classification and diagnosis of headache disorders
TRANSCRIPT

HdtsamOt(egbbwgih�3ub
hhm
Seminars in Pain Medicine Vol. 2 No. 2 2004
Classification and Diagnosis of Headache Disorders
DAVID M. BIONDI, DO
ABSTRACT
Headache is a common medical condition often associated with high personal andsocioeconomic burdens. Before 1988, there were no internationally accepted means bywhich to identify, classify, and study the hundreds of different headache syndromespresenting to the medical community for evaluation. With the introduction of theInternational Classification of Headache Disorders (ICHD) in 1988, a system forheadache classification became available that has standardized headache diagnosis foruse in research and clinical practice. The second edition of the ICHD (ICHD-II) waspublished in 2004 and has introduced important revisions to the classification schemabased on our growing understanding of the many headache types found in the generalpopulation and their pathogenesis. General principles related to the clinical evaluationand diagnostic classification of headache disorders using the ICHD-II are reviewed inthis article.Key words: ICHD, headache, migraine, classification, diagnosis.
bbaaahhsahatmscnpor
i
MN
Introduction
eadache of any etiology is a common medical con-ition with a high prevalence in the general popula-ion.1,2 In the United States, headache accounts foreveral million outpatient medical visits annuallynd over one million patient-days bedridden eachonth.3 Migraine, recognized by the World Healthrganization (WHO) as a highly disabling condi-
ion,4 has an annual prevalence of 12% to 13%18.2% for women and 6.5% for men), affecting anstimated 31 million people in the USA alone.5 Mi-raine is a public health concern that in the USA haseen associated with annual economic losses in theillions of dollars from missed workdays, reducedork productivity, and direct medical costs.3,6 Mi-
raine’s worldwide prevalence and socioeconomicmpact are equally impressive.2,7,8 Chronic dailyeadache, a condition defined by the occurrence of15 headache-days per month, is estimated to affect
% to 5% of the world’s population,9-12 and carriesnknown but predictably large societal and financialurdens.There are literally hundreds of potential causes for
ead and face pain. Pain-sensitive structures of theead include the scalp tissues, peripheral nerves,
uscles, periosteum, dural linings of the brain, and54
oth intracranial and extracranial blood vessels. Therain parenchyma itself is insensate. Primary head-che disorders are those that are not attributable ton identifiable structural or disease-related etiologynd include the diagnostic categories of tension-typeeadache, migraine, and cluster headache. Primaryeadaches are defined by their presenting signs andymptoms. In the general population, the most prev-lent primary headache disorder is tension-typeeadache, but migraine is the most prevalent dis-bling primary headache disorder. Presumably dueo its associated disability, migraine is the most com-
on primary headache disorder among patients pre-enting to an outpatient medical setting with a chiefomplaint of headache or admit to experiencing sig-ificant headaches when questioned.13 Treatment ofrimary headache disorders has improved greatlyver the last two decades as pre-clinical and clinicalesearch continues to define the pathogenesis and
From the Headache Management Program, Spaulding Rehabil-tation Hospital, Harvard Medical School, Boston, MA.
Address reprint requests to David M. Biondi, DO, Headacheanagement Program, Spaulding Rehabilitation Hospital, 125ashua Street, Boston, MA 02114. E-mail: [email protected]© 2004 Elsevier Inc. All rights reserved.1537-5897/04/0202-0002/$30.00/0
doi:10.1016/j.spmd.2004.03.002
satmotroScdp
tdSpHeeclIuc(dcfishsndaIscwdiahs
mnihcga
aatdmb
H
fttlost
11
111
Headache Disorders ● David M. Biondi 55
pecific treatments for each headache type. Second-ry headache disorders are those that are attributedo another condition, underlying structural abnor-
ality, or disease process, and include a broad rangef conditions such as headaches associated with in-racranial tumor, blood vessel abnormalities, hemor-hage, infection, trauma, medication, metabolic dis-rder, or other systemic medical conditions.econdary headaches are defined by their etiologicause and treatments are specifically targeted to ad-ress that cause as well as to provide symptomaticain relief.
Headache Classification and Diagnosis
Prior to 1988 there were no systematic or interna-ionally recognized criteria for the evaluation andiagnosis of headaches. The Headache Classificationubcommittee of the International Headache Societyublished the first International Classification ofeadache Disorders (ICHD) in 1988.14 The second
dition of the ICHD (ICHD-II) was published inarly 2004.15 The diagnostic criteria and headachelassifications are based on clinical and epidemio-ogic research as well as expert consensus. TheCHD-II has been recognized by the WHO and wassed as a basis for coding headache diagnoses in-luded in the International Classification of DiseasesICD-10). The ICHD-II uses a hierarchical systemivided into three parts. The first part has four majorategories of primary headache disorders subclassi-ed into a total of 57 subtypes and subforms. Theecond part has 8 major categories of secondaryeadache disorders subclassified into a total of 152ubtypes and subforms. The third part defines cranialeuralgias, facial pain, and other headaches yet to beefined. The major categories of headache disordersnd some of the common subtypes defined in theCHD-II are presented in Table 1. Although all clas-ification systems have limitations when applied tolinical practice, the ICHD-II provides a tool byhich headaches can be diagnosed, studied, andiscussed in a consistent manner throughout the
nternational research and academic community. Itlso provides a thoughtfully devised framework foreadache diagnosis in the medical office or clinicetting.
