clinical case discussion on protease inhibitor treatment
TRANSCRIPT

Clinical case Discussion on Protease Inhibitor treatment in experienced
patients 2nd Global Workshop on HCV Therapy Advances
New Antivirals in Clinical Practice
G M Dusheiko
Royal Free Hospital London UK

Rationale for treatment with first generation protease inhibitors
• Progressive disease, associated with persistence of viral replication and ongoing necro-inflammation and fibrosis
– Remission (SVR) is associated with loss of active viral replication
– Improvement in hepatic fibrosis
– Probably equates to modification of natural history

The natural history of fibrosis in chronic
viral hepatitis
F0 F2 F3 F4
Courtesy Pierre Bedossa

What have we learned from clinical experience with the first generation PI’s
• Shortening of treatment to 24 weeks therapeutic
advance (naïve patients)
• High positive predictive value of > 90% in patients with RVR – important motivator
• Clinical experience with cirrhosis – tempered by the potential for serious adverse events
– Long duration of interferon treatment
• Management and intensive monitoring

The need to treat cirrhosis; balancing efficacy,
safety and likelihood of response
Patients with cirrhosis at greatest need
Response rates impaired in patients with cirrhosis
Response rates in genotype 1 naive and
experienced patients with cirrhosis improved by
first generation protease inhibitors

Question
You are given a restricted budget for treating non responders
Who would you prioritise:
– A. Prior IFN null responder without cirrhosis?
– B. Prior IFN partial responder without cirrhosis?
– C. Prior IFN relapser irrespective of fibrosis stage?
– D. Prior IFN null responder with cirrhosis
6

REALIZE (telaprevir): SVR by baseline fibrosis
stage and prior response to Peg-IFN/RBV
SVR was defined as HCV RNA <25 IU/mL at last observation within the Week 72 visit window. In
case of missing data, the last HCV RNA data point from Week 12 of follow-up onwards was used Pol S, et al. Hepatology 2011;54(Suppl. S1):374A
32
13 7
18
0
20
6 0
10
87 85 84 77
56
34 41 42
14
0
20
40
60
80
100
53/62 n/N= 2/15 12/38 145/167 10/18 0/5 3/17 36/47 16/38 0/9 1/5 11/32
No, minimal
or portal
fibrosis
Cirrhosis Stage
Pbo/PR48
Pooled T12/PR48
SV
R (
%)
48/57 1/15 1/18 24/59 1/10 7/50
Bridging
fibrosis
No, minimal
or portal
fibrosis
Cirrhosis Bridging
fibrosis
No, minimal
or portal
fibrosis
Cirrhosis Bridging
fibrosis
Prior
relapsers
Prior partial
responders
Prior null
responders

RESPOND-2 (boceprevir): SVR by baseline fibrosis
stage and prior response to Peg-IFN/RBV
Prior
relapsers
Prior partial
responders
Prior null
responders
32
20
9
0
75
50 47
30
75
83
55
46
0
20
40
60
80
100
2/10 n/N= 58/77 12/38 59/79 0/5 23/42 2/23 18/38 3/10 6/13
No, minimal
or portal
fibrosis
(F0–F2)
Stage
PR48
BOC RGT
SV
R (
%)
15/18 11/22
Bridging
fibrosis / cirrhosis
(F3/F4)
Excluded from
RESPOND-2
BOC44/PR48
No, minimal
or portal
fibrosis
(F0–F2)
Bridging
fibrosis / cirrhosis
(F3/F4)
Bruno S, et al. J Hepatol 2011;54(Suppl. 1):S4

