clinical implications of regular marijuana use: what
TRANSCRIPT
LESSON 10Volume 44*9/16/2021
*The use of this volume for Class A CE Credits will expire 05/31/2024Copyright© 2021 by Current Reviews for Nurse Anesthetists®, Ft. Lauderdale, Florida
Clinical Implications of Regular Marijuana Use:What Clinicians Need to Know
Kathryn E. McGoldrick, MD, FCAI (Hon)Professor and Chair, Emerita
Department of AnesthesiologyAdvisory Dean for Student Affairs, Emerita
New York Medical CollegeValhalla, New York
Clinical Learning Environment Review (CLER)Department of Institutional Accreditation
Accreditation Council for Graduate Medical Education (ACGME)Chicago, Illinois
2 Current Reviews for Nurse Anesthetists®
Associate Publishers
Joan McNulty Elizabeth Moya, JD
Circulation Assistants
Myriam Montes
Kimberly Gutierrez Tiffany Lazarich
EDITORIAL BOARD
John Aker, CRNA, DNAPCoralville, Iowa
Linda Callahan, CRNA, PhDKlamath Falls, Oregon
Nancy Gaskey-Spear, CRNA, PhDGastonbury, Connecticut
Derrick C. Glymph, DNAP, CRNA, APRN, COL., USARMiami, Florida
Joseph A. Joyce, CRNA, BSGreensboro, North Carolina
Nina McLain-Calkins, PhD, CRNAPhiladelphia, Mississippi
ADVISORY BOARD
Kim Alexander, CRNASalisbury, North Carolina
Charles Barton, MSN, MEdAkron, Ohio
Carol G. Elliott, CRNA, MPA, PhDKansas City, Kansas
Linda J. Kovitch, CRNA, MSNBedford, Massachusetts
David Lott, CRNAHollywood, Florida
Frank T. Maziarski, CRNASeattle, Washington
Laura Wild, CRNA, MSNPennington, New Jersey
Sponsor -Frank Moya Continuing Education Programs, LLC
Subscription Offi ce - Editorial Offi ce –Current Reviews® Frank Moya, M.D. 1828 S.E. First Avenue 1450 Madruga Ave Ft. Lauderdale, FL 33316 Suite 207Phone: (954) 763-8003 Coral Gables, FL 33146Fax: (800) 425-1995Email: [email protected]
AccreditationThis program has been prior approved by the American Association of Nurse Anesthetists for 39 Class A CE credits; Code Number 1039844; Expiration Date May 31, 2024. AANA designated this program as meeting the criteria for up to 28.50 CE credits in Pharmacology/Therapeutics. Approved by Frank Moya Continuing Education Programs, LLC. Provider approved by the California Board of Registered Nursing, Provider Number CEP 1754, for 39 contact hours and Florida Board of Nursing, Provider Number FBN 2210 for 39 contact hours. In Accordance with AANA directives, you must get 88% of the answers correct to receive 1.5 credits for each lesson and if there is a failure when mailing in your answer cards, there is no retaking. When submitting your answers online you will be given three (3) attempts to pass the exam. You must get seven (7) of eight (8) answers correct to receive 1.5 credits per lesson. If you retake the exam online the questions will be different with each attempt.
Disclosure PolicyFrank Moya Continuing Education Programs, LLC, will disclose the existence of any relevant fi nancial relationship a faculty member, the sponsor or anyone else who may be in a position to control the content of this Activity has with any commercial interest. BEFORE STARTING, PLEASE SEE LAST PAGE OF LESSON TO READ WHETHER THERE ARE ANY RELEVANT RELATIONSHIPS TO DISCLOSE AND, IF SO, THE DETAILS OF THOSE RELATIONSHIPS.
Current Reviews® is intended to provide it’s subscribers with information that is relevant to anesthesia providers. However, the information published herein refl ects the opinions of it’s authors and does not represent the views of Current Reviews in Clinical Anesthesia®, Current Reviews for Nurse Anesthetists®, or Frank Moya Continuing Education Programs, LLC. Anesthesia practitioners must utilize their knowledge, training and experience in their clinical practice of anesthesiology. No single publication should be relied upon as the proper way to care for patients. The information presented herein does not guarantee competency or profi ciency in the performance of procedures discussed.
Copyright 2021 by Current Reviews®. Reproduction in whole or in part prohibited except by written permission. All rights reserved. Information has been obtained from sources believed to be reliable, but it’s accuracy and completeness, and that of the opinions based therein are not guaranteed. Printed in U.S.A. Current Reviews® is published biweekly by Current Reviews®, 1828 S.E. First Avenue, Ft. Lauderdale, FL 33316. POSTMASTER: Send address changes to Current Reviews®, 1828 S.E. First Avenue, Ft. Lauderdale, FL 33316 or email [email protected].
Publisherand
Editor-in-ChiefFRANK MOYA, MDCoral Gables, Florida
Assistant to the PublisherGwyneth Clarke-Bell
EditorMONTE LICHTIGER, MD
Coral Gables, FL
David O’ Connor, PhD, DNAP, CRNANew York, New York
Maria Garcia-Otero, CRNA, PhDCoral Gables, Florida
Sandra Ouellette CRNA, DSc (Hon)Winston-Salem, North Carolina
Amanda Faircloth Ward, PhD, DNAP, CRNARichmond, Virginia
Assistant Publisher
Assistant Editor Medical Illustrator
Barbara McNulty Carrie Scott

123Curr Rev Nurs Anesth 44(10):121-132 2021
Clinical Implications of Regular Marijuana Use:What Clinicians Need to Know
Kathryn E. McGoldrick, MD, FCAI (Hon)Professor and Chair, EmeritaDepartment of Anesthesiology
Advisory Dean for Student Affairs, EmeritaNew York Medical College
Valhalla, New York
Clinical Learning Environment Review (CLER)Department of Institutional Accreditation
Accreditation Council for Graduate Medical Education (ACGME)Chicago, Illinois
Upon completion of this lesson the reader should be able to:
LESSON OBJECTIVES
1. Discuss the extent to which marijuana has been legalized and decriminalized in the United States. 2. Quantify current estimates of the prevalence of marijuana use in the United States. 3. Summarize the history of marijuana use during the last five millennia. 4. Discuss the salient pharmacology of marijuana. 5. Enumerate the indications for the medical use of marijuana. 6. List the contraindications to medical use of marijuana. 7. Articulate the short-term effects of marijuana. 8. Summarize the long-term effects of cannabis use. 9. Discuss the cannabinoid hyperemesis syndrome.10. Summarize the perioperative concerns associated with regular use of marijuana and formulate an anesthetic plan for a patient with a history of chronic recreational use of marijuana.