Since the introduction of the ICHD, the conduct ofost headache research includes this system’s diag-
ostic criteria in order to provide consistency in thedentification and classification of the many differenteadache disorders being studied in laboratories andlinics around the world. Having a common lan-uage and terminology has led to an acceleration of
dvancements in research regarding headache mech- lnisms and type-specific headache treatments. Withn improved understanding of characteristics specifico a headache type, deriving an accurate headacheiagnosis can and has substantially improved treat-ent outcomes through mechanism- and evidence-
ased treatment strategies.
The Headache Evaluation
eadache History
Although secondary headache disorders accountor only a small proportion of headache presenta-ions in the outpatient setting,2 the medical evalua-ion must first exclude these potentially serious orife-threatening conditions. The patient’s descriptionf his or her pain characteristics and associatedymptoms together with the clinician’s assessment ofhe patient’s physical examination and appropriate
Table 1. International Classification of HeadacheDisorders (not inclusive of all subtypes and subforms)15
1. Migraine1.1. Migraine without aura (previously used term: common
migraine)1.2. Migraine with aura (previously used term: classic
migraine)2. Tension-type headache
2.1. Infrequent episodic tension-type headache2.2. Frequent episodic tension-type headache2.3. Chronic tension-type headache
3. Cluster headache and other trigeminal autonomiccephalalgias3.1. Cluster3.1.1. Episodic cluster headache3.1.2. Chronic cluster headache
4. Other primary headaches5. Headache attributed to head and/or neck trauma6. Headache attributed to cranial or cervical vascular disorder7. Headache attributed to nonvascular intracranial disorder
7.1. Headache attributed to high cerebrospinal fluidpressure
7.2. Headache attributed to low cerebrospinal fluidpressure
7.3. Headache attributed to noninfectious inflammatorydisease
7.4. Headache attributed to intracranial neoplasm8. Headache attributed to a substance or its withdrawal
8.1. Headache induced by acute substance use or exposure8.2. Medication overuse headache (MOH)
9. Headache attributed to infection0. Headache attributed to disorder of homeostasis1. Headache or facial pain attributed to disorder of the
cranium, neck, eyes, ears, nose, sinuses, teeth, mouth, orother facial or cranial structures
2. Headache attributed to psychiatric disorder3. Cranial neuralgias and central causes of facial pain4. Other headache, cranial neuralgia, or central or primary
facial pain
aboratory testing are needed to formulate an accu-

ratqdhttoTbdt
hfiabdcputuopntta
sapeotlttacmrtmmtiiosaiiashsgmthotcad
A
B
C
D
E
F
G
H
56 Seminars in Pain Medicine Vol. 2 No. 2 June 2004
ate headache diagnosis. A comprehensive medicalnd headache history is an essential component ofhe headache evaluation. Because the attack fre-uency, temporal profiles, and associated symptomsefine the various headache disorders, a detailedeadache history is required. Components of a de-
ailed headache history modeled after the informa-ion needed to establish a headache diagnosis basedn the ICHD diagnostic criteria are presented inable 2. A headache questionnaire can be completedy the patient prior to the physician’s evaluation, butirect questioning of the patient is often very useful
Table 2. Headache History
. Initial headache presentation and progression1. Acute, fulminant, or cataclysmic2. Subacute or gradual3. Chronic or protracted4. Paroxysmal5. Cyclic6. Prodromal symptoms or neurologic aura7. Any precipitating event, illness, or activity
. Pain location1. Generalized, holocephalic2. Unilateral with or without side shift3. Focal or discretely localized4. Bilateral or band-like
. Pain expression1. Intermittent
(a) Frequency(b) Duration
2. Constant3. Intensity (mild, moderate, severe)
(a) Level of disability. Pain quality
1. Throbbing, pounding2. Squeezing, vise-like, tightening, pressure3. Boring, drilling, knife-like4. Jabbing, jolting, shock-like, shooting5. Burning, searing
. Associated signs and symptoms1. Nausea, vomiting, diarrhea2. Photophobia, phonophobia, osmophobia3. Paresthesia, numbness4. Scalp sensitivity5. Muscle weakness
(a) Focal(b) Generalized
6. Dizziness, vertigo, dysequilibrium7. Blurred vision, visual scotoma, diplopia, visual field cuts8. Cognitive dysfunction, language disturbances, confusion,
altered consciousness9. Autonomic signs
(a) Lacrimation, rhinorrhea nasal congestion, miosis,mydriasis, flushing, diaphoresis, blood pressurealterations, syncope
. Diurnal, weekly, monthly, or annual headache cycles orpatterns
. Headache triggers, exacerbating factors, and amelioratingfactors
. Family headache history
o identify small nuances and unusual features of the b
eadache presentation often missed on a structuredorm. Associated symptoms and signs that are atyp-cal of ICHD-defined primary headache disordersnd a progressively worsening clinical course oftenetray the diagnosis of secondary headache disor-ers. When a secondary headache disorder is ex-luded through proper investigation, the search for arimary headache diagnosis can proceed. It is notnusual for a patient to experience more than oneype of primary headache disorder. The evaluationsually proceeds by focusing on the headache that isf most concern to the patient, but all headacheresentations merit further examination with diag-oses ascribed to each. Asking the patient to main-
