clinical presentation and risk factors of age related
TRANSCRIPT

i
CLINICAL PRESENTATION AND RISK FACTORS OF AGE
RELATED MACULAR DEGENERATION IN UNIVERSITY OF BENIN
TEACHING HOSPITAL, EDO STATE, NIGERIA.
SUBMITTED BY
LORETTA OMONZUSI EKECHUKWU
M.B.B.S. 2009 (BENIN)
TO
THE NATIONAL POSTGRADUATE MEDICAL COLLEGE OF
NIGERIA IN PART FULFILMENT OF THE REQUIREMENTS FOR
THE AWARD OF THE FINAL FELLOWSHIP OF THE MEDICAL
COLLEGE IN OPHTHALMOLOGY (FMCOPH).
MAY, 2017.

ii
DECLARATION
I hereby declare that the work contained in this dissertation is original unless otherwise
acknowledged. It has not been submitted to any other college for the award of a fellowship or
degree and has not been submitted elsewhere for publication.
……..………………………..
DR. L.O. EKECHUKWU

iii
ATTESTATION
This is to certify that the study reported in this dissertation was performed by Dr. L.O.
EKECHUKWU and was supervised by:
…………………………
PROF. A.E. OMOTI (FMCOph, FWACS)
Consultant Ophthalmologist,
Department of Ophthalmology,
University of Benin Teaching Hospital,
Benin City.
…………………………
DR. O.M. UHUMWANGHO (FMCOph, FWACS)
Consultant Ophthalmologist,
Department of Ophthalmology,
University of Benin Teaching Hospital,
Benin City.

iv
CERTIFICATION
I certify that this dissertation was written by Dr. Loretta Omonzusi EKECHUKWU of the
Department of Ophthalmology, University of Benin Teaching Hospital, Benin City, Edo State
under my headship.
………………………………….
DR. O.M. UHUMWANGHO (FMCOph, FWACS)
Head, Department of Ophthalmology
University of Benin Teaching Hospital,
Benin City, Edo State.

v
DEDICATION
This work is dedicated to The Lord God Almighty, for His unflinching grace and mercy and
seeing me through residency programme despite all the hurdles faced; to my beloved
husband, Engr. Chinedum John Chimeremeze Ekechukwu for his love, undying support,
encouragement and understanding; my parents (Dr. and Mrs L.C. Ekechukwu, Mr. and Dr
M.O. Obaedo,) and siblings (Esther, Irene, Cassiel, Victoria, Michelle, Chidinma, Joshua-
Daniel) for being there for me at all times.

vi
ACKNOWLEDGEMENT
My heartfelt gratitude to my supervisors, Prof. A.E. Omoti and Dr. O.M. Uhumwangho for
accepting to supervise this work and for their constant care and availability all the way
despite their busy schedules.
Immense and profound appreciation to my teachers at the department of Ophthalmology,
University of Benin Teaching Hospital, Prof. J. Ayanru, Prof. O.T. Edema, Prof. MJM
Waziri-Erameh, Prof. A.I. Osahon, Prof. O.A. Dawodu, Prof. C.U. Ukponmwan, Dr. V.W.
Okeigbemen, Dr. R.O. Momoh, Dr. V.B. Osaguona, Dr. O.J. Olubor, Dr. J. Ese-Onakewhor,
Dr. D.H Kayoma for their appreciated inputs in this research.
Sincere words of appreciation to my colleagues turned brothers and sisters – Drs Akpata,
Eboh, Azeta, Umolo, Obasuyi, Okolo, Oronsaye, Ebalu, Salimonu, Osho, Iyiriaro, Edet,
Ugboka, Okoro for their support.
Special thanks to the Management of University of Benin Teaching Hospital headed by Prof.
M.O. Ibadin for creating an enabling environment to conduct this research.

vii
TABLE OF CONTENTS
Title i
Declaration ii
Attestation iii
Certification iv
Dedication v
Acknowledgement vi
Table of contents vii
List of Tables viii
List of Figures ix
List of Abbreviations x
Summary xi
Introduction 1
Aim and Objectives 3
Literature review 4
Materials and Method 21
Results 29
Discussion 45
Limitation(s) 52
Conclusion 52
Recommendations 53
References 54
Appendices 66

viii
LIST OF TABLES
TABLE 1 : Sociodemographic characteristics of cases and controls 29
TABLE 2 : Chronic conditions and lifestyle behaviours in cases with ARMD and controls 31
TABLE 3 : Major sources of animal protein by cases and controls 32
TABLE 4 : Ocular history of cases and controls 33
TABLE 5 : Refractive state among the cases and controls 34
TABLE 6 : Anthropometric measurements in cases with ARMD and controls 35
TABLE 7 : Visual acuity of both eyes among cases with ARMD and controls 37
TABLE 8 : Ocular examination of both eyes across study groups of cases and
Controls 38
TABLE 9 : Biochemical parameters of cases with ARMD and controls 42
TABLE 10 : Risk factors for ARMD among the cases 43

ix
LIST OF FIGURES
FIGURE 1 : Body mass index of controls and cases with ARMD 36
FIGURE 2: Pattern of ARMD seen among cases 39
FIGURE 3 : Drusen patterns in the right and left eyes of respondents with ARMD 40
FIGURE 4 : Pattern of retinal pigmentation among the respondents with ARMD 41

x
LIST OF ABBREVIATIONS
ARMD: Age-Related Macular Degeneration
AREDs: Age-Related Eye Diseases
GA: Geographic Atrophy
CNV: Choroidal Neovascularization
UBTH: University of Benin Teaching Hospital
ARM: Age-Related Maculopathy
RPE: Retinal Pigment Epithelium
UK: United Kingdom
USA: United States of America
ARMS2: Age-Related Maculopathy Susceptibility 2
SPSS: Statistical Package for Social Sciences
SD: Standard Deviation
OCT: Optical Coherence Tomography

xi
SUMMARY
Aim: To determine the clinical characteristics and risk factors of Age-related Macular
Degeneration at the University of Benin Teaching Hospital (UBTH), Benin City, Nigeria.
Study Design: A descriptive cross-sectional analytical study was carried out. A structured
interviewer-administered protocol was used.
Method: In this Hospital-based study, all consenting consecutive new patients aged 50 years
and above presenting at the out-patient clinic of the UBTH within the study period were
enrolled. A structured interviewer-administered protocol was used to obtain relevant
demographic and clinical information which included biodata, medical and social history,
ocular history, anthropometric measurements and ocular examination. Standard photographs
from the International ARM Epidemiological Study Group were used to grade ARMD-
related fundus changes. Registered participants had their fasting blood glucose and serum
lipid profiles checked. Data was cleaned and analysed using the Statistical Product for
Scientific Solutions version 20 software (SPSS Inc, Chicago IL., U.S.A.).
Results: A total of 240 respondents (120 cases made up of 40% males, 60% females and 120
age and sex matched controls made up of 40.8% males and 59.2% females),were enrolled
from December 2015 – June 2016. The higher proportion of respondents in both study groups
were in the age group 60 – 69 years; cases 48 (40.0%) and controls 49 (40.8%). There was a
female preponderance in cases of ARMD seen (60%). A year increase in the age of
respondents led to 1.13 increase in the odds of developing ARMD. Cigarette smoking led to a
higher risk 0.76 (95% CI: 0.46 – 4.54) of developing AMD than non-smokers. Myopia was
found to be significantly more common among cases with ARMD than in the controls. Early
ARMD was the predominant pattern seen, with hard drusen and retinal hyperpigmentation
being more predominant. Two cases of late ARMD were seen with features suggestive of
neovascular ARMD.

xii
Conclusion: There was a greater preponderance of ARMD among females. The presence of
lens opacities and increasing age were significantly associated with increased risk of Age-
related Macular Degeneration. The risk of having ARMD was shown to be reduced in
subjects with increasing level of education and the use of tinted or photochromic lenses. The
presenting pattern is predominantly the early type. The clinical features are largely
characterised by reduction in visual acuity, especially for the late type where it is more
marked, the presence of retinal hyperpigmentation and hard drusen.

1
CHAPTER 1
INTRODUCTION
Age-related macular degeneration (ARMD) is one of the age-related eye diseases (AREDs) in
relation to low vision and blindness of great concern globally. It is a progressive neuroretinal
degenerative disease in which patients advance from early and intermediate stages
characterised by changes in pigment and drusen deposits to more advanced pathology, such
as geographic atrophy (GA) and choroidal neovascularization (CNV).1 It ranks third among
the global causes of visual impairment with a blindness prevalence of 8.7%.2 It commonly
occurs in the sixth decade of life and is generally bilateral.3 ARMD increases with age in men
and women, but no significant sex differences in rates has been found.4
It is the leading cause of visual loss and blindness in Western countries.3,5-8 In developing
countries, there is paucity of data on the prevalence of this disease, possibly due to the non-
availability of equipment needed to make an accurate diagnosis of this important cause of low
vision and blindness in the aging population.9
Generally, two pathological forms of the disease have been identified, namely neovascular
(wet ARMD) and atrophic. However, a third form has been documented, which is the
indeterminate group.2 The exact pathogenic mechanisms of ARMD are not completely
understood. Precise clinical characterization of early lesions of ARMD and their progression
over time can provide insight into the pathophysiology to guide research on treatments.10-13
Treatment of ARMD ranges from careful observation, nutritional supplements, to laser
therapy, photodynamic therapy, intravitreal injection of antivascular endothelial growth
factor (anti VEGF) and surgical therapy. Current options for prevention are limited, but new
treatments are being developed to preserve or restore vision in some patients with the wet
form. Since life expectancy is increasing, we expect to see more aged people.14 This will
2
result in an increase in patients with Age-related Eye Diseases (AREDs). There is a paucity
of studies on ARMD in Nigeria. More studies are needed to actually characterise the disease
in Nigerians, hence this study.
JUSTIFICATION FOR THE STUDY
ARMD is increasingly being recognised as an important cause of visual impairment and
blindness globally.2 There is however a dearth of information on the prevalence and
characteristics of ARMD in our environment. Despite the fact that the prevalence of the
disease as a cause of blindness appears low, it is a cause of treatable blindness with severe
sequelae and has been noted to be an important cause of blindness and low vision in
Nigerians.15-18 The prevalence of ARMD and the contribution to blindness has been noted to
be significantly higher in Caucasians than in blacks.4 It is therefore possible that the clinical
characteristics of ARMD, manifestations and predominant type may show racial and possibly
environmental differences. The possibility of having a higher yield of individuals with Age-
related Macular degeneration in the hospitals than in the community prompted this study to
be hospital-based. This study will show if the clinical features of ARMD differ in Benin City
where blacks constitute the population, when compared to Caucasians. It is also possible that
the risk factors in western countries may differ from that in the Nigerian elderly patients.
These may affect the prevalence and characteristics of ARMD in sub-Saharan Africa when
compared to Western countries. This study will also identify risk factors for cases with
ARMD in our environment. Knowing this will help make recommendations on ways to
reduce the risk of developing, or progression of ARMD in our environment. Treatment is
available only for the wet form. The available treatments are indicated only if the condition is
detected early. All these necessitate further studies on ARMD in Nigerians.

3
CHAPTER 2
AIM AND OBJECTIVES
AIM
To determine the clinical characteristics and risk factors of Age-related Macular
Degeneration at the University of Benin Teaching Hospital (UBTH), Benin City, Nigeria,
with a view to proffering appropriate recommendations to decrease the rate of blindness from
ARMD in the population.
OBJECTIVES
1. To determine the pattern and clinical features of Age-related Macular Degeneration in
UBTH.
2. To identify the risk factors for Age-related Macular Degeneration in UBTH.
3. To make recommendations on early detection and possible measures to reduce the
risk of developing Age-related Macular Degeneration in Nigerians.

4
CHAPTER 3
REVIEW OF LITERATURE
The International Age-related Maculopathy Epidemiological Study Group19 defines Age-
related Maculopathy (ARM) as a degenerative disorder of the macular area, most often
clinically apparent after 50years of age, characterised by discrete whitish-yellowish spots
identified as drusen, increased pigment or hyperpigmentation associated with drusen, sharply
demarcated areas of depigmentation or hypopigmentation of the retinal pigment epithelium
(RPE) and associated drusen. These result in progressive accumulation of debris under the
retina. Visual acuity is not used to define the presence of ARM.
Early ARM is defined as the presence of drusen and RPE pigmentary abnormalities. Late
ARM is similar to age-related macular degeneration (ARMD) and includes dry ARMD
(geographic atrophy of the RPE in the absence of neovascular AMD) or neovascular AMD
(RPE detachment, haemorrhages and / or scars, choroidal neovascular membrane).19,20 It is
the leading cause of blindness among people aged 55years and older in the United States of
America (U.S.A.) and other western countries and was estimated to be responsible for 5% of
global blindness in 2010.21,22 Neovascular ARMD results in severe visual impairment if left
untreated with an average loss of about four lines of visual acuity within two years of disease
onset.23 Visual impairment resulting from advanced ARMD significantly reduces quality of
life and consumes more than fifty percent (50%) of eye care cost in the Medicare budget.24
EPIDEMIOLOGY
Age-related macular degeneration ranks third among the global causes of visual impairment
with a blindness prevalence of 8.7%.2 Many population and hospital-based studies of age-
related macular degeneration have been reported around the world.18, 25 – 31, 35, 36 - 46
5
In Australia, the commonest cause of blindness (presenting visual acuity of less than 6/60,
based on the guidelines for the study) is ARMD (48%), and the predicted numbers of
Australians who will have low vision or blindness from ARMD will almost double over years
2000 – 2024.25 Macular degeneration affects 1 in 7 Australians over the age of 50, with the
incidence increasing with age.12 In another Australian study (The Blue Mountains Eye Study)
done to examine the prevalence of age related maculopathy (drusen and retinal pigmentary
abnormalities) and end-stage age-related macular degeneration lesions (neovascular
maculopathy or geographic atrophy) in a defined older Australian urban population, there
was a marked age-related increase in all typical lesions of age-related maculopathy.12 End-
stage age-related macular degeneration was present in 1.9% of the population, rising from 0%
among people younger than 55 years of age to 18.5% among those 85 years of age or older.
In a clinical study done in England and Wales in the United Kingdom (UK), ARMD
accounted for 42% of blindness in individuals aged 65 – 75 years.26 This figure increased
dramatically with age such that ARMD accounted for 75% of blindness in those aged 85
years and above.26 Half of 30,000 people registered blind or partially sighted every year have
macular degeneration.27
In the United States of America alone, where the population is approximately 312 million, the
Eye Diseases Prevalence Research Group have estimated that more than 7.3 million people
are affected by ARMD.28 In another report, they further estimated that the number of
advanced ARMD cases will reach almost 3million by 2020.29
In Asia, population-based studies have been done to estimate the prevalence of ARMD and
comparisons made with the white population. A meta-analysis carried out to determine the
prevalence of ARMD in Asians showed that pooled estimates of early and late ARMD in
Asian populations aged 40 – 79 years were 6.8% (95% CI, 4.6% - 8.9%) and 0.56% (95% CI,

