cjd guideline 301120101
TRANSCRIPT
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 2 of 18 30/11/2010
CONTENTS
1 POLICY STATEMENT--------------------------------------------------------------------------- 3
2 SCOPE OF GUIDELINE------------------------------------------------------------------------ 3
3 LEGISLATION/OTHER RELATED POLICIES -------------------------------------- 3
3 GLOSSARY OF TERMS AND OTHER DEFINITIONS --------------------------- 4
4 ROLES AND RESPONSIBILITIES ------------------------------------------------------- 5
5 GUIDELINE FOR THE PREVENTION OF TRANSMISSION OGF TSES 6 5.1 Patient Risk Groups 6 5.2 Known or suspected patients 6 5.3 At risk patients-asymptomatic 6 5.4 Infectivity of tissues with TSEs 6 5.5 Risk Assessment 7 5.6 Precautions on known or suspect patients 8 5.7 Precautions on at risk patients 8 5.8 Labelling & transportation of instruments 10 5.9 Quarantine of instruments 10 5.10 Labelling of specimens 11 5.11 Healthcare Risk waste 11 5.12 Clinical Spillages 11 5.13 Last Offices 11
6 IMPLEMENTATION & EDUCATION PLAN ---------------------------------------- 11
7 EVALUATION AND AUDIT ---------------------------------------------------------------- 11
8 REFERENCES ------------------------------------------------------------------------------------- 12
9 APPENDICES ------------------------------------------------------------------------------------- 13 9.1 Appendix 1 – Risk categorisation of persons 13 9.2 Appendix 2 - Diagnostic Criteria for TSEs 14 9.3 Appendix 3 – Risk Assessment Form 17
10 SIGNATURE SHEET --------------------------------------------------------------------------180
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 3 of 18 30/11/2010
1 POLICY STATEMENT
1.1. Transmissible Spongiform Encephalopathies (TSEs) are caused by unconventional infectious agents currently thought to be proteins known as prions. TSE agents exhibit unusual resistance to conventional decontamination methods (e.g. autoclaving or chemical disinfection)
1.2. The human TSEs cause a variety of neurological symptoms including dementia and personality disorders as well as neuromuscular symptoms e.g. unsteadiness, involuntary muscular jerking. All human TSEs are extremely rare but all are usually fatal
2 SCOPE OF GUIDELINE The purpose of this guideline is to;
2.1. Provide guidance to staff on the precautions necessary to minimize the risk of occupational exposure to Transmissible Spongiform Encephalopathies (TSEs).
2.2. To prevent the onward transmission of TSEs via surgical instrumentation.
2.3. This guideline applies to patients known or suspected to have CJD, i.e. those with clinical symptoms and potential patients at risk of developing the disease i.e. patients having a clinical or family history that places them in a risk group or patients who received UK sourced plasma factor concentrates (1980- 2001).
2.4. This guideline applies to all staff involved in the care of patients with known or suspected CJD or patients in the at-risk category.
2.5. It applies to staff involved with surgical instruments/endoscopes their handling, storage, cleaning and decontamination or disposal used on patients infected with CJD.
3 LEGISLATION/OTHER RELATED POLICIES
3.1. NDSC Guidelines on Minimising the Risk of Transmission of Transmissible Spongiform Encephalopathies in healthcare settings in Ireland, NDSC and Department of Health & Children; 2004
3.2. Standard and Transmission based precautions guideline (HPSC 2009)
3.3. Hand Hygiene policy
3.4. Guidelines on the wearing of personal protective equipment to prevent exposure to blood/body fluids
3.5. Policy on healthcare risk waste-segregation and disposal
3.6. Procedure for the management of blood and bodily fluid spillages
3.7. The Safety, Health and Welfare at Work Act 2005, No. 10
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 4 of 18 30/11/2010
3 GLOSSARY OF TERMS AND OTHER DEFINITIONS
3.1 Transmissible Spongiform Encephalopathies
-known as prion diseases, are fatal degenerative brain diseases which occur in humans and certain other animal species. A common feature of all TSEs is the appearance of microscopic vacuoles (holes) in the grey matter of the brain, giving a sponge-like appearance, from which the conditions derive their name.
All TSEs are invariably fatal once clinical signs appear; there is no known treatment or prophylaxis. Person to person transmission of TSEs through direct contact does not occur. Diagnosis is usually made clinically, there are currently no widely available laboratory tests for human TSEs although the diagnosis can be confirmed by examination of brain tissue after death. Brain biopsy may be used in investigating cases of suspected TSE but may not be definite in establishing a diagnosis. Cerebral cortical signal increase and high signal in caudate nucleus and putamen on fluid attenuated inversion recovery or diffusion-weighted imaging magnetic resonance imaging are useful in the diagnosis of sporadic CJD.
The recognised human TSEs include:
• Creutzfeldt-Jacob disease (CJD) including classical sporadic, familial, iatrogenic and new variant
• Gerstmann-Straussler-Scheinker syndrome (GSS) • Fatal Familial insomnia • Kuru
3.2 Creutzfelt- Jacob Disease (CJD)
- The best known human TSE is Creutzfelt- Jacob Disease. Most cases of CJD are sporadic and the incidence is thought to reflect the rate of spontaneous mutation of naturally occurring prion protein to the altered form.
3.3 Variant Creutzfeldt-Jacob disease (vCJD)
- In 1995 a new form of TSE was described in the UK and labelled variant CJD. Patients with vCJD tend to be younger than those with sporadic CJD and have a longer duration of illness. A link has been established between vCJD and bovine spongiform encephalopathy (BSE) in cattle and vCJD appears to have arisen through the consumption of BSE-infected animal products.
Apart from CJD and vCJD there are a number of other prion diseases including Kuru, Gerstmann Straussler syndrome (GSS), Fatal Familial Insomnia (FFI).
