clinical health information systems ch.3. p retest (t rue /f alse ) a patient who has surgery at an...
TRANSCRIPT
Clinical Health Information Systems
Ch.3
PRETEST (TRUE/FALSE)
A patient who has surgery at an ambulatory care facility is required to remain overnight.
The emergency department is considered an outpatient service.
The average length of stay in a long-term care facility is greater than 30 days.
PRETEST (TRUE/FALSE) (CONTINUED)
If a patient is readmitted to a hospital, the hospital will use the same patient chart it used for that patient previously, rather than starting a new chart.
The size of an outpatient facility is determined by the number of patients it sees each day.

HEALTH DELIVERY FUNDAMENTALS
AMBULATORY CARE FACILITIES
Also called outpatient care facilities Provide care to patients who do not require
an overnight stay Privately or publicly owned

EXAMPLES OF AMBULATORY CARE FACILITIES
Doctor’s offices Medical clinics Public health departments Walk-in clinics Urgent care centers Outpatient surgery centers Diagnostic centers

ACUTE CARE FACILITIES
Treat patients (inpatients) with more serious illnesses or injuries
Keep patients overnight or longer Owned by either for-profit corporations or
not-for-profit organizations Typically called a hospital
EXAMPLES OF ACUTE CARE FACILITIES
Acute care hospital Not-for-profit hospital For-profit hospital Long-term care facility Rehabilitation facility
HOSPITAL DEPARTMENTS
Surgery Radiology Pediatrics Laboratory Emergency (ED or ER) Trauma centers Intensive care units (ICUs)

LENGTH OF STAY (LOS)
Outpatient facility: Patients do not stay overnight
Inpatient facility: ALOS less than 30 days (acute care) ALOS greater than 30 days (long-term care)
Note: ALOS=Average LOS

DETERMINING FACILITY SIZE
Outpatient facility: Number of patient encounters per day
Inpatient facility: Number of licensed beds Bed count
ADMISSION/DISCHARGE
Outpatient facility: No formal process
Inpatient facility: Formal process for both Doctor must perform physical exam within 24
hours of admission Discharge requires doctor’s order Date and time of both determine LOS and
number of days for billing
ORGANIZATIONAL CHARTS
Used in business and other organizations to illustrate managerial relationships
Place most responsible position at top Place next management level below, and so
forth
ORGANIZATIONAL CHARTS
Use vertical lines to connect managers with subordinates
Use horizontal lines to indicate equal jobs reporting to same manager

