civilizational conditions of proliferative diseases
TRANSCRIPT
CIVILIZATIONAL CONDITIONS OF PROLIFERATIVE DISEASES
Julian Aleksandrowicz
I I I KIinika Wewnetrznych A kademii Medycznei
Krakow, Poland
This paper considers the problem of the relations existing between the characteristic civilization of some given population, with ethology (as the science of morals) as its essential component, and the incidence of pro- liferative diseases of various types, including leukemia.
In different social groups the prevailing cultural patterns are, of course, different and so also are their ethical attitudes. There are, moreover, known geographical differences in the occurrence of proliferative diseases.
The evidence assembled to date is sufficient for us to conclude that in various social groups there must be some specific biological, physical, chemical, and psychosociological factors whose combined action influences the rate of occurrence of one or another proliferative disease.'. 3, 4 9 O-lo
A better knowledge of these factors is of tremendous significance for the healthy development of mankind; such understanding would allow us to identify, utilizing scientific principles of investigation, the pathogenic factors in the environment that cause the excessive rate of particular proliferative dis- eases and to develop methods for controlling these factors. The effectiveness of the prophylactic measures will, however, depend not only on man's intel- lectual and scientific effort but also on the degree of his emotional involvement in the attempts to eliminate the pathogens. In other words, the effectiveness of prophylactic measures depends on the mode of action and on the methods used to make real the system of values, which has as its highest aim the achievement of the health of mankind in the broadest sense.
I will, in the following discussion, restrict my consideration of the dynamism of proliferative diseases within a set of ecological conditions to one type only, i.e., to leukemia in men and animals. The working hypothesis may be sum- marized in the assumption that, because the evidence supplied by epidemiolog- ical statistics is already sufficient to demonstrate differences in the rate of occurrence of various kinds of leukemia within the same parameters of time and space, it is now possible to pass to the next stage of research and to identify and check leukemogenic factors by scientific methods. The third stage will then be the control and the elimination of these factors from the environment, i.e., prophylaxis.
Historical Variability of Diseases and Their Dependence on Civilization and Social Structures
Before presenting the current state of knowledge about the forms of leukemia in men and animals in different parts of the world, in different countries, in different districts of a country, and even in limited districts of a town or village, I would like to review briefly the changing pattern of human
167
168
diseases in different epochs and different parts of the world. We will see that diseases were influenced by the civilization prevailing at some particular period of history and in particular parts of the inhabited world.
When we look back on the past, we see how each new environmental factor, one after the other, influenced the animals living on the earth. With changing climates, the soil changed, causing, in turn, change of the flora. New environmental factors appearing one by one caused the “variability” phenom- ena, which shaped the bodies of the anthropoid apes. As the forests disap- peared from the surface of the earth, the apes were forced to come down to the ground. New species with erect bodies then appeared. Their further development reflected their way of life, determined by the conditions of their habitat, the open plains of South Africa. The local flora and fauna determined the forms by which these animals satisfied their energy needs. In the glacial epoch of the next stage of evolution, the equilibrium between the living crea- tures and their environment was dangerously disturbed. Our ancestors died in large numbers of starvation and cold. Only individuals capable of protecting themselves from cold and starvation could survive.
Thus, the appearance of Homo sapiens recens depended on the influences of climatic factors, such as the amount of sunshine, humidity, winds, etc. For example, in the course of the lengthy process of adaptation, melanin was con- centrated in the epidermis of the human skin and protected the body from the deadly effects of ultraviolet radiation. But before a new morphological type completed its development by adapting to environmental conditions, many in- dividuals must have suffered, and many may have died, from diseases caused by insolation and thus, presumably, also from proliferative diseases.
It, therefore, becomes clear that abiotic factors exerted an influence on the modeling of the human body in the process leading to the development of the particular varieties of the human species. These morphological changes and, hence, the psychological structure of man, depended solely on the random action of natural forces lasting for many millions of years.
It is only when mankind had developed the ability to think and to organize consciously the social environment that the morphological and psychological structure began to change more rapidly.