IntroductionThe recreational use of marijuana is currently le-gal in 11 states and the District of Columbia. An additional 15 states and the U.S. Virgin Islands have decriminalized its use. Prior to January, 2018, the Cole Memorandum provided some protec-tion against enforcement of federal anti-marijua-na laws in states that have legalized recreational marijuana, but the memorandum was rescinded by then Attorney General Jeff Sessions.
The medical use of cannabis is legalized, with a physician’s recommendation, in 33 states and the District of Columbia. The Rohrabacher-Farr amendment that prohibits federal prosecution of individuals complying with state medical cannabis laws became law in December, 2014, but must be
renewed each fiscal year to remain in effect. Four-teen additional states have laws that limit tetra-hydrocannabinol (THC) content to allow access to products that are rich in cannabidiol (CBD), a non-psychoactive component of marijuana.
Although the use of cannabis remains fed-erally illegal and the substance is categorized as a Schedule I drug, some of its derivatives have been approved by the Food and Drug Administration (FDA) for prescription use. Those drugs that have received FDA approval in-clude Marinol (THC), Syndros (THC), Cesamet (nabilone), and Epidiolex (CBD).
Marijuana is prescribed for children as well as adults, provided the child has parental permission and physician certification. Most pediatric patients using marijuana for medical indications suffer from
Current Reviews for Nurse Anesthetists® designates this lesson for 1.5 contact hours in Pharmacology/Therapeutics.

124 Current Reviews for Nurse Anesthetists®
debilitating, chronic conditions such as refractory epilepsy or chronic pain. Medical administration in children is usually via either the oral or topical route rather than the inhalational route.
In addition to its medical and recreational use, cannabis may also be used for spiritual or religious purposes. Indeed, cannabis has enjoyed sacred sta-tus in several religions and has functioned as an entheogen in the Indian subcontinent since the Ve-dic period dating back to approximately 1500 BCE, if not earlier.
Although the cultivation, possession, and use of marijuana is illegal in the majority of nations worldwide, in 2016, a CBS news presentation re-ported that 51% of people in the United States had used cannabis in their lifetime for a variety of reasons, approximately 12% had used it in the past year, and 7.3% had used it in the past month. Marijuana use in the United States is three times higher than the global average, but consistent with consumption in other Western democracies. Be-cause the number of individuals using marijuana regularly is growing, and since these patients may require surgery, it is important for anesthesia pro-viders to understand the pharmacology of cannabis and its synthetic derivatives, as well as the periop-erative implications of regular marijuana use.
This lesson is not intended to debate the pros and cons of regular marijuana use. Rath-er, the purpose of the lesson is to acknowledge that regular, widespread use of marijuana is a real-ity, and it behooves clinicians to be knowledgeable about the multiple potential drug interactions and other signifi cant perioperative complications that can occur in patients who regularly use marijuana.
PharmacologyIndigenous to Central Asia and the Indian sub-continent where cannabis plants have been grown
since at least the third millennium BCE, cannabis was used for fabric and rope in the Neolithic age in China and Japan. It is unclear exactly when the psychoactive properties of cannabis were fi rst rec-ognized, but evidence indicates that cannabis was known to the ancient Assyrians, who discovered its psychoactive properties through the Iranians. Evi-dence suggests that cannabis was smoked for its psychoactive effects at least 2,500 years ago in the Pamir Mountains.
Also known as hemp or marijuana, the cannabis plant is one of the most ancient documented medi-cations in history. Although the pharmacologic ef-fects of cannabis have been exploited for several millennia for medicinal purposes, it is only during the last few decades that important scientifi c dis-coveries have signifi cantly advanced our knowl-edge of cannabinoids.
Cannabis is said to contain more than 500 chemical compounds, 104 of which are active can-nabinoids; the rest are fl avonoids, terpenes, fatty acids, and numerous other compounds, all with po-tential medicinal uses.
Of the more than 70 phytocannabinoids in marijuana, the three main cannabinoids are delta-9 tetrahydrocannabinol (Δ-9 THC), CBD, and cannabinol (CBN).
Recently, endogenous cannabinoids were discov-ered, the two principal ones being anandamide and 2-arachidonoylglycerol. As mentioned, CBD lacks psychoactive properties, whereas cannabinol is a mildly psychoactive chemical. The canna-bis compounds interact with two identifi ed recep-tors, CB1 and CB2. The former is found predomi-nantly in the central nervous system (CNS), where activation mediates psychoactive effects. CB2 re-ceptors are located mainly in peripheral tissues with immune function and their action is being studied for use in conditions that might respond to anti-infl ammatory and antineoplastic activi-ties. The CB2 receptor, however, is also expressed in neuroglial cells. While THC is an agonist at CB1 and CB2 receptors and indirectly enhances dopa-mine release and produces psychotropic effects, CBD has potentiating effects and possible antago-nistic effects at CB1 and CB2 receptors, providing sedating, anti-epileptic, and anti-emetic actions in the absence of psychotropic effects. CBD also acts as an allosteric modulator of μ- and δ-opioid recep-tors. It has not been determined whether, or how, these actions contribute to the effects of cannabis.