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 5 of 18 30/11/2010
4 ROLES AND RESPONSIBILITIES
4.1 The patient’s consultant
The Consultant in charge of the patient is responsible for ensuring: • That the Theatre Nurse Manager is aware of the patients status so that she/he
has adequate time to prepare the department • That all members of the surgical team including anaesthetics are aware of the
requirements required
4.2 The Consultant Microbiologist The consultant microbiologist is responsible for ensuring:
4.2.1 Guidance from the HPSC and other expert groups is followed.
4.2.2 Advising the hospital on the appropriate use of single use disposable equipment for any required invasive medical/surgical procedures.
4.2.3 Notifying all confirmed or strongly suspected cases to the CJD surveillance unit in Edinburgh and the Regional Director of Public Health.
4.2.4 Ensure any incident relating to a TSE is managed as described in the Hospital Major Outbreak Guideline.
4.3 The infection Prevention and Control Team The Infection Prevention and Control Team is responsible for;
4.3.1 Auditing this policy at least every two years.
4.3.2 Updating the policy to reflect current guidance.
4.3.3 Providing education to support the implementation of this policy.
4.4 Medical & Nursing Staff
Medical & Nursing Staff are responsible for;
4.4.1 Ensuring that staff members in their area are aware of this policy. 4.4.2 Facilitating education on the content of this policy.
4.4.3 Alerting the Infection Prevention & Control Team to any potential breach of this
policy.
4.4.4 Notifying the HPSC/ Consultant Microbiologist (out of hours) “on call” if any patient has been identified as suspected CJD/vCJD.
4.4.5 The Health Care Professional responsible for the patients care must ask whether
they have been notified that they are at increased risk of CJD/vCJD for public health purposes. This is to identify patients with known or suspected CJD, or potentially at risk of acquiring CJD prior to any invasive procedure on high or medium risk tissues, or any intervention involving contact with the eye. The assessment should be included in the initial consultation and the results placed into the patients notes under Procedure.
4.5 Occupation Health Department Occupation Health Department are responsible for keeping records of employees that are known to have been exposed to CJD infective material. Records must be kept for 40 years from the date of exposure.
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 6 of 18 30/11/2010
5 GUIDELINE FOR THE PREVENTION OF TRANSMISSION OF TSEs
5.1 Patient Risk Groups When considering measures to prevent transmission of CJD, a distinction should be made between patients known or suspected to have CJD (i.e. those with clinical symptoms) and potential patients at risk of developing the disease i.e. asymptomatic, but having a clinical or family history which places them in one of the risk groups. Appendix 1 outlines a risk categorisation of patients.
5.2 Known or suspected patients 5.2.1 Patients diagnosed as having CJD or a related disorder e.g. vCJD,
GSS, FFI and Kuru. 5.2.2 Patients suspected of having CJD or a related disorder, whose clinical
symptoms are suggestive of CJD but where the diagnosis has not yet been confirmed.
5.3 At risk patients-asymptomatic Asymptomatic patients who are potentially at risk of developing CJD or a related disorder e.g. recipients of hormone derived from human pituitary glands i.e. growth hormone gonadotrophin, recipients of human dura mater grafts, people with a family history of CJD and patients who have received UK sourced plasma factor concentrates (between 1980-2001) are also considered “at risk” for transmission of vCJD (1%), although no cases have been reported to date.
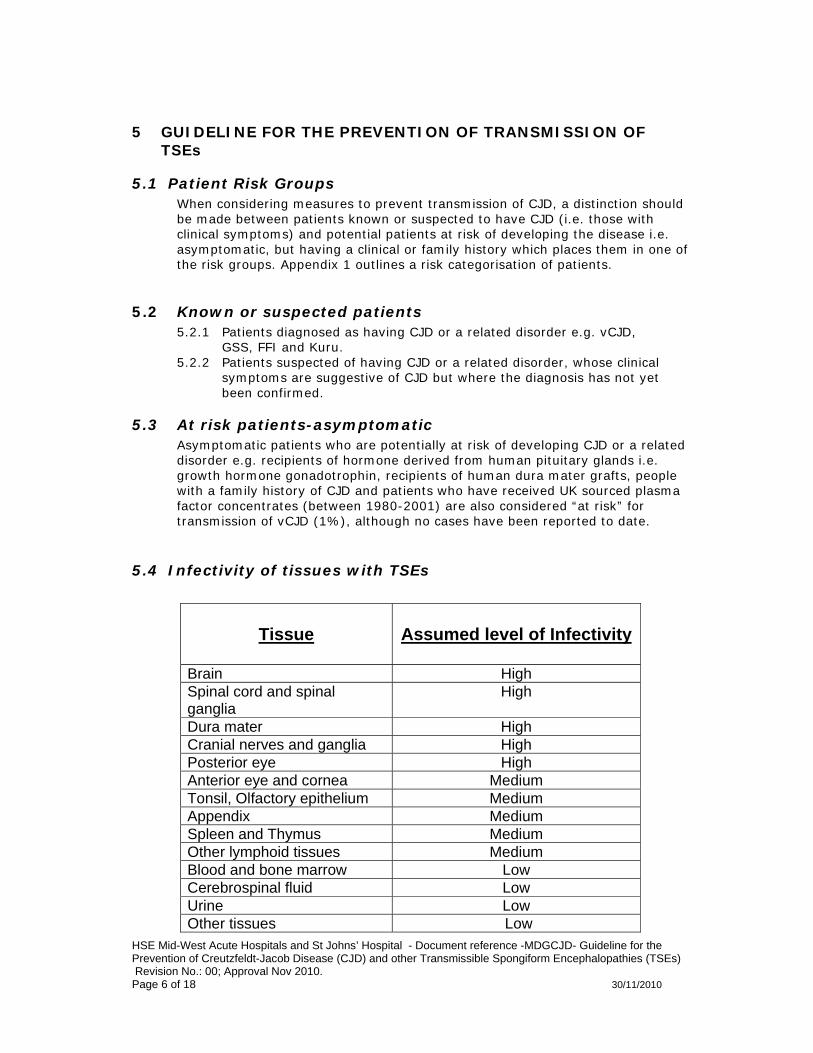
5.4 Infectivity of tissues with TSEs
Tissue
Assumed level of Infectivity
Brain High Spinal cord and spinal ganglia
High
Dura mater High Cranial nerves and ganglia High Posterior eye High Anterior eye and cornea Medium Tonsil, Olfactory epithelium Medium Appendix Medium Spleen and Thymus Medium Other lymphoid tissues Medium Blood and bone marrow Low Cerebrospinal fluid Low Urine Low Other tissues Low
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 7 of 18 30/11/2010
5.5 Risk Assessment
5.5.1 In most routine clinical contact, no additional precautions are needed for
the care of patients in the risk groups. However, when certain invasive interventions are performed there is the potential for exposure to the agents of TSE. The tissues that present the highest risk of exposure to the agents of TSE are the brain, spinal cord, and eyes. Therefore, special precautions need to be taken for interventions involving these tissues for known, suspect or at risk patients. Diagnostic criteria for these patient groups are outlined in Appendix 2.
