clinical significance of serum insulin-like growth factor-1 (igf-1) and insulinlike growth factor...
TRANSCRIPT

RESEARCH ARTICLE
Clinical significance of serum insulin-like growth factor-1(IGF-1) and insulinlike growth factor binding protein-3(IGFBP-3) in patients with epithelial ovarian cancer
Faruk Tas & Senem Karabulut & Murat Serilmez &
Rumeysa Ciftci & Derya Duranyildiz
Received: 12 October 2013 /Accepted: 6 November 2013# International Society of Oncology and BioMarkers (ISOBM) 2013
Abstract Insulin-like growth factor-1 (IGF-1) and its primarybinding protein IGFBP-3 play an important role in cellularproliferation, differentiation, and apoptosis in many tumors,including ovarian cancer. The objective of this study was todetermine the clinical significance of the serum levels of IGF-1 and IGFBP-3 in epithelial ovarian cancer (EOC) patients. Atotal of 50 patients with a pathologically confirmed diagnosisof EOC were enrolled into this study. Serum IGF-1 andIGFBP-3 levels were determined by the solid-phase sandwichELISA method. Twenty age- and sex-matched healthy con-trols were included in the analysis. Median age of patients was56.5 years old (range 22 to 83 years). Majority of the patientshad advanced disease (FIGO stage III–IV; 90 %). No signif-icant difference was observed in baseline serum IGF-1 andIGFBP-3 levels between EOC patients and healthy controls(p =0.99 and p =0.80, respectively). The young patients hadhigher serum IGF-1 and IGFBP-3 concentrations (p =0.04and p =0.02, respectively). Patients with normal CA-125levels had higher serum IGFBP-3 concentrations comparedwith those with higher CA-125 levels (p =0.008). However,no other clinical variables including histology, tumor grade,stage of disease, and response to chemotherapy were found tobe correlated with serum IGF assays (p >0.05). A trend tosignificant relationship was found between the serum levels ofIGF-1 and IGFBP-3 (r s=0.212, p =0.07). The patients withelevated serum IGF-1 levels had favorable progression-freeand overall survivals than those with lower levels (p =0.04and p =0.03, respectively). However, serum IGFBP-3 concen-trations were found to have no prognostic role for both sur-vivals (p =0.12 and p =0.26, respectively). In conclusion,
elevated serum level of IGF-1 is associated with favorableprogression-free and overall survivals in EOC patients.
Keywords Serum . IGF-1 . IGFBP-3 . Ovarian cancer .
Prognostic factor
Introduction
Insulin-like growth factor-1 (IGF-1) is a multifunctional pep-tide, which plays an important role in cellular proliferation,differentiation, and apoptosis in many tumors, including epi-thelial ovarian cancer (EOC) [1–10]. In vitro studies show thatIGF-1 increases ovarian cell growth and invasive potential,suggesting a role of the IGF-1 pathway in ovarian canceretiology [1, 2]. Epidemiological data regarding plasma IGF-1 levels and EOC risk are conflicting [3]. Two prospectivestudies observed that plasma IGF-1 levels are associated withan increased risk of EOC among younger women [4, 5],whereas the other study suggested that it may be inverselycorrelated with EOC risk [6, 7]. These trials report lower IGF-1 concentrations in EOC patients compared with healthywomen.
The insulin-like growth factor binding protein (IGFBP)family of binding proteins consists of six structurally relatedproteins, and all members are expressed in the normal ovary[10]. Their role is to bind and regulate the effects of the IGFs.IGFBP-3 is the primary binding protein of IGF-1 and regu-lates the mitogenic and anti-apoptotic actions of IGFs [1–10].In addition, notably, IGFBP-3 has direct IGF-independenteffects on cellular growth and apoptosis. With respect toIGFBPs, prospective studies agree that there are no clearassociations of IGFBP-3 with EOC risk [4, 5, 7]. An associ-ation between serum levels of this family and the presence ofEOC has also been identified [6]. Serum levels of IGFBP-3
F. Tas (*) : S. Karabulut :M. Serilmez : R. Ciftci :D. DuranyildizInstitute of Oncology, University of Istanbul, Capa, 34390 Istanbul,Turkeye-mail: [email protected]
Tumor Biol.DOI 10.1007/s13277-013-1405-8

are significantly decreased in EOC patients relative to thosewith benign tumors and healthy controls [6, 11]. Moreover, inEOCs, IGFBP-3 has been associated with disease stage andresidual tumor volume when measured by ELISA or by quan-titative reverse transcription PCR [12, 13].