Because of reconstructions made possible by archeological findings, we can now look back over many thousands of years and with a high degree of probability define the environmental conditions in which diseases developed. The outlines of the history of diseases in different periods and different geo- graphical regions may be traced from the information supplied by the study of preserved human skeletons and by observations of certain primitive peoples, whose way and standard of life, even today, often corresponds to the prehis- toric epochs.
The most common diseases of the Paleolithic civilization were, according to Jean Bernard, those caused by parasites, as is frequently the case among today’s primitive nomad tribes, whose way of life is still governed by archaic social structures. In that distant period, diseases and anemias resulting from food deficiency were not widespread, and men suffered mainly from bacterial and protozoan parasitic diseases, ague, schistostomiasis, etc. Paleontological examinations of 40,000-year-old skeletons show that in the distant past man was not afflicted with deficiency diseases. The nomadic and pastoral way of life and cannibalism permitted him to satisfy his energy requirements sufficiently.
In the more recent past of the neolithic civilization, the important change
Annals New York Academy of Sciences

Biological and Medical Sciences 169
from the nomadic to the settled way of life occurred. Men domesticated some animals and learned to select some plants for cultivation. This settled way of life produced special conditions for the development of a new civilization. It was during this epoch that the first signs appeared of social stratification and of groups specialized in particular handicrafts. This, in turn, produced a situation favoring armed conflicts between the tribes. Ever since, wars have had as their consequence hunger and outright starvation. Characteristic for this epoch are such deficiency diseases as the anemias. This is confirmed by neolithic skeletons, which, in their histological structure, show symptoms of dietary deficiency.
We are, thus, justified in presuming that blood diseases, in which various deficiency symptoms were superimposed on the parasitic invasion, were characteristic for the neolithic period. We may, therefore, suppose that the common diseases then afflicting mankind, especially when crops failed, were the counterparts of what today are known as malnutritional disease, kwashiorkor, tropical macrocytic anemia, etc.
Such nutritional deficiencies may have been associated with the disap- pearance of cannibalism from the territories of Europe and North Africa. This was, however, a critical period, and mankind, having passed through an all-important revolution, reached a turning point in its moral history.
It seems highly probable that in the distant past men also suffered from proliferative disease of various types; they could have been exposed to such natural oncogenic factors as 3,4 benzpyrene, which sometimes was excessively concentrated in the vicinity of asphalt deposits near volcanoes, or telluric radiation. Nevertheless, these factors must have been incomparably more rare than they are today, when the chemical industry is developing increasing numbers of new products with mutational, teratogenic, carcinogenic, and leukemogenic effects.
Contemporary civilization has been dominated during the last two centuries by the industrial revolutions, which have changed the pattern of prevailing diseases. Progress in hygiene and the growth of the pharmaceutical industry have undoubtedly limited parasitic infections and the advance of factors caus- ing nutritional deficiency diseases. Appearing in their place today are dis- eases caused by the toxic effects of industrial by-products that often possess carcinogenic properties. Technical civilization, which represents man at a definite stage of his evolution, brings with it both favorable and unfavorable conditions for his further development. It has made possible the suppression of the epidemics that harassed mankind for centuries. It has added many years to human life. By reducing infant mortality, it has produced, along with highly desirable effects, a new demographic explosion and its concomitant alarming economic and social consequences.
Thus, the contemporary epoch is characterized by a steady growth of the number of tumors, exceeded in the developed countries only by premature death from arteriosclerosis, heart disease, and traffic accidents, Tumors and leukemias, which, during the first decades of this century, were not observed in young people and children or in animals and fish, have become much more frequent.
All these observations lead to the conclusion that the extremely rare oc- currence of proliferative diseases in the primitive civilizations was due to man’s very limited exposure to a very limited number of oncogenic factors. Today, our industrial civilization increasingly exposes man and the higher vertebrates
170 Annals New York Academy of Sciences
to carcinogenic and leukemogenic factors that accumulate in the environment. They disturb the biocenotic equilibrium, a fact becoming increasingly obvious in the particular links of the water-soil-plant-animal-man chain.