Many patients use cannabis oils, which are pre-pared by a variety of methods, with the concentra-tion of THC and CBD dependent on temperature and time of extraction. CBD oils typically are ad-ministered sublingually, but may be sprinkled on
BCE Before the common eraCBD Cannabidiol CBN CannabinolCNS Central nervous systemEEG ElectroencephalogramFDA Food and Drug AdministrationHIV/AIDS Human immunodefi ciency virus/ Acquired immunodefi ciency syndromeIOP Intraocular pressureLGS Lennox-Gastaut syndromeTHC Tetrahydrocannabinol
Acronyms

125Curr Rev Nurs Anesth 44(10):121-132 2021
food or applied directly to a painful site. A recent investigation identifi ed wide variability in both the concentration and the ratio of THC and CBD in these oils. The one exception is Charlotte’s Web, the high-concentration CBD oil produced in Colorado, which consistently contains <0.3% THC. Charlotte’s Web is named after Charlotte Figi, born in 2006, whose story has resulted in her being de-scribed as “the girl who is changing medical mari-juana laws across America.” Charlotte experienced a reduction of her epileptic seizures brought on by Dravet syndrome after her fi rst dose of medical marijuana at fi ve years of age. (Charlotte’s Web was initially called “Hippie’s Disappointment” be-cause it is a strain that had a high concentration of CBD and could not induce a “high”). Three phase 3 clinical trials completed in 2017 demonstrated the effi cacy of CBD in reducing convulsive seizure ac-tivity at doses of 10-20 mg/kg per day in children with treatment-resistant Dravet syndrome and treatment-resistant Lennox-Gastaut syndrome (LGS) (Table 1).
Cannabis can be consumed by smoking, vaporiz-ing, or ingesting within food, or used as an extract. When smoked, onset of effects typically is experi-enced within minutes; when cooked and ingested, onset usually occurs within 30 to 60 minutes. Ef-fects generally last for two to six hours. Cannabis is mainly metabolized by CYP3A4 and CYP2C9 en-zymes in the liver, and interactions are possible with other medications similarly metabolized. (These interactions will be elucidated later in this lesson). The plasma elimination half-life of marijuana is 56 hours (shorter with chronic use) and its tissue half-life is fi ve to 13 days, with total excretion taking up to 25 days. Metabolites are eliminated via uri-nary excretion or secreted through the biliary tract. The high lipid solubility of cannabinoids re-sults in signifi cant accumulation in the body, especially in the lipid membranes of neurons.
Purported Indications for Medical Use of Marijuana
There is no universally agreed-upon defi nition as to what constitutes the medical use of marijuana. Specifi cally, there is no consensus as to whether cannabis is used to treat disease or ameliorate symptoms. The cannabinoids available to treat certain disorders include predominantly phytocan-nabinoids (with varying THC and/or CBD constitu-ents) and synthetic cannabinoids, such as nabilone, dronabinol (trade names Marinol or Syndros), and nabiximols (THC-CBD extracts). There is some evidence suggesting cannabinoids can be used to reduce nausea and vomiting during chemotherapy, stimulate appetite in people with human immuno-defi ciency virus (HIV)/acquired immune defi ciency syndrome (AIDS), or treat chronic pain and muscle spasm. Cannabis has not been shown to be ef-fective in the management of acute pain.
Dronabinol, a synthetic THC available in oral capsules, was approved by the FDA for HIV/AIDS wasting syndrome and chemotherapy-induced nau-sea and vomiting. Nabilone, a synthetic compound similar to THC and available in oral capsules, is also approved by the FDA for chemotherapy-in-duced nausea and vomiting. Nabiximol, a purifi ed extract of THC and CBD in a 1:1 ratio, is available in a mucosal spray in the United Kingdom and Canada for neuropathic pain associated with mul-tiple sclerosis and cancer; the extract is currently under review by the FDA. Plant-derived, pure CBD (Epidiolex) is an oral solution that shows promise for treatment of epilepsy.
Suffi ce it to say that the literature supports the concept that currently available cannabinoids are somewhat effective analgesics that offer a safe therapeutic option for managing chronic non-can-cer-related pain and possibly cancer-related pain. The use of cannabis for medical applications other than those listed above is insuffi cient for drawing
Dravet syndrome, a rare genetic disorder (1:20,000-1:40,000 births), previously known as severe myo-clonic epilepsy of infancy. The syndrome is characterized by prolonged febrile and non-febrile seizures beginning in the fi rst year of life. The condition is associated with cognitive impairment, behavioral disor-ders (hyperactivity and impulsiveness), and motor defi cits. Seizures worsen as the patient ages, and tend to be drug-resistant. CBD was approved for treatment of Dravet syndrome in the US in 2018.
Lennox-Gastaut syndrome (LGS), a form of rare, complex, and severe childhood-onset epilepsy with a poor prognosis. The syndrome is characterized by multiple and concurrent seizure types, with a typical onset between the ages of three and fi ve years. It is associated with a triad of seizures, cognitive dysfunc-tion, and slow spike waves on EEG. Symptoms vary and progress with age. CBD has been reported to reduce seizure frequency.
Table 1: Characteristics of Some Syndromes Responsive to CBD Therapy

126 Current Reviews for Nurse Anesthetists®
conclusions about safety or effi cacy. There remains a need to establish acceptable risk-to-benefi t ratios.
Contraindications (relative or absolute) to medical use of cannabis include the following: age less than 25 years (in the absence of treatment-resistant convulsive epilepsy), personal or family history of psychosis, current or past history of can-nabis use disorder, active substance use disorder, notable respiratory or cardiovascular disease, and pregnancy or breast-feeding (Table 2).
Cautions regarding the medical use of cannabis involve a contemporaneous mood or anxiety disor-der, use of tobacco, risk factors for cardiac disease, and heavy use of alcohol, benzodiazepines, and/or opioids.
Physiologic Consequences of Marijuana Use
Cannabinoids are highly protein bound, in-duce cytochrome P450, and have several physiologic effects on the neurologic, cardio-vascular, and immunosuppressive systems.