6
0.30% - 0.81%) respectively.30 Another population-based study among one thousand four
hundred and eighty six (1,486) residents of Hisayama town, Japan, to determine the
prevalence of ARM in a representative older Japanese population showed the prevalence rate
of drusen in both gender was 9.6%.31 The prevalence of late ARMD was comparable to that
in Western populations.32-34 A population-based cross-sectional study by Cheung et al35 to
describe the prevalence and risk factors for ARMD in a multi-ethnic group among persons of
Chinese, Indian and Malay ethnicities concluded that the prevalence of ARMD in the three
ethnic groups studied was comparable with that observed in whites.
Very little is known about ARMD in African populations. There is a paucity of population-
based studies and the majority of the few available are hospital based. In a population-based
study in Kenya, East Africa, 100 clusters of 50 people aged 50 years or older were selected
by probability-proportional-to-size sampling between 26 January 2007 and 11 November
2008. Age-related macular degeneration was found to be a significant contributor to visual
impairment and blindness in the elderly. Early and late ARMD prevalence were 11.2% and
1.2% respectively, among participants graded on images.36
Studies from Nigeria have mainly been hospital-based. Abdulraheem et al37 found that age-
related macular degeneration was the fourth commonest cause of bilateral blindness with a
prevalence of 8.1% in a five year review of elderly patients seen in the eye clinic of the
University of Ilorin Teaching Hospital, in the North Central region of Nigeria. In Western
Nigeria, Abiose38 reported that age-related macular degeneration accounted for 25.9% of
retinal diseases in Lagos (1.2% of all patients seen) in a study of five hundred and ninety five
(595) new patients in the eye clinic of Lagos University Teaching Hospital thirty years ago
(1976). Fafowora and Osuntokun39 documented a prevalence of 3.4% for age-related macular
degeneration and found that age-related macular degeneration represented a sizeable amount
of retinal diseases even in rural communities. Onakpoya et al40 found 13% of patients with

7
vitreo-retinal disease in a five year review of the new patients seen in the eye clinic of
Obafemi Awolowo University Teaching Hospital, Ile-Ife. ARMD was the most frequent
macular disease with a prevalence of 13.7%. Oluleye et al41 found that 35.6% of the patients
had macular disease and ARMD accounted for 17.2% of all retinal diseases in a five year
review of vitreo-retinal patients seen in the eye clinic of the University College Hospital,
Ibadan. In the East, Nwosu42 in a retrospective study conducted between 1997 and 2004 on
seven thousand nine hundred and sixty six (7,966) new patients aged 50 years and above at
the Guinness Eye Centre Onitsha, found that two hundred and fifty six patients had ARMD,
an incidence of 3.2%. ARMD was the main cause of blindness in 7.4% of the patients. Eze et
al43 found that vitreo-retinal disease accounted for 3.9% of which ARMD (third in the order)
accounted for 10.7% in a four year review of new patients seen at the eye clinic of the
University Teaching Hospital, Enugu. Macular degeneration accounted for 2.9% of blindness
in the rainforest (south-west) region of Nigeria, as stated in the Nigerian National Blindness
and Visual Impairment Survey.44
In the Mid-Western/South-South region, Ayanru45 noted that macular degeneration was
common among Nigerians with a prevalence of 2.2% in a study done in Benin City, thirty
years ago (1976). In a review of ARMD in Benin City, Omoti46 reported an incidence of 5%
and for those over 50 years of age, 16.16%. Age-related macular degeneration was found to
be the third leading cause of binocular blindness after cataract and glaucoma.46 In a study to
determine the pattern of retinal diseases in a tertiary hospital in Southern Nigeria by
Uhumwangho et al18, ARMD accounted for 15.0% of retinal cases seen and was noted to be
the leading cause of bilateral blindness in the elderly (38.1%).

8
PATHOGENESIS OF ARMD
The exact pathogenic mechanisms of ARMD are not completely understood. However, it has
been postulated that buildup of free oxygen radicals causes oxidative stress, resulting in
retinal pigment epithelium (RPE) injury. This elicits an inflammatory response which
involves the complement system and specific polymorphisms of complement genes,
including Complement Factor H (CFH). An abnormal extracellular matrix is formed and this
impairs with the normal diffusion of nutrients to the RPE and retina. A constellation of these
features lead to retinal atrophy and new vessel growth (in advanced cases).3
CLASSIFICATION OF ARMD
This is based on the International ARM Epidemiological Study Group.19
ARMD is classified as:
Early ARM
Soft drusen> 63µm
Areas of increased pigment or hyperpigmentation (in the outer retina or choroid)
associated with drusen
Areas of depigmentation of the RPE, most often more sharply demarcated than
drusen, without any visibility of choroidal vessels, associated with drusen.
Late ARM = Age-related Macular Degeneration (AMD)
Geographic atrophy (“dry” AMD)
- Any sharply delineated roughly round or oval area of hypopigmentation or
depigmentation or apparent absence of the RPE in which choroidal vessels are more
visible than in surrounding areas that must be at least 175µm in diameter.

9
Neovascular AMD (“disciform”, “exudative”, or “wet” AMD)
- RPE detachment(s) which may be associated with neurosensory retinal detachment,
associated with other forms of ARM.
- Sub-retinal or sub-RPE neovascular membrane(s)
- Epiretinal (with exclusion of idiopathic puckers), intraretinal, subretinal or sub-
pigment epithelial scar / glial tissue or fibrin-like deposits.
- Subretinal haemorrhages that may be nearly black, bright red or whitish-yellow and
that are not related to other retinal vascular disease.
- Hard exudates (lipids) within the macular area related to any of the above and not
related to other retinal vascular disease.
DEFINITION OF TERMS
DRUSEN
Defined as tiny yellow or white accumulations of extracellular material that build up in
Bruch’s membrane. Drusen could be soft or hard.
Soft drusen: > 63 micrometres (µm) in diameter.
Hard drusen : Well defined and <63 micrometres (µm) in diameter.
RETINAL PIGMENTARY ABNORMALITIES
a) Retinal hypopigmentation: Defined as a discrete area of retinal pigment degeneration
without visible choroidal vessels.
b) Retinal hyperpigmentation: Defined as presence of clumps of grey or black pigment
beneath the retina.
10
EARLY AGE RELATED MACULOPATHY (ARM)
Presence of one or more drusen≥ 125 µm (with or without pigmentary abnormalities) or one
or more drusen 63 - 124µm with pigmentary abnormalities in a 6000µm diameter grading
grid centred on the fovea, in the absence of advanced AMD (geographic atrophy or
neovascular AMD).
LATE AGE RELATED MACULOPATHY (AMD)
Tagged AMD by the International ARM group,19 this includes:
a) Geographic atrophy: Disease area of retinal depigmentation characterized by sharp edges
>175µm in diameter and visible choroidal vessels in the absence of exudative AMD.
b) Exudative / Neovascular AMD: Includes the presence of:
i. Serous or haemorrhagic detachment of RPE of sensory retina.
ii. Sub-retinal or sub-pigment epithelial haemorrhage or sub-retinal fibrous scar.
iii. Photocoagulation scars from laser therapy for sub-retinal neovascular membrane.
iv. Choroidal neovascularization.

11
RISK FACTORS
Many risk factors have been identified for ARMD and these include:
1. Age
Age has been implicated as the strongest risk factor for age related macular degeneration. It is
a leading cause of visual loss in the elderly globally.47-49 There is an increased preponderance
of the disease as age increases, being more clinically apparent after 50 years of age, though
data from the United Kingdom reflects individuals aged 65-75 years having age-related
macular degeneration.12,19,26 Data from three population-based studies namely the Blue
Mountains Eye Study, Beaver Dam Eye Study and the Rotterdam Study show an increase in
prevalence of ARMD from 0 – 2% in patients aged 55 – 64 years to about 13% in patients
over 85 years.50 Findings from the Eastern and Mid-Western parts of Nigeria show an
increase in the occurrence of this disease with advancing age.42,46
2. Lifestyle
a. Tobacco smoking
Cigarette smoking is a well-established risk factor for the development of age related macular
degeneration.51-54 It is a major modifiable risk factor for the development of age-related
macular degeneration. Studies have shown that those who smoke are three times at risk of
developing macular degeneration.50 Smokers may develop macular degeneration about ten
years earlier than non-smokers and there is a dose-response relationship between pack years
of smoking and the development of ARMD.52,55-57 A pack year reflects the lifetime exposure
to tobacco by an individual and is expressed as a numerical value. It is calculated by
multiplying the number of years an individual has smoked cigarettes by the number of packs
of cigarettes smoked per day.55 Several studies have investigated and confirmed this dose-

12
response relationship. The Rotterdam and POLA (Pathologies Oculaires Liées à l'Age)
studies showed increased risk of neovascular ARMD in individuals who had smoked 10
pack-years or more.58,59 The Physicians’ Health Study and the Nurses’ Health Study found a
two-fold higher risk of ARMD in individuals who had smoked more than 25 cigarettes per
day.60,61 The Beaver Dam Offspring Study confirmed that smoking 11 pack-years or more
was associated with the presence of early ARMD.62 Despite cessation of smoking, evidence
shows that the risk of neovascular ARMD persists in ex-smokers of up to 20years, as
confirmed by The Rotterdam and POLA studies.58,59 Smoking has been implicated in the
reduction of serum antioxidant levels which is a plausible mechanism by which age-related
macular degeneration results in smokers.63 Though smoking has been confirmed to be
strongly associated with ARMD, some studies found no association or only a very weak link
between them.64-69 West et al64 found an insignificant reduced risk of ARMD in those who
had ever smoked cigarettes, in a small cross-sectional study, and Blumenkranz et al65 found a
small insignificant increase among current smokers in a small case–control study. A large
French case–control study found only a weak and insignificant association between ARMD
with previous and current smoking.66 Although the Beaver Dam Eye Study found a strong
association between smoking and neovascular ARMD,67 the association at the 5- and 10-year
follow-up examinations was weaker.68,69
b. Alcohol intake
Although the pathophysiology of ARMD is not fully understood, some of the current theories
on aetiology could implicate alcohol in their mechanisms of action. Alcohol is a known
neurotoxin that can cause oxidative brain damage and, hence, it is logical that the retina could
be similarly affected.70,71 Two cross-sectional and three incidence studies found an
association between alcohol consumption and risk of ARMD.72-76 These were population-

13
based studies which showed that heavy consumption of alcohol (> 5 drinks per session)
increased the incidence of late ARMD. Beer drinking was associated with an increased risk
of advanced ARMD but wine drinking was shown to be protective to the retinal pigment. In a
prospective population-based study in Beaver Dam, heavy drinking (four or more drinks
daily) at baseline was related to the 15-year cumulative incidence of pure geographic atrophy
in men (odds ratio: 9.2, 95% confidence interval: 1.7-51.2). There were no consistent
associations with the amount of beer, wine or liquor consumption and the incidence or
progression of ARMD.77 No association was found between overall or specific alcohol
consumption and development of early ARMD or dry or wet late ARMD in the Rotterdam
Study.78 Cross-sectional analyses of the results of The Blue Mountains Eye Study79 found no
association between ARMD and overall alcohol intake and more specifically beer
consumption; however, consumption of spirits was associated with the presence of early
ARMD.
c. Diet and nutrition
Diet is emerging as a potentially modifiable risk factor for ARMD.80-83 Research suggests
that diet could influence the risk of ARMD, but the associations found have not been
consistent across studies.84-86 Diet high in trans fat, and red meat, have been associated with
an increased risk of ARMD,81,87,88 whereas higher intakes of fish have been associated with a
lower risk of ARMD.86,89 Dietary pattern rather than specific food items have been
implicated. Amirul et al90 reported that a diet characterised by frequent consumption of boiled
rice, muesli, fish (not fried), chicken (not fried), and a variety of vegetables and avoidance of
white bread was associated with a lower prevalence of advanced ARMD, whereas a diet
characterised by a pattern of eating red and processed meats and fried foods was associated
with a higher prevalence of advanced ARMD. Evidence is continuing to mount that the

14
choices we make about food we consume may play a role in contributing to the risk of
developing ARMD.90
d. Obesity
Body Mass Index (BMI) calculated as weight in kilogrammes divided by height in metres
squared, a measure of obesity, has been implicated as a risk factor for ARMD. In a hospital –
based study conducted in Boston, higher BMI was shown to increase the risk of progression
to advanced form of ARMD.91 Relative risk (RR) was 2.35 (95% CI, 1.27 – 4.34) for a BMI
of at least 30 and 2.32 (95% CI, 1.32 – 4.07) for a BMI of 25 – 29. Increased physical activity
tended to be associated with a reduced rate of progression of ARMD (25% reduction for
exercising 3 times weekly versus none, P = 0.05 – P = 0.07).
Another study showed that the incidence of visually significant dry ARMD was lowest in
men with normal BMI, but no significant relationship of BMI and neovascular ARMD could
be proven due to the few number of cases analysed in the study.92 The Beaver Dam Eye
Study93 examined the relationship between exercise and ARMD, concluding that walking at
least 12 blocks a day decreased the incidence of wet ARMD by 30% over 15 years (OR 0.7,
95% CI 0.6 to 0.97). An active lifestyle (regular activity ≥ 3times weekly) decreased the risk
of exudative ARMD (OR 0.3, 95% CI 0.1 – 0.7) compared with individuals with a sedentary
lifestyle.93 In general, reported findings suggest an increased risk of ARMD with increasing
BMI and abdominal obesity.94-96

15
3. Ocular
a. Refractive status
A number of studies have reported an increased risk of ARMD associated with hyperopia.97-
102 Statistically significant associations were demonstrated between senile macular
degeneration and hyperopia in a case – control study carried out in Baltimore, United States
of America.97 Sandberg et al98 showed that patients with a refractive error of ≥ +0.75 D were
more likely to have neovascular ARMD compared with patients with other refractive errors
(odds ratio, 2.40; 95% confidence interval, 1.53-3.78; P < 0.001). Hyperopia was the most
significant risk factor for ARMD in a study from North India.102 Studies from Australia
confirmed an association between hyperopia and AMD.100,101
The Eye Disease Case-Control Study found that persons with hyperopia had a slightly higher
risk of neovascular AMD, but the association did not remain statistically significant after
multivariate modelling.103 One caveat in the interpretation of findings in these case-control
studies is that because the controls were recruited from ophthalmology clinics, the control
groups may be enriched in the proportion of myopes compared with the general
population.103
b. Iris colour
Evidence is inconsistent for an association between iris colour and development of ARMD,
but a plausible explanation is that the lower risk for ARMD among subjects with darker iris
colour may be due to the fact that these individuals have more tissue melanin. This increased
pigmentation may provide some protection to the retina from exposure to sunlight, reducing
direct photo-oxidative damage and thus reducing the risk of ARMD. Despite this theoretic
protective effect, iris colour has not consistently been associated with ARMD. Weiter et al104
found that 76% of 650 patients with ARMD had light irides compared with 40% of 363
controls (p = 0.0001). In contrast, the Beaver Dam Eye Study found an inconsistent