As can be seen from the above discussion, the kind of social structure characteristic of the particular stages of historical evolution, i.e., considered in relation to time, determines the occurrence of specific proliferative diseases. Any change of the social structure obviously leads to change in the environment and, in turn, in the manner that proliferative diseases afflict humanity.
Contemporary Regional Differences in Proliferative Diseases and Their Incidence
R. Doll has published maps showing the worldwide distribution of cancers of the esophagus, stomach, lungs, colon, breast, and liver.5
It appears that cancer of the esophagus has three main high-incidence foci: Kazakstan on the northern coast of the Caspian Sea, Bulawayo in Southern Rhodesia, and the region of Transkei in South Africa.
Comparison of esophageal cancer occurrence in various countries shows that in the Guryev district in Kazakstan, its incidence is 200 times higher than in the Netherlands and Nigeria. This phenomenon has not yet been satisfactorily explained. Burrell and co-workers have suggested that the factors responsible for these differences lie in a deficiency of certain soil components and the infection of crops with substances causing the production of nitrosamine.
Cancer of the stomach is most frequent in Japan, the U.S.S.R., South Africa, Chile, and Colombia. Its incidence is particularly low in southwest England and among the white population of the U.S. Such a distribution is attributed by various authors to dietary factors. Associating this form of can- cer with substances in decaying foods, they suggest that improved methods of preserving food that are widely applied in the United States determine its low incidence of stomach cancer.
Lung and bronchial cancer is most common in Great Britain, Central Europe, especially Germany, Belgium, Czechoslovakia, Hungary, the Soviet Union, Canada, the United States, Uruguay, and New Zealand. On the other hand, in Spain, France, Italy, Yugoslavia, Romania, and the Balkan States, it is less frequent. Men are more often attacked than women, except in Great Britain, where women patients are more numerous.
A remarkable property of cancer of the large intestine is its apparent asso- ciation with the Anglo-American way of life and not with race. It is equally common among white and black. Its occurrence is very low among the African population of South Africa and in the Balkans, India, the Philippines, and Japan.
The incidence of breast cancer is highest in the countries of western Europe, South Africa, Australia, New Zealand, and Israel. The further east, the lower the incidence of this disease; it is very low in Uganda and Mozam- bique, Taiwan, and Indonesia. In the U.S., the rate of the disease among white and black women is the same. Japanese living in the Hawaiian Islands suffer a higher breast cancer incidence than those living in Japan.
The data on the distribution of cancer of the liver refer to man between the ages of 15 and 44. This age group was chosen for observation because in countries with an especially high incidence of hepatic cancer, it appears

Biological and Medical Sciences 171
earlier in that age group. Another reason for choosing this age group was that it ensured the fewest diagnostic errors, because in older persons it is often difficult to distinguish between primary cancer of the liver and cancer of the biliary ducts.
It appears that in this age group hepatic cancer is rare everywhere in the world except in some areas in Africa: the province of Ibadan in Nigeria, Johannesburg, and Mozambique, where it occurs as frequently as lung cancer in Great Britain and is more than 1,000 times higher than primary liver cancer in various parts of Europe. It is believed that aflatoxin, a metabolic product of Aspergillus flavus, is responsible for the high incidence of hepatic carcinoma. This mold develops with special abundance on such substrates as groundnuts and foodstuffs kept in a damp and warm environment.
Lymphatic leukemias in men and animals are extremely rare in China and the Far East, a fact pointed out to me during my visits in 1960 to the clinics and hospitals of Peking, Ulan Bator, and Canton. On the other hand, in the Netherlands and the countries bordering on the Baltic Sea, i.e. Denmark; Schleswig, West Germany; and the Polish northern provinces, morbidity from lymphatic leukemia in both men and cattle is particularly high.
