clinical protocol, workflow primary and metastatic liver
TRANSCRIPT

Clinicalprotocol,Workflow
Primary and metastatic liver tumors SBRTAmsterdam2017

Nodisclosures

Learning objective
• Specifics ofliver SBRTcompared toother sites(lung)

Basic principle:
StartSBRTprogramwith lung
Copy asmuch aspossible from experience inlung SBRT!
àLiver SBRTis“identical”but morecomplex

LiverSBRT:
Bothprimarytumorsandmets
NW-Europe:livermets!
Inmanyothercountries:primarylivercancer

SBRTLIVER
•DOESITWORK??

Publishedresultsbothmets andprimarylever:• Widevarietyoftechniquesanddoseschedules,>10yearsexperience
Author Nooflesions Dose Localcontrol Remarks
Blomgren1995 42 4x7.7Gy– 1x30Gy@50%
80%
Wulf 2006 56 Various:4x7Gy-1x26Gy@80%
Actuarial:HCC:100%Mets:1yr:92%
2yr:66%2yrOS:32%
Localcontrolincreasedathigherdoses(trend)
Tse2008 31HCC10IHC
6x4-9Gyisoc 1yr:65%
Chiba2005 192HCC Various,median16x4.5Gy
5yr87% Protons/gating/chemo-embolisation
Kavanagh2006
36 Max3x20Gy 93% Doseescalation,MTDnotreached

8

Consider when starting SBRTliver program
• Getting patients
• Imaging (planningandtreatment)
• Motionmanagement(Tumorand OAR!)
• Followup
Radiationtherapyinlivertumors:
• Historicalproblem:RILDà Radiationinducedliverdisease
• Wholeliverradiation:RILDafter>30Gy• 30Gynotenoughforlocalcontrol(mosttumors>60Gy)
àRadiationoncologists:-nohistory/notmuchinterest-notinvolvedinspecificlivertumorboards/liverguidelines-specificknowledgerequired!
Getting patients referred

BarcelonaCriteria(HCC)

SBRT SBRT SBRT SBRT/Conventional XRT
BarcelonaCriteria(HCC)


Gettingpatientsreferred:Manycompetinglocaltreatmentoptions:
• Surgery• RFA• TACE/Radioembolisation• Electroporation (“IRE/Nanoknife”)
• Alltreatmentshavedifferent:– (contra)indications(anesthesia/bleedingdisordersetc)– localcontrol(tumorsize)– “difficult”locations

ProSBRT(attumorboardmeetings):• Highlocalcontrol(especiallylargertumorscomparedtocompetingtechniques)
• Overlapwithlargevessels/hilar structuresnoproblem• Outpatientprocedure• Nogeneralanesthesia• Completelynon-invasive(ifwithoutfiducials)• Bleedingdisorders:noproblem
Patientselection:
• “Oligometastases”oroligoprogression– Nopatientswithactivewidespreaddisease– Reasonablelifeexpectancy
• Nomaximumsizeornumber– dependingonsparednormalliver– mostcommon:one(ortwo)mets
• Somemarginneededbetweentumorandbowel/stomach/esophagusà SBRT-likedoseshouldbepossible
Diagnostics• Mostcasesheavilypretreated:tissueproofofM1diseaseavailableformostpatients
• 4-phase CTscan(contrastenhancementpattern)– DifferentcontrasttimingHCCvs mets
• PET-CTscan– Ruleoutwidespreaddistantmets– LesionFDGpos??(usefulnessofmakingplanningPETCT)
• OftenMRIisavailable– RoleofPET-MRIstillunclear

Step by step CASE(pre-MRIdian)
• Mr X• Age 66• Excellent performance score
• Dec 2010 sigmoid carcinoma: resection• Widespread synchronous liver metastases: chemotherapy (capecitabine +
oxaliplatin + bevacizumab)• July 2011: RFA liver metastases segment I, II, III, VI, 2 x VII and 2 x in VIII. • December 2011: 6 liver metastases: 4 x RFA (segment II, III, IVa, IV) and 2 x
microwave ablation (segment III, VIII). • April 2012: Multifocal recurrence ablation cavity segment 8. No extrahepatic
disease: • Microwafe +TACE. • October 2012: recurrence same location• SABR???

