clinical commissioning and the future of urgent & emergency care rick stern urgent care lead,...
TRANSCRIPT
Clinical commissioning and the future of urgent & emergency care
Rick SternUrgent care lead, NHS Alliance & Director, Primary Care Foundation Reforming urgent & emergency care – where do we go from here?
8th November 2011

What I hope to do …
1. Explore the opportunities and challenges for the new clinical commissioners
2. Reflect on what this might mean for urgent & emergency care

NHS Alliance Urgent Care Network – recent achievements●Offering an informed critique of 111●Supporting CQC in registration of
OOH providers●Leading a national pilot to learn
from each other when things go wrong in out of hours services
●Preparing a major report on urgent care commissioning with the Primary Care Foundation

© Primary Care Foundation
Reports for Department of Health:● Primary Care in A&E● Urgent Care in general practice● Benchmark of out of hours services● Urgent care centres● Urgent care commissioning
The Primary Care has looked at urgent care from a number of angles

Principles of Clinical Commissioning• Clinical
leadership
• Primary care focus
• Local sensitivity
• Clinical Commissioning Groups are, in legislation, membership groups of constituent GP practices

Moving services from hospital to primary care

An agenda for Clinical Commissioners• Integrating general practice, community services and social services
• Long term disease becomes a primary care speciality
• Better care for elderly acute ill in the community
• More diagnostics in the community
• Integrating mental health
• Integrated urgent and emergency care

Better use of Resources
• Elective referrals
• Prescriptions
• Diagnostics
• Within general practice
• Urgent and emergency care – reducing emergency admissions
• Reducing variation

What does this mean for individual GPs and practices?• Make sure they are ‘on the
bridge’ of their Clinical Commissioning Group
• Develop relationships with local GP practices and others
• Diversify provision
• Create an effective patient participation group

• PCT Cluster support• 47% of CCGs were fully involved, 32% said they were not involved, with
21% replying ‘not sure’.
• Relationship with PCT clusters• enabling & permissive (35%), developmental & supportive (34%),
controlling & directing (32%), performance managing & centralist (30%), mirroring previous style (28%), too early to tell (16%)
• Obstacles in making the transition into CCGs
• layers of management bureaucracy • top down direction stifling innovation• Lack of time• The debt we may inherit“There are too many meetings focused on structures with no relevance to empowering CCGs or transforming clinical care... This is not a liberating process - it is painful, slow and bureaucratic.”
How is the development of CCGs going so far? A mixed picture … NHS Alliance/NAPC Survey September 2011
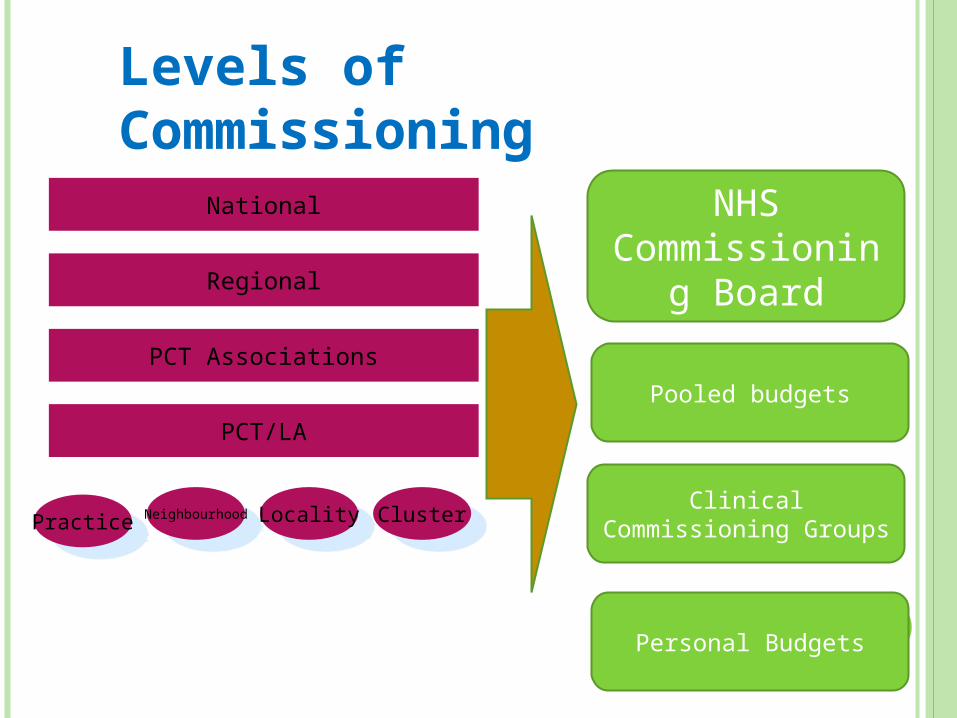
National
Regional
PCT/LA
PracticePractice Locality
LocalityNeighbourhood
NeighbourhoodCluster
Cluster
PCT Associations
NHS Commissionin
g Board
Clinical Commissioning Groups
Pooled budgets
Personal Budgets
Levels of Commissioning

Breaking the mould without breaking the system: new ideas and resources for clinical commissioners onthe journey towards integrated 24/7 urgent care
So what does all this mean for the commissioning of urgent & emergency care?