ORGANIZATIONAL CHARTS (CONTINUED)
Inpatient care facilities generally have more complex organizational structures
Outpatient care facilities generally have a simpler management structure
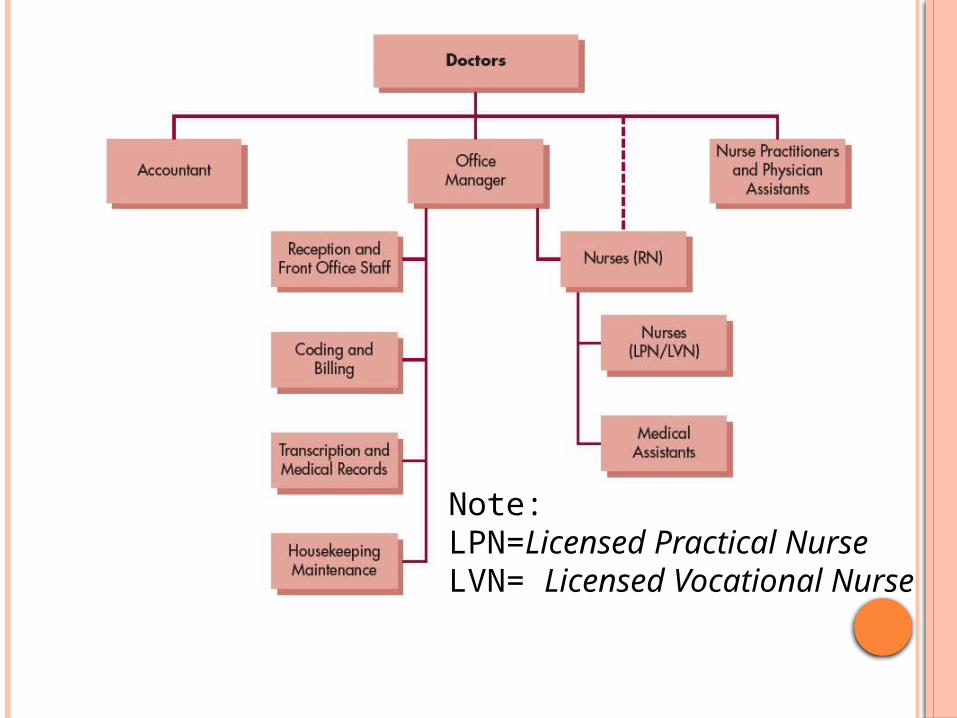
Note: LPN=Licensed Practical NurseLVN= Licensed Vocational Nurse
SUBACUTE CARE FACILITIES
Offer services appropriate for patients whose nursing care needs are less frequent and intensive
Include physical rehabilitation facilities, long-term care facilities, home care
REHABILITATION FACILITIES
Offer inpatient care Help patient return to maximum functionality
possible Specialize in physical medicine, PT
(PhysioTherapy), OT (Occupational Therapy), addiction recovery
LONG-TERM CARE FACILITIES
Offer inpatient care at less intense level than acute care facility
Provide LOS greater than 30 days Include skilled nursing facilities, nursing
homes, residential care facilities, rehabilitation hospitals

HOME CARE
Offered regularly in patient’s home, not in a facility
Provided by home health agencies Includes the following healthcare providers:
Nurses PTs OTs
OUTPATIENT CHART
Single chart per patient Contains records of all visits, plus associated
reports or results from other providers Focuses on longitudinal care of patient Used primarily used by physician, nurse,
billing staff
OUTPATIENT CHART (CONTINUED)
Includes detailed physician’s notes about each visit
Has smaller quantity of data than inpatient chart
INPATIENT CHART
New chart started each time patient admitted
Focuses on information related to current stay
Used extensively by wide number of caregivers and administrative personnel
Includes brief physician exam notes

INPATIENT CHART (CONTINUED)
Includes doctor’s orders and nurses’ notes as main elements
Contains greater quantity of data than outpatient chart