Livermetastases:referralpatterns• WhoarereferredforSBRT:
– Colorectal liver metastases– (very)poorperformancescore– Afterresection– AftermultipleRFA/TACE– Centrallocation- overlaplargevessels– Contra-indicationorrefusalinvasivetreatment– Inmostcasesalloftheabove
-NonColorectallivermetastasespatients-lessheavilypretreated-lessaggressivelocaltreatmentànon-invasive
treatmentmoreimportant!

Typicalreferralcasenon-colorectal
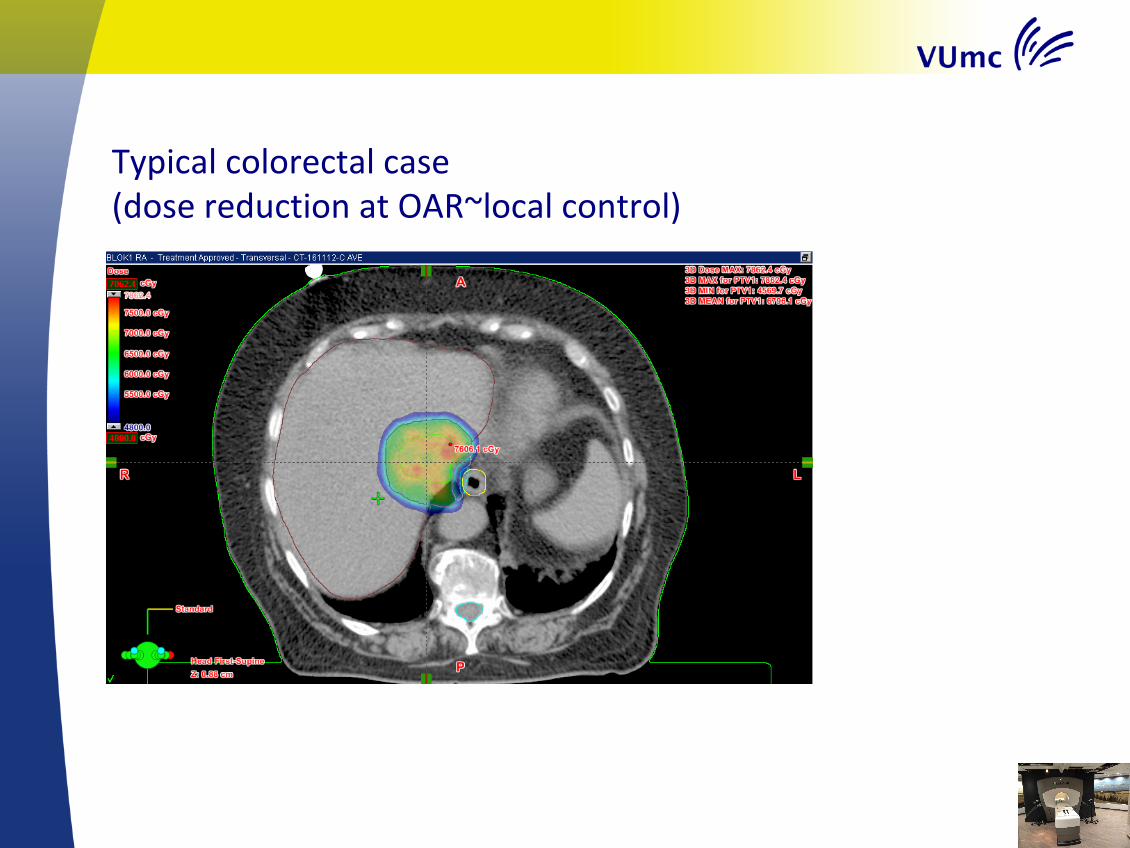
Typicalcolorectalcase(dosereductionatOAR~local control)