16
relationship between iris colour and 10-year incidence of drusen and pigmentary
abnormalities.105 The reasons for these disparities are not clear.
c. Macular pigment
Macular pigment is composed of two carotenoids, lutein and zeaxanthin, which are solely of
dietary origin and which are found in a wide variety of green leafy plants such as spinach and
kale and in some animal products such as egg yolk.106 In the Age-related Eye Disease Study
(AREDS), a higher dietary intake of lutein and zeaxanthin, measured using a self-
administered food frequency questionnaire was associated with a statistically lower risk of
developing advanced ARMD compared to having a lower intake.107
4. Systemic morbidities
a. Hypertension
Hypertension plausibly increases the risk of ARMD due to its effects on the choroidal
circulation.108 Some large population-based studies have shown a small and consistent
association between ARMD and systemic hypertension. Kahn et al109, using data from the
Framingham Heart and Eye Studies found a positive association between the presence of
ARMD and higher levels of diastolic blood pressure measured many years before eye
examination. Sperduto and Hiller110, using data from the Framingham Heart and Eye Studies,
found the age and sex adjusted relative risk for any ARMD was 1.18 (95% CI, 1.01 – 1.37),
for persons diagnosed with hypertension 25 years before eye examination and 1.04 (95% CI,
0.96 – 1.23) for persons with hypertension at the time of the eye examination, when
compared with those without hypertension. Other population-based cross-sectional studies
detected no association between hypertension and ARMD, including the Blue Mountains Eye
Study, Atherosclerosis Risk in Community Study and Andhra Pradesh Eye Disease Study.111-
113
17
b. Diabetes mellitus
Many studies have investigated the relationship between diabetes mellitus and ARMD but
few studies have found any link. 114 The Blue Mountains Eye Study found geographic atrophy
to be significantly associated with diabetes (OR, 4.0; 95% CI, 1.6 – 10.3), but no association
was found with either neovascular ARMD (OR, 1.2; 95% CI, 0.4 – 3.5) or early ARMD (OR,
1.0; 95% CI, 0.5 – 1.8). There was also no association found between impaired fasting
glucose and ARMD in the Blue Mountains Eye Study and the Atherosclerosis Risk in
Communities Study.112,115 Choi et al116 in a population-based study of 3008 participants aged
50 – 87 years found a significant association between diabetes mellitus and early age related
macular degeneration (OR 1.87; 95% CI, 1.07 – 3.25). The mechanism is by altering the
haemodynamics, increasing oxidative stress, with resultant accumulation of advanced
glycation end-products.117
c. Hyperlipidaemia
Dietary fat intake, particularly intake of saturated fat and cholesterol has been suggested to be
associated with an increased risk for atherosclerosis, thus increasing the risk for ARMD. The
Eye Disease Case- Control Study118 found that individuals with mid-range (4.889 – 6.748
mmol/L) and high (> 6.748mmol/L) total cholesterol levels compared with those with low
levels (< 4.889mmol/L) had OR for neovascular ARMD of 2.2 (95% CI, 1.3 – 3.4) and 4.1
(95% CI, 2.3 – 7.3), respectively, after controlling for other factors. A slight but not
statistically significant increased risk of neovascular ARMD was seen with increasing levels
of serum triglycerides in the same study. Several other studies including the Rotterdam study,
Blue Mountains Eye Study and Atherosclerosis Risk in Communities Study did not find any
association between serum cholesterol and HDL cholesterol with AMD.111,112,119 The Beaver
18
Dam Eye Study and Blue Mountains Eye Study found no association between the use of
lipid-lowering agents and the risk of developing ARMD.115
5. Genetic
A family history of ARMD is a risk factor for ARMD. In 2005 it was established that a
mutation in a key regulator of the complement pathway: complement factor H (CFH) located
on chromosome 1q31 is strongly associated with a risk of ARMD.120,121 The Y402H
polymorphism in this gene has a minor allele frequency of 40% and is highly associated with
AMD.121 Other genes with sequence variants established in all studies related to genetics and
AMD include LOC 387715/PRSS 11 and BF/C2 protective variants. Some other variations
have been reported to be associated with an increase in the risk of ARMD, but minimal
support for these associations exist.
6. Others
a. Sunlight
It has been hypothesized that sun exposure is a risk factor for ARMD.122-124 Light exposure,
specifically blue light, bright sunlight, and ultraviolet (UV) radiation, has been implicated in
photochemical oxidative damage and light-induced apoptosis of the RPE cells.125,126
b. Gender
Studies have reported a higher prevalence of ARMD in women, but much of this increased
risk can be attributed to increased longevity in women.69 In the Blue Mountains Eye Study127
conducted in Sydney, Australia, women had higher prevalence of ARMD than men although
no significant statistical difference was observed.

19
c. Social class
Studies have suggested that increasing years of education are associated with a decreased risk
of ARMD but no strong associations have been observed, hence the unlikelihood that social
class would impact on the incidence of ARMD.128,129
d. Race
Age-related macular degeneration has been shown to have a racial predilection. A cross –
sectional population-based study in East Baltimore conducted among blacks and whites
identified drusen in both groups, large drusen (>125µm) occurring more frequently among
older whites over 70years of age (15% versus 9%).130 Pigmentary abnormalities were found
to be more prevalent among the white population (7.9% versus 0.4%). Age-related macular
degeneration had a prevalence rate of 2.1% among the white population over 70years of age
with no ARMD detected in black subjects in this group.
In a multi-ethnic study of atherosclerosis among four racial ethnic groups (white, black,
Hispanic and Chinese), the prevalence of ARMD was lower in blacks compared with whites
(2.4% versus 5.4%).131 White persons are generally more likely than black persons to have
medium or large drusen, focal pigment abnormalities, and advanced ARMD. More severe
forms of age-related maculopathy are more prevalent in older whites.130
e. Cataract and cataract surgery
It is thought that both ARMD and cataract result from accumulation of oxidative damage in
the form of reactive oxygen species, from both internal sources (mitochondria) and external
sources (sunlight).132 A meta-analysis found that cataract surgery was associated with late
ARMD with an odds risk ratio from pooled prospective studies of 3.05 (95% confidence
intervals 2.05 - 4.55).133 The Beaver Dam Eye Study was included in that meta-analysis, but

20
has since published 15 year results, finding that cataract surgery is associated with increased
ARMD risk, after correcting for other risk factors including complement factor H and age-
related maculopathy susceptibility 2 (ARMS2) risk alleles.134 The risk was greatest if surgery
had been performed more than five years previously rather than less than five years from the
study time-point.
21
CHAPTER 4
MATERIALS AND METHOD
STUDY AREA
This study was carried out in the out-patient clinic of the Department of Ophthalmology,
University of Benin Teaching Hospital (UBTH), Benin City, Nigeria. Established in 1973,
the hospital is situated on the outskirts of Benin City on a 150 acre site along the Lagos-
Benin express road in Egor local government area of Edo state. It is located in the rainforest
belt with high humidity, high annual rainfall and average temperature of 320C.
It has a well-defined catchment area – Edo, Delta, Ondo, Kogi and Anambra states and has
over 600 bed spaces.
STUDY DESIGN
This was a descriptive hospital-based study.
STUDY DURATION
This study was carried out over a period of six months (December 2015 – June 2016).
STUDY POPULATION
The study was conducted among consecutive consenting new adults aged 50 years and above,
who were registered patients at the eye clinic of UBTH.
Inclusion criteria:
Cases
a. New patients attending the eye clinic, with a diagnosis of ARMD
b. Consenting adults aged 50 years and above
22
Controls
a. New patients attending the eye clinic, without a diagnosis of ARMD
b. Consenting adults aged 50 years and above
Exclusion criteria:
a. Non-consenting adults
b. Adults aged below 50years
c. Significant media opacities obscuring fundus visualization
d. Prior history of severe trauma to the eyes
e. Retinal lesions/pathology e.g. retinal vascular occlusions, proliferative diabetic
retinopathy, diabetic macular oedema
SAMPLE SIZE DETERMINATION
The total population is more than 10,000 for the catchment area. The sample population was
calculated using the formula135:
2
2
d
pqZn
Where:
n = desired sample size (population greater than 10,000)
Z = the standard normal deviate, usually set at 1.96, corresponding to 95% confidence
interval
p = proportion of the target population estimated to have a particular characteristic.
The prevalence of age-related macular degeneration from a previous hospital-based study
was 7.4% .42
q = 1.0 – p

23
= 1.0 – 0.074
= 0.926
d = degree of precision required which is 5% (set at 0.05) for this study.
Thus,
2
2
d
pqZn
n = (1.96)2 X 0.074 X 0.926
0.052
= 105.30
≈ 106
In order to make an allowance for non-responders and attrition, 10% of the minimum sample
size calculated was added to the sample size.
i.e. 106 + (0.10 X 106) = 106 + 10.6
= 116.6
≈ 120
One hundred and twenty (120) new patients was the targeted sample size for this study.
Age and sex-matched healthy controls were recruited for the study. Thus a minimum of 120
cases and 120 controls were recruited.
SAMPLING TECHNIQUE
Convenience sampling was done.

24
PRE-STUDY ACTIVITIES
1. Ethical clearance to conduct this research was sought and obtained from the Ethics
and Research Committee of the University of Benin Teaching Hospital, Benin City,
Nigeria, before commencement of this study.
2. Permission was obtained from the National Postgraduate Medical College of Nigeria
before commencement of this study.
3. A three-day training for the survey team was conducted by the principal investigator.
4. Written informed consent was obtained from each respondent before the conduct of
interviews.
5. Confidentiality and privacy was respected during the course of the interviews.
Participants were treated with dignity and respect.
6. There was no risk of harm or injury to the participants during or after the study was
conducted.
PROTOCOL
A structured interviewer-administered questionnaire was used to collect the data. The
developed questionnaire was read by two ophthalmologists (supervisors) to ensure clarity and
adherence to objectives of the study. The questionnaire was categorized into three (3)
sections: A, B and C. Section A contained the biodata of the participants in the study. Section
B contained the medical and social history which included the presence or absence of
diabetes mellitus, hypertension, dyslipidaemia, duration of diagnosis and current medical
therapy. Questions were asked on indulgence in cigarette smoking, alcohol consumption,
intake of junk food, fruits and vegetables. Section C consisted of the ocular history and
examination.
25
THE STUDY TEAM
1. An Ophthalmologist-in-training (the principal investigator)
2. Two trained Ophthalmology registrars
3. An Optometrist
4. Two nurses
STUDY MATERIALS
1. Sphygmomanometer
2. Stethoscope (Littman’s)
3. Standometer
4. Weighing scale
5. Illiterate “E” chart and Snellen chart
6. Near vision chart (N5 chart)
7. Trial lens box
8. +20D, +78D lens
9. Pen torches, batteries
10. Direct ophthalmoscopes (Welch Allyn)
11. Binocular Indirect ophthalmoscope (Appasamy) – Model AAIO wireless
12. Carl Zeiss Slit lamp biomicroscope (Model SL 115)
13. Amsler grid chart
14. Dilating drops –Guttae 1% tropicamide and 2.5% phenylephrine (AppamidePlusR)and
Guttae Tropicamide (in hypertensives)
15. Fundus camera - 30° Zeiss FF 450 plus mydriatic camera
16. Stationeries
17. Standard photographs from the International ARM Epidemiological Study Group

26
PRE-TEST
Following completion of the training of the survey team, a pre-test was carried out in the out-
patient clinic of the Department of Ophthalmology, Stella Obasanjo Hospital, Benin City.
Twenty (20) consenting adults were selected for administration of questionnaire and
ophthalmic examination. The aim was to provide a practical field experience to the survey
team as well as test the feasibility of the study procedure, data collection process and
standardize the questionnaire. One more question (intake of fish, red meat or white meat) was
included after pretesting.
DATA COLLECTION
All consecutive consenting new patients, aged 50 years and above, who met the inclusion
criteria presenting at the Ophthalmology out-patient clinic of the UBTH within the study
period were enrolled. Convenience sampling was done. Informed consent (Appendix II) was
obtained by the trained Ophthalmology registrars. Basic demographic data was collected by
the registrars using the structured interviewer-administered questionnaire. The accurate age
of illiterate participants was determined using landmark historical events. Case files of
registered participants were specially marked to prevent duplication of respondents.
The nurses measured the blood pressure using a sphygmomanometer and a stethoscope and
anthropometric measurements (weight and height) using a weighing scale and a standometer
respectively.
Registered respondents proceeded to the next stage which involved a personal interview
conducted by the trained Ophthalmology registrars and the principal researcher. A structured
interviewer - based questionnaire (Appendix III) was administered.
27
Visual acuity was done by the Optometrist using an illuminated Snellen’s chart or an illiterate
E chart depending on the literacy level of the participant. Near vision was tested using a new
version near chart held at 33cm from the patient. The Snellen / Illiterate E chart was placed at
a distance of 6m from the participant in a well lit room. The test was performed monocularly.
The last completed line read on the chart was recorded as the visual acuity for that eye.
Visual acuity using a pin hole disc was performed if the visual acuity was less than 6/6. For
those with VA < 6/60, the ability to count fingers at 3m, to perceive hand movements or light
was determined. Refraction was done by the optometrist to obtain the best corrected visual
acuity of patients who showed improvement in their visual acuity using a pin hole disc and
for aphakic patients. Respondents were then examined by the principal investigator
(researcher) in one of the clinic rooms. The anterior segment examination was done using a
bright pen torch and a Carl Zeiss slit lamp biomicroscope. Direct ophthalmoscopy was done
and dilatation was performed to facilitate indirect ophthalmoscopy. Participants with features
suggestive of age-related macular degeneration were examined using the slit lamp
biomicroscope with a +78D lens. Examination findings were documented using the
examination proforma (Appendix III).
Respondents with features of age-related macular degeneration proceeded to have fundus
photographs taken. Photographs were taken in a darkened room, with patient seated having
both eyes dilated and given a fixation target. Photographs were then compared using standard
photographs from the International ARM Epidemiological Study Group to help get an
objective assessment of the lesion and classification. Measurements of the size of the lesion
were taken using the optic disc as a scale (assuming that a disc diameter is 1500 µm). The
photographed lesions were reviewed with the supervisors for agreement on the diagnosis.
Further investigation of Fundus Fluorescein Angiography and/or Optical Coherence
Tomography was performed when indicated in cases suspected to have neovascular ARMD.