5.5.2 For the care and clinical management of known, suspect or at risk
patients it may be necessary to undertake a range of clinical procedures. In these situations every effort should be made to plan carefully not only the procedure, but also the practicalities surrounding the procedure, e.g. communication, instrument handling, storage, cleaning and decontamination or disposal.
5.5.3 While it is important that staff are aware of the risks so that appropriate
precautions can be taken, healthcare staff are reminded of the need to maintain patient confidentiality.
5.5.4 For non-invasive investigations, e.g. x-ray procedures, no specific
precautions, other than those that would normally be applied to safeguard patient well-being are required.
5.5.5 Surgical instrumentation used for known or suspect patients should be
disposed of, whereas, for at risk patients, disposal is recommended only where there is contact with a high risk tissue, i.e. brain, spinal cord or eye.
5.5.6 A risk assessment (Appendix 3) should be completed prior to any surgery
/ endoscopy / invasive procedure where contact with high/medium risk TSE tissue is likely. High/medium risk tissue includes brain, spinal cord, posterior/anterior eye, olfactory epithelium and lymphoid tissue.
5.5.7 If a patient has had a procedure/surgery performed and is subsequently
found to be in the above mentioned patient group, the instruments used will be tracked, traced and quarantined.
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 8 of 18 30/11/2010
5.6 Precautions on known or suspect patients 5.6.1 The following precautions should be taken for all clinical procedures on
known or suspect patients. 5.6.2 Wherever appropriate and possible, the intervention should be performed
in an operating theatre. 5.6.3 Perform the procedure at the end of the list to allow normal cleaning of
theatre surfaces before the next session. 5.6.4 Involve only the minimum number of healthcare personnel required. 5.6.5 Wear the following single-use protective clothing:
• Liquid repellent operation gown, over a plastic apron • Gloves • Mask • Visor or goggles
5.6.6 Maintain a one-way flow of instruments. 5.6.7 Use single-use disposable surgical instruments and equipment where
possible. 5.6.8 Re-usable surgical instruments and equipment must not be re-used until
the recommended decontamination procedures has been carried out as outlined in Table 1 and 2 below.
5.7 Precautions on at risk patients
5.7.1 If the clinical intervention involves brain, spinal cord, or eyes, the precautions recommended above for procedures on known or suspect patients should be taken.
5.7.2 If the clinical intervention does not involve brain, spinal cord or eyes the
following precautions should be taken. 5.7.3 Wear the following protective clothing:
• Liquid repellent operation gown, over a plastic apron • Gloves • Mask • Visor or goggles
5.7.4 Use single use surgical instruments and equipment wherever reasonably
practicable. 5.7.5 Destroy all single use items by incineration. 5.7.6 Re-usable surgical instruments and equipment must not be re-used until
the recommended decontamination procedures has been carried out as outlined in Table 1 and 2 below.