ain a detailed headache diary can be an invaluableool for confirming a provisional or uncertain head-che diagnosis.Initial headache presentation and headache progres-
ion. Factors inciting or initiating recurrent head-ches, the temporal pattern of individual attacks, androgression of attack patterns over time can providessential information regarding a headache’s etiol-gy. Recurrent or chronic headaches beginning forhe first time in patients �50 years of age are moreikely attributable to an underlying condition such asumor or temporal arteritis, and therefore patients inhis age group will usually require closer medicalttention. Headaches that begin during or after exer-ise, Valsalva, sexual intercourse, or head injuryight be associated with intracranial hemorrhage or
elated to an abnormality at the craniocervical junc-ion such as a Chiari malformation. Physical exertion
ight also incite primary headache disorders such asigraine or benign exertional headache. Headache
hat has a sudden onset and is immediately at max-mal pain intensity is of concern for the possibility ofntracranial hemorrhage from a ruptured aneurysmr arteriovenous malformation (AVM). Headache as-ociated with apoplexy of the pituitary can also havecataclysmic onset. Severe headaches that begin dur-
ng pregnancy and postpartum can be related tontracranial venous thrombosis, especially if associ-ted with altered consciousness or focal neurologicigns. Head pain referred from the neck (cervicogeniceadache) can begin after neck injury associated withports, motor vehicle accidents, or a fall. Subacute orradual headache progression over hours to weeksight be indicative of a subdural hematoma, infec-
ion, or vasculitis. A chronic progressive or protractedeadache course might suggest an intracranial tumorr metabolic disorder. This pattern can also indicateransformation of intermittent to chronic migraineatalyzed by medication overuse. Paroxysmal head-che attacks can describe several primary headacheisorders such as migraine or cluster but might also
e associated with cerebral ischemia or epilepsy. A
cloiia
sMidaaibelsstpai
tdhae3Trt2Sstm
mimtaiDcppesstov
chmFhsphsoaornnlsdcnwcCtm
cmppatuonoaafkfiahtusnpwtwosp
Headache Disorders ● David M. Biondi 57
yclic headache pattern can describe hormonally re-ated migraine attacks but it is a classic presentationf cluster. Headaches that occur during sleep can
nclude cluster and migraine, but can also suggest anntracranial tumor or headache associated with sleeppnea or excessive snoring.Head pain location. Alternating hemicrania or side
hift during a headache attack is typical of migraine.igraine pain can also be holocephalic or occipital
n its location. Neck pain is very commonly reporteduring migraine attacks. Cluster headache is invari-bly unilateral without side shift and is locatedround the orbit or temple. Focal or discretely local-zed pain without change in the site affected mighte indicative of a fixed intracranial lesion or periph-ral nerve injury in the scalp or upper neck. Side-ocked head pain with predominant neck pain isuggestive of cervicogenic headache. Bilateral pres-ure or band-like headache is a common presenta-ion for tension-type headache, but, if persistent orrogressive, might be indicative of headache associ-ted with elevated cerebrospinal fluid pressure or anntracranial mass.
Pain duration and attack frequency. Episodic tension-ype headaches have durations of 30 minutes to 7ays. Episodic migraine attacks last from 4 to 72ours. Cluster attacks last from 15 to 180 minutesnd occur at a frequency of one every other day up toight per day. Paroxysmal hemicrania attacks last 2 to0 minutes and occur more than five times per day.he SUNCT syndrome (short-lasting, unilateral, neu-algiform headache with conjunctival injection andearing) is defined by attacks lasting between 5 and40 seconds that occur from 3 to 200 times per day.econdary headache disorders usually do not have atereotypic time course or diurnal frequency owingo the wide variability of etiologies and pathogenic
echanisms.Pain quality. Tension-type headache has a mild tooderate pain intensity and is described as squeez-
ng, band-like, or vise-like. Migraine most often has aoderate to severe pain intensity and is described as
hrobbing, pounding, or jabbing. Migraine mightlso be described as constant with a sensation ofntense pressure: “like my head is going to explode.”rilling or boring are terms often used to describe
luster headaches. Many patients will describe theain as “a hot poker jammed into my eye.” Burningain is sometimes used to describe cluster or well-stablished migraine, but is more commonly a de-criptor for a cranial neuralgia. Pain associated withecondary headache disorders, such as intracranialumor, infection, or psychiatric conditions, is mostften holocephalic in location, constant in duration,
ariable in pain intensity, and progressive in course. oSymptoms associated with headache. Symptoms asso-iated with headache are a very important part of theeadache history because they are the features thatost often raise suspicion for underlying pathology.