28
Registered participants had their fasting blood glucose and fasting serum lipid profiles
checked. The participants were asked to come to the clinic the next morning at a particular
time for the blood samples to be taken. This ensured uniformity of results obtained
throughout the course of the study. Results were analysed by a chemical pathologist.
FLOW CHART OF ACTIVITIES
DATA MANAGEMENT
The collected data was entered into a database, cleaned and analysed using the International
Business Machine Statistical Product for Scientific Solutions version 20 software (IBM SPSS
Inc, Chicago IL., U.S.A.). An initial frequency count of all variables was done and results
were presented as tables or figures. Means and standard deviations (SD) were determined.
Tests of statistical significance included Chi-squared test, Student t-test, Independent sample
t-test, Fisher’s exact test, Mann-Whitney U test and Regression analysis. The analysis was
considered to show significant associations when the p value was less than 0.05.
Registration of participants
( Ophthalmology registrar)
Measurement of BP, Weight, Height
(Nurses)
Administration of questionnaire
(Ophthalmology registrar)
Ocular examination (Principal Investigator)
Dilatation of eyes (Ophthalmology
registrar)
Slit Lamp Biomicroscopy
(Principal Investigator)
Fundus photography and FFA
(Principal Investigator)
Blood sample collection
(Chemical pathology intern)
Blood sample analysis (Chemical Pathologist)

29
CHAPTER 5
RESULTS
A total of 240 respondents: 120 cases and 120 controls participated in the study. There were
97 males (40.4%) and 143 females (59.6%), giving a male to female ratio of 1:1.5. The age
range was 50 – 88 years and the mean age was 66.7 years (SD ± 8.0).
Table 1: Socio-demographic characteristics of cases with ARMD and controls.
Variables Cases
n = 120 (%)
Control
n = 120 (%)
p-value**
Age group (years)*
50 – 59 19 (15.8) 26 (21.7) 0.514
60 – 69 48 (40.0) 49 (40.8)
70 – 79 43 (35.8) 39 (32.5)
80+ 10 (8.3) 6 (5.0)
Sex
Male 48 (40.0) 49 (40.8) 0.895
Female 72 (60.0) 71 (59.2)
Employment status
Employed 69 (57.5) 77 (64.2) 0.290
Unemployed 51 (42.5) 43 (35.8)
Level of education
None 1 (0.8) 4 (3.3) 0.010+
Primary 47 (39.2) 29 (24.2)
Secondary 50 (41.7) 47 (39.2)
Tertiary 22 (18.3) 40 (33.3)
Residence
Urban 117 (97.5) 112 (93.3) 0.130
Rural
Social class
1
2
3
4
5
3 (2.5)
0 (0.0)
5 (4.2)
46 (38.3)
5 (4.2)
64 (53.3)
8 (6.7)
0 (0.0)
2 (1.7)
54 (45.0)
8 (6.7)
56 (46.6)
0.369 **
*Mean ± standard deviation: 66.7 ± 8.0 years (cases: 67.8 ± 8.1 years, control: 65.5 ± 7.8
years), **Chi-square test, +Fisher’s exact test

30
A higher proportion of the respondents in both study groups were in the age group 60 – 69
years; cases 48 (40.0%), controls 49 (40.8%) years (Table 1). The mean ages of the
respondents were cases; 67.8 ± 8.1 years, control; 65.5 ± 7.8 years. The difference in
proportions of age group categories between the study groups was not statistically significant
(p=0.514). There were equal number of males and females in both study groups. The
difference in proportion of sex in both groups was not statistically significant (p=0.895).
Sixty nine (57.5%) of the cases were employed compared to 49 (40.8%) of the controls. The
differences in the proportions of categories of employment status between the study groups
was not statistically significant (p=0.290). Forty seven (39.2%), and 22 (18.3%) of the cases
had primary and tertiary education respectively compared to 29 (24.2%) and 40 (33.3%) of
the controls. The differences in proportion was statistically significant (p=0.010). Similar
proportions of respondents in both cases 117 (97.5%) and controls 112 (93.3%) resided in an
urban area. This difference in proportions was not statistically significant (p=0.130).

31
Table 2: Chronic conditions and lifestyle behaviours in cases with ARMD and controls
Chronic conditions and
lifestyle
Cases Control
p-value* n (%) Duration
years
(mean ± sd)
n (%) Duration
years
(mean ± sd)
Diabetics 24 (20.0) 7.8 ± 6.5 19 (15.8) 10.1 ± 7.9 0.400
Hypertensives 46 (38.3) 8.3 ± 7.6 57 (47.5) 8.7 ± 7.1 0.151
On lipid lowering drugs 1 (0.8) 1.0 ± 0.0 3 (2.5) 1.7 ± 0.6 0.313+
Smoked cigarette (per
week)
2 (1.7) 25.0 ± 7.1 1 (0.8) - 0.561+
Take alcohol (per week) 7 (5.8) 9.7 ± 7.8 4 (3.3) 11.5 ± 12.8 0.354
Ate Fast food (per week) 1 (0.8) - 2 (1.7) 2.0 ± 0.0 0.561+
Ate fruits (per week) 17 (14.2) 3.7 ± 1.8 35 (29.2) 3.3 ± 1.3 0.005
Ate vegetables (per week) 53 (44.2) 3.6 ± 0.7 61 (50.8) 4.0 ± 1.4 0.301
*Chi-square test of proportions, +Fisher’s exact test
Table 2 shows that weekly consumption of fruits was statistically significantly more common
among the controls than in the cases with ARMD (P = 0.005). There was no statistically
significant relationship between the presence of chronic medical conditions such as diabetes
mellitus, hypertension, dyslipidaemia and risk of having ARMD in both cases and controls.

32
Table 3: Major sources of animal protein by cases with ARMD and controls
Variables Cases
n = 120 (%)
Control
n = 120 (%)
p-value
Fish 118 (98.3) 114 (95.0) 0.407+
Red meat 1 (0.8) 4 (3.3)
White meat 1 (0.8) 2 (1.7)
+Fisher’s exact test
Table 3 shows that the majority of the respondents in both study groups obtained proteins
predominantly through eating of fish; cases 118 (98.3%), controls 114 (95.0%). This
difference in proportion was not statistically significant (p=0.407).

33
Table 4: Ocular history of cases and controls
Variables Cases
n = 120 (%)
Control
n = 120 (%)
p-value
Used glasses 46 (38.3) 64 (53.3) 0.026*
- Glasses tinted/photochromic 0 (0.0) 8 (11.8) 0.003+
Use sunshades 1 (0.8) 1 (0.8) 0.999+
*Chi-square test of proportions, +Fisher’s exact test
Majority of those who used glasses were the control group. This difference in proportion was
statistically significant (p=0.026).

34
Table 5: Refractive state among the cases with ARMD and controls
Variables Cases
n = 120 (%)
Control
n = 120 (%)
p-value
Hypermetropia 93 (77.5) 108 (90.0) 0.003+
Myopia
Emmetropia
25 (20.8)
2 (1.7)
8 (6.7)
4 (3.3)
+Fisher’s exact test
Ninety three (77.5%) of the cases had hypermetropia compared to 108 (90.0%) of the control
group (Table 5). However, a significant portion of the cases (20.8%) were myopic compared
to controls (6.7%).

35
Table 6: Anthropometric measurements in cases with ARMD and controls
Variables Cases
(mean ± sd)
Control
(mean ± sd)
p-value*
Weight (kg) 74.4 ± 7.6 78.0 ± 11.5 0.004
Height (m) 1.61 ± 0.06 1.64 ± 0.10 0.001
Body mass index (kg/m2) 28.9 ± 2.9 29.3 ± 5.7 0.493
*Independent sample t-test
Table 6 shows that the controls weighed more and were averagely taller than the cases with
ARMD, and these were statistically significant (P < 0.05).The difference in the mean body
mass index of the two study groups was not statistically significant.

36
Figure 1: Body mass index of controls and cases with ARMD
Figure 1 shows that overall, most cases (90%) and controls (80%) were overweight.
0 (0.0)
12 (10.2)
106 (89.8)
1 (0.8)
23 (19.2)
96 (80.0)
0
20
40
60
80
100
120
Underweight Normal Overweight
Freq
uen
cy (
%)
Body mass index category
Cases
Control

37
Table 7: Visual acuity of both eyes among cases with ARMD and controls
Visual
acuity†
Right eye
Median (IQR)
p-
value*
Left eye
Median (IQR)
p-
value* Cases Control Cases Control
Unaided 6/18 (6/9 – CF at 1.5m) 6/12 (6/6 – 6/24) 0.120 6/18 (6/9 – 6/24) 6/12 (6/6 – 6/24) 0.014
Pinhole 6/12 (6/6 – CF at 1.5m) 6/9 (6/6 – 6/12) 0.004 6/9 (6/9 – 6/18) 6/9 (6/6 – 6/12) 0.013
Best
corrected
6/9 (6/6 – CF at 1.5m) 6/6 (6/6 – 6/9) 0.001 6/9 (6/6 – 6/12) 6/6 (6/6 – 6/9) 0.001
*Mann-Whitney U test (comparing difference in median values), IQR: interquartile
range, †values are denominators (while 6 is the numerator).
Table 7 shows that the median unaided visual acuity in the right eye of those with ARMD
was 6/18 while it was 6/12 in the controls. Unaided visual acuity was significantly improved
in the right eye using a pin hole in both cases and controls (P=0.004) and the overall best
corrected visual acuity in both eyes was significantly improved in both study groups
(P=0.001).

38
Table 8: Ocular examination of both eyes across study groups of cases with ARMD and
controls.
Right eye
p-
value*
Left eye
p-
value*
Cases
n = 120 (%)
Control
n = 120 (%)
Cases
n = 120 (%)
Control
n = 120 (%)
Lens
Transparent
Opacities
Amsler grid
Normal
Abnormal
Vitreous
16 (13.3)
104 (86.7)
92 (76.7)
28 (23.3)
50 (41.7)
70 (58.3)
119 (99.2)
1 (0.8)
<0.001*
<0.001*
17 (14.2)
103 (85.8)
93 (77.5)
27 (22.5)
46 (38.3)
74 (61.7)
119 (99.2)
1 (0.8)
<0.001*
<0.001*
Clear 114 (95.0) 120 (100.0) 0.013† 113 (94.2) 120 (100.0) <0.001†
Hazy 6 (5.0) 0 (0.0) 7 (5.8) 0 (0.0)
Macula
Normal 12 (10.0) 120 (100.0) <0.001 11 (9.2) 120 (100.0) <0.001
Abnormal 108 (90.0) 0 (0.0) 109 (90.8) 0 (0.0)
Disc (VCDR)‡
0.4 (0.3 – 0.6) 0.4 (0.2 – 0.5) 0.615# 0.4 (0.3 – 0.6) 0.4 (0.2 – 0.5) 0.812#
Drusen (present )
Yes 16 (13.3) 0 (0.0) <0.001 15 (12.5) 0 (0.0) <0.001
No
104 (86.7) 120 (100.0) 105 (87.5) 120 (100.0)
RPE abnormality
(present)
Yes 113 (94.2) 0 (0.0) <0.001 113 (94.2) 0 (0.0) <0.001
No
Geographic atrophy
Yes
No
Neovascular ARMD
Yes
No
7 (5.8)
0 (0.0)
120 (100.0)
2 (1.7)
118 (98.3)
120 (100.0)
0 (0.0)
120 (100.0)
0 (0.0)
120 (100.0)
7 (5.8)
0 (0.0)
120 (100.0)
0 (0.0)
120 (100.0)
120 (100.0)
0 (0.0)
120 (100.0)
0 (0.0)
120 (100.0)
*Chi-square test, †Fisher’s exact test, ‡Median (IQR), #Mann-Whitney U test.

39
A greater proportion of the cases with ARMD had lens opacities compared to the controls
and this was statistically significant (p<0.001). Amsler grid was abnormal in some of the
cases with ARMD (23.3%) and this was statistically significant (p<0.001). Of the cases with
ARMD, about 10% of them had unilateral macula abnormalities. Retinal pigment epithelium
abnormality was the more common posterior segment finding among cases with ARMD
(94.2%) compared to drusen (≈13%).
Figure 2: Pattern of ARMD seen among cases.
Figure 2 shows that the predominant form of ARMD seen was early (98.3%)
Pattern of ARMD seen
Early ARMD Late ARMD
40
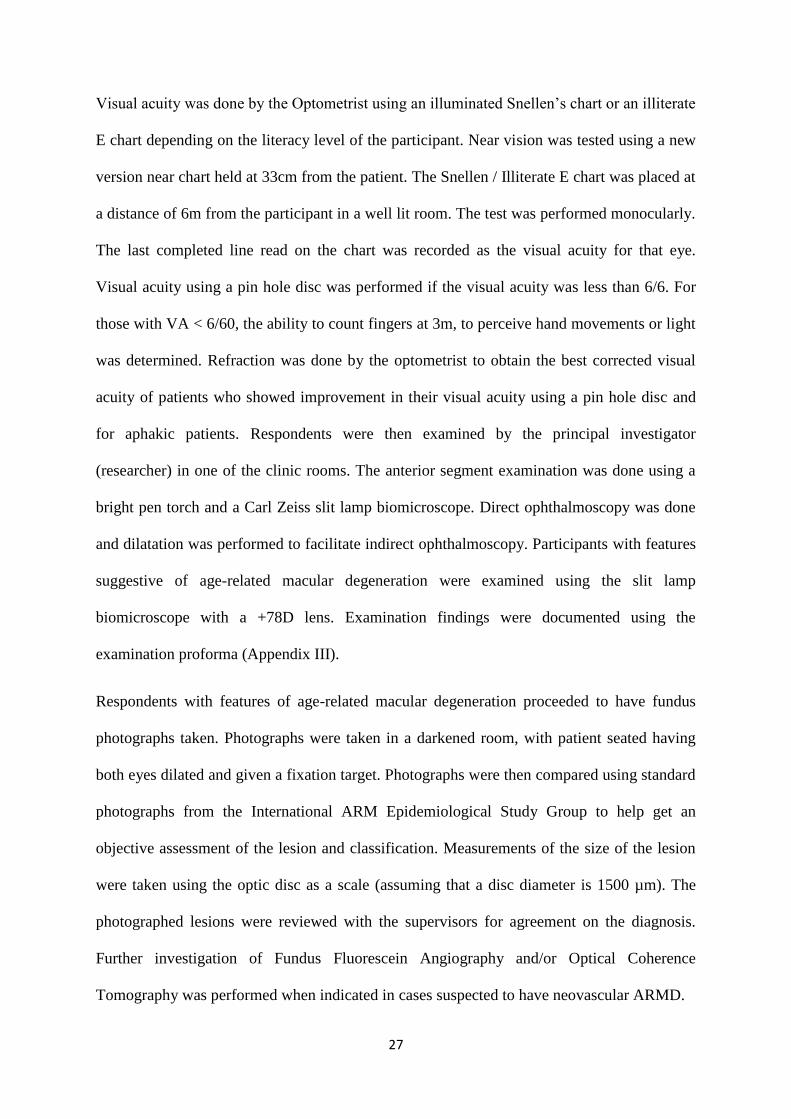
Figure 3: Drusen pattern in the right and left eyes of respondents with ARMD
Sixteen respondents (13.3%) in the case group had drusen in the right eye of which 15
(93.8%) had hard drusen and 1 (6.3%) had soft drusen (Figure 2). Fifteen (12.5%) of the
respondents in the case group had drusen in the left eye of which 13 (86.7%) had hard drusen
and 2 (13.3%) had soft drusen.
Hard, 15 (93.8%)
Soft, 1 (6.3%)
Drusen Absent RE 104 (86.7%)
Drusen Present RE 16 (13.3%)
Hard 13 (86.7%)
Soft, 2 (13.3%)
Drusen Absent LE105 (87.5%)
Drusen Present LE 15 (12.5%)