Step by step CASE
• July:Diagnostic4-phaseCTscan

Step by step CASE
• October: Diagnostic 4-phase CT scan

Step by step CASE
• Diagnostic PET/CT scan

Patientfixation/respiration
– Standard:identicaltolungSBRT– Armsup– Noextrafixation(nobodyframe,vacuummattressetc)– Freebreathing
– Consider(notusedinVumc):Abdominal compression device
– Reduces motion– Interfraction reproducibility poor– Not patient friendly
àConsider when no gating/breathhold available
ImagingforliverSABR• ‘Large’area4DCTscanwithoutivcontrast
– Dosecalculation
• ‘Smallarea’4DCTscanofliverareawithivcontrast– Contrasttimingeasierwithsmallscanarea

ImagingforSABR• Insomecases:double4DCTwithivcontrast(differentdays)• Duringplanning4DCTand4DPETCT
– Influenceofrespiratorybeltonanatomyandbreathingpattern– RPMsystemonlyavailableon4DCT– Difficultimagingandivcontrasttiming:doubleismore…

• Noroutinelyimplantedfiducials– Logistical
– Time– Somerad oncs implantmarkersthemselves…
– KeeptreatmentNon-invasive!– Complications
• Manypatientshavecavities/clipsfromprevioustreatmentsthatcanbeused
• Thinktwiceaboutusinggoldmarkers…

Prostategoldmarkersimplanted inliver
àalso CTfollow-upproblem

4DCTwithoutivcontrast(AveIP)

4DCTwithivcontrast(AveIP)
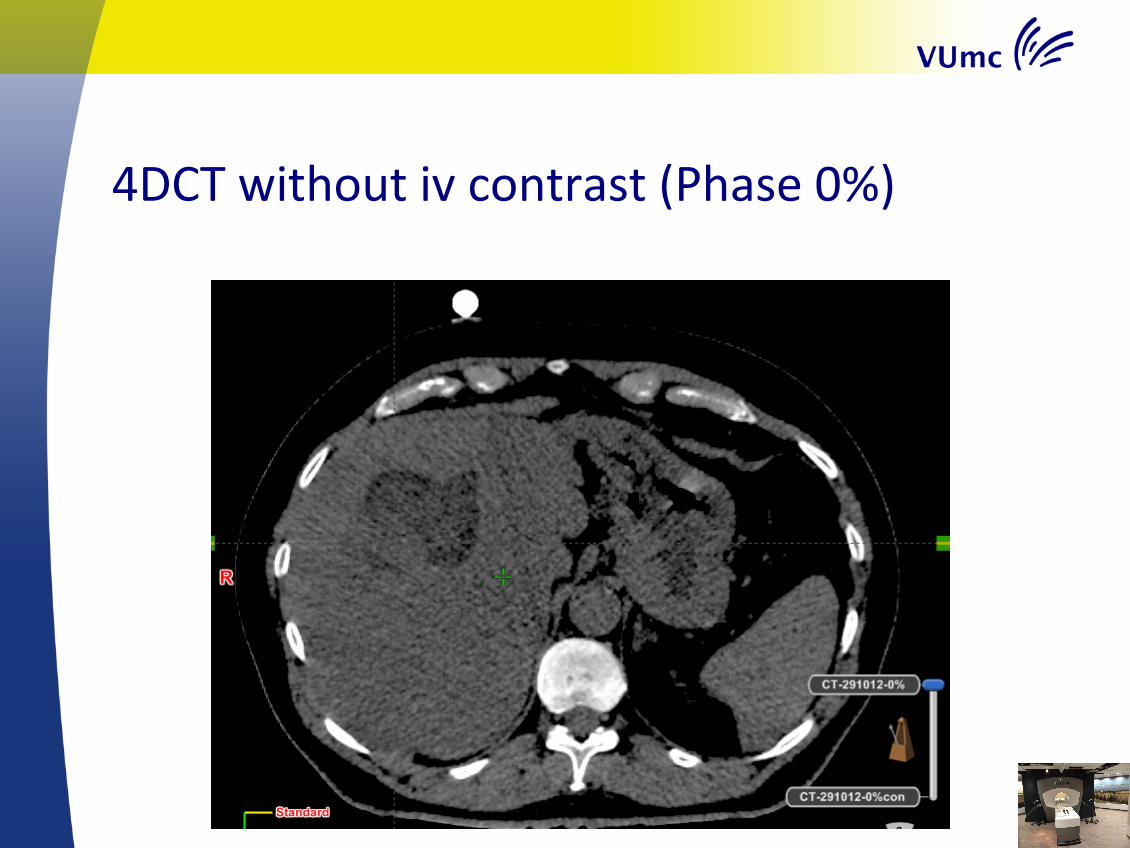
4DCTwithoutivcontrast(Phase0%)