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 9 of 18 30/11/2010
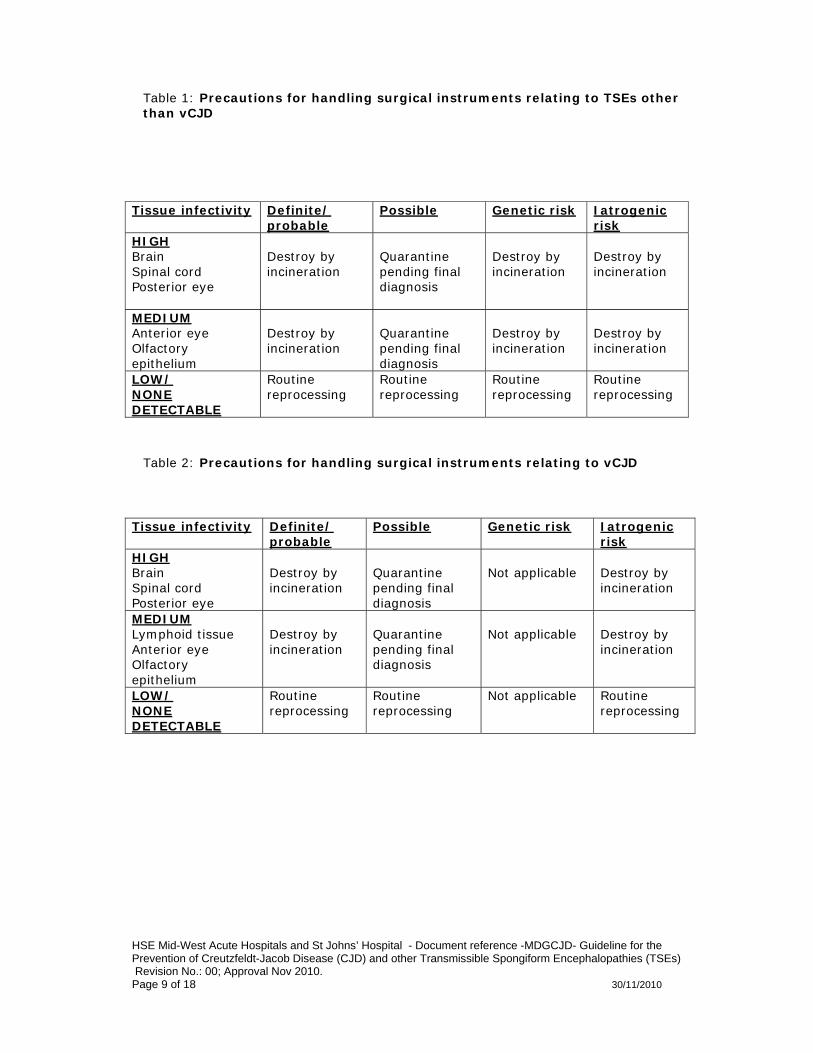
Table 1: Precautions for handling surgical instruments relating to TSEs other than vCJD
Table 2: Precautions for handling surgical instruments relating to vCJD
Tissue infectivity Definite/ probable
Possible Genetic risk Iatrogenic risk
HIGH Brain Spinal cord Posterior eye
Destroy by incineration
Quarantine pending final diagnosis
Destroy by incineration
Destroy by incineration
MEDIUM Anterior eye Olfactory epithelium
Destroy by incineration
Quarantine pending final diagnosis
Destroy by incineration
Destroy by incineration
LOW/ NONE DETECTABLE
Routine reprocessing
Routine reprocessing
Routine reprocessing
Routine reprocessing
Tissue infectivity Definite/ probable
Possible Genetic risk Iatrogenic risk
HIGH Brain Spinal cord Posterior eye
Destroy by incineration
Quarantine pending final diagnosis
Not applicable
Destroy by incineration
MEDIUM Lymphoid tissue Anterior eye Olfactory epithelium
Destroy by incineration
Quarantine pending final diagnosis
Not applicable
Destroy by incineration
LOW/ NONE DETECTABLE
Routine reprocessing
Routine reprocessing
Not applicable Routine reprocessing
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 10 of 18 30/11/2010
5.8 Labelling & transportation of instruments 5.8.1 All instruments and items of equipment that have been in contact with
known, suspect or at risk patients should be clearly identified.
5.8.2 Items used on known or suspect patients should be labelled for disposal. 5.8.3 Items used on at risk patients, where there has been contact with brain,
spinal cord or eye should also be labelled for disposal, whilst those used on other tissues should be labelled either for re-processing or disposal as appropriate.
5.8.4 Items for re-processing should be securely contained in a robust, leak
proof container, and transferred to the Central Sterile supplies department as soon as possible after use. Items should be transferred by a designated person from the theatre team to the CSSD Manager.
5.8.5 Items for disposal by incineration should be isolated in a rigid clinical
waste container and transported to the designated area in the waste compound to await collection by the waste contractor. This should occur after consultation with the Maintenance officer, who will arrange appropriate management while awaiting collection.
5.9 Quarantine of instruments 5.9.1 Detergents or disinfectants should not be added to the container prior to
transfer to CSSD, as these could potentially damage the instruments or act as protein fixatives.
5.9.2 Instruments should be physically cleaned prior to quarantine, preferably
using automated methods. 5.9.3 Decontaminate washer-disinfector prior to re-use. 5.9.4 After cleaning, instruments should be placed on a disposable instrument
tray and allowed to air dry, before being transferred to a leak proof container for quarantine.
5.9.5 Label container recording the following details:
• Date of procedure • Type of procedure • Risk category of procedure • Clinician responsible for the patients care • Patients name, date of birth and hospital identification number • Number of instruments in the container • Type of instruments in the container • Identification number of container • Whether instruments were manually cleaned prior to quarantine or
placed directly into quarantine container • Name and contact details of designated person with responsibility
for instrument quarantine • Indicate whether the instruments are quarantined pending a final
diagnosis or have been quarantined following use on a known TSE case and being held for further use only on known TSE case
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 11 of 18 30/11/2010
• The quarantine area must be separated from areas used to store instruments that have been reprocessed or are awaiting reprocessing.
5.10 Labelling of specimens TSEs are categorised as hazard group 3 organisms. All pathology including central nervous system specimens from at risk patients must be labelled as ‘DANGER OF INFECTION’.
5.11 Healthcare Risk waste
5.11.1 Body fluids i.e. blood, urine, faeces from patients at risk of a TSE should be handled and
disposed of using the same precautions as for any other patient. 5.11.2 TSE infectious waste is defined as high or moderate infectivity tissues from patients with
a known or suspected TSE or high infectivity tissue from a patient at increased risk of developing a TSE and any disposable items that have come in contact with any of these tissues. All such materials should be placed in secure, leak-proof containers with a black lid and disposed of by incineration.
5.12 Clinical Spillages In the event of cleaning surfaces that have been contaminated with TSE infectious material hypochlorite 20,000ppm should be used.
5.13 Last Offices Laying out of the body should be carried out using standard infection prevention and control practices.