41
Figure 4: Pattern of retinal pigmentation among the respondents with ARMD
The majority of cases with ARMD had RPE hyperpigmentation as against hypopigmentation
(Figure 3).
114 (99.1%)
1 (0.9%)
113 (98.3%)
2 (1.7%)
0
20
40
60
80
100
120
Hyperpigmentation Hypopigmentation
Fre
qu
en
cy (
%)
Eye Pigmentation
Right
Left

42
Table 9: Biochemical parameters of cases with ARMD and controls
Variables Cases
n = 120 (%)
Control
n = 120 (%)
p-value*
Fasting blood glucose
Normal 117 (97.5) 114 (95.0) 0.309
Abnormal 3 (2.5) 6 (5.0)
Total cholesterol
Normal 117 (97.5) 117 (97.5) 0.999
Abnormal 3 (2.5) 3 (2.5)
HDL-Cholesterol
Normal 117 (97.5) 119 (99.2) 0.314
Abnormal 3 (2.5) 1 (0.8)
LDL-Cholesterol
Normal 117 (97.5) 119 (99.2) 0.314
Abnormal 3 (2.5) 1 (0.8)
Triglycerides
Normal 117 (97.5) 119 (99.2) 0.314
Abnormal 3 (2.5) 1 (0.8)
*Fisher’s exact test
Table 10 shows that one hundred and seventeen (97.5%) of the respondents in the case group
compared to 114 (95.0%) of the respondents in the control group had normal fasting blood
glucose. This difference in proportions was not statistically significant (p=0.120). Equal
number of respondents in both study groups had normal cholesterol levels.
One hundred and seventeen (97.5%) of the respondents in the case group compared to 119
(99.2%) of the respondents in the control group had normal HDL-cholesterol levels. This
difference in proportions was not statistically significant (p=0.314). Same values were
observed for LDL-cholesterol and triglycerides.

43
Table 10: Risk factors for ARMD among the cases
Risk factors Unadjusted OR (95% CI) Adjusted OR (95% CI)**
Age (years) 1.08 (1.05 – 1.12) 1.13 (1.05 – 1.21)†
Sex (Male)* 1.99 (1.14 – 3.46) 3.07 (0.92 – 10.23)
Residence (Urban)* 2.74 (0.71 – 10.59) 3.08 (0.13 – 73.14)
Level of education*
None 0.48 (0.05 – 4.54) 0.67 (0.01 – 33.59)
Primary 3.09 (1.53 – 6.23) 1.98 (0.46 – 8.52)
Secondary 1.99 (1.02 – 3.85) 2.67 (0.59 – 12.19)
Employment (employed)* 0.79 (0.47 – 1.33) 1.45 (0.46 – 4.54)
Smokes cigarette (yes)* 2.05 (0.18 – 22.94) 0.76 (0.00 – 529.98)
Takes alcohol (yes)* 1.83 (0.52 – 6.42) 1.86 (0.21 – 16.61)
Ate junk food (yes)* 0.50 (0.05 – 5.64) 1.43 (0.00 – 2355.87)
BMI (obesity)* 0.89 (0.53 – 1.50) 1.39 (0.46 – 4.16)
Used glasses (yes)* 0.56 (0.33 – 0.94) 0.43 (0.14 – 1.35)
Macula (abnormal)* 107.00 (43.64 – 262.33) 251.23 (67.49 – 935.20)
Hypertensive (yes)* 0.71 (0.42 – 1.18) 0.99 (0.35 – 2.79)
Diabetic (yes)* 1.36 (0.70 – 2.64) 1.31 (0.30 – 5.63)
Hyperlipidaemia (yes)* 0.33 (0.03 – 3.25) 0.43 (0.00 – 446.71)
*Reference categories: , R2 = 60.1% - 80.1%, **Logistic regression adjustment for all
the other variables in the model (shown on the table). †Statistically Significant.
Table 10 shows that the variables in the regression model explained between 60.1% and
80.1% of the variation observed in the outcome variable (Age-related macular disease).
Adjusting for the other co-variables in the regression model, a year increase in the age of the
respondents leads to 1.13 increase in the odds of developing ARMD. Male respondents were
3.07 (95% CI: 0.92 – 10.23) times more likely to develop ARMD compared to females.
Respondents who resided in urban areas were 3.08 (95% CI: 0.13 – 73.14) times more likely
to develop ARMD compared to those who resided in rural areas. Respondents who had no
formal education, primary education and secondary education were 0.67, 1.98 and 2.67 times
more likely to develop ARMD compared to those with tertiary education. The respondents
who were employed were 1.45 (95% CI: 0.46 – 4.54) times more likely to develop ARMD

44
compared to those who were unemployed. The respondents who smoked cigarettes were 0.76
(95% CI: 0.46 – 4.54) times more likely to develop ARMD compared to those who did not
smoke cigarettes. The respondents who took alcohol were 1.86 (95% CI: 0.21 – 16.61) times
more likely to develop ARMD compared to those who did not take alcohol. The respondents
who ate fast food were 1.43 (95% CI: 0.00 – 2355.87) times more likely to develop ARMD
compared to those who did not eat fast foods. The respondents who were obese were 1.39
(95% CI: 0.46 – 4.16) times more likely to develop ARMD compared to those who were not
obese. The respondents whose glasses were not tinted were 0.43 (95% CI: 0.14 – 1.35) times
more likely to develop ARMD compared to those who used tinted glasses. The respondents
who were hypertensives were 0.99 (95% CI: 0.35 – 2.79) times more likely to develop
ARMD compared to those who were not hypertensives. The respondents who were diabetic
were 1.31 (95% CI: 0.30 – 5.63) times more likely to develop ARMD compared to those who
were not diabetic. The respondents who had hyperlipidaemia were 0.43 (95% CI: 0.00 –
446.71) times more likely to develop ARMD compared to those who did not have
hyperlipidaemia. Only the age of the respondents showed statistically significant association
with ARMD.

45
CHAPTER 6
DISCUSSION
In this descriptive cross-sectional analytical study, an attempt was made at ascertaining the
pattern and clinical features, as well as identifying the modifiable risk factors for Age-related
Macular Degeneration (AMD) among patients, aged 50 years and above, in UBTH, Benin
City. In this study, the predominant presenting unaided visual acuity of patients with ARMD
ranged from 6/18 to counting fingers (CF) at 2.5m. There was bilateral occurrence of ARMD
in approximately 90% of cases. This was similar to findings by Nwosu42 where 86.3% of the
cases of ARMD seen had bilateral involvement of the eyes. About 10% of those with ARMD
had significant unilateral involvement. The possibility of the disease occurring bilaterally but
in an asymmetrical pattern could be alluded to this finding. The common posterior segment
findings seen in this study among cases with ARMD were hyperpigmented retinal pigment
epithelial abnormality (94.2%) and drusen (≈ 13%), of which over 90% were hard drusen.
The predominant pattern of Age-related Macular Degeneration seen was early, characterised
by the presence of drusen and retinal pigment epithelium (RPE) abnormalities. This was
similar to findings by Oluleye et al,41 Leske et al136 and Evans.137 There were only two cases
of late ARMD seen during the study period, and features were suggestive of neovascular
ARMD. There was no case of geographic atrophy seen. The reduced proportion of
individuals with late ARMD as shown by this study agrees with other studies performed
showing that more cases of late ARMD are seen in the Western world.12,32-34
A higher proportion of respondents were aged 60 – 69 years. This is in agreement with the
fact that Age-related Macular Degeneration (ARMD) becomes more clinically apparent as
age increases, especially after the age of 50 years.47-49 This finding was similar to data from
the United Kingdom where it was shown that individuals aged 65 – 75 years had Age-related

46
Macular Degeneration.12,19,26 Similar findings were shown by Nwosu42 and Omoti46 in
Nigeria.
In this study, the greater proportion of individuals with ARMD were females (60.0%). Such
was the case in the Nigerian hospital studies by Onakpoya et al,40 Nwosu et al42 and Omoti46
where there was a female preponderance of cases with ARMD. This was the case in the Blue
Mountains Eye Study127 which is a population-based study, conducted in Sydney, Australia,
where the higher prevalence of ARMD was seen in females compared to males. Increased
longevity in females has been attributed to this finding.69 Of note however is the fact that this
study was a hospital-based study as compared to the Blue Mountains Eye Study which was a
population-based study.
Significantly less cases with ARMD had tertiary level of education, showing a reduction in
the risk of having ARMD with increasing level of education. This result is in keeping with
earlier studies done which showed that the risk of having ARMD reduces with increasing
level of education, though this has not been sufficiently proven.128,129 The role of education in
influencing the social living standards of individuals, by creating better awareness on healthy
lifestyle behaviours could attribute to this.
As much as 97.5% of persons with ARMD lived in urban areas. This was comparable to the
percentage of controls (93.3%). Other factors rather than environmental could attribute to a
proportion of the study population coming down with ARMD and another proportion not
having ARMD, despite residing within the same geographical location. In Nigeria, there are
five social class systems: upper-upper class (the president and the presidency, top
government officials, wealthy royal families, elders in council), lower-upper class (military
officers, top entrepreneurs, top politicians, top professors), upper-middle class (professors,
lecturers, public servants, teachers), lower-middle class (owners of small businesses,

47
policemen) and the working class (petty traders, brick layers, temporary job workers).138 The
greater percentage of the population were in social class five (53.3% cases, 46.7% controls).
This difference was not statistically significant. This buttresses the unlikelihood of social
class, impacting on the incidence of AMD.128,129
About one fifth (20%) of those with ARMD were diabetics, with a mean duration of 7.8 ±
6.5 years. The difference in proportions in both study groups was not statistically significant
(P=0.400). This was similar to the Blue Mountains Eye Study127 where no association was
found between diabetes mellitus and early ARMD. However, the same study found a
significant relationship with geographic atrophy.
The difference in proportions between both study groups who were hypertensives was not
statistically significant. This is in agreement with other population-based cross-sectional
studies where no association was found between hypertension and ARMD.111-113 This yet
buttresses the fact that other factors, probably genetic, are responsible for a hypertensive
coming down with ARMD and not necessarily the hypertension itself.
Of the study population, four persons (1 case, 3 controls) had hyperlipidaemia and were on
lipid-lowering medication. This did not reflect an association between the use of lipid-
lowering medication and development of ARMD as shown by the Beaver Dam and Blue
Mountains Eye studies which showed a relationship between them.115
Only two (1.7%) individuals diagnosed with ARMD during the study period alluded to
smoking cigarettes compared to one control. The difference was not statistically significant.
This reduced number could be due to the fact that the study population do not smoke as much
cigarettes when compared to those in the Western world. An average of one packet of
cigarettes was smoked per day, for up to 25 years (25 pack years). This finding was in
agreement with studies conducted by Klein et al62 and Evans63 which showed individuals who
48
had smoked 11 pack years or more coming down with early ARMD, reflecting a dose-
response relationship of cigarette smoking and development of ARMD. In contrast to this,
West et al64 and Blumenkranz et al65 had findings which did not reflect this relationship.
Though studies show an increased risk of neovascular ARMD in individuals who had smoked
10 or more pack years, this study revealed otherwise, as none of those identified with
neovascular ARMD were smokers.58,59 However, since only two subjects in this study had
neovascular ARMD, the number is too small to draw valuable conclusions. The possibility of
genetics playing a more significant role in the development of late ARMD could be
entertained. In addition, increasing western exposure and lifestyle could increase the risk of
an individual coming down with ARMD.
Alcohol consumption, beer especially, in this study did not contribute significantly to the
development of ARMD. This was similar to a study by Knudtson et al77 where the amount of
beer, wine or liquor ingested did not affect the incidence or progression of ARMD. Similar
findings were seen in the Rotterdam study.78 The Blue Mountains Eye Study79 associated
early ARMD with ingestion of spirits, not beer consumption. The major form of alcohol
ingested by participants in this study was beer.
Diet and nutrition was shown to significantly influence the development of ARMD in this
study. Frequent consumption of fruits (predominantly watermelon, oranges) was significantly
more common among controls than participants with ARMD (P<0.005). This indicates a
measure of protection from ARMD by these fruits. Although 44.2% of cases with ARMD
attested to frequent weekly consumption of vegetables, there was no statistically significant
difference between both study groups regarding intake of vegetables. This finding contrasts
that by Amirul et al90 where frequent intake of varied types of vegetables was associated with
a lower prevalence of advanced ARMD. The reason for this disparity could possibly be due
to the differences in the state of the vegetables at the point of consumption seen in the

49
Western continent and that seen here in Sub-saharan Africa. In the Western world, vegetables
are mostly eaten raw, while here in Sub-Saharan Africa, the vegetables tend to be overcooked
before they are consumed. The nutrients remain intact at the point of consumption when
eaten raw, while they are destroyed when overcooked, losing the protection possibly offered
by these vegetables. Another plausible reason could be the difference in the population
studied, as the participants in this study majorly had features of early ARMD against
advanced ARMD as was seen in the study by Amirul et al.90 Weekly consumption of junk
food was not common among the study population. This was probably due to the prevailing
economic situation of most families, making it difficult for individuals to indulge in fast food
consumption. Of the few who took fast foods weekly (1 case, 2 controls), no statistically
significant difference in proportions was noticed. Despite this finding, Amirul et al90
associated the risk of having ARMD with consumption of high fat diet. Compared to red
meat and white meat, it was found that the greater proportion of the study population (98.3%
cases and 95% controls) consumed fish (majorly crayfish, Titus). The majority of the
respondents in both study groups obtained proteins predominantly through eating fish. This
could be attributed to the low purchasing power of the participants and the relatively low cost
of procurement of fish in the Nigerian markets and yet benefitting from the high nutritional
value. Though higher intake of fish rich in omega-3 fatty acids (salmon, tuna, mackerel) has
been associated with a lower risk of development of ARMD as shown by Tan et al86 and
Swenor et al,89 this study did not show any statistically significant difference between the two
study populations regarding intake of fish. It was observed in this study that despite the high
proportion of fish consumption among the cases (98.3%), the risk of ARMD was still high.
Studies carried out have shown inconsistent associations between intake of fish and the risk
of developing ARMD.84-86