Week 24 and end-of-treatment response for
DAA-based therapy in Veterans with chronic HCV
692/859 (81%) G1 Veterans had
ended therapy at analysis
532/661 BOC; 160/198 TVR
Backus L, et al. AASLD 2012, Boston, #LB-30
Week 24 and EOT virologic response rates
did not differ between DAAs
Cirrhotics had lower response than
non-cirrhotic
Prior null responders had lower response
rates
BOC
Wk 24 (n/N)
TVR
Wk 24 (n/N)
p-
value
Overall 69% (457/661) 64% (126/198) 0.15
Subgroups of interest:
Naive non-cirrhotic 74% (231/314) 60% (36/60) 0.03
All cirrhotic 64% (103/161) 60% (49/81) 0.60
Prior treatment response (including cirrhotic and non-cirrhotic):
Prior null responder 44% (28/64) 53% (20/38) 0.39
Prior partial responder 69% (50/72) 67% (18/27) 0.79
Prior relapser 76% (91/119) 88% (29/33) 0.15
HCV RNA undetectable rates at Week 24 (n=859)
HCV RNA undetectable rates at EOT (n=692) BOC EOT
(n/N)
TVR EOT
(n/N)
p-
value
Overall 60% (320/532) 55% (88/160) 0.25
Subgroups of interest:
Naive non-cirrhotic 66% (179/270) 60% (31/52) 0.35
All cirrhotic 49% (55/112) 45% (26/58) 0.60
Prior treatment response (including cirrhotic and non-cirrhotic):
Prior null responder 19% (9/48) 26% (8/31) 0.46
Prior partial responder 59% (32/54) 62% (13/21) 0.83
Prior relapser 67% (64/95) 85% (22/26) 0.08
Demographic and clinical data BOC TVR
Age (y) 57 ± 6 58 ± 5
Sex = male 95% 97%
Race/ethnicity
Black
Hispanic
White
25%
6%
60%
30%
6%
58%
Cirrhosis 24% 41%
Diabetes 23% 29%
Naive 59% 49%
Prior null responder 10% 19%
Prior partial responder 11% 14%
Prior relapser 18% 17%

Albumin and MELD score predict decompensation in patients
with HCV cirrhosis and thrombocytopenia on IFN therapy:
Analysis from the ENABLE studies
Afdhal N, et al. AASLD 2012, Boston, #1138
IFN therapy increases the risk of hepatic decompensation
MELD score and albumin are most robust indicators of
disease progression in multivariate analysis
Patients with decompensation rarely achieved SVR ≤10%
Compensated disease and
thrombocytopenia (<75,000/µL)
N=1439
955 IFN/RBV/eltrombopag
484 IFN/RBV/placebo
252 events
13% on eltrombopag
6% ascites; 3% hepatic encephalopathy
7% on placebo
3% ascites; <1% hepatic encephalopathy
Risk factors for decompensation included:
Age ≥50
MELD ≥10
Albumin ≤3.5 g/L
ALT <3x ULN
Bilirubin >0.7 mg/dL
History of alcohol abuse
Multivariate analysis of risk factors for
hepatic decompensation
Treatment
(eltrombopag vs placebo)
Age (50–60 vs <50)
Age (>60 vs <50)
MELD score (≥10 vs <10)
Albumin (≤35 vs >35)
Total bilirubin
(>1.0 vs ≤1.0 mg/mL)
ALT (<3x vs ≥3x ULN)
Alcohol abuse (Yes vs No)
0.1 10 Adjusted odds ratio
1
p
0.0024
0.0038
0.0038
0.0022
0.0002
0.0497
0.0216
0.0021

Case 1
11

• 66-year-old woman • Prior relapser after PEG IFN and RBV
Description
• Genotype 1b – IL28b CC • Non-biopsy proven cirrhosis with MRI scan appearance of portal
hypertension
• Fibroscan 26.3 kPa (5 July 2011) • Ultrasound showed irregular liver outline and coarse echotexture in
keeping with CLD (14 September 2012) • Splenomegaly (MRI)
HCV disease characteristics
• Weight: 65kg
Other medical information

Question
• The patient chooses to be retreated with a first generation protease inhibtior. For how long should this patient be treated with the interferon and ribavirin backbone?
A. 12 weeks
B. 24 weeks
C. 48 weeks

DAA regimens for treatment-experienced
patients with compensated cirrhosis
48 4 0 12 36 24
Telaprevir
+ Peg-IFN + RBV Peg-IFN + RBV
Peginterferon alfa-2b 135 µg/week + ribavirin 1200 mg/day
Boceprevir
Peg-
IFN +
RBV
Boceprevir + Peg-IFN + RBV
Telaprevir EU SmPC; Boceprevir EU SmPC

Start treatment: Boceprevir
Time Hb
(g/dL
)
Platelets
(x 103/mm3)
Neutrophils
(x 103/mm3)
Albumin
(g/dL)
Bilirubin
(μmol/L)
ALT
(IU/L)
HCV RNA
(IU/mL)
Baseline 12.3 61.0 0.95 45.0 27.0 69.0 2,403,150
Week 4 9.7 72.0 0.75 43.0 30.0 36.0 1,205
Week 8 8.5 67.0 0.55 38.0 19.0 29.0 Not
detected
Week 12* 7.4 74.0 0.37 34.0 17.0 24.0 Not
detected
*Admitted to hospital; Hb: hemoglobin; ALT: alanine aminotransferase