ixed or long-lasting (�1 hour) neurologic deficits,emiplegia, confusion, diplopia, alterations of con-ciousness, and seizures are rare accompaniments ofrimary headache disorders and suggest a secondaryeadache disorder. Nausea, vomiting, and hypersen-itivity to sensory stimuli such as light, sound, ordors are common features of migraine. Protractednd projectile vomiting suggests intracranial pathol-gy and elevated intracranial pressure. Cluster andelated forms of hemicrania are associated with cra-ial parasympathetic symptoms such as lacrimation,asal congestion, rhinorrhea, and face sweating ipsi-
ateral to the side of head pain. High blood pressure,low pulse rate, and altered consciousness might in-icate elevated intracranial pressure due to an intra-ranial mass lesion or an obstruction of cerebrospi-al fluid (CSF) flow. Headache that is most severehen the patient is sitting or standing but dramati-
ally improves when supine suggests one of the lowSF pressure syndromes. Headache exacerbated by
he supine position, Valsalva, and physical exertionight indicate an elevated CSF pressure syndrome.Other information from headache history. In cases of
hronic headache, special attention is given to theedication history, because new medications, both
rescribed and over-the-counter (OTC), taken by theatient for a coexisting condition, can cause head-che as a side effect or interfere with other headachereatments. A complete medication history is partic-larly important in migraineurs because the overusef migraine-specific medications (5-HT1B/D ago-ists, ergotamine derivatives) and analgesics (opioidr nonopioid, prescribed or OTC), even if taken fornother medical condition, has been found to causeprogressive worsening of headache intensity and
requency in some patients, a condition commonlynown as “analgesic rebound headaches” and classi-ed in the ICHD-II as “medication overuse head-che” (MOH).16-19 Migraineurs are recognized toave common or predictable triggers such as emo-
ional or physical stress, missed meals, alterations insual sleep patterns, weather changes, humidity, andtrong sensory stimuli, including bright light, glare,oise, or perfume scents. Menstrual-associated andharmacologically induced hormonal changes areell-known migraine triggers for women. Cluster at-
acks are invariably triggered by alcohol ingestionhile a patient is in an attack cycle. Headaches mightccur after taking certain prescribed medicationsuch as nitrates, calcium channel blockers, antide-ressants, or insulin, among many others. Caffeine
veruse (�200 mg per day) is suspected to be an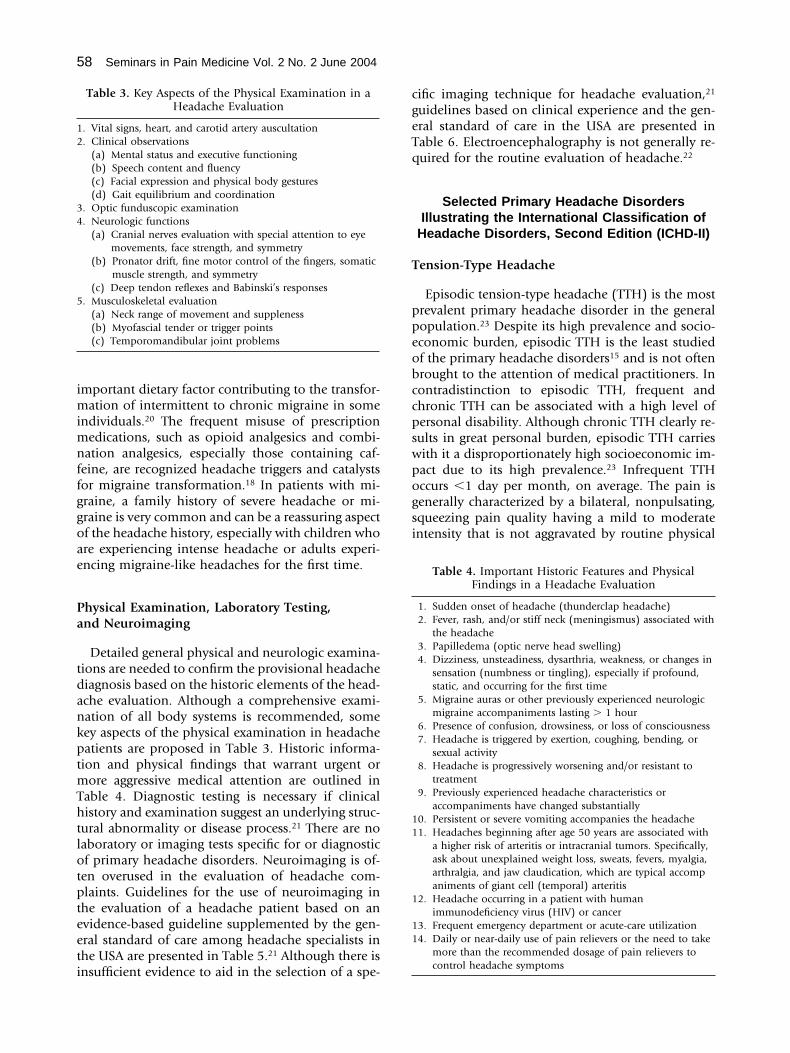
imimnffggoae
Pa
tdankptmThtlotpteeti
cgeTq
T
ppeobccpswpogsi
12
34
5
11
1
11
58 Seminars in Pain Medicine Vol. 2 No. 2 June 2004
mportant dietary factor contributing to the transfor-ation of intermittent to chronic migraine in some
ndividuals.20 The frequent misuse of prescriptionedications, such as opioid analgesics and combi-
ation analgesics, especially those containing caf-eine, are recognized headache triggers and catalystsor migraine transformation.18 In patients with mi-raine, a family history of severe headache or mi-raine is very common and can be a reassuring aspectf the headache history, especially with children whore experiencing intense headache or adults experi-ncing migraine-like headaches for the first time.