The significance of the serological levels of IGF-1 andIGFBP-3 in EOC patients is not known yet. Given the con-flicting results from recent epidemiological studies examiningthe IGF axis and EOC, we conducted this study to test thediagnostic, predictive, and prognostic roles of serum IGF-1and IGFBP-3 concentrations in EOC patients.
Materials and methods
Patients
A total of 50 EOC patients with histologically proven diag-nosis treated at Istanbul University Institute of Oncology wereenrolled into the study. The staging was established in accor-dance with the International Federation of Gynecologists andObstetricians (FIGO) classification. Patients with stage IIIwith bulky disease or stage IV disease were initially treatedwith neoadjuvant chemotherapy and operated afterwards.Patients with operable stage III disease who had under-gone primary surgery consisting of total abdominal hys-terectomy, bilateral salpingo-oophorectomy, appendecto-my, omentectomy, and pelvic and/or para-aortic lymph-adenectomy were treated with adjuvant chemotherapy.All patients received standard paclitaxel–carboplatin-containing chemotherapy regimen.
For comparison of serum IGF-1 and IGFBP-3 levels, 20age- and sex-matched healthy controls were included in theanalysis. Informed consent was obtained from all patients, andthe study was reviewed and approved by a local ethicalcommittee.
Measurement of serum IGF-1 and IGFBP-3 levels
Serum samples were obtained on first admission before anyadjuvant and metastatic treatment was given and patients werefollowed up. Blood samples were obtained from EOC patientsand healthy controls by venipuncture and clotted at roomtemperature. The sera were collected following centrifugationand frozen immediately at −20 °C until analysis.
Serum IGF-1 (Mediagnost, Germany) and IGFBP-3(Mediagnost, Germany) levels were determined by the solid-phase sandwich ELISA method.
The IGF-1 ELISA (Mediagnost, Germany) uses a double-antibody sandwich enzyme-linked immunosorbent assay todetermine the level of human IGF-1 in samples. Serum sam-ples and standards were added to the wells which are pre-coated with human IGF-1 monoclonal antibody. IGF-1
monoclonal antibody was allowed to incubate for 1 h. Theunbound material was washed away. Biotin-conjugated anti-human IGF-1 antibody and streptavidin–horseradish peroxi-dase (HRP) were added to incubate for 30 min. Biotin-conjugated anti-human IGF-1 antibody binds to human IGF-1 captured by the first antibody. Streptavidin–HRP binds tothe biotin-conjugated anti-human IGF-1 antibody. Followingincubation (30 min), unbound streptavidin–HRP was re-moved during a wash step, and a substrate solution reactive
Table 1 Characteristicsof the patients anddisease
Variables Number
No. of patients 50
Age of patients (year)
<55 24
≥55 26
Histology
Serous papillary 21
Endometrioid 5
Mixed 4
Clear cell 2
Mucinous 1
Undifferentiated 17
Histological grade
I 2
II 6
III 13
Stage of disease
I–II 5
III 33
IV 12
CA-125 level (35 IU/mL)
Normal 10
High 40
Response to chemotherapy
Yes 25
No 12
Platinum sensitivity in relapse
Sensitive 8
Resistant 15
Table 2 The values of serum marker levels in EOC patients and inhealthy controls
Assay Patients (n=50) Controls (n=20) p value
Median Range Median Range
Serum IGF-1level (ng/mL)
43.7 9.2–245.1 45.9 7.9–97.8 0.99
Serum IGFBP-3level (ng/mL)
5,286.3 1,957.9–9,750.5
5,249.2 2,717.9–6,834.2
0.80
Tumor Biol.
with HRP was added to the wells and incubated for 15 min. Acolored product was formed in proportion to the amount ofhuman IGF-1 present in the sample or standard. The reactionwas terminated by an addition of acid (stop solution), andabsorbance is measured at 450 nm using an automated ELISA
reader (Rayto, RT-1904C Chemistry Analyzer, Atlanta, GA,USA). The results were expressed as nanograms per milliliter.