Subsequent course
Week 12 – admitted to hospital
– Pyrexial illness with neutropenia
– Positive blood cultures with gram-negative rods
– E-coli detected (UTI with bacteraemia)
– Sensitive to Augmentin; responded well
– Required GCSF
Week 28 – developed painful skin rash
– Saw dermatologist same day in clinic
– Responded well to topical corticosteroids
Continued throughout treatment with low neutrophils requiring
GSCF (last day of treatment = 0.19 GCSF given in clinic)
Treatment weeks 24_36_48 – HCV RNA not detected
UTI: urinary tract infection; GCSF: granulocyte colony stimulating factor

Case 2
17

• 59 year old male. Criminal lawyer
• Prior null responder after PEG IFN and RBV (2006)
Description
Hepatomegaly
ALT 61 AST 72 albumin 43 bilirubin 5
Genotype 1 infection HBsAg negative
Liver biopsy Nov 2005
Liver distortion, fibrous expansion portal tracts spicule formation
focal portal linking and bridging mod steatosis
August 2007 Fibroscan median stiffness 9/2.3/100%
IL28b genotype -860 TT genotype
Intermittently raised AFP
HCV disease characteristics
3-4 bottles wine per week; refused gastroscopy
2011 anal cancer treated radiotherapy and chemotherapy
Other medical information

Subsequent course
4 Feb 2012
– Ultrasound irregular liver no obvious focal lesions
– Slight but definite rise in AFP: 27
MRI scan 14 May 16 x 10 mm arterialised lesion in segment 8
– exhibits washout consistent with HCC
– Spleen normal size no ascites
26 June 2012
– Segment 8 wedge resection HCC + radiofrequency ablation
Moderately differentiated HCC 20 x 16 mm and 16 mm from
nearest surgical margin; No microvascular invasion
– Separate focus small cell dysplasia
Liver moderate chronic hepatitis moderate steatosis and
developing cirrhosis

Requested retreatment
Commenced treatment 17 August 2012
Telaprevir 750 mg tds peg alpha 2a 180 ug and ribavirin 600 mg
bd
Amlodipine interaction?

Time Hb (g/dL)
Platelets (x 103/mm3)
Neutrophils (x 103/mm3)
Albumin (g/dL)
Bilirubin (μmol/L)
ALT (IU/L)
HCV RNA (IU/mL)
Baseline 14.2 210 1.94 46 5 56 2,129,500
Week 4 10.8 177 1.59 44 16 31 3716
Start telaprevir, PEG IFN and ribavirin

What would you do next
A.Continue treatment and measure HCV RNA at week 8
B.Stop all treatment
C.Switch to boceprevir
D. Continue treatment to 12 weeks?

Time Hb (g/dL)
Platelets (x 103/mm3)
Neutrophils (x 103/mm3)
Albumin (g/dL)
Bilirubin (μmol/L)
ALT (IU/L)
HCV RNA (IU/mL)
Baseline 14.2 210 1.94 46 5 56 2,129,500
Week 4 10.8 177 1.59 44 16 31 3716
Stopped treatment Week 4 post treatment
44 6 44 426,216
Start telaprevir, PEG IFN and ribavirin

Stopping rules during telaprevir dosing period
Telaprevir EU SmPC
0 Weeks 4 8 12
If >1000 IU/mL at Week 4 or 12:
stop all drugs*
*In prior null responders, consideration should be given to conducting an additional HCV RNA test between Weeks 4 and 12.
If the HCV RNA concentration is >1000 IU/mL, telaprevir and Peg-IFN/RBV should be discontinued

Viral kinetics in patients who met the >1000 IU/mL
HCV RNA Week 4 stopping rule with telaprevir
Adda N, et al. HepDART 2011. Abstract 45
Treatment-naïve
patients
Treatment-experienced
patients
108
107
106
105
104
103
102
10 0 4 6 8 12 10 2
Weeks
HC
V R
NA
(IU
/mL
)
0 4 6 8 12 10 2
Weeks
HC
V R
NA
(IU
/mL
)
108
107
106
105
104
103
102
10