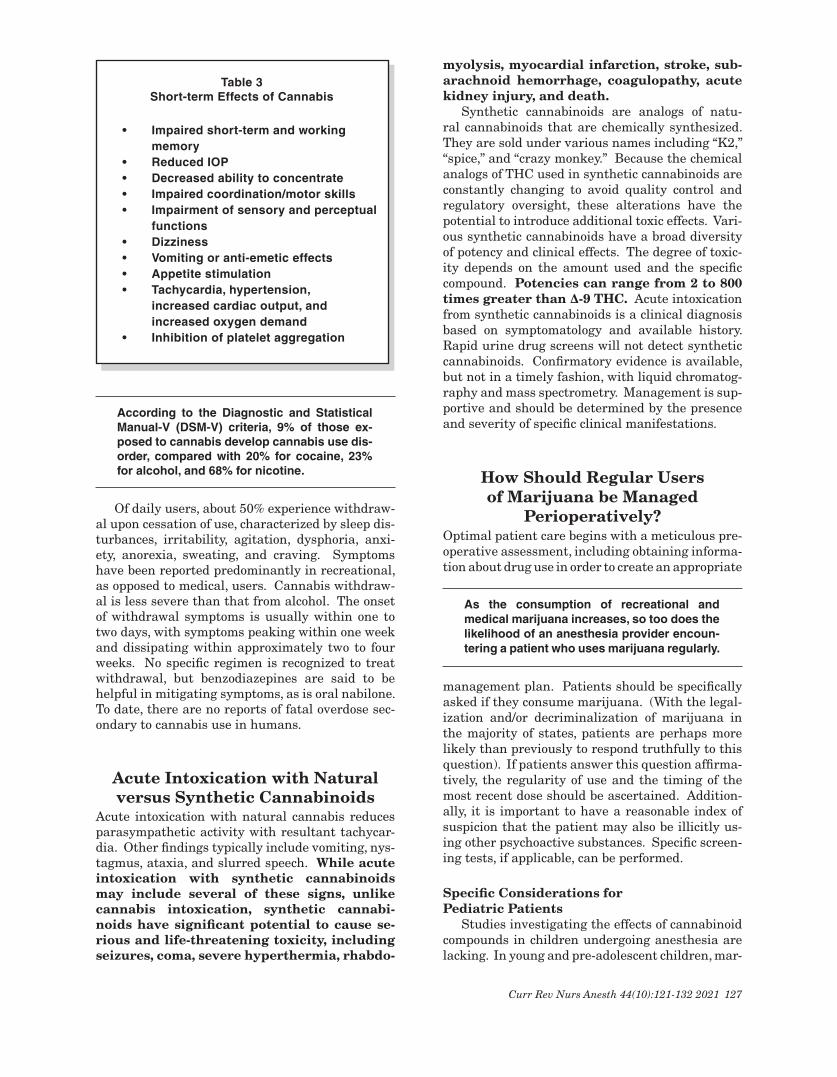
Short-term Eff ects of CannabisA myriad of fi ndings have been associated with
the short-term use of cannabis. These include, but are not limited to, impairment of short-term and working memory, reduced intraocular pressure (IOP), reduced ability to concentrate, transient impairment of sensory and perceptual functions, impaired coordination/motor skills affecting driv-ing performance, conjunctival injection, dizziness, fatigue, vomiting and/or anti-emetic effects, appe-tite stimulation and increased food consumption, delayed gastric emptying, tachycardia, increased cardiac output, increased oxygen demand, vasodi-lation, hypertension, and inhibition of platelet ag-gregation (Table 3). Moreover, the short-term ef-fects of cannabis can be altered if it has been laced with opioid drugs such as fentanyl or heroin.
Long-term Eff ects of CannabisThe long-term effects of cannabis use are char-
acterized by striking variability (Table 4), and it is important to underscore that, to date, there are no published studies in children pertaining to this issue. Although cannabis use in low doses is as-sociated with tachycardia and hypertension, bra-dycardia and orthostatic hypotension are generally associated with chronic usage and high doses. Ar-rhythmias and ST-segment and T-wave abnormali-ties have also been identifi ed.
Current knowledge suggests that adults who have chronically consumed cannabis may have an increased risk of addiction and susceptibility to cer-
tain infections. Those who started regular use as adolescents may have reduced mental acuity and augmented risk of early-onset psychosis/schizo-phrenia; behavioral problems may be more common in children whose mothers used marijuana during pregnancy. Although global abnormalities in white matter and grey matter do not appear to be asso-ciated with cannabis abuse, reduced hippocampal volume is consistently identifi ed and abnormalities in the amygdala have been inconsistently docu-mented. Evidence that marijuana damages young brains triggered an opinion piece, published June 16, 2019, in The New York Times by Drs. Kenneth L. Davis, President and CEO of Mount Sinai Medi-cal Center in Manhattan, and Mary Jeanne Kreek, an eminent researcher at Rockefeller University. These distinguished physician-scientists called for New York and New Jersey to set a minimum age of 25 years when considering their marijuana legal-ization proposals.
Cannabinoid hyperemesis syndrome is a paradoxical condition of undetermined pathogenesis characterized by hyperemesis, as opposed to the more familiar anti-emetic properties of cannabinoids. Specifi cally, mari-juana hyperemesis syndrome involves the pattern of cyclic nausea, vomiting, and cramping abdomi-nal pain in the context of chronic cannabis use. (Weekly cannabis use is usually required for the syndrome to occur). Symptoms may improve tem-porarily by taking a hot bath or shower, or by ap-plying capsaicin cream to the abdomen. Complica-tions may include electrolyte imbalance, prerenal azotemia, kidney failure, and skin burns from hot water. Death, although unusual, has been reported.
• Age <25 years (in the absence of treatment-resistant convulsive epilepsy)• Personal or family history of psychosis• Current or past history of cannabis use disorder• Active substance use disorder• Signifi cant respiratory disease• Signifi cant cardiovascular disease• Pregnancy• Breast feeding
Table 2 Contraindications to
Medical Use of Cannabis
127Curr Rev Nurs Anesth 44(10):121-132 2021
According to the Diagnostic and Statistical Manual-V (DSM-V) criteria, 9% of those ex-posed to cannabis develop cannabis use dis-order, compared with 20% for cocaine, 23% for alcohol, and 68% for nicotine.