The IGFBP-3 ELISA (Mediagnost, Germany) uses adouble-antibody sandwich enzyme-linked immunosorbent as-say to determine the level of human IGFBP-3 in samples.
Table 3 Results (median andrange) of comparisons betweenthe assays and various clinical/laboratory parameters
Variables IGF-1 IGFBP-3(ng/mL) (ng/mL)
Age, years (p) 0.04 0.02
Young (<55) 53.9 (9.2–245.1) 5,465.9 (2,147.3–9,750.5)
Older (≥55) 40.3 (9.9–212.9) 4,791.4 (1,957.9–7,389.2)
Histology (p) 0.61 0.62
Serous papillary 50.5 (13.1–173.7) 4,819.2 (2,116.0–9,750.5)
Others 45.6 (9.2–245.1) 5,380.3 (1,957.9–8,093.6)
Grade (p) 0.21 0.86
I+II 60.0 (23.6–173.7) 5,838.6 (3,570.4–8,093.6)
III 45.5 (10.3–126.5) 5,464.6 (3,463.8–9,526.3)
Stage (p) 0.60 0.25
Non-metastatic 47.7 (9.2–245.1) 5,383.3 (1,957.9–9,750.5)
Metastatic 36.6 (10.3–212.9) 4,915.4 (2,116.0–6,539.8)
Serum CA-125 level (p) 0.27 0.008
Normal 51.0 (12.0–245.1) 6,446.0 (3,570.4–8,093.6)
High 42.7 (9.2–221.9) 4,901.8 (1,957.9–9,750.5)
Response to chemotherapy (p) 0.76 0.69
Yes 42.8 (9.2–212.9) 5,038.4 (2,116.0–9,750.5)
No 42.6 (21.9–187.7) 4,804.8 (1,957.9–6,539.8)
Platinum sensitivity in relapse (p) 0.48 0.59
Sensitive 42.3 (9.2–212.9) 4,648.3 (2,116.0–6,868.0)
Resistant 43.0 (21.9–187.7) 5,038.4 (1,957.9–7,389.2)
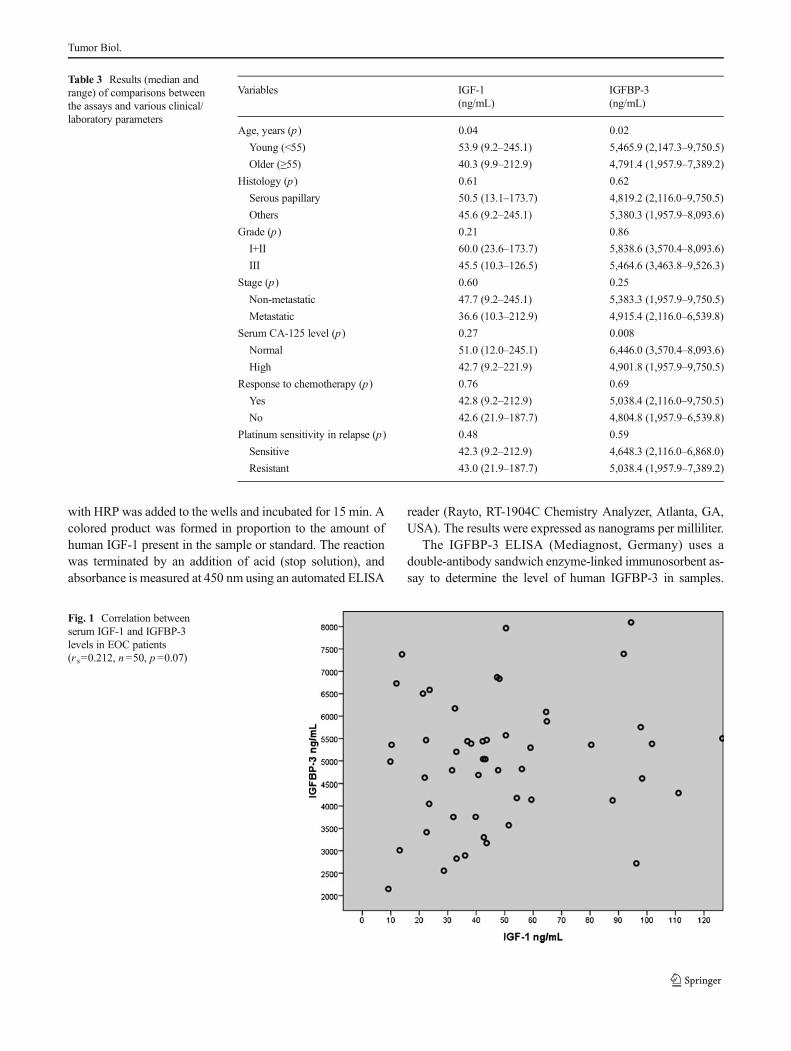
Fig. 1 Correlation betweenserum IGF-1 and IGFBP-3levels in EOC patients(r s=0.212, n=50, p =0.07)
Tumor Biol.

Serum samples and standards were added to the wellswhich are pre-coated with human IGFBP-3 monoclonalantibody. IGFBP-3 monoclonal antibody was allowed toincubate for 1 h. The unbound material was washedaway. Biotin-conjugated anti-human IGFBP-3 antibodyand streptavidin–HRP were added to incubate for 1 h.Biotin-conjugated anti-human IGFBP-3 antibody bindsto human IGBP-3 captured by the first antibody.Streptavidin–HRP binds to the biotin-conjugated anti-human IGBP-3 antibody. Following incubation(30 min), unbound streptavidin–HRP was removed dur-ing a wash step, and a substrate solution reactive withHRP was added to the wells and incubated for 30 min.A colored product was formed in proportion to theamount of human IGBP-3 present in the sample or
