clinical case report of long-term follow-up in shibukawa...
TRANSCRIPT

Posted at the Institutional Resources for Unique Collection and Academic Archives at Tokyo Dental College,
Available from http://ir.tdc.ac.jp/
Title
Clinical Case Report of Long-term Follow-up in
Type-2 Diabetes Patient with Severe Chronic
Periodontitis and Nifedipine-induced Gingival
Overgrowth.
Author(s) Shibukawa, Y; Fujinami, K; Yamashita, S
Journal Bulletin of Tokyo Dental College, 53(2): 91-99
URL http://hdl.handle.net/10130/2831
Right

Clinical Case Report of Long-term Follow-up in Type-2 Diabetes Patient with Severe Chronic Periodontitis and Nifedipine-induced Gingival Overgrowth
Yoshihiro Shibukawa, Koushu Fujinami and Shuichiro Yamashita*
Division of Conservative Dentistry, Department of Clinical Oral Health Science, Tokyo Dental College,2-9-18 Misaki-cho, Chiyoda-ku, Tokyo 101-0061, Japan
* Division of Prosthodontics, Department of Clinical Oral Health Science, Tokyo Dental College,
2-9-18 Misaki-cho, Chiyoda-ku, Tokyo 101-0061, Japan
Received 10 January, 2012/Accepted for publication 20 February, 2012
Abstract
In this case report, we describe the clinical course over a 14-year follow-up in a 47-year-old diabetes patient with severe chronic periodontitis and nifedipine-induced gingival overgrowth. The patient had a history of hypertension for over 5 years and uncontrolled type 2 diabetes. Overgrown gingiva was observed in most of the teeth and was marked in the upper and lower anterior teeth. A probing pocket depth of ≥4 mm and bleeding on probing (BOP) were observed in 94 and 90% of sites examined, respectively. At baseline, his hemoglobin A1c (HbA1c) was 8.5%. The patient received periodontal and diabetic treatment simultaneously. Medication was changed from nife-dipine chloride to an angiotensin-converting enzyme inhibitor. After initial therapy and subsequent periodontal surgery, gingival overgrowth disappeared and probing depth and BOP showed a significant improvement. No recurrence was observed during supportive periodontal therapy (SPT). The HbA1c level improved from 8.5 to 6.3% after periodontal treatment, subsequently remaining at a good level during SPT over 10 years. This study demonstrated that periodontal treatment, withdrawal of medication and control of diabetes can result in remarkable improvements in type 2 diabetes patients with chronic periodontitis and nifedipine-induced gingival overgrowth. These results suggest that comprehensive periodontal treatment in combination with treatment for diabetes mellitus can exert a positive influence on blood glucose levels and periodontal condition in diabetic patients.
Key words: Chronic periodontitis — Nifedipine — Gingival overgrowth — Type 2 diabetes — Case report
Case Report
91
Bull Tokyo Dent Coll (2012) 53(2): 91–99
Introduction
Poor metabolic control of diabetes mellitus
(DM) has often been associated with severe periodontal disease18,21). Diabetes mellitus is a complex disease with both metabolic and

92
vascular components, and is characterized by hyperglycemia due to defects in insulin secretion or action or both. It is a systemic disease of the innate immune system14), and patients with DM are prone to severe peri-odontitis11), which is considered its sixth complication8). No significant differences were observed in the subgingival biofilm between periodontitis patients with or with-out DM24). Therefore, it was hypothesized that DM-induced exaggeration of host immune responses played a crucial role in periodontal pathogenesis12), as glucose-mediated advanced glycation end products can increase the pro-duction of proinflammatory cytokines and mediators, which could contribute to peri-odontal destruction22).
Periodontal disease may also affect blood glucose levels in diabetic patients through insulin resistance5). There has been a recent focus on understanding the negative influ-ences of oral chronic inflammation on sys-temic health10,12).
Nifedipine, a dihydropyridine, is a calcium channel blocker that has been widely pre-scribed for various cardiovascular diseases, particularly hypertension3). The most promi-nent side effect of nifedipine therapy in oral tissue is gingival overgrowth9), which is characterized by an accumulation of extracel-lular matrix in the gingival connective tissue and epithelial hyperplasia with elongated, branched rete pegs penetrating deep into the connective tissue, with various degrees of chronic inflammatory infiltration1).