6 IMPLEMENTATION & EDUCATION PLAN Plan to implement this guideline from Jan 2011 following workshops with all GI, ENT and Eye services (including medical and nursing personnel from relevant theatres and endoscopy suites) advising on the completion of a risk assessment pre procedure. Decontamination officers from all CSSDs will also be invited to an educational workshop.
.
EVALUATION AND AUDIT This guideline will be revised every 2 years and audit of compliance with the guideline will be undertaken once every 2 years by the decontamination team Earlier review may be required in response to exceptional circumstances, organisational change or relevant changes in legislation or guidance
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 12 of 18 30/11/2010
7 REFERENCES Advisory Committee on Dangerous Pathogens, Spongiform Encephalopathy Advisory Committee (1999) Transmissible Spongiform Encephalopathy Agents: Safe Working and the Prevention of Infection, UK.HMSO. Department of Health and Children (2004) Guidelines on Minimising the Risk of Transmission of Transmissible Spongiform Encephalopathies in Healthcare Settings in Ireland, CJD Infection Control Committee and Scientific Advisory Committee, National Disease Surveillance Centre.
The Royal Wolverhampton Hospitals NHS Trust Control and Management of Transmissible Spongiform Encephalopathies, including Creutzfeldt Jakob Disease (CJD); April 2009
St Vincent’s Healthcare Group. Transmissible Spongiform Encephalopathies. 2009
University Hospitals Coventry and Warwickshire NHS Trust. Trustwide guidelines for the management of patients with known or suspected Creutzfeldt-Jakob disease. 2005.
Updated clinical diagnostic criteria for sporadic Creutzfeldt-Jakob disease. Brain 2009: 132: 2659-2668.
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 13 of 18 30/11/2010
8 APPENDICES
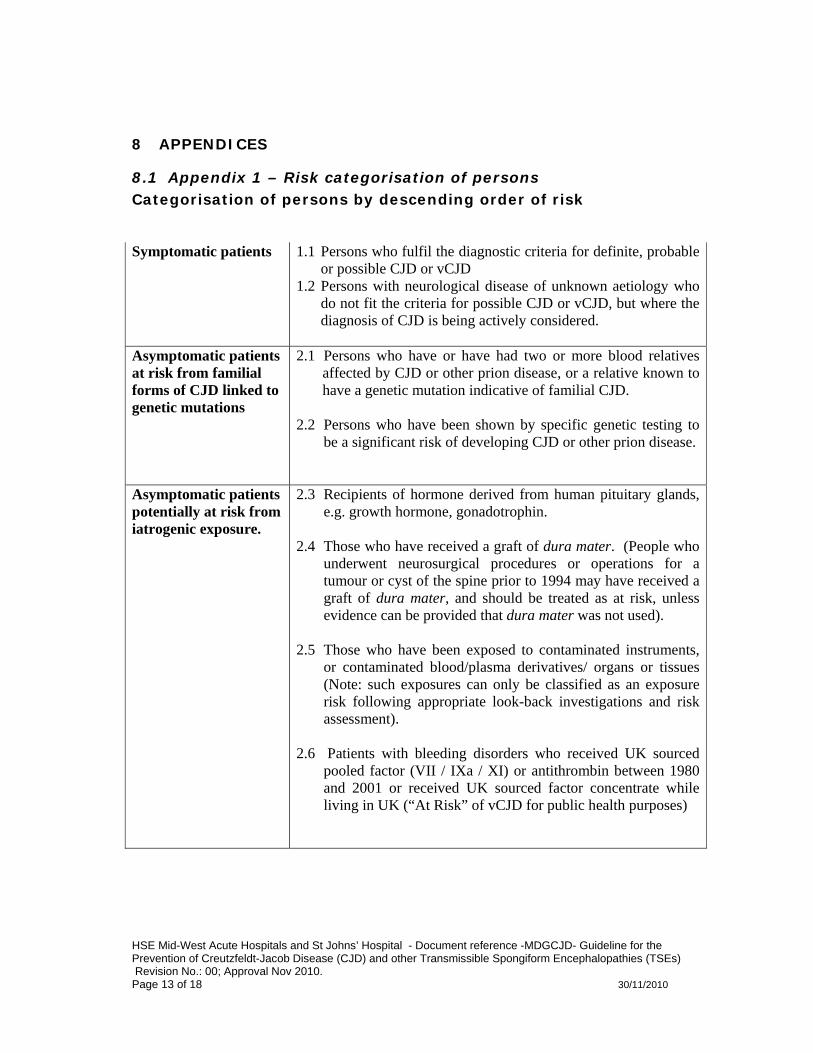
8.1 Appendix 1 – Risk categorisation of persons Categorisation of persons by descending order of risk Symptomatic patients
1.1 Persons who fulfil the diagnostic criteria for definite, probable or possible CJD or vCJD
1.2 Persons with neurological disease of unknown aetiology who do not fit the criteria for possible CJD or vCJD, but where the diagnosis of CJD is being actively considered.
Asymptomatic patients at risk from familial forms of CJD linked to genetic mutations
2.1 Persons who have or have had two or more blood relatives affected by CJD or other prion disease, or a relative known to have a genetic mutation indicative of familial CJD.
2.2 Persons who have been shown by specific genetic testing to
be a significant risk of developing CJD or other prion disease.
Asymptomatic patients potentially at risk from iatrogenic exposure.
2.3 Recipients of hormone derived from human pituitary glands, e.g. growth hormone, gonadotrophin.
2.4 Those who have received a graft of dura mater. (People who
underwent neurosurgical procedures or operations for a tumour or cyst of the spine prior to 1994 may have received a graft of dura mater, and should be treated as at risk, unless evidence can be provided that dura mater was not used).
2.5 Those who have been exposed to contaminated instruments,
or contaminated blood/plasma derivatives/ organs or tissues (Note: such exposures can only be classified as an exposure risk following appropriate look-back investigations and risk assessment).