REALIZE (telaprevir): baseline factors and eRVR
status as predictors of SVR*
Variable
eRVR
Prior response to PR
LDL (mmol/L)
Fibrosis stage
Baseline log10 HCV RNA (IU/mL)
HCV genotype subtype (1a/1b)
Maximum ALT, AST
0.1 1 10
Odds ratio (95% CI)
With eRVR included
0.1 1 10
Odds ratio (95% CI)
Without eRVR included
Berg T, et al. Hepatology 2011;54(Suppl. S1):375A *Multiple logistic regression analysis subset (N=465); telaprevir treatment arms were pooled
Additional factors included in the analyses but found to be non-significant include: medical history of hypertension; age; BMI; triglycerides; HDL; gender; log HOMA-IR; race (black/nonblack); and GGT

Case 3
27

• 64year old male.
• G1 b
• Jan 2010 PEG IFN RBV 48 week
• Undetectable at EOT: relapse
Description
• Diffuse large cell B cell lymphoma stage 4b well controlled
• Reactivation hepatitis B during treatment
• Fibroscan 3.5/0.9/100%
• ALT 32 AST 61
HCV disease characteristics
Other medical information
• Creatinine133 creatinine clearance 49 ml/s
• Doppler ultrasound portal vein
• Single functioning kidney

– Telaprevir, IFN RBV 1000 mg started 7 Oct 2011

TW 4 Nov 2011 Platelets 22
1 Dec 2011 TW8 Platelets 23
Subsequent course

What would you do next
A.Reduce dose of interferon
B.Reduce dose of both interferon and ribavirin
C.Stop all treatment
D.Give eltrombopag or romiplostin

TW 44 Nov 2011 Platelets 22
1 Dec 2011 TW8 Platelets 23
Eltrombopag started 25 mg increased to 50 mg; given one month
TW11 (22 Dec 2011) platelets 48
TW12 (29 Dec 2011) platelets 47
TW 20 (31 May 12) Platelets 34
TW24 (5 July 2012) Platelets 48
Current platelet count 48
Subsequent course

Side effects: Anemia
– Anaemia:
– Transfusion 3 units blood December 2012
– Haemoglobin rose from 6.2 to 9.7
– Dose reductions Ribavirin
– Erythropoetin
EPO 20,000 per week
RBV 200 mg /day 45 ug IFN
– HB 7.7, eGFR 34 ALT 11 AST 17
Patient 8 DF

HCV RNA 401,752 iu/ml at baseline
Start treatment October 2011
TW4 Undetectable
TW12 undetectable
Subsequently undetectable
End of treatment: HCV RNA undetectable
End of treatment blood tests:
HB 7.9 WCC 3.76 platelets 135,000; ALT 26 AST 36
Creatinine 129, eGFR 50 ml/min
Subsequent SVR
HCV RNA concentrations
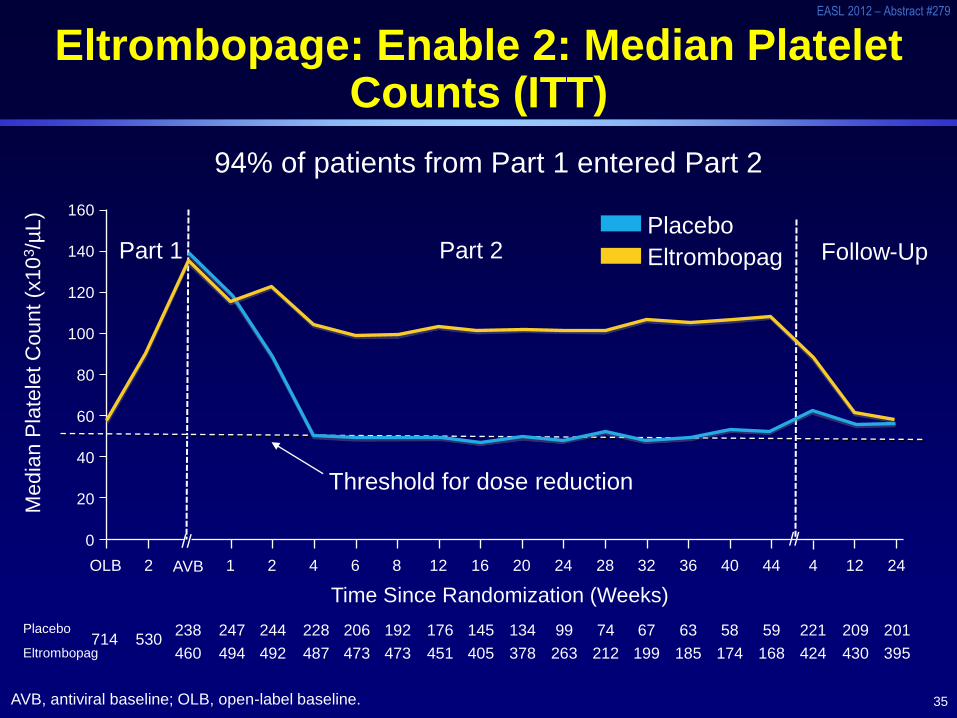
35
EASL 2012 – Abstract #279
Eltrombopage: Enable 2: Median Platelet Counts (ITT)
AVB, antiviral baseline; OLB, open-label baseline.
Part 1 Part 2 Follow-Up
Me
dia
n P
late
let C
ou
nt
(x1
03/µ
L)
// //
Time Since Randomization (Weeks)
Threshold for dose reduction
OLB 2 AVB 1 2 4 6 8 12 16 20 24 28 32 36 40 44 4 12 24
160
140
120
100
80
60
40
20
0
Placebo
94% of patients from Part 1 entered Part 2
714 530
Placebo
Eltrombopag
238 247 244 228 206 192 176 145 134 99 74 67 63 58 59 221 209 201
460 494 492 487 473 473 451 405 378 263 212 199 185 174 168 424 430 395 Eltrombopag