hysical Examination, Laboratory Testing,nd Neuroimaging
Detailed general physical and neurologic examina-ions are needed to confirm the provisional headacheiagnosis based on the historic elements of the head-che evaluation. Although a comprehensive exami-ation of all body systems is recommended, someey aspects of the physical examination in headacheatients are proposed in Table 3. Historic informa-ion and physical findings that warrant urgent or
ore aggressive medical attention are outlined inable 4. Diagnostic testing is necessary if clinicalistory and examination suggest an underlying struc-
ural abnormality or disease process.21 There are noaboratory or imaging tests specific for or diagnosticf primary headache disorders. Neuroimaging is of-en overused in the evaluation of headache com-laints. Guidelines for the use of neuroimaging inhe evaluation of a headache patient based on anvidence-based guideline supplemented by the gen-ral standard of care among headache specialists inhe USA are presented in Table 5.21 Although there is
Table 3. Key Aspects of the Physical Examination in aHeadache Evaluation
. Vital signs, heart, and carotid artery auscultation
. Clinical observations(a) Mental status and executive functioning(b) Speech content and fluency(c) Facial expression and physical body gestures(d) Gait equilibrium and coordination
. Optic funduscopic examination
. Neurologic functions(a) Cranial nerves evaluation with special attention to eye
movements, face strength, and symmetry(b) Pronator drift, fine motor control of the fingers, somatic
muscle strength, and symmetry(c) Deep tendon reflexes and Babinski’s responses
. Musculoskeletal evaluation(a) Neck range of movement and suppleness(b) Myofascial tender or trigger points(c) Temporomandibular joint problems
nsufficient evidence to aid in the selection of a spe-
ific imaging technique for headache evaluation,21
uidelines based on clinical experience and the gen-ral standard of care in the USA are presented inable 6. Electroencephalography is not generally re-uired for the routine evaluation of headache.22
Selected Primary Headache DisordersIllustrating the International Classification of
Headache Disorders, Second Edition (ICHD-II)
ension-Type Headache
Episodic tension-type headache (TTH) is the mostrevalent primary headache disorder in the generalopulation.23 Despite its high prevalence and socio-conomic burden, episodic TTH is the least studiedf the primary headache disorders15 and is not oftenrought to the attention of medical practitioners. Inontradistinction to episodic TTH, frequent andhronic TTH can be associated with a high level ofersonal disability. Although chronic TTH clearly re-ults in great personal burden, episodic TTH carriesith it a disproportionately high socioeconomic im-act due to its high prevalence.23 Infrequent TTHccurs �1 day per month, on average. The pain isenerally characterized by a bilateral, nonpulsating,queezing pain quality having a mild to moderatentensity that is not aggravated by routine physical
Table 4. Important Historic Features and PhysicalFindings in a Headache Evaluation
1. Sudden onset of headache (thunderclap headache)2. Fever, rash, and/or stiff neck (meningismus) associated with
the headache3. Papilledema (optic nerve head swelling)4. Dizziness, unsteadiness, dysarthria, weakness, or changes in
sensation (numbness or tingling), especially if profound,static, and occurring for the first time
5. Migraine auras or other previously experienced neurologicmigraine accompaniments lasting � 1 hour
6. Presence of confusion, drowsiness, or loss of consciousness7. Headache is triggered by exertion, coughing, bending, or
sexual activity8. Headache is progressively worsening and/or resistant to
treatment9. Previously experienced headache characteristics or
accompaniments have changed substantially0. Persistent or severe vomiting accompanies the headache1. Headaches beginning after age 50 years are associated with
a higher risk of arteritis or intracranial tumors. Specifically,ask about unexplained weight loss, sweats, fevers, myalgia,arthralgia, and jaw claudication, which are typical accompaniments of giant cell (temporal) arteritis
2. Headache occurring in a patient with humanimmunodeficiency virus (HIV) or cancer
3. Frequent emergency department or acute-care utilization4. Daily or near-daily use of pain relievers or the need to take
more than the recommended dosage of pain relievers tocontrol headache symptoms

amipqheow
2D
A
BC
D
E
M
raMTfaawpcmanoTmhmctmnlfpesrs
A
B
C
N(
C(
M(
(
(
(
Headache Disorders ● David M. Biondi 59
ctivity. Episodic TTH episodes can last from 30inutes to 7 days. Nausea and vomiting are absent
n episodic TTH. Associated symptoms can includehotophobia or phonophobia, but not both. Fre-uent TTH is defined by episodes of �1 but �15eadache-days per month. It has all other features ofpisodic TTH. Headache episodes of chronic TTHccur �15 days per month and may be associatedith mild nausea.