2.6 Patients with bleeding disorders who received UK sourced
pooled factor (VII / IXa / XI) or antithrombin between 1980 and 2001 or received UK sourced factor concentrate while living in UK (“At Risk” of vCJD for public health purposes)
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 14 of 18 30/11/2010
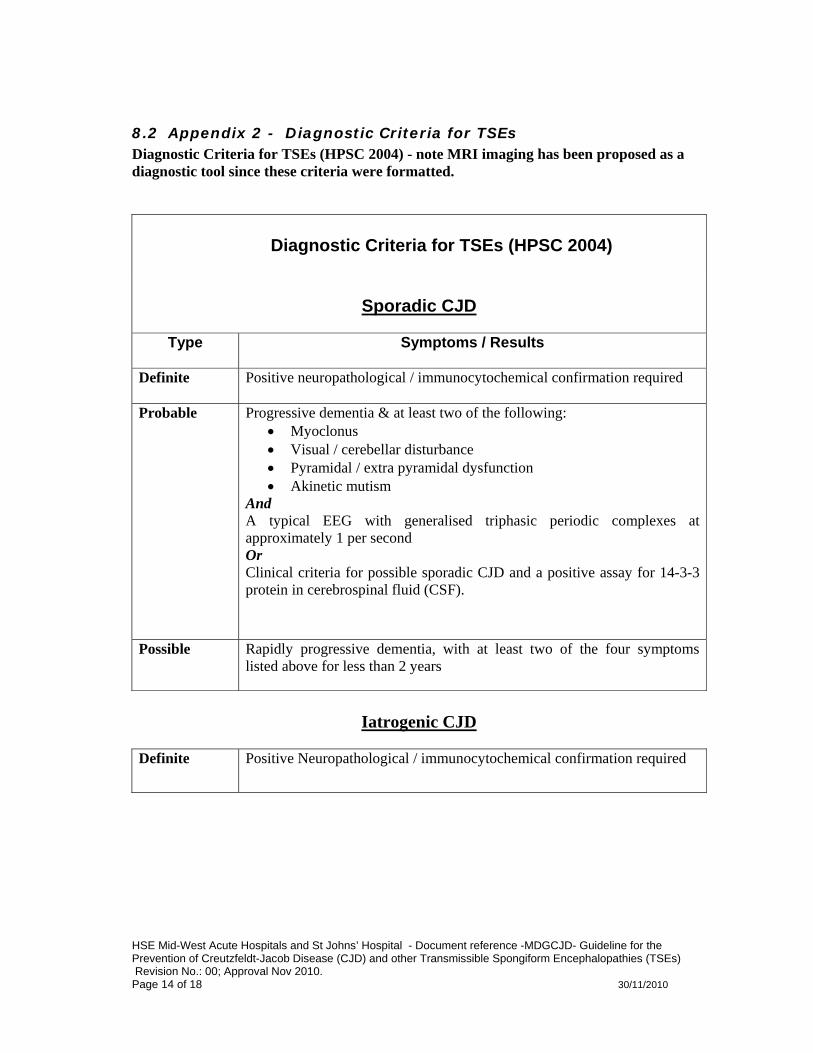
8.2 Appendix 2 - Diagnostic Criteria for TSEs Diagnostic Criteria for TSEs (HPSC 2004) - note MRI imaging has been proposed as a diagnostic tool since these criteria were formatted.
Diagnostic Criteria for TSEs (HPSC 2004)
Sporadic CJD
Type Symptoms / Results
Definite
Positive neuropathological / immunocytochemical confirmation required
Probable
Progressive dementia & at least two of the following: • Myoclonus • Visual / cerebellar disturbance • Pyramidal / extra pyramidal dysfunction • Akinetic mutism
And A typical EEG with generalised triphasic periodic complexes at approximately 1 per second Or Clinical criteria for possible sporadic CJD and a positive assay for 14-3-3 protein in cerebrospinal fluid (CSF).
Possible Rapidly progressive dementia, with at least two of the four symptoms listed above for less than 2 years
Iatrogenic CJD
Definite
Positive Neuropathological / immunocytochemical confirmation required
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 15 of 18 30/11/2010
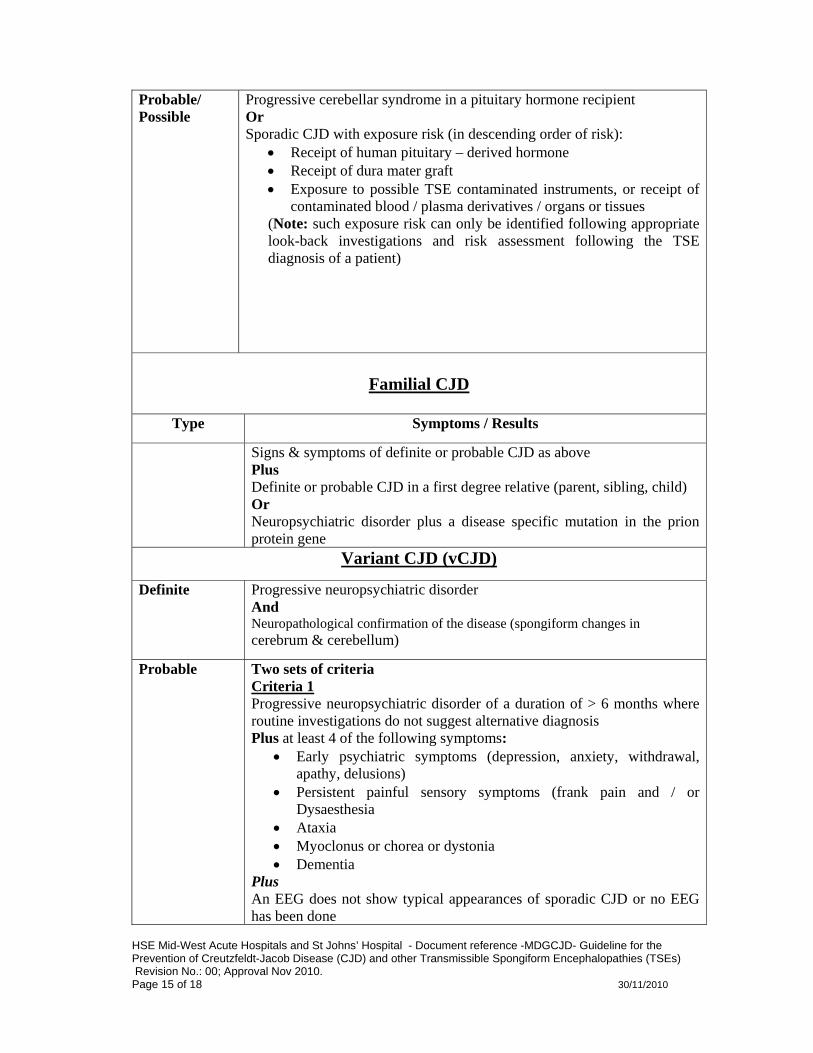
Probable/ Possible
Progressive cerebellar syndrome in a pituitary hormone recipient Or Sporadic CJD with exposure risk (in descending order of risk):
• Receipt of human pituitary – derived hormone • Receipt of dura mater graft • Exposure to possible TSE contaminated instruments, or receipt of
contaminated blood / plasma derivatives / organs or tissues (Note: such exposure risk can only be identified following appropriate look-back investigations and risk assessment following the TSE diagnosis of a patient)