50
Majority of those who used glasses were the control group. The difference in proportion was
statistically significant. Of these, 6.8% of them had their glasses tinted or wore photochromic
lenses. It has been hypothesized that exposure to sunlight is a plausible risk factor for
ARMD.123-125 The possibility of the tint offering some form of protection from bright sunlight
could be attributed to the controls not coming down with ARMD earlier. In this study,
myopia was found to be significantly more common among cases with ARMD than in the
controls. This is in contrast to findings from North India, Australia and a case-control study
done in Baltimore, United States of America where statistically significant associations were
demonstrated between ARMD and hypermetropia.97,100-102 This finding needs to be evaluated
further before valuable conclusions can be drawn, since the number of cases and controls
with myopia were small.
In this study, it was found that there was a statistically significant difference in the weight
and height of the controls compared to the cases with ARMD (P < 0.05). The cases in this
study were more overweight. This shows that weight, the modifiable aspect of BMI, is an
important predictor in an individual coming down with ARMD, though it was not singularly
assessed as a risk factor for ARMD in other studies reviewed. Documented findings in
literature show an increased risk of Age-related Macular Degeneration with increasing body
mass index (BMI).94-96 This study however did not show any statistically significant
relationship between BMI and the risk of having ARMD. It has been postulated that BMI
does not take into account the body composition of an individual (lean muscle mass and fat
mass). Hence, an individual can be said to have a high BMI and be tagged as being
overweight or obese, whereas the body fat constituent is low.139 This drawback could
possibly explain the finding in this study.
A greater proportion of the cases with ARMD had lens opacities compared to the controls
and this was statistically significant (p<0.001). This agrees with the study by Fletcher132
51
where a link was shown in the pathogenesis of ARMD and cataract, both resulting from
accumulation of reactive oxygen species from the mitochondria and from sunlight exposure.
Though studies reviewed did not single out a relationship between Amsler grid findings and
the pattern of ARMD seen, this study showed that Amsler grid was normal in the majority of
cases with ARMD (>75%) and this was statistically significant (p<0.001). This could be due
to the fact that the majority of cases had features suggestive of early ARMD, in which case
image distortions noticeable on Amsler grid would not have become prominent enough to be
noticed on examination.
The increase in age of the respondents by a year gave rise to a 1.13 increase in the odds of
developing AMD. This correlates with the already established fact that age is the strongest
risk factor for AMD 47-49 and is comparable with other research findings from studies done in
Western nations12,19,26,50 and Nigeria.42,46 This strongly corroborates the widely accepted
notion that the focal accumulation of extracellular deposits beneath the RPE gives rise to the
formation of age-dependent macular drusen, which precedes the age-dependent formation of
macular degeneration.140

52
STUDY LIMITATIONS
Recall bias among respondents to definitely quantify intake of alcohol, fruits and
vegetables in Section B of the protocol.
Non – availability of facilities to objectively quantify food intake by respondents.
Being a hospital-based study, the sample may not be truly representative of the
population.
CONCLUSION
This study showed that the risk of Age-related Macular Degeneration increases with age, with
a greater preponderance among females (60%). The presenting pattern of ARMD is
predominantly the early type. The clinical features are largely characterised by reduction in
visual acuity and especially for the late type where it is more marked, with the presence of
retinal hyperpigmentation and hard drusen.
There was bilateral occurrence of ARMD in approximately 90% of cases. Myopia was found
to be significantly more common among cases with ARMD than in the controls The risk of
having ARMD was shown to be reduced with increasing level of education and social class
was not a significant risk factor for ARMD. The use of tinted or photochromic lenses was
shown to offer some form of protection from direct sunlight, reducing the risk of ARMD. The
presence of lens opacities was associated with an increased risk of having ARMD and Amsler
grid was normal in patients with early ARMD.

53
RECOMMENDATIONS
Health education to elderly patients on the importance of frequent consumption of
fruits which is likely to reduce the burden of this disease or retard its progression.
Health education on measures to avoid overweight such as exercise and dietary
control, which would help reduce the risk of developing ARMD.
Government to promulgate policies to improve the level of education of the
population, as it has been shown that increasing level of education reduces the risk of
having ARMD.
Routine examination of individuals aged 50 years and above to recognise features of
early ARMD.
Lenses of individuals should preferably be tinted/photochromic as this has been
shown to offer some form of protection or retard the onset of ARMD.
More multi-centre hospital-based and population-based studies to be conducted to
characterise the pattern and risk factors of ARMD in Sub-Saharan Africa, as the
disease is increasingly becoming a major cause of blindness.

54
REFERENCES
1. Christenbury JG, Folgar FA, O’Connell RV, Chiu SJ, Farsiu S, Toth CA. Progression
of intermediate age-related macular degeneration with proliferation and inner retinal
migration of hyper reflective foci. Ophthalmology 2013;120: 1038-1045.
2. WHO/ Priority eye diseases. www.who.int/blindness/causes/priority/en/. Assessed
Feb 13, 2015.
3. Agarwal S, Agarwal A, Apple DJ. Textbook of Ophthalmology. Jaypee Brothers
Publishers, New Delhi. 2002; 2466-2474.
4. Friedman DS, O’Colmain BJ, Munoz B, Tomany SC, McCarty C, De Jong PT, et al.
Prevalence of age-related macular degeneration in the United States. Arch
Ophthalmol 2004;122: 564-572.
5. Munier A, Gunning T, Kenny D, O’keefe M. Causes of blindness in the adult
population of the Republic of Ireland. Br J Ophthalmol 1998;82: 630 -633.
6. Leat SJ and Rumney NJ. The experience of a university-based low vision clinic.
Ophthalmic Physiol Opt 1990; 10:8-15.
7. Cooper RL. Blind registrations in Western Australia: a five year study. Aust NZJ
Ophthalmol 1990;18: 421-426.
8. Chan CW and Billson FA. Visual disability and major causes of blindness in NSW: a
study of people aged 50 and over attending the Royal blind Society 1984 to 1989.
Aust NZJ Ophthalmol 1991; 19: 321-325.
9. Oluleye TS. Age-related macular degeneration: Current concepts in pathogenesis and
management. Nig J Ophthalmol 2007; 15: 5 – 11.
10. Klein R, Klein BE, Knudtson MD, Meuer SM, Swift M, Gangnon RE. Fifteen year
cumulative incidence of age-related macular degeneration: the Beaver Dam Eye
Study. Ophthalmology 2007; 114: 253 – 262.
11. Tomany SC, Wang JJ, van Leeuwen R, Klein R, Mitchell P, Vingerling JR et al. Risk
factors for incident age-related macular degeneration: pooled findings from 3
continents. Ophthalmology 2004; 111: 1280-1287.
12. Wang JJ, Rochtchina E, Lee AJ, Chia EM, Smith W, Cumming RG et al. Ten- year
incidence and progression of age-related maculopathy: the Blue Mountains Eye
Study. Ophthalmology 2007; 114: 92-98.

55
13. Klein ML, Ferris FL 3rd, Armstrong J, Hwang TS, Chew EY, Bressler SB et al.
Retinal precursors and the development of geographic atrophy in age-related macular
degeneration. Ophthalmology 2008; 115: 1026 – 1031.
14. World Health Statistics 2014.www.who.int/mediacentre/news/releases/2014/world-
health-statistics-2014/en. Assessed Mar 24, 2015.
15. Nwosu SN. Prevalence and pattern of retinal diseases at the Guinness Eye Hospital,
Onitsha, Nigeria. Ophthalmic Epidemiol 2000; 7: 41–48.
16. Amoni SS. Pattern of macular diseases in Nigerians: a preliminary report. Ann
Ophthalmol 1983; 15: 384–388.
17. Fafowora OF, Osuntokun BO. Age related eye diseases in the elderly of rural African
community. East Afr Med J 1997; 74: 435–437.
18. Uhumwangho OM, Itina EI. Retinal diseases in a tertiary hospital in Southern
Nigeria. J West AfrCollSurg. 2015; 5: 1-16.
19. Bird AC, Bressler NM, Bressler SB, Chisholm IH, Coscas G, Davis MD et al. An
international and grading system for age-related maculopathy and age related macular
degeneration. The International ARM Epidemiological Study Group. SurvOphthalmol
1995; 39: 367-374.
20. Klein R, Davis MD, Magli YL, Segal P, Klein BE, Hubbard L: The Wisconsin age-
related maculopathy grading system. Ophthalmology 1991, 98: 1128-1134.
21. Jager RD, Mieler WF, Miller JW: Age-related macular degen. N Engl J Med 2008;
358: 2606-2617.
22. World Health Organisation. Global data on visual impairment 2010. Available at:
http://www.who.int/blindness/GLOBALDATAFINALforweb.pdf. Accessed February
17, 2015.
23. Wong TY, Chakravarthy U, Klein R, Mitchell P, Zlateva G, Buggage R, et al. The
natural history and prognosis of neovascular age-related macular degeneration: A
systematic review of the literature and meta-analysis. Ophthalmology 2008; 115: 116-
126.
24. Day S, Acquah K, Lee PP, Mruthyunjaya P, Sloan FA. Medicare costs for
neovascular age-related macular degeneration, 1994 – 2007. Am J Ophthalmol 2011;
152: 1014-1020.
25. Taylor HR, Keeffe JE, Vu HTV, Wang JJ, Rochtchina E, Mitchell P, et al. Vision loss
in Australia. Med J Aust 2005; 182: 565-568.

56
26. Bunce C, Wormald R. Causes of blind certifications in England and Wales: April
1999-March 2000. Eye (Lond). 2008; 22: 905-911.
27. Evans JR. Causes of blindness and partial sight in England and Wales 1990 – 1991.
Studies on Medical and population subjects, HSMO, London.1995; 57: 9-11.
28. Eye Diseases Prevalence Research Group. Prevalence of age-related macular
degeneration in the United States. Arch Ophthalmol 2004; 102: 564-572.
29. Eye Diseases Prevalence Research Group. Causes and prevalence of visual
impairment among adults in the United States. Arch Ophthalmol 2004; 122: 477-485.
30. Kawasaki R, Yasuda M, Song SJ, Chen SJ, Jonas JB, Wang JJ et al. The prevalence
of age-related macular degeneration in Asians: a systematic review and meta-analysis.
Ophthalmology 2010; 117: 921-927.
31. Oshima Y, Ishibashi T, Murata T, Tahara Y, Kiyohara Y, Kubota T. Prevalence of
age related maculopathy in a representative Japanese population: the Hisayama study.
Br J Ophthalmol 2001; 85: 1153-1157.
32. Kawasaki R, Wang JJ, Aung T, Tan DT, Mitchell P, Sander M et al; Singapore Malay
Eye Study Group. Prevalence of age-related macular degeneration in a Malay
population: the Singapore Malay Eye Study. Ophthalmology 2008; 115:1735-1741.
33. Krishnan T, Ravindran RD, Murthy GV, Vashist P, Fitzpatrick KE, Thulasiraj RD et
al. Prevalence of early and late age-related macular degeneration in India: the
INDEYE study. Invest Ophthalmol Vis Sci 2010; 51: 701-707.
34. Li Y, Xu L, Jonas JB, Yang H, Ma Y, Li J. Prevalence of age-related maculopathy in
the adult population in China: the Beijing Eye Study. Am J Ophthalmol 2006; 142:
788-793.
35. Cheung CM, Tai ES, Kawaski R, Tay WT, Lee JL, Hamzah H, et al. Prevalence of
and risk factors for age-related macular degeneration in a multi-ethnic Asian cohort.
Arch Ophthalmol 2012; 130: 480 – 486.
36. Mathenge W, Bastawrous A, Peto T, Leung I, Foster A, Kuper H. Prevalence of Age-
Related Macular Degeneration in Nakuru, Kenya: A Cross-Sectional Population-
Based Study. PLoS Med 10: e1001393. doi:10.1371/journal.pmed.1001393.
37. Abdulraheem IS, Adepoju FG, Salaudeen AG, Akanbi AA. Pattern of eye problems of
the elderly in a Nigerian tertiary health institution. Nig Medic Pract. 2007; 51: 29-32.
38. Abiose A. Retinal diseases in Nigerians – A preliminary report. Niger Med J. 1976;
6:180 – 183.

57
39. Fafowora OF, Osuntokun BO. Age related eye diseases in the elderly members of a
rural African community. East Afr Med J. 1997; 74: 435-437.
40. Onakpoya OH, Olateju SO, Ajayi IA. Retinal diseases in a tertiary hospital: the need
for establishment of a vitreo-retinal care unit. J Natl Med Assoc. 2008; 100: 1286-
1289.
41. Oluleye TS, Ajaiyeoba AI. Retinal diseases in Ibadan. Eye. 2006; 20: 1461-1463.
42. Nwosu S. Age-related macular degeneration in Onitsha, Nigeria. Niger J ClinPract
2011; 14: 327-331.
43. Eze BI, Uche JN, Shiweobi JO. The burden and spectrum of vitreo-retinal diseases
among ophthalmic outpatients in a resource-deficient tertiary eye care setting in South
Eastern Nigeria. Middle East Afr J Ophthalmol 2010; 17: 246-249.
44. Kyari F, Gudlvalletti MV, Sivsubramaniam S, Gilgert CE, Abdul MM, Entekume G
et al. Nigerian National Blindness and Visual Impairment Study Group. Prevalence of
blindness and visual impairment in Nigeria: the National Blindness and Visual
Impairment Study. Invest Ophthalmol Vis Sci 2009; 50: 2033-2039.
45. Ayanru JO. Blindness in Mid-western state of Nigeria. Trop Geogr Med 1974; 26:
325-332.
46. Omoti AE. Age-related macular degeneration in Benin City Nigeria. JMBR 2004; 3:
7-11.
47. Klein R, Klein BE, Cruickshanks KJ. The prevalence of age-related maculopathy by
geographic region and ethnicity. ProgRetin Eye Res 1999; 18: 371-389.
48. Klaver CC, Assink JJ, van Leeuwen R, Wolfs RC, Vingerling JC, Stijnen T, et al.
Incidence and progression rates of age-related maculopathy: the Rotterdam Study.
Invest Ophthalmol Vis Sci 2001; 42: 2237-2241.
49. Wong TY, Loon SC, Saw SM. The epidemiology of age related eye diseases in Asia.
Br J Ophthalmol 2006; 90: 506-511.
50. Smith W, Assink J, Klein R, Mitchell P, Klaver CC, Klein BE et al. Risk factors for
age related macular degeneration: pooled findings from three continents.
Ophthalmology 2001; 108: 697-704.
51. Thornton J, Edwards R, Mitchell P, Harrison RA, Buchan I, Kelly SP. Smoking and
age-related macular degeneration: a review of association. Eye (Lond). 2005: 935-
944.