Studying morbidity from leukemias in cattle in Poland, Karaczkiewicz found that the rate was very high, sometimes higher than 200 per 100,000 in the northwest provinces, although in the southwest provinces it was as low as about six per 100,000. The geographical difference between these high and low rates of leukemia incidence in cattle corresponds to the partition boundaries between the parts of Poland, which before 1918 were attached to Germany on the one hand and Austria and Russia on the other. According to Karaczkie- wicz, this remarkable epidemiological situation was caused by the differences in agricultural techniques in the partitioned parts of the country. It is com- mon knowledge that agriculture was more advanced in Prussia than in the other two partitioning countries; potassium fertilizers were used in much greater quantities, which led to the reduction of the magnesium content of the soil, thus disturbing the biocenotic balance in a direction that favored the proliferative processes in tissues, a problem I shall deal with below.
Cultural and Industrial Causes of Proliferative Diseases
The problem at this point is to find an explanation for the differences de- scribed above in the geographic distribution of cancers. Recent epidemiologi- cal research has proved that morbidity in the proliferative processes depends to a much higher extent than previously supposed on man’s conditions of life. For this reason, nearly 90 per cent of cancers are today believed to be stimulated by human activities, and thus, theoretically speaking, it lies in man’s power to prevent them.
Some authors, for instance Higginson, classify cancers according to the nature of the precipitating factors into cultural cancers, industrial cancers, and idiopathic cancers.
The first of these groups are the cancers that may be attributed to tradi- tional customs of a particular population. For example, in India, oral cancer is common, and the cause, in the Bombay region, is the custom of chewing betel leaves. A small piece of the betel leaf, which has narcotic properties, is placed in the mouth between the tongue and the cheek. The leaves are pow-

172 Annals New York Academy of Sciences
dered with lime, which causes congestion of the mucous membrane of the mouth, thus improving assimilation of the drug. I t is not surprising, therefore, that cancer of the mucous membrane of the mouth is a common disease among these people.
In South Africa, similarly, there is a custom of using snuff made from the leaves of the aloe plant, and this seems to be the cause of cancer of the sinuses.
It is now well known that among cigarette smokers, lung cancer is two to three times more frequent than cancer of the mouth. On the other hand, among peoples where there is a custom of using naswayam, a mixture of tobacco, ash, lime, and oil, independently of cigar and cigarette smoking, cancer of the mouth is twice as frequent as lung cancer. In the Kashmir, a common form of cancer called kangir develops on the skin of the abdomen; among the peoples of this area, there is, reportedly, a custom of warming the abdomen with a lump of hot clay.
Our second grouping, industrial and occupational cancers, includes as- bestos tumors that occur in workers living near asbestos deposits or working in asbestos mines. In South Africa, mesothelioma caused by irritation with chrysolite frequently occurs. Arsenic compounds, to which farmers are often exposed because of the extensive use of pesticides and insecticides in modern agriculture, are also responsible for a substantial proportion of lung cancers.
Case reported that naphthylamine used by the textile industry for dyeing fabrics caused tumors of the bladder in 15 workers employed as distillers. He concluded that everybody was susceptible to exposure to carcinogenic factors when their dose was sufficiently high.
Finally, it is a well-known fact that leukemia and erythroleukemia occur among persons working in a benzene-contaminated environment.
In the last groupidiopathic cancers-Higginson lists different forms of cancer for which an etiological background could not be identified with research methods existing at present.
Ecological Conditioning of Etiology and Pathogenesis of Proliferative Diseases
The evidence presented here to prove both quantitative and qualitative differences between various forms of proliferative disease in various cultural formations seems also to indicate that there must be differences of concentra- tions of the known and suspected carcinogenic and leukemogenic factors within the particular ecological environments. In an attempt to obtain a clearer picture of these factors, we undertook a group of investigations of small areas, such as districts, towns, and villages, and even individual farmsteads and houses, together with the environment in the homes of cancerous marriages and families.
These studies showed that in specific areas there were centers of cancerous and leukemic diseases and that their distribution was not accidental but was determined by specific factors. In order to show more clearly to what extent environmental conditions, shaped by man himself to a much greater degree than by the forces of nature, are responsible for the spread of proliferative diseases, I shall outline here the present state of knowledge about oncogenesis.