Of daily users, about 50% experience withdraw-al upon cessation of use, characterized by sleep dis-turbances, irritability, agitation, dysphoria, anxi-ety, anorexia, sweating, and craving. Symptoms have been reported predominantly in recreational, as opposed to medical, users. Cannabis withdraw-al is less severe than that from alcohol. The onset of withdrawal symptoms is usually within one to two days, with symptoms peaking within one week and dissipating within approximately two to four weeks. No specifi c regimen is recognized to treat withdrawal, but benzodiazepines are said to be helpful in mitigating symptoms, as is oral nabilone. To date, there are no reports of fatal overdose sec-ondary to cannabis use in humans.
Acute Intoxication with Natural versus Synthetic Cannabinoids
Acute intoxication with natural cannabis reduces parasympathetic activity with resultant tachycar-dia. Other fi ndings typically include vomiting, nys-tagmus, ataxia, and slurred speech. While acute intoxication with synthetic cannabinoids may include several of these signs, unlike cannabis intoxication, synthetic cannabi-noids have signifi cant potential to cause se-rious and life-threatening toxicity, including seizures, coma, severe hyperthermia, rhabdo-
myolysis, myocardial infarction, stroke, sub-arachnoid hemorrhage, coagulopathy, acute kidney injury, and death.
Synthetic cannabinoids are analogs of natu-ral cannabinoids that are chemically synthesized. They are sold under various names including “K2,” “spice,” and “crazy monkey.” Because the chemical analogs of THC used in synthetic cannabinoids are constantly changing to avoid quality control and regulatory oversight, these alterations have the potential to introduce additional toxic effects. Vari-ous synthetic cannabinoids have a broad diversity of potency and clinical effects. The degree of toxic-ity depends on the amount used and the specifi c compound. Potencies can range from 2 to 800 times greater than ∆-9 THC. Acute intoxication from synthetic cannabinoids is a clinical diagnosis based on symptomatology and available history. Rapid urine drug screens will not detect synthetic cannabinoids. Confi rmatory evidence is available, but not in a timely fashion, with liquid chromatog-raphy and mass spectrometry. Management is sup-portive and should be determined by the presence and severity of specifi c clinical manifestations.
How Should Regular Users of Marijuana be Managed
Perioperatively?Optimal patient care begins with a meticulous pre-operative assessment, including obtaining informa-tion about drug use in order to create an appropriate
As the consumption of recreational and medical marijuana increases, so too does the likelihood of an anesthesia provider encoun-tering a patient who uses marijuana regularly.
management plan. Patients should be specifi cally asked if they consume marijuana. (With the legal-ization and/or decriminalization of marijuana in the majority of states, patients are perhaps more likely than previously to respond truthfully to this question). If patients answer this question affi rma-tively, the regularity of use and the timing of the most recent dose should be ascertained. Addition-ally, it is important to have a reasonable index of suspicion that the patient may also be illicitly us-ing other psychoactive substances. Specifi c screen-ing tests, if applicable, can be performed.
Specifi c Considerations for Pediatric Patients
Studies investigating the effects of cannabinoid compounds in children undergoing anesthesia are lacking. In young and pre-adolescent children, mar-
• Age <25 years (in the absence of treatment-resistant convulsive epilepsy)• Personal or family history of psychosis• Current or past history of cannabis use disorder• Active substance use disorder• Signifi cant respiratory disease• Signifi cant cardiovascular disease• Pregnancy• Breast feeding
• Impaired short-term and working memory• Reduced IOP• Decreased ability to concentrate• Impaired coordination/motor skills• Impairment of sensory and perceptual functions• Dizziness• Vomiting or anti-emetic effects• Appetite stimulation• Tachycardia, hypertension, increased cardiac output, and increased oxygen demand• Inhibition of platelet aggregation
Table 3 Short-term Effects of Cannabis

128 Current Reviews for Nurse Anesthetists®
ijuana is mainly used for medical indications (often refractory epilepsy) and is administered orally or topically. Use of medical marijuana in the pediatric population can pose challenges for the anesthesia provider. Predictably, parents want confi rmation and reassurance that the perioperative care team has a plan to minimize disruption of marijuana therapy during the child’s hospitalization, which can be diffi cult in the face of potential legal and institutional barriers. If the patient is on synthetic THC or CBD, it is thought to be safe to continue the dosage on the day of surgery and during the course of the child’s hospitalization. If the patient is on a plant-derived cannabis product, individual-ized decisions should be made about perioperative administration, although generally speaking, con-tinuance is safe. If perioperative anxiolysis with benzodiazepines is needed, the patient’s level of se-dation should be carefully monitored as additive ef-fects may occur. Other potential drug interactions should also be meticulously monitored and are dis-cussed below.
Adolescents may be using marijuana recre-ationally, and the American Academy of Pediatrics recommends that it should be discontinued periop-eratively. For elective procedures, inhaled (vaped or smoked) marijuana should be held for a mini-mum of 72 hours. Similar to tobacco smoking, in-haled marijuana is an airway irritant and has been associated with airway (including uvular) edema, obstruction, coughing, bronchitis, emphysema, and bronchospasm. There is a case report of intraop-erative uvular edema that was successfully treated with dexamethasone in a 17-year-old boy who had smoked marijuana shortly before induction.
The possibility of withdrawal symptoms in chronic users must be acknowledged, and the peri-
operative period may afford a teachable moment to discuss risk reduction in patients who regularly use recreational marijuana.