In this case report, we describe the clinical course over a 14-year follow-up in a 47-year-old type 2 diabetes patient with severe chronic periodontitis and nifedipine-associated gingi-val overgrowth. His diabetes and periodontal condition were evaluated longitudinally over 14 years.
Case
In September 1993, a 47-year-old man was referred to the Clinic of Conservative Den-tistry at the Chiba Hospital of Tokyo Dental
College with the chief complaint of gingival swelling around the upper and lower anterior teeth. The patient provided informed consent before entry into this study.
1. Clinical Oral ExaminationOvergrown gingiva was observed at all
the intradental gingival papillae in most of the teeth and was marked in the upper and lower anterior teeth. The consistency was generally fibrotic, with an erythematic appear-ance (Fig. 1). The patient stated that he first noticed the gingival enlargement approxi-mately 6 months prior to the initial visit and reported rapid growth during this period of time. The maxillary and mandibular ante-rior teeth were flared out, and the patient had lost several teeth and had no prosthodontic treatment. The plaque control record (PCR) (O’Leary et al.13)) score was 85%. A probing pocket depth of ≥4 mm and bleeding on probing (BOP) were observed in 94 and 90% of sites examined, respectively (Table 1). Teeth with severe bone loss showed mobility ranging from 2 to 3 (Lindhe and Nyman7)). Radiographic examination revealed moder-ate horizontal alveolar bone loss, calculus, and localized severe vertical alveolar bone loss (#16, 17, 31, 37, 41, 42, 44, 45, 46) (Fig. 2).
2. Systemic conditionThe patient’s weight was 80.2 kg and height
173.6 cm. Hypertension had been diagnosed 5 years prior to the patient’s initial visit and medication (calcium antagonist; nife-dipine 40 mg/day) had been prescribed and taken for 18 months. Blood pressure was 135/85 mmHg. Two years prior to visiting our hospital, type 2 diabetes had also been diagnosed in this patient, who had been taking an oral antidiabetic agent (metformin, 500 mg/day) for 18 months. Further medical examination revealed uncontrolled type 2 diabetes. The hemoglobin A1c (HbA1c) value was 8.5%. No diabetic complications or his-tory of smoking were found.
3. DiagnosisBased on the clinical findings, a diagnosis
Shibukawa Y et al.

93Periodontitis with Gingival Overgrowth and DM
of severe generalized chronic periodontitis with gingival overgrowth associated with nife-dipine was made. It was also considered possible that high blood glucose levels result-ing from uncontrolled type 2 diabetes may have exacerbated periodontal inflammation.
4. TreatmentA collaborative dental-medical treatment
plan was devised for diabetes-associated severe chronic periodontitis and nifedipine-induced gingival overgrowth.
First of all, a physician was consulted regard-
Table 1 Clinical findings at baseline, after initial therapy and SPT
Baseline
Re-evaluation SPT (0 y) SPT (11y)
(After initial therapy)
No. of teeth 27 27 20 20
Mean probing depth (%)*
<4 mm 6 34 98 100
≥4 mm, <6 mm 18 27 2 0
≥6 mm 76 39 0 0
Bleeding on probing (%) 90 23 3 2
HbAlc (%) 8.5 6.5 6.3 6.3
*Percent of sites with indicated probing depthBaseline, first visit (September 1993)Re-evaluation (after initial therapy) (September 1994)SPT (0 y); start of supportive periodontal therapy phase ( January 1996)SPT (11 y); ( January 2007)
Fig. 1 Oral photographs at baselineModerate gingival inflammation and overgrowth were observed. Hard and fibrotic swelling was noted in upper and lower anterior gingiva, which may be attributable to effect of calcium antagonist (nifedipine).