For the development of a proliferative disease, the following hypothetical
Biological and Medical Sciences 173
conditions must be fulfilled: ( 1 ) predisposition, (2) presence of the virus in- fection factor, and (3) presence of cocarcinogens. Predisposition consists of a set of biological phenomena occurring at the molecular level of the genetic structure. It is precisely these phenomena that are responsible for the fact that in the same environmental conditions some persons are attacked by proliferative disease, which suggests a predisposition, whereas others are not.
The differences in predisposition are due to deoxyribonucleic acid (DNA), which carries the structural, and hence the metabolic, code of cells and determines that the daughter cells have the same structure and functions as the parent cells.
The genetic system and the molecular structures of cells are weakened with regard to lysosomes and genes by the absence of some stabilizers, of which so far Mg++ ions have been identified, a result of the work of Goldberg and others. A deficiency of Mg++ ions facilitates penetration of the genetic struc- ture of cells by viral oncogenic factors; these factors then cause the uncon- trolled multiplication of cells, resulting in proliferative growths. Among the carcinogens, the best known are ionizing radiation, some chemical com- pounds, and mold metabolites and are referred to by the general terms of physical, chemical, and biological cocarcinogens, respectively. Under specific conditions these cocarcinogens activate the nucleic acid molecule, which probably has the same nature as a virus and causes a structural change in the genetic apparatus of the cell. This disturbs the daughter cells and makes them form a clone that differs in structure and function from the parental cells and assumes the form of neoplasmic growth.
This viruslike factor, the particle C , as it has been called, has now been identified by electron microscopy by Dmochowski and others. The particle C seems to be responsible for the vertical and horizontal transfer of the pro- liferative disease from experimental animals to animals with a specific immuno- logical structure, from man to animals,ll* l2 from one farm animal to another, an occurrence often observed in agriculture, and perhaps from animals to man. In this last case, the direction of the transfer is indicated by some results of prospective experiments to which, of necessity, we have to restrict ourselves.
The aim of our ecological researches-I present here only one of the investigated cases-is to identify the environmental factors that may, in the present state of knowledge, be responsible for oncogenesis due to mutual infection or to exposure to conditions having an oncogenic effect both on men and on animals.
We conducted our investigation,2 in collaboration with professors of agri- culture, University of Krakow, Ewy, Litynski, Komornicki, and Smyk, in the village of Okocim-Pomianowa. In this village there was a “cancerous” house where five persons, three of them relatives, suffered from cancer. Adjacent to the house was a cow shed where for years the cows had had leukemia (leukemia herd). The farm was an experimental one belonging to the School of Agri- culture in Krakow. This environment was very suitable for ecological studies on oncogenesis.
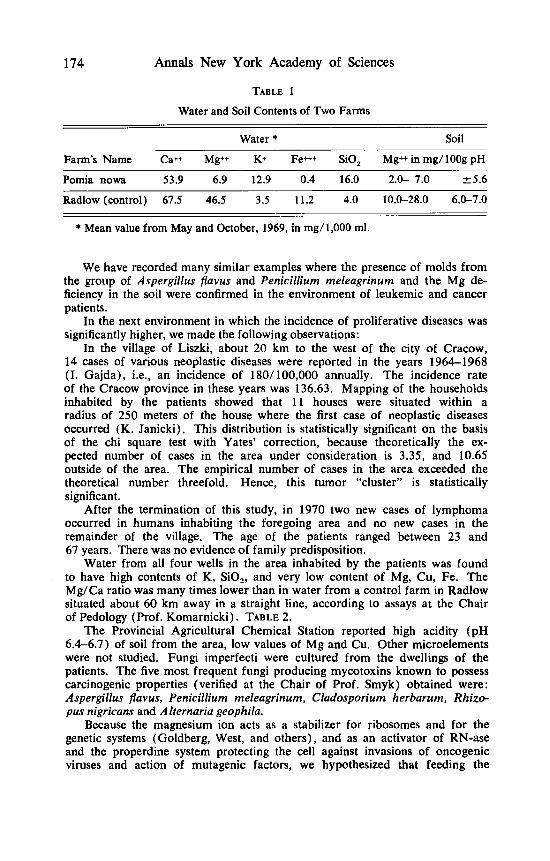
We found that in the farm there was (1) a reservoir of oncogenic viruses in cows with leukemia, (2) a reservoir of biological cocarcinogens from molds producing carcinogenic metabolites, i.e., Aspergillus flaws, Penicillium meleagrinurn, and Rhizopus nigricans, in the walls of the “cancerous” house, barns, and soil, and (3) a magnesium deficiency in the Uszwica River, in the soil, and in the wells (TABLE 1).