Adult PatientsAlthough cannabis may affect many different
systems and functions, its effects on the cardiovas-cular, respiratory, and CNS arguably are the most important interactions during the perioperative period. Smoked cannabis produces similar dam-age to the respiratory mucosa as that infl icted by tobacco, and its consequences were listed above. Acute cannabis use in low doses is associated with tachycardia and hypertension. In contrast, bra-dycardia and orthostatic hypotension are usually associated with chronic use and high doses. Supra-ventricular or ventricular ectopy has been reported with cannabis use, together with ST-segment and T-wave abnormalities. A study of adults aged 20 to 92 years who had sustained a myocardial infarc-tion showed that the risk increased almost 5-fold in the fi rst hour after smoking marijuana due to an increase in cardiac output, myocardial oxygen demand, catecholamine levels, and carboxyhemo-globin as well as postural hypotension.
Marijuana not infrequently is used and/or abused by women of childbearing age. Delta-9 THC crosses the placenta and the blood-brain barrier; its use may directly affect the fetus. Marijuana con-sumption in pregnant women has been associated with intrauterine growth retardation and preterm labor. Cannabinoids are highly lipid soluble and accumulate in breast milk. Marijuana consump-tion during pregnancy has been associated with ventricular septal defect (in the fetus) as well as delayed cognitive development. Parturients who chronically use marijuana have an increased risk of respiratory complications, and acute marijuana use may be associated with cardiovascular stimula-tion at moderate doses and myocardial depression at higher doses.
Because cannabis is predominantly metab-olized by CYP3A4 and CYP2C9 in the liver, in-teractions are possible---and unpredictable---with other medications that undergo similar metabolism. For CYP3A4, these substances in-clude fentanyl, oxycodone, codeine, and others. For CYP2C9, these drugs include warfarin, clopidogrel, nonsteroidal anti-infl ammatory drugs (NSAIDs), and celecoxib. The clinical effects of these interac-tions are diffi cult to predict, and both an increase and a decrease in hepatic metabolism is possible. Hence, either an additive or an attenuated effect may be seen. When cannabis is combined with sed-ative drugs, such as alcohol, hypnotics, or benzodi-azepines, an increased level of fatigue is observed. When marijuana is consumed with excitatory sub-stances, such as amphetamines or cocaine, an in-
• Enormous variability in conse- quences of long-term use• Bradycardia• Orthostatic hypotension• Increased risk of early-onset psychosis/schizophrenia • Decreased hippocampal volume• Cannabinoid hyperemesis syndrome• Increased risk of cannabis use disorder• 50% incidence of withdrawal upon cessation of use
Table 4 Long-term Effects of Cannabis
129Curr Rev Nurs Anesth 44(10):121-132 2021
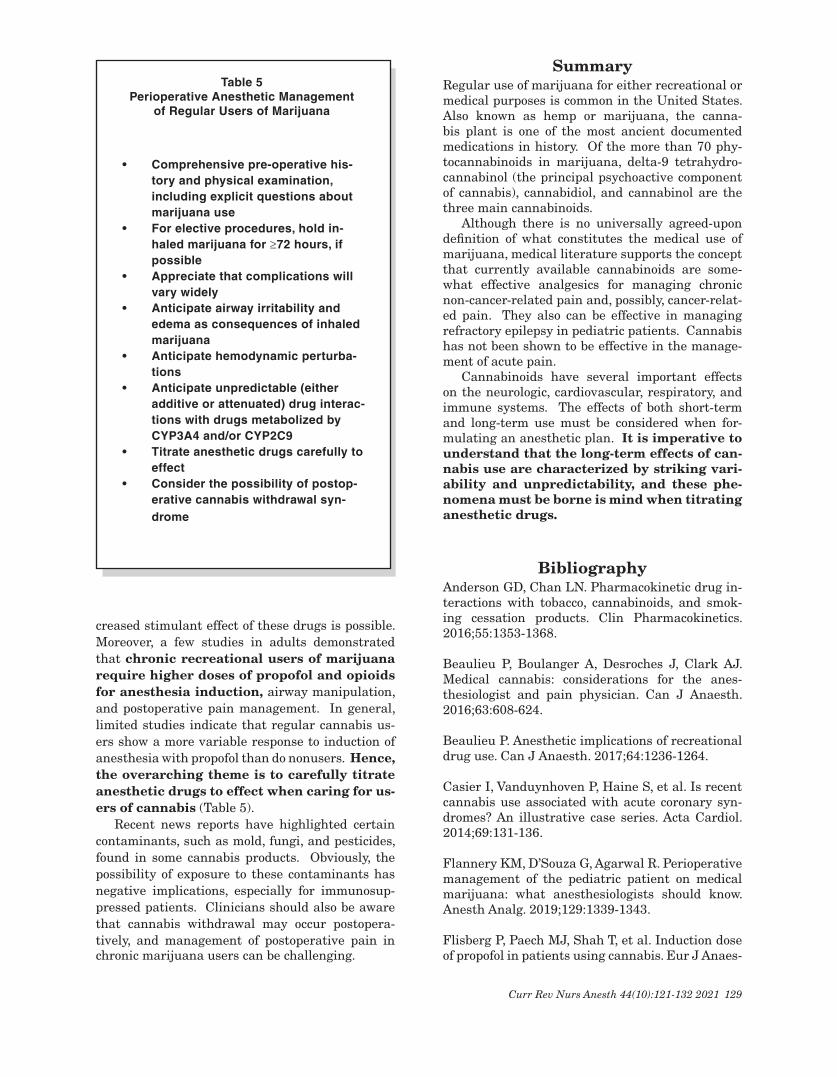
creased stimulant effect of these drugs is possible. Moreover, a few studies in adults demonstrated that chronic recreational users of marijuana require higher doses of propofol and opioids for anesthesia induction, airway manipulation, and postoperative pain management. In general, limited studies indicate that regular cannabis us-ers show a more variable response to induction of anesthesia with propofol than do nonusers. Hence, the overarching theme is to carefully titrate anesthetic drugs to effect when caring for us-ers of cannabis (Table 5).
Recent news reports have highlighted certain contaminants, such as mold, fungi, and pesticides, found in some cannabis products. Obviously, the possibility of exposure to these contaminants has negative implications, especially for immunosup-pressed patients. Clinicians should also be aware that cannabis withdrawal may occur postopera-tively, and management of postoperative pain in chronic marijuana users can be challenging.