58
52. Mitchell P, Wang JJ, Smith W, Leeder SR. Smoking and the 5-year incidence of age-
related maculopathy: the Blue Mountains Eye Study. Arch Ophthalmol. 2002; 120:
1357-1363.
53. Tan JS, Mitchell P, Kifley A, Flood V, Smith W, Wang JJ. Smoking and the long-
term incidence of age-related macular degeneration: the Blue Mountains Eye Study.
Arch Ophthalmol 2007; 125:1089-1095.
54. Klein R, Knudtson MD, Cruikshanks KJ, Klein BE. Further observations on the
association between smoking and the long-term incidence and progression of age-
related macular degeneration: the Beaver Dam Eye Study. Arch Ophthalmol 2008;
126: 115-121.
55. Chakravarthy U, Augood C, Bentham GC, de Jong PT, Rahu M, Seland J, et al.
Cigarette smoking and age-related macular degeneration in the EUREYE Study.
Ophthalmology 2007; 114: 1157-1163.
56. Khan JC, Thurlby DA, Shahid H, Clayton DG, Yates JR, Bradley M, et al. Smoking
and age related macular degeneration: the number of pack years of cigarette smoking
is a major determinant of risk for both geographical atrophy and choroidal
neovascularization. Br J Ophthalmol. 2006; 90: 75-80.
57. SolbergY, Rosner M, Belkin M. The association between cigarette smoking and
ocular diseases. Survey of ophthalmology. 1998; 42: 535-547.
58. Vingerling JR, Hofman A, Grobbee DE, De JongPT. Age-related macular
degeneration and smoking: the Rotterdam study. Arch Ophthalmol 1996; 114: 1193 –
1196.
59. Delcourt C, Diaz JL, Ponton-Sanchez A, Papoz L. Smoking and age –related macular
degeneration: the POLA study. Arch Ophthalmol 1998; 116: 1031 – 1035.
60. Seddon JM, Willet WC, Speizer FE, Hankinson SE. A prospective study of cigarette
smoking and age-related macular degeneration in women. JAMA 1996; 276: 1141 –
1146.
61. Christen WG, Glynn RJ, Manson JE, Ajani UA, Buring JE. A prospective study of
cigarette smoking and risk of age-related macular degeneration in men. JAMA 1996;
276: 1147 – 1151.
62. Klein R, Cruickshanks KJ, Nash SD. The prevalence of age-related macular
degeneration and associated risk factors. Arch Ophthalmol 2010; 128: 750 – 758.

59
63. Evans JR. Risk factors for age-related macular degeneration. Progr. In Ret Eye Res
2001; 20: 227-253.
64. West SK, Rosenthal FS, Bressler NM, Bressler SB, Munoz B, Fine SL et al. Exposure
to sunlight and other risk factors for age-related macular degeneration. Arch
Ophthalmol 1989; 107: 875−879.
65. Blumenkranz MS, Russell SR, Robey MG, Kott-Blumenkranz R, Penneys N. Risk
factors in age-related maculopathy complicated by choroidal
neovascularization. Ophthalmology 1986; 93: 552−558.
66. Chaine G, Hullo A, Sahel J, Soubrane G, Espinasse-Berrod MA,
Schutz Detal.Case−control study of the risk factors for age related macular
degeneration. France-DMLA Study Group. Br J Ophthalmol 1998; 82: 996−1002.
67. Klein R, Klein BE, Linton KL, DeMets DL. The Beaver Dam Eye Study: the relation
of age-related maculopathy to smoking. Am J Epidemiol 1993;137: 190−200.
68. Klein R, Klein BE, Moss SE. Relation of smoking to the incidence of age-related
maculopathy. The Beaver Dam Eye Study. Am J Epidemiol 1998;147: 103−110.
69. Klein R, Klein BE, Tomany SC, Moss SE. Ten-year incidence of age-related
maculopathy and smoking and drinking: the Beaver Dam Eye Study. Am J
Epidemiol 2002; 156: 589−598.
70. Agar E, Demir S, Amanvermez R, Bosnak M, Ayyildiz M, Celik C. The effects of
ethanol consumption on the lipid peroxidation and glutathione levels in the right and
left brains of rats. Int J Neurosci 2003; 113: 1643-1652.
71. Cederbaum AI. Role of lipid peroxidation and oxidative stress in alcohol toxicity.
Free RadicBiol Med 1989; 7: 537-539.
72. Ritter LL, Klein R, Klein BE, Mares-Perlman JA, Jensen SC. Alcohol use and age-
related maculopathy in the Beaver Dam Eye Study. Am J Ophthalmol 1995; 120: 190-
196.
73. Fraser-Bell S, Wu J, Klein R, Azen SP, Varma R. Smoking, alcohol intake, estrogen
use, and age-related macular degeneration in Latinos: the Los Angeles Latino Eye
Study. Am J Ophthalmol 2006; 141: 79- 87.
74. Cho E, Hankinson SE, Willett WC, Stampfer MJ, Spiegelman D, Speizer FE, et al.
Prospective study of alcohol consumption and the risk of age-related macular
degeneration. Arch Ophthalmol 2000; 118: 681- 688.

60
75. Buch H, Vinding T, la Cour M, Jensen GB, Prause JU, Nielsen NV. Risk factors for
age-related maculopathy in a 14-year follow-up study: the Copenhagen City Eye
Study. ActaOphthalmolScand 2005; 83: 409- 418.
76. Klein R, Klein BE, Tomany SC, Moss SE. Ten-year incidence of age-related
maculopathy and smoking and drinking: the Beaver Dam Eye Study. Am J Epidemiol
2002; 156: 589- 598.
77. KnudtsonMD, Klein R, Klein BE. “Alcohol Consumption and the 15-Year
Cumulative Incidence of Age-Related Macular Degeneration (AMD).” AmJ
Ophthalmol 2007; 143.6: 1026–1029.
78. Boekhoorn SS, Vingerling JR, Hofman A, De Jong PM. Alcohol Consumption and
Risk of Aging Macula Disorder in a General Population: The Rotterdam Study. Arch
Ophthalmol. 2008; 126: 834-839.
79. Smith W, Mitchell P. Alcohol intake and age-related maculopathy. Am J Ophthalmol
1996; 122: 743-745.
80. Seddon JM, George S, Rosner B. Cigarette smoking, fish consumption, omega-3 fatty
acid intake, and associations with age-related macular degeneration: the US Twin
Study of Age-Related Macular Degeneration. Arch Ophthalmol 2006; 124: 995-1001.
81. Chong EW, Simpson JA, Robman LD, Hodge AM, Aung KZ, English DR, et al. Red
meat and chicken consumption and its association with age-related macular
degeneration. Am J Epidemiol 2009; 169: 867-876.
82. Chong EW, Robman LD, Simpson JA, Hodge AM, Aung KZ, Dolphin TK, et al. Fat
consumption and its association with age-related macular degeneration. Arch
Ophthalmol 2009; 127: 674-680.
83. Seddon JM, Rosner B, Sperduto RD, Yannuzzi L, Haller JA, Blair NP, et al. Dietary
fat and risk for advanced age-related macular degeneration. Arch Ophthalmol 2001;
119: 1191-1199.
84. Smith W, Mitchell P, Leeder SR. Dietary fat and fish intake and age-related
maculopathy. Arch Ophthalmol 2000; 118: 401-404.
85. Mares JA, Voland RP, Sondel SA, Millen AE, Larowe T, Moeller SM, et al. Healthy
lifestyles related to subsequent prevalence of age-related macular degeneration. Arch
Ophthalmol 2011; 129: 470-480.
86. Tan JS, Wang JJ, Flood V, Mitchell P. Dietary fatty acids and the 10-year incidence
of age-related macular degeneration: the Blue Mountains Eye Study. Arch
Ophthalmol 2009; 127: 656-665.

61
87. Chong EW, Kreis AJ, Wong TY, Simpson TA, Guymer RH. Alcohol consumption
and the risk of age-related macular degeneration: a systematic review and meta-
analysis. Am J Ophthalmol 2008; 145: 707-715.
88. Adams MK, Chong EW, Williamson E, Aung KZ, Makeyeva GA, Giles GG, et al.
20/20-Alcohol and Age-related Macular Degeneration: The Melbourne Collaborative
Cohort Study. Am J Epidemiol 2012; 176: 289-298.
89. Swenor BK, Bressler S, Caulfield L, West SK. The impact of fish and shellfish
consumption on age-related macular degeneration. Ophthalmology 2010; 117: 2395-
2401.
90. Amirul IFM, Chong EW, Hodge AM, Guymer RH, Aung KZ, Makayeva GA, et al.
Dietary patterns and their associations with age-related macular degeneration: The
Melbourne Collaborative Cohort Study. Am J Ophthalmol 2014; 121: 1428-1434.
91. Seddon JM, Cote J, Davis N, Rosner B. Progression of age-related macular
degeneration: association with body mass index, waist circumference and waist – hip
ratio. Arch Ophthalmol 2003; 121: 785 – 792.
92. Schaumberg DA, Christen WG, Hankinson SE, Glynn RJ. Body mass index and the
incidence of visually significant ARMD in men. Arch Ophthalmol 2001; 119: 1259 –
1265.
93. Knudtson MD, Klein P, Klein BE. Physical activity and the 15-year cumulative
incidence of age-related macular degeneration: the Beaver Dam Eye Study. Br J
Ophthalmol 2006; 90: 1461 – 1463.
94. Risk factors for neovascular age-related macular degeneration. The Eye Disease Case-
Control Study Group. Arch Ophthalmol 1992; 110: 1701-1708.
95. Delcourt C, Michel F, Colvez A, Lacroux A, Delage M, Vernet MH. Associations of
cardiovascular disease and its risk factors with age-related macular degeneration: the
POLA study. Ophthalmic Epidemiol. 2001; 8: 237-249.
96. Seddon JM, Cote J, Davis N, Rosner B. Progression of age-related macular
degeneration: association with body mass index, waist circumference and waist-hip
ratio. Arch Ophthalmol 2003; 121: 785-792.
97. Hyman LG, Lilienfield AM, Ferris FL, Fine SL. Senile macular degeneration: a case-
control study. Am JEpidemiol. 1983; 118: 213-227.
98. Sandberg MA, Tolentino MJ, Miller S, Berson EL, Gaudio AR. Hyperopia and
neovascularization in age-related macular degeneration.Ophthalmology. 1993; 100:
1009-1013.

62
99. Goldberg J, Flowerdew G, Smith E, Brody JA, Tso MO. Factors associated with age-
related macular degeneration. An analysis of data from the first National Health and
Nutrition Examination Survey. Am J Epidemiol 1988; 128: 700-710.
100. Wang JJ, Mitchell P, Smith W. Refractive error and age-related maculopathy: the
Blue Mountains Eye Study. Invest Ophthalmol Vis Sc. 1998; 39:2167-2171.
101. Ikram MK, van Leeuwen R, Vingerling JR, Hofman A, De Jong PT. Relationship
between refraction and prevalent as well as incident age-related maculopathy: the
Rotterdam Study. Invest Ophthalmol Vis Sci. 2003; 44: 3778-3782.
102. Narendran V, Tulsiram RD, Kim R, Selvaray, Katz J, Robin AR. The prevalence of
ARMD in South-India. Invest Ophthalmol Vis Sci 2000; 41: s119.
103. The Eye Disease Case-Control Study Group. Risk factors for neovascular age-related
macular degeneration. The Eye Disease Case-Control Study Group. Arch.
Ophthalmol. 1992; 110: 1701 – 1708.
104. Weiter JJ, Delori FC, Wing GL, Fitch KA. Relationship of senile macular
degeneration to ocular pigmentation. Am J Ophthalmol. 1985; 99: 185–187.
105. Tomany SC, Klein R, Klein BE, Beaver Dam Eye S. The relationship between iris
color, hair color, and skin sun sensitivity and the 10-year incidence of age-related
maculopathy: the Beaver Dam Eye Study. Ophthalmology. 2003; 110: 1526-1533.
106. Mares-Perlman JA, Millen AE, Ficek TL, Hankinson SE. The body of evidence to
support a protective role for lutein and zeaxanthin in delaying chronic disease.
Overview. J Nutr. 2002; 132: 518S-524S.
107. Age-Related Eye Disease Study Research G, SanGiovanni JP, Chew EY, Clemons
TE, Ferris FL 3rd , Gensler G, et al. The relationship of dietary carotenoid and vitamin
A, E, and C intake with age-related macular degeneration in a case-control study:
AREDS Report No. 22. Arch Ophthalmol. 2007; 125: 1225-1232.
108. Wong TY, Mitchell P. The eye in hypertension. Lancet. 2007; 369: 425-435.
109. Kahn HA, Leibowitz HM, Ganley JP, Kini MM, Colton T, Nickerson RS, et al. The
Framingham Eye Study II. Association of ophthalmic pathology with single variables
previously measured in the Framingham Heart Study. Am J Epidemiol 1977; 106: 33-
41.
110. Sperduto RD, Hiller R. Systemic hypertension and age related maculopathy in the
Framingham study. Arch Ophthalmol. 1986; 104: 216 –219.