174 Annals New York Academy of Sciences
TABLE 1
Water and Soil Contents of Two Farms
Water * Soil
Farm’s Name Cat+ Mg++ K+ Fe+++ SiO, Mg++ in mg/100g pH
Pomia nowa 53.9 6.9 12.9 0.4 16.0 2.0- 7.0 k5.6
Radlow (control) 67.5 46.5 3.5 11.2 4.0 10.0-28.0 6.0-7.0
* Mean value from May and October, 1969, in mg/1,000 ml.
We have recorded many similar examples where the presence of molds from the group of Aspergillus flavus and Penicillium meleagrinum and the Mg de- ficiency in the soil were confirmed in the environment of leukemic and cancer patients.
In the next environment in which the incidence of proliferative diseases was significantly higher, we made the following observations:
In the village of Liszki, about 20 km to the west of the city of Cracow, 14 cases of various neoplastic diseases were reported in the years 1964-1968 (I. Gajda), i.e., an incidence of 180/100,000 annually. The incidence rate of the Ctacow province in these years was 136.63. Mapping of the households inhabited by the patients showed that 11 houses were situated within a radius of 250 meters of the house where the first case of neoplastic diseases occurred (K. Janicki) . This distribution is statistically significant on the basis of the chi square test with Yates’ correction, because theoretically the ex- pected number of cases in the area under consideration is 3.35, and 10.65 outside of the area. The empirical number of cases in the area exceeded the theoretical number threefold. Hence, this tumor “cluster” is statistically significant.
After the termination of this study, in 1970 two new cases of lymphoma occurred in humans inhabiting the foregoing area and no new cases in the remainder of the village. The age of the patients ranged between 23 and 67 years. There was no evidence of family predisposition.
Water from all four wells in the area inhabited by the patients was found to have high contents of K, SO2, and very low content of Mg, Cu, Fe. The Mg/Ca ratio was many times lower than in water from a control farm in Radlow situated about 60 km away in a straight line, according to assays at the Chair of Pedology (Prof. Komarnicki) . TABLE 2.
The Provincial Agricultural Chemical Station reported high acidity (pH 6.4-6.7) of soil from the area, low values of Mg and Cu. Other microelements were not studied. Fungi imperfecti were cultured from the dwellings of the patients. The five most frequent fungi producing mycotoxins known to possess carcinogenic properties (verified at the Chair of Prof. Smyk) obtained were: Aspergillus flavus, Penicillium meleagrinum, Cladosporium herbarum, Rhizo- pus nigricans and Alternaria geophila.
Because the magnesium ion acts as a stabilizer for ribosomes and for the genetic systems (Goldberg, West, and others), and as an activator of RN-ase and the properdine system protecting the cell against invasions of oncogenic viruses and action of mutagenic factors, we hypothesized that feeding the

Biological and Medical Sciences 175
animals a diet deficient in Mg would favor oncogenesis. This hypothesis was confirmed by the work of McCreary, Battifora, and P. Bois, and, in Poland, by Kowalczykowa and Stachura, who caused leukemic proliferation in rats fed Mg-deficient diet.
The experimental results suggest the hypothesis that in countries in which dietary magnesium is high, the incidence of leukemia should be low. This is confirmed by Seelig, who reported that in the Far East, where leukemia in cattle and lymphatic leukemia in men were rare, the daily dose of magnesium was 6-10 mg per kg food. On the other hand, the daily dose of the Euro- American population is less than 5 mg of magnesium and is steadily dropping.