‘There is a massive learning curve in coming new to commissioning care. We started with a clear view of how we wanted to change our local healthcare system in a way that was challenging for others and it took us a while to realise just how complex the system is. You need to have bold ideas, but you need to work out how you are going to see them through. To be suddenly given a great deal of power is also to be given a great deal of responsibility. The real challenge is to break the mould without breaking the system.’
Donal Hynes, GP leader in Somerset

Commissioning Urgent Care:Six Central Themes1. Build care around the patient not the existing services
2. Simplify an often complicated and fragmented system
3. Ensure the urgent care system works together rather than pulling apart
4. Acknowledge prompt care is good care
5. Focus on all the stages for effective commissioning
6. Offer clear leadership across the system, while acknowledging its complexity

Towards an integrated urgent care system• Involving networks in commissioning
• Commissioning patient pathways
• Commission for quality - including making clear the ‘quality cost’
• Importance of whole system metrics
• Integrated audit across urgent care services
• Single point of access & the new 111 service for urgent care

Towards an integrated urgent care system
• Aligning financial incentives
• Commissioning based on patient experience
• Effective performance management of urgent care systems
• Learning from mistakes
• Tendering – the final option
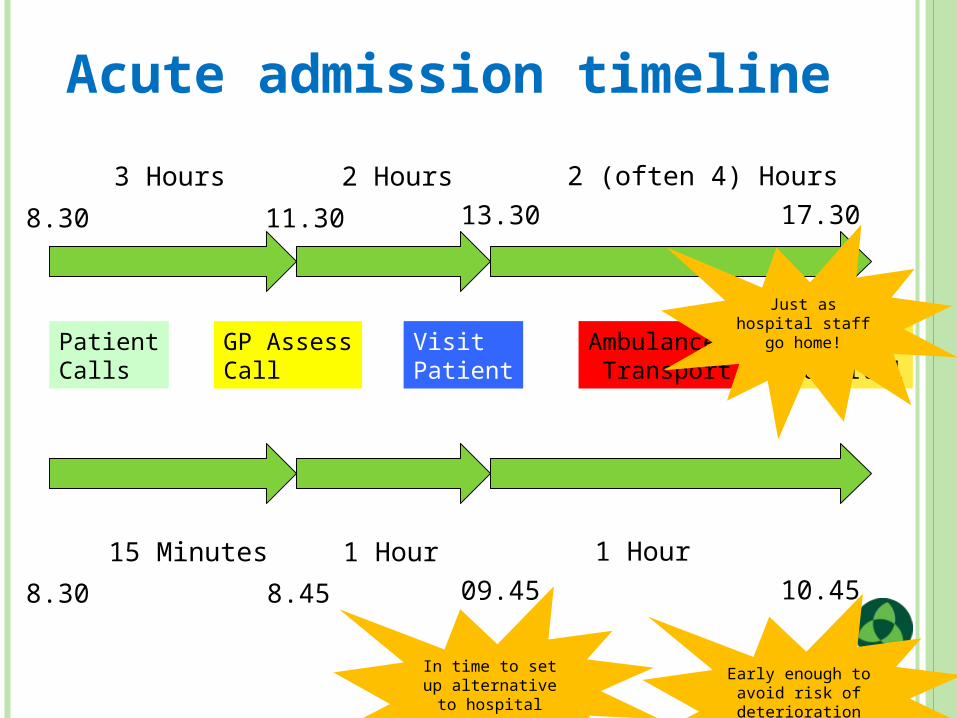
Ambulance Transport
ArriveHospital
8.30 11.30 13.30 17.30
3 Hours 2 Hours 2 (often 4) Hours
8.30 8.45 09.45 10.45
15 Minutes 1 Hour 1 Hour
Just as hospital staff go home!
In time to set up alternative to hospital
Early enough to avoid risk of deterioration
PatientCalls
GP AssessCall
VisitPatient
Acute admission timeline

Final take home messages …
1. General practice is the bedrock of the urgent care system. There is a gearing effect - small changes in many practices have a major impact on the system as a whole. We ignore general practice at our peril.
2. There is too much on offer between GP and A&E, confusing patient. Evidence suggests it increases demand rather than reducing pressure elsewhere in the urgent care system.
3. There is a need to see patients promptly and at whatever point they access urgent care.
4. There is a great opportunity for the new clinical commissioners to bring some good sense to the current confusion - developing a clear local vision.