Figure 1-10 Medical specialties and subspecialties
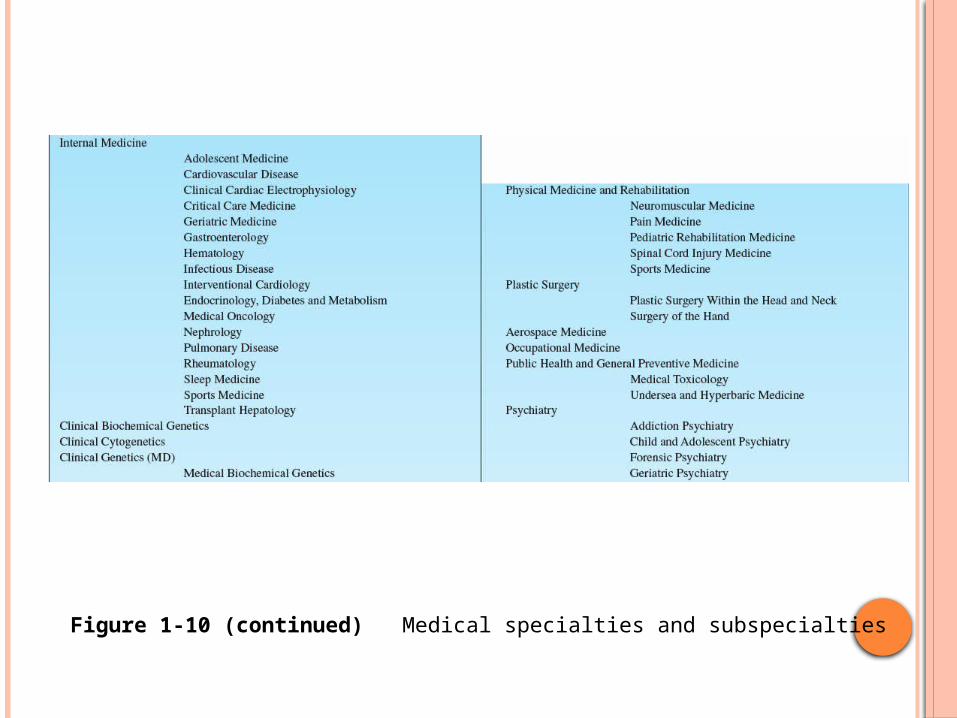
Figure 1-10 (continued) Medical specialties and subspecialties
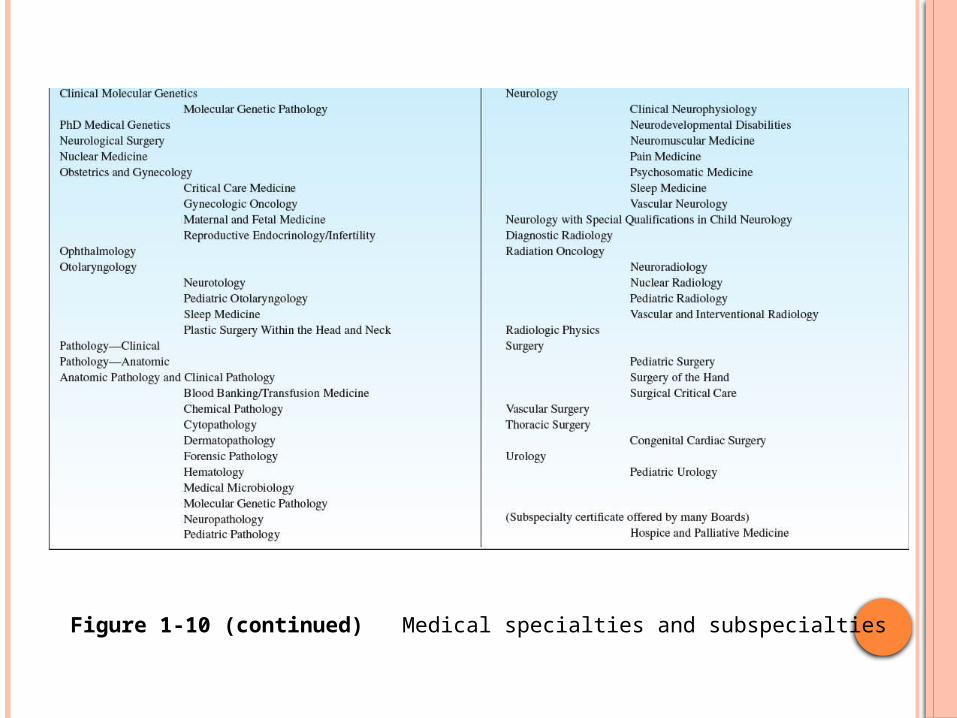
Figure 1-10 (continued) Medical specialties and subspecialties
DIRECT CARE PROVIDERS
Provide healthcare services directly to patient
Require state license to practice Actions regulated by professional or licensing
boards
DIRECT CARE PROVIDERS (CONTINUED)
Must document patient care, including time spent with, observations, actions
Depend on accuracy and completeness of health record to make patient care decisions
DOCTORS
Include several different types of healthcare professionals
Require specialized training and licensing Oversee patient’s care Order medications, therapy, diagnostic tests,
referrals, consults with other physicians
DOCTORS (CONTINUED)
Authorize medical orders and patient documentation
EXAMPLES OF DOCTORS
Chiropractors Dentists Psychologists Osteopaths Medical doctors
American boards of specialties and subspecialties
NURSES
Spend largest amount of time in direct patient care Several levels of nursing licensure:
LPN (Licensed Practical Nurse) RN (ADN= Associate Degree in Nursing, BSN= Bachelor
of Science Nursing ) CRNA(Certified Registered Nurse Anesthetists ) Nurse midwives Nurse practitioners
PHYSICIAN ASSISTANTS
Work under supervision of physicians Conduct physical exams Diagnose and treat illnesses Order and interpret tests Counsel patients Assist in surgery
ALLIED HEALTHCARE PROFESSIONALS
Provide care directly to patient Operate based on orders of licensed provider
(doctor, nurse practitioner, PA) Examples include:
Physical therapists (PTs) Occupational therapists (OTs) Respiratory therapists (RTs)
ALLIED HEALTHCARE PROFESSIONALS (CONTINUED)
Clinical laboratory technicians Diagnostic technologists Pharmacists Registered dietitians (RDs) Audiologists Speech pathologists Clinical medical assistants