4DCTwithivcontrast(Phase0%)

ITVincludingallmotiononcontrastenhanced4DCT
Delineation

MatchofdiagnosticPETtocontrastenhanced4DCT
Mismatchbetween diagnostic PETCTandplanning4DCT-mismatchPETCTand4DCT?-mismatchPETenlowdoseCT?-deformation ofliver?-differentbreathing pattern?(à insome centersmax inspiration diagnostic CTduring PET)
àDonot rely on diagnostic PETCTonly,dedicated RTimaging neededàSame problem applies todiagnostic MRI
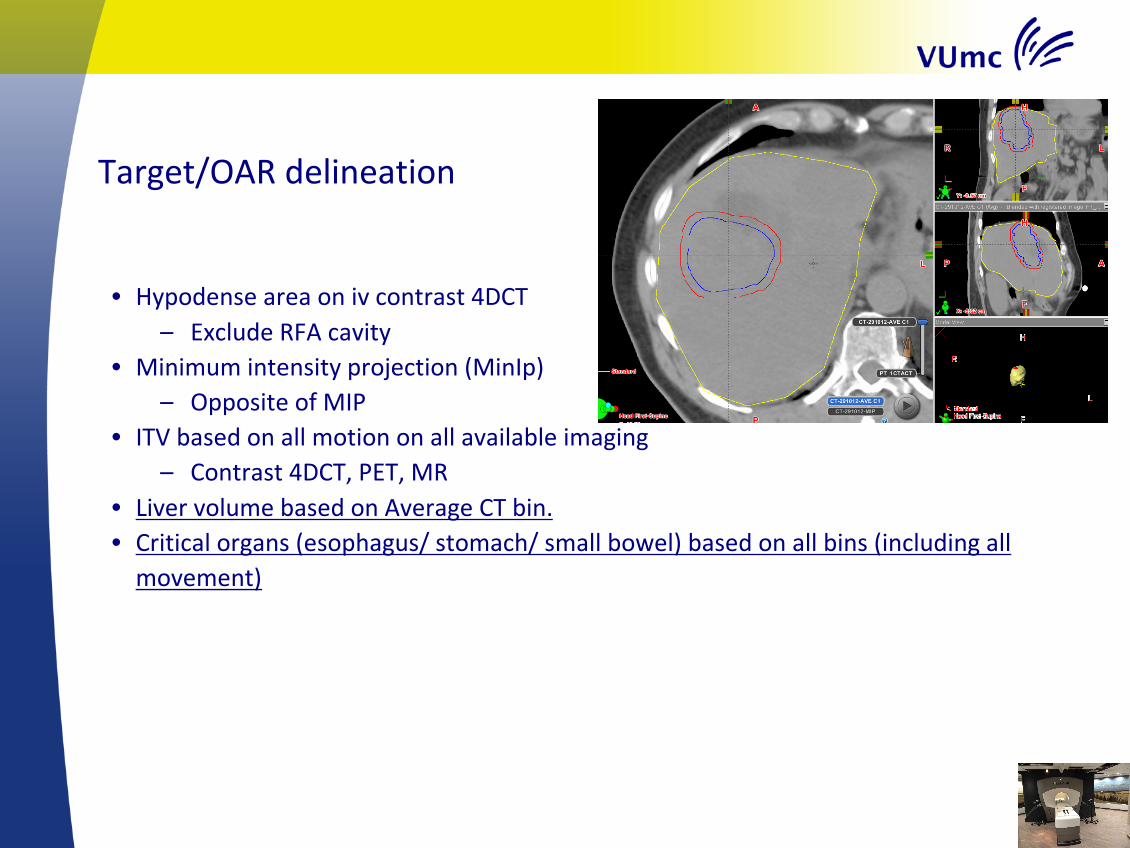
Target/OARdelineation
• Hypodense areaonivcontrast4DCT– ExcludeRFAcavity
• Minimumintensityprojection(MinIp)– OppositeofMIP
• ITVbasedonallmotiononallavailableimaging– Contrast4DCT,PET,MR
• LivervolumebasedonAverageCTbin.• Criticalorgans(esophagus/stomach/smallbowel)basedonallbins(includingallmovement)