standard. The reaction was terminated by an additionof acid (stop solution), and absorbance was measured at450 nm using an automated ELISA reader (Rayto, RT-1904C Chemistry Analyzer, Atlanta, GA, USA). Theresults were expressed as nanograms per milliliter.
Statistical analysis
Continuous variables were categorized using median valuesas cutoff point. Assessment of relationships, comparisonsbetween various clinical/laboratory parameters, was accom-plished using the Mann–Whitney U test. Overall survival(OS) was calculated from the date of first admission to theclinics to the disease-related death or date of last contact withthe patient or any family member. Progression-free survival(PFS) was calculated from the date of admission to the date offirst radiologic progression with/without elevated serum tu-mor marker. The Kaplan–Meier method was used for estima-tion of survival distribution, and differences in survival wereassessed by the log-rank statistics. A p value <0.05 wasconsidered significant. Statistical analysis was carried outusing SPSS 16.0 software.
Results
A total of 50 patients with a pathologically confirmed diag-nosis of EOC were enrolled into this study. Baseline histo-pathological characteristics and demographic features of pa-tients are listed in Table 1. Median age of patients was56.5 years old (range 22 to 83 years). Majority of the patientshad advanced disease (FIGO stage III–IV; 90 %).
No significant difference was observed in baseline serumIGF-1 and IGFBP-3 levels between EOC patients and controls(p =0.99 and p =0.80, respectively; Table 2). Table 3 showsthe correlations between the serum assay levels and clinico-pathological factors. The young patients had higher serumIGF-1 and IGFBP-3 concentrations (p =0.04 and p =0.02,respectively). Patients with normal CA-125 levels had higherserum IGFBP-3 concentrations compared with those withhigher CA-125 levels (p =0.008). However, no other clinicalvariables including histology, tumor grade, stage of disease,and response to chemotherapy were found to be correlatedwith serum IGF assays (p >0.05).
A trend to significant relationship was found between theserum levels of IGF-1 and IGFBP-3 (r s=0.212, n =50,p =0.07, Spearman's correlation; Fig. 1).