.1. Infrequent episodic tension-type headache15
iagnostic criteria:
. At least 10 episodes occurring on �1 day per month, onaverage (�12 days per year) and fulfilling criteria B-D.
. Headache lasting from 30 minutes to 7 days.. Headache has at least two of the following characteristics:
1. Bilateral location.2. Pressing/tightening (nonpulsating) quality.3. Mild or moderate intensity.4. Not aggravated by routine physical activity such as walking
or climbing stairs.
. Both of the following:1. No nausea or vomiting (anorexia may occur).2. No more than one of photophobia or phonophobia.
Table 5. Guidelines for Neuroimaging in the Evaluationof Headache
. Urgent neuroimaging recommended(1) Thunderclap or abrupt onset headache with abnormal
neurologic exam(2) Headache associated with seizure or altered
consciousness(3) Prior to lumbar puncture in situations where headache
is accompanied by:• Signs of increased intracranial pressure• Fever and nuchal rigidity• Localizing neurologic signs
. Neuroimaging generally recommended(1) Isolated or first-time “thunderclap” headache without
focal neurologic exam(2) Significant change in previous headache characteristics
or progressive worsening of headache pattern overhours, days, or weeks
(3) Predominant occipitonuchal headache(4) New onset of or change in previous headache
characteristics in an older individual(5) Headache accompanied by abnormal neurologic
examination, including papilledema, unilateral loss ofsensation, weakness, hyperreflexia, or dysequilibrium
(6) New onset headache in patient who:• Is HIV positive or immunocompromised• Has a prior diagnosis of cancer• Is in a population at high risk for intracranial disease
. Neuroimaging generally not required(1) Migraine with normal neurologic examination(2) Recurrent migraine attacks with stable and stereotypic
presentations(3) Tension-type headache with normal neurologic
examination(4) Other headaches with normal neurologic examination
. Not attributed to another disorder.
igraine
Migraine without aura is a highly prevalent, neu-ologic disorder, most commonly characterized byttacks of intense head pain lasting 4 to 72 hours.5
igraine is three times more prevalent in women.he head pain of migraine is classically unilateral,rontotemporal in location, throbbing in quality,nd moderate to severe in intensity. The pain canlternate sides from attack to attack or shift sidesithin an attack. The pain is aggravated by routinehysical activity. Migraine is also defined by its asso-iated features, which include sensitivity to environ-ental stimuli, nausea, and vomiting. Migraine with
ura differs only by the presence of reversible focaleurologic symptoms that usually develop graduallyver 5 to 20 minutes and resolve within 60 minutes.he aura can precede the onset of headache by asuch as 60 minutes or can occur concurrently with
eadache onset. Aura can occasionally occur after theigraine headache is well established. Typical aura is
haracterized by visual, sensory, and speech symp-oms singly or in any combination. The aura of
igraine is usually a mix of positive and negativeeurologic features such as scintillating scotoma fol-
owed by visual obscurations or sensory paresthesiaollowed by numbness. Migraine aura is a graduallyrogressive event typified by a march of sensory par-sthesia moving up an arm or visual fortificationpectra moving across a visual field that completelyesolves in the area or region first affected. Aura-likeymptoms can be caused by vascular malformations,
Table 6. Guidelines for the Selection of DiagnosticNeuroimaging (CT versus MRI)
oncontrast computerized tomography (CT)1) Recommended when urgent neuroimaging is necessary in
cases of:(a) Suspected intracranial hemorrhage(b) Suspected elevated intracranial pressure or focal
neurologic deficit before lumbar puncture(c) Headache associated with neurologic accompaniments(d) Headache presenting with a substantial change in
previously experienced headache characteristicsontrast-enhanced CT
1) Recommended if abnormality is found on noncontrast CT,or a vascular abnormality or tumor are suspected and anurgent evaluation is necessary.