94
ing the patient’s uncontrolled type 2 diabetes and changes in dietary habits combined with an oral antidiabetic agent (metformin, 750 mg/day) were prescribed. The goal of dental treatment was to reduce periodontal infection and bacteremia, which may have affected the diabetic condition and gingi- val overgrowth, and to restore masticatory function, which may have affected dietary care for diabetes. Moreover, a physician was consulted regarding gingival overgrowth, which was a side effect of nifedipine, and whether it was possible change the medi-cation. The patient had been taking nife-dipine for 18 months, but now the medication was changed to an angiotensin-converting enzyme inhibitor (enalapril maleate, 10 mg/day). Thus, treatment was restricted to periodontal therapy that mainly focused on plaque control until improvement of glycemic control. Treatment consisted of meticulous oral hygiene instruction and supragingival scaling. Pocket irrigation with 0.2% ethacridine lactate (acrinol®) was per-formed following the above procedures.
During the first 2 months on the new medication, gingival overgrowth gradually subsided. Tooth-brushing instruction resulted in an improvement in oral hygiene (PCR 19%). In March 1994, subgingival scaling and
root planing were performed using Gracey curettes and an ultrasonic scaler as the base-line HbA1c (8.5%) had decreased to 6.9%. Although prognosis for teeth #16, 17, 27, 37, 44, 45, and 46 was judged to be hopeless, they were retained during initial therapy until HbA1c dropped to 6.5% or less16).
In June 1994, the HbA1c decreased to 6.5% and these teeth were extracted with premedi-cation using cephem antibiotics. A temporary prosthesis was applied.
In September 1994, re-evaluation was per-formed. The initial therapy resulted in an improvement in clinical parameters. Gingival inflammation, in particular, showed a sig- nificant reduction (BOP, 23%, Fig. 3A, 3B, Table 1). Periodontal surgery (flap opera-tion) was carried out between October 1994 and March 1995 in areas (teeth #11–15, 21–26, 31–-34, 38, 41–43, 48) where probing depth was ≥5 mm and osseous defects were present. The flap operation was performed with premedication using cephem antibiotics. To prevent postoperative infection, cephem antibiotics (3 days) were prescribed and irrigation with 0.2% ethacridine lactate (acrinol®) performed frequently at the wound surface. Postoperative healing was unevent-ful. Re-evaluation after 3 months healing showed a marked improvement in clinical
Fig. 2 Dental radiographs at baselineGeneralized horizontal alveolar bone loss was observed. Advanced bone loss was observed at lower incisor, molar and upper right molar.
Shibukawa Y et al.
95
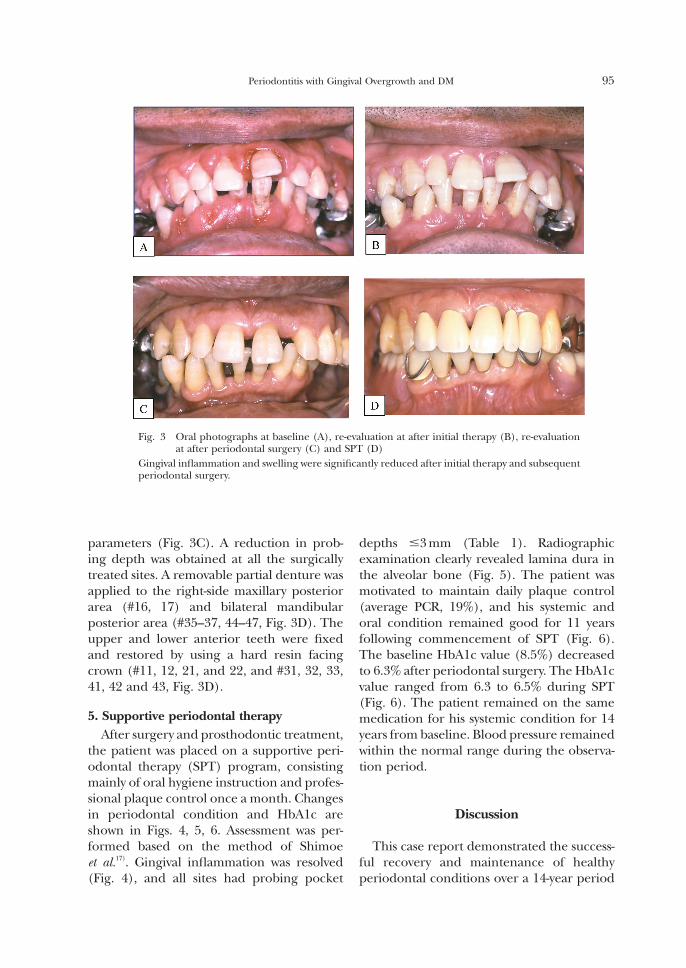
parameters (Fig. 3C). A reduction in prob- ing depth was obtained at all the surgically treated sites. A removable partial denture was applied to the right-side maxillary posterior area (#16, 17) and bilateral mandibular posterior area (#35–37, 44–47, Fig. 3D). The upper and lower anterior teeth were fixed and restored by using a hard resin facing crown (#11, 12, 21, and 22, and #31, 32, 33, 41, 42 and 43, Fig. 3D).