63
111. Smith W, Mitchell P, Leeder SR, Wang JJ. Plasma fibrinogen levels, other
cardiovascular risk factors and age related maculopathy. The Blue Mountains Eye
Study. Arch Ophthalmol. 1998; 116: 583 – 587.
112. Klein R, Clegg L, Cooper LS, Hubbard LD, Klein BE, King WN et al. Prevalence of
age-related maculopathy in the Atherosclerosis Risk in Communities Study. Arch
Ophthalmol 1999; 117: 1203–1210.
113. Krishnaiah S, Das T, Nirmalan PK, Nutheti R, Shamanna BR, Rao GN, et al. Risk
factors for AMD; findings from the Andhra Pradesh eye disease study in South India.
Invest Ophthalmol. Vis Sci 2005; 46: 4442 – 4449.
114. Snow KK, Seddon JM. Do age-related macular degeneration and cardiovascular
disease share common antecedents? Ophthalmic Epidemiol. 1999; 6: 125-143.
115. Klein R, Klein BE, Jensen SC, Cruickshanks KJ, Lee KE, Danforth LG, et al.
Medication use and the 5-year incidence of early age-related maculopathy: the Beaver
Dam Eye Study. Arch Ophthalmol 2001; 119: 1354 – 1359.
116. Choi JK, Lym YL, Moon JW, Shin HJ, Cho B. Diabetes mellitus and early age-
related macular degeneration. Arch Ophthalmol 2011; 129: 196 – 199.
117. Li X, Wang YS. Effects of diabetes mellitus on the occurrence of age-related macular
degeneration. Zonghua Yan KeZaZhi 2011; 47: 273 – 275.
118. The Eye Disease Case-Control Study Group. Risk factors for neovascular age-related
macular degeneration. Arch Ophthalmol 1992; 110: 1701 – 1708.
119. Vingerling JR, Dielmans I, Bots ML, Hofman A, Grobbee DE, de Jong PT. Age-
related macular degeneration is associated with atherosclerosis. The Rotterdam Study.
Am J Epidemiol 1995; 142: 404 – 409.
120. Klein RJ, Zeiss C, Chew EY, Tsai JY, Sackler RS, Haynes C, et al. Complement
factor H polymorphism in age-related macular degeneration. Science. 2005; 308: 385-
389.
121. Edwards AO, Ritter R, Abel KJ, Manning A, Panhuysen C, Farrer LA. Complement
factor H polymorphism and age-related macular degeneration. Science. 2005; 308:
421-424.
122. Fletcher AE, Bentham GC, Agnew M, Young IS, Augood C, Chakravarthy U, et al.
Sunlight exposure, antioxidants and age-related macular degeneration. Arch
Ophthalmol 2008; 126: 1396-1403.

64
123. Khan JC, Shahid H, Thurlby DA, Bradley M, Clayton DG, Moore A, et al. Age-
related macular degeneration and sun exposure, iris colour and skin sensitivity to
sunlight. Br J Ophthalmol 2006; 90: 29-32.
124. Tomany SC, Cruickshanks KJ, Klein R, Klein BE, Knudtson MD. Sunlight and the
10-year incidence of age-related maculopathy: the Beaver Dam Eye Study. Arch
Ophthalmol 2004; 122: 750-757.
125. Feigl B. Age-related maculopathy – linking etiology and pathophysiological changes
to the ischemiahypothesis. ProgRetin Eye Res. 2009; 28: 63 – 86.
126. Klein EK, Klein R. Perspective: lifestyle exposures and eye diseases in adults. Am J
Ophthalmol. 2007; 144: 961–969.
127. Smith W, Mitchell P, Wang JJ. Gender, oestrogen, hormone replacement and age-
related macular degeneration. Aust N Z J Ophthalmol. 1997; 25: S13-S15.
128. Cruickshanks KJ, Hamman RF, Klein R, Nondahl DM, Shetterly SM. The prevalence
of age-related maculopathy by geographic region and ethnicity. The Colorado-
Wisconsin Study of Age-Related Maculopathy.Arch Ophthalmol. 1997; 115: 242-
250.
129. Varma R, Fraser-Bell S, Tan S, Klein R, Azen SP. Prevalence of age-related macular
degeneration in Latinos: the Los Angeles Latino eye study. Ophthalmology. 2004;
111: 1288-1297.
130. Friedman DS, Katz J, Bressler NM, Rahmani B, Tielsch JM. Racial differences in the
prevalence of age-related macular degeneration: The Baltimore Eye Survey.
Ophthalmology 1999; 106: 1049 – 1055.
131. Klein R, Klein BE, Knudtson MD, Wong TY, Cotch MF, Liu K, et al. Prevalence of
Age-related macular degeneration in 4 racial/ethnic groups in the Multiethnic study of
atherosclerosis. Ophthalmology 2006; 113: 373 – 380.
132. Fletcher AE. Free radicals, antioxidants and eye diseases: evidence from
epidemiological studies on cataract and age-related macular degeneration. Ophthalmic
Res. 2010; 44: 191-198.
133. Chakravarthy U, Wong TY, Fletcher A, Piault E, Evans C, Zlateva G, et al. Clinical
risk factors for age-related macular degeneration: a systematic review and meta-
analysis. BMC Ophthalmol. 2010; 10: 31.
134. Klein BE, Howard KP, Lee KE, Iyengar SK, Sivakumaran TA, Klein R. The
relationship of cataract and cataract extraction to age-related macular degeneration:
the Beaver Dam Eye Study. Ophthalmology. 2012; 119: 1628-1633.
65
135. Araoye MO. Research Methodology with Statistics for Health and Social Sciences.
Nathadex publishers, Ilorin. 1st ed. 2003: 119.
136. Leske MC, Wu S. Hennis A, Nemesure B, Yang L, Hyman L et al. Barbados Eye
Study Group. Nine year incidence of age related macular degeneration in the
Barbados eye studies. Ophthalmol 2006; 113: 29 – 35.
137. Evans JR. Risk factors for age-related macular degeneration. Prog in Ret Eye Res
2001; 20: 227 – 253.
138. Nigeria – Social structure – Country studies. http://www.countrystudies.us > Nigeria.
Assessed 25th May, 2017.
139. Padwal R, Leslie WD, Lix LM, Majumdar SR. Relationship among body fat
percentage, body mass index and all-cause mortality: a cohort study. Ann Intern Med.
2016; 164: 532-541.
140. Nishiguchi KM, Yokoyama Y, Fujii Y, Fujita K, Tomiyama Y, Kawasaki R, et al.
Analysis of Macular Drusen and Blood Test Results in 945 Macacafascicularis. PLoS
ONE 11: e0164899. doi: 10.1371/journal.pone.0164899.

66
APPENDIX I

67
APPENDIX II
68
APPENDIX III
CONSENT FORM
My name is EKECHUKWU, Loretta Omonzusi, a senior resident doctor in Ophthalmology at
the University of Benin Teaching Hospital, Benin City. I am conducting a study on Age-
related Macular Degeneration in Benin City. This study would involve asking you questions
about yourself, your medical history, past and current eye problems and examination of your
eyes.
During the examination, your vision will be tested and a bright light will be shone into your
eyes. It will not cause any harm. It may be necessary to apply some eye drops to your eyes in
order to allow us examine the back of your eyes. The eye drops may cause temporary
blurring of vision for about 4-6 hours, but it is reversible and not harmful.
This study will avail you the opportunity to have a comprehensive eye check at no cost as the
author has borne the cost of the tests. Data collected from this study will be of benefit in
planning appropriate eye care management for age-related macular degeneration towards
reducing the adverse impact of this clinical condition.
Your sincere response and cooperation is required and will be appreciated. Your response and
examination findings will be kept completely confidential.
If you voluntarily agree to take part in the study, please indicate by signing this form.
Thank you and God bless.
…………………………… …………………………
Signature of participant Date

69
APPENDIX IV
PROTOCOL FOR CLINICAL CHARACTERISTICS OF AGE-RELATED
MACULAR DEGENERATION IN UNIVERSITY OF BENIN TEACHING
HOSPITAL, BENIN CITY, EDO STATE.
Serial number: Hospital number:
A. BIODATA
i. Age …………………..
ii. Sex M { } F{ }
iii. Residence a. Urban { } b. Rural { }
iv. Occupation ……………………………
v. Level of education No formal{ } 10{ } 20{ } 30{ }
B. MEDICAL AND SOCIAL HISTORY
vi. Are you diabetic? Yes { } No { } If yes, for how long? ………………..
What drugs are you on? ………………………………….
vii. Are you hypertensive? Yes { } No { } If yes, for how long?......................
What drugs are you on? ……………………………………
viii. Are you on lipid lowering medication? Yes { } No { } If yes, for how long? ....................
What drug(s) are you on? ……………………………………
ix. Do you smoke cigarettes? Yes { } No{ }If yes, for how long? ………………..
Number of sticks per day …………………………
x. Do you take alcohol? Yes { } No { } If yes, for how long?…………………………. What
type?............................... Quantity per day ………………………
xi. Do you indulge in junk food? Yes { } No { } If yes, how often? ……..weekly
xii. Do you take fruits frequently? Yes { } No { } If yes, how often? …………… weekly.
Specify type………. Quantity…………………
xiii. Do you take vegetables regularly? Yes { } No { } If yes, how often? …………. weekly.
Specify type …….. Quantity …………….
xiv. Which do you take more often? Fish { }, Red meat { }, White meat { }.
C. OCULAR HISTORY
xv. Do you use glasses? Yes { } No { } If yes, for how long?………………
xvi. Type of error ………………
xvii. Are your glasses tinted or photochromic? Yes{ } No { }
xviii. Do you make use of sunshades? Yes { } No { }

70
EXAMINATION PROFORMA
Measurements
a. Weight: ………………..kg
b. Height: …………………m
c. Body mass index (BMI): …………………..
[BMI = Weight (kg) ÷ Height (m)2]
Ocular Examination
RE LE
1. Unaided VA ….…..……………. ……………………
2. Pin hole VA ……………………. ……………………
3. Best corrected VA ……………………. ………………..
4. Anterior segment: Normal { } Abnormal { } Normal { } Abnormal { }
5. Lens …………………………………… ……………………………
6. IOP (mmHg) ………………………. ……………………….
7. Amsler grid Normal { } Abnormal { } Normal { } Abnormal { }
8. Posterior segment
a. Vitreous Clear { } Hazy { } Clear{ } Hazy { }
b. Disc (VCDR) …………………. …………………….
c. Macula Normal { } Abnormal { } Normal { } Abnormal { }
d. Drusen
i. Present Yes { } No { } Yes { } No { }
ii. Type Soft { } Hard { } Soft { } Hard { }
e. RPE abnormalities
i. Present Yes { } No { } Yes { } No { }
ii. Pigmentation: Hyper- { } Hypo-{ }Hyper- { } Hypo- { }
f. Geographic atrophy Present { } Absent { } Present { } Absent { }
g. Exudative AMD Present { } Absent { } Present { } Absent { }
h.Retina diagram
Diagnosis
71
INVESTIGATION RESULTS
Fasting Blood Glucose: …………………………..
Fasting Serum Lipid Profile:
Total cholesterol …………………………
High Density Lipoprotein (HDL) …………………………..
Low Density Lipoprotein (LDL) ……………………………
Triglycerides (TG) …………………………….
Fundus Fluorescein Angiography Findings:

72
APPENDIX V
Map of Edo state showing the catchment areas of the University of Benin
Teaching Hospital

73
APPENDIX V
STANDARD PHOTOS: INTERNATIONAL ARM
EPIDEMIOLOGICAL STUDY GROUP
Standard grid for classification of ARMD
The circles should be reduced on a transparent sheet, according to the magnification of the
fundus camera used, so that they have approximate diameters of 1000, 3000 and 6000 µm
respectively in the fundus of an average eye. These circles represent respectively the central,
middleand outer sub field. The spokes may be of help in centring the grid on the macula.
Standard circles for grading ARMD-related fundus changes.
Approximate diameters in the average fundus of 63µm, 125µm, 175µm, 250µm and 500µm.

74
FUNDUS PHOTOGRAPH OF PARTICIPANT WITH EARLY ARMD

75
FUNDUS FLUORESCEIN ANGIOGRAM OF PARTICIPANT WITH EARLY ARMD
(RED FREE)
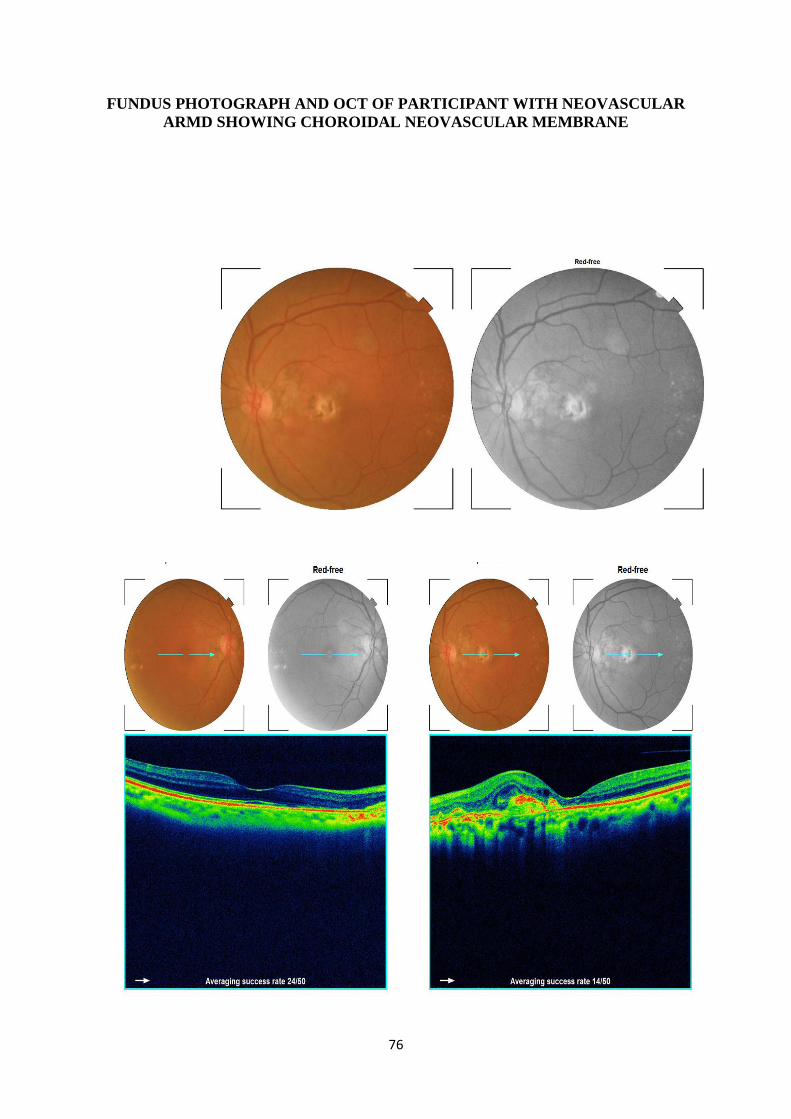
76
FUNDUS PHOTOGRAPH AND OCT OF PARTICIPANT WITH NEOVASCULAR
ARMD SHOWING CHOROIDAL NEOVASCULAR MEMBRANE

77
FUNDUS FLUORESCEIN ANGIOGRAM OF PARTICIPANT WITH
NEOVASCULAR ARMD SHOWING CHOROIDAL NEOVASCULAR MEMBRANE

78
PRINCIPAL RESEARCHER TAKING FUNDUS PHOTOGRAPHS

79
PRINCIPAL RESEARCHER TAKING FUNDUS PHOTOGRAPHS