The level of magnesium in soil is determined by the contemporary cultural pattern; modern agricultural techniques are dominated by potassium fertiliza- tion; because of the magnesium-potassium antagonism, the magnesium content of soil, and therefore of plants, animals, and men, is steadily reduced.
* * * In contemporary civilization, the dominant pattern of interhuman rela-
tions is characterized by malnutrition of two-thirds of the inhabitants of the world; therefore, the use of chemical compounds for more intensive farming and higher agricultural output is justified, even if it leads to a disturbed bio- cenotic balance and, consequently, to-among other problems-proliferative disease caused by overuse of chemical fertilizers. The logical consequence of this situation should be, however, such interhuman and international relations that would allow man to preserve the biocenotic equilibrium, thus acting prophylactically to prevent the spread of proliferative diseases.
It remains to be seen whether the attempts to correct the supply of mag- nesium and probably copper, iron, etc., in soil, water, and plants, will reduce the incidence of proliferative diseases in the districts where the deficiency of these elements and proliferative disease morbidity are high.
In sum, we present the opinion that one of the most important ways to prevent neoplasm is by protection of the balance in biocenosis; it means a conservation of nature. Conservation of nature is conditioned by war prophylaxis. It is obvious that in some situations, war industry pollutes water, soil, and food with carcinogens destroying the biophysical environment con- siderably more strongly than would industry without military purposes. Hate, fanaticism, and racism are ruining the psychosocial environment connected
TABLE 2
MICROELEMENTS IN WELL WATER IN CLUSTER OF HUMAN CANCER IN LISZKI VERSUS CONTROL IN RADLOW
Mg++ Ca++ Ca/Mg SO, Fe+++ a++ K+Na+ Liszki well 1 42.2 321.6 7.62 26.0 0 0.022 292.7
6 L '* 2 36.2 162.2 4.46 22.0 0 0.009 496.8
" " 3 51.3 260.9 5.08 20.0 0 0.009 388.5
" '& 4 30.2 200.1 6.62 32.0 0 0.009 396.9
Radlow well central 46.5 67.5 1.45 4.0 11.2 - 26.5

176 Annals New York Academy of Sciences
with the biophysical environment. In this way, the vicious circle devastating human kind is being closed.
We believe that the human being-the highest value-creates new values and is dependent on them. So, the fate of humanity in our own hands.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11. 12.
ALEKSANDROWICZ, J. 1969. Estudios sobre la influencia del Mg++ en la pato- genesis, terapeutica y prophylaxis del sistema linforreticular. Folia Clin. Int. 19(4): 3-4.
ALEKSANDROWICZ, J. & B. SMYK. 1971. Mycotoxins and their role in oncogenesis, with special reference to blood diseases. Polish Med. Bull. (In press.)
BATTIFORA, H. A., P. A. MCCREARY, B. M. HANEMAN, G. H. LAING & G. M. HASS. 1968. Chronic magnesium deficiency in the rat. Arch. Path. 122: 610.
BOIS, P., E. B. SANDBORN & P. E. MEISSIER. 1969. A study of thymic lymphosar- coma developing in magnesium deficient rats. Cancer Res. 29: 763.
DOLL, R. 1967. Prevention of Cancer, Pointers from Epidemiology. Nuff. Provinc. Hosp. Trust.
DELBET, P. 1944. Politique prkventive du cancer. La Vie Claire. Montreuil, France.
SEELIG, M. S. 1964. The requirement of magnesium by the normal adult. Amer. J. Clin. Nutr. 14: 342.
STRIEBEL, A. 1966. Uber das Calcium-Magnesium Verhaltnis in Urin von Gesunden und Krebskranken. Oncologia 20(3): 209.
VOISIN, A. 1964. Les Nouvelles Lois Scientifiques d’application les Engrais. Quebec, Canada.
TROMP, S. W. & J . H. DIEHL. 1955. A statistical study of the possible relation- ship between cancer of the stomach and soil. Brit. J. Cancer 9: 3.
ADAMS, R. A. 1968. Cancer Res. 28: 1121. LIKNAITZKY, D. G. 1969. Cancer 23(1): 94.