5. Supportive periodontal therapyAfter surgery and prosthodontic treatment,
the patient was placed on a supportive peri-odontal therapy (SPT) program, consisting mainly of oral hygiene instruction and profes-sional plaque control once a month. Changes in periodontal condition and HbA1c are shown in Figs. 4, 5, 6. Assessment was per-formed based on the method of Shimoe et al.17). Gingival inflammation was resolved (Fig. 4), and all sites had probing pocket
depths ≤3 mm (Table 1). Radiographic examination clearly revealed lamina dura in the alveolar bone (Fig. 5). The patient was motivated to maintain daily plaque control (average PCR, 19%), and his systemic and oral condition remained good for 11 years following commencement of SPT (Fig. 6). The baseline HbA1c value (8.5%) decreased to 6.3% after periodontal surgery. The HbA1c value ranged from 6.3 to 6.5% during SPT (Fig. 6). The patient remained on the same medication for his systemic condition for 14 years from baseline. Blood pressure remained within the normal range during the observa-tion period.
Discussion
This case report demonstrated the success-ful recovery and maintenance of healthy periodontal conditions over a 14-year period
Fig. 3 Oral photographs at baseline (A), re-evaluation at after initial therapy (B), re-evaluation at after periodontal surgery (C) and SPT (D)
Gingival inflammation and swelling were significantly reduced after initial therapy and subsequent periodontal surgery.
Periodontitis with Gingival Overgrowth and DM
96
following a diagnosis of nifedipine-induced gingival overgrowth in a patient with diabetes and advanced chronic periodontitis. More-over, the patient’s HbA1c level improved from 8.5 to 6.3% after periodontal treatment, sub-sequently remaining at a good level during
SPT over a 10-year period. The present find-ings agree with data previously reported in treatment and maintenance studies of short duration20). Controlled studies have shown that the response of diabetics to non-surgical and surgical periodontal therapy is similar
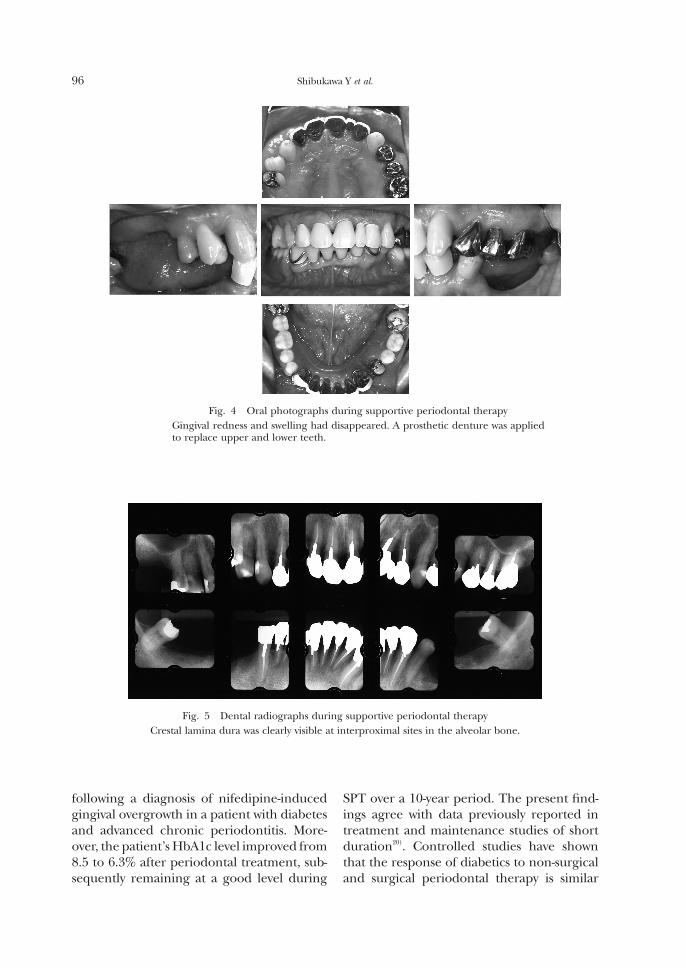
Fig. 4 Oral photographs during supportive periodontal therapyGingival redness and swelling had disappeared. A prosthetic denture was applied to replace upper and lower teeth.