The median follow-up time was 12 months (range 1–78 months). Median progression-free survival for allpatients was 8±2.8 months (95 % confidence interval(95 %CI)=3–14 months). The 1-year progression-freesurvival rate was 27.3 % (95 %CI=8.7–45.9). Medianoverall survival for all patients was 52±7.5 months
Table 4 Univariate analyses of progression-free and overall survivals
Variables Survival (month)
Progression-freesurvival
Overallsurvival
Median (±SE) Median (±SE)
Age, years (p) 0.60 0.12
Young (<55) 29.3 (9.9) 61.2 (8.9)
Older (≥55) 12.6 (2.6) 24.1 (2.3)
Histology (p) 0.85 0.74
Serous papillary 10.4 (2.2) 26.8 (2.6)
Others 27.3 (7.1) 52.6 (9.5)
Grade (p) 0.78 0.17
I+II 10.0 (0.0) NR
III 9.4 (3.1) NR
Stage (p) 0.76 0.34
Non-metastatic 25.0 (7.0) 55.4 (8.3)
Metastatic 14.5 (3.6) 24.2 (4.3)
Serum CA-125 level (p) 0.06 0.11
Normal 52.0 (0.0) NR
High 8.3 (1.4) NR
Response to chemotherapy (p) <0.001 <0.001
Yes 34.2 (7.0) 60.2 (7.9)
No 3.3 (0.5) 14.5 (4.5)
Platinum sensitivity in relapse(p)
0.001 0.003
Sensitive 46.2 (5.3) 66.0 (10.4)
Resistant 6.9 (1.5) 15.1 (3.2)
Serum IGF-1 level (p) 0.04 0.03
High (>median) 14.0 (2.9) 70.2 (5.3)
Low (<median) 5.0 (1.3) 23.2 (2.8)
Serum IGFBP-3 level (p) 0.12 0.26
High (>median) 8.0 (4.4) 64.5 (6.1)
Low (<median) 5.0 (0.7) 25.1 (2.2)
NR not reached
Tumor Biol.

(95 %CI=37–67 months). The 1-, 2-, and 3-year overallsurvival rates were 84.9 % (95 %CI=73.5–96.2), 77 %(95 %CI=62.3–91.7), and 55 % (95 %CI=27–83), re-spectively. Patients with no chemotherapy response andwith platinum resistance in relapsed disease had worseoutcome in both PFS and OS analyses (Table 4). Thepatients with elevated serum IGF-1 levels had favorablePFS and OS than those with lower levels (p =0.04 andp =0.03, respectively; Table 4 and Fig. 2a, b). However,serum IGFBP-3 concentrations were found to have noprognostic role for PFS and OS (p =0.12 and p =0.26,respectively; Table 4 and Fig. 3a, b).
Discussion
In the literature, only a limited number of studies have inves-tigated serum IGF-1 and IGFBP-3 concentrations in humanEOC [6, 8, 9, 11–13]. A small pioneering study by Flyvberget al. performed an RIA for IGFBP-3 and a Western ligandblotting (WLB) in serum samples from 20 patients with EOC,10 patients with benign ovarian tumors, and 8 age-matchedhealthy controls [11]. Serum IGFBP-3 was decreased in pa-tients with EOC and not correlated with CA-125. Additional-ly, no difference was seen between tumor staging and levels ofserum IGFBP-3.
Fig. 2 a Progression-freesurvival curves in EOC patientsaccording to IGF-1 levels(p =0.04). b Overall survivalcurves in EOC patients accordingto IGF-1 levels (p =0.03)
Tumor Biol.

Subsequently, in order to study the role of IGFBP-3 in EOCprogression, Katsaros et al. measured IGFBP-3 concentrationsin tumor tissues from 147 patients with EOC and examinedtheir associations with clinicopathological features of the dis-ease and patient survival [12]. IGFBP-3 levels were measuredwith a commercial immunoassay kit. Low IGFBP-3 levelswere significantly associated with unfavorable prognostic fea-tures of the disease and a significantly increased risk of diseaseprogression (p =0.034), but the association was not sustainedwhen other clinical and pathological variables were adjustedfor in the analysis. No significant associations were observedbetween the IGFBP-3 level and patients' overall survival andresponse to chemotherapy. Findings of the study indicate that
IGFBP-3 may play a role in the progression of EOC, but it hasno independent value in predicting either disease prognosis orthe response of patients to chemotherapy.