Familial CJD
Type Symptoms / Results
Signs & symptoms of definite or probable CJD as above Plus Definite or probable CJD in a first degree relative (parent, sibling, child) Or Neuropsychiatric disorder plus a disease specific mutation in the prion protein gene
Variant CJD (vCJD)
Definite
Progressive neuropsychiatric disorder And Neuropathological confirmation of the disease (spongiform changes in cerebrum & cerebellum)
Probable Two sets of criteria Criteria 1 Progressive neuropsychiatric disorder of a duration of > 6 months where routine investigations do not suggest alternative diagnosis Plus at least 4 of the following symptoms:
• Early psychiatric symptoms (depression, anxiety, withdrawal, apathy, delusions)
• Persistent painful sensory symptoms (frank pain and / or Dysaesthesia
• Ataxia • Myoclonus or chorea or dystonia • Dementia
Plus An EEG does not show typical appearances of sporadic CJD or no EEG has been done
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 16 of 18 30/11/2010
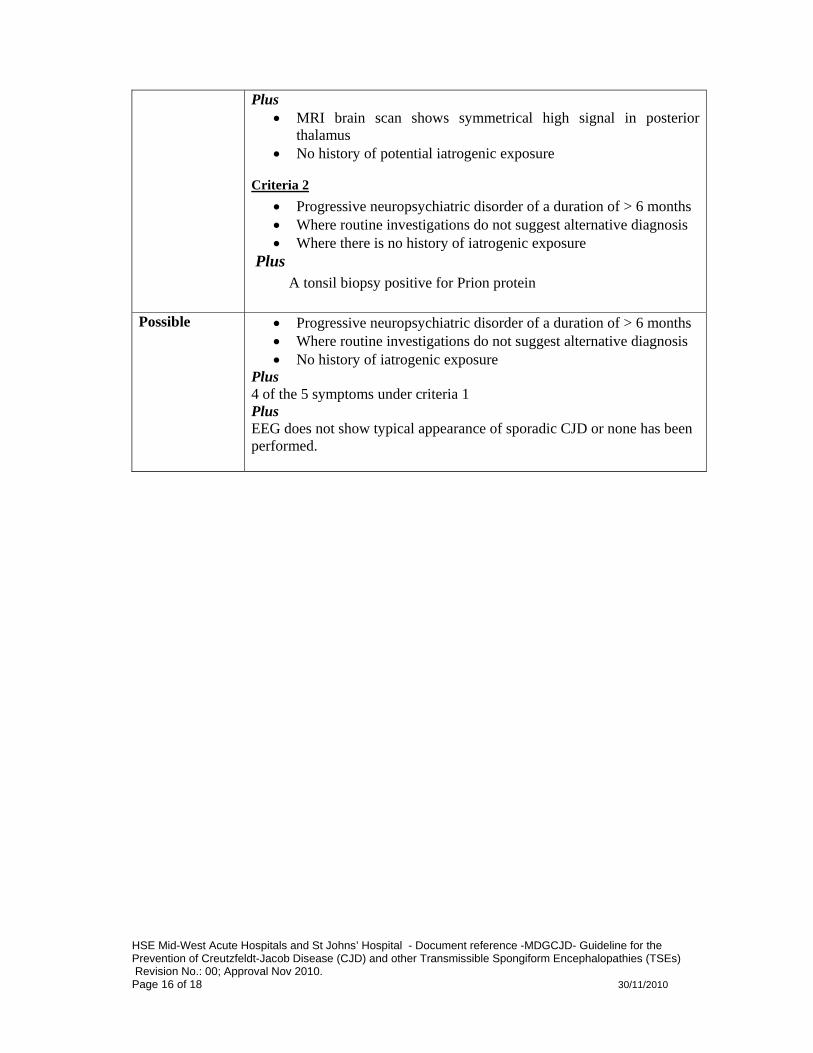
Plus • MRI brain scan shows symmetrical high signal in posterior
thalamus • No history of potential iatrogenic exposure
Criteria 2 • Progressive neuropsychiatric disorder of a duration of > 6 months • Where routine investigations do not suggest alternative diagnosis • Where there is no history of iatrogenic exposure
Plus A tonsil biopsy positive for Prion protein
Possible • Progressive neuropsychiatric disorder of a duration of > 6 months • Where routine investigations do not suggest alternative diagnosis • No history of iatrogenic exposure
Plus 4 of the 5 symptoms under criteria 1 Plus EEG does not show typical appearance of sporadic CJD or none has been performed.