CLINICAL PROFESSIONAL ORGANIZATIONS
American Medical Association (AMA) American Nurses Association (ANA) American Hospital Association (ANA)

OUTLINE
• Clinical Information Systems—adoption, use, value– Electronic Health Record– Computerized Provider Order Entry (CPOE)– Medication Administration – Telemedicine/Telehealth– Personal Health Record
• Fitting Applications Together• Information Exchange Across Boundaries• Overcoming Barriers to Adoption
CLINICAL INFORMATION SYSTEMS

VARIOUS TERMS USED OVER TIME
CPRCompu
ter-Based Patient Record
EMRElectro
nic Medica
l Record
PHRPerson
al Health Recor
d
EHR Electronic
Health Recor
d
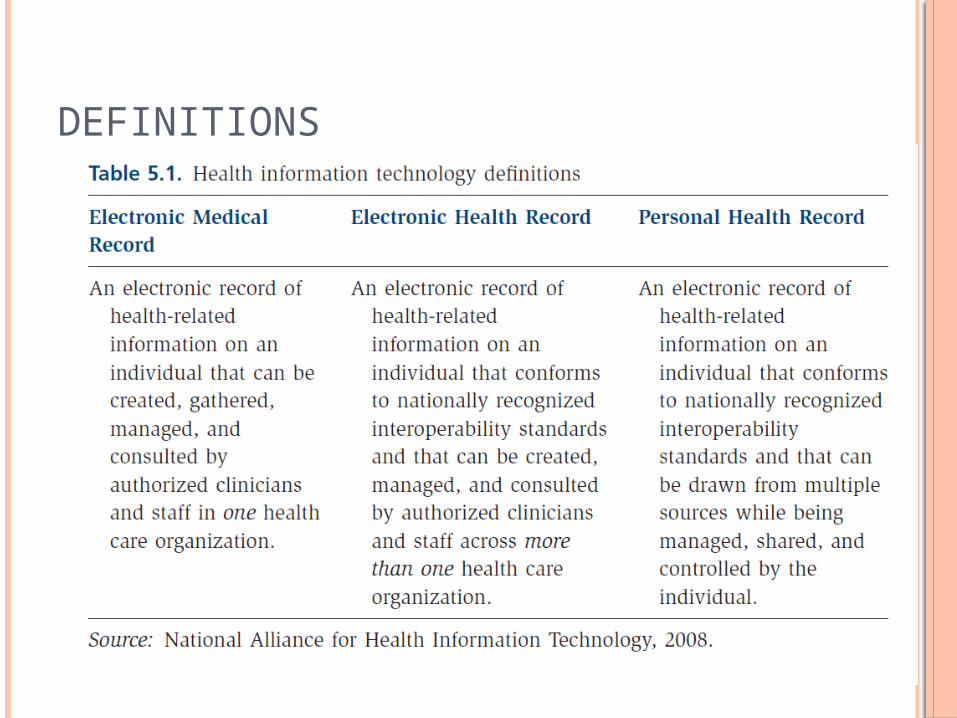
DEFINITIONS