In a preliminary study, mean preoperative blood IGF-1levels were significantly higher in patients younger than50 years old (p =0.01) [8]. In contrast, mean preoperativeIGFBP-3 levels were significantly higher in patients withnon-serous histology when compared with those with seroushistology (p =0.03). Also, preoperative serum IGF-1 andIGFBP-3 levels were significantly higher in patients withnormal preoperative CA-125 levels. These preliminary find-ings suggested that preoperative blood IGF-1 and IGFBP-3levels may be used as a marker in young patients with normal
Fig. 3 a Progression-freesurvival curves in EOC patientsaccording to IGFBP-3 levels(p =0.12). b Overall survivalcurves in EOC patients accordingto IGFBP-3 levels (p =0.26)
Tumor Biol.

serum CA-125 levels and/or patients with non-serous ovariantumors. As a result of these results, the authors believe thatpreoperative IGF-1 and IGFBP-3 levels may be used as adiagnostic tool for adnexal masses in the reproductive agegroup and/or as a screening marker in the normal population.
In another study by Baron-Hay et al., serum sampleswere collected from women newly diagnosed with EOC(n =99) before debulking surgery [6]. Both IGF-1 andIGFBP-3 levels were significantly lower in women withovarian cancer compared with women with benign pathol-ogy and control groups. These levels also have no signif-icant difference between the levels analyzed for tumorstage, histological grade, degree of surgical debulking,or neoadjuvant chemotherapy. Moreover, the serum IGF-1 and IGFBP-3 concentrations were found to be stronglypositively interrelated (r =0.64, p <0.0001). Afterwards,Lu et al. studied fresh tumor specimens from 215 patientswith primary EOC and analyzed for IGFBP-3 expressionsusing quantitative reverse transcription PCR. IGFBP-3expression was higher in less aggressive tumors but wasnot associated with disease progression [13]. The studyalso indicated that IGFBP-3 have a limited value in prog-nosis because of their strong associations with diseasestage and tumor grade.
These assays were also studied in only postmenopausalpatients preoperatively [9]. Serum IGF-1 concentrations sig-nificantly decreased in patients with malignant (n =23) andbenign ovarian tumors (n =24) compared with controls. Se-rum IGFBP-3 concentrations were also found to be lower inwomen with malignant ovarian tumors than in women withbenign tumors. The present data suggest that low concentra-tions of IGF-1 and IGFBP-3 could be a reliable marker todifferentiate benign from malignant ovarian tumors.
In this trial, we studied serum IGF-1 and IGFBP-3 levels in50 patients with a pathologically confirmed diagnosis of EOCand 20 age- and sex-matched healthy controls determined bythe solid-phase sandwich ELISA method. No significant dif-ference was observed in baseline serum IGF-1 and IGFBP-3levels between EOC patients and healthy controls. The youngpatients had higher serum IGF-1 and IGFBP-3 concentrations.Patients with normal CA-125 levels had higher serum IGFBP-3 concentrations compared with those with higher CA-125levels. However, no other clinical variables including histolo-gy, tumor grade, stage of disease, and response to chemother-apy were found to be correlated with serum levels. A trend tosignificant relationship was found between the serum levels ofIGF-1 and IGFBP-3 (r s=0.212, p =0.07). The patients withelevated serum IGF-1 levels had favorable PFS and OS thanthose with lower levels. However, serum IGFBP-3 concentra-tions were found to have no prognostic role for both survivals.In conclusion, we found that elevated serum level of IGF-1 isassociated with favorable progression-free and overall sur-vivals in EOC patients.
