clinical observation of montelukast as a partner agent for complementary therapy
Post on 19-Dec-2015
231 views
TRANSCRIPT

Clinical Observation of Montelukast as a Partner Agent for Complementary
Therapy
Study Objectives
• To compare the clinical benefits of adding montelukast to inhaled budesonide with doubling the dose of inhaled budesonide in adult patients who were symptomatic on inhaled budesonide alone
Price DB et al Thorax 2003;58:211-216.
• Patients aged between 15 and 75 years • Diagnosed with asthma for >1 year• Asthma not optimally controlled (as judged
by investigator) • Regular use of inhaled corticosteroids • Baseline FEV1 value 50% predicted• Beta-agonist reversibility in FEV1 12%• Symptoms requiring 1 puff / day of
beta agonist
Inclusion Criteria
Price DB et al Thorax 2003;58:211-216.
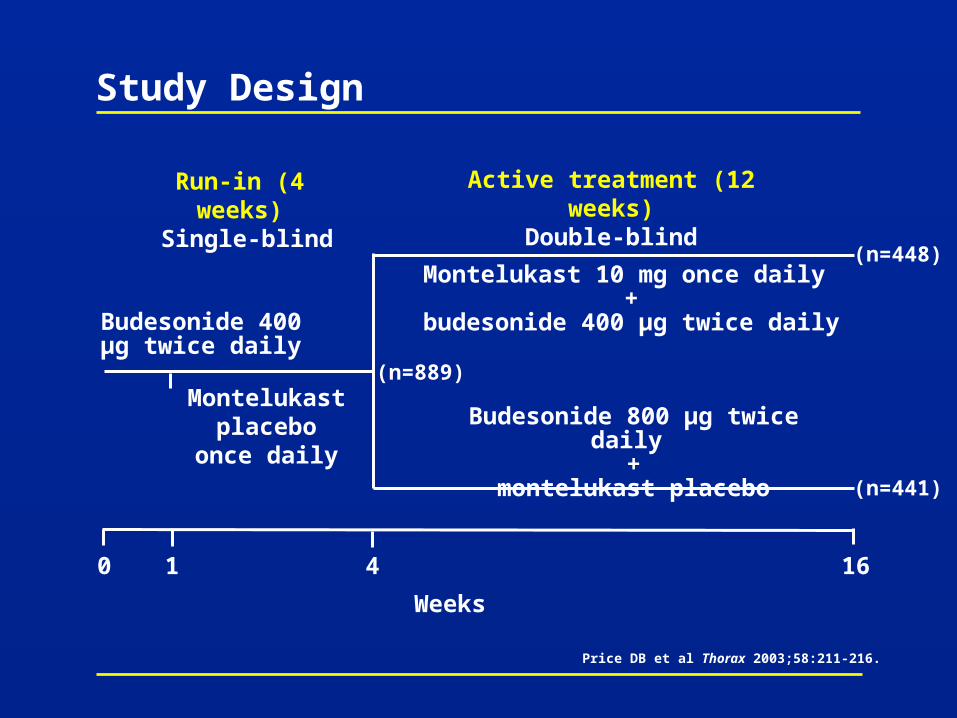
Study Design
Montelukast 10 mg once daily +
budesonide 400 µg twice daily
Budesonide 800 µg twice daily +
montelukast placebo
Budesonide 400 µg twice daily
Run-in (4 weeks) Single-blind
Active treatment (12 weeks)Double-blind
0 4 16
Weeks
1
Montelukastplacebo
once daily
(n=889)
(n=448)
(n=441)
Price DB et al Thorax 2003;58:211-216.
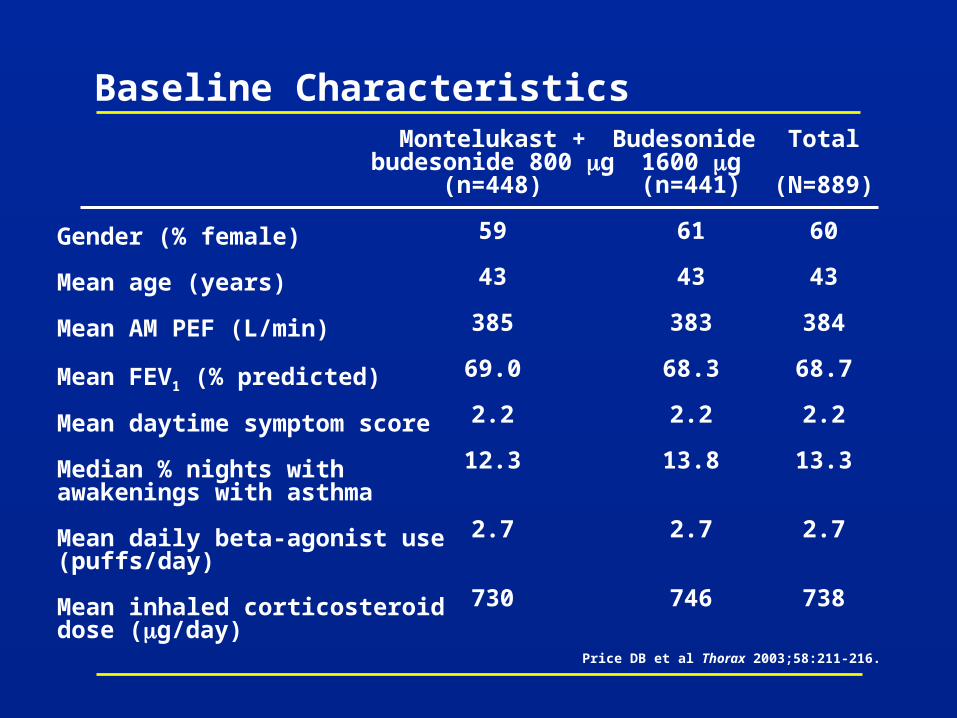
Baseline Characteristics
Gender (% female)
Mean age (years)
Mean AM PEF (L/min)
Mean FEV1 (% predicted)
Mean daytime symptom score
Median % nights with awakenings with asthma
Mean daily beta-agonist use (puffs/day)
Mean inhaled corticosteroid dose (g/day)
Montelukast +budesonide 800 g
(n=448)
59
43
385
69.0
2.2
12.3
2.7
730
Budesonide 1600 g(n=441)
61
43
383
68.3
2.2
13.8
2.7
746
Price DB et al Thorax 2003;58:211-216.