Fig. 5 Dental radiographs during supportive periodontal therapyCrestal lamina dura was clearly visible at interproximal sites in the alveolar bone.
Shibukawa Y et al.
97
to that of non-diabetics23). On the other hand, it was reported that poorly controlled dia- betics respond less successfully to periodon- tal therapy relative to well-controlled and non-diabetics19). Tervonen and Karjalainen19) reported that although poorly controlled diabetics responded to nonsurgical therapy similarly to controls in the short term (4 weeks), in the absence of maintenance ther-apy, more rapid recurrence of periodontal pockets and subgingival calculus was found. The data from the present study, however, seem to indicate that careful control of dis-ease in patients with diabetes will result in a similar low frequency of recurrent periodon-titis to that seen in non-diabetic patients if they receive treatment for periodontal disease and follow a careful plaque control program. These findings suggest that information on the level of glycemic control in diabetics is useful in determining periodontal progno-sis and the need for periodontal therapy on an individual basis. Therefore, assessment of metabolic status is important in determining the prognosis and recall interval for peri-
odontal therapy.In the present case, the patient’s HbA1c
level showed a marked improvement from 8.5 to 6.3% after periodontal treatment. Much evidence indicates a bidirectional relationship between diabetes and periodontal disease10,12). It is possible that periodontitis plays some role in the development of insulin resistance2). Iwamoto et al.5) reported that antimicrobial periodontal therapy was effective in improv-ing metabolic control in diabetics, possibly through reduced serum TNF-α and improved insulin resistance. The authors also suggested that increased TNF-α caused by chronic inflam- mation may have an additive effect on insulin resistance in type 2 diabetes patients. This indicates that controlling periodontal infec-tion would play an important role in the overall management of this disease. However, to date, relatively few intervention studies have examined the effect of periodontal therapy on the metabolic status of diabetes. Therefore, there is no consistent agreement as to the beneficial effects of periodontal treatment on the metabolic control of patients
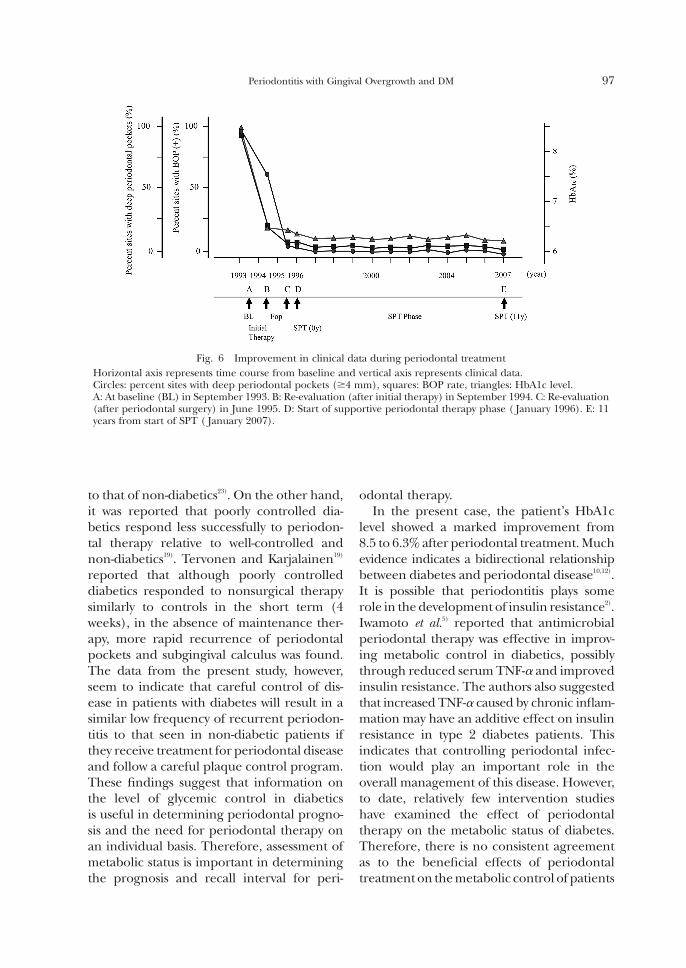
Fig. 6 Improvement in clinical data during periodontal treatmentHorizontal axis represents time course from baseline and vertical axis represents clinical data.Circles: percent sites with deep periodontal pockets (≥4 mm), squares: BOP rate, triangles: HbA1c level.A: At baseline (BL) in September 1993. B: Re-evaluation (after initial therapy) in September 1994. C: Re-evaluation (after periodontal surgery) in June 1995. D: Start of supportive periodontal therapy phase ( January 1996). E: 11 years from start of SPT ( January 2007).