SummaryRegular use of marijuana for either recreational or medical purposes is common in the United States. Also known as hemp or marijuana, the canna-bis plant is one of the most ancient documented medications in history. Of the more than 70 phy-tocannabinoids in marijuana, delta-9 tetrahydro-cannabinol (the principal psychoactive component of cannabis), cannabidiol, and cannabinol are the three main cannabinoids.
Although there is no universally agreed-upon defi nition of what constitutes the medical use of marijuana, medical literature supports the concept that currently available cannabinoids are some-what effective analgesics for managing chronic non-cancer-related pain and, possibly, cancer-relat-ed pain. They also can be effective in managing refractory epilepsy in pediatric patients. Cannabis has not been shown to be effective in the manage-ment of acute pain.
Cannabinoids have several important effects on the neurologic, cardiovascular, respiratory, and immune systems. The effects of both short-term and long-term use must be considered when for-mulating an anesthetic plan. It is imperative to understand that the long-term effects of can-nabis use are characterized by striking vari-ability and unpredictability, and these phe-nomena must be borne is mind when titrating anesthetic drugs.
BibliographyAnderson GD, Chan LN. Pharmacokinetic drug in-teractions with tobacco, cannabinoids, and smok-ing cessation products. Clin Pharmacokinetics. 2016;55:1353-1368.
Beaulieu P, Boulanger A, Desroches J, Clark AJ. Medical cannabis: considerations for the anes-thesiologist and pain physician. Can J Anaesth. 2016;63:608-624.
Beaulieu P. Anesthetic implications of recreational drug use. Can J Anaesth. 2017;64:1236-1264.
Casier I, Vanduynhoven P, Haine S, et al. Is recent cannabis use associated with acute coronary syn-dromes? An illustrative case series. Acta Cardiol. 2014;69:131-136.
Flannery KM, D’Souza G, Agarwal R. Perioperative management of the pediatric patient on medical marijuana: what anesthesiologists should know. Anesth Analg. 2019;129:1339-1343.
Flisberg P, Paech MJ, Shah T, et al. Induction dose of propofol in patients using cannabis. Eur J Anaes-
• Comprehensive pre-operative his- tory and physical examination, including explicit questions about
marijuana use• For elective procedures, hold in- haled marijuana for ≥72 hours, if
possible• Appreciate that complications will
vary widely• Anticipate airway irritability and
edema as consequences of inhaled marijuana
• Anticipate hemodynamic perturba- tions• Anticipate unpredictable (either
additive or attenuated) drug interac- tions with drugs metabolized by
CYP3A4 and/or CYP2C9• Titrate anesthetic drugs carefully to
effect• Consider the possibility of postop- erative cannabis withdrawal syn- drome
Table 5 Perioperative Anesthetic Management
of Regular Users of Marijuana

130 Current Reviews for Nurse Anesthetists®
thesiol. 2009;26:192-195.
Friedman D, Devinsky O. Cannabinoids in the treatment of epilepsy. N Engl J Med. 2015;373:1048-1058.
Galli JA, Sawaya RA, Friedenberg FK. Cannabi-noid hyperemesis syndrome. Curr Drug Abuse Rev. 2011:4:241-249.
Hill KP. Medical marijuana for treatment of chronic pain and other medical and psychiatric problems: a clinical review. JAMA. 2015; 313:2474-2483.
Mittleman MA, Lewis RA, Maclure M, et al. Trig-gering myocardial infarction by marijuana. Circu-
lation. 2001;103:2805-2809.
Ryan SA, Ammerman SD; Committee on Substance Use and Prevention. Counseling parents and teens about marijuana use in the era of legalization of marijuana. Pediatrics. 2017;139e20164069.
Thomas G, Kloner RA, Rezkalla S. Adverse cardio-vascular, cerebrovascular, and peripheral vascular effects of marijuana inhalation: what cardiologists need to know. Am J Cardiol. 2014;113:187-190.
Ware MA, Ziemianski D. Medical education on can-nabis and cannabinoids: perspectives, challenges, and opportunities. Clin Pharm Ther. 2015;97:548-550.
Kathryn E. McGoldrick, MD, FCAI (Hon)Dr. McGoldrick, a graduate of Dartmouth College and Cornell University Medical College,
served for 15 years as Professor and Chair of Anesthesiology at New York Medical College, where she also was Residency Program Director and Advisory Dean for Medical Student Affairs. She was previously on the faculty of Harvard Medical School and then Yale University School of Medicine. Currently, she works full time for the Accreditation Council for Graduate Medical Education (AC-GME) in the Department of Institutional Accreditation, focusing on the Clinical Learning Environ-ment Review (CLER).
Dr. McGoldrick completed residency training in Anesthesiology at Brigham and Women’s Hos-pital in Boston, followed by subspecialty training in Pediatric Anesthesiology at Boston Children’s Hospital. She has authored more than 85 book chapters and more than 120 articles. Dr. McGold-rick also has authored or edited 17 books. She served from 2009 to 2013 on the Executive Com-mittee of the International Association for Ambulatory Surgery (IAAS), and from 2005-2014 on the Board of the Foundation for Anesthesia Education and Research (FAER). Dr. McGoldrick has served as President of multiple organizations, including the Wood Library Museum of Anesthesi-ology, the Connecticut State Society of Anesthesiologists, the Society for Ambulatory Anesthesia (SAMBA), and The Academy of Anesthesiology. A member of Alpha Omega Alpha honor medical society, Dr. McGoldrick was the 2013 recipient of the SAMBA Distinguished Service Award (DSA), and in 2014 was awarded Honorary Fellowship in the College of Anaesthetists of Ireland. In 2017, she received the DSA of the Wood Library-Museum of Anesthesiology.