Total
(N=889)
60
43
384
68.7
2.2
13.3
2.7
738
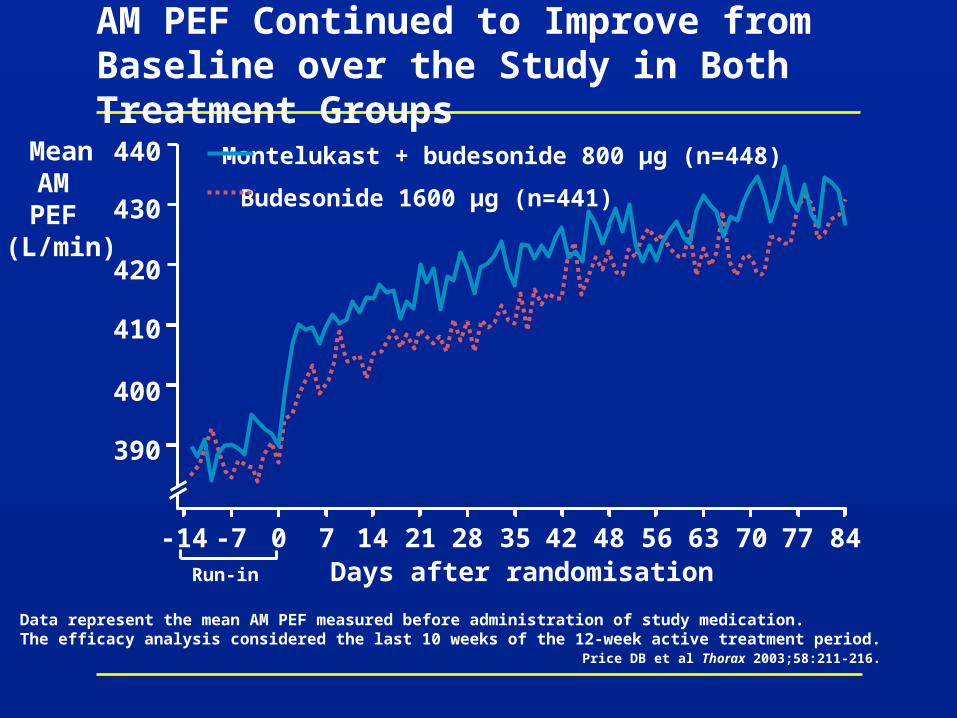
AM PEF Continued to Improve from Baseline over the Study in Both Treatment Groups
MeanAM PEF
(L/min)
Days after randomisation-14 -7 0 7 14 21 28 35 42 48 56 63 70 77 84
Montelukast + budesonide 800 µg (n=448)
Budesonide 1600 µg (n=441)
440
390
400
410
420
430
Run-in
Price DB et al Thorax 2003;58:211-216.
Data represent the mean AM PEF measured before administration of study medication. The efficacy analysis considered the last 10 weeks of the 12-week active treatment period.
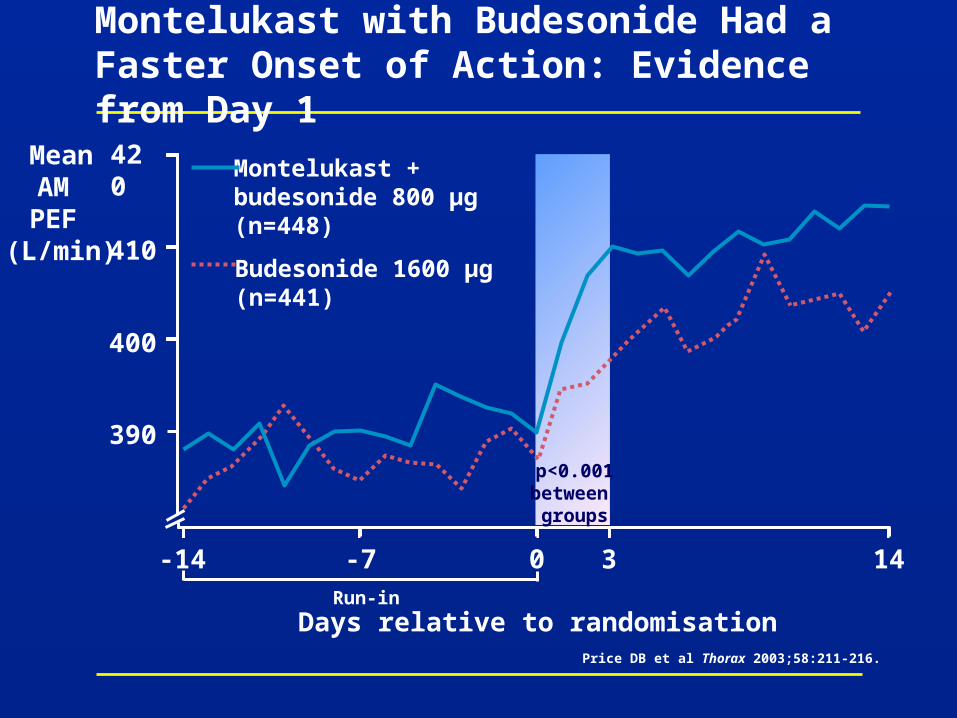
Montelukast with Budesonide Had a Faster Onset of Action: Evidence from Day 1
MeanAM PEF
(L/min)
Days relative to randomisation
420
Run-in
390
400
410
Montelukast + budesonide 800 µg (n=448)
Budesonide 1600 µg (n=441)
-14 -7 0 14
3
p<0.001between groups
Price DB et al Thorax 2003;58:211-216.
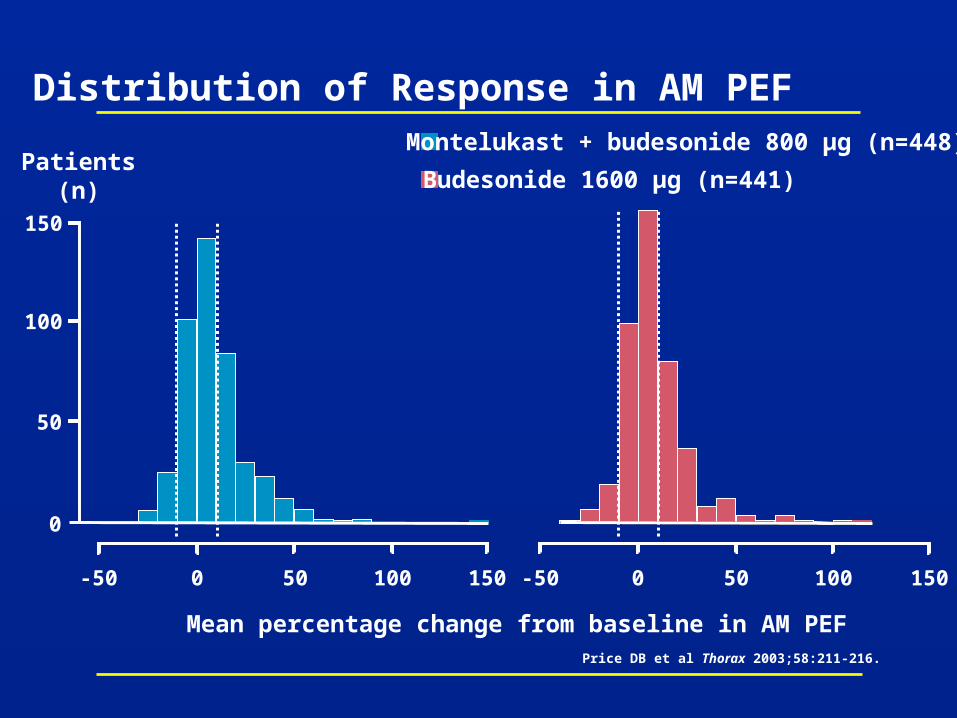
Mean percentage change from baseline in AM PEF
Patients(n)
0
50
100
150
-50 0 50 100 150 -50 0 50 100 150
Distribution of Response in AM PEFMontelukast + budesonide 800 µg (n=448)
Budesonide 1600 µg (n=441)
Price DB et al Thorax 2003;58:211-216.
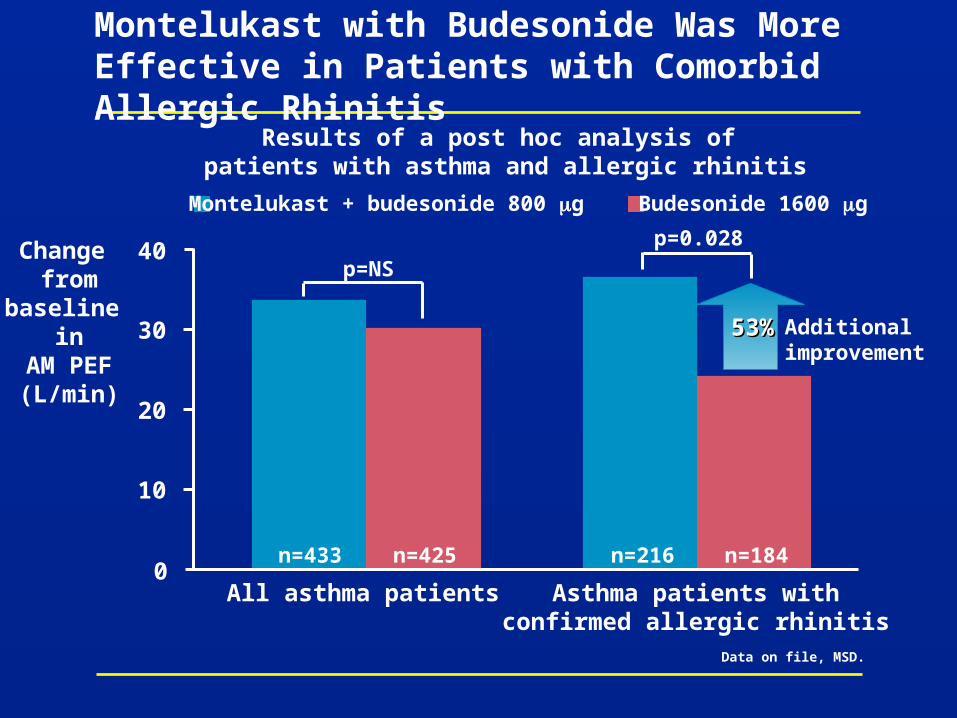
Montelukast with Budesonide Was More Effective in Patients with Comorbid Allergic Rhinitis
Data on file, MSD.
Montelukast + budesonide 800 g Budesonide 1600 g
Change from
baseline in
AM PEF(L/min)
All asthma patients Asthma patients withconfirmed allergic rhinitis
0
10
20
30
40p=NS
n=433 n=425 n=216 n=184
p=0.028
Results of a post hoc analysis of patients with asthma and allergic rhinitis
53%53% Additionalimprovement
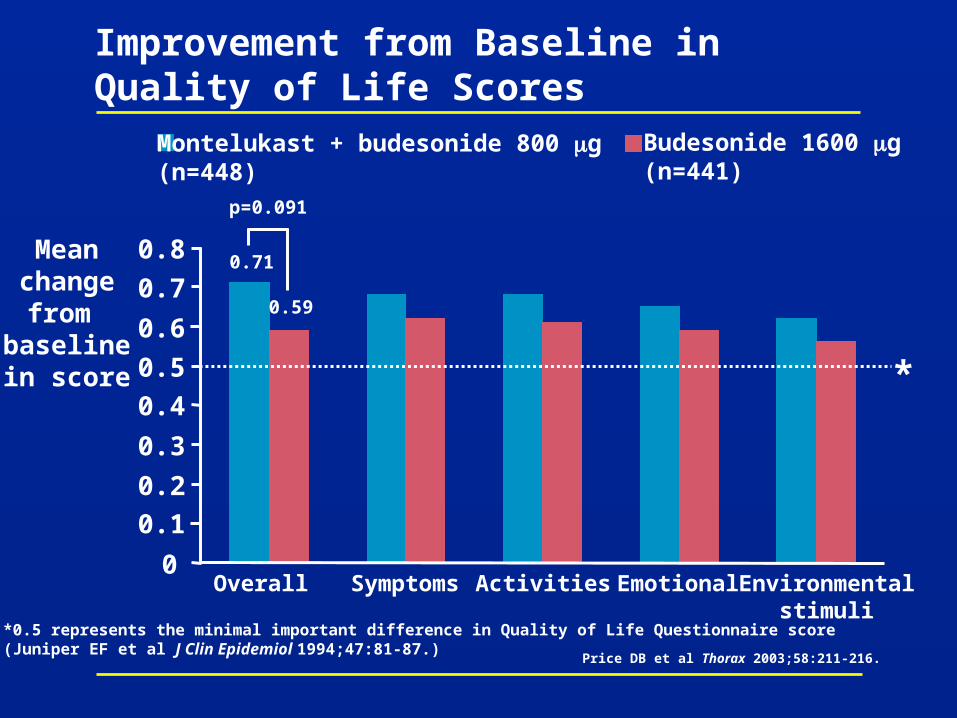
Improvement from Baseline in Quality of Life Scores
Montelukast + budesonide 800 g(n=448)
Budesonide 1600 g(n=441)
Meanchangefrom
baselinein score
*0.5 represents the minimal important difference in Quality of Life Questionnaire score (Juniper EF et al J Clin Epidemiol 1994;47:81-87.)
p=0.091
Overall Symptoms Activities Emotional Environmentalstimuli
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8 0.71
0.59
*
Price DB et al Thorax 2003;58:211-216.

Average Daily Use of Beta Agonist
Meanbeta-agonist
use(puffs/day)
p=0.510
Budesonide 1600 g (n=441)
Montelukast + budesonide 800 g (n=448)3.0
2.8
2.6
2.4
2.2
2.0
Weeks after randomisation0 2 4 6 8 10 12
Price DB et al Thorax 2003;58:211-216.
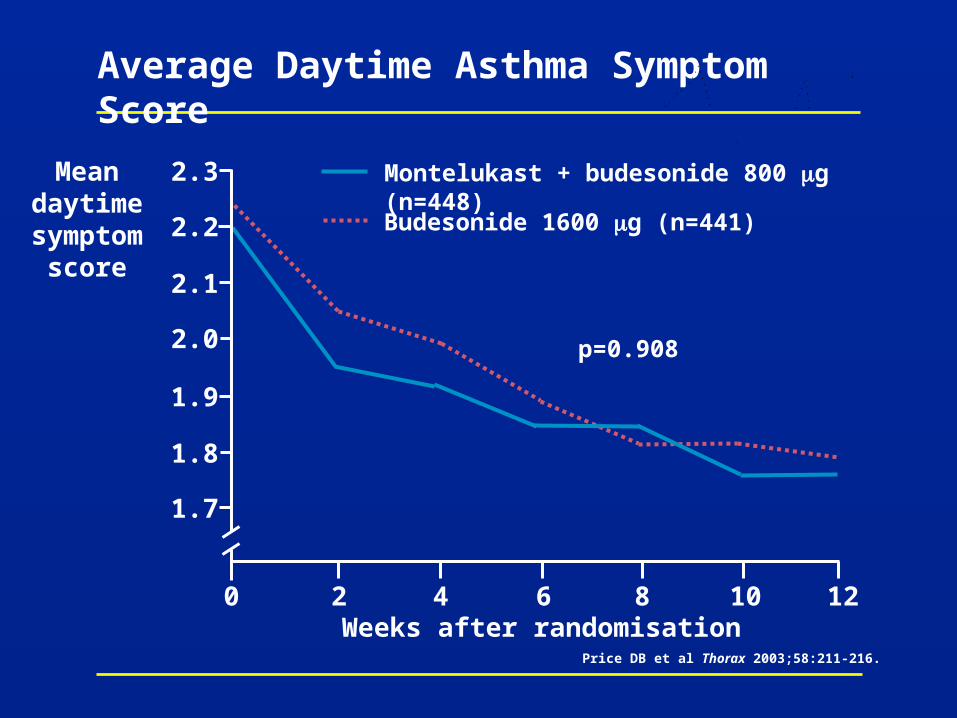
Meandaytime
symptomscore
Average Daytime Asthma Symptom Score
0 2 4 6 8 10 12
2.3
2.2
2.1
2.0
1.9
1.8
1.7
p=0.908
Weeks after randomisation
Budesonide 1600 g (n=441)
Montelukast + budesonide 800 g (n=448)
Price DB et al Thorax 2003;58:211-216.
Asthma Exacerbations andAsthma-Free Days
• An asthma exacerbation day was defined as a day with any one of the following events– A decrease from baseline in AM PEF of >20%– AM PEF <180 L/min– An increase from baseline in beta-agonist use of >70% (and a minimum increase of 2 puffs)– An increase from baseline in symptom score of 50%– An asthma attack
• An asthma-free day was defined as a day free of:– Oral corticosteroid use– Emergency care– Nocturnal awakenings
with use of 2 puffs of beta agonist
Price DB et al Thorax 2003;58:211-216.
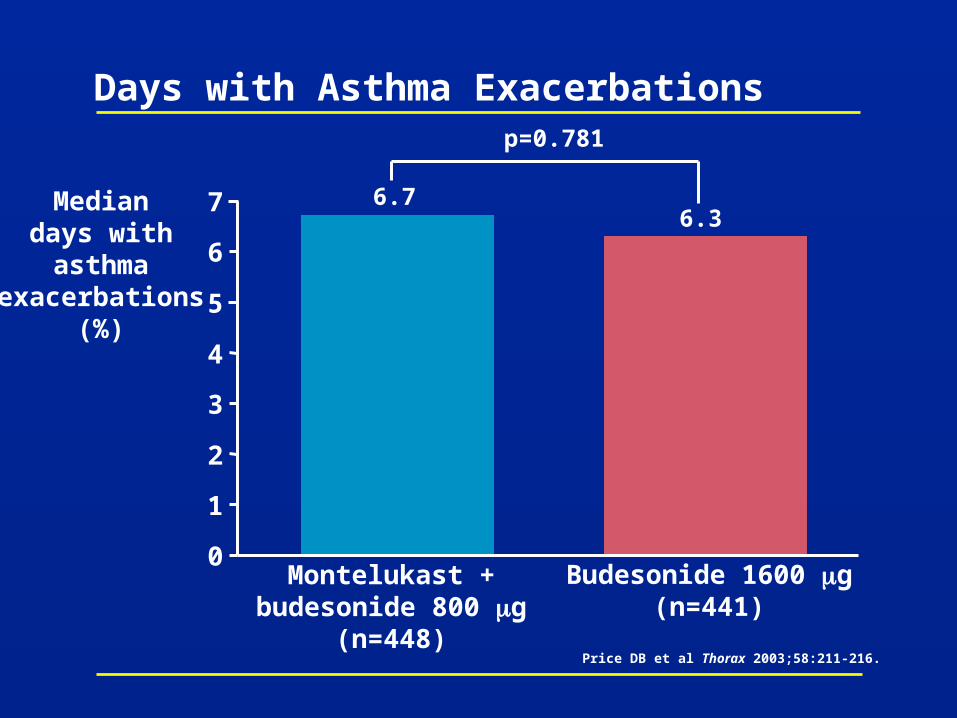
Days with Asthma Exacerbations
Montelukast +budesonide 800 g
(n=448)
Mediandays withasthma
exacerbations(%)
Budesonide 1600 g(n=441)
p=0.781
0
1
2
3
4
5
6
7 6.76.3
Price DB et al Thorax 2003;58:211-216.
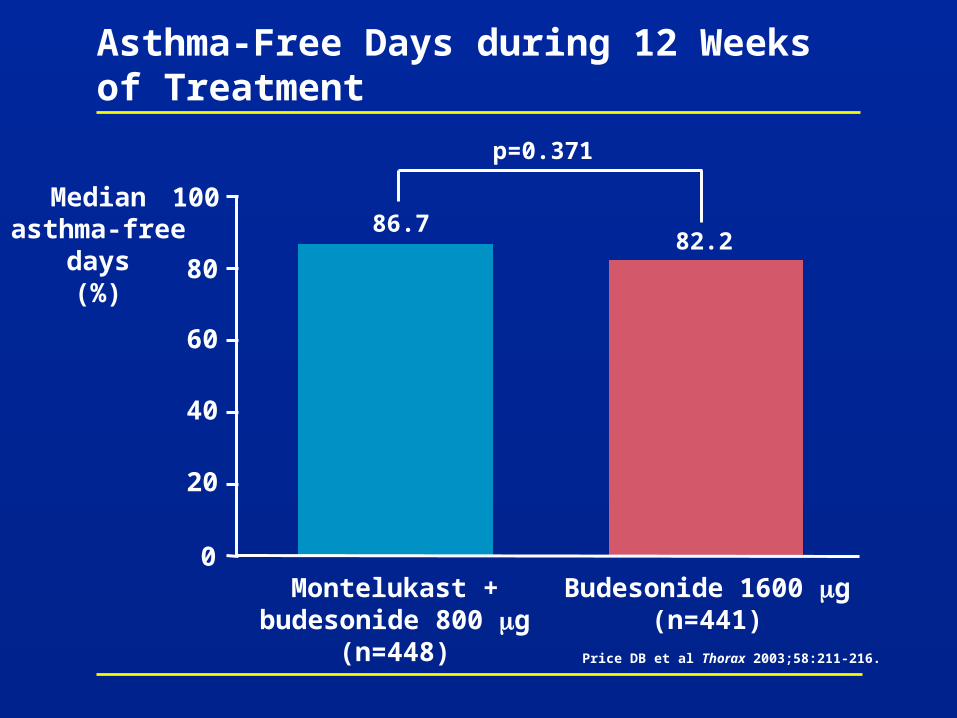
Asthma-Free Days during 12 Weeks of Treatment
Medianasthma-free
days(%)
0
20
40
60
80
100
Montelukast +budesonide 800 g
(n=448)
Budesonide 1600 g(n=441)
86.782.2
p=0.371
Price DB et al Thorax 2003;58:211-216.
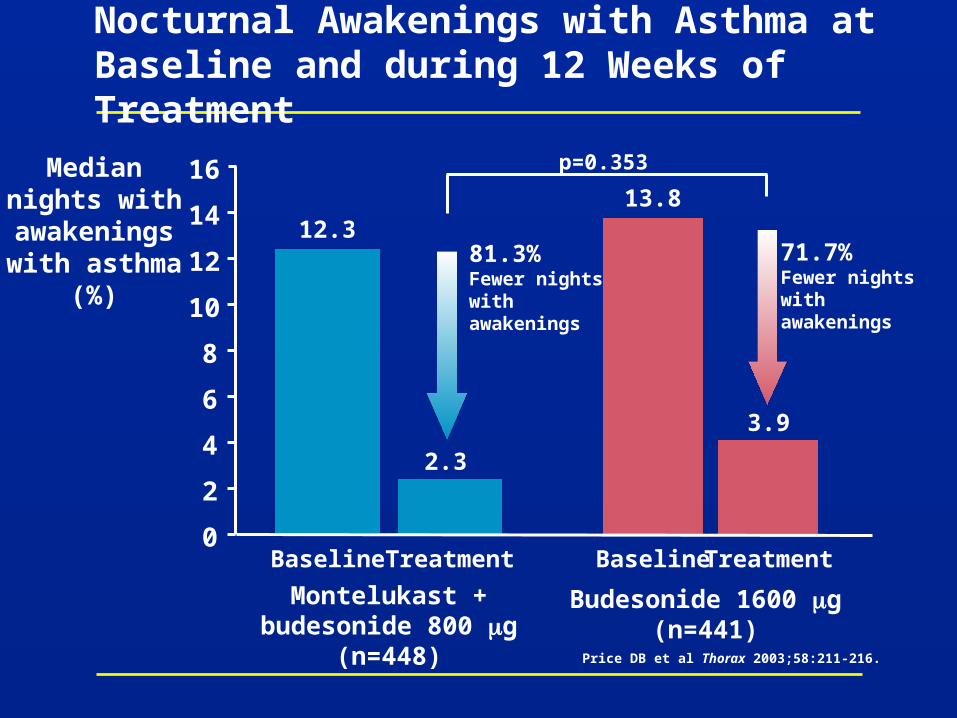
Nocturnal Awakenings with Asthma at Baseline and during 12 Weeks of Treatment
Mediannights withawakeningswith asthma
(%)
Montelukast +budesonide 800 g
(n=448)
Budesonide 1600 g(n=441)
2.3
13.812.3
3.9
Baseline Treatment Baseline Treatment
81.3%Fewer nightswith awakenings
71.7%Fewer nightswith awakenings
p=0.353
0
2
4
6
8
10
12
14
16
Price DB et al Thorax 2003;58:211-216.
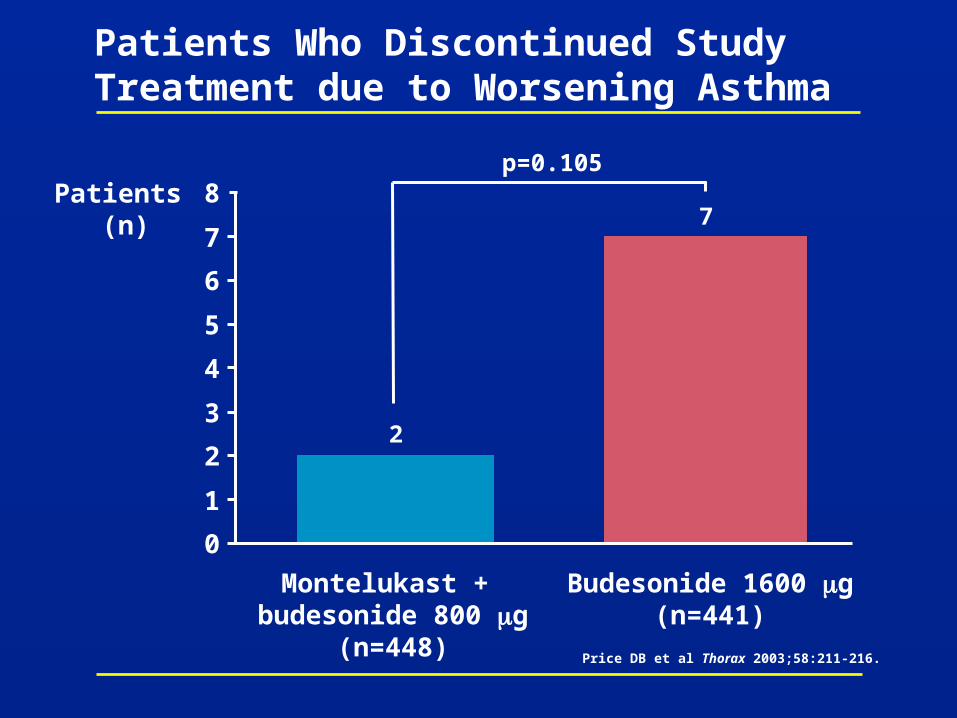
Patients Who Discontinued Study Treatment due to Worsening Asthma
Patients (n)
0
1
2
3
4
5
6
7
8
Montelukast + budesonide 800 g
(n=448)
Budesonide 1600 g(n=441)
2
7
p=0.105
Price DB et al Thorax 2003;58:211-216.
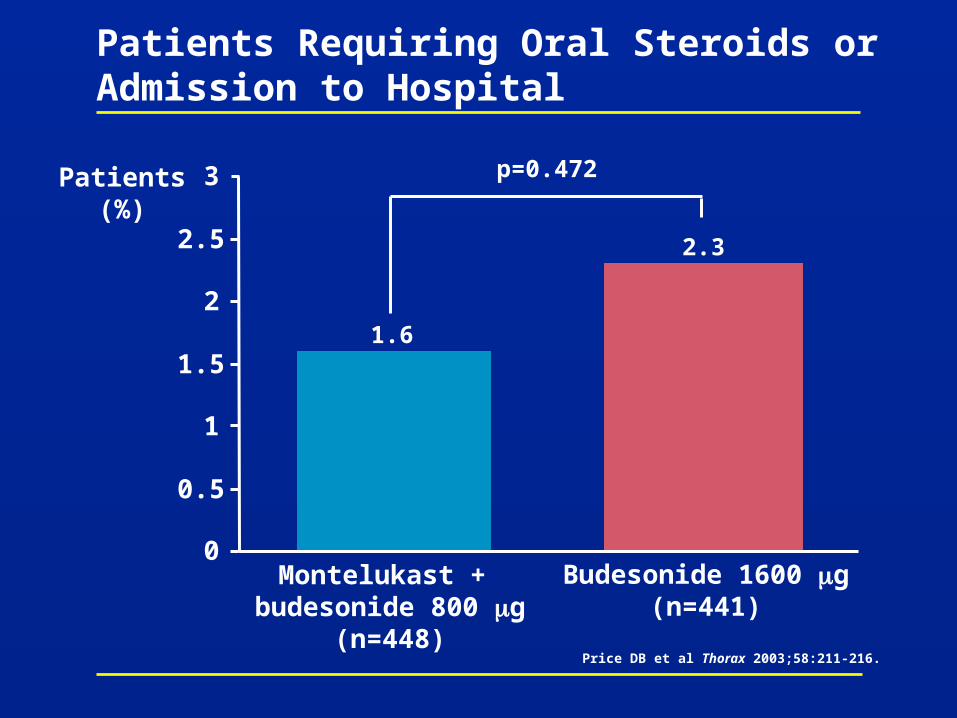
Patients Requiring Oral Steroids or Admission to Hospital
Patients(%)
Montelukast + budesonide 800 g
(n=448)
Budesonide 1600 g(n=441)
1.6
2.3
0
0.5
1
1.5
2
2.5
3 p=0.472
Price DB et al Thorax 2003;58:211-216.
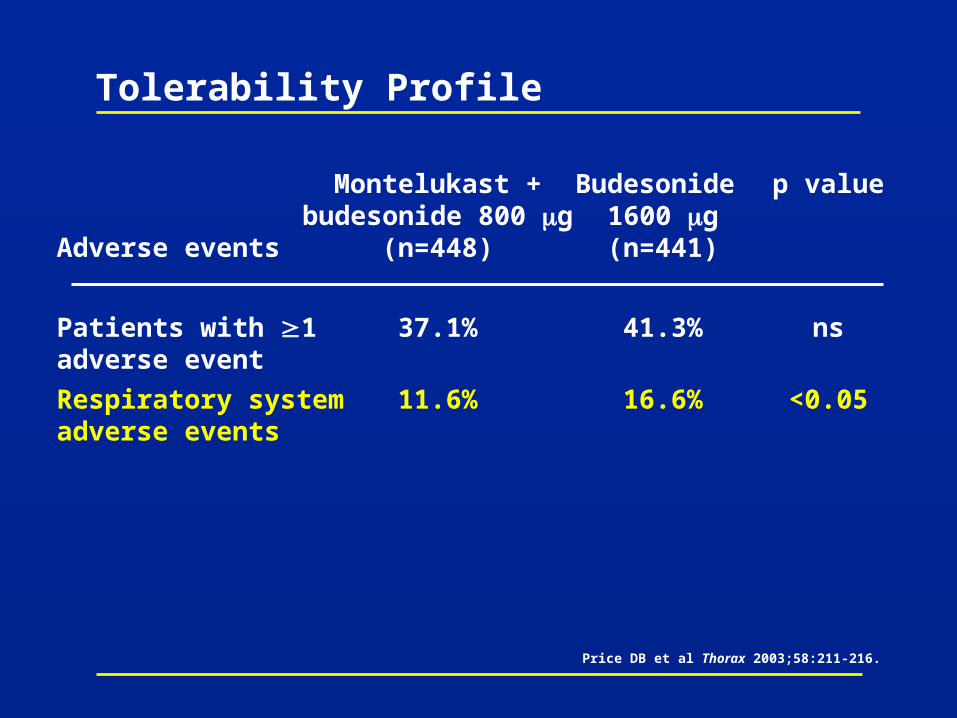
Tolerability Profile
Adverse events
Patients with 1 adverse event
Respiratory system adverse events
Montelukast +budesonide 800 g
(n=448)
37.1%
11.6%
Budesonide 1600 g(n=441)
41.3%
16.6%
p value
ns
<0.05
Price DB et al Thorax 2003;58:211-216.
Summary
• In COMPACT, treatment with montelukast 10 mg with budesonide 800 g
– Was at least as effective as doubling the budesonide dose to 1600 g
– Was more effective than doubling the dose of budesonide in a post hoc substudy of patients with asthma and allergic rhinitis
– Had a faster onset of action than doubling the budesonide dose to 1600 g
• Both treatments were generally well tolerated, with no significant difference in overall incidence of adverse events
• There was a significantly lower incidence of respiratory adverse events with montelukast with budesonide 800 g compared with budesonide 1600 g (p<0.05)
Price DB et al Thorax 2003;58:211-216.
References
See notes page for references
Before prescribing, please consult the manufacturers’ prescribing information.
Merck does not recommend the use of any product in any different manner than as described in the
prescribing information.
Copyright © 2004 Merck & Co., Inc., Whitehouse Station, NJ, USA.
All rights reserved. 3-05 SGA 2002-W-6560-SS Printed in USA
VISIT US ON THE WORLD WIDE WEB AT http://www.merck.com