation and prolong survival time. Ann ThoracSurg 21:284–290, 1976
23. Beyar R, Kishon Y, Kimmel E, et al: Intrathoracic andabdominal pressure variations as an efficient methodfor cardiopulmonary resuscitation: Studies in dogscompared with computer model results. CardiovascRes 19:335–342, 1985
24. Babbs CF, Geddes LA: Effects of abdominal counter-pulsation in CPR as demonstrated in a simple electri-cal model of the circulation. Ann Emerg Med12:247, 1983
25. Coletti RH, Kaskel PS, Cohen SR, et al: Abdominalcounterpulsation (AC): A new concept in circulatoryassistance. Trans Am Soc Artif Intern Organs 28:563–566, 1982
26. Ralston SH, Babbs CF, Niebauer MJ: Cardiopulmo-nary resuscitation with interposed abdominal com-pression in dogs. Anesthesia and Analgesia 61:645–651, 1982
27. Beyar R, Kishon Y, Sideman S, et al: Computer stud-ies of systemic and regional blood flow during car-diopulmonary resuscitation. Medical & Biological En-gineering and Computing 22:499–506, 1984
28. Babbs CF, Weaver JC, Ralston SH, et al: Cardiac,thoracic, and abdominal pump mechanisms in CPR:Studies in an electrical model of the circulation. AmJ Emerg Med 2:299–308, 1984
29. Babbs CF, Ralston SH, Geddes LA: Theoretical ad-vantages of abdominal counterpulsation in CPR asdemonstrated in a simple electrical model of the cir-culation. Ann Emerg Med 13:660–671, 1984
30. Babbs CF, Thelander K: Theoretically optimal dutycycles for chest and abdominal compression duringexternal cardiopulmonary resuscitation. Acad EmergMed 2:698–707, 1995
31. Babbs CF: CPR techniques that combine chest andabdominal compression and decompression: Hemo-dynamic insights From a spreadsheet model. Circula-tion 100:2146–2152, 1999
32. Maier GW, Newton JR, Wolfe JA, et al: The influenceof manual chest compression rate on hemodynamicsupport during cardiac arrest: High-impulse cardio-pulmonary resuscitation. Circulation 74(suppl IV):IV-51–IV-59, 1986

58 BABBS
33. Maier GW, Tyson GS, Olsen CO, et al: The physiologyof external cardiac massage: High-impulse cardiopul-monary resuscitation. Circulation 70:86–101, 1984
34. Babbs CF: High-impulse compression CPR: Simplemathematics points to future research. Acad EmergMed 1:418–422, 1994
35. Halperin HR, Tsitlik JE, Guerci AD, et al: Determi-nants of blood flow to vital organs during cardiopul-monary resuscitation in dogs. Circulation 73:539–550, 1986
36. Halperin HR, Tsitlik JE, Beyar R, et al: Intrathoracicpressure fluctuations move blood during CPR: Com-parison of hemodynamic data with predictions froma mathematical model. Ann Biomed Eng 15:385–403,1987
37. Tucker KJ, Idris A: Clinical and laboratory investiga-tions of active compression-decompression cardio-pulmonary resuscitation [editorial]. Resuscitation28:1–7, 1994
38. Tucker KJ, Khan JH, Savitt MA: Active compression-decompression resuscitation: Efects on pulmonaryventilation. Resuscitation 26:125–131, 1993
39. Babbs CF, Tacker WA: Cardiopulmonary resuscita-tion with interposed abdominal compression. Circu-lation 74(suppl IV):37–41, 1986
40. Babbs CF: Interposed abdominal compression-CPR:A case study in cardiac arrest research. Ann EmergMed 22:24–32, 1993
41. Einagle V, Bertrand F, Wise RA, et al: Interposedabdominal compressions and carotid blood flow dur-ing cardiopulmonary resuscitation: Support for athoracoabdominal unit. Chest 93:1206–1212, 1988
42. Sack JB, Kesselbrenner MB, Bregman D: Survivalfrom in-hospital cardiac arrest with interposed ab-dominal counterpulsation during cardiopulmonaryresuscitation. JAMA 267:379–385, 1992
43. Sack JB, Kesselbrenner MB: Hemodynamics, survivalbenefits, and complications of interposed abdominalcompression during cardiopulmonary resuscitation.Acad Emerg Med 1:490–497, 1994