In conclusion, although little is known, evidence to datesuggests that the IGF family may be involved in the etiologyand progression of EOC. However, there are much conflictingevidences in the literature regarding the patterns of expressionof these gene products; therefore, the precise functional rele-vance of these alterations is not yet well understood. Similarcomments were true for patterns of quantifying the circulatingserum IGF concentrations. The small sample size of our studycould be considered as a significant limitation and might haveinfluenced these results. However, our study contributes to theliterature. A standardized method remains to be establishedand validated in larger series of patients in prospective studiesto determine the potential clinical significance of these assaysin EOC patients.
References
1. Resnicoff M, Ambrose D, Coppola D, Rubin R. Insulin-likegrowth factor-1 and its receptor mediate the autocrine prolif-eration of human ovarian carcinoma cell lines. Lab Investig.1993;69:756–60.
2. Khandwala HM, McCutcheon IE, Flyvberg A, Friend KE. Theeffects of insulin-like growth factors on tumorigenesis and neoplasticgrowth. Endocrinol Rev. 2000;21:215–44.
3. Terry KL, Tworoger SS, Gates MA, Cramer DW, Hankinson SE.Common genetic variation in IGF1, IGFBP1 and IGFBP3 and ovar-ian cancer risk. Carcinogenesis. 2009;30:2042–6.
4. Lukanova A, Lundin E, Toniolo P, Micheli A, AkhmedkhanovA, Rinaldi S, et al. Circulating levels of insulin-like growthfactor-1 and risk of ovarian cancer. Int J Cancer. 2002;101:549–54.
5. Peeters PH, Lukanova A, Allen N, Berrino F, Key T, Dossus L,et al. Serum IGF-1, its major binding protein (IGFBP-3) andepithelial ovarian cancer risk: the European ProspectiveInvestigation into Cancer and Nutrition (EPIC). Endocr RelatCancer. 2007;14:81–90.
6. Baron-Hay S, Boyle F, Ferrier A, Scott C. Elevated seruminsulin-like growth factor binding protein-2 as a prognosticmarker in patients with ovarian cancer. Clin Cancer Res.2004;10:1796–806.
7. Tworoger SS, Lee IM, Buring JE, Pollak MN, Hankinson SE.Insulin-like growth factors and ovarian cancer risk: a nested case–control study in three cohorts. Cancer Epidemiol Biomarkers Prev.2007;16:1691–5.
8. Dursun P, GultekinM, Esin S. Preoperative serum IGF-1 and IGFBP-3 levels in patients with ovarian carcinoma: preliminary results. Int JGynecol Cancer. 2004;14 Suppl 1:105–6.
9. Serin IS, Tanriverdi F, Yilmaz MO, Ozcelik B, Unluhizarci K.Serum insulin-like growth factor (IGF)-1, IGF binding protein(IGFBP)-3, leptin concentrations and insulin resistance in be-nign and malignant epithelial ovarian tumors in postmenopausalwomen. Gynecol Endocrinol. 2008;24:117–21.
10. El-Roiey A, Chen A, Roberts VJ, LeRoith D, Roberts CT,Yen SS. Expression of insulin-like growth factors (IGF-I andII), the IGF and insulin receptors, and IGF-binding proteins1–6 and the localization of their gene products in normal andpolycystic ovary syndrome ovaries. J Clin Endocrinol Metab.1994;78:1488–96.
Tumor Biol.

11. Flyvberg A, Mogensen O, Mogensen B, Nielsen OS. Elevated seruminsulin-like growth factor-binding protein 2 (IGFBP-2) and decreasedIGFBP-3 in epithelial ovarian cancer: correlation with cancer antigen125 and tumour-associated trypsin inhibitor. J Clin EndocrinolMetab. 1997;82:2308–13.
12. Katsaros D, Yu H, Levesque MA, Danese S, Genta F, Richiardi G,et al. IGFBP-3 in epithelial ovarian cancer and its association with
clinico-pathological features and patients survival. Eur J Cancer.2001;37:478–85.
13. Lu L, Katsaros D, Wiley A, Rigault de la Longrais IA, Risch HA,Puopolo M, et al. The relationship of insulin-like growth factor-II,insulin-like growth factor binding protein-3, and estrogen receptor-alpha expression to disease progression in epithelial ovarian cancer.Clin Cancer Res. 2006;12:1208–14.
Tumor Biol.