CORE FUNCTIONS

WHERE ARE WE TODAY?
Broad Spectrum
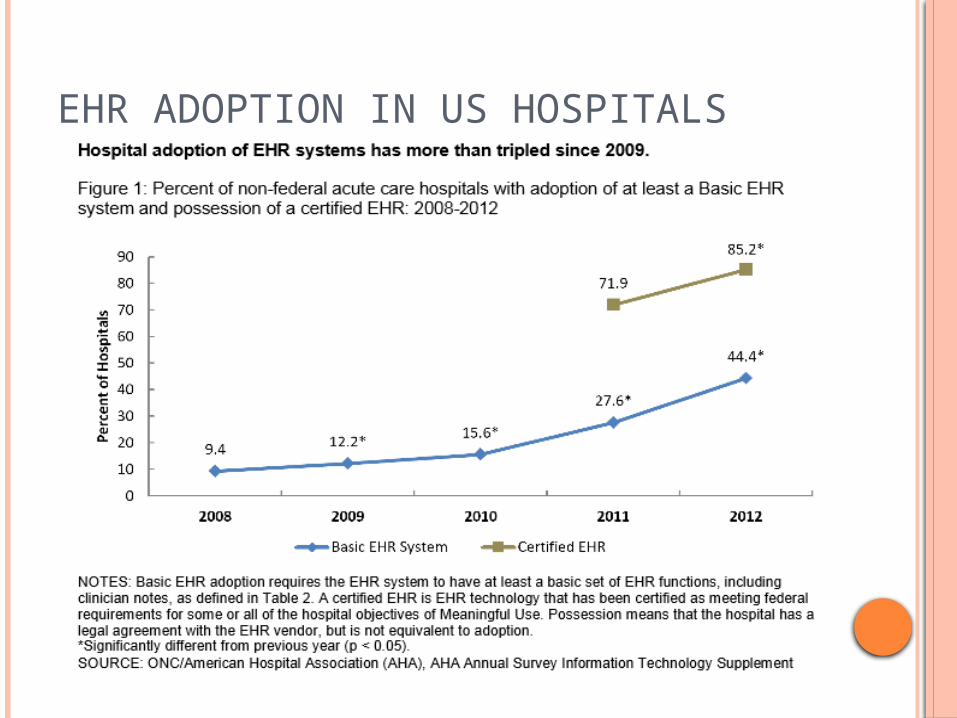
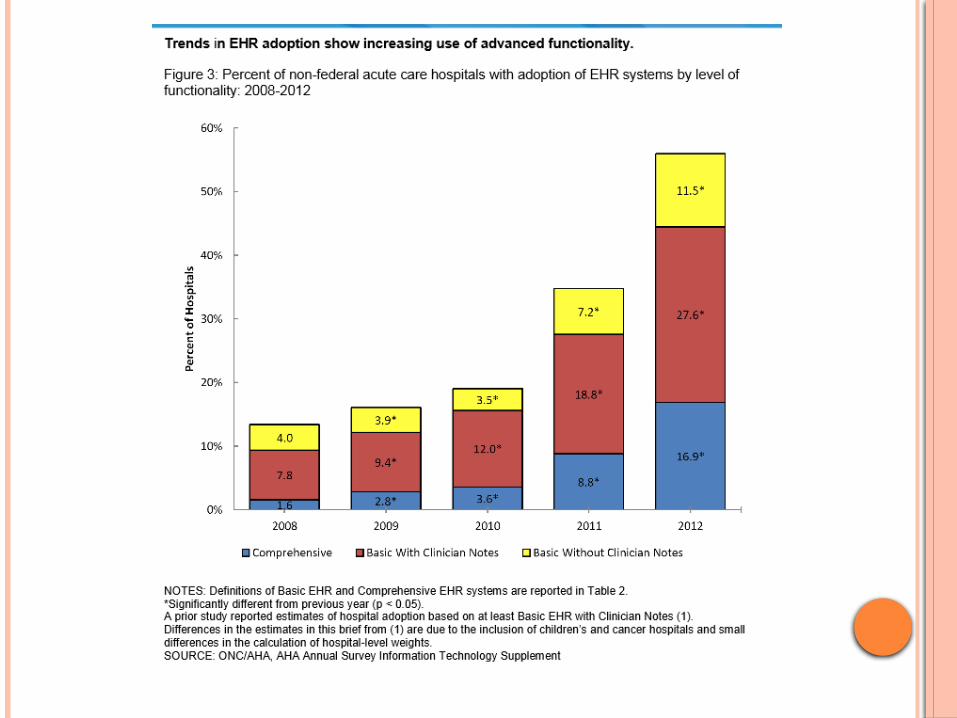
EHR ADOPTION IN US HOSPITALS