44. Tang W, Weil MH, Schock RB, et al: Phased chestand abdominal compression-decompression: A newoption for cardiopulmonary resuscitation. Circulation95:1335–1340, 1997
45. DelGuercio L, Feins NR, Cohn JD, et al: Comparisonof blood flow during external and internal cardiacmassage in man. Circulation 31(suppl I):171–180,1965
46. Lurie KG, Coffeen P, Shultz J, et al: Improving activecompression-decompression cardiopulmonary resus-citation with an inspiratory impedance valve. Circu-lation 91:1629–1632, 1995
47. Lindner KH, Pfenninger EG, Lurie KG, SchurmannW, Lindner IM, Ahnefeld FW: Effects of active com-pression-decompression resuscitation on myocardialand cerebral blood flow in pigs. Circulation 88:1254–1263, 1993
48. Lurie KG, Lindo C, Chin J: CPR: The P stands forplumber’s helper. JAMA 264:1661, 1990
49. Cohen TJ, Tucker KJ, Lurie KG, et al: Active compres-sion-decompression: A new method of cardiopulmo-nary resuscitation: Cardiopulmonary ResuscitationWorking Group. JAMA 267:2916–2923, 1992
50. Chang MW, Coffeen P, Lurie KG, et al: Active com-pression-decompression CPR improves vital organperfusion in a dog model of ventricular fibrillation.Chest 106:1250–1259, 1994
51. Plaisance P, Lurie KG, Payen D: Inspiratory imped-ance during active compression-decompression car-
diopulmonary resuscitation: A randomized evalua-tion in patients in cardiac arrest. Circulation101:989–994, 2000
52. Wik L, Naess PA, Ilebekk A, et al: Effects of variousdegrees of compression and active decompressionon haemodynamics, end-tidal CO2, and ventilationduring cardiopulmonary resuscitation of pigs. Resus-citation 31:45–57, 1996
53. Sunde K, Wik L, Naess PA, et al: Effect of differentcompression–decompression cycles on haemody-namics during ACD-CPR in pigs. Resuscitation36:123–131, 1998
54. Chandra NC: Mechanisms of blood flow during CPR.Ann Emerg Med 22:281–288, 1993
55. Berryman CR, Phillips GM: Interposed abdominalcompression-CPR in human subjects. Ann EmergMed 13:226–229, 1984
56. Lindner KH, Ahnefeld FW, Bowdler IM: Cardiopul-monary resuscitation with interposed abdominalcompression after asphyxial or fibrillatory cardiacarrest in pigs. Anesthesiology 72:675–681, 1990
57. Babbs CF: Interposed abdominal compression-car-diopulmonary resuscitation: Are we missing themark in clinical trials? [editorial]. Am Heart J126:1035–1041, 1993
58. Rosborough JP, Niemann JT, Criley JM, et al: Lowerabdominal compression with synchronized ventila-tion: A CPR modality. Circulation 64(IV):303, 1981
59. Voorhees WD, Niebauer MJ, Babbs CF: Improvedoxygen delivery during cardiopulmonary resuscita-tion with interposed abdominal compressions. AnnEmerg Med 12:128–135, 1983
60. Babbs CF, Sack JB, Kern KB: Interposed abdominalcompression as an adjunct to cardiopulmonary resus-citation. Am Heart J 127:412–421, 1994
61. Ward KR, Sullivan RJ, Zelenak RR, et al: A compari-son of interposed abdominal compression CPR andstandard CPR by monitoring end-tidal PCO2. AnnEmerg Med 18:831–837, 1989
62. Sack JB, Kesselbrenner MB, Jarrad A: Interposed ab-dominal compression CPR and resuscitation outcomeduring asystole and electromechanical dissociation.Circulation 86:1692–1700, 1992
63. Mateer JR, Steuven HA, Thompson BM, et al: Pre-hospital IAC-CPR versus standard CPR: Paramedicresuscitation of cardiac arrests. Am J Emerg Med3:143–146, 1985
64. Waldman PJ, Walters BL, Grunau C: Pancreatic injuryassociated with interposed abdominal compressionsin pediatric cardiopulmonary resuscitation. Am J Em-erg Med 2:510–512, 1984
65. Clark DT: Complications following closed-chest car-diac massage. JAMA 181:337–338, 1962
66. Nagel EL, Fine EG, Krischer JP, et al: Complicationsof CPR. Critical Care Medicine 9:424, 1981
67. Silberberg B, Rachmaninoff N: Complications follow-ing external cardiac massage. Surg Gynecol Obstet119:6–10, 1964