agnetic resonance imaging (MRI)1) Recommended as an initial or urgent diagnostic
examination if there is suspicion of venous sinusthrombosis or vasculitis
2) Recommended when an abnormality is suspected in theposterior cranial fossa or at the craniocervical junction
3) Recommended when an aneurysm or vascularmalformation is suspected; evaluated with magneticresonance angiography (MRA)
4) If an abnormality is detected on CT, MRI may furtherdefine the abnormality

tdo“tttmwoodpmTeaaaag
1D
AB
C
D
E
1D
AB
C
D
E
C
ctoawccebesspwuTntssDww
3D
AB
C
D
E
3D
AB
60 Seminars in Pain Medicine Vol. 2 No. 2 June 2004
umors, ischemia, and epilepsy, but these are oftenefined by a very short or long duration (�5 minutesr �1 hour), lack of the characteristic progression ormarch” of symptoms, dense neurologic deficits, al-ered levels of consciousness, and abnormalities onhe neurologic examination, thereby differentiatinghem from migraine aura. Status migrainosus is a
igraine attack lasting �72 hours and associatedith intense pain and disability. The migraine istherwise typical of episodic migraine attacks previ-usly experienced by the patient. Chronic migraine isefined by migraine headache occurring �15 dayser month for at least 3 months in the absence ofedication overuse or other underlying condition.
he majority of chronic migraines transform frompisodic over a period of months to years, somessociated with medication overuse, whereas othersre not.10,24 As migraine becomes chronic, it is char-cterized by features of chronic tension-type head-che punctuated by intermittent migraine or mi-raine-like attacks.
.1. Migraine without aura15
iagnostic criteria:
. At least five attacks fulfilling criteria B-D.
. Headache attacks lasting 4 to 72 hours (untreated or unsuc-cessfully treated).
. Headache has at least two of the following characteristics:1. Unilateral location.2. Pulsating quality.3. Moderate or severe pain intensity.4. Aggravation by or causing avoidance of routine physical
activity (e.g., walking or climbing stairs).
. During headache there is at least one of the following:1. Nausea and/or vomiting.2. Photophobia and phonophobia.
. Headache is not attributed to another disorder.
.2.1. Typical aura with migraine headache15
iagnostic criteria:
. At least two attacks fulfilling criteria B-D.
. Aura consisting of at least one of the following but no motorweakness:1. Fully reversible visual symptoms including positive features
(eg, flickering lights, spots, or lines) and/or negative fea-tures (ie, loss of vision).
2. Fully reversible sensory symptoms including positive fea-tures (ie, pins and needles) and/or negative features (ie,numbness).
3. Fully reversible dysphasic speech disturbances.
. At least two of the following:1. Homonymous visual symptoms and/or unilateral sensory
symptoms.2. At least one aura symptom develops gradually over �5
minutes and/or different aura symptoms occur in succes-sion over �5 minutes.
3. Each symptom lasts �5 minutes and �60 minutes.
. Headache fulfilling criteria B-D for “1.1. Migraine withoutaura” begins during the aura or follows aura within 60 min-utes.
. Not attributed to another disorder.
luster
Cluster is less prevalent than migraine but is asso-iated with a high level of disability because of mul-iple daily attacks of severe pain, many of whichccur during and interrupt sleep.26 Men are affectedpproximately four times more commonly thanomen. Episodic cluster occurs in recurrent attack
ycles lasting from 2 weeks to 3 months. When inycle, attacks can occur from once every other day toight per day. The attacks of cluster are characterizedy severe or extremely severe pain occurring unilat-rally in the orbital or temporal regions. The pain istrictly unilateral during an attack and rarely shiftsides from cycle to cycle. Attacks tend to “cluster” atredictable times during the day and classically occurithin 60 to 120 minutes of initiating sleep. Individ-al attacks last from 15 to 180 minutes in duration.he hallmark of cluster is the association of promi-ent cranial parasympathetic autonomic features
hat include lacrimation, conjunctival injection, na-al congestion, rhinorrhea, eyelid swelling, facialweating, miosis, and ptosis ipsilateral to the pain.uring the attack, the patient is restless and agitated,hich is in contradistinction to the migraine patientho prefers to be calm and motionless.
.1 Cluster headache15
iagnostic criteria:
. At least five attacks fulfilling criteria B-D.
. Severe or very severe unilateral orbital, supraorbital and/ortemporal pain lasting 15 to 180 minutes if untreated.
. Headache is accompanied by at least one of the following:1. Ipsilateral conjunctival injection and/or lacrimation.2. Ipsilateral nasal congestion and/or rhinorrhea.3. Ipsilateral eyelid edema.4. Ipsilateral forehead and facial sweating.5. Ipsilateral miosis and/or ptosis.6. A sense of restlessness or agitation.
. Attacks have a frequency from one every other day to eight perday.
. Headaches not attributed to another disorder.
.1.1. Episodic cluster headache15
iagnostic criteria:
. Attacks fulfilling criteria A-E for “3.1. Cluster headache.”
. At least two cluster periods lasting 3 to 365 days and separated
by pain-free remission periods of �1 month.
3D
AB
fTdadichsicie
Headache Disorders ● David M. Biondi 61
.1.2. Chronic cluster headache15
iagnostic criteria:
. Attacks fulfilling criteria A-E for “3.1. Cluster headache.”