ITV-PTVmargin5mm

Planning• DoseschedulesandplanningidenticaltolungSBRT
– Prescriptionisodose covers95%ofPTVvolume
– DosereductionofpartofPTVifnecessaryfororgansatrisk,andusemorefractionatedschedules(8-12x)
– RapidArc:2(partial)arcs
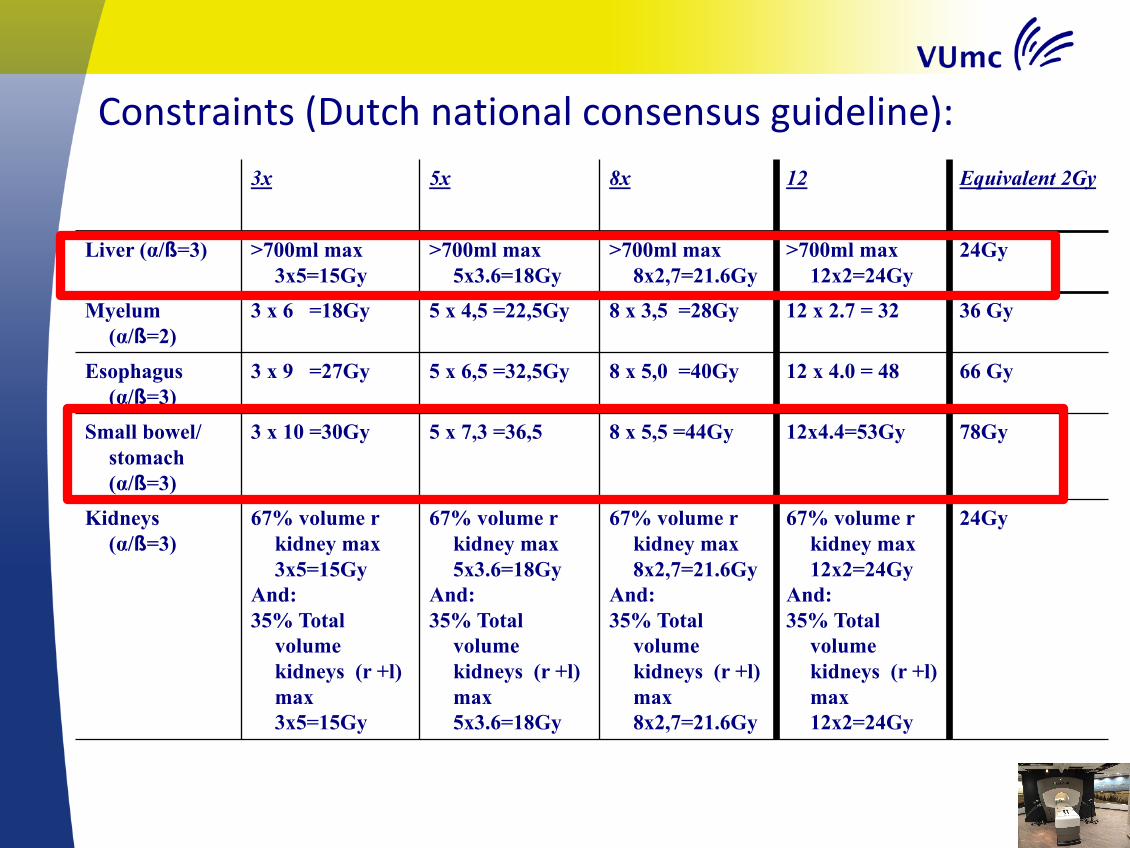
Constraints(Dutchnationalconsensusguideline):3x 5x 8x 12 Equivalent 2Gy
Liver (α/ß=3) >700ml max 3x5=15Gy
>700ml max 5x3.6=18Gy
>700ml max 8x2,7=21.6Gy
>700ml max 12x2=24Gy
24Gy
Myelum (α/ß=2)
3 x 6 =18Gy 5 x 4,5 =22,5Gy 8 x 3,5 =28Gy 12 x 2.7 = 32 36 Gy
Esophagus (α/ß=3)
3 x 9 =27Gy 5 x 6,5 =32,5Gy 8 x 5,0 =40Gy 12 x 4.0 = 48 66 Gy
Small bowel/ stomach (α/ß=3)
3 x 10 =30Gy 5 x 7,3 =36,5 8 x 5,5 =44Gy 12x4.4=53Gy 78Gy
Kidneys (α/ß=3)
67% volume r kidney max 3x5=15Gy
And:35% Total
volume kidneys (r +l) max 3x5=15Gy
67% volume r kidney max 5x3.6=18Gy
And:35% Total
volume kidneys (r +l) max 5x3.6=18Gy
67% volume r kidney max 8x2,7=21.6Gy
And:35% Total
volume kidneys (r +l) max 8x2,7=21.6Gy
67% volume r kidney max 12x2=24Gy
And:35% Total
volume kidneys (r +l) max 12x2=24Gy
24Gy