2012 PHYSICIAN ADOPTION OF EHRS

EHR USE IN OTHER POST ACUTE AND LTC SETTINGS
Extremely low 6%--Long term care 4%--Rehabilitation 2%--Psychiatric
Source: Health Affairs, 2012

VALUE OF EHR
Improved quality, outcomes and safety Computerized reminders and alerts Improved compliance with practice guidelines Reduction in medical errors
Improved efficiency, productivity, and cost reduction
Improved service and satisfaction

OTHER MAJOR TYPES OF CIS
Computerized provider order entry (CPOE) Medication administration using barcoding Telemedicine Telehealth—for our purposes, we will focus on
online communication (e.g. email) between patients and providers
Personal health record
CPOE• Driven by need to
improve patient safety
• Automates the ordering process
• Accepts orders electronically, provides decision support, may aid in diagnosis and treatment

USE AND STATUS OF CPOE
Estimates vary from 8-20% Historically teaching hospitals more likely to
use Many organizations are in various stages of
implementation Required for achieving meaningful use

HISTORICAL BARRIERS TO CPOE USE
• Complexity of ordering process• Physician entry an issue• Takes longer to place order; many systems
are ‘cumbersome’, take too many steps• Incentives may not be aligned with use• Lack of confidence in system reliability• Insufficient training• Mandating use – should you?
MEDICATION ADMINISTRATION
• Use of barcoding becoming more widespread
• Aids in correctly identifying patient, drug, dose, etc.
• HIMSS implementation guide—good resource
• More widely accepted
• Has been used successfully by many health care organizations
• Again, has potential to aid in making sure the right meds, get to the right patient, at the right dose…
TELEMEDICINE
• Use of telecommunciations for the direct provision of care to patients at a distance– Over 200 telemedicine
programs involving over 3500 health care institutions
– Store and forward– Two-way interactive TV
• Funding an issue• Cost effectiveness
not fully known
TELEHEALTH
Using telecommunications to communicate with patients and deliver services Electronic consultations (e-consultations) Patient portals Refilling prescriptions Registering patient Scheduling appointments
TELEHEALTH
Current use of email communication between patients and physicians
Value to patients and providers Issues
Complexity of infrastructureDegree of integrationMessage structureCostSecurityReimbursement

PERSONAL HEALTH RECORD & PATIENT PORTALS
Managed by consumer May include both health and wellness
information Patient portal—secure web site through
which patients can access PHR or EHR Approximately 7% of consumers have PHR

FITTING PIECES TOGETHER

BARRIERS TO ADOPTION & STRATEGIES FOR OVERCOMING THEM
Financial Organizational or Behavioral Technical Barriers Privacy and Security Barriers
STRATEGIES FOR OVERCOMING BARRIERS
What strategies are being employed to help overcome— Financial barriers? Behavioral barriers? Technical barriers?

SUMMARY
• Examined five clinical information systems—their current use, status, and value & their relationship to each other
• Discussed the value of sharing health information across organizations
• Discussed the three major barriers to adoption of these systems—financial, behavioral and technical and strategies to overcome them