68. Babbs CF, Schoenlein WE, Lowe MW: Gastric insuf-flation during IAC-CPR and standard CPR in a ca-nine model. Am J Emerg Med 3:99–103, 1985
69. Standards and guidelines for cardiopulmonary resus-citation (CPR) and emergency cardiac care (ECC).JAMA 244:453–509, 1980
70. Silver DI, Murphy RJ, Babbs CF, et al: Cardiac outputduring CPR: A comparison of two methods. CritCare Med 9:419–420, 1981
71. Cummins RO: Introduction to the internationalguidelines 2000 for CPR and ECC. Circulation102(suppl I):I-1–I-11, 2000
CIRCULATORY ADJUNCTS 59
72. Plaisance P, Adnet F, Vicaut E, et al: Benefit of activecompression-decompression cardiopulmonary resus-citation as a prehospital advanced cardiac life sup-port: A randomized multicenter study. Circulation95:955–961, 1997
73. Panzer W, Bretthauer M, Klingler H, et al: ACD ver-sus standard CPR in a prehospital setting. Resuscita-tion 33:117–124, 1996
74. Schwab TM, Callaham ML, Madsen CD, et al: Arandomized clinical trial of active compression-de-compression CPR versus standard CPR in out-of-hospital cardiac arrest in two cities. JAMA 273:1261–1268, 1995
75. Luiz T, Ellinger K, Denz C: Active compression-de-compression cardiopulmonary resuscitation does notimprove survival in patients with prehospital cardiacarrest in a physician-manned emergency medical sys-tem. J Cardiothorac Vasc Anesth 10:178–186, 1996
76. Stiell IG, Hebert PC, Wells GA, et al: The Ontariotrial of active compression-decompression cardiopul-monary resuscitation for in-hospital and prehospitalcardiac arrest. JAMA 275:1417–1423, 1996
77. Mauer DK, Nolan J, Plaisance P, et al: Effect of activecompression-decompression resuscitation (ACD-CPR) on survival: A combined analysis using indi-vidual patient data. Resuscitation 41:249–256, 1999
78. Wik L, Schneider T, Baubin M, et al: Active compres-sion-decompression cardiopulmonary resuscitation:Instructor and student manual for teaching and train-ing: Part II: A student and instructor manual. Resus-citation 32:206–212, 1996
79. Wik L, Mauer D, Robertson C: The first European
Address reprint requests to
Charles F. Babbs, MD, PhDDepartment of Basic Medical Sciences
Purdue UniversityWest Lafayette, IN 47907–1246
e-mail: [email protected]
pre-hospital active compression-decompression(ACD) cardiopulmonary resuscitation workshop: Areport and a review of ACD-CPR. Resuscitation30:191–202, 1995
80. Rabl W, Baubin M, Haid C, et al: Review of activecompression-decompression cardiopulmonary resus-citation (ACD-CPR): Analysis of iatrogenic complica-tions and their biomechanical explanation. ForensicSci Int 89:175–183, 1997
81. Klintschar M, Darok M, Radner H: Massive injury tothe heart after attempted active compression-decom-pression cardiopulmonary resuscitation. Int J LegalMed 111:93–96, 1998
82. Baubin M, Schirmer M, Nogler M, et al: Rescuer’swork capacity and duration of cardiopulmonary re-suscitation. Resuscitation 33:135–139, 1996
83. Babbs CF: IAC-CPR: Are we missing the mark inclinical trials? Am Heart J 126:1035–1041, 1993
84. Yakaitis RW, Ewy GA, Otto CW, et al: Influence oftime and therapy on ventricular defibrillation indogs. Crit Care Med 8:157–163, 1980
85. Marwick TH, Case C, Siskind V, et al: Adverse effectof early high-dose adrenaline on outcome of ventric-ular fibrillation. Lancet 2:66–68, 1988
86. Sack JB, Kesselbrenner MB, Bregman D: Survivalfrom in-hospital cardiac arrest with interposed ab-dominal counterpulsation during cardiopulmonaryresuscitation. JAMA 267:379–385, 1992
87. Babbs CF: Efficacy of interposed abdominal compres-sion-cardiopulmonary resuscitation (CPR), activecompression and decompression-CPR and LifestickCPR: Basic physiology in a spreadsheet model. CritCare Med 28:N199–202, 2000