Periodontitis with Gingival Overgrowth and DM

98
with diabetes. In the present case, too, it is unclear as to the precise reason for the observed improvement in the patient’s dia- betes, as periodontal and diabetic treatment were performed simultaneously. The improve-ment in HbA1c level may have been due to the improvement in insulin resistance follow-ing reduction of circulating levels of several proinflammatory cytokines, which is probably associated with the effect of periodontal treat-ment10,12). Moreover, periodontal treatment including restoration of masticatory function appears to affect dietary care for diabetes.
In this case, the withdrawal of medication and removal of plaque provided relative reso-lution of gingival tissues. Earlier reports on treatment for nifedipine-induced gingival overgrowth involved reduction or elimina- tion of the drug or surgical excision9,15). It was been reported that the presence of dental plaque and inflammation might be a signifi-cant risk factor for gingival overgrowth4). We emphasized plaque control as the first step in our treatment program and during SPT. A recent study on patients with type 2 diabetes showed that nifedipine intake was associ- ated with a significantly deeper probing depth and greater extent of sites with increased probing depth6). It remains unknown as to whether hyperglycemic status and its effects on gingival tissue play a synergistic role in drug-influenced gingival enlargement. This study demonstrated that withdrawal of medi-cation and control of diabetes resulted in remarkable improvements. Further controlled investigations should be carried out to further clarify this possible complex interaction.
In summary, this study demonstrated that periodontal treatment, withdrawal of medi-cation and control of diabetes can result in remarkable improvements in type 2 diabetes patients with chronic periodontitis and nife-dipine-induced gingival overgrowth. These results suggest that comprehensive periodon-tal treatment in combination with treatment for diabetes mellitus can exert a positive influ-ence on blood glucose levels and periodontal condition in diabetic patients.
Acknowledgements
We would like to thank Associate Professor Jeremy Williams, Tokyo Dental College, for his assistance with the preparation of this manuscript.
References
1) Barak S, Engelberg IS, Hiss J (1987) Gingival hyperplasia caused by nifedipine. Histopatho-logic findings. J Periodontol 58:639–642.
2) Benguigui C, Bongard V, Ruidavets JB, Chamontin B, Sixou M, Ferriéres J, Amar J (2010) Metabolic syndrome, insulin resis-tance, and periodontitis: a cross-sectional study in a middle-aged French population. J Clin Periodontol 37:601–608.
3) Ferlinz J (1986) Nifedipine in myocardial ischemia, systemic hypertension, and other cardiovascular disorders. Ann Intern Med 105:714–729.
4) Hancock RH, Swan RH (1992) Nifedipine-induced gingival overgrowth. Report of a case treated by controlling plaque. J Clin Periodon-tol 19:12–14.
5) Iwamoto Y, Nishimura F, Nakagawa M, Sugi-moto H, Shikata K, Makino H, Fukuda T, Tsuji T, Iwamoto M, Murayama Y (2001) The effect of antimicrobial periodontal treatment on circulating tumor necrosis factor-alpha and glycated hemoglobin level in patients with type 2 diabetes. J Periodontol 72:774–778.