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 17 of 18 30/11/2010
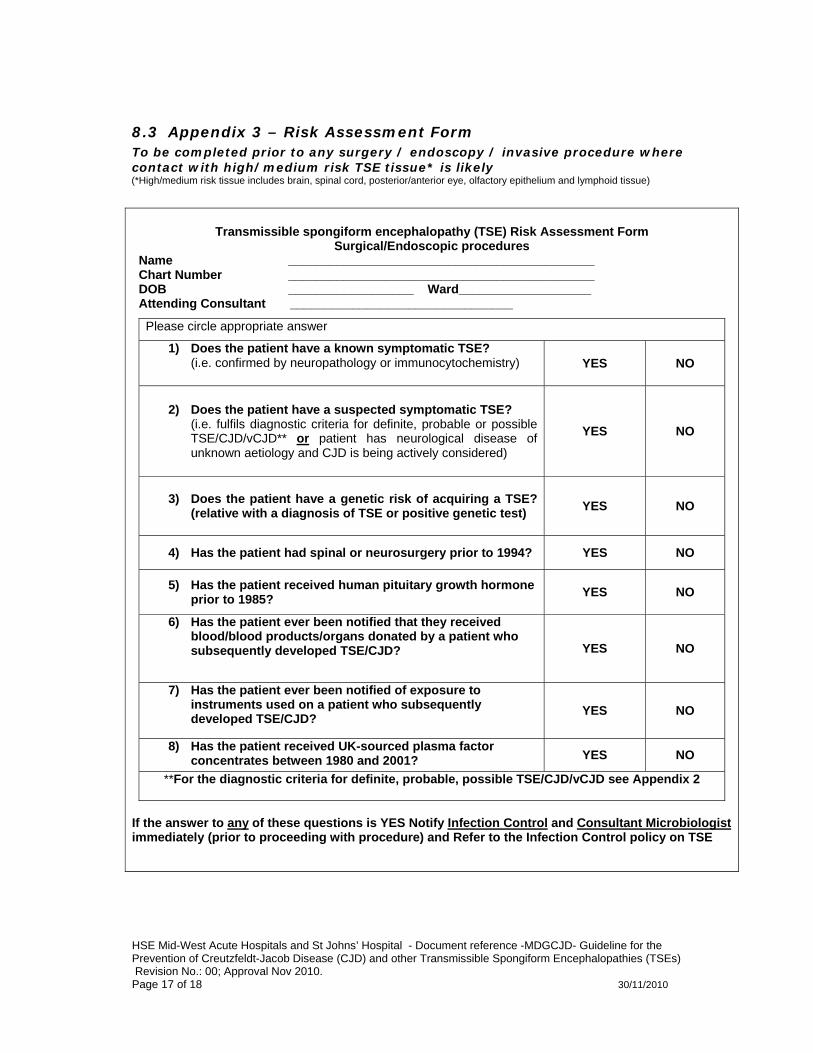
8.3 Appendix 3 – Risk Assessment Form To be completed prior to any surgery / endoscopy / invasive procedure where contact with high/medium risk TSE tissue* is likely
(*High/medium risk tissue includes brain, spinal cord, posterior/anterior eye, olfactory epithelium and lymphoid tissue)
Transmissible spongiform encephalopathy (TSE) Risk Assessment Form
Surgical/Endoscopic procedures Name ____________________________________________ Chart Number ____________________________________________ DOB __________________ Ward___________________ Attending Consultant ________________________________
Please circle appropriate answer
1) Does the patient have a known symptomatic TSE? (i.e. confirmed by neuropathology or immunocytochemistry)
YES
NO
2) Does the patient have a suspected symptomatic TSE? (i.e. fulfils diagnostic criteria for definite, probable or possible TSE/CJD/vCJD** or patient has neurological disease of unknown aetiology and CJD is being actively considered)
YES
NO
3) Does the patient have a genetic risk of acquiring a TSE? (relative with a diagnosis of TSE or positive genetic test)
YES
NO
4) Has the patient had spinal or neurosurgery prior to 1994? YES NO
5) Has the patient received human pituitary growth hormone prior to 1985? YES NO
6) Has the patient ever been notified that they received blood/blood products/organs donated by a patient who subsequently developed TSE/CJD? YES NO
7) Has the patient ever been notified of exposure to instruments used on a patient who subsequently developed TSE/CJD? YES NO
8) Has the patient received UK-sourced plasma factor concentrates between 1980 and 2001? YES NO
**For the diagnostic criteria for definite, probable, possible TSE/CJD/vCJD see Appendix 2
If the answer to any of these questions is YES Notify Infection Control and Consultant Microbiologist immediately (prior to proceeding with procedure) and Refer to the Infection Control policy on TSE
HSE Mid-West Acute Hospitals and St Johns’ Hospital - Document reference -MDGCJD- Guideline for the Prevention of Creutzfeldt-Jacob Disease (CJD) and other Transmissible Spongiform Encephalopathies (TSEs) Revision No.: 00; Approval Nov 2010. Page 18 of 18 30/11/2010
9 SIGNATURE SHEET Signature Sheet: I have read, understand and agree to adhere to the attached Policy, Procedure, Protocol or Guideline:
PRINTED NAME SIGNATURE AREA OF WORK DATE