55Gy
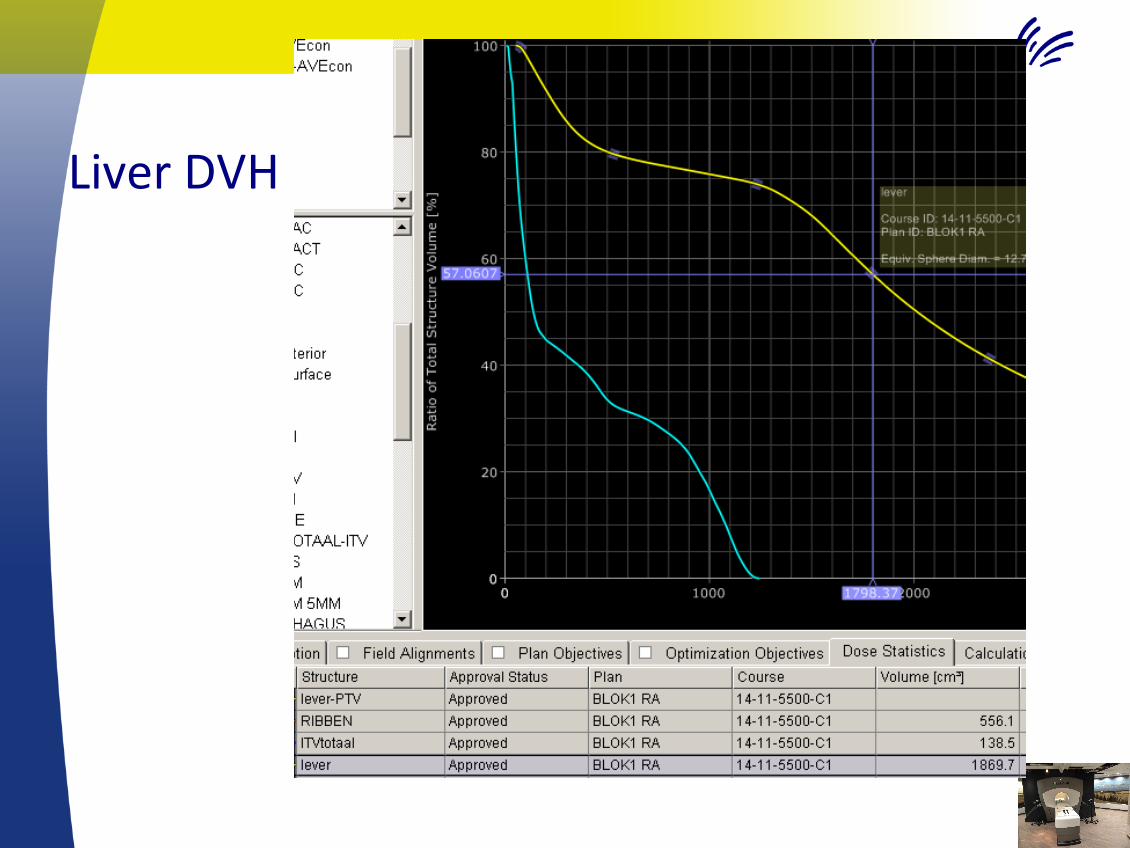
LiverDVH

Planning/treatmentdelivery:
• Standard:freebreathing
• Onlyinexceptionalcases(overlapboweletc):– Gatingduringin- orexpirationphases(audiocoaching)– Breathhold(FFF)
– Newimaging(breathhold oraudiocoachedCT)neededL

Treatmentdelivery• Patientpositioning:
– Dayly onlineCBCTsetupduringfreebreathing– CBCTqualitypoor– PTVmatchoftennotsensible(ITV/PTV/liverallgrey…)– Matchonlivercontourand/orcriticalorganatrisk– MakeuseofoldclipsandRFAcavities
– Intra-fractionmonitoringbreathingandpatientmotion:– RPMsystem/ExacTrac

CBCTPTVmatchimpossibe

CBCT(partial)livermatch

PTVmargins
• Theoretically5mmshouldbeenough….
• Clinicalpractice:liversmuchmoredifficultthanlung– ITVàPTVmargin1cmiffeasible(liverandotherconstraints).

Followup
• IfinRad Onc department:– 3-modiagnosticCTwithivcontrast.
• Bothhyperandhypodens areas(halo’s)described inthe>30GySBRTarea after 3-6months!
• Heavilypretreatedpatients:– OftenFUonlybyreferringphysician
– FrequentCTorPET/CT
GeneralPatientinformation
• Promisingtreatmentwithhighlocalcontrol(~lung>80%)
• Possibleacutetox:Nausea/pain
• Chanceofhighgradetoxicity– Dependingontumorlocation
– Smallbowel/esophagus/stomachperforation– Fibrosis/stenosis biliary tract
• Mostpatients:notoxicity!
àMostpatientsheavilypretreated- noother/betteroptions..

Generalremarks
• Nostandard profylactic medication (no dexa,no anti-emetics)
• Noroutineblood tests(except creatinine for iv contrast)

Conclusions/Takehome- LiverSBRT:
• ExcellentresultsforhighdoseSBRT
• Keepitsimple(useexperienceinlungSBRT)!
• Bewareofoverlapwithesophagus/stomach/bowelandlargechangesbetweenfractions
• Additionalcomparedtolung:– 4DCTusingivcontrast(extraprotocols/equipment)– Consider larger PTVmargin
• Liver istheideal indication for MRguided SBRT!

Questions…