Dr. McGoldrick currently serves on the Board of the Anesthesia Foundation and is a Fellow of the New York Academy of Medicine. She was Chief Editor of Survey of Anesthesiology for 22 years, until 2017, and continues to serve on the Editorial Board of Current Reviews in Clinical Anes-thesia®. Dr. McGoldrick delivered the Lewis H. Wright Memorial Lecture at the 2018 American Society of Anesthesiologists Annual Meeting in San Francisco, discussing “Airway Management through the Ages.” She also delivered the 2017 Ether Day Lecture at Massachusetts General Hos-pital/Harvard Medical School and the 2019 Allen I. Hyman Lecture on the History of Medicine and Anesthesiology at Columbia Presbyterian Hospital/Columbia University College of Physicians and Surgeons. Her interests outside medicine include travel, photography, volunteer work, and writing essays and poetry.

131Curr Rev Nurs Anesth 44(10):121-132 2021
Tips for Your Clinical Practice: Key Points
Monte Lichtiger, MDEditor, Current Reviews®
● The likelihood of an anesthesia provider caring for a patient who regularly uses marijuana has increased since the legalization of marijuana in many states. A corollary to this is that patients will now be more truthful about their marijuana use.
● Low doses of cannabis are associated withtachycardia and hypertensionwhile chronic use and higher doses are associated withbradycardia and orthostatic hypotension.Arrhythmias and ST-segment and T-wave abnormalities have also been identified.
● Pediatric patients receiving marijuana for epilepsyneed to have the disruption of this therapy minimized during their hospitalization.
● Inhaled marijuana useshould be discontinued for at least 72 hours prior to elective surgery. It is an airway irritant that has been associated with airway edema, obstruction, coughing, bron- chitis, emphysema, and bronchospasm.
● The risk of a myocardial infarction is increased almost 5-fold in the first hour after smoking marijuana due to increases in cardiac output, myocardial oxygen demand, catecholamine levels and carboxyhemoglobin levels.
● Regular cannabis users showamore variable response to drugsused during anesthesia. Anesthesia providers shouldcarefully titrateanesthetic drugs to effect when caring for these patients.
FRANK MOYA CONTINUING EDUCATION PROGRAMS, INC. & FACULTY DISCLOSURE
THIS AUTHOR’S AND FMCEP’S SPECIFIC DISCLOSURES:
● The author / faculty has indicated that there is no relevant financial interest or relationship with any commercial interest.● The author / faculty has indicated that, as appropriate, he/she has disclosed that a product is not labeled for the use under discussion, or is still under investigation.● As a matter of policy, FMCEP does not have any relevant financial interest or relationship with any commercial interest. In addition, all members of the staff, Governing Board, Editorial Board and CME Committee who may have a role in planning this activity have indicated that there is no relevant financial interest or relationship with any commercial interest.● Current Reviews® is intended to provide its subscribers with information that is relevant to anesthesia providers. However, the information published herein reflects the opinions of its authors. Anesthesia practitioners must utilize their knowledge, training and experience in their clinical practice of anesthesiology. No single publication should be relied upon as the proper way to care for patients. DESIGNATION OF SPECIFIC CONTENT AREAS:
Current Reviews for Nurse Anesthetists® (CRNA) is designed to meet the standards and criteria of the American Association of Nurse Anesthetists (AANA) for the prior approved continuing medical education activity, Provider-Directed Independent Study, also known as home-study. CRNA is an ap-proved program provider.
CRNA has designated the lessons which meet specific content areas such as Pharmacology, HIV/AIDS, etc. However, only the Board of Nursing of an individual State is the final authority in the determination of whether or not these lessons meet the State’s licensure requirements.

MARK ONLY THE ONE BEST ANSWER PER QUESTION ON YOURANSWER CARD OR ONLINE EXAM FORM AT WWW.CURRENTREVIEWS.COM
MARK THIS PAGE AND KEEP FOR YOUR RECORDS.
POST-STUDY QUESTIONS
LESSON
MARK ALL ANSWERS ON BOTH THIS PAGE AND YOUR ANSWER CARD 10
1. Marijuana:□A. IscategorizedasaScheduleIIdrug.□B. Isfederallylegal.□C. Useislegalordecriminalizedinthemajorityof statesandtheDistrictofColumbia.□D. Isillegaltoadministertochildren.
2. Cannabis is administered by all of the following routes EXCEPT: □A. Smoking.□B. Vaporizing.□C. Ingesting.□D. Intravenously.
3. Cannabidiol:□A. HasahighconcentrationofTHC.□B. Isacomponentofmanycannabisoils.□C. Hasnotablepsychoactiveproperties,inducinga pronounced“high".□D. Isineffectivefortreatingmedicalconditions.
4. Charlotte’s Web: □A. Isahigh-concentrationCBDoilproducedin Colorado.□B. Consistentlycontains<0.3%THC.□C. Appearstohaveefficacyinreducingconvulsive seizureactivityinchildrenwithrefractoryDravet syndrome.□D. Alloftheabove.
5. Cannabis:□A. Hasnotbeenshowntobeeffectiveinmanaging acutepain.□B. Hasnoknowncontraindications.□C. Issafeforuseinpregnancy.□D. Isofnovalueinstimulatingappetiteinpatients withHIV/AIDS.
6. Contraindications to medical use of cannabis include all of the following EXCEPT:□A. Glaucoma.□B. Personalorfamilyhistoryofpsychosis.□C. Significantcardiovasculardisease.□D. Currentorpasthistoryofcannabisusedisorder.
7. Marijuana: □A..Undergoesesterhydrolysis.□B. Ishighlylipidsoluble.□C. Hasanextremelybriefplasmaeliminationhalf-life.□D. Doesnotaccumulatesignificantlyinthebody.
8. Cannabinoid hyperemesis syndrome:□A. Iscommoninsporadicusersofmarijuana.□B. Hasnoknownseriousconsequences.□C. Isresponsivetotreatmentwithopioids.□D. Ischaracterizedbycyclicepisodesofnausea, vomiting,andabdominalcramping.
Moving?
Please notify us at least 4 weeks before you move to your new address, so you won’t miss any issues of your subscription.
The post office will not forward your subscription to Current Reviews for Nurse Anesthetists®.
Phone: (954) 763-8003 or Fax: (954) 762-9111Email: [email protected]