Protease inhibitor regimens with PEG IFN RBV
Requisite backbone of PEG IFN:
– All problems associated with PEG IFN and RBV use
Including depression, psychiatric symptoms worsening of liver function and severe infections
(Prolonged) use required in patients with cirrhosis?
– render a large group requiring careful management

Predicted impact of treatment on reduction in cumulated
incidence of HCV-related cirrhosis 2012–2021
13
24
18
8
14
8
16
34
24
10
18
12
27
37
30
20
34
31
0
10
20
30
40
50
Belgium France Germany Italy Spain UK
Pegylated bitherapy
PI-based triple therapy
PI-based triple therapy + reinforcement of HCV screening and treatment access
Red
ucti
on
in
in
cid
en
ce o
f H
CV
-rela
ted
cir
rho
sis
(%
)
Deuffic-Burban S, et al. Gastroenterology 2012 [ePub ahead of print]

The paradox of progress
• Advances have brought higher rates of cure
– but more complexity to treatment of hepatitis C- a paradox of progress
– Do not make treatment more straightforward
– Complex process of decision making is required to assess

What threat do you think resistance to a first generation protease inhibitor poses?
A. No threat at all
B. A major problem
C. A problem but one that future regimens will solve

Will we have better, more tolerable interferons?

First SVR24 results from EMERGE:
PegIFN-λ1A (lambda) vs PegIFN-α2A (alfa) P
atie
nts
95%
CI (%
)
58.3
70.6
62.5 66.7
70.6
83.3
57.1
40.0
0
25
50
75
100
G2
n = 12 17 17 12 16 14 15 15
Lambda
120 μg
Lambda
180 μg
Lambda
240 μg
Alfa
180 μg
SVR24 by HCV genotype
Zeuzem S, et al. EASL 2012, Barcelona, #10
G2 G2 G2 G3 G3 G3 G3

Overcoming null response
• May be nullified in patients treated with potent regimens given for sufficient time to effect clearance of HCV from the liver and perhaps extrahepatic sites.
• An inverse correlation between the influence of the innate response and potency of DAA agents?
• Need more data

Decision process
• Ultimately what drives a patient, averse to inteferon to be treated with telaprevir or boceprevir and PEG IFN and RBV?
• What motivates a patient, already treated with IFN, want to do it again with a first generation PI regimen?
• What role does the physician have in influencing those choices?
• Unique decision process: – pushes the doctor - patient relationship, past easily
defined boundaries
– Need Aronsohn A, Jensen D. Informed deferral: A moral requirement for entry into the HCV treatment warehouse. Hepatology 2012;10.