6) Li X, Luan Q, Wang X, Sha Y, He L, Cao C, Jin L (2008) Nifedipine intake increases the risk for periodontal destruction in subjects with type 2 diabetes mellitus. J Periodontol 79:2054–2059.
7) Lindhe J, Nyman S (1987) Clinical trials in periodontal therapy. J Periodontal Res 22: 217–221.
8) Löe H (1993) Periodontal disease. The sixth complication of diabetes mellitus. Diabetes Care 16:329–334.
9) Lucas RM, Howell LP, Wall BA (1985) Nifedipine-induced gingival hyperplasia. A histochemical and ultrastructural study. J Periodontol 56:211–215.
10) Mealey BL, Oates TW (2006) Diabetes melli-tus and periodontal diseases. J Periodontol 77:1289–1303.
11) Nelson RG, Shlossman M, Budding LM, Pettitt DJ, Saad MF, Genco RJ, Knowler WC (1990) Periodontal disease and NIDDM in Pima Indians. Diabetes Care 13:836–840.
Shibukawa Y et al.

99
12) Nishimura F, Iwamoto Y, Soga Y (2007) The periodontal host response with diabetes. Periodontol 2000 43:245–253.
13) O’Leary TJ, Drake RB, Naylor JE (1972) The plaque control record. J Periodontol 43:38.
14) Pickup JC (2004) Inflammation and activated innate immunity in the pathogenesis of type 2 diabetes. Diabetes Care 27:813–823.
15) Pilloni A, Camargo PM, Carere M, Carranza FA Jr (1998) Surgical treatment of cyclo- sporine A- and nifedipine-induced gingival enlargement: gingivectomy versus periodontal flap. J Periodontol 69:791–797.
16) Shichiri M, Kishikawa H, Ohkubo Y, Wake N (2000) Long-term results of the Kumamoto Study on optimal diabetes control in type 2 diabetic patients. Diabetes Care 23:21–29.
17) Shimoe M, Yamamoto T, Iwamoto Y, Shiomi N, Maeda H, Nishimura F, Takashiba S (2011) Chronic periodontitis with multiple risk factor syndrome: a case report. J Int Acad Peri-odontol 13:40–47.
18) Taylor GW, Burt BA, Becker MP, Genco RJ, Shlossman M (1998) Glycemic control and alveolar bone loss progression in type 2 dia-betes. Ann Periodontol 3:30–39.
19) Tervonen T, Karjalainen K (1997) Periodontal disease related to diabetic status. A pilot study of the response to periodontal therapy in type 1 diabetes. J Clin Periodontol 24:505–510.
20) Tervonen T, Knuuttila M, Pohjamo L, Nurk-kala H (1991) Immediate response to non-surgical periodontal treatment in subjects
with diabetes mellitus. J Clin Periodontol 18: 65–68.
21) Tsai C, Hayes C, Taylor GW (2002) Glycemic control of type 2 diabetes and severe peri-odontal disease in the US adult population. Community Dent Oral Epidemiol 30:182– 192.
22) Vlassara H, Brownlee M, Manogue KR, Dinarello CA, Pasagian A (1988) Cachectin/TNF and IL-1 induced by glucose-modified proteins: role in normal tissue remodeling. Science 240:1546–1548.
23) Westfelt E, Rylander H, Blohmé G, Jonasson P, Lindhe J (1996) The effect of periodontal therapy in diabetics. Results after 5 years. J Clin Periodontol 23:92–100.
24) Zambon JJ, Reynolds H, Fisher JG, Shlossman M, Dunford R, Genco RJ (1988) Microbiologi-cal and immunological studies of adult perio-dontitis in patients with noninsulin-dependent diabetes mellitus. J Periodontol 59:23–31.
Reprint requests to: Dr. Yoshihiro Shibukawa Division of Conservative Dentistry, Department of Clinical Oral Health Science, Tokyo Dental College, 2-9-18 Misaki-cho, Chiyoda-ku, Tokyo 101-0061, Japan E-mail: [email protected]
Periodontitis with Gingival Overgrowth and DM