clinical pharmacokinetics of vancomycin
DESCRIPTION
Clinical Pharmacokinetics of VANCOMYCIN. Mohd Bin Makmor Bakry, PhD, RPh Senior Lecturer in Clinical Pharmacy Faculty of Pharmacy Universiti Kebangsaan Malaysia Kuala Lumpur. INTRODUCTION. Inhibits bacterial cell wall synthesis Time-dependent effect Gram positive bacteria Indications : - PowerPoint PPT PresentationTRANSCRIPT

Clinical Pharmacokinetics of Clinical Pharmacokinetics of VANCOMYCINVANCOMYCIN
Mohd Bin Makmor Bakry, PhD, RPhMohd Bin Makmor Bakry, PhD, RPhSenior Lecturer in Clinical PharmacySenior Lecturer in Clinical Pharmacy
Faculty of PharmacyFaculty of PharmacyUniversiti Kebangsaan MalaysiaUniversiti Kebangsaan Malaysia
Kuala LumpurKuala Lumpur

INTRODUCTIONINTRODUCTION• Inhibits bacterial cell wall synthesisInhibits bacterial cell wall synthesis• Time-dependent effect Time-dependent effect • Gram positive bacteriaGram positive bacteria• Indications :Indications :
• Documented infections:Documented infections:• Methicillin/Cephalosporin-Resistant Staphycoccal infection.Methicillin/Cephalosporin-Resistant Staphycoccal infection.
• Penicillin/Cephalosporin-Resistant Streptococcal infection.Penicillin/Cephalosporin-Resistant Streptococcal infection.
• Staphy./Strep. infection in patient allergic to penicillin.Staphy./Strep. infection in patient allergic to penicillin.
• Staphy. infection in patient with renal disease undergoing Staphy. infection in patient with renal disease undergoing hemodialysis. hemodialysis.
• Penicillin-Resistant Diphtheroid infection.Penicillin-Resistant Diphtheroid infection.
• Severe antibiotic-associated enterocolitis.Severe antibiotic-associated enterocolitis.
• Indications (cont’) :Indications (cont’) :
• Empiric Therapy:Empiric Therapy:• Suspected MRSA nosocomial infection.Suspected MRSA nosocomial infection.
• Meningitis in patient who had neurosurgery.Meningitis in patient who had neurosurgery.
• Neutropenic febrile patient not responding or allergic to Neutropenic febrile patient not responding or allergic to penicillin.penicillin.
• Suspected Staphy. infection in patient with renal disease Suspected Staphy. infection in patient with renal disease undergoing hemodialysis.undergoing hemodialysis.
• Prophylaxis:Prophylaxis:• Endocarditis in patient allergic to penicillin.Endocarditis in patient allergic to penicillin.
• Prosthetic valve placement in patient allergic to Prosthetic valve placement in patient allergic to penicillin.penicillin.

ADVERSE DRUG REACTIONADVERSE DRUG REACTION• Ototoxicity Ototoxicity (tinnitus, fullness in the ear)(tinnitus, fullness in the ear)
• NephrotoxicityNephrotoxicity• An increase in SrCr of 0.5mg/dL or greater, or as 50% An increase in SrCr of 0.5mg/dL or greater, or as 50%
increase from baseline.increase from baseline.
• Occurs at a rate of 5% with Vancomycin alone and increase to Occurs at a rate of 5% with Vancomycin alone and increase to 22% with addition of Aminoglycosides.22% with addition of Aminoglycosides.