. Attacks recur over �1 year without remission periods or withremission periods lasting �1 month.
Summary
Headache is a common medical complaint havingar reaching personal and socioeconomic burdens.he International Classification of Headache Disor-ers has provided a systematic approach for the di-gnosis of over 200 primary and secondary headacheisorders. The initial goal of the medical practitioner
s to exclude potentially serious or life-threateningonditions causing headache. Once a secondaryeadache is excluded, the focus is to then identify apecific primary headache disorder. Having the abil-ty to derive an accurate diagnosis using the ICHDan result in improved treatment outcomes by allow-ng the application of type-specific mechanism- andvidence-based headache treatment strategies.
References
1. Rasmussen BK: Epidemiology of headache. Cepha-lalgia 21:774-777, 2001
2. Rasmussen BK, Jensen R, Schroll M, et al: Epidemi-ology of headache in a general population—a prev-alence study. J Clin Epidemiol 44:1147-1157, 1991
3. Hu XH, Markson Le, Lipton RB, et al: Burden ofmigraine in the United States: disability and eco-nomic costs. Arch Intern Med 159:813-818, 1999
4. Menken M, Munsat TL, Toole JF: The global burdenof disease study. Arch Neurol 57:418-420, 2000
5. Lipton RB, Stewart WF, Diamond S, et al: Prevalenceand burden of migraine in the United States: datafrom the American Migraine Study II. Headache41:646-657, 2001
6. Osterhaus JT, Gutterman DL, Plachetka JR: Health-care resource and lost labor costs of migraine head-ache in the US. Pharmacoeconomics 2:67-76, 1992
7. Edmeads J, Mackell JA: The economic impact ofmigraine: an analysis of direct and indirect costs.Headache 42:501-509, 2002
8. Gerth WC, Carides GW, Dasbach EJ, et al: The mul-tinational impact of migraine symptoms on health-care utilization and work loss. Pharmacoeconomics19:197-206, 2001
9. Scher AI, Lipton RB: The frequent headache epide-miology (FrHE) study. Pain 16:81-89, 2003
10. Scher AI, Stewart WF, Liberman J, et al: Prevalence
of frequent headache in a population sample. Head-ache 38:497-506, 1998
11. Castillo J, Munoz P, Guitera V, et al: Epidemiologyof chronic daily headache in the general population.Headache 39:190-196, 1999
12. Ravishankar K: Headache pattern in India-a head-ache clinic analysis of 1000 patients. Cephalalgia17:316-317, 1997
13. Dowson A: Landmark study. Cephalalgia 22:590,2002
14. Headache Classification of the International Head-ache Society: Classification and diagnostic criteriafor headache disorders, cranial neuralgias and facialpain. Cephalalgia 8:1-96, 1988 (suppl 7)
15. Headache Classification of the International Head-ache Society: The International Classification ofHeadache Disorders, 2nd edition. Cephalalgia 24:1-160, 2004 (suppl 1)
16. Rapoport AM, Stang P, Gutterman DL, et al: Anal-gesic rebound headache in clinical practice: datafrom a physician survey. Headache 36:14-19, 1996
17. Schneider P, Aull S, Baumgartner C, et al: Long-termoutcome of patients with headache and drug abuseafter inpatient withdrawal: five-year follow-up.Cephalalgia 16:481-485, 1996
18. Fritsche G, Eberl A, Katasarava Z, et al: Drug-in-duced headache: long-term follow-up of withdrawaltherapy and persistence of drug misuse. Eur Neurol45:229-235, 2001
19. Pini LA, Cicero AF, Sandrini M: Long-term fol-low-up of patients treated for chronic headache withanalgesic overuse. Cephalalgia 21:878-883, 2001
20. Bigal ME, Sheftell FD, Rapoport AM, et al: Chronicdaily headache: identification of factors associatedwith induction and transformation. Headache 42:575-581, 2002
21. Frishberg B, Rosenberg JH, Matchar DB, et al: Evi-dence-based guidelines in he primary care setting:neuroimaging in patients with nonacute headache.http://www.aan.com. Accessed March 13, 2004
22. American Academy of Neurology Practice Parame-ter. The electroencephalogram in the evaluation ofheadache. Neurology 45:1411-1413, 1995
23. Schwartz BS, Stewart WF, Simon D, et al: Epidemi-ology of tension-type headache. JAMA 279:381-383,1998
24. Diener HC, Dahlof CGH: Headache associated withchronic use of substances, in Olesen J, Tfelt-HansenP, Welsh KMA (eds): The Headaches (ed 2). Phila-delphia, Lippincott Williams & Wilkins, 2000, pp871-878
25. Swanson JW, Yanagihara T, Stang PE, et al: Inci-dence of cluster headaches: a population-basedstudy in Olmstead County, Minnesota. Neurology44:433-437, 1994
26. Finkel AG: Epidemiology of cluster headache. Curr
Pain Headache Rep 7:144-149, 2003