• Red-Man SyndromeRed-Man Syndrome (hypotension, upper body (hypotension, upper body maculopapular rash)maculopapular rash)
• Cutaneous reactionCutaneous reaction (urticaria, angioedema, erythema)(urticaria, angioedema, erythema)
• NeutropeniaNeutropenia (within 15 – 30 days of drug initiation)(within 15 – 30 days of drug initiation)
• FeverFever
PHARMACOKINETIC CHARACTERISTICSPHARMACOKINETIC CHARACTERISTICS
• Two- or three-compartment model.Two- or three-compartment model.• BioavailabilityBioavailability
• Per oral < 5%Per oral < 5%• Intravenous 100%Intravenous 100%
• Protein binding 30 – 55%Protein binding 30 – 55%• ExcretionExcretion
• Renal: >90% unchanged in urineRenal: >90% unchanged in urine
KEY PARAMETERSKEY PARAMETERS• CCtargettarget ConventionallyConventionally P = 40 – 50 mg/LP = 40 – 50 mg/L
T = 10 – 15 mg/LT = 10 – 15 mg/L
Continuous infContinuous infusionusion CCaveavessss = 12 – 18 mg/L = 12 – 18 mg/L
• FF <0.05 PO<0.05 PO
• VVdd 0.7 (0.5 – 1.0)0.7 (0.5 – 1.0) (L/kg)(L/kg)
• CLCLVancoVanco 0.65CL0.65CLCr Cr x 0.06 x 0.06 (L/H)(L/H)
• tt½½ 7 7 (H)(H)
• KKee 0.00083(CL0.00083(CLCrCr) + 0.0044) + 0.0044 (H(H-1-1))
*CL*CLCrCr in ml/min in ml/min
INITIATING VANCOMYCININITIATING VANCOMYCIN
• CulturesCultures• Appropriate C&S obtain within 48hrs before Appropriate C&S obtain within 48hrs before
starting therapy.starting therapy.
• Antibiotic therapy modified (if necessary) within Antibiotic therapy modified (if necessary) within 24hrs of the C&S results.24hrs of the C&S results.
• Renal FunctionRenal Function• Estimated CLEstimated CLCrCr within 24hrs of initiating therapy. within 24hrs of initiating therapy.
• Monitoring CLMonitoring CLCrCr every 3 – 5 days during therapy. every 3 – 5 days during therapy.
INITIATING VANCOMYCIN (CONT’)INITIATING VANCOMYCIN (CONT’)
• Dosage Regimen & Monitoring NeedsDosage Regimen & Monitoring Needs• Conventional dosingConventional dosing
• Peak & Trough concentration methodPeak & Trough concentration method
• Continuous infusionContinuous infusion• Trough concentration methodTrough concentration method
INITIATING VANCOMYCIN (CONT’)INITIATING VANCOMYCIN (CONT’)
• Conventional Dosage RegimenConventional Dosage Regimen• Initial per dose is between 10 – 15 mg/kg body wtInitial per dose is between 10 – 15 mg/kg body wt• Dosage interval based on estimated CLDosage interval based on estimated CLCrCr..• Rate of infusion not more than 20 mg/min.Rate of infusion not more than 20 mg/min.• Adjustment based on measured levels.Adjustment based on measured levels.
• Serum Drug ConcentrationSerum Drug Concentration• Levels taken at steady-state.Levels taken at steady-state.• If stable renal function, repeat trough levels once a If stable renal function, repeat trough levels once a
week.week.• Trough levels obtained if with other nephrotoxic drugs.Trough levels obtained if with other nephrotoxic drugs.• Trough and peak levels obtained if:Trough and peak levels obtained if:
• Not responding to therapy.Not responding to therapy.• Altered physiologic parametersAltered physiologic parameters
INITIATING VANCOMYCIN (CONT’)INITIATING VANCOMYCIN (CONT’)
• Continuous Infusion RegimenContinuous Infusion Regimen• Infusion rate is based on estimated CLInfusion rate is based on estimated CLCr Cr and and
targeted Ctargeted Caveavessss (15 mg/L). (15 mg/L).
• Rate of infusion, RRate of infusion, Roo (mg/H) (mg/H)
RRoo = CL = CLvancovancoCCaveavessss
= V= VddKKeeCCaveavessss
• Adjustment based on measured CAdjustment based on measured Caveavessss
• Lake’s MethodLake’s Method• Target serum levels:Target serum levels:
T = 5 – 10 mg/L (30 min before the next T = 5 – 10 mg/L (30 min before the next infusion)infusion)
P = 20 – 30 mg/L (15 min after the end of P = 20 – 30 mg/L (15 min after the end of infusion)infusion)
• Maintenance dose (per dose) = 8 mg/kg (LBW)Maintenance dose (per dose) = 8 mg/kg (LBW)
• To be give at QTo be give at Q H interval:H interval:
CLCLCrCr (ml/min) (ml/min) (H) (H) >90>90 6 6 70 – 8970 – 89 8 8 46 – 69 46 – 69 12 12 30 – 45 30 – 45 18 18 15 – 29 15 – 29 24 24
INITIATING VANCOMYCIN (CONT’)INITIATING VANCOMYCIN (CONT’)
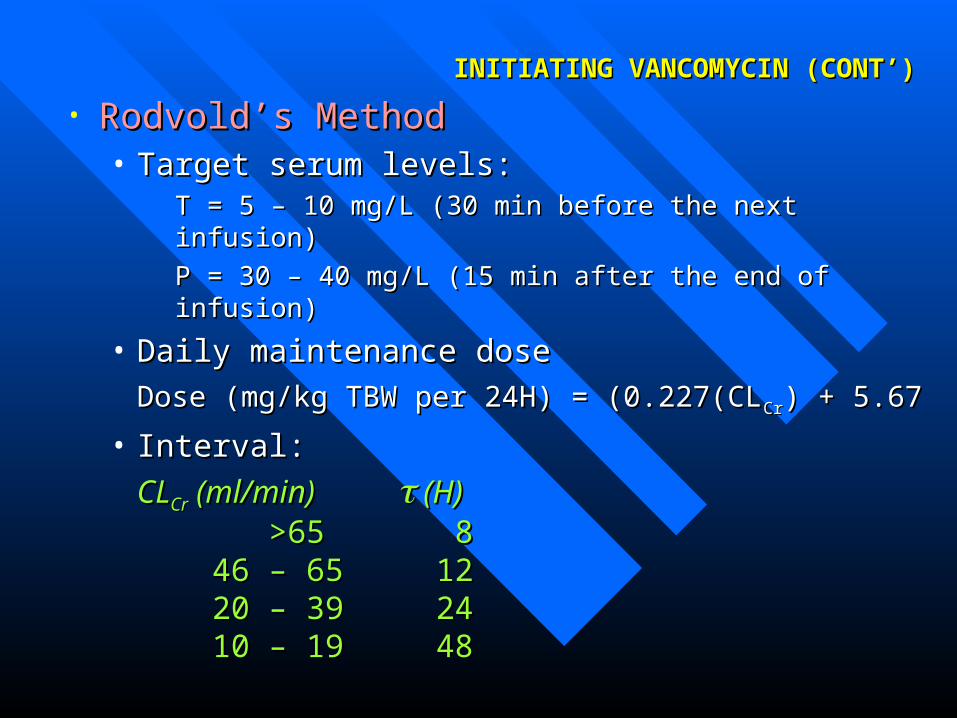
• Rodvold’s MethodRodvold’s Method• Target serum levels:Target serum levels:
T = 5 – 10 mg/L (30 min before the next T = 5 – 10 mg/L (30 min before the next infusion)infusion)
P = 30 – 40 mg/L (15 min after the end of P = 30 – 40 mg/L (15 min after the end of infusion)infusion)
• Daily maintenance dose Daily maintenance dose
Dose (mg/kg TBW per 24H) = (0.227(CLDose (mg/kg TBW per 24H) = (0.227(CLCrCr) + 5.67) + 5.67
• Interval:Interval:
CLCLCrCr (ml/min) (ml/min) (H) (H) >65>65 8 8 46 – 65 46 – 65 12 12 20 – 39 20 – 39 24 24 10 – 19 10 – 19 48 48
INITIATING VANCOMYCIN (CONT’)INITIATING VANCOMYCIN (CONT’)
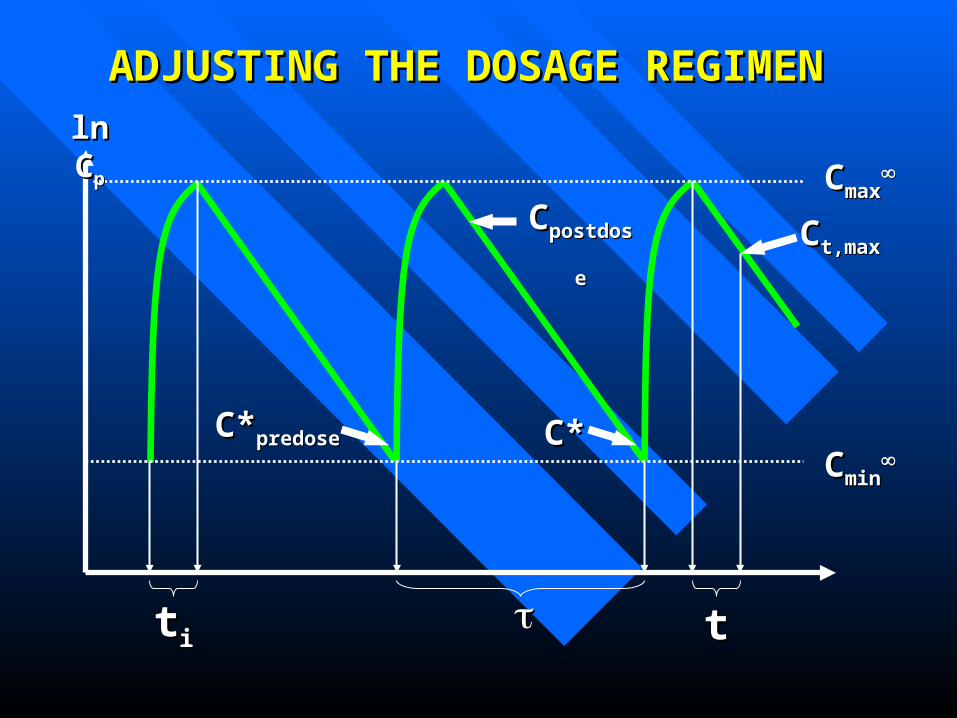
ADJUSTING THE DOSAGE REGIMEN ADJUSTING THE DOSAGE REGIMEN
ln Cln Cpp
ttii tt
CCminmin
CCmaxmax
C*C*predosepredose C*C*
CCpostdosepostdose CCt,maxt,max
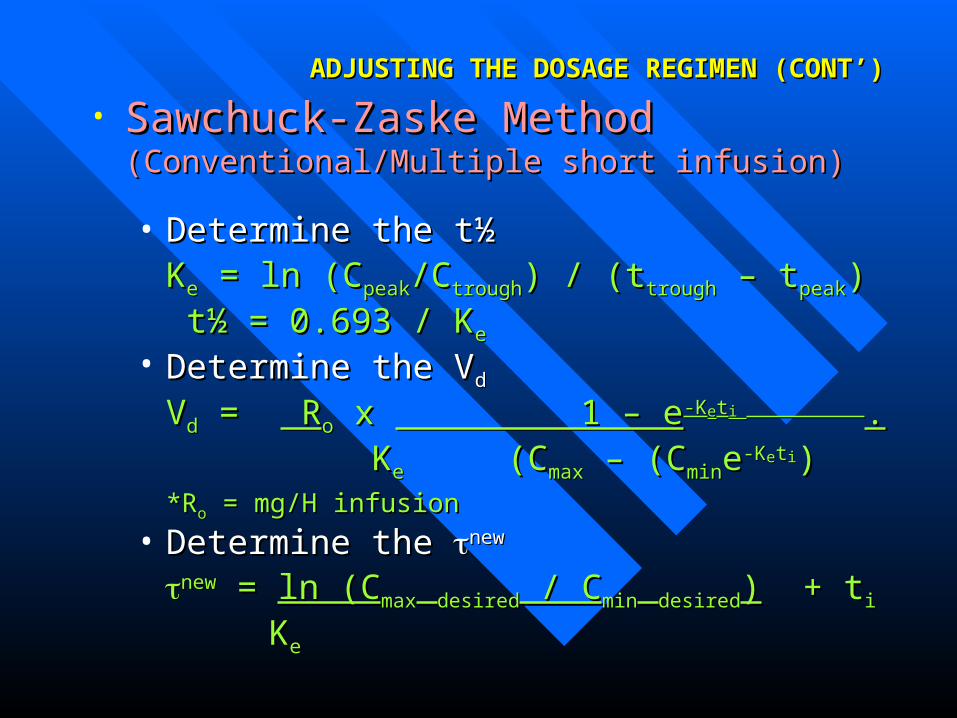
• Sawchuck-Zaske Method Sawchuck-Zaske Method (Conventional/Multiple short infusion)(Conventional/Multiple short infusion)
• Determine the tDetermine the t½½KKee = ln (C = ln (Cpeakpeak/C/Ctroughtrough) / (t) / (ttroughtrough – t – tpeakpeak))
tt½ = 0.693 / K½ = 0.693 / Kee
• Determine the VDetermine the Vdd
VVdd = = R Roo x x 1 – e 1 – e-K-Keetti i ..
KKee (C (Cmaxmax – (C – (Cminminee-K-Keettii))*R*Roo = mg/H infusion = mg/H infusion
• Determine the Determine the newnew
newnew = = ln (Cln (Cmaxmax desireddesired / C / Cminmin desireddesired)) + t + tii
KKee
ADJUSTING THE DOSAGE REGIMEN (CONT’) ADJUSTING THE DOSAGE REGIMEN (CONT’)
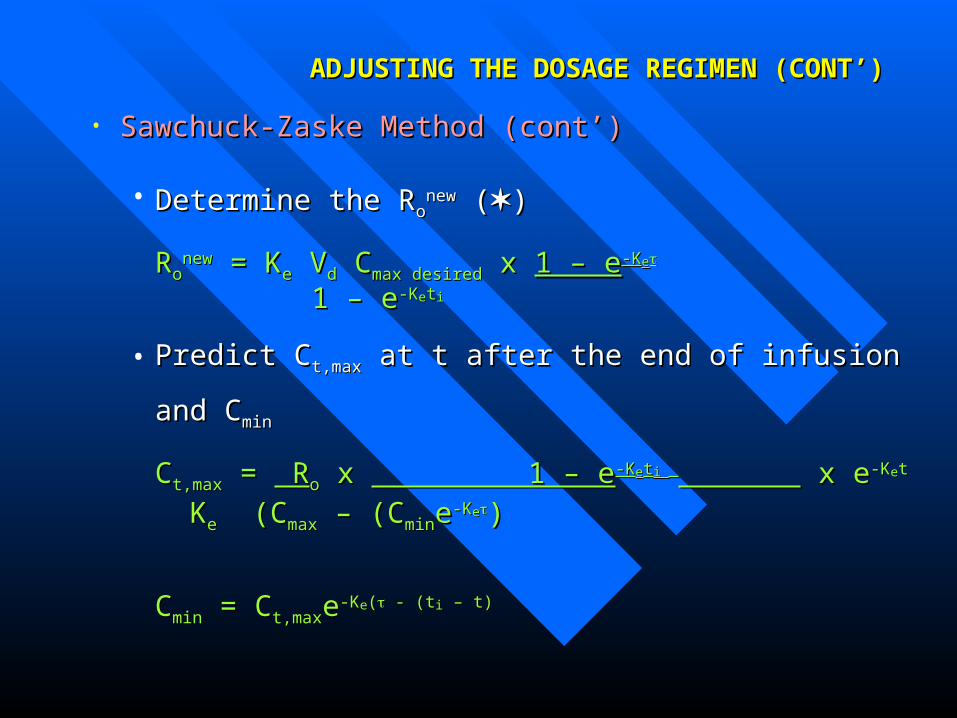
• Sawchuck-Zaske Method (cont’)Sawchuck-Zaske Method (cont’)
• Determine the RDetermine the Roonewnew ( ())
RRoonewnew = K = Kee V Vdd C Cmax desiredmax desired x x 1 – e1 – e-K-Kee
1 – e1 – e-K-Keettii
• Predict CPredict Ct,maxt,max at t after the end of infusion and C at t after the end of infusion and Cminmin
CCt,maxt,max = = R Roo x x 1 – e 1 – e-K-Keetti i x e x e-K-Keett
KKee (C (Cmaxmax – (C – (Cminminee-K-Kee))
CCminmin = C = Ct,maxt,maxee-K-Kee(( - (t - (tii – t) – t)
ADJUSTING THE DOSAGE REGIMEN (CONT’) ADJUSTING THE DOSAGE REGIMEN (CONT’)
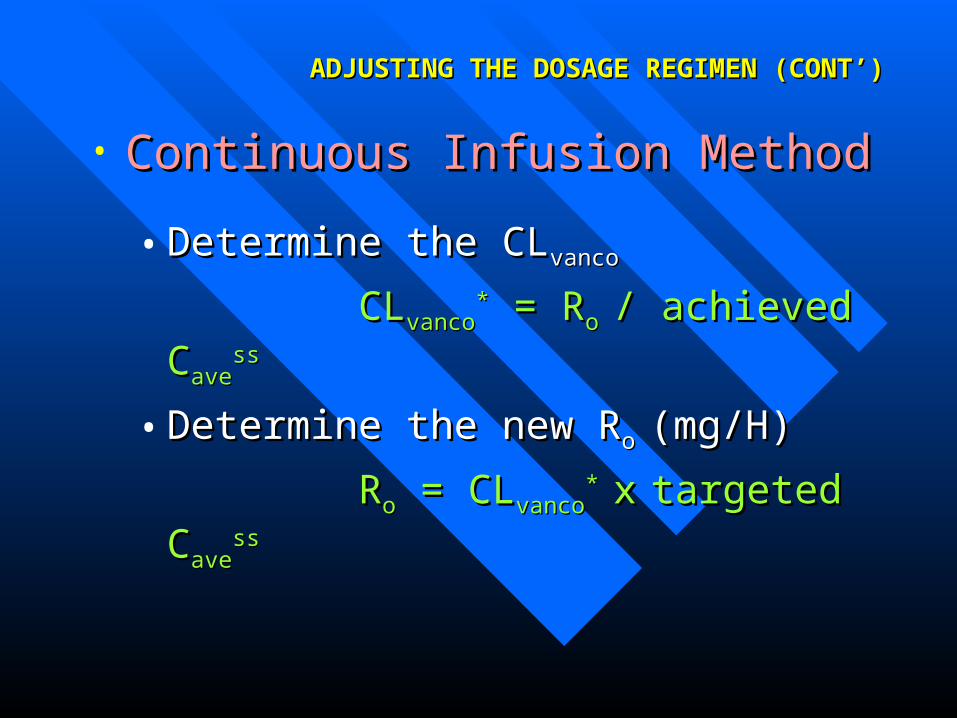
• Continuous Infusion Method Continuous Infusion Method
• Determine the CLDetermine the CLvancovanco
CLCLvancovanco** = R = Ro o / achieved C/ achieved Caveave
ssss
• Determine the new RDetermine the new Ro o (mg/H)(mg/H)
RRoo = CL = CLvancovanco* * xx targeted Ctargeted Caveave
ssss
ADJUSTING THE DOSAGE REGIMEN (CONT’) ADJUSTING THE DOSAGE REGIMEN (CONT’)
EXAMPLE OF CASESEXAMPLE OF CASESCASE 1CASE 1• Mr. AD, 62 years old patient was diagnosed to have MRSA Mr. AD, 62 years old patient was diagnosed to have MRSA
and allergic to penicillin, Body weight is 98 kg and height is and allergic to penicillin, Body weight is 98 kg and height is 165 cm. 165 cm. Lab results: SrLab results: SrCrCr 95 95 mol/L, Urea 8.5mol/L, Urea 8.5
Suggest the best Vancomycin dosage regimen to achieve Suggest the best Vancomycin dosage regimen to achieve
CCpeak peak = 40.0 mg/L and C= 40.0 mg/L and Ctroughtrough = 10.0 mg/L. = 10.0 mg/L.
Estimate the dose to be given through continuous infusion, CEstimate the dose to be given through continuous infusion, Cpp = 15 mg/L = 15 mg/L
CASE 2CASE 2• Mrs. PS, 55 years old patient was diagnosed Mrs. PS, 55 years old patient was diagnosed
to have MRSA sepsis. Body weight is 85 kg to have MRSA sepsis. Body weight is 85 kg and height is 170 cm. and height is 170 cm. Given Short Inf. for 0.5H Vancomycin 500 mg Q8HGiven Short Inf. for 0.5H Vancomycin 500 mg Q8H
Lab results: C&S Lab results: C&S S. aureusS. aureus., SrCr 150 ., SrCr 150 mol/L, Urea mol/L, Urea 9.2, C9.2, Cpeakpeak = 40 mg/L, C = 40 mg/L, Ctroughtrough = 24.0 mg/L = 24.0 mg/L
Adjust the Vancomycin dose regimen to achieve Adjust the Vancomycin dose regimen to achieve
CCpeak peak = 40.0 mg/L and C= 40.0 mg/L and Ctroughtrough = 10.0 mg/L. = 10.0 mg/L.
CASE 3CASE 3• Mrs. SP, 40 years old patient was diagnosed to have Mrs. SP, 40 years old patient was diagnosed to have
endocarditis and allergic to penicillin. Body weight is endocarditis and allergic to penicillin. Body weight is 45 kg and height 165 cm. 45 kg and height 165 cm. Given Short Inf. for 1H Vancomycin 750 mg Q12HGiven Short Inf. for 1H Vancomycin 750 mg Q12H
Lab results: C&S Lab results: C&S S. aureusS. aureus., SrCr 120 ., SrCr 120 mol/L, Urea 9.0, Cmol/L, Urea 9.0, Cpeakpeak = 30 mg/L, C= 30 mg/L, Ctroughtrough = 22.0 mg/L = 22.0 mg/L
The doctor would like to change the method of administration The doctor would like to change the method of administration to continuous infusion for 24 hours and targeted Cto continuous infusion for 24 hours and targeted Cpp = 15mg/L. = 15mg/L.
Suggest new dosage regimen to reach this later target and Suggest new dosage regimen to reach this later target and when to start this new regimen?when to start this new regimen?

CASE 4CASE 4• Mr. IZ, 50 years old patient was diagnosed with CoNS Mr. IZ, 50 years old patient was diagnosed with CoNS
and allergic to penicillin. Body weight is 60 kg and and allergic to penicillin. Body weight is 60 kg and height 150 cm. height 150 cm. Given continuous infusion of Vancomycin 80 mg/HGiven continuous infusion of Vancomycin 80 mg/H
Lab results at day 3: SrCr 200 Lab results at day 3: SrCr 200 mol/L (120 mol/L (120 mol/L at D1), mol/L at D1), CCaveave = 26.0 mg/L = 26.0 mg/L
The doctor would like to change the method of administration The doctor would like to change the method of administration to conventional method and targeted Cto conventional method and targeted Ctroughtrough = 10 mg/L. = 10 mg/L.
Suggest new dosage regimen to reach this later target and Suggest new dosage regimen to reach this later target and when to start this new regimen?when to start this new regimen?

THANK